
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Cell. Infect. Microbiol. , 24 September 2020
Sec. Fungal Pathogenesis
Volume 10 - 2020 | https://doi.org/10.3389/fcimb.2020.574584
 Duc Nguyen1,2
Duc Nguyen1,2 Mathieu Nacher2,3,4*Loic Epelboin2Alessia Melzani2
Mathieu Nacher2,3,4*Loic Epelboin2Alessia Melzani2 Magalie Demar4,5,6Denis Blanchet5,6Romain Blaizot7Kinan Drak Alsibai8Philippe Abboud2Félix Djossou2,5Pierre Couppié4,7Antoine Adenis1,3
Magalie Demar4,5,6Denis Blanchet5,6Romain Blaizot7Kinan Drak Alsibai8Philippe Abboud2Félix Djossou2,5Pierre Couppié4,7Antoine Adenis1,3Introduction: Haemophagocytic Lymphohistiocytosis (HLH), during HIV infection is a rare complication with a poor prognosis. There are few data on HLH within the Amazon region. The objective was to describe epidemiological, clinical and therapeutic features of HIV-related HLH in French Guiana.
Methods: A retrospective analysis of adult HIV patients at Cayenne hospital with HLH between 2012 and 2015. A diagnosis of HLH was given if the patient presented at least 3 of 8 criteria of the HLH-2004 classification.
Results: Fourteen cases of HLH were tallied during the study period. The mean age was 46 years with a sex ratio of 1.8. The most frequent etiology of HLH was an associated infection (12/14). Confirmed disseminated histoplasmosis, was found in 10 of 14 cases, and it was suspected in 2 other cases. The CD4 count was below 200/mm3 in 13/14 cases. An HIV viral load >100,000 copies/ml was observed in 13/14 cases. An early treatment with liposomal amphotericin B was initiated in 12/14 cases. The outcome was favorable in 12/14 of all cases and in 10/12 cases involving histoplasmosis. Case fatality was 2/14 among all cases (14.3%) et 1/10 among confirmed disseminated histoplasmosis with HLH (10%). During the study period 1 in 5 cases of known HIV-associated disseminated histoplasmosis in French Guiana was HLH.
Conclusion: Histoplasmosis was the most frequent etiology associated with HLH in HIV-infected patients in French Guiana. The prognosis of HLH remains severe. However, a probabilistic empirical first line treatment with liposomal amphotericin B seemed to have a favorable impact on patient survival.
French Guiana is the French overseas territory where the HIV epidemic is most important (Nacher et al., 2018). The most frequent opportunistic infection in HIV patients is disseminated histoplasmosis, and it has long been the first cause of AIDS-related death (Nacher et al., 2011). Hence the overall incidence of disseminated histoplasmosis in a cohort of HIV-infected persons was 1.5 per 100 person-years, but for persons with CD4 counts <50 per mm3 it was >10 per 100 person-years (Nacher et al., 2014). For tuberculosis, the incidence in the HIV cohort was 0.9 per 100-person years. In Latin America, it has been described as a neglected disease (Nacher et al., 2013), and the burden of disseminated histoplasmosis among persons with HIV is estimated to be on par with that of tuberculosis (Nacher et al., 2016; Adenis et al., 2018). The Haemophagocytic Lymphohistiocytosis (HLH) is a rare, but often fatal, syndrome of immune hyperactivation corresponding to a cytokine storm. The HLH-2004 definition criteria require either a molecular diagnosis or five of the eight following criteria: fever, splenomegaly, cytopenias affecting at least two of three lineages, hyperferritinemia, hypertriglyceridemia and/or hypofibrinogenemia, low or absent natural killer (NK)-cell activity, elevated soluble CD25 and confirmatory evidence of hemophagocytosis in the bone marrow, the spleen or the lymph nodes (Henter et al., 2007). Genetic mutations can cause HLH, usually in children. Trigger factors such as infection, immunodeficiency, neoplasm, autoimmunity commonly causes HLH in adults (Hayden et al., 2016). HLH has been previously reported among HIV patients with and without disseminated infections. HLH is notably a known complication of acute disseminated histoplasmosis in both HIV+ and HIV- patients (Subedee and Van Sickels, 2015; Townsend et al., 2015; Jabr et al., 2019). Besides histoplamosis, the main etiology for HLH in AIDS patients are Kaposi sarcoma or lymphoma (B cell, T cell, or primary effusion lymphoma), but also toxoplasmosis, CMV disease, mycobacterial infections, and other opportunistic infections, such as candidiasis and pneumocystosis (Bhatia et al., 2003). HLH may also occur during primary HIV infection or Immune Reconstitution Inflammatory Syndrome (IRIS) (Sun et al., 2004; Breton et al., 2006; Melzani et al., 2020). Treatment mostly relies on treatment of histoplasmosis and HIV, corticosteroids, certain chemotherapeutic agents (etoposide), and interleukin-1 receptor antagonists and immune globulins (Ocon et al., 2017). HLH during HIV infection remains a rare event, which has been rarely described, especially in our Amazonian context. Our initial hypothesis was that disseminated histoplasmosis was the main cause of HLH in HIV-infected persons and that antifungals targeting this pathogen would have a beneficial role on prognosis. We therefore conducted an observational retrospective study with the objectives of describing the particularities of HLH in HIV-infected adults in French Guiana.
The study was observational, monocentric, descriptive, and retrospective between 01/01/2012 and 05/01/2016.
The study involved the hospital wards caring for HIV-infected patients requiring hospitalization.
The source population consisted of patients hospitalized in Cayenne hospital between 01/01/2012 and 05/01/2016 and with HIV-specific ICD 10 principal or associated diagnostic codes in the hospital information database. Another source was HIV infected patients included in the HIV computerized medical records eNADIS® (Figure 1). The target population consisted of patients having presented a HLH during their hospital stay.
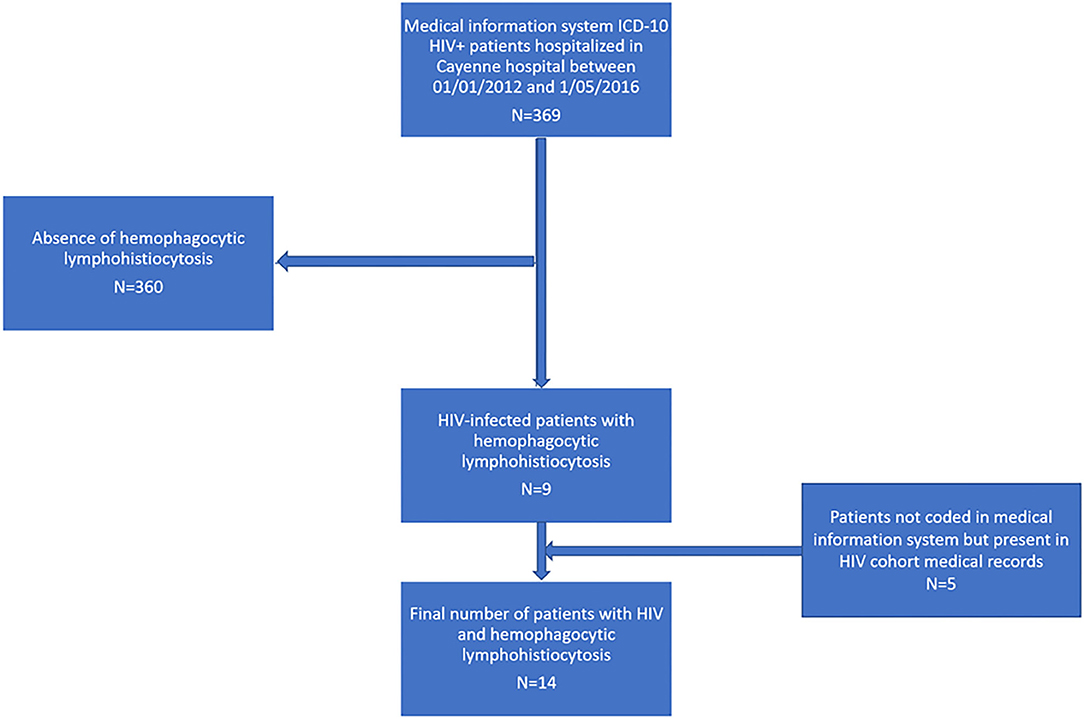
Figure 1. Inclusion diagram of HIV-infected patients with a hemophagocytic lymphohistiocytosis in Cayenne Hospital between 2012 and 2015.
- Person aged ≥ 18 years
- Confirmed HIV Infection (2 ELISA tests and 1 Western-Blot confirmation).
- ICD 10 Codes CIM-10 as principal diagnosis or associated diagnosis: hemophagocytic syndrome (D761, D762, D763) and HIV infection (B20, B21, B22, B23, B24).
- Diagnosis of the HLH in the eNADIS computerized medical records.
- Less than 3 of 8 diagnostic criteria HLH-2004 (Henter et al., 2007).
- HScore (Fardet et al., 2014) below 169 corresponding to a sensitivity of 93% and a specificity of 86%.
The main judgement criterion was the presence or absence of a HLH defined according to the HLH-2004 diagnostic criteria (Henter et al., 2007).
A diagnosis of HLH was given if the patient presented at least 3 of 8 criteria of the HLH-2004 classification (Henter et al., 2007). This definition was chosen in order to be more sensitive, and thus to avoid missing cases. A probability HScore was given for each patient as defined by Fardet et al. (2014) in order to refine the specificity of the diagnosis.
The identification of target patients required queries in the hospital medical information system Programme de Médicalisation des Systèmes d'Information (PMSI, which includes the main diagnoses and is used to calibrate hospital funding) and eNADIS® a specialized patient record system for HIV patients, which includes detailed follow up data. The modalities of the queries were guided by the ICD-10 codes for HLH as principal diagnosis which allowed obtaining patient identities and dates of hospitalization. Medical records were then reviewed before inclusion in order to extract information. The eNADIS® medical records of the Hospital cohort (>1,200 outpatients, ~90 hospitalizations of HIV patients with opportunistic infections per year; Figure 1) were also searched to identify records with a history of HLH.
For included patients, data were retrospectively collected at Cayenne General Hospital from medical records. Data collection included socio-demographic variables (sex, age, and country of birth), medical data (including general condition, fever, pulmonary signs, digestive signs, lymphadenopathies.) imagery data (chest X ray, CT scan, ultrasound, endoscopy results), biological results (hemoglobin, leukocytes, CRP, LDH, ferritin, albumin etc.), microbiological data (direct examination, culture, pathology, PCR), immunovirological data (CD4 and CD8 counts, viral load before antiretroviral therapy and at the time of HLH) therapeutic data (antifungals, antibiotics, corticosteroids, antiretrovirals.) and the last consultation date after the considered HLH.
In conformity with the diagnostic criteria defining HLH, the highest values during hospitalization of the variables: temperature, aspartate aminotransferase (ASAT), triglycerides and ferritine, and the lowest values of the variables hemoglobin, leukocytes, platelets, fibrinogen were specifically collected at the time of hospitalization for this study.
The data from the study were analyzed using Stata 12 (®College Station, Texas, USA) and Microsoft Excel 2013. Descriptive analysis allowed describing sociodemographic, clinical, immunovirological, and therapeutic data. Means and standard deviations, or medians and interquartile ranges, were used depending on the variable distribution.
All HIV-infected patients followed at Cayenne Hospital are included in the DAT'AIDS® database. This database allows the clinical care of HIV patients with the eNADIS® computerized medical records. It is part of the French Hospital Database on HIV (FHDH), a national cohort which has led to numerous scientific publications. This database received approval from the Commission Nationale Informatique et Libertés (CNIL) since 27/11/1991. All included patients signed an informed consent form after presentation of the database by the treating physician. The present analysis was hence part of the ongoing approved hospital cohort study and did not require any additional approval.
This retrospective study allowed identifying 14 HIV-infected patients presenting a confirmed or suspected HLH between the 01/01/2012 and the 05/01/2016. Figure 1 shows the study flowchart. During the time period considered there were 57 cases of disseminated histoplasmosis in Cayenne Hospital, among which 10 (17.5%) were HLH cases.
In our series, 3 patients presented only 3 of 8 HLH-2004 criteria and 6 patients presented at least 5 of 8 HLH-2004 criteria. The HScore was >200, corresponding to a probability of 89% to have a HLH in 13/14 patients. Only one patient had an HScore of 183 and 3 of 8 HLH-2004 criteria (Table 1).
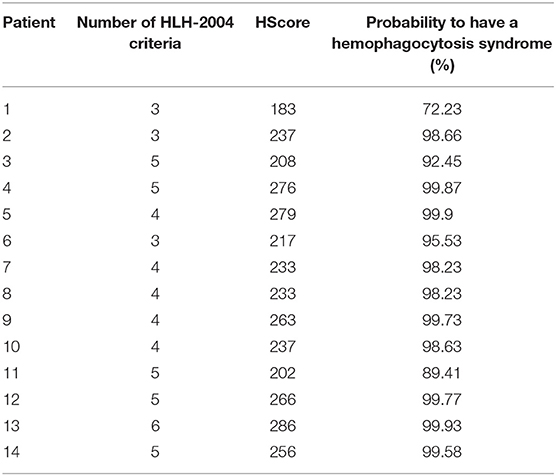
Table 1. Diagnostic criteria for hemophagocytic lymphohistiocytosis and patient HScore.
Among the 14 patients, 9 were males (M/F sex ratio = 1.8), the mean age was 46 ± 6 years. Among 14 patients 4 were French born, including French territories of America, and 10 were born in a foreign country. Overall, 9/14 were unemployed and 5/14 had a job; 10/14 cases had health insurance (6 had normal health insurance and 4 had health insurance for precarious populations) and 4/14 had no health insurance.
In this case series, an advanced HIV stage (stage C3) was observed in most patients (11/14), and all but one patient had a temperature > 38°C (mean = 39.3°C ± 0.8) with varied clinical presentations. Only 3 patients did not have hepatomegaly (5/14) or splenomegaly (7/14) or lymphadenopathy (9/14). Two patients had a complete clinical presentation with all 4 signs (Table 2).
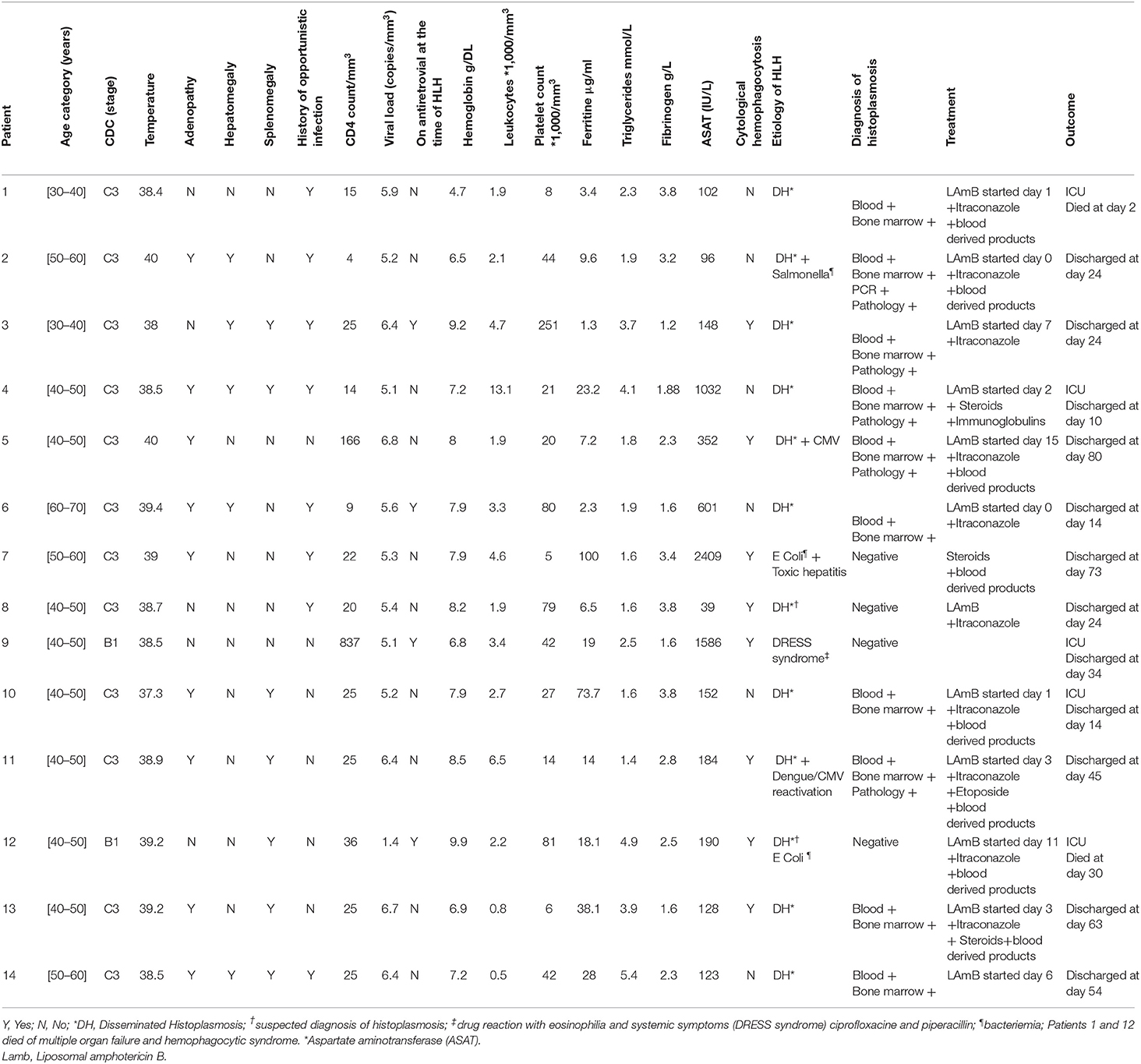
Table 2. Clinical criteria of patients with hemophagocytic lymphohistiocytosis.
A history of opportunistic infection was described for 8 patients. The number of patients on antiretroviral treatment at the time of the HLH was 4 out of 14. The CD4 count at the time of HLH diagnosis was below 250/mm3 in 13 cases (median 25 per mm3 Interquartile range = 16–25 per mm3). Only one patient had CD4 counts above 500/mm3. The HIV viral load was >100 000 copies/ml in 13 out of 14 cases (median 341,097 copies/mm3. Interquartile range = 159 374–2 551 033).
Anemia (with hemoglobin <9 g/dl) was present in 13 patients. Leucopenia (leukocytes <4,000/mm3) and low platelets (platelets <100,000/mm3) were, respectively, observed in 10 and 13 out of 14 cases (Table 2).
Increased ferritin (ferritin > 500 ng/ml) and elevated ASAT were observed in all patients. The median triglyceride concentration was 3 mmol/L (IQR = 2.12–5.2). The median fibrinogen concentration was 2.9 g/L (IQR = 2.4–4.6 g/L).
The presence of signs of hemophagocytosis were present on the bone marrow examination for 8 patients.
Among the causes observed in patients with HLH, infectious causes were predominant (12/14) with a predominance of fungal causes, notably disseminated histoplasmosis with 10 confirmed cases and 2 suspicions treated as histoplasmosis (12/14) (Table 2).
Fungal/bacterial coinfections were observed in 2 of 14 cases, and fungal/viral coinfections in 2 of the 14 cases. Two non-infectious causes were observed and were linked to a drug reaction, one of which was a Drug Reaction with Eosinophilia and Systemic Symptoms (DRESS), the other being a toxic hepatitis associated with an E. Coli infection.
The etiologic diagnosis of HLH consecutive to histoplasmosis was based on positive fungal blood cultures in most cases (10/12) (Table 2). In 9 cases, Histoplasma capsulatum was simultaneously found in fungal blood cultures and on bone marrow culture. Histoplasmosis serology was negative in all patients. Histoplasma PCR was only found in 1 case. Pathological examination was contributive in 5 of 12 cases. In 2 of 12 cases, Histoplasma capsulatum could not be identified in any sample, the etiologic diagnostic resting on a favorable evolution on probabilistic antifungal therapy.
The etiologic treatment with first line systemic antifungal treatment with liposomal amphotericin B was given in 12 of 14 HLH (Table 2). Relay antifungal treatment with itraconazole was also initiated in 10 of 14 cases. Only 1 patient, who probably had a HLH linked to a DRESS syndrome did not receive systemic antifungals.
Among the 4 patients having received probabilistic antifungal treatment, histoplasmosis was not retained as the etiologic agent of HLH for patient n°7. A drug-related hepatitis was suspected in this patient on antibiotics for a urinary tract infection and negative mycological examinations.
Two patients (n°8 and 12) received presumptive antifungal treatment despite negative samples for histoplasmosis. A favorable evolution without any other treatment than antifungals and without any associated pathogen was considered as plausibly indicating histoplasmosis despite the lack of formal evidence.
Specific treatment for HLH was only given in 4 patients with the use of corticosteroids, immunoglobulins and etoposide. The use of blood products was observed in 9 of 14 cases. The delay for initiating antifungal therapy was short with a median of 3 days (IQR: 1–8 days). Five patients presented a severe form of HLH requiring transfer in intensive care unit (ICU), with a fatal evolution in 2 cases. For patient n°1, death occurred within 24 h of admission in ICU and initiation of liposomal amphotericin B. For patient n°12, death was observed 19 days after the initiation of liposomal amphotericin B and 18 days after admission in ICU. The duration of hospitalization was often long with a median of 27 days (IQR: 16–52 days). Case fatality was 2/14 among all cases (14%) et 1/10 among confirmed disseminated histoplasmosis (DH) with HLH (10%), and 2/12 among confirmed and suspected (17%).
In the present study we described 14 HIV-infected patients having presented HLH in a 4.5 year period in Cayenne hospital during which a total 369 patients with HIV were hospitalized. Most patients had severe immunosuppression (most had CD4 counts <100/mm3) in the absence of antiretroviral treatment. The diagnosis of HLH was based on an HScore > 200 with a probability > 89 % in 13/14 patients in this series. The main trigger was an infectious pathogen, Histoplasma capsulatum, in HLH. Few concomitant coinfections were associated with HLH. The treatment of the infectious trigger was mostly systemic antifungal therapy targeting Histoplasma capsulatum, with a rapid initiation delay (3 days). The observed mortality was 14 % for all HLH (2/14) and 10% (1/10) for HLH linked to confirmed disseminated histoplasmosis.
This study was retrospective based on different databases which rely on clinician subjectivity in coding. Some of the diagnostic criteria are specific and may not have been systematically sought for all patients. In addition, there may have been selection biases in Cayenne hospital. Although this small series does not allow statistical inferences, it allows observing general trends on HLH, in HIV patients.
HLH is a complex pathology with variable organ tropism, accounting for the diversity of clinical and biological signs and the absence of pathognomonic elements. Historically, the diagnosis of HLH rested on HLH-2004 criteria proposed by the Histiocyte Society (Henter et al., 2007). These criteria are mixed with clinical, biological, and cytological criteria, and a total of at least 5 of 8 criteria is required. The absence of weighting of these criteria represents a diagnostic difficulty. Fardet et al. proposed a diagnostic score for HLH (HScore) from a multicentric cohort of 162 patients with HLH (Fardet et al., 2014). In our study, the diagnostic of HLH was given if the patient had at least 3 of 8 HLH-2004 criteria instead of the 5 criteria in the HLH-2004 definition. This less restrictive definition was chosen in order to be more sensitive, and thus to avoid missing cases. For 2 of the 14 cases, an HScore value > 200 reflected the interest of this less stringent definition. The patient with an HScore <200 and 3 of 8 HLH-2004 criteria could presumably not express the other criteria because of a short hospitalization and a rapid death at day 2.
Moreover, the cytological element of hemophagocytosis was absent in 6 cases (42 %) and an HScore showing a probability of HLH >90% was observed in 12 cases (85%). This is consistent with other studies showing that the absence of hemophagocytosis on the bone marrow smear was observed in 30% of patients (Fardet et al., 2014). These results suggest that the cytological criterion lacks sensitivity and that the diagnosis of HLH should not be excluded in the absence of this criterion.
The determination of the activity of NK cells and soluble CD25 were not performed here because these analyses are not part of routine explorations. These 2 criteria are often not taken into account by different authors and are not mandatory to assert the HLH diagnosis. Few articles in the literature mention NK activity or soluble CD25 (Karras, 2009; Kolopp-Sarda and Malcus, 2014; Grom et al., 2016). These 2 markers are also not included in the calculation of the HScore.
The specificity of HLH among HIV-infected patients in French Guiana is that its etiology is mostly infectious and mostly due to the disseminated infection by the fungus Histoplasma capsulatum. These results are different from those observed in mainland France but are consistent with previous studies on causes of death by opportunistic agents in French Guiana emphasizing differences in pathogen ecology between Europe and the Amazonian area (Nacher et al., 2011). Our observations also contrast with a retrospective study in São Paulo, Brazil, where the main causes of HLH in HIV patients were disseminated histoplasmosis only represented 8% of the trigger factors, with mycobacteria (34%), cytomegalovirus (14%), and cryptococcus (11%) representing the leading causal pathogens. The bibliographic data are varied on the causes of HLH in HIV patients (Koduri et al., 1995; Fiszbin et al., 1998; Fardet et al., 2003; Sproat et al., 2003; Concetta et al., 2004; Sun et al., 2004; Telles et al., 2019). Our series shows a singular etiologic homogeneity, with the exception of an American study (Townsend et al., 2015). It is interesting to note that, although tuberculosis is a frequent opportunistic infection in French Guiana, and it is identified as a cause of HLH in other series, here it was not found to be associated with HLH. Although HLH in HIV patients are rare, systematic probabilistic first line antifungal treatment with liposomal amphotericin B seems justified given our results and those of the literature (De Lavaissière et al., 2009; Castelli et al., 2015; Subedee and Van Sickels, 2015; Townsend et al., 2015). A bibliographic review of HLH secondary to histoplasmosis in HIV-infected patients reports 34 cases with a mean age of 39 ± 11 years (Table 3). The immunosuppression was severe with a median CD4 count of 16 (IQR: 7–39)/mm3. Cases were defined on the basis of 4 to 8 HLH-2004 diagnostic criteria. Systemic antifungal treatment was mentioned in 18 of 34 patients. The mortality rate was 14 of 34 patients (41%).
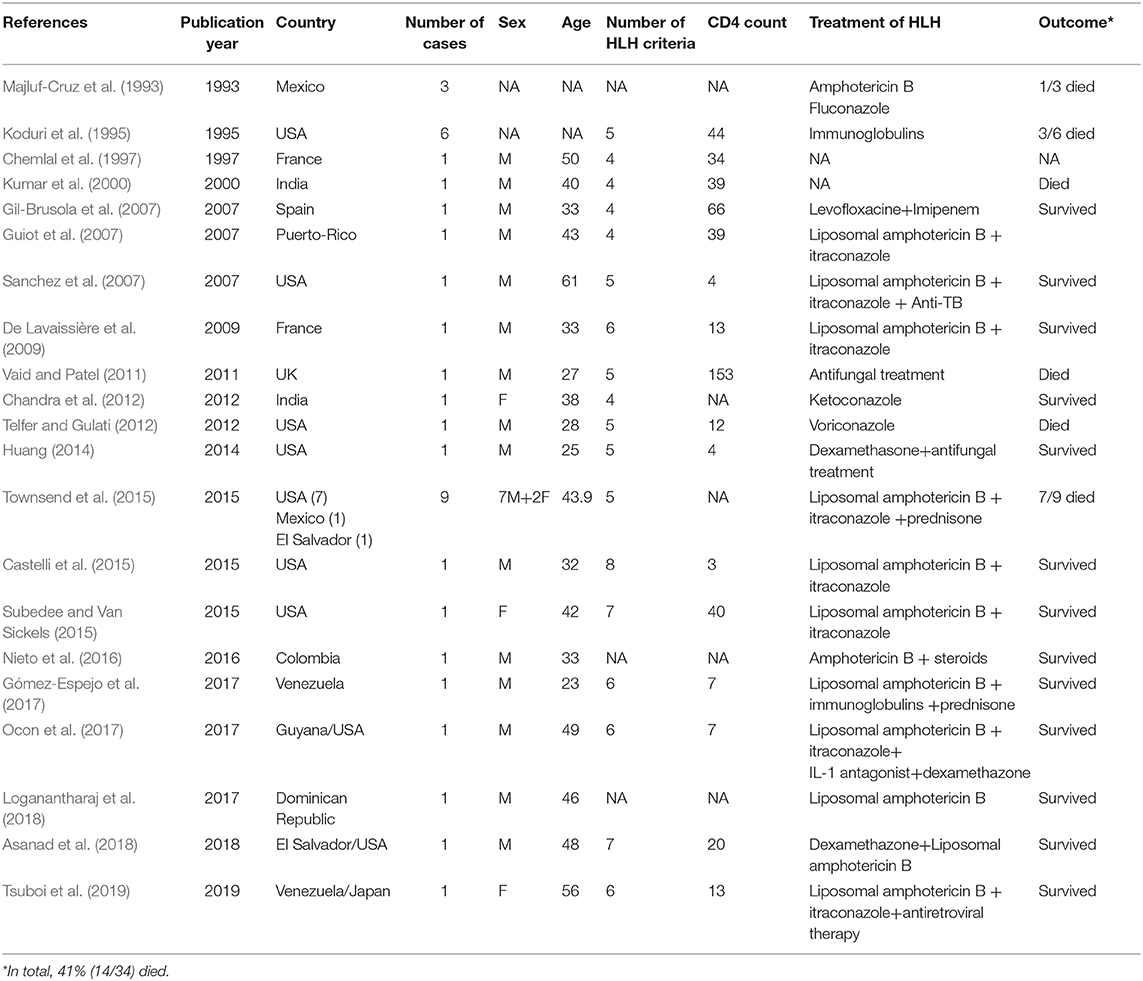
Table 3. Case reports and case series on reactive hemophagocytosis due to histoplasmosis in HIV patients.
In contrast with other reports, specific treatment of HLH were rarely used in our series, but in most cases the evolution was favorable (Silva and França, 2014; Townsend et al., 2015; Le Joncour et al., 2016; Usman et al., 2016). This difference is probably linked to the fact that whereas most specific treatments of HLH are used for non-infectious triggers of an autoimmune nature, in our series the triggers were infectious.
Our series presents severe forms of HLH with 5 cases requiring ICU and, in these, a mortality below 50%. The mortality results of our series (14% globally and 17% only for disseminated histoplasmosis cases) seems lower than the mean mortality rates of HLH in HIV patients with histoplasmosis, evaluated at 41% for HLH linked to disseminated histoplasmosis (Koduri et al., 1995; Chemlal et al., 1997; Kumar et al., 2000; Gil-Brusola et al., 2007; Guiot et al., 2007; De Lavaissière et al., 2009; Vaid and Patel, 2011; Chandra et al., 2012; Huang, 2014; Castelli et al., 2015; Subedee and Van Sickels, 2015; Townsend et al., 2015; Le Joncour et al., 2016; Usman et al., 2016). The hypothetical explanation would be that knowledge of the local epidemiology leads to the use of an aggressive diagnostic and therapeutic strategy with a rapid first line treatment strategy using empirical systemic antifungals targeting disseminated histoplasmosis, the most frequent opportunistic infection in HIV patients in French Guiana. Perhaps the rapid response to Liposomal amphotericin B explains this lower case-fatality in comparison to HLH cases linked to Lymphoma or Kaposi. Finally, although the cascade of care has greatly improved, it is noteworthy that during the study period 12 of the 57 reported cases of histoplasmosis in French Guiana (Nacher et al., 2020a,b) were HLH, which emphasizes that the problem is not an anecdotal one if 1 in 5 patients with disseminated histoplasmosis are concerned. The opportunistic pathogen ecology in French Guiana is similar in the Guianas and the Amazon, and for histoplasmosis the high incidence observed in French Guiana can also be observed in much of South and Central America (Adenis et al., 2018). The present results therefore suggest that in HIV-infected patients with HLH in these regions should benefit from active search for H. capsulatum and from prompt antifungal treatment with amphotericin B, preferably in its liposomal formulation.
HLH is usually considered to be rare and usually occurs in severely immunocompromised patients. The diagnosis is difficult and therefore presumably underestimated. The present results suggest that it is indeed more frequent than previously thought. The more frequent use of the HScore, in addition to HLH-2004 criteria, seems pertinent given the actual state of knowledge.
For the first time, in the context of French Guiana, disseminated histoplasmosis appears as the most frequent etiology of HLH in HIV patients. Hence the rapid initiation of probabilistic first line antifungal therapy with liposomal amphotericin B seems pertinent and beneficial on the vital prognosis of HIV patients with HLH. This further emphasizes the importance of early diagnosis and treatment of disseminated histoplasmosis. It also suggests that the incidence of disseminated histoplasmosis-associated HLH in patients with advanced HIV in Latin America is presumably far more frequent than the literature suggests. The recent reports from Latin American countries are only the tip of the problem and greater awareness will presumably unveil the true magnitude of the problem (Adenis et al., 2018; Caceres et al., 2019).
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation, to any qualified researcher.
All HIV-infected patients followed at Cayenne Hospital are included in the DAT'AIDS database. This database allows the clinical care of HIV patients with the eNADIS computerized medical records. It is part of the French Hospital Database on HIV, a national cohort which has led to numerous scientific publications. This database received approval from the Commission Nationale Informatique et Libertés (CNIL) since 27/11/1991. All included patients signed an informed consent form after presentation of the database by the treating physician.
DN and AA: conception. DN, MN, LE, AM, MD, DB, RB, KD, PA, FD, PC, and AA: data collection and study conduct and manuscript validation. DN, MN, and AA: manuscript drafting. MN: final manuscript validation. All authors contributed to the article and approved the submitted version.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Adenis, A. A., Valdes, A., Cropet, C., McCotter, O. Z., Derado, G., Couppie, P., et al. (2018). Burden of HIV-associated histoplasmosis compared with tuberculosis in Latin America: a modelling study. Lancet Infect. Dis. 18, 1150–1159. doi: 10.1016/S1473-3099(18)30354-2
Asanad, S., Cerk, B., and Ramirez, V. (2018). Hemophagocytic lymphohistiocytosis (HLH) secondary to disseminated histoplasmosis in the setting of Acquired Immunodeficiency Syndrome (AIDS). Med. Mycol. Case Rep. 20, 15–17. doi: 10.1016/j.mmcr.2018.01.001
Bhatia, S., Bauer, F., and Bilgrami, S. A. (2003). Candidiasis-associated hemophagocytic lymphohistiocytosis in a patient infected with human immunodeficiency virus. Clin. Infect. Dis. 37, e161–e166. doi: 10.1086/379615
Breton, G., Adle-Biassette, H., Therby, A., Ramanoelina, J., Choudat, L., Bissuel, F., et al. (2006). Immune reconstitution inflammatory syndrome in HIV-infected patients with disseminated histoplasmosis. AIDS Lond. Engl. 20, 119–121. doi: 10.1097/01.aids.0000199014.66139.39
Caceres, D. H., Adenis, A., de Souza, J. V. B., Gomez, B. L., Cruz, K. S., Pasqualotto, A. C., et al. (2019). The manaus declaration: current situation of histoplasmosis in the Americas, Report of the II regional meeting of the international histoplasmosis advocacy group. Curr. Fungal Infect. Rep. 13, 244–249. doi: 10.1007/s12281-019-00365-3
Castelli, A. A., Rosenthal, D. G., Bender Ignacio, R., and Chu, H. Y. (2015). Hemophagocytic lymphohistiocytosis secondary to human immunodeficiency virus-associated histoplasmosis. Open Forum Infect. Dis. 2:ofv140. doi: 10.1093/ofid/ofv140
Chandra, H., Chandra, S., and Sharma, A. (2012). Histoplasmosis on bone marrow aspirate cytological examination associated with hemophagocytosis and pancytopenia in an AIDS patient. Korean J. Hematol. 47, 77–79. doi: 10.5045/kjh.2012.47.1.77
Chemlal, K., Andrieu-Bautru, V., and Couvelard, A. (1997). Hemophagocytic syndrome during Histoplasma capsulatum infection. Haematologica 82, 726–726.
Concetta, C., Roberta, P., Giuliana, B., Antonio, C., Vito, G., Silvia, C., et al. (2004). Hemophagocytic syndrome in a patient with acute human immunodeficiency virus infection. Clin. Infect. Dis. 38, 1792–1793. doi: 10.1086/392512
De Lavaissière, M., Manceron, V., Bourée, P., Garçon, L., Bisaro, F., Delfraissy, J.-F., et al. (2009). Reconstitution inflammatory syndrome related to histoplasmosis, with a hemophagocytic syndrome in HIV infection. J. Infect. 58, 245–247. doi: 10.1016/j.jinf.2008.11.010
Fardet, L., Blum, L., Kerob, D., Agbalika, F., Galicier, L., Dupuy, A., et al. (2003). Human herpesvirus 8-associated hemophagocytic lymphohistiocytosis in human immunodeficiency virus-infected patients. Clin. Infect. Dis. 37, 285–291. doi: 10.1086/375224
Fardet, L., Galicier, L., Lambotte, O., Marzac, C., Aumont, C., Chahwan, D., et al. (2014). Development and validation of the HScore, a score for the diagnosis of reactive hemophagocytic syndrome. Arthritis Rheumatol. 66, 2613–2620. doi: 10.1002/art.38690
Fiszbin, M., Jeunne, C. L., Quint, L., and Hugues, F. C. (1998). Pancytopénie fébrile au cours du sida: un syndrome d hémophagocytose. Rev. Méd. Interne 19, 673–675. doi: 10.1016/S0248-8663(99)80050-2
Gil-Brusola, A., Pemán, J., Santos, M., Salavert, M., Lacruz, J., and Gobernado, M. (2007). Disseminated histoplasmosis with hemophagocytic syndrome in a patient with AIDS: description of one case and review of the Spanish literature. Rev. Iberoam. Micol. 24, 312–316. doi: 10.1016/S1130-1406(07)70063-3
Gómez-Espejo, S. M., Olalla-Sierra, J., Marí-Jiménez, P., Pereda-Salguero, T., Pérez-Stachowski, J., de-la-Torre-Lima, J., et al. (2017). Reconstitution inflammatory syndrome like reactive hemophagocytic syndrome associated with disseminated histoplasmosis in a HIV patient. Mycopathologia 182, 767–770. doi: 10.1007/s11046-017-0144-6
Grom, A. A., Horne, A., and De Benedetti, F. (2016). Macrophage activation syndrome in the era of biologic therapy. Nat. Rev. Rheumatol. 12, 259–268. doi: 10.1038/nrrheum.2015.179
Guiot, H. M., Bertrán-Pasarell, J., Tormos, L. M., González-Keelan, C., Procop, G. W., Fradera, J., et al. (2007). Ileal perforation and reactive hemophagocytic syndrome in a patient with disseminated histoplasmosis: the role of the real-time polymerase chain reaction in the diagnosis and successful treatment with amphotericin B lipid complex. Diagn. Microbiol. Infect. Dis. 57, 429–433. doi: 10.1016/j.diagmicrobio.2006.09.010
Hayden, A., Park, S., Giustini, D., Lee, A. Y. Y., and Chen, L. Y. C. (2016). Hemophagocytic syndromes (HPSs) including hemophagocytic lymphohistiocytosis (HLH) in adults: a systematic scoping review. Blood Rev. 30, 411–420. doi: 10.1016/j.blre.2016.05.001
Henter, J.-I., Horne, A., Aricó, M., Egeler, R. M., Filipovich, A. H., Imashuku, S., et al. (2007). HLH-2004: diagnostic and therapeutic guidelines for hemophagocytic lymphohistiocytosis. Pediatr. Blood Cancer 48, 124–131. doi: 10.1002/pbc.21039
Huang, A. M. (2014). Hemophagocytic lymphohistiocytosis and disseminated histoplasmosis. Blood J. Am. Soc. Hematol. 123, 2449–2449. doi: 10.1182/blood-2014-01-550657
Jabr, R., El Atrouni, W., Male, H. J., and Hammoud, K. A. (2019). Histoplasmosis-associated hemophagocytic lymphohistiocytosis: a review of the literature. Can. J. Infect. Dis. Med. Microbiol. 2019:7107326. doi: 10.1155/2019/7107326
Karras, A. (2009). What nephrologists need to know about hemophagocytic syndrome. Nat. Rev. Nephrol. 5, 329–236. doi: 10.1038/nrneph.2009.73
Koduri, P. R., Chundi, V., deMarais, P., Mizock, B. A., Patel, A. R., and Weinstein, R. A. (1995). Reactive hemophagocytic syndrome: a new presentation of disseminated histoplasmosis in patients with AIDS. Clin. Infect. Dis. 21, 1463–1465. doi: 10.1093/clinids/21.6.1463
Kolopp-Sarda, M.-N., and Malcus, C. (2014). Perturbations biologiques et immunologiques au cours des syndromes hémophagocytaires. Rev. Francoph. Lab. 2014, 29–35. doi: 10.1016/S1773-035X(14)72746-7
Kumar, N., Jain, S., and Singh, Z. N. (2000). Disseminated histoplasmosis with reactive hemophagocytosis: aspiration cytology findings in two cases. Diagn. Cytopathol. 23, 422–424. doi: 10.1002/1097-0339(200012)23:6<422::AID-DC13>3.0.CO;2-F
Le Joncour, A., Bidegain, F., Ziol, M., Galicier, L., Oksenhendler, E., Mechai, F., et al. (2016). Hemophagocytic lymphohistiocytosis associated with Bartonella henselae infection in an HIV-infected patient. Clin. Infect. Dis. 62, 804–806. doi: 10.1093/cid/civ999
Loganantharaj, N., Oliver, B., Smith, T., Jetly, R., Engel, L., and Sanne, S. (2018). Hemophagocytic lymphohistiocytosis in an HIV-positive patient with concomitant disseminated histoplasmosis. Int. J. STD AIDS 29, 925–928. doi: 10.1177/0956462417753008
Majluf-Cruz, A. S., Hurtado, R. M., Souto-Meirino, C., and Simón, J. (1993). Hemophagocytic syndrome associated with histoplasmosis in the acquired immunodeficiency syndrome: description of 3 cases and review of the literature. Sangre. 38, 51–55.
Melzani, A., de Reynal de Saint Michel, R., Ntab, B., Djossou, F., Epelboin, L., Nacher, M., et al. (2020). Incidence and trends in immune reconstitution inflammatory syndrome associated with histoplasma capsulatum among people living with human immunodeficiency virus: a 20-year case series and literature review. Clin. Infect. Dis. 70, 643–652. doi: 10.1093/cid/ciz247
Nacher, M., Adenis, A., Abboud, P., Djossou, F., Demar, M., Epelboin, L., et al. (2020a). HIV patients dying on anti-tuberculosis treatment: are undiagnosed infections still a problem in French Guiana? BMC Res. Notes 13:209. doi: 10.1186/s13104-020-05054-w
Nacher, M., Adenis, A., Adriouch, L., Dufour, J., Papot, E., Hanf, M., et al. (2011). What is AIDS in the Amazon and the Guianas? Establishing the burden of disseminated histoplasmosis. Am. J. Trop. Med. Hyg. 84, 239–240. doi: 10.4269/ajtmh.2011.10-0251
Nacher, M., Adenis, A., Arathoon, E., Samayoa, B., Lau-Bonilla, D., Gomez, B. L., et al. (2016). Disseminated histoplasmosis in Central and South America, the invisible elephant: the lethal blind spot of international health organizations. AIDS 30, 167–170. doi: 10.1097/QAD.0000000000000961
Nacher, M., Adenis, A., Blanchet, D., Vantilcke, V., Demar, M., Basurko, C., et al. (2014). Risk factors for disseminated histoplasmosis in a cohort of HIV-infected patients in French Guiana. PLoS Negl. Trop. Dis. 8:e2638. doi: 10.1371/journal.pntd.0002638
Nacher, M., Adenis, A., Mc Donald, S., Gomes, M. D. S. M., Singh, S., Lima, I. L., et al. (2013). Disseminated histoplasmosis in HIV-infected patients in South America: a neglected killer continues on its rampage. PLoS Negl. Trop. Dis. 7:e2319. doi: 10.1371/journal.pntd.0002319
Nacher, M., Adriouch, L., Huber, F., Vantilcke, V., Djossou, F., Elenga, N., et al. (2018). Modeling of the HIV epidemic and continuum of care in French Guiana. PLoS ONE 13:e0197990. doi: 10.1371/journal.pone.0197990
Nacher, M., Ouedraogo, E., Succo, T., Guarmit, B., Djossou, F., Stettler, L., et al. (2020b). HIV in French Guiana: historical review and current trends. Bull. Epidémiol. Hebd. 43–51. Available online at: http://beh.santepubliquefrance.fr/beh/2020/2-3/2020_2-3_2.html
Nieto, J. F., Gómez, S. M., Moncada, D. C., Serna, L. M., and Hidrón, A. I. (2016). Tratamiento exitoso de linfohistiocitosis hemofagocítica y coagulación intravascular diseminada secundarias a histoplasmosis en un paciente con HIV/sida. Biomédica 36, 9–14. doi: 10.7705/biomedica.v36i2.2797
Ocon, A. J., Bhatt, B. D., Miller, C., and Peredo, R. A. (2017). Safe usage of anakinra and dexamethasone to treat refractory hemophagocytic lymphohistiocytosis secondary to acute disseminated histoplasmosis in a patient with HIV/AIDS. BMJ Case Rep. (2017) 2017:bcr2017221264. doi: 10.1136/bcr-2017-221264
Sanchez, A., Celaya, A. K., and Victorio, A. (2007). Histoplasmosis-Associated Hemophagocyti Syndrome: A Case Report. Available online at: https://www.patientcareonline.com/view/histoplasmosis-associated-hemophagocytic-syndrome-case-report
Silva, S. V., and França, M. (2014). HIV infection presenting as haemophagocytic syndrome. Eur. J. Case Rep. Intern. Med. 1. doi: 10.12890/2014_000099
Sproat, L. O., Pantanowitz, L., Lu, C. M., and Dezube, B. J. (2003). Human immunodeficiency virus—associated hemophagocytosis with iron-deficiency anemia and massive splenomegaly. Clin. Infect. Dis. 37, e170–e173. doi: 10.1086/379613
Subedee, A., and Van Sickels, N. (2015). Hemophagocytic syndrome in the setting of AIDS and disseminated histoplasmosis: case report and a review of literature. J. Int. Assoc. Provid. AIDS Care 14, 391–397. doi: 10.1177/2325957415570740
Sun, H.-Y., Chen, M.-Y., Fang, C.-T., Hsieh, S.-M., Hung, C.-C., and Chang, S.-C. (2004). Hemophagocytic lymphohistiocytosis: an unusual initial presentation of acute HIV infection. JAIDS J. Acquir. Immune Defic. Syndr. 37, 1539–1540. doi: 10.1097/01.qai.0000136725.92886.b8
Telfer, M., and Gulati, S. (2012). Hemophagocytic lymphohistiocytosis in a patient with disseminated histoplasmosis: a case report. J. Hosp. Med. 7(suppl 2). Available online at: http://www.shmabstracts.com/abstract/hemophagocytic-lymphohistiocytosis-in-a-patient-with-disseminated-histoplasmosis-a-case-report/
Telles, J. P., de Andrade Perez, M., Marcusso, R., Correa, K., Teixeira, R. F. A., and Tobias, W. M. (2019). Hemophagocytic syndrome in patients living with HIV: a retrospective study. Ann. Hematol. 98, 67–72. doi: 10.1007/s00277-018-3500-9
Townsend, J. L., Shanbhag, S., Hancock, J., Bowman, K., and Nijhawan, A. E. (2015). Histoplasmosis-induced hemophagocytic syndrome: a case series and review of the literature. Open Forum Infect. Dis. 2:ofv055. doi: 10.1093/ofid/ofv055
Tsuboi, M., Nishijima, T., Nagi, M., Miyazaki, Y., Teruya, K., Kikuchi, Y., et al. (2019). Case Report: hemophagocytic lymphohistiocytosis caused by disseminated histoplasmosis in a venezuelan patient with HIV and epstein–barr virus reactivation who traveled to Japan. Am. J. Trop. Med. Hyg. 100, 365–367. doi: 10.4269/ajtmh.18-0478
Usman, M., Thapa, S. D., Hadid, H., and Yessayan, L. T. (2016). HIV infection presenting proliferation of CD8+ T lymphocyte and hemophagocytic lymphohistiocytosis. Int. J. STD AIDS 27, 411–413. doi: 10.1177/0956462415585254
Keywords: haemophagocytic lymphohistiocytosis, reactive hemophagocytic syndrome, macrophage activation syndrome, HIV, histoplasmosis, liposomal amphotericin B, French Guiana
Citation: Nguyen D, Nacher M, Epelboin L, Melzani A, Demar M, Blanchet D, Blaizot R, Drak Alsibai K, Abboud P, Djossou F, Couppié P and Adenis A (2020) Hemophagocytic Lymphohistiocytosis During HIV Infection in Cayenne Hospital 2012–2015: First Think Histoplasmosis. Front. Cell. Infect. Microbiol. 10:574584. doi: 10.3389/fcimb.2020.574584
Received: 20 June 2020; Accepted: 19 August 2020;
Published: 24 September 2020.
Edited by:
Miguel Cacho Teixeira, University of Lisbon, PortugalReviewed by:
Rossana Cordeiro, Federal University of Ceara, BrazilCopyright © 2020 Nguyen, Nacher, Epelboin, Melzani, Demar, Blanchet, Blaizot, Drak Alsibai, Abboud, Djossou, Couppié and Adenis. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Mathieu Nacher, bWF0aGlldS5uYWNoZXI2NkBnbWFpbC5jb20=
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.