
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Cardiovasc. Med., 28 February 2025
Sec. Sex and Gender in Cardiovascular Medicine
Volume 12 - 2025 | https://doi.org/10.3389/fcvm.2025.1511464
This article is part of the Research TopicSex-Specific Risk Factors and Cardiovascular Disease Risk in WomenView all 10 articles
 Liwei Huang1,2,†
Liwei Huang1,2,† Luwei Ye1,2,†
Luwei Ye1,2,† Hongmei Zhang1,2
Hongmei Zhang1,2 Qingfeng Zhang1,2
Qingfeng Zhang1,2 Geqi Ding1,2
Geqi Ding1,2 Chunmei Li1,2
Chunmei Li1,2 Yan Deng1,2
Yan Deng1,2 Lixue Yin1,2*
Lixue Yin1,2* Yi Wang1,2*
Yi Wang1,2*
Background: Non-invasive myocardial work (MW) is a more precise parameter for evaluating left ventricular (LV) systolic function. However, studies examining sex-based differences in MW during exercise stress echocardiography (SE) in healthy individuals are scarce. Previous research has shown that global work efficiency (GWE) decreases following exercise.
Objectives: To characterize sex-based differences in MW during exercise SE in healthy adults and to explore the factors influencing the decline in GWE post-exercise.
Methods: The study enrolled 200 healthy adults, all of whom underwent echocardiographic assessments both at rest and immediately after completing a symptom-limited treadmill stress test. We measured LV volume, ejection fraction (EF), force, peak positive strain (PPS), global work index (GWI), global constructive work (GCW), global wasted work (GWW), and GWE at rest and post-exercise.
Results: GWI, GCW, and GWW increased, while GWE decreased after exercise. There were no significant differences in any of the global MW parameters between sexes at rest (all p > 0.05). The change in △GWE was greater in women (p < 0.05), but no significant differences were found in other MW reserve parameters between sexes. The multivariable linear regression analysis revealed that GWW was independently associated with PPS (β = 0.842, p < 0.0001) and force (β = 0.306, p = 0.023). Furthermore, the multivariable linear regression analysis showed that GWE was independently associated with PPS (β = −0.395, p = 0.018) and EF (β = −0.236, p < 0.001).
Conclusion: Sex had a minimal effect on MW-based LV systolic function in healthy adults. GWE decreased post-exercise, and both PPS and force were independently associated with GWW. These findings suggest that higher contractility is achieved at the cost of increased wasted work, which subsequently leads to a decrease in mechanical efficiency.
The assessment of myocardial function is a critical component of routine clinical practice. Myocardial strain provides additional insights into cardiac performance beyond traditional parameters of left ventricular (LV) systolic function (1). However, strain does not reflect myocardial work (MW) and oxygen consumption, as it does not adjust for loading conditions. MW, which incorporates both deformation and load into the analysis, has been proposed as an alternative tool for evaluating LV myocardial systolic function. MW assessment was initially calculated using invasive pressure measurements, which limited its widespread application in clinical practice (2, 3). Russell et al. (4) proposed a method for the non-invasive estimation of regional and global MW through the analysis of pressure-strain loops (PSLs). To date, some studies have used this technique to analyze the reference ranges of MW in normal adults (5, 6). The technique has also been employed to analyze LV systolic function in patients with coronary artery disease and cardiac amyloidosis (7–9). However, studies on MW parameters and sex differences during exercise stress echocardiography (SE) in normal adults are scarce. Borrie et al.’s study found that global work efficiency (GWE) decreased after exercise in healthy subjects, but their sample size was small and sex differences were not explored (10). The aims of this study were to characterize sex differences in MW changes during exercise SE and explore the factors influencing the decline in GWE after exercise.
In this cross-sectional study, we prospectively enrolled 258 healthy volunteers between March 2018 and December 2022. The normal participants had blood pressure values within the normal reference range; normal resting and SE results; negative coronary computed tomography (CT) or angiography findings; no history of medication use; no history of hypertension, diabetes, or cardiac diseases; and were non-smokers. Based on these criteria, 58 subjects were excluded for the following reasons: electrocardiographic abnormalities during SE (11 subjects), poor acoustic window during SE (20 subjects), lack of blood pressure measurement during transthoracic echocardiography (16 subjects), and inability to analyze MW (11 subjects) (Figure 1).
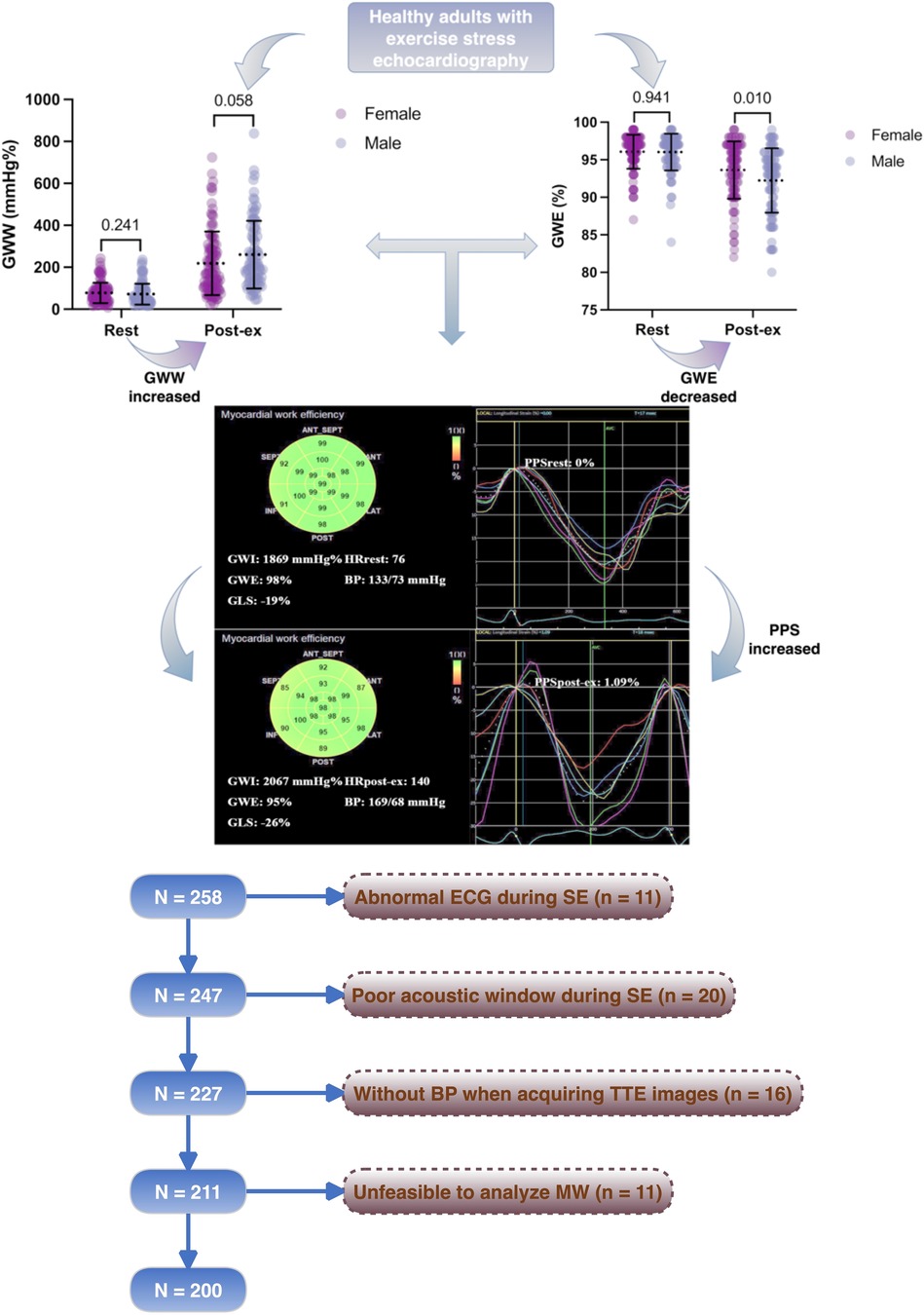
Figure 1. Flowchart of this study.
All subjects underwent clinical examinations, resting 12-lead electrocardiography (ECG), and comprehensive transthoracic echocardiography both at rest and immediately following maximal treadmill stress testing. The clinical examination included measurements of height, weight, body mass index (BMI), and resting blood pressure. Body surface area (BSA) was calculated using the Du Bois formula (11). The normal adults were categorized into male and female groups for subsequent analysis. All subjects were over 18 years of age and were included after providing informed written consent in accordance with the principles of the Declaration of Helsinki. The study was approved by the local scientific ethics committee of Sichuan Provincial People's Hospital.
All subjects underwent standard transthoracic echocardiography using a commercially available ultrasound system, Vivid E95 equipped with an M5S 3.5-MHz transducer (GE Vivid E95, Vingmed Ultrasound, Horten, Norway), at rest and immediately after exercise in the left lateral decubitus position. Electrocardiogram-triggered echocardiographic data were acquired and digitally stored in a cine-loop format for offline analysis using EchoPAC (EchoPAC 203, General Electric Vingmed Ultrasound). At rest, all subjects underwent a comprehensive two-dimensional echocardiographic assessment in accordance with the current guidelines (12). LV end-diastolic and end-systolic volumes (LVEDV and LVESV) were measured in the apical two- and four-chamber views. LVEF was calculated using the Simpson biplane method (13). LVEDV and LVESV were indexed into BSA, presented as LV end-diastolic volume index (LVEDVI) and LV end-systolic volume index (LVESVI), respectively. Ventricular-arterial coupling (VAC) was calculated as stroke volume (SV) divided by ESV. Force was calculated as the ratio of peak systolic blood pressure (SBP) to ESV (14). Arterial elastance (AE) was calculated by dividing LV end-systolic pressure (LVESP) by SV, with LVESP estimated as arterial systolic pressure × 0.9 (15).
LV global longitudinal strain (GLS) was obtained using automated function imaging in standard two-dimensional cine loops with a frame rate >70 frames per second (16). The regional speckle area of interest was manually adjusted for optimal tracking results. The GLS was calculated at the point of peak value during systole using a 17-myocardial segment model (17).
The principles for estimating LV pressure and work have been described previously (4). Constructive work (CW) included the sum of work performed during shortening in systole and the negative work during lengthening in the isovolumetric relaxation phase. Myocardial work index (WI) denotes the total work within the area of the LV pressure-strain loop calculated from mitral valve closure to mitral valve opening. Wasted work (WW) comprises negative systolic work due to systolic lengthening and the work of shortening in the isovolumic relaxation phase. Myocardial work efficiency (WE) was calculated as the ratio of CW to (CW + WW). LV global constructive work index (GWI), global constructive work (GCW), global wasted work (GWW), and global work efficiency (GWE) were calculated as the average of myocardial WI, CW, WW, and WE across all segmental values.
All the MW parameters were analyzed both at rest and post-exercise. Event timing (mitral valve opening and closing, and aortic valve opening and closing) was manually adjusted. Each echocardiographic parameter was averaged over three consecutive cardiac cycles. From the longitudinal speckle-tracking curve, we obtained the peak positive strain (PPS) during the early systole phase (18). If no early systolic lengthening (ESL) occurred during the early systole phase, the PPS was set to zero. If ESL was present, the maximum value of the positive strain during the ESL duration was considered the PPS (Figure 1). Therefore, ESL can also be described as the PPS. △EF, △GLS, and △force were calculated as the differences in EF, GLS, and force between rest and post-exercise values. MW reserve was calculated as the difference in GWI, GCW, GWW, and GWE between rest and post-exercise values, presented as △GWI, △GCW, △GWW, and △GWE, respectively.
All subjects performed a symptom-limited treadmill exercise test (TMX-425, Full Vision Inc., Kansas, USA) using standard Bruce protocols (19). Participants were encouraged to exercise until exhaustion. A baseline 12-lead ECG and blood pressure were recorded, and measurements were repeated at 2-min intervals during the examination, at peak exertion, and after exercise. The maximum exercise capacity in metabolic equivalents (METs) was recorded, where 1 MET corresponds to 3.5 ml/kg/min oxygen consumption, estimated based on the protocol, speed, and grade achieved (20). Exercise duration and the ratio of peak heart rate (HR) to target HR (calculated using the 220 − age formula) were also recorded automatically.
All statistical analyses were performed using SPSS version 23.0 (SPSS, Armonk, NY). Continuous variables are presented as the mean ± standard deviation (SD). Skewed data are presented as median [interquartile range (IQR)]. The normality of distribution was assessed using the Kolmogorov–Smirnov test. Comparisons of continuous variables with normal distributions between groups were performed using unpaired t-tests, while non-normally distributed variables were analyzed using the Mann–Whitney test. The 95% confidence interval was calculated as ±1.96 SDs from the mean. Correlations between two parameters were analyzed using Pearson's correlation test. Stepwise multivariable linear regression analyses were conducted to identify independent factors associated with GWW and GWE. A p-value < 0.05 was considered statistically significant.
GWI analyses at baseline and immediately after exercise were repeated in 10 randomly selected patients at least 4 weeks after the initial analysis. These analyses were performed by the original investigator and a second investigator, both of whom were blinded to the original measurements, to assess intraobserver and inter-observer variability. The intraclass correlation coefficient (ICC) was calculated to evaluate variability.
Resting and treadmill exercise SE were performed in 200 healthy adults (53% women; aged 47.0 ± 12.8 years; age range, 23–69 years). The clinical characteristics of the whole population are displayed in Table 1. The men had larger BSA and higher SBP and METs than the women (all p < 0.05).
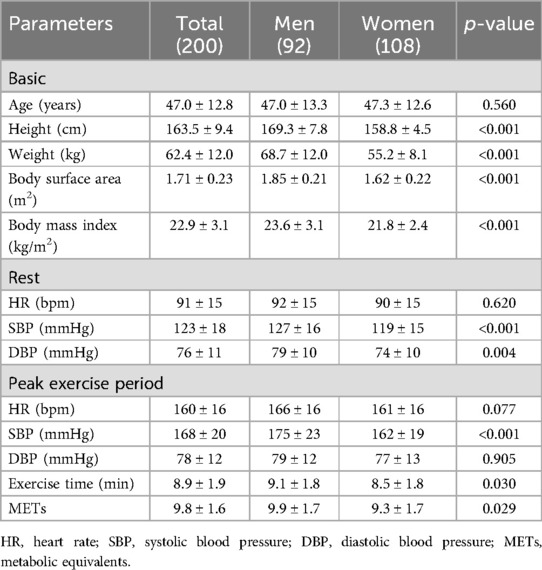
Table 1. Characteristics of the population.
The SE parameters are displayed in Table 2. EF, AE, VAC, force, GLS, and PPS all increased after exercise. The women had higher EF and GLS than the men both at rest and load (p < 0.05). The women had higher AE at rest (p < 0.05), but no significant difference was observed after exercise. The men had higher force than the women at rest (p < 0.05), but there was no significant difference after exercise. PPS was lower in the men at rest, but higher than that in the women after exercise (p < 0.05). △EF and △force in the men were much higher than those in the women (p < 0.05). In addition to differences between sexes, a comparison of the two age groups (<48 vs. ≥48 years) was also conducted (Supplementary Table S1).
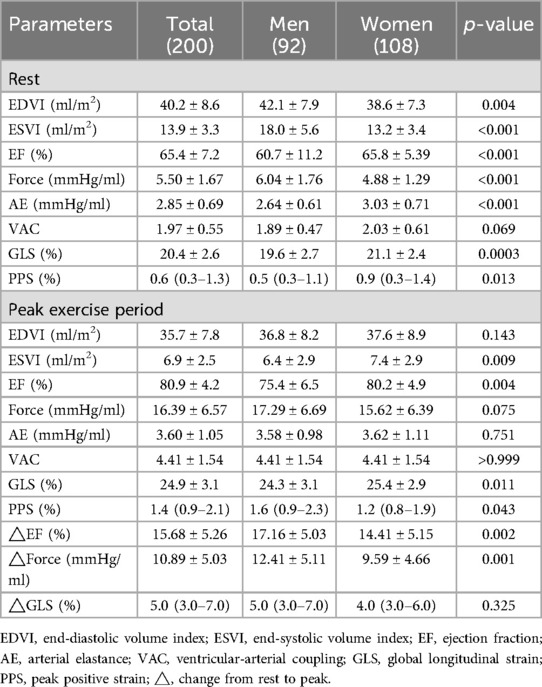
Table 2. Stress echocardiographic parameters of left ventricular systolic function by sex in normal adults.
MW parameters are displayed in Table 3 and Figure 2. GWI, GCW, and GWW increased, but GWE decreased after exercise (Figure 3). There was no significant difference in all global MW parameters between sexes at rest. GWE was significantly higher in the women after exercise (p < 0.05). △GWE was higher in the women (p < 0.05) but no significant differences were observed in other MW reserve parameters between sexes.
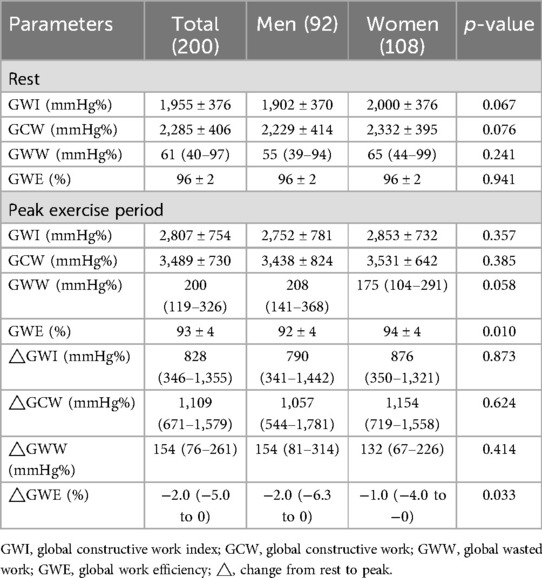
Table 3. Global MW parameters and MW reserve during SE.
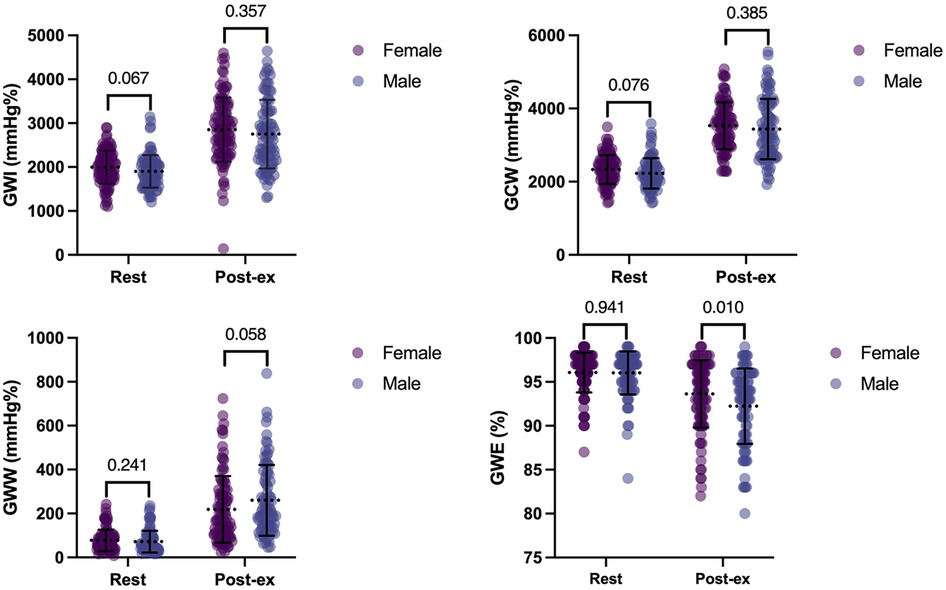
Figure 2. MW parameters in normal adults. There was no significant difference in all the MW parameters between sexes at rest. GWE was significantly higher in the women after exercise. GWI, global constructive work index; GCW, global constructive work; GWW, global wasted work; GWE, global work efficiency.
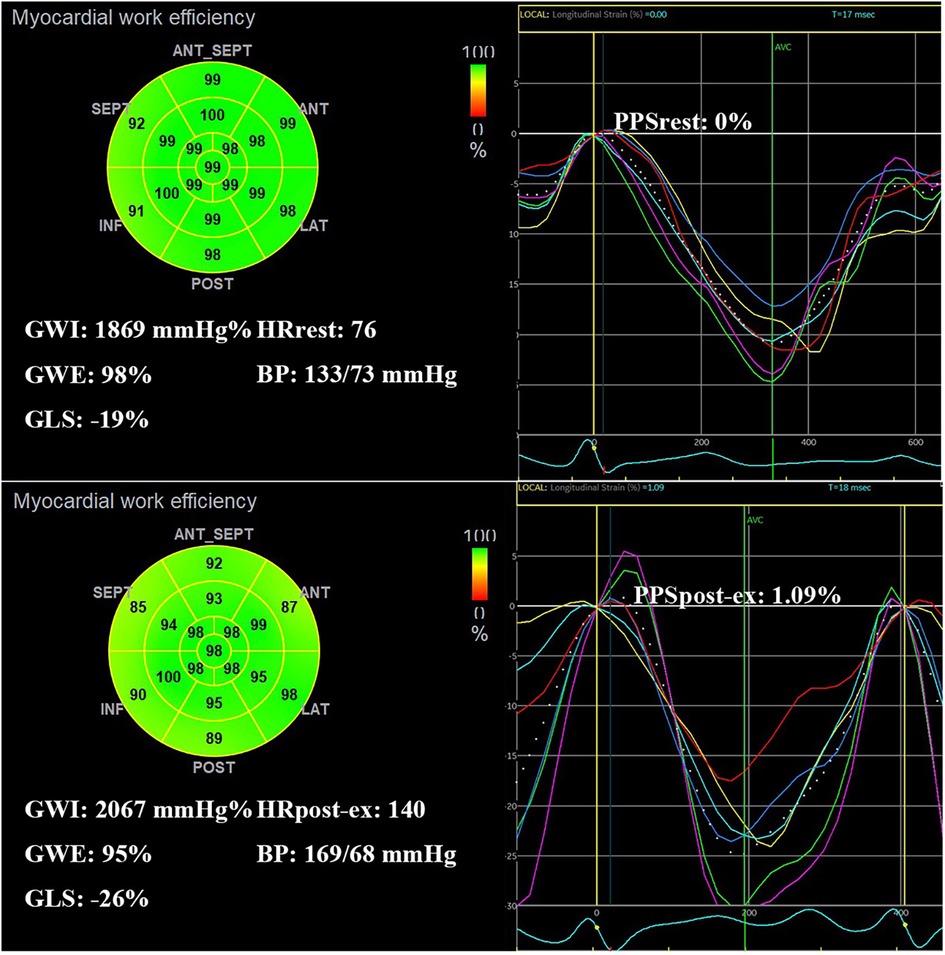
Figure 3. Example of a normal adult with decreased GWE and increased PPS after exercise. A bull's-eye plot of myocardial work shows GWE is 98% at rest and 95% after exercise. Time-strain curve during one cardiac cycle (white dotted line) shows PPS increased from 0% at rest to 1.09% after exercise. GWI, global constructive work index; GWE, global work efficiency; GLS, global longitudinal strain; HR, heart rate; BP, blood pressure; PPS, peak positive strain; post-ex, immediately after exercise.
Tables 4, 5 and Figure 4 show the relationship between GWW, GWE, and other echocardiographic parameters. Pearson’s correlation test showed that GWW was significantly correlated to GLS, EF, PPS, and force (all p < 0.0001). The multivariable linear regression analysis showed that GWW was independently associated with PPS (β = 0.842, p < 0.0001) and force (β = 0.306, p = 0.023). Pearson’s correlation test showed that GWE was significantly correlated to CI, VAC, AE, EF, PPS, and force (all p < 0.0001). Finally, the multivariable linear regression analysis showed that GWE was independently associated with PPS (β = −0.395, p = 0.018) and EF (β = −0.236, p < 0.001).
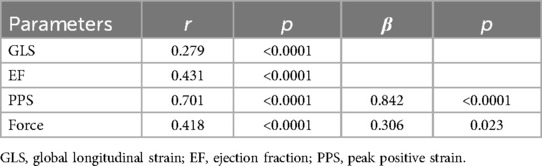
Table 4. Univariable and multivariable linear regression of global wasted work.
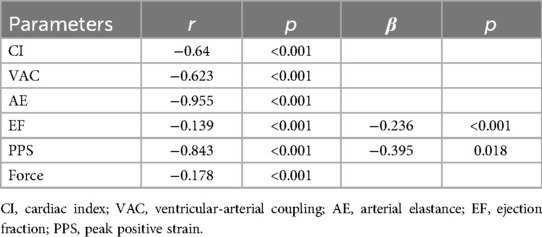
Table 5. Univariable and multivariable linear regression of global work efficiency.
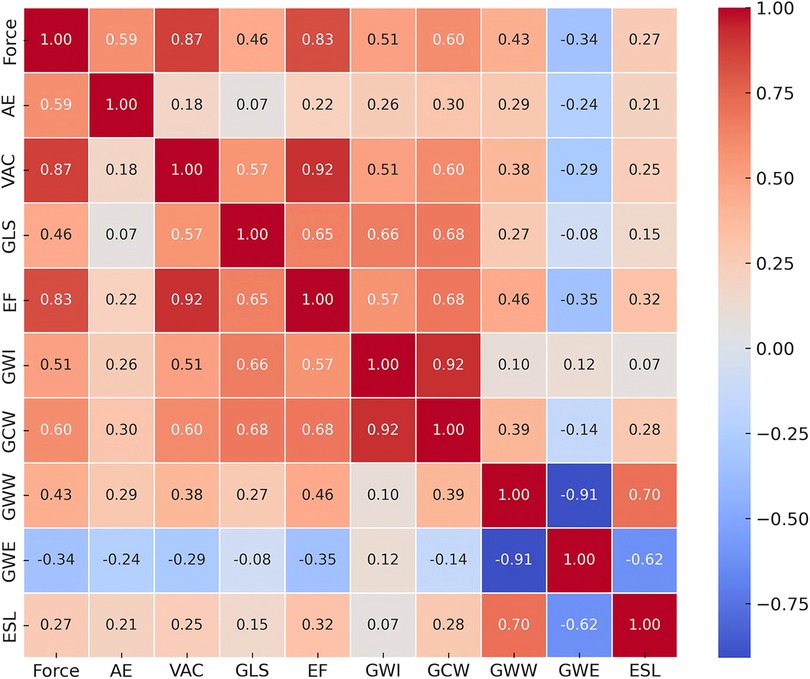
Figure 4. A heat map of the correlation analysis of myocardial work and other echocardiographic parameters. Red indicates a negative correlation and blue indicates a positive correlation. GLS, global longitudinal strain; EF, ejection fraction; GWI, global constructive work index; GCW, global constructive work; GWW, global wasted work; GWE, global work efficiency; ESL, early systolic lengthening; VAC, ventricular-arterial coupling; AE, arterial elastance.
The ICC for intraobserver variability was 0.92 for GWI at rest and 0.89 for GWI after exercise. The ICC for inter-observer variability was 0.91 for GWI at rest and 0.87 for GWI after exercise.
The main findings of the present study can be summarized as follows: (1) there were no significant differences in most of the MW parameters between the men and women, which indicates MW is a non-sex-specific parameter to evaluate LV systolic function; (2) GWE decreased after exercise in healthy adults and PPS and force were independently associated with GWW, suggesting that higher contractility is achieved at the expense of increased wasted work, leading to decreased mechanical efficiency.
A previous study showed that SBP is an important determinant of myocardial strain (21). Increased afterload has a negative impact on strain. MW is emerging as an alternative tool for studying LV systolic function because it incorporates both deformation and load into its analysis. Russell et al. (4) demonstrated that pressure-strain loops can estimate LV performance in a non-invasive manner, deriving LV pressure curves from non-invasively acquired brachial artery cuff pressure. However, there are few reports on MW combined with treadmill exercise stress echocardiography in normal adults, and its application remains to be explored. Galli et al. (5) studied 115 normal (mean age 36.3 years, 67% men) adults and found that GWI and GCW were significantly higher in the women at rest (p < 0.05), but there was no significant difference in GWE between the sexes. Manganaro et al. (6) studied 226 normal adults (mean age 45 ± 13 years, 38% men). They found that only the GWE of the men at rest was significantly lower than that of the women. In our study, only the GWE of the men was significantly lower than that of the women after exercise, as other global MW parameters showed no significant difference both at rest and at load. Previous studies and this study have revealed that global MW parameters are consistent between sexes at rest, and this study further confirms that these parameters remain consistent after exercise.
It is well-known that the differences in the cardiac chamber and great arterial dimensions among the sexes are largely attributable to variations in body size (22). In this study, many of the parameters in the men were significantly higher than those in the women, which suggests that it is important to take into account the impact of sex. Previous studies have found that △GLS is significantly higher in men; however, no significant difference between the sexes was observed after adjustment for BSA (23). In this study, most of the MW reserve parameters showed no statistically significant differences. This suggests that the MW reserve is more stable than △GLS and is less influenced by sex.
When LV pressure rises during early systole, myocardial fibers with reduced contractility tend to stretch rather than shorten. This interval is referred to as the duration of ESL. It has been hypothesized that ESL occurs due to heterogeneity in the contractility profile of myocardial segments, making it a potential early marker of myocardial dysfunction (24). Previous studies have suggested that ESL may be a useful diagnostic marker for significant coronary artery disease. In addition, ESL has been shown to correlate with final infarct size following myocardial infarction (25, 26).
However, Prinzen and Lumens (27) observed that in patients with left bundle branch block (LBBB), the early-activated regions begin to shorten before aortic valve opening, thereby stretching the later-activated regions. This early systolic stretching enhances the contractile force of the late-activated regions due to the local Frank–Starling mechanism. At the same time, some studies have reported that ESL is also present in healthy adults without heart disease (24, 25). Our study also found that ESL, which can also be described as PPS, occurs in healthy adults both at rest and load. According to the definition of strain, the stretching strain during systole is represented as a positive value on the longitudinal speckle-tracking curve. The maximum value of this positive strain during the early systolic phase corresponds to PPS. Based on Russell's theory, MW is calculated from PSLs. The work performed by myocardial stretching during the systolic phase is referred to as WW. Therefore, the myocardial work during ESL duration is calculated as WW (4). Our study also found that PPS increased after exercise in healthy adults. Both previous studies and our findings indicate an increase in GWW and a decrease in GWE after loading in healthy adults. However, the underlying mechanisms and causes of these changes remain unexplained (10). Why does this phenomenon occur?
LVEF is not synonymous with LV contractility. Unlike LVEF, force is a systolic function parameter that is independent of preload and afterload (28). In both ischemic and non-ischemic hearts, preserved force is associated with a more favorable prognosis. Recently, the core protocol of SE has been enhanced by incorporating LV contractile reserve assessment based on force (14). In our study, both force and PPS increased after exercise, indicating that LV contractility improved following exercise stress. At the same time, we found that GWW was independently associated with PPS and force. This suggests that PPS may contribute to an increase in myocardial mechanical work during stress. During the early systolic phase, the myocardium initially stretches and then contracts, likely to enhance the force of myocardial contraction. As a result, LV contractility increases at the expense of elevated GWW, which subsequently leads to a reduction in myocardial mechanical efficiency.
This is a single-center study with a moderate sample size. Further studies involving larger sample sizes are needed to explore the characteristics across different age subgroups. Second, the image quality issues inherent to speckle-tracking echocardiography were exacerbated after exercise. However, we excluded subjects without optimal image quality from the MW analysis. In addition, increased HR reduces temporal resolution and strain accuracy.
MW-based LV systolic function, including contractile reserve, was less influenced by sex in healthy adults. GWE decreased and GWW increased after exercise. GWW was independently associated with PPS and force, suggesting that higher contractility is achieved at the expense of increased WW, ultimately leading to reduced myocardial mechanical efficiency.
The original contributions presented in the study are included in the article/Supplementary Material, further inquiries can be directed to the corresponding authors.
The studies involving humans were approved by the local scientific Ethics Committee of the Sichuan Provincial People's Hospital. The studies were conducted in accordance with the local legislation and institutional requirements. Written informed consent for participation in this study was provided by the participants' legal guardians/next of kin.
LH: Conceptualization, Writing – original draft. LY: Investigation, Writing – review & editing. HZ: Validation, Writing – review & editing. QZ: Software, Validation, Writing – review & editing. GD: Data curation, Writing – review & editing. CL: Resources, Supervision, Writing – review & editing. YD: Funding acquisition, Resources, Writing – review & editing. LY: Resources, Writing – review & editing. YW: Conceptualization, Methodology, Resources, Supervision, Writing – review & editing, Writing – original draft.
The author(s) declare financial support was received for the research, authorship, and/or publication of this article. This work was supported by a research grant from the Science and Technology Department of Sichuan Province Project (grant number: 23NSFSC0118).
We would like to thank all participants for their support and contributions to this study.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The author(s) declare that no Generative AI was used in the creation of this manuscript.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fcvm.2025.1511464/full#supplementary-material
1. Ersbøll M, Valeur N, Mogensen UM, Andersen MJ, Møller JE, Velazquez EJ, et al. Prediction of all-cause mortality and heart failure admissions from global left ventricular longitudinal strain in patients with acute myocardial infarction and preserved left ventricular ejection fraction. J Am Coll Cardiol. (2013) 61(23):2365–73. doi: 10.1016/j.jacc.2013.02.061
2. Tyberg JV, Forrester JS, Wyatt HL, Goldner SJ, Parmley WW, Swan HJ. An analysis of segmental ischemic dysfunction utilizing the pressure-length loop. Circulation. (1974) 49(4):748–54. doi: 10.1161/01.cir.49.4.748
3. Delhaas T, Arts T, Prinzen FW, Reneman RS. Regional fibre stress-fibre strain area as an estimate of regional blood flow and oxygen demand in the canine heart. J Physiol. (1994) 477(Pt 3):481–96. doi: 10.1113/jphysiol.1994.sp020209
4. Russell K, Eriksen M, Aaberge L, Wilhelmsen N, Skulstad H, Remme EW, et al. A novel clinical method for quantification of regional left ventricular pressure-strain loop area: a non-invasive index of myocardial work. Eur Heart J. (2012) 33(6):724–33. doi: 10.1093/eurheartj/ehs016
5. Galli E, John-Matthwes B, Rousseau C, Schnell F, Leclercq C, Donal E. Echocardiographic reference ranges for myocardial work in healthy subjects: a preliminary study. Echocardiography. (2019) 36(10):1814–24. doi: 10.1111/echo.14494
6. Manganaro R, Marchetta S, Dulgheru R, Ilardi F, Sugimoto T, Robinet S, et al. Echocardiographic reference ranges for normal non-invasive myocardial work indices: results from the EACVI NORRE study. Eur Heart J Cardiovasc Imaging. (2019) 20(5):582–90. doi: 10.1093/ehjci/jey188
7. Lin J, Wu W, Gao L, He J, Zhu Z, Pang K, et al. Global myocardial work combined with treadmill exercise stress to detect significant coronary artery disease. J Am Soc Echocardiogr. (2022) 35(3):247–57. doi: 10.1016/j.echo.2021.10.009
8. Edwards NFA, Scalia GM, Putrino A, Appadurai V, Sabapathy S, Anderson B, et al. Myocardial work and left ventricular contractile reserve during stress echocardiography: an angiographic validation. Echocardiography. (2021) 38(10):1711–21. doi: 10.1111/echo.15194
9. Clemmensen TS, Eiskjær H, Mikkelsen F, Granstam SO, Flachskampf FA, Sørensen J, et al. Left ventricular pressure-strain-derived myocardial work at rest and during exercise in patients with cardiac amyloidosis. J Am Soc Echocardiogr. (2020) 33(5):573–82. doi: 10.1016/j.echo.2019.11.018
10. Borrie A, Goggin C, Ershad S, Robinson W, Sasse A. Noninvasive myocardial work index: characterizing the normal and ischemic response to exercise. J Am Soc Echocardiogr. (2020) 33(10):1191–200. doi: 10.1016/j.echo.2020.05.003
11. Daros CB, Ciampi Q, Cortigiani L, Gaibazzi N, Rigo F, Wierzbowska-Drabik K, et al. Coronary flow, left ventricular contractile and heart rate reserve in non-ischemic heart failure. J Clin Med. (2021) 10:3405. doi: 10.3390/jcm10153405
12. Lang RM, Badano LP, Mor-Avi V, Afilalo J, Armstrong A, Ernande L, et al. Recommendations for cardiac chamber quantification by echocardiography in adults: an update from the American society of echocardiography and the European association of cardiovascular imaging. J Am Soc Echocardiogr. (2015) 28(1):1–39.e14. doi: 10.1016/j.echo.2014.10.003
13. Pugliese NR, DE Biase N, Balletti A, Filidei F, Pieroni A, D'Angelo G, et al. Characterization of hemodynamic and metabolic abnormalities in the heart failure spectrum: the role of combined cardiopulmonary and exercise echocardiography stress test. Minerva Cardiol Angiol. (2022) 70(3):370–84. doi: 10.23736/S2724-5683.21.05743-4
14. Picano E, Bombardini T, Kovačević Preradović T, Cortigiani L, Wierzbowska-Drabik K, Ciampi Q. Left ventricular contractile reserve in stress echocardiography: the bright side of the force. Kardiol Pol. (2019) 77(2):164–72. doi: 10.5603/KP.a2019.0002
15. Sunagawa K, Maughan WL, Burkhoff D, Sagawa K. Left ventricular interaction with arterial load studied in isolated canine ventricle. Am J Physiol. (1983) 245(5 Pt 1):H773–80. doi: 10.1152/ajpheart.1983.245.5.H773
16. Reisner SA, Lysyansky P, Agmon Y, Mutlak D, Lessick J, Friedman Z. Global longitudinal strain: a novel index of left ventricular systolic function. J Am Soc Echocardiogr. (2004) 17(6):630–3. doi: 10.1016/j.echo.2004.02.011
17. Cerqueira MD, Weissman NJ, Dilsizian V, Jacobs AK, Kaul S, Laskey WK, et al. Standardized myocardial segmentation and nomenclature for tomographic imaging of the heart. A statement for healthcare professionals from the cardiac imaging committee of the council on clinical cardiology of the American heart association. Circulation. (2002) 105(4):539–42. doi: 10.1161/hc0402.102975
18. Brainin P, Biering-Sørensen T, Jensen MT, Møgelvang R, Fritz-Hansen T, Vilsbøll T, et al. Prognostic value of early systolic lengthening by strain imaging in type 2 diabetes. J Am Soc Echocardiogr. (2021) 34(2):127–35. doi: 10.1016/j.echo.2020.09.008
19. Pellikka PA, Arruda-Olson A, Chaudhry FA, Chen MH, Marshall JE, Porter TR, et al. Guidelines for performance, interpretation, and application of stress echocardiography in ischemic heart disease: from the American society of echocardiography. J Am Soc Echocardiogr. (2020) 33(1):1–41.e8. doi: 10.1016/j.echo.2019.07.001
20. Mahfouz RA, El Zayat A, Yousry A. Left ventricular restrictive filling pattern and the presence of contractile reserve in patients with low-flow/low-gradient severe aortic stenosis. Echocardiography. (2015) 32(1):65–70. doi: 10.1111/echo.12586
21. Yingchoncharoen T, Agarwal S, Popović ZB, Marwick TH. Normal ranges of left ventricular strain: a meta-analysis. J Am Soc Echocardiogr. (2013) 26(2):185–91. doi: 10.1016/j.echo.2012.10.008
22. Yao GH, Deng Y, Liu Y, Xu MJ, Zhang C, Deng YB, et al. Echocardiographic measurements in normal Chinese adults focusing on cardiac chambers and great arteries: a prospective, nationwide, and multicenter study. J Am Soc Echocardiogr. (2015) 28(5):570–9. doi: 10.1016/j.echo.2015.01.02
23. Wang Y, Li W, Zhang H, Zhang Q, Ding G, Guo Z, et al. Echocardiographic normal reference of left ventricular contractile reserve during treadmill exercise stress echocardiography in healthy Chinese adults—new non-sex-specific parameter for left ventricular contractile reserve evaluation. Int J Gen Med. (2021) 14:7089–98. doi: 10.2147/IJGM.S334400
24. Smedsrud MK, Sarvari S, Haugaa KH, Gjesdal O, Ørn S, Aaberge L, et al. Duration of myocardial early systolic lengthening predicts the presence of significant coronary artery disease. J Am Coll Cardiol. (2012) 60(12):1086–93. doi: 10.1016/j.jacc.2012.06.022
25. Brainin P, Biering-Sørensen SR, Møgelvang R, Jensen JS, Biering-Sørensen T. Duration of early systolic lengthening: prognostic potential in the general population. Eur Heart J Cardiovasc Imaging. (2020) 21(11):1283–90. doi: 10.1093/ehjci/jez262
26. Minamisawa M, Koyama J, Kozuka A, Miura T, Saigusa T, Ebisawa S, et al. Duration of myocardial early systolic lengthening for diagnosis of coronary artery disease. Open Heart. (2018) 5(2):e000896. doi: 10.1136/openhrt-2018-000896
27. Prinzen FW, Lumens J. Investigating myocardial work as a CRT response predictor is not a waste of work. Eur Heart J. (2020) 41(39):3824–6. doi: 10.1093/eurheartj/ehaa677
Keywords: myocardial work, exercise echocardiography, peak positive strain, force, healthy adults
Citation: Huang L, Ye L, Zhang H, Zhang Q, Ding G, Li C, Deng Y, Yin L and Wang Y (2025) Characteristics of myocardial work during exercise stress echocardiography in healthy adults. Front. Cardiovasc. Med. 12:1511464. doi: 10.3389/fcvm.2025.1511464
Received: 15 October 2024; Accepted: 10 February 2025;
Published: 28 February 2025.
Edited by:
Anita Cote, Trinity Western University, CanadaReviewed by:
Attila Oláh, Semmelweis University, HungaryCopyright: © 2025 Huang, Ye, Zhang, Zhang, Ding, Li, Deng, Yin and Wang. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Lixue Yin, eWlubGl4dWVfY2FyZGlhY0AxNjMuY29t; Yi Wang, d2FuZ3lpaGRsQDEyNi5jb20=
†These authors have contributed equally to this work
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.