 Massimo Baudo
Massimo Baudo Francesco Cabrucci
Francesco Cabrucci Amanda Yakobitis2
Amanda Yakobitis2 Gianluca Torregrossa
Gianluca Torregrossa
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
BRIEF RESEARCH REPORT article
Front. Cardiovasc. Med., 03 March 2025
Sec. Cardiovascular Surgery
Volume 12 - 2025 | https://doi.org/10.3389/fcvm.2025.1555394
This article is part of the Research TopicSurgical Revascularization of the Ischemic Myocardium in the third millenniumView all 3 articles
Introduction: Numerous techniques have been developed to minimize risk of perioperative stroke during coronary artery bypass grafting (CABG), including off-pump approach, preoperative and intraoperative imaging of the ascending aorta (CT scan and epiaortic ultrasound), anaortic CABG with bilateral internal thoracic artery, clampless devices for the construction of proximal anastomosis and minimal aortic manipulation with a single aortic inflow for all proximal grafts (piggyback proximal anastomosis). The aim of this study was to evaluate the clinical outcomes of CABG patients who underwent off pump CABG with proximal anastomosis constructed with the use of a clampless device and in a piggyback fashion.
Methods: This observational study included 112 consecutive patients undergoing CABG with the piggyback proximal technique at the Lankenau Heart Institute between June 2021 and January 2024. Primary endpoints included overall mortality, cardiac-related mortality, stroke, myocardial infarction, repeat revascularization. Intraoperative transit time flow measurement (TTFM) was also analyzed.
Results: The mean age of the cohort was 67.8 ± 8.7 years, with 75.9% (85/112) being male. All patients underwent off-pump CABG. The piggyback anastomosis consisted of vein-on-vein (52.7%, 59/112), artery-on-vein (43.8%, 49/112), and double vein/artery configurations (3.6%, 4/112). Postoperatively, no strokes occurred. At 30 days no patient died or required repeat revascularization. The mean hospital stay was 5.5 [4.0–8.0] days. At a mean follow-up of 1.0 [0.5–1.7] years, no cardiac deaths were recorded, with an overall survival of 98.2% (110/112). Repeat piggyback revascularization was 3.6% (4/112) at a mean of 2.0 ± 0.5 years. TTFM demonstrated superior flow rates in artery-on-vein grafts [50 (40–70) ml/min] compared to vein-on-vein grafts [40 (30–53.5), p < 0.001].
Conclusions: When a proximal anastomosis cannot be avoided during off pump CABG, the combination of a piggyback proximal anastomosis together with the use of a clampless aortic device, demonstrated promising early mid-term outcomes almost nullifying the perioperative risk of clinical stroke. Intraoperative TTFM showed excellent flow rates, especially when arterial grafts were used. The technique is a viable option in high-risk patients with severe aortic disease, offering a safe and effective approach to multivessel revascularization with minimal aortic manipulation. Further studies with longer follow-up are warranted to confirm its long-term benefits.
Coronary artery bypass grafting (CABG) remains the most effective revascularization strategy for patients with advanced coronary artery disease (CAD). Despite its success in reducing mortality and improving cardiac function, CABG carries inherent risks, most notably stroke and postoperative cognitive decline (1, 2). Cerebrovascular accidents, which include overt strokes and silent brain infarcts (SBI) that lack discernible neurological symptoms, can significantly impact postoperative outcomes. These SBI may accumulate over time, potentially contributing to long-term cognitive decline in CABG patients (3, 4).
Since SYNTAX trial that reported a stroke rate of 2.2% (5), minimizing aortic manipulation has become a key strategy in reducing the incidence of stroke during CABG (6). The aorta is a primary source of atheromatous debris, which can embolize during surgery and lead to cerebrovascular events. To mitigate this risk, several techniques have been developed, including single aortic cross clamp to complete proximal anastomosis during on pump CABG, off pump anaortic CABG using bilateral thoracic arteries for inflow (7), preoperative CT scans to assess aortic calcification, and intraoperative epiaortic ultrasound to identify the optimal site for aortic puncture (8, 9). In addition to these methods, two more techniques should be incorporated into the coronary surgeon's armamentarium.
First, the piggyback proximal anastomosis technique, where multiple grafts are attached through a single anastomotic site on the ascending aorta (10, 11). This approach reduces the number of aortic punctures and manipulation, lowering the risk of atheroembolism and potentially decreasing the incidence of both clinical and SBI. In addition to neuroprotection, the piggyback technique provides a stable anastomotic site that supports the use of a second arterial conduit, such as the radial artery or right internal thoracic artery (RITA) in free-graft configuration, preventing kinking or flattening that may occur with direct aortic anastomosis (10, 11).
Second, the use of clampless proximal anastomosis devices, avoiding the need for aortic side-biting clamp, offers a valid solutions for safer and more efficient aortic anastomoses during off-pump CABG (OPCABG) or during on pump beating heart CABG. These devices aim to reduce the risk of cerebral embolic complications associated with aortic clamping, particularly in patients with a high burden of atherosclerotic disease (12).
This study aimed to evaluate early mid-term clinical outcomes in patients undergoing OPCABG with clampless devices and the piggyback proximal aortic-coronary graft anastomosis technique, providing data to demonstrate that using a clampless single hole for all proximal anastomoses is safe, reproducible, and beneficial. Specifically, this approach may reduce stroke risk, enhance graft flow, and improve graft patency, particularly when a second arterial conduit is used. We hypothesize that this method may also contribute to better cognitive outcomes postoperatively.
The study protocol received approval from the Main Line Health Hospitals Institutional Review Board (IRB 45CFR164.512). Given the retrospective nature of the study, individual patient consent was waived. This was an observational study in which all consecutive patients undergoing OPCABG with the piggyback proximal technique at Lankenau Heart Institute (Lankenau Medical Center, Wynnewood, PA, USA) between June 2021 and January 2024 were enrolled. All piggyback anastomoses were performed by a single surgeon. Patients were included by all demographics and preoperative characteristics.
The primary objective was to evaluate the incidence of stroke, overall mortality, cardiac-related mortality, cardiac readmissions, myocardial infarction, and the need for repeat target revascularization in patients undergoing OPCABG utilizing clampless devices and the piggyback proximal anastomosis technique.
Secondary endpoints included the transit time flow measurements (TTFM) of the aortocoronary grafts in different piggyback configurations: vein-on-vein, artery-on-vein, double vein and artery.
All patients underwent a preoperative non-contrast CT scan of the chest to evaluate the burden, extent, and location of aortic wall calcification. Additionally, irrespective of the CT findings, intraoperative epiaortic ultrasound was systematically performed to assess the aortic wall quality.
When extensive aortic calcification is detected the preferred approach is anaortic OPCABG to minimize aortic manipulation. In cases where a proximal anastomosis is deemed feasible, a clampless device is consistently utilized to mitigate the atheroembolic risk. Specifically, when the aortic wall is thickened with scattered calcifications involving the posterior wall, the Heartstring III Proximal Seal System® (Getinge, Sweden) device is favored for its adaptability. Conversely, when the aortic wall is more accessible and less burdened by calcification, the Enclose® II (Peters Surgical, USA) device is preferred, as it provides superior sealing (Figure 1). A comprehensive description of the technique for using clampless devices is beyond the scope of this paper and has been previously detailed (13).
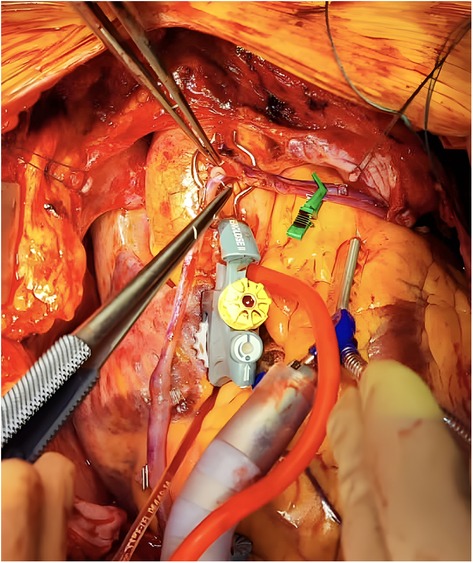
Figure 1. Intraoperative creation of a piggyback anastomosis with a proximal anastomosis device.
After creating a single hole in the ascending aorta with one of the aforementioned devices, a segment of the saphenous vein graft (SVG) is first anastomosed to the aorta in the usual fashion using a 6.0 polypropylene suture. Following our institutional culture of safety, the first proximal anastomosis—the foundation of the piggyback configuration—is consistently secured using a CorKnot®Micro (LSI Solution) (14). This approach facilitates subsequent identification and selective catheterization of the aortocoronary grafts by interventional cardiologists, thereby ensuring optimal visualization when required.
Instead of punching a second hole in the aorta, the hood of the SVG, directly over the aortotomy, is longitudinally incised with a scalpel to create an orifice. A second graft, either another SVG or an arterial conduit, is then anastomosed to the hood of the first anastomosis using a 7.0 or 8.0 polypropylene suture, completing the piggyback configuration (Figure 2).

Figure 2. Piggyback anastomosis example.
Preventing postoperative strokes is paramount, given their potential to negate the benefits of surgical revascularization and their long-term sequelae, including subtle sensory, motor, and memory impairments. A clampless piggyback technique is advocated as part of a broader strategy to minimize aortic manipulation and reduce stroke risk. Recognizing that routine postoperative neuroimaging for asymptomatic patients is not always feasible, a dedicated protocol has been established to identify patients at high risk for strokes. This protocol integrates preoperative factors (e.g., aortic wall calcification burden, atrial fibrillation, carotid atherosclerosis, history of cerebrovascular events, reduced ejection fraction) with intra- and postoperative variables [e.g., prolonged hypotension during OPCABG or in the intensive care unit (ICU), low hemoglobin levels] to determine a threshold of clinical suspicion. In the ICU, thorough neurological evaluations upon sedation cessation, followed by continuous monitoring, and systematic assessments in the step-down unit enable prompt neuroimaging when changes in sensory, motor, or neurocognitive function are detected. This comprehensive approach provides a framework for the early detection of both overt and SBI.
Categorical variables were expressed as numbers and percentages. The Kolmogorov–Smirnov test was used to assess normal distribution. Continuous variables are presented as mean and standard deviation (SD) if normally distributed and compared using the student's t-test or ANOVA accordingly. While they were presented as median and interquartile range (IQR) if not normally distributed and compared using the Mann–Whitney U test or Kruskal–Wallis test. Microsoft Office Excel program (Microsoft, Redmond, Washington) was used for data extraction and all analyses were performed in R, version 4.3.1 (R Software for Statistical Computing) within RStudio.
A total of 112 patients were enrolled and patient's baseline characteristics were summarized in Table 1. The mean age was 67.8 ± 8.7 and 85 (75.9%) patients were men. More than 90% of patients suffered from hypertension (104/112), 44 (39.3%) from diabetes, and 51 (45.5%) from dyslipidemia. Previous percutaneous coronary interventions were performed in 29 (25.9%) patients, while 2 (1.8%) had a previous cardiac surgery. The mean ejection fraction was 54.9% ± 11.8%, and the median STS-PROM was 1.04% [IQR: 0.64–1.92].
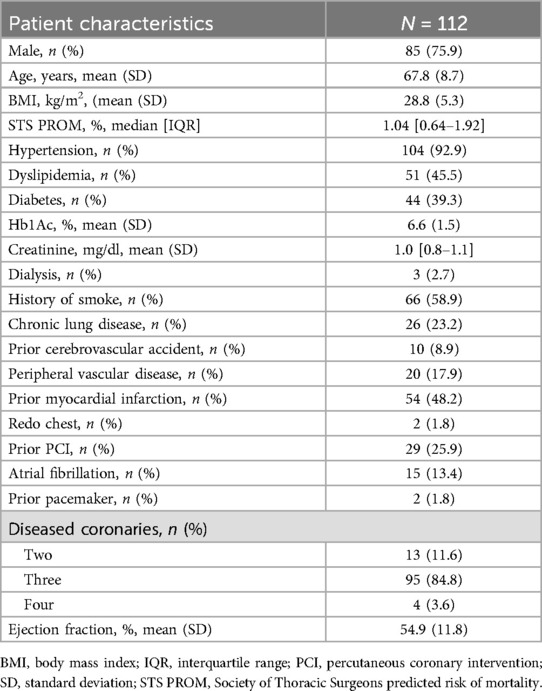
Table 1. Preoperative patient's characteristics.
All patients underwent OPCABG, and the mean number of anastomoses was 3.4 ± 0.6. The radial artery was the most common (54/112, 48.2%) second arterial graft. A Y-graft, I-graft, and sequential grafting were used 15 (13.4%), 8 (7.1%), and 17 (15.2%) times respectively, Table 2. Overall, in 33 patients (29.5%) a concomitant procedure was performed. The full list of procedures is listed in Table 2.
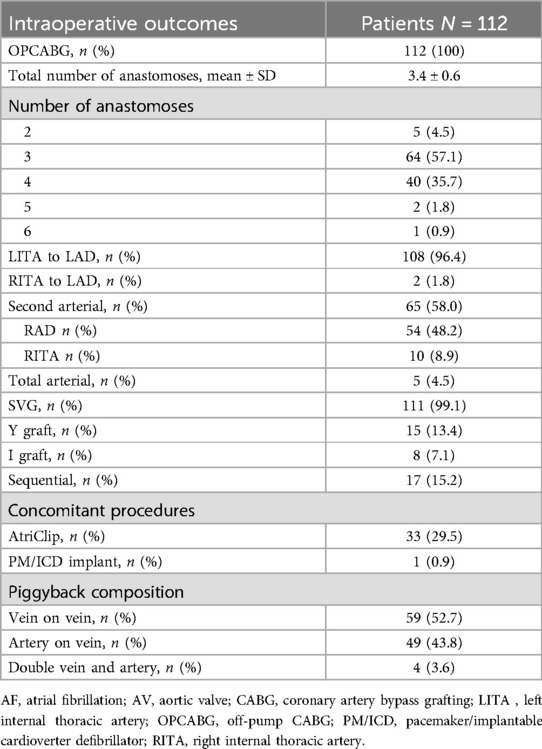
Table 2. Intraoperative outcomes.
As far as the piggyback composition is concerned, 59 (52.7%) patients received a vein-on-vein piggyback anastomosis, 49 (43.8%) an artery-on-vein, and 4 (3.6%) a double vein and artery.
Two (1.8%) patients required ventilation longer than 24 h. Importantly, no strokes or myocardial infarctions occurred, and only one (0.9%) patient needed surgical re-exploration for bleeding. The mean length of hospital stay was 5.5 [4.0–8.0] days. At 30 days, no patient died or required repeat revascularization. Cardiac readmission occurred in 3 (2.7%) patients, Table 3. Patients who underwent postoperative angiography demonstrated no evidence of thrombosis, occlusion, kinking, or torsion of the piggyback anastomoses (Figure 3). Furthermore, the feasibility of angiographic assessment of the piggyback technique was confirmed, as interventional cardiologists experienced no difficulties in identifying or injecting the piggyback proximal anastomosis during the procedure. At a mean follow-up of 1.0 [0.5–1.7] years, there were no cardiac-related deaths, with an overall survival of 98.2% (110/112). Only one myocardial infarction occurred (0.9%), and four strokes (3.6%) were reported. In this regard, one stroke occurred in a patient with a known arteriovenous malformation that eventually ruptured, and one confirmed after a subsequent percutaneous coronary intervention, thus not directly related to the CABG surgery or anastomotic technique. Repeat Piggyback revascularization rate was 3.6% (4/112) at a mean of 2.0 ± 0.5 years. Among the revascularized grafts, three were veins and one was an artery. As far as the piggyback configuration of these patients who underwent percutaneous interventions, revascularization was performed on two grafts attached directly to the aorta and two grafts placed on top of the first graft, thus showing that repeat revascularization is independent of the piggyback configuration, Table 4.
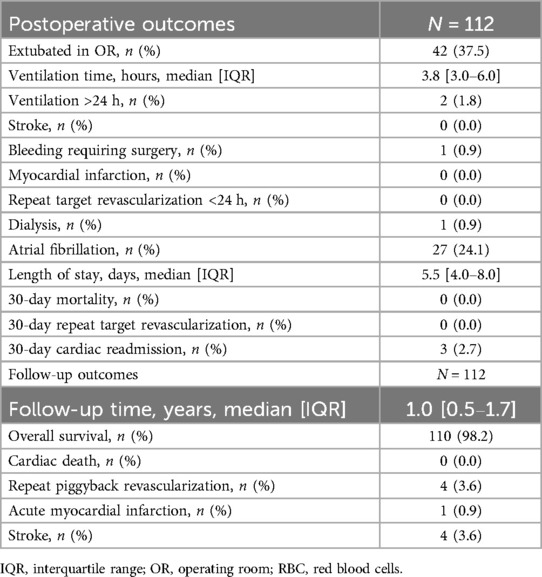
Table 3. Postoperative outcomes.
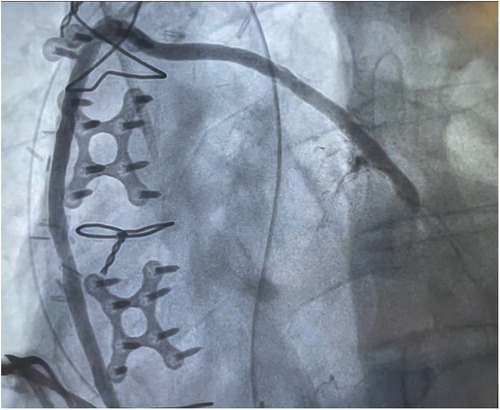
Figure 3. Postoperative angiographic visualization of the piggyback proximal anastomosis.

Table 4. Repeat revascularization analysis.
Coronary flow at transit time flow measurement of the left internal thoracic (LITA) – left anterior descending (LAD) was 50 [38–75] ml/min. The TTFM of the piggyback proximal anastomosis is described in Table 5. All grafts showed sufficient flow to their target coronary. The second graft demonstrated superior flow rates, especially when an artery was utilized, as compared to either a second SVG graft or the first SVG graft (p = 0.003). This was particularly true considering the posterior descending artery (PDA), p = 0.019. The median pulsatility index for the vein-on-vein, artery-on-vein, and vein-on-aorta were 2.1 [2.0–2.8], 2.0 [1.8–2.0], and 2.5 [2.0–3.0], p = 0.026, respectively. It is conceivable that the arterial conduit (from an artery-on-vein piggyback configuration) exhibited a higher average flow compared to the venous conduit (from a vein-on-vein piggyback configuration) due to a selection bias in conduit choice based on target vessel characteristics. The surgical strategy prioritizes the use of the radial artery for chronic total occlusions (CTOs) or vessels with a very high degree of stenosis—particularly the posterior descending artery (PDA)—while a venous conduit is typically employed for vessels with a lower degree of stenosis. Consequently, the higher runoff in the target vessel receiving the arterial conduit may account for the increased TTFM values observed.
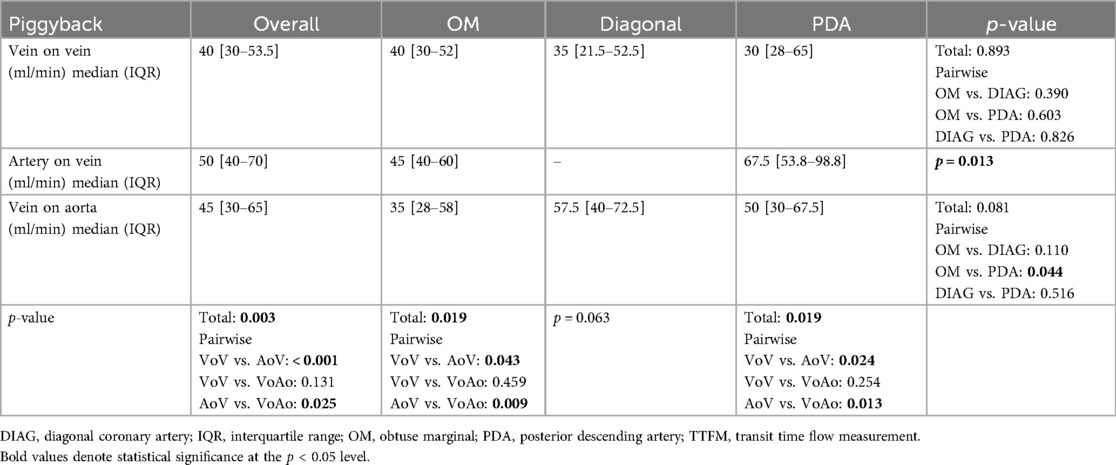
Table 5. Intraoperative TTFM flows on the piggyback proximal anastomosis.
The artery-on-vein piggyback technique was the only approach to show a significant difference among revascularization districts, favoring the PDA territory. Anastomoses to the diagonal artery were limited to only two cases of artery-on-vein piggyback configurations, preventing a thorough analysis. There only flow distinctions observed concerning the other target coronary arteries occurred between the OM and PDA conduits of the vein-on-aorta configurations (p = 0.044).
The results from our study combining clampless devices and the piggyback proximal anastomosis technique during OPCABG focused on postoperative outcomes and intraoperative TTFM data, with particular attention given to the potential advantages of reducing aortic manipulation.
Our analysis highlights three key benefits. First, adopting a single clampless aortic inflow for all the proximal anastomosis is safe and provides strong early mid-term outcomes. Second, by reducing aortic manipulation and minimizing additional holes, this approach significantly lowers the risk of stroke, offering an alternative strategy to anaortic OPCABG in patients with some degree of calcium in the ascending aorta, when anaortic technique is not achievable. Third, intraoperative TTFM demonstrated excellent flows, especially when arterial grafts were used with no postoperative myocardial infarctions.
These results on the piggyback technique are in line with previous reports: Yanagawa et al. described a single surgeon experience of 17 patients undergoing OPCABG with the piggyback technique aided with the Heartstring III Proximal Seal System (10). No graft failure or revisions were described, and TTFM showed no competitive flow between the two piggyback conduits. In a study by Hayashi et al., 175 piggyback anastomoses were carried out among 213 CABG patients where the RITA was employed (11). However, a specific analysis of the piggyback outcomes was not conducted. Finally, Hamasaki et al. described their cohort of 28 piggyback proximal anastomoses highlighting no cases of graft damage or bleeding at the anastomosis site, no strokes or other complications associated with proximal anastomosis (15).
Our findings revealed a very low incidence of postoperative strokes, affirming the hypothesis that reduced aortic manipulation minimizes cerebrovascular complications. Furthermore, we observed no postoperative myocardial infarctions, and the need for transfusion support was within acceptable limits. These outcomes suggest that our technique is both safe and effective in maintaining cardiac perfusion without increasing bleeding risks. With a low rate of readmissions and no in-hospital or 30-day mortality, the technique demonstrates favorable short-term survival and excellent postoperative results. Most importantly, the equal distribution of repeat revascularization among the piggyback grafts shows that these events are independent of the configuration.
The combination of piggyback and clampless technique provides a valuable alternative for patients with high cerebrovascular risk or significant aortic disease. By reducing the number of aortic punctures, it decreases the risk of clinical stroke and embolization. Additionally, it offers mechanical advantages when using smaller arterial conduits, such as the radial artery or RITA, with a proximal inflow in the aorta. Direct proximal anastomoses of these conduits to the aorta carry risks, including graft kinking or flattening, which can compromise graft patency. By utilizing a single, well-supported anastomotic site, the piggyback method avoids these complications and enhances long-term graft functionality (10, 11, 15). These benefits underscore its potential as a safer, more streamlined approach, particularly for patients with complex aortic conditions.
Further supporting the efficacy of this technique, observations from redo-CABG procedures show that proximal anastomotic sites of old SVG often remain patent, even when the grafts themselves have occluded (16, 17). This finding highlights the durability of the proximal anastomotic site and reinforces the potential benefits of limiting aortic manipulation. By avoiding the so-called “Swiss cheese phenomenon”, where multiple punctures in the aorta are made for individual grafts, the piggyback technique offers a more streamlined and possibly safer approach with potential benefit in reducing the burden of SBI with clinical implications in the mid and long term outcomes of patients post CABG (6).
This study has some limitations, including an early mid-term follow-up period, a relatively small cohort size, and a single-surgeon experience. Further multicenter studies with larger patient groups and extended follow-up are needed to confirm the long-term benefits of the clampless piggyback technique, particularly for graft patency and potential cognitive outcomes.
Standardized neuropsychological tests like objective measures of memory, attention and concentration, executive function, and processing speed and reaction time were not routinely incorporated to evaluate postoperative cognitive dysfunction (POCD). Therefore, the assessment may not have fully captured the subtle cognitive deficits associated with SBI and POCD.
The clampless piggyback proximal anastomosis technique demonstrates promising early mid-term outcomes in CABG patients, particularly in minimizing stroke risk and maintaining graft patency. The combination of venous and arterial conduits using this method appears to optimize flow, as evidenced by the TTFM data, while avoiding the pitfalls of traditional anastomosis techniques that involve multiple aortic punctures. The low incidence of major postoperative complications and favorable clinical outcomes support the continued use of this method, particularly in high-risk patients. Further studies with extended follow-up are warranted to confirm the long-term benefits of this technique.
The data that supports the findings of this study are available upon reasonable request to the corresponding author, pending institutional approval. Requests to access the datasets should be directed to bWFzc2ltby5iYXVkb0BpY2xvdWQuY29t.
The studies involving humans were approved by Main Line Health Hospitals Institutional Review Board (IRB 45CFR164.512). The studies were conducted in accordance with the local legislation and institutional requirements. The ethics committee/institutional review board waived the requirement of written informed consent for participation from the participants or the participants' legal guardians/next of kin because of the retrospective nature of the study.
MB: Conceptualization, Data curation, Formal analysis, Investigation, Methodology, Project administration, Software, Validation, Visualization, Writing – original draft, Writing – review & editing. FC: Data curation, Investigation, Validation, Visualization, Writing – review & editing. AY: Data curation, Investigation, Visualization, Writing – review & editing. CM: Investigation, Visualization, Writing – review & editing. GT: Conceptualization, Investigation, Methodology, Project administration, Resources, Supervision, Validation, Writing – original draft, Writing – review & editing.
The author(s) declare that no financial support was received for the research, authorship, and/or publication of this article.
GT reports a relationship with Peters Surgical SAS that includes consulting or advisory.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The author(s) declare that no Generative AI was used in the creation of this manuscript.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Puskas JD, Winston AD, Wright CE, Gott JP, Brown WM, Craver JM, et al. Stroke after coronary artery operation: incidence, correlates, outcome, and cost. Ann Thorac Surg. (2000) 69:1053–6. doi: 10.1016/s0003-4975(99)01569-6
2. Roach GW, Kanchuger M, Mangano CM, Newman M, Nussmeier N, Wolman R, et al. Adverse cerebral outcomes after coronary bypass surgery. Multicenter study of perioperative ischemia research group and the ischemia research and education foundation investigators. N Engl J Med. (1996) 335:1857–63. doi: 10.1056/NEJM199612193352501
3. Sun X, Lindsay J, Monsein LH, Hill PC, Corso PJ. Silent brain injury after cardiac surgery: a review: cognitive dysfunction and magnetic resonance imaging diffusion-weighted imaging findings. J Am Coll Cardiol. (2012) 60:791–7. doi: 10.1016/j.jacc.2012.02.079
4. Guo J, Zhou C, Yue L, Yan F, Shi J. Incidence and risk factors for silent brain infarction after on-pump cardiac surgery: a meta-analysis and meta-regression of 29 prospective cohort studies. Neurocrit Care. (2021) 34:657–68. doi: 10.1007/s12028-020-01048-5
5. Serruys PW, Morice M-C, Kappetein AP, Colombo A, Holmes DR, Mack MJ, et al. Percutaneous coronary intervention versus coronary-artery bypass grafting for severe coronary artery disease. N Engl J Med. (2009) 360:961–72. doi: 10.1056/NEJMoa0804626
6. Baudo M, Torregrossa G, Puskas JD. The 10 commandments for proximal anastomosis during CABG: techniques and technologies for vein and arterial grafts. Innovations (Phila). (2024) 19(5):464–70. doi: 10.1177/15569845241279249
7. Bonacchi M, Prifti E, Bugetti M, Cabrucci F, Cresci M, Lucá F, et al. In situ skeletonized bilateral thoracic artery for left coronary circulation: a 20-year experience. Eur J Cardiothorac Surg. (2020) 57:160–7. doi: 10.1093/ejcts/ezz138
8. Yamaguchi A, Adachi H, Tanaka M, Ino T. Efficacy of intraoperative epiaortic ultrasound scanning for preventing stroke after coronary artery bypass surgery. Ann Thorac Cardiovasc Surg. (2009) 15:98–104. Available online at: https://www.atcs.jp/pdf/2009_15_2/98.pdf19471223
9. Daniel WT, Kilgo P, Puskas JD, Thourani VH, Lattouf OM, Guyton RA, et al. Trends in aortic clamp use during coronary artery bypass surgery: effect of aortic clamping strategies on neurologic outcomes. J Thorac Cardiovasc Surg. (2014) 147:652–7. doi: 10.1016/j.jtcvs.2013.02.021
10. Yanagawa B, Orozco-Sevilla V, Pawale A, Puskas JD. Piggyback technique facilitates off-pump coronary artery bypass graft by using a proximal anastamostic device with arterial conduits. J Thorac Cardiovasc Surg. (2015) 150:725–7. doi: 10.1016/j.jtcvs.2015.05.065
11. Hayashi Y, Ito T, Maekawa A, Sawaki S, Tokoro M, Yanagisawa J, et al. Effect of modified proximal anastomosis of the free right internal thoracic artery: piggyback and foldback techniques. Interact Cardiovasc Thorac Surg. (2016) 22:265–72. doi: 10.1093/icvts/ivv333
12. Salenger R, Rodriquez E, Efird JT, Gouge CA, Trubiano P, Lundy EF. Clampless technique during coronary artery bypass grafting for proximal anastomoses in the hostile aorta. J Thorac Cardiovasc Surg. (2013) 145:1584–8. doi: 10.1016/j.jtcvs.2012.05.045
13. Kikuchi K, Tambara K, Yamamoto T, Yamasaki M, Hirose H, Amano A. The use of enclose(®)II anastomosis assist device for the proximal coronary branch anastomosis to vascular graft. Ann Vasc Dis. (2010) 3:84–6. doi: 10.3400/avd.AVDhdi08023
14. Torregrossa G, Baudo M, Yakobitis A, Murray C, Cavanaugh SM, Purrman KC. Evaluating the feasibility of a novel micro Titanium fastener to facilitate robot-assisted coronary artery bypass grafting. Innovations (Phila). (2024) 19:439–42. doi: 10.1177/15569845241266596
15. Hamasaki A, Uchida T, Kuroda Y, Yamashita A, Sadahiro M. Piggyback anastomosis using a single heartstring device: a low-invasiveness, low-cost technique. Multimed Man Cardiothorac Surg. (2019) 2019. doi: 10.1510/mmcts.2019.034
16. Sano K, Mintz GS, Carlier SG, Fujii K, Yasuda T, Kimura M, et al. Intravascular ultrasonic differences between aorto-ostial and shaft narrowing in saphenous veins used as aortocoronary bypass grafts. Am J Cardiol. (2006) 97:1463–6. doi: 10.1016/j.amjcard.2005.11.080
Keywords: proximal anastomosis, CABG, stroke, OPCABG, piggyback, aortic manipulation
Citation: Baudo M, Cabrucci F, Yakobitis A, Murray C and Torregrossa G (2025) Minimizing stroke risk in off-pump CABG: the role of clampless devices and the piggyback proximal anastomosis technique. Front. Cardiovasc. Med. 12:1555394. doi: 10.3389/fcvm.2025.1555394
Received: 4 January 2025; Accepted: 17 February 2025;
Published: 3 March 2025.
Edited by:
Antonio Maria Calafiore, Henry Dunant Hospital, GreeceReviewed by:
Laura DiChiacchio, Cedars Sinai Medical Center, United StatesCopyright: © 2025 Baudo, Cabrucci, Yakobitis, Murray and Torregrossa. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Massimo Baudo, bWFzc2ltby5iYXVkb0BpY2xvdWQuY29t
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.