 Miguel Borregón1*
Miguel Borregón1* María Valero1Asia Ferrández1Álvaro Muñoz1Carmen Roque2Javier-David Benítez-Fuentes1
María Valero1Asia Ferrández1Álvaro Muñoz1Carmen Roque2Javier-David Benítez-Fuentes1
- 1Department of Medical Oncology, Hospital General Universitario de Elche, FISABIO, Alicante, Spain
- 2Department of Radiology, Hospital General Universitario de Elche, FISABIO, Alicante, Spain
Background: Arterial thrombosis is an uncommon complication in cancer patients, often overshadowed by venous thromboembolic events. Its occurrence in patients with solid tumors on active antineoplastic treatment poses a significant clinical challenge.
Key clinical question: Given the lack of consensus on the optimal therapy for arterial thrombosis in cancer patients, the best practices for managing an aortic thrombus, and the benefit of low molecular weight heparin (LMWH) must be reviewed.
Clinical approach: We present the case of a 70-year-old female with stage IVA lung adenocarcinoma who developed an aortic thrombus during chemo-immunotherapy. The thrombus was successfully treated with LMWH, avoiding further complications, and allowing for the continuation of her cancer therapy.
Conclusions: This case highlights the importance of early detection and management of arterial thrombus in cancer patients. LMWH proved effective in resolving the thrombus, underscoring its role in managing such complications.
Introduction
Cancer-associated thrombosis (CAT) is a well-recognized complication in cancer patients, contributing significantly to morbidity and mortality in this population. Thrombosis in cancer patients is multifactorial, involving tumor-related factors, patient characteristics, and treatment modalities (1). While venous thromboembolism (VTE) is the most common type of CAT, arterial thromboembolism (ATE), although less frequent, poses a critical risk, leading to severe cardiovascular events, including myocardial infarction, cerebrovascular events, and peripheral artery disease (2).
The pathophysiology of ATE in cancer involves complex interactions between pro-thrombotic states induced by malignancy, endothelial damage, and hypercoagulability exacerbated by cancer treatments (3). Different epidemiological studies indicate that cancer patients have an elevated risk of ATE compared to the general population (4). However, information related to its management is scarce (3).
The case discussed herein involves a 70-year-old woman with a history of limited stage small cell lung carcinoma (SCLC) treated with radical chemo-radiotherapy in 2008 and a recent diagnosis of stage IVA adenocarcinoma of the lung in December 2023. Her current treatment includes a combination of chemotherapy and immunotherapy (maintenance pemetrexed and pembrolizumab). After a partial response to treatment, the patient developed an arterial thrombus in the ascending aorta. This complication highlights the potential risk for serious thrombotic complications in cancer patients, the importance of cardiovascular monitoring and prompt treatment of CAT in oncology patients.
Case description
A timeline of the key events in this case is presented in Table 1. A 70-year-old Caucasian woman with a significant past medical history presented with asymptomatic aortic thrombosis. Her personal history includes a former smoking habit (35 pack-years, ceased in 2008), hypertension, dyslipidemia, osteoporosis under oral zoledronic acid treatment, and actinic keratosis on the nose. Her surgical history includes resection of breast fibroadenomas and a basal cell carcinoma excision from the right shoulder in 2006. She had no previous medical history of thrombosis.

Table 1. Timeline of key events.
The patient's oncological history is notable for two metachronous neoplasms. In July 2008, she was diagnosed with limited stage SCLC of the right lung with a 9.5 cm right anterior mediastinal lymph node mass, which compressed the superior cava vein, a 4.5 cm subpleural right lung mass, and enlarged subcarinal nodes. She underwent five cycles chemotherapy with cisplatin (80 mg/m2 IV infusion) and etoposide (100 mg/m2 IV infusion) every 3 weeks and concurrent radiotherapy 50.4 Gy in 30 sessions on the pulmonary mass and the affected lymph nodes. In January 2009 she received prophylactic cranial irradiation (PCI), 30 Gy in 10 sessions. She achieved a major partial response and was followed up until March 2020 with no evidence of progression, when she was discharged from oncology following an unremarkable FDG-PET scan.
In December 2023, she was diagnosed with stage IVA (cT2b cN1 cM1a) adenocarcinoma of the lung, characterized by a 5 cm necrotic mass in inferior right lobe (SuvMax 10.9), a small node located in lingula (SuvMax 4.5), and two right hilar adenopathies (SuvMax 6.6). The biopsy sample was negative for PD-L1 expression, and driver mutations. She started first-line treatment with carboplatin (AUC 5 IV infusion), pemetrexed (500 mg/m² IV infusion) and pembrolizumab (200 mg IV infusion) every 3 weeks. After four cycles, an FDG-PET scan in March 2024 showed a partial response, and maintenance therapy with pemetrexed (500 mg/m² IV infusion) and pembrolizumab (200 mg IV infusion) was initiated.
On June 5, 2024, during a routine follow-up visit, she was diagnosed with an asymptomatic ascending aorta arterial thrombus after completing four cycles of pemetrexed and pembrolizumab maintenance therapy. The thoraco-abdominal CT scan for her tumor evaluation, carried out on May 31, 2024, revealed a new hypodense nodular image adhered to the anterior wall of the ascending thoracic aorta, consistent with an 8 mm thrombus (Figures 1–3). The CT scan also noted chronic post-radiation changes in the right lung and a stable subpleural necrotic mass in the right lower lobe, with no evidence of new mediastinal adenopathy or pleural/pericardial effusion.

Figure 1. Transversal CT-scan plane showing the 8 mm thrombus in the ascending aorta.
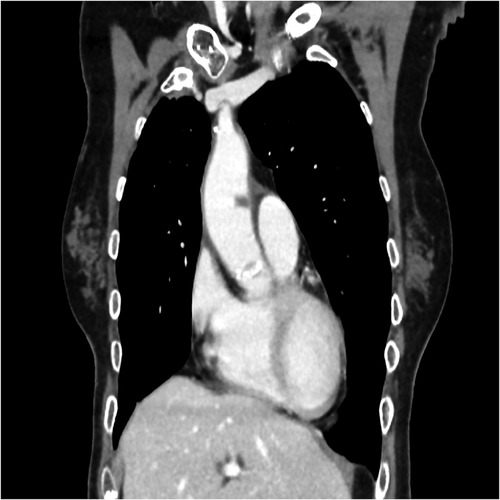
Figure 2. Coronal CT-scan plane showing the 8 mm thrombus in the ascending aorta.

Figure 3. Sagittal CT-scan plane showing the 8 mm thrombus in the ascending aorta.
As risk factors for the thrombus development, besides her oncology history, the patient had also been diagnosed 2 weeks before with a fracture of the sacrum. It was related to her osteoporosis and an accidental fall at home days before. Magnetic resonance performed on May 22, 2024, described a vertical and bilateral sacral ala fracture, with marrow edema, with no tumoral component. She was experiencing severe pain and was prescribed transdermal fentanyl.
Given the thrombus diagnosis, the oncology team suspended the patient's maintenance therapy and consulted the cardiology team, that evaluated the patient on the same day. Cardiology evaluation found no chest pain, signs of heart failure, syncope, palpitations, or neurological symptoms. An echocardiogram revealed a non-dilated and non-hypertrophic left ventricle with preserved ejection fraction and no segmental wall motion abnormalities. There was moderate bi-atrial dilation, a normal-sized aortic root (31 mm) and ascending aorta (36 mm) without alterations. A small nodule was visualized where the aortic thrombus was located in the CT. No pericardial effusion or intracavitary thrombus were seen. For therapeutic decision-making, we conducted a thorough review of the literature regarding ATE treatment in cancer patients. In most published case reports, asymptomatic ATE has been managed with LMWH. Therefore, we decided to start enoxaparin 1 mg/kg every 12 hours.
Two weeks later, on June 14, 2024, a follow-up CT scan of the chest to monitor the aortic thrombus showed its complete resolution (Figures 4–6). Due to the patient's preference to avoid twice-daily injections, her anticoagulation therapy was changed to bemiparin 115 IU/Kg every 24 hours and she resumed her treatment with pemetrexed and pembrolizumab. The patient reported no new symptoms and developed no complications related to the anticoagulation therapy. At the three-month follow-up, she remained asymptomatic.

Figure 4. Transversal CT-scan plane showing the resolution of the 8 mm thrombus in the ascending aorta.
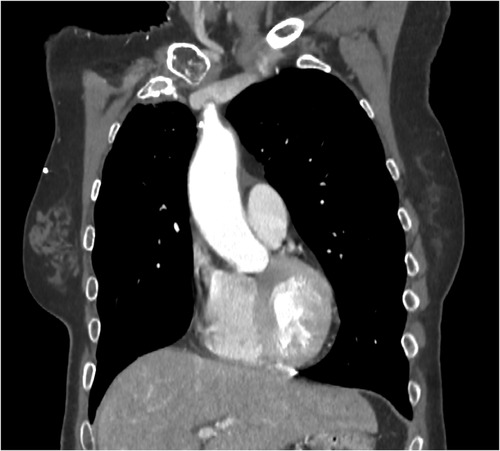
Figure 5. Coronal CT-scan plane showing the resolution of the 8 mm thrombus in the ascending aorta.

Figure 6. Sagittal CT-scan plane showing the resolution of the 8 mm thrombus in the ascending aorta.
Discussion
This case highlights the importance of vigilant cardiovascular monitoring in cancer patients, especially those undergoing active treatment, due to the heightened risk of thrombotic events. Early identification and prompt management of arterial thrombosis are critical in improving outcomes in this vulnerable population. Our patient was exposed to several well-known risk factors for thrombotic events, including her past SCLC, her current adenocarcinoma of the lung, the chemotherapy, thoracic radiotherapy and PCI in 2008, her current treatment with chemotherapy and immunotherapy, and her recent sacrum fracture. However, our patient did not exhibit the typical clinical presentation of VTE. Instead, she developed an ATE in the ascending aorta, which is particularly challenging to treat due to its critical location and associated compromise. The literature on managing ATEs is scarce, underscoring the need for individualised assessment and management in each case.
Cancer patients experience an increased risk of thromboembolic events due to a hypercoagulable state induced by the malignancy itself, as well as by the therapeutic interventions they undergo. It has been reported that the risk of VTE increases four- to six-fold in cancer patients receiving chemotherapy (5, 6), and especially in the case of ATE it can lead to catastrophic outcomes (7). Risk factors for ATE in the general population are severe atherosclerosis, aortic aneurysm, cardiovascular surgery, uncontrolled diabetes mellitus and polytrauma (8–10). Some ATE risk factors documented in cancer patients are: the first month after diagnosis of cancer, hypertension, smoking, pre-existing cardiovascular diseases, age over 65 years, previous history of ATE, distant metastasis and chemotherapy (11). While ATE in cancer patients is less common than VTE, both conditions share overlapping pathophysiological mechanisms (12). Recognized cancer-related mechanisms contributing to these complications include tumour cell-induced activation of coagulation pathways, a decrease in anticoagulant molecules, structural or functional changes in the vascular wall, endothelial damage, platelet activation, alterations in the fibrinolytic system, and the release of cytokines such as vascular endothelial growth factor (VEGF), tumour necrosis factor (TNF)-α, and interleukin-1β (13–18).
Antineoplastic agents, including hormone therapy, chemotherapy, and immunotherapy play an additional role, further exacerbating the risk by inducing endothelial injury and enhancing procoagulant activity (19, 20). Radiotherapy has also been suggested as a risk factor for VTE development. In a prospective study focused on curative intent radiotherapy, Daguenet et al. found an incidence rate of VTE 6 months post-radiotherapy of 2% (21).
Cisplatin and carboplatin are some of the frequently used chemotherapy drugs associated with ATE. It has been speculated that cisplatin may enhance tissue factor activity and platelet activation and elevate the von Willebrand factor, which can cause endothelial injury and potentiate arterial thrombosis. Dehydration and hypomagnesemia, are factors related to cisplatin treatment that might also contribute to thrombosis (22–25).
Some clinical cases specifically explore the relationship between cisplatin and ATE. Table 2 summarizes these cases. Chin et al. described the case of one patient with limited stage SCLC treated with cisplatin and etoposide, who was diagnosed with an aortic arch thrombus and its improvement when started on LMWH (26). Weijl et al. studied the incidence of thrombosis in 179 germ cell cancer patients treated with cisplatin and bleomycin, finding it to be approximately 8.4% (18). Of these events, three (16.7%) were arterial events, including two cerebral ischemic strokes and one lower limb arterial thrombosis. Numico et al. found in 108 stage III-IV NSCLC patients treated with cisplatin and gemcitabine chemotherapy a VTE incidence of approximately 17.6% (27). Of these events, ten were arterial events (2 myocardial infarctions, 7 lower limb arterial thrombosis, and 1 cerebral ischemic stroke). Dieckmann et al. reported the case of a man with advanced seminoma receiving cisplatin, etoposide and bleomycin chemotherapy who developed thrombotic deposits in the descending thoracic aorta and in the infrarenal abdominal aorta respectively. He was placed on anticoagulant therapy and 6 months after completion of chemotherapy, thrombotic deposits had completely resolved (28). Apiyasawat et al. reported the case of a patient that developed a thrombus in the distal arch of the aorta when she was receiving radiotherapy, cisplatin and 5-fluorouracil for stage IIB cervical cancer (29). Numerous vascular emboli were occluding her distal common femoral artery. The patient underwent successful surgical thrombectomy. Ito et al. described a patient suffering a thrombosis in the descending arch of the thoracic aorta and the infrarenal abdominal aorta during cisplatin-based chemotherapy for stage IV gastric cancer that was successfully treated with intravenous heparin and warfarin (30). Morlese et al. described a case of spontaneous arterial thrombosis in a 42-year-old male with localised oesophageal adenocarcinoma the day after receiving his first cycle of preoperative cisplatin-5-fluorouracil chemotherapy (31). It was identified a large thrombus in the abdominal aorta, beginning in the mid-aorta, just superior to the origin of the renal arteries, and continuing distally into both common iliac vessels. The patient received a surgical embolectomy and bilateral lower limb fasciotomies, but she finally died 7 days later due to small bowel infarction. Moore et al. performed a large retrospective analysis of all patients treated with cisplatin-based chemotherapy at Memorial Sloan-Kettering Cancer Center in 2008. Among 932 patients, 169 (18.1%) experienced a VTE and/or an ATE event during cancer treatment or within 4 weeks after finishing it. Most of them suffered VTE, but arterial thrombosis alone was found in 8.3% of these patients, and co-occurrence of ATE and VTE in 3.0% (32).
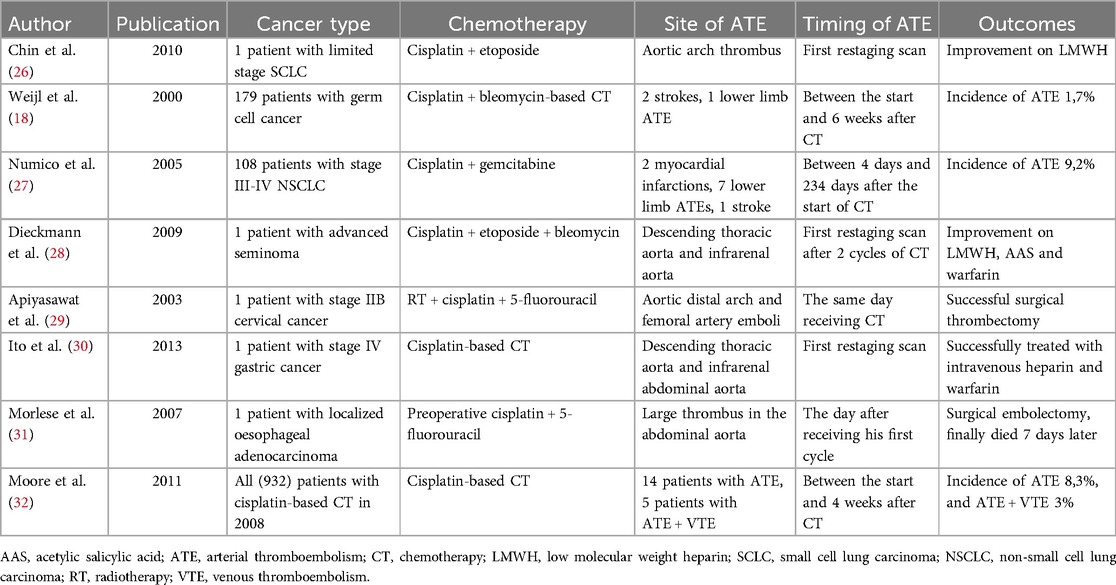
Table 2. Clinical cases exploring the relationship between cisplatin and arterial thromboembolism (ATE).
The patient we present in this case report has a history of thoracic radiotherapy for her previous SCLC, another notable risk factor for ATE development. A post-hoc analysis from the COMPASS-CAT trial, whose primary objective was to study a predictive model for VTE diagnosis in cancer, was focused on 361 patients with early, locally advanced, or metastatic breast, lung, colon, or ovarian cancer who received radiotherapy. At a median follow up of 6 months, 33 patients (9.1%) developed a VTE event. After applying a competing risk model, radiotherapy remained significantly associated with increased risk for VTE (HR 2.47, 95% CI: 1.47–4.12, p = 0.001) (33). Radiation injury has been demonstrated to cause acute and late alterations in the endothelium, favouring vascular events, as it has been studied in patients with central nervous system tumours presenting radionecrosis (34–36). Rishi et al. published the case of a 54-year-old male suffering extensive abdominal aortic thrombus along with involvement of left common iliac, saphenous-popliteal, and tibial arteries as well as moderate stenosis coronary arteries three days after receiving her first cycle of cisplatin-based chemotherapy given concurrently with radiotherapy for squamous cell carcinoma of the base of tongue (37).
Another risk factor for CAT development exhibited by the patient of our clinical case is her current exposure to pembrolizumab, as immune checkpoint inhibitors (ICI) have been associated with VTE and ATE risk in cancer patients (38–41). Moik et al. in the Vienna General Hospital conducted a retrospective study focused on patients treated with ICI. Melanoma, lung cancer and renal cancer were the most common types of cancer included. Nivolumab, pembrolizumab and ipilimumab were the most frequent ICI included. A total of 47.6% patients were also treated with radiation therapy. Cumulative incidences of VTE and ATE were 12.9% and 1.8% respectively (38). Based on the same hypothesis, Sussman et al. conducted a retrospective study of 228 patients with melanoma receiving ICI between 2015 and 2017 at the Cleveland Clinic. Fifty-one thrombotic events occurred in 47 patients (20.6%), including 37 VTE and 14 ATE (39). Roopkumar et al. conducted a retrospective cohort study including 1.686 patients who received ICI for a variety of malignancies to determine the incidence of VTE. VTE occurred in 404 patients (24%) and was associated with decreased overall survival [HR = 1.22 (95% CI 1.06–1.41), p < 0.008]. Patients developing VTE expressed significantly higher pretreatment levels of myeloid-derived suppressor cells, interleukin 8, and soluble vascular cell adhesion protein 1, postulated as drivers in VTE pathogenesis (40).
The information regarding the management of ATE in cancer patients is scarce and it should involve a multidisciplinary approach. Standard treatment modalities remain controversial. Systemic anticoagulation alone, aortic thromboendarterectomy, open-surgery for thrombus removal, or endovascular placement of stent grafts has been suggested (41–45). Goto et al. published the case of a 51-year-old woman with early esophageal cancer who presented an aortic mural thrombus. She was started on intravenous heparin and later changed to warfarin and three months later the thrombus had disappeared (46). Han et al. described a patient presenting ascending aortic thrombosis occurring 9 days after cisplatin-based chemotherapy for his lung cancer. He was successfully treated with LMWH and warfarin (47).
Conclusion
Although less frequent than VTE, ATE in cancer patients requires prompt recognition and management due to its severe potential consequences. This case describes an ascending aortic ATE in a cancer patient successfully treated with LMWH. Anticoagulation with LMWH resolved the thrombus, demonstrating its efficacy in managing CAT. LMWH for ATE in cancer patients may prevent further vascular complications, and allow for the continuation of the antineoplastic treatment. We hypothesize that if there are no life-threatening symptoms and no contraindications, based on the scarce available evidence, multidisciplinary evaluation, anticoagulation with LMWH alone and a close follow-up could be a good option for cancer-related ATE.
Data availability statement
The original contributions presented in the study are included in the article/Supplementary Material, further inquiries can be directed to the corresponding author.
Ethics statement
Written informed consent was obtained from the individual(s) for the publication of any potentially identifiable images or data included in this article.
Author contributions
MB: Conceptualization, Data curation, Formal Analysis, Funding acquisition, Investigation, Methodology, Project administration, Resources, Software, Supervision, Validation, Visualization, Writing – original draft, Writing – review & editing. MV: Conceptualization, Investigation, Writing – original draft. AF: Software, Supervision, Writing – review & editing. ÁM: Conceptualization, Data curation, Formal Analysis, Funding acquisition, Methodology, Resources, Validation, Writing – review & editing. CR: Conceptualization, Methodology, Project administration, Supervision, Writing – original draft. JB: Conceptualization, Data curation, Formal Analysis, Funding acquisition, Investigation, Methodology, Project administration, Resources, Software, Supervision, Validation, Visualization, Writing – original draft, Writing – review & editing.
Funding
The author(s) declare financial support was received for the research, authorship, and/or publication of this article. “Foundation for the Promotion of Health and Biomedical Research in the Valencian Region (FISABIO)” has funded this research.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Khorana AA, Mackman N, Falanga A, Pabinger I, Noble S, Ageno W, et al. Cancer-associated venous thromboembolism. Nat Rev Dis Primers. (2022) 8(1):11. doi: 10.1038/s41572-022-00336-y
2. Gervaso L, Dave H, Khorana AA. Venous and arterial thromboembolism in patients with cancer: JACC: CardioOncology state-of-the-art review. JACC CardioOncol. (2021) 3(2):173–90. doi: 10.1016/j.jaccao.2021.03.001
3. De Stefano V. Arterial thrombosis and cancer: the neglected side of the coin of Trousseau syndrome. Haematologica. (2018) 103(9):1419–21. doi: 10.3324/haematol.2018.197814
4. Zamorano JL, Lancellotti P, Muñoz DR, Aboyans V, Asteggiano R, Galderisi M, et al. 2016 ESC position paper on cancer treatments and cardiovascular toxicity developed under the auspices of the ESC committee for practice guidelines: the task force for cancer treatments and cardiovascular toxicity of the European Society of Cardiology (ESC). Eur Heart J. (2016) 37(36):2768–801. doi: 10.1093/eurheartj/ehw211
5. Khorana AA, Kuderer NM, Culakova E, Lyman GH, Francis CW. Development and validation of a predictive model for chemotherapy-associated thrombosis. Blood. (2008) 111:4902–7. doi: 10.1182/blood-2007-10-116327
6. Streiff MB, Holmstrom B, Angelini D, Ashrani A, Elshoury A, Fanikos J, et al. Cancer-associated venous thromboembolic disease, version 2.2021, NCCN clinical practice guidelines in oncology. J Natl Compr Canc Netw. (2021) 19(10):1181–201. doi: 10.6004/jnccn.2021.0047
7. Erbel R, Aboyans V, Boileau C, Bossone E, Di Bartolomeo R, Eggebrecht H, et al. ESC guidelines on the diagnosis and treatment of aortic diseases: document covering acute and chronic aortic diseases of the thoracic and abdominal aorta of the adult. The task force for the diagnosis and treatment of aortic diseases of the European Society of Cardiology. Eur Heart J. (2014) 35(41):2873–926. doi: 10.1093/eurheartj/ehu281
8. Cañadas V, Vilacosta I, Luaces M, Bustos A, Ferreirós J, Aragoncillo P, et al. Thrombosis of an apparently normal thoracic aorta and arterial embolism. Rev Esp Cardiol. (2008) 61:196–200. doi: 10.1157/13116207
9. Hahn TL, Dalsing MC, Sawchuk AP, Cikrit DF, Lalka SG. Primary aortic mural thrombus: presentation and treatment. Ann Vasc Surg. (1999) 13:52–9. doi: 10.1007/s100169900220
10. Vaideeswar P, Deshpande JR. Non-atherosclerotic aorto-arterial thrombosis: a study of 30 cases at autopsy. J Postgrad Med. (2001) 47:8–14.11590283
11. Pernod G, Cohen A, Mismetti P, Sanchez O, Mahé I; INNOVTE CAT Working Group. Cancer-related arterial thromboembolic events. Arch Cardiovasc Dis. (2024) 117(1):101–13. doi: 10.1016/j.acvd.2023.11.007
12. Aronson D, Brenner B. Arterial thrombosis and cancer. Thromb Res. (2018) 164(Suppl 1):S23–8. doi: 10.1016/j.thromres.2018.01.003
13. Lowe GDO. Common risk factors for both arterial and venous thrombosis. Br J Haematol. (2008) 140:488–95. doi: 10.1111/j.1365-2141.2007.06973.x
14. Alsamman M, Pothen J, Inoyatov M, Cruz Salcedo EM, Ramesh C. Aortic thrombus extending to left subclavian in a patient with diffuse venous thromboembolism on aromatase inhibitor therapy. Cureus. (2021) 13(7):e16698. doi: 10.7759/cureus.16698
15. Alcocer J, Ascaso M, Quintana E, Sandoval E, Castellá M. Operative management of ascending aorta thrombus and bilateral pulmonary embolism in the setting of breast cancer. J Card Surg. (2021) 36(4):1550–3. doi: 10.1111/jocs.15347
16. Previtali E, Bucciarelli P, Passamonti SM, Martinelli I. Risk factors for venous and arterial thrombosis. Blood Transfus. (2011) 9:120–38. doi: 10.2450/2010.0066-10
17. Haddad T, Greeno E. Chemotherapy-induced thrombosis. Thromb Res. (2006) 118:555–68. doi: 10.1016/j.thromres.2005.10.015
18. Weijl N, Rutten M, Zwinderman A, Keizer J, Nooy M, Rosendaal F, et al. Thromboembolic events during chemotherapy for germ cell cancer: a cohort study and review of the literature. J Clin Oncol. (2000) 18(10):2169–78. doi: 10.1200/JCO.2000.18.10.2169
19. Ay C, Pabinger I, Cohen AT. Cancer-associated venous thromboembolism: burden, mechanisms, and management. Thromb Haemost. (2017) 117(2):219–30. doi: 10.1160/TH16-08-0615
20. Wang TF, Khorana AA, Carrier M. Thrombotic complications associated with immune checkpoint inhibitors. Cancers (Basel). (2021) 13(18):4606. doi: 10.3390/cancers13184606
21. Daguenet E, Maison M, Tinquaut F, Giroux EA, Bertoletti L, Suchaud JP, et al. Venous thromboembolism and radiation therapy: the final radiation-induced thrombosis study analysis. Cancer Med. (2022) 11(8):1753–62. doi: 10.1002/cam4.4559
22. Mathews J, Goel R, Evans WK, Shamji F, Stewart DJ. Arterial occlusion in patients with peripheral vascular disease treated with platinum-based regimens for lung cancer. Cancer Chemother Pharmacol. (1997) 40:19–22. doi: 10.1007/s002800050619
23. Walsh J, Wheeler H, Geczy C. Modulation of tissue factor on human monocytes by cisplatin and adriamycin. Br J Haematol. (1992) 81(4):480–8. doi: 10.1111/j.1365-2141.1992.tb02978.x
24. Cool R, Herringon J, Wong L. Recurrent peripheral arterial thrombosis induced by cisplatin and etoposide. Pharmacotherapy. (2002) 22(9):1200–4. doi: 10.1592/phco.22.13.1200.33524
25. Licciarello J, Moake J, Rudi C, Karp D, Hong W. Elevated plasma von Willebrand factor levels and arterial occlusive complications associated with cisplatin-based chemotherapy. Oncology. (1985) 42:296–300. doi: 10.1159/000226049
26. Chin SO, Lee JJ, Hwang YH, Han JJ, Maeng CH, Baek SK, et al. Aortic thrombosis resolved with enoxaparin in a patient treated with cisplatin-based regimen for small cell lung cancer. Int J Hematol. (2010) 91(5):892–6. doi: 10.1007/s12185-010-0571-3
27. Numico G, Garrone O, Dongiovanni V, Silvestris N, Colantonio I, Di Costanzo G, et al. Prospective evaluation of major vascular events in patients with nonsmall cell lung carcinoma treated with cisplatin and gemcitabine. Cancer. (2005) 103(5):994–9. doi: 10.1002/cncr.20893
28. Dieckmann KP, Gehrckens R. Thrombosis of abdominal aorta during cisplatin-based chemotherapy of testicular seminoma—a case report. BMC Cancer. (2009) 9:459. doi: 10.1186/1471-2407-9-459
29. Apiyasawat S, Wongpraparut N, Jacobson L, Berkowitz H, Jacobs LE, Kotler MN. Cisplatin induced localized aortic thrombus. Echocardiography. (2003) 20(2):199–200. doi: 10.1046/j.1540-8175.2003.03002.x
30. Ito S, Nakamura Y, Noumi T, Sasaki Y. Acute aortic thrombosis during cisplatin based chemotherapy for gastric cancer. Intern Med. (2013) 52(9):973–5. doi: 10.2169/internalmedicine.52.9337
31. Morlese JF, Jeswani T, Beal I, Wylie P, Bell J. Acute ventricular and aortic thrombosis post chemotherapy. Br J Radiol. (2007) 80(952):e75–7. doi: 10.1259/bjr/26948582
32. Moore RA, Adel N, Riedel E, Bhutani M, Feldman DR, Tabbara NE, et al. High incidence of thromboembolic events in patients treated with cisplatin-based chemotherapy: a large retrospective analysis. J Clin Oncol. (2011) 29(25):3466–73. doi: 10.1200/JCO.2011.35.5669
33. Temraz S, Moukalled N, Gerotziafas GT, Elalamy I, Jara-Palomares L, Charafeddine M, et al. Association between radiotherapy and risk of cancer associated venous thromboembolism: a sub-analysis of the COMPASS-CAT study. Cancers (Basel). (2021) 13(5):1033. doi: 10.3390/cancers13051033
34. Yoshii Y. Pathological review of late cerebral radionecrosis. Brain Tumor Pathol. (2008) 25(2):51–8. doi: 10.1007/s10014-008-0233-9
35. Gonzalez J, Kumar AJ, Conrad CA, Levin VA. Effect of bevacizumab on radiation necrosis of the brain. Int J Radiat Oncol Biol Phys. (2007) 67(2):323–6. doi: 10.1016/j.ijrobp.2006.10.010
36. Levin VA, Bidaut L, Hou P, Kumar AJ, Wefel JS, Bekele BN, et al. Randomized double-blind placebo-controlled trial of bevacizumab therapy for radiation necrosis of the central nervous system. Int J Radiat Oncol Biol Phys. (2011) 79(5):1487–95. doi: 10.1016/j.ijrobp.2009.12.061
37. Rishi A, Ghoshal S. Acute multiple arterial thrombosis after cisplatin in base of tongue carcinoma: case report. Head Neck. (2013) 35(9):E269–71. doi: 10.1002/hed.23123
38. Moik F, Chan WSE, Wiedemann S, Hoeller C, Tuchmann F, Aretin MB, et al. Incidence, risk factors, and outcomes of venous and arterial thromboembolism in immune checkpoint inhibitor therapy. Blood. (2021) 137(12):1669–78. doi: 10.1182/blood.2020007878
39. Sussman TA, Li H, Hobbs B, Funchain P, McCrae KR, Khorana AA. Incidence of thromboembolism in patients with melanoma on immune checkpoint inhibitor therapy and its adverse association with survival. J Immunother Cancer. (2021) 9(1):e001719. doi: 10.1136/jitc-2020-001719
40. Roopkumar J, Swaidani S, Kim AS, Thapa B, Gervaso L, Hobbs BP, et al. Increased incidence of venous thromboembolism with cancer immunotherapy. Med. (2021) 2(4):423–34. doi: 10.1016/j.medj.2021.02.002
41. Toyama M, Nakayama M, Hasegawa M, Yuasa T, Sato B, Ohno O. Direct oral anticoagulant therapy as an alternative to surgery for the treatment of a patient with a floating thrombus in the ascending aorta and pulmonary embolism. J Vasc Surg Cases Innov Tech. (2018) 4(2):170–2. doi: 10.1016/j.jvscit.2018.03.002
42. Choukroun EM, Labrousse LM, Madonna FP, Deville C. Mobile thrombus of the thoracic aorta: diagnosis and treatment in 9 cases. Ann Vasc Surg. (2002) 16:714–22. doi: 10.1007/s10016-001-0314-2
43. Zhang WW, Abou-Zamzam AM, Hashisho M, Killeen JD, Bianchi C, Teruya TH. Staged endovascular stent grafts for concurrent mobile/ulcerated thrombi of thoracic and abdominal aorta causing recurrent spontaneous distal embolization. J Vasc Surg. (2008) 47:193–6 doi: 10.1016/j.jvs.2007.07.050
44. Tsilimparis N, Hanack U, Pisimisis G, Yousefi S, Wintzer C, Rückert RI. Thrombus in the non-aneurysmal, non-atherosclerotic descending thoracic aorta—an unusual source of arterial embolism. Eur J Vasc Endovasc Surg. (2011) 41:450–7. doi: 10.1016/j.ejvs.2010.11.004
45. Shames ML, Rubin BG, Sanchez LA, Thompson RW, Sicard GA. Treatment of embolizing arterial lesions with endoluminally placed stent grafts. Ann Vasc Surg. (2002) 16:608–12. doi: 10.1007/s10016-001-0278-2
46. Goto I, Okamoto R, Sawai T, Takasaki A, Takeuchi T, Matsuo H, et al. A case of aortic thrombosis and embolism preceding the progression of early esophageal cancer. J Cardiol Cases. (2013) 7(5):e123–5. doi: 10.1016/j.jccase.2012.12.008
Keywords: cancer-associated thrombosis (CAT), venous thromboembolism (VTE), arterial thromboembolism (ATE), low molecular weight heparin (LMWH), small cell lung carcinoma (SCLC) and cisplatin
Citation: Borregón M, Valero M, Ferrández A, Muñoz Á, Roque C and Benítez-Fuentes J-D (2025) Cancer-associated thoracic aorta arterial thrombosis: case report and review of the literature. Front. Cardiovasc. Med. 12:1480310. doi: 10.3389/fcvm.2025.1480310
Received: 13 August 2024; Accepted: 7 January 2025;
Published: 29 January 2025.
Edited by:
Reto Asmis, Wake Forest University, United StatesReviewed by:
Omer Iqbal, Loyola University Chicago, United StatesKirtipal Bhatia, Mount Sinai Morningside, United States
Copyright: © 2025 Borregón, Valero, Ferrández, Muñoz, Roque and Benítez-Fuentes. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Miguel Borregón, bWlndWVsYm9ycmVnb25yaXZpbGxhQGdtYWlsLmNvbQ==