 Yuping Xiang
Yuping Xiang Tianhui Luo†
Tianhui Luo†
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Cardiovasc. Med., 07 April 2025
Sec. Cardiovascular Surgery
Volume 12 - 2025 | https://doi.org/10.3389/fcvm.2025.1479922
Background: There is a high incidence of postoperative hyperglycemia (PHG) in cardiac surgery with cardiopulmonary bypass (CPB), as well as increased morbidity and mortality. The purpose of this study was to evaluate the incidence of PHG after cardiac surgery with CPB, the independent risk factors, and its association with clinical outcomes.
Methods: This was a retrospective, observational study of patients who underwent cardiac surgery with CPB between January 2023 and March 2024 in West China Hospital of Sichuan University. A total of 1,008 consecutive postoperative cardiac surgery patients admitted to the cardiac surgery intensive care unit (ICU) were divided into a non-PHG group and a PHG group. Patients’ blood glucose levels were evaluated immediately after cardiac surgery and every 3–4 h daily for 10days, until discharge from the ICU. For patients with PHG, intravenous insulin infusion was performed according to the institution's protocol, and perioperative risk factors for hyperglycemia and clinical outcomes were assessed.
Results: PHG, defined as random blood glucose ≥10.0 mmol/L (180 mg/dl) on two occasions within 24 h, occurred in 65.28% of cardiac surgery patients. Multivariable logistic regression analysis identified that age [odds ratio (OR) 1.054, 95% confidence interval (CI) 1.040–1.069; p < 0.001], female sex (OR 1.380, 95% CI 1.023–1.864; p = 0.035), diabetes (OR 13.101, 95% CI 4.057–42.310; p < 0.001), pulmonary infection (OR 1.918, 95% CI 1.129–3.258; p = 0.016), aortic cross-clamp time (OR 1.007, 95% CI 1.003–1.010; p < 0.001), and intraoperative highest glucose (OR 1.515, 95% CI 1.370–1.675; p < 0.001) emerged as independent risk factors for PHG. Moreover, PHG had higher rates of acute kidney injury (12.61% vs. 4.00%; p < 0.001), delirium (9.57% vs. 3.43%; p < 0.001), pulmonary infection (12.01% vs. 5.14%; p < 0.001), longer duration of mechanical ventilation (19 vs. 14 h; p < 0.001), length of ICU stay (74 vs. 58 h; p < 0.001), length of hospitalization (13 vs. 11 days; p < 0.001), and higher rate of self-discharge or death (3.95% vs. 0.57%; p = 0.002) compared with patients with non-PHG.
Conclusions: PHG occurs frequently in patients after cardiac surgery. Age, female, diabetes, pulmonary infection, aortic cross-clamp time, and intraoperative highest glucose were independent risk factors for PHG. PHG is associated with worse clinical outcomes, including a higher rate of acute kidney injury, delirium, and pulmonary infection, greater duration of mechanical ventilation, length of ICU stay, length of hospitalization, and higher rate of automatic discharge or death.
Cardiac surgery with cardiopulmonary bypass (CPB) is a primary treatment for heart valve disease or coronary artery disease. Globally, approximately 2 million cardiac surgeries using CPB are performed annually (1). In China in 2022, 263,292 cardiac surgeries were conducted, with 159,949 involving CPB (2). During CPB, patients are susceptible to postoperative hyperglycemia (PHG) because of general inflammatory reactions, surgical stressors, hypothermia, catecholamine release, increased catabolism, and the use of corticosteroids or positive inotropic drugs, regardless of preoperative diabetes status (3–5). Hyperglycemia can contribute to endothelial dysfunction, glucose metabolism dysfunction, oxidative stress, inflammation, and mitochondrial dysfunction (6–8).
PHG is defined as blood glucose levels >140 mg/dl (7.8 mmol/L). Its incidence in cardiac surgery is in the range of 60%–80%, with approximately 60% of PHG patients being diagnosed with diabetes mellitus within 1 year of follow up (9). Previous studies have examined the impact of preoperative or intraoperative hyperglycemia on adverse outcomes, such as an increased risk of postoperative infections (10), cognitive dysfunction (11), acute kidney injury (AKI) (12, 13), end-organ dysfunction (14), and death (15).
Several studies have examined the risk factors and outcomes associated with PHG (16–18). Independent risk factors for PHG include higher body mass index (BMI), advanced age, aortic cross-clamp duration, blood transfusion, diabetes, high Euro-SCORE II, and preoperative leukocytosis. Hyperglycemia is also linked to worse clinical outcomes, including a higher incidence of AKI, arrhythmias, intensive care unit (ICU)-acquired weakness, prolonged mechanical ventilation, extended ICU stays, and increased rates of multiorgan failure. In addition, Gillinov et al. (19) reported that non-diabetic cardiac surgery patients with PHG incurred significantly higher hospital costs than those without PHG ($38,642 vs. $28,987). Therefore, postoperative hyperglycemia has become a hot topic in cardiac surgery. Our hospital is the largest cardiac surgery center in southwest China. The aim of the present study was to evaluate postoperative blood glucose levels, risk factors for hyperglycemia, and their association with clinical outcomes in patients undergoing cardiac surgery with CPB.
This retrospective, observational clinical study included consecutive patients who underwent cardiac surgery with cardiopulmonary bypass at West China Hospital of Sichuan University between January 2023 and March 2024. The study was conducted in accordance with the “Declaration of Helsinki” and was approved by the ethics committee of West China Hospital of Sichuan University (reference number: 2024 Annual Audit 848). Due to the observational and retrospective nature of this study, the requirement for written informed consent was waived.
The study included 1,008 consecutive patients who were admitted to the intensive care unit after cardiac surgery during this period. The exclusion criteria were as follows: pregnancy, death during surgery, age <18 years, missing data exceeding 20%, and corticosteroid use. Patients were categorized according to their blood glucose levels: those with blood glucose ≥10.0 mmol/L (n = 658) and those with blood glucose <10.0 mmol/L (n = 350) for group comparison.
Patients’ clinical data were collected from the electronic medical records system of West China Hospital. Preoperative variables included demographic factors (age, sex, BMI, smoking and drinking history, level of education, marital status), clinical conditions [hypertension, diabetes mellitus, coronary heart disease, stroke, chronic kidney disease, chronic lung disease, pulmonary infection, and history of cardiovascular surgery, New York Heart Association (NYHA) ≥ 3], and laboratory tests [hemoglobin, white blood cell count, neutrophil count, lymphocyte count, red blood cell count, platelet count, hemoglobin, neutrophil percentages, albumin, blood glucose, creatinine, glomerular filtration rate, triglyceride, cholesterol, high-density lipoprotein (HDL), low-density lipoprotein (LDL), left ventricle (LV), and left ventricular ejection fraction (LVEF)]. Operative variables included operation time, CPB time, aortic cross-clamp time, intraoperative highest glucose and lactate levels, and urgency and type of surgery. Postoperative variables included postoperative hyperglycemia, acute kidney injury, delirium, pulmonary infection, duration of mechanical ventilation, ICU and hospital length of stay, self-discharge or death, and 30-day readmission.
Postoperative hyperglycemia is defined as a random blood glucose level ≥10 mmol/L on two occasions within 24 h (20, 21). Blood glucose monitoring was performed immediately postoperatively and then every 3–4 h daily up to 10 days or until discharge from the ICU. Blood glucose levels were measured using arterial blood gas analysis and capillary blood glucose monitoring. At our center, when postoperative random blood glucose reaches ≥11.1 mmol/L on two or more occasions, the electronic medical record system issues an alert, prompting nurses to administer intravenous insulin and adjust the dose accordingly. Insulin infusion was discontinued when blood glucose levels dropped below 11.1 mmol/L. AKI was defined according to the Kidney Disease Improving Global Outcomes (KDIGO) (22): (1) an increase in serum creatinine (SCr) by 0.3 mg/dl within 48 h or (2) an increase in SCr by 1.5 times the baseline value within 7 days, or initiation of renal replacement therapy. Serum creatinine levels were measured preoperatively and monitored for 10 days postoperatively. Delirium was assessed daily using the confusion assessment method for the ICU (CAM-ICU) (23). A patient was considered to have developed delirium if they tested positive on the CAM-ICU assessment, which ICU was conducted by ICU nurses six times per day until ICU discharge. Pulmonary infection was recorded in the electronic medical record by the doctor, with diagnoses based on imaging (chest X-ray and CT scans) and examination indicators (e.g., white blood cells).
Statistical analyses were conducted using SPSS version 22.0 (IBM Corp., Armonk, NY, USA). Continuous variables with a normal distribution are presented as mean ± SD, while those with a non-normal distribution are expressed as median (25th–75th percentiles). The Shapiro–Wilk test was used to assess the normal distribution of values. Categorical variables are reported as absolute values and relative frequencies. Univariate logistic regression analysis was performed on all variables to evaluate risk factors for hyperglycemia.
A multivariate logistic regression analysis model (enter method) was also performed to identify independent predictors of hyperglycemia for those variables with statistical significance in the univariate analysis (p < 0.05) and to compare clinical outcomes between the PHG and non-PHG groups. A p-value of <0.05 was considered statistically significant.
There were 1,013 patients who underwent cardiac surgery with cardiopulmonary bypass at West China Hospital of Sichuan University between January 2023 and March 2024. Among them, five patients were excluded: one patient was aged <18 years, two patients died within 24 h after surgery, and two patients had missing data. Finally, 1,008 patients were included in this study.
Preoperative and operative variables of these patients are shown in Tables 1 and 2. Of the 1,008 patients, 658 had PHG according to the definition above. The mean age of patients in the non-PHG and PHG groups was 53 and 59 years, respectively. In the non-PHG group, 55.71% of patients were male, compared to 49.24% in the PHG group. The prevalence of diabetes was significantly higher in the PHG group than in the non-PHG group (16.26% vs. 0.86%; p < 0.001).
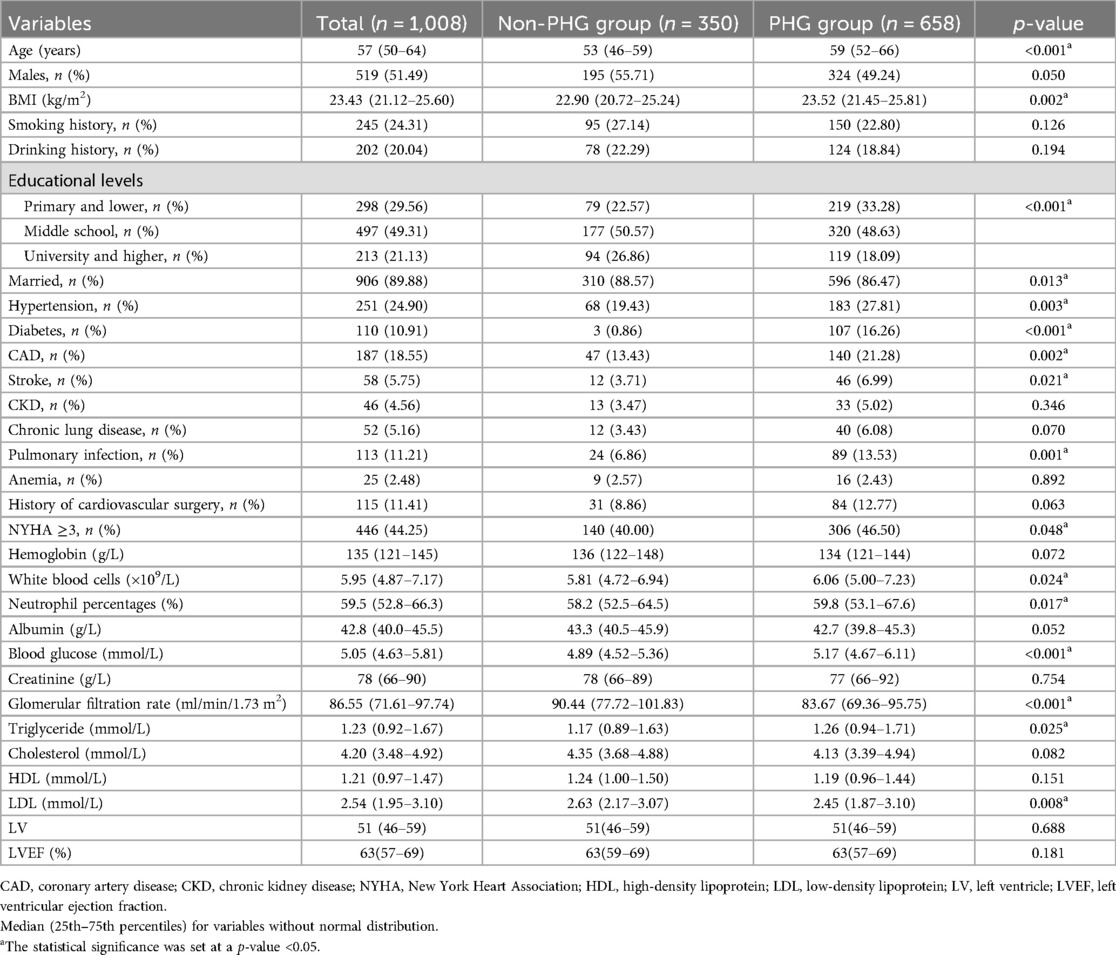
Table 1. Preoperative and operative variables of patients in different groups.
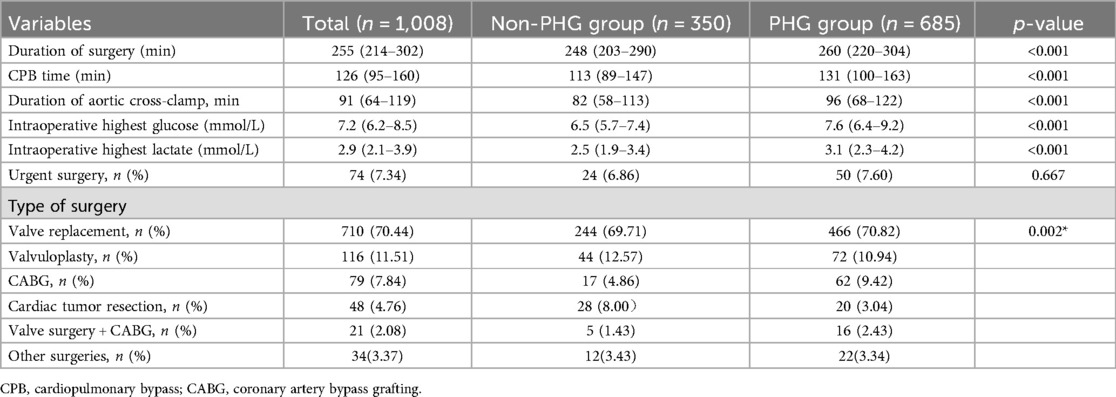
Table 2. Operative variables of patients in different groups.
We observed that the mean BMI of patients in the PHG group was significantly higher than that of patients in the non-PHG group (23.52 vs. 22.90; p = 0.002). The proportion of patients with a primary or lower education level was significantly higher in the PHG group (33.28% vs. 22.57%; p < 0.001). There was also a significant difference in preoperative blood glucose levels between the two groups.
Regarding operative variables, operation time, CPB time, aortic cross-clamp time, and intraoperative highest glucose and lactate levels showed significant differences between groups. During ICU hospitalization, 65.28% of patients had glucose levels ≥10.0 mmol/L. In addition, the mean daily highest blood glucose levels during the ICU period are illustrated in Figure 1.
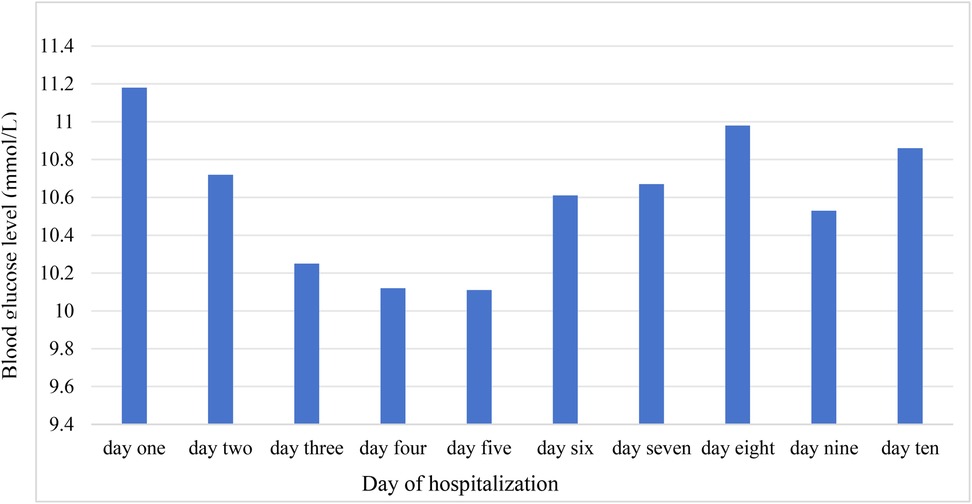
Figure 1. The trend of highest mean blood glucose during the ICU period.
In multivariable analysis (Table 3), it was determined that age [odds ratio (OR) 1.054, 95% confidence interval (CI) 1.040–1.069; p < 0.001], female sex (OR 1.380, 95% CI 1.023–1.864; p = 0.035), diabetes (OR 13.101, 95% CI 4.057–42.310; p < 0.001), pulmonary infection (OR 1.918, 95% CI 1.129–3.258; p = 0.016), aortic cross-clamp time (OR 1.007, 95% CI 1.003–1.010; p < 0.001), and intraoperative highest glucose level (OR 1.515, 95% CI 1.370–1.675; p < 0.001) were independent risk factors for PHG. We also analyzed the impact of PHG on clinical outcomes in cardiac surgery patients. The results suggest that patients in the PHG group experienced significantly worse postoperative outcomes compared to those in the non-PHG group: AKI = 12.61% vs. 4.00% (p < 0.001), delirium = 9.57% vs. 3.43% (p < 0.001), pulmonary infection = 12.01% vs. 5.14% (p < 0.001), and self-discharge or death = 3.95% vs. 0.57% (p = 0.002). Postoperative ventilation time (19 vs. 14 h; p < 0.001), length of ICU stay (74 vs. 58 h; p < 0.001), and length of hospitalization (13 vs. 11 days; p < 0.001) for patients in the PHG group were significantly longer than those of patients in the non-PHG group (Table 4).
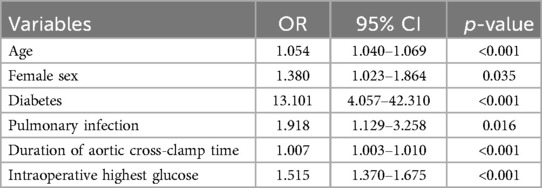
Table 3. Multivariable analysis of PHG.
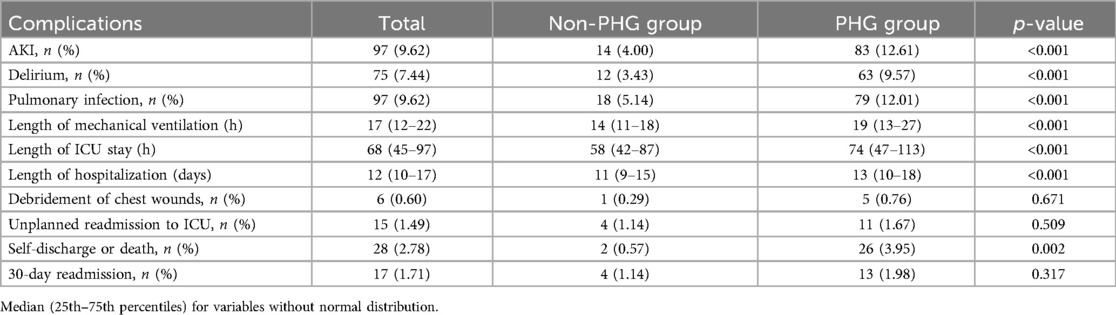
Table 4. Postoperative complications in different groups.
CPB is a standard procedure in cardiac surgery; however, it may trigger several biochemical changes in the microcirculation, leading to a systemic inflammatory response (24). This results from factors such as blood contact with the CPB device's surface, surgical trauma, endotoxemia, blood loss, and ischemic reperfusion injury (25). Systemic inflammation has recently been associated with hyperglycemia and insulin resistance in the adult diabetic population. A recent study reported that inflammation induced by CPB may contribute to insulin resistance, leading to postoperative hyperglycemia (26). In addition, other factors, such as planned hypothermia during surgery, surgical stress, the use of glucocorticoids, and positive inotropes, may disrupt glucose metabolism (27). Therefore, hyperglycemia occurs frequently in patients undergoing cardiac surgery, regardless of their history of diabetes mellitus. It has also been associated with an increased risk of postoperative complications, morbidity, and mortality (18).
This study found that the incidence of hyperglycemia (≥10.0 mmol/L) in cardiac surgery patients was 65.28%. Independent risk factors for PHG included age, female sex, diabetes, pulmonary infection, aortic cross-clamp time, and intraoperative highest glucose levels. Kourek et al. (17) reported that PHG (≥10 mmol/L) occurred in 30% of cardiac surgery patients, with diabetes, high Euro-SCORE II, and preoperative leukocytosis as independent risk factors. Moorthy et al. (16) identified higher BMI, age, aortic cross-clamp time, and blood transfusion as independent risk factors of PHG after cardiac surgery in non-diabetic patients. Chen et al. (18) reported that 42.36% of adult patients undergoing type A aortic dissection developed PHG, with neutrophil count, platelet count, lactic acid levels, weight, and lymphocyte count as predictors. Compared with previous studies (16–18), the incidence of hyperglycemia in our center was significantly higher. A possible explanation is that patients undergoing cardiac surgery at our hospital are started on an intravenous insulin infusion when their blood glucose reaches ≥11.1 mmol/L. Consistent with previous studies, age (16, 28) and female sex (28) were identified as risk factors for PHG, and Kourek et al. (17) demonstrated a sex-related association with PHG levels.
Our study’s novel and most significant finding is that preoperative pulmonary infection and maximum intraoperative glucose are independent risk factors for PHG in patients undergoing cardiac surgery with CPB. The mechanism linking PHG to preoperative pulmonary infection remains unclear. The physiological stress induced by pulmonary infection can lead to metabolic disorders, including altered hepatic glucose metabolism, increased peripheral insulin resistance, and hyperglycemia (29). In patients with pneumonia, elevated C-reactive protein (CRP) have been positively associated with insulin resistance (30). Salonen et al. (31) demonstrated that advanced age, high gHbA1c, elevated CRP, and high blood leukocyte levels are risk factors for hyperglycemia in patients with pneumonia, with inflammation markedly enhancing insulin resistance. Therefore, reducing preoperative pulmonary infections in cardiac surgery patients could reduce the incidence of PHG.
Our study also found that intraoperative blood glucose levels were significantly higher in the PHG group than in the non-PHG group and that the highest intraoperative blood glucose was a risk factor for PHG. In their study, Nair et al. (32) reported that intraoperative hyperglycemia increases the odds for PHG, and Yamamoto et al. (33) found that intraoperative hyperglycemia, longer CPB time, younger age, and chromosomal abnormalities were risk factors for severe PHG (blood glucose ≥250 mg/dl) in pediatric cardiac surgery patients. Intraoperative hyperglycemia increases the risk of acute kidney injury (34), delirium (35), infection (10), and 30-day mortality (36) in patients undergoing cardiac surgery. Currently, there is no definitive consensus on the optimal perioperative blood glucose range for cardiac surgery patients. Current guidelines recommend maintaining blood glucose below 180 mg/dl (10 mmol/L) during CPB (37). In addition, aortic cross-clamp time was associated with PHG, consistent with the research by Moorthy et al. (16). Longer aortic cross-clamp times may increase inflammatory mediators (e.g., IL-6, IL-8, and IL-10), which can predispose patients to hyperglycemia (38).
In this study, patients who experienced PHG had higher rates of kidney injury, delirium, and pulmonary infection, as well as longer durations of mechanical ventilation, ICU stay, hospitalization, and a higher rate of self-discharge or death. Although many studies have examined perioperative blood glucose management in cardiac surgery patients, fewer have focused on PHG. Kourek et al. (17), Moorthy et al. (16), and Chen et al. (18) identified PHG as a strong predictor of AKI, multiorgan failure, hepatic dysfunction, cardiac arrhythmias, and mortality, regardless of diabetes status. Although guidelines recommend keeping postoperative blood glucose below 10 mmol/L (20), a study (39) found that among insulin-treated diabetic patients, maintaining glucose levels in the range of 180–240 mg/dl was associated with cost reductions of $6,225 per patient, a 1.6-day reduction in length of hospital stay, a 4.1% reduction in infections, and a 12.5% reduction in respiratory complications. Therefore, optimal postoperative glycemic management should be further explored in post-cardiac surgery patients.
There are several limitations to this study. First, this is a single-center retrospective study. Second, some studies defined PHG as blood glucose ≥10 mmol/L (16–18), while others define it as blood glucose ≥11.1 mmol/L (40, 41). Even though we used relaxed blood glucose control criteria, our center still followed guideline recommendations (20, 21) and defined hyperglycemia as ≥10.0 mmol/L. Third, patients with diabetes mellitus were not excluded and postoperative insulin use not considered. Finally, unfortunately, variables such as Hba1C and EUROSCORE were not included in our study due to missing values.
Age, female sex, diabetes, pulmonary infection, aortic cross-clamp time, and intraoperative highest glucose are independent risk factors for PHG. PHG was also significantly associated with the occurrence of AKI, delirium, pulmonary infection, automatic discharge or death, increased ventilation time, and longer ICU and hospital stays. Our study highlights that cardiac surgeons, anesthesiologists, intensive care physicians, and nurses should pay attention to perioperative hyperglycemia and develop prevention and management strategies.
The original contributions presented in the study are included in the article/Supplementary Material, further inquiries can be directed to the corresponding author.
The studies involving humans were approved by West China Hospital of Sichuan University. The studies were conducted in accordance with the local legislation and institutional requirements. The ethics committee/institutional review board waived the requirement for written informed consent for participation from the participants or the participants’ legal guardians/next of kin because it was a retrospective case-control study.
YX: Conceptualization, Methodology, Writing – original draft, Writing – review & editing. TL: Formal Analysis, Methodology, Software, Writing – review & editing. LZ: Writing – review & editing, Project administration, Supervision.
The author(s) declare that no financial support was received for the research and/or publication of this article.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Tsao CW, Aday AW, Almarzooq ZI, Alonso A, Beaton AZ, Bittencourt MS, et al. Heart disease and stroke statistics-2022 update: a report from the American Heart Association. Circulation. (2022) 145:e153–639. doi: 10.1161/CIR.0000000000001052
2. Hao X. White book of Chinese cardiovascular surgery and extracorporeal circulation in 2022. ChinJECC. (2023) 21:197–200. doi: 10.13498/j.cnki.chin.j.ecc.2023.04.2
3. Tsai LL, Jensen HA, Thourani VH. Intensive glycemic control in cardiac surgery. Curr Diab Rep. (2016) 16:25. doi: 10.1007/s11892-016-0719-5
4. Girish G, Agarwal S, Satsangi DK, Tempe D, Dutta N, Pratap H. Glycemic control in cardiac surgery: rationale and current evidence. Ann Card Anaesth. (2014) 17:222–8. doi: 10.4103/0971-9784.135873
5. Punke MA, Goepfert MS, Kluge S, Reichenspurner H, Goetz AE, Reuter DA. Perioperative glycemic control with a computerized algorithm versus conventional glycemic control in cardiac surgical patients undergoing cardiopulmonary bypass with blood cardioplegia. J Cardiothorac Vasc Anesth. (2014) 28:1273–7. doi: 10.1053/j.jvca.2014.04.017
6. Dungan KM, Braithwaite SS, Preiser JC. Stress hyperglycaemia. Lancet. (2009) 373:1798–807. doi: 10.1016/S0140-6736(09)60553-5
7. Vanhorebeek I, Ellger B, De Vos R, Boussemaere M, Debaveye Y, Perre SV, et al. Tissue-specific glucose toxicity induces mitochondrial damage in a burn injury model of critical illness. Crit Care Med. (2009) 37:1355–64. doi: 10.1097/CCM.0b013e31819cec17
8. Langouche L, Vanhorebeek I, Vlasselaers D, Vander PS, Wouters PJ, Skogstrand K, et al. Intensive insulin therapy protects the endothelium of critically ill patients. J Clin Invest. (2005) 115:2277–86. doi: 10.1172/JCI25385
9. Galindo RJ, Fayfman M, Umpierrez GE. Perioperative management of hyperglycemia and diabetes in cardiac surgery patients. Endocrinol Metab Clin North Am. (2018) 47:203–22. doi: 10.1016/j.ecl.2017.10.005
10. Xiong X, Chen D, Cai S, Qiu L, Shi J. Association of intraoperative hyperglycemia with postoperative composite infection after cardiac surgery with cardiopulmonary bypass: a retrospective cohort study. Front Cardiovasc Med. (2022) 9:1060283. doi: 10.3389/fcvm.2022.1060283
11. Zhang X, Yan X, Gorman J, Hoffman SN, Zhang L, Boscarino JA. Perioperative hyperglycemia is associated with postoperative neurocognitive disorders after cardiac surgery. Neuropsychiatr Dis Treat. (2014) 10:361–70. doi: 10.2147/NDT.S57761
12. Oezkur M, Wagner M, Weismann D, Krannich JH, Schimmer C, Riegler C, et al. Chronic hyperglycemia is associated with acute kidney injury in patients undergoing CABG surgery–a cohort study. BMC Cardiovasc Disord. (2015) 15:41. doi: 10.1186/s12872-015-0028-y
13. Mendez CE, Der Mesropian PJ, Mathew RO, Slawski B. Hyperglycemia and acute kidney injury during the perioperative period. Curr Diab Rep. (2016) 16:10. doi: 10.1007/s11892-015-0701-7
14. Matsumoto S, Omiya H, Fujinaka W, Morimatsu H. Association between intraoperative hyperglycemia and postoperative end-organ dysfunctions after cardiac surgery: a retrospective observational study. J Anesth. (2022) 36:174–84. doi: 10.1007/s00540-021-03024-5
15. Doenst T, Wijeysundera D, Karkouti K, Zechner C, Maganti M, Rao V, et al. Hyperglycemia during cardiopulmonary bypass is an independent risk factor for mortality in patients undergoing cardiac surgery. J Thorac Cardiovasc Surg. (2005) 130:1144. doi: 10.1016/j.jtcvs.2005.05.049
16. Moorthy V, Sim MA, Liu W, Chew STH, Ti LK. Risk factors and impact of postoperative hyperglycemia in nondiabetic patients after cardiac surgery: a prospective study. Medicine (Baltimore). (2019) 98:e15911. doi: 10.1097/MD.0000000000015911
17. Kourek C, Georgopoulou M, Kolovou K, Rouvali N, Panoutsopoulou M, Kinti C, et al. Intensive care unit hyperglycemia after cardiac surgery: risk factors and clinical outcomes. J Cardiothorac Vasc Anesth. (2024) 38:162–9. doi: 10.1053/j.jvca.2023.09.022
18. Chen Y, Ouyang T, Yin Y, Fang C, Tang CE, Luo F, et al. The prognosis of patients with postoperative hyperglycemia after Stanford type A aortic dissection surgery and construction of prediction model for postoperative hyperglycemia. Front Endocrinol (Lausanne). (2023) 14:1063496. doi: 10.3389/fendo.2023.1063496
19. Gillinov AM, Shi W, Rosen A, O'Gara P, Welsh S, Bagiella E, et al. Costs of postoperative hyperglycemia in cardiac surgery patients. J Am Coll Cardiol. (2014) 63:A1860. doi: 10.1016/S0735-1097(14)61863-5
20. Lazar HL, McDonnell M, Chipkin SR, Furnary AP, Engelman RM, Sadhu AR, et al. The society of thoracic surgeons practice guideline series: blood glucose management during adult cardiac surgery. Ann Thorac Surg. (2009) 87:663–9. doi: 10.1016/j.athoracsur.2008.11.011
21. Honarmand K, Sirimaturos M, Hirshberg EL, Bircher NG, Agus MSD, Carpenter DL, et al. Society of critical care medicine guidelines on glycemic control for critically ill children and adults 2024. Crit Care Med. (2024) 52(4):e161–81. doi: 10.1097/CCM.0000000000006174
22. Khwaja A. Kdigo clinical practice guidelines for acute kidney injury. Nephron Clin Pract. (2012) 120:c179–84. doi: 10.1159/000339789
23. Chen TJ, Chung YW, Chang HR, Chen PY, Wu CR, Hsieh SH, et al. Diagnostic accuracy of the CAM-ICU and ICDSC in detecting intensive care unit delirium: a bivariate meta-analysis. Int J Nurs Stud. (2021) 113:103782. doi: 10.1016/j.ijnurstu.2020.103782
24. Ferreira LO, Vasconcelos VW, Lima JS, Vieira NJ, Da CG, Esteves JC, et al. Biochemical changes in cardiopulmonary bypass in cardiac surgery: new insights. J Pers Med. (2023) 13:1506. doi: 10.3390/jpm13101506
25. Baehner T, Boehm O, Probst C, Poetzsch B, Hoeft A, Baumgarten G, et al. Cardiopulmonary bypass in cardiac surgery. Anaesthesist. (2012) 61:846–56. doi: 10.1007/s00101-012-2050-0
26. Floh AA, Manlhiot C, Redington AN, McCrindle BW, Clarizia NA, Caldarone CA, et al. Insulin resistance and inflammation are a cause of hyperglycemia after pediatric cardiopulmonary bypass surgery. J Thorac Cardiovasc Surg. (2015) 150:498–504. doi: 10.1016/j.jtcvs.2015.06.028
27. Thiessen S, Vanhorebeek I, Van den Berghe G. Glycemic control and outcome related to cardiopulmonary bypass. Best Pract Res Clin Anaesthesiol. (2015) 29:177–87. doi: 10.1016/j.bpa.2015.03.003
28. Zhang M, Zhang Z, Zhu N, Wang L, Huang H, Wang Y, et al. Systematic review and meta-analysis of risk factors associated with postoperative stress hyperglycemia in patients without diabetes following cardiac surgery. Rev Cardiovasc Med. (2025) 26:25485. doi: 10.31083/RCM25485
29. Baker EH, Wood DM, Brennan AL, Clark N, Baines DL, Philips BJ. Hyperglycaemia and pulmonary infection. Proc Nutr Soc. (2006) 65:227–35. doi: 10.1079/pns2006499
30. Dungu AM, Ryrso CK, Hegelund MH, Jensen AV, Kristensen PL, Krogh-Madsen R, et al. Diabetes status, C-reactive protein, and insulin resistance in community-acquired pneumonia-A prospective cohort study. J Clin Med. (2024) 13:245. doi: 10.3390/jcm13010245
31. Salonen PH, Koskela HO, Niskanen L. Prevalence and determinants of hyperglycaemia in pneumonia patients. Scand J Infect Dis. (2013) 45(2):88–94. doi: 10.3109/00365548.2012.713117
32. Nair BG, Horibe M, Neradilek MB, Newman SF, Peterson GN. The effect of intraoperative blood glucose management on postoperative blood glucose levels in noncardiac surgery patients. Anesth Analg. (2016) 122:893–902. doi: 10.1213/ANE.0000000000001100
33. Yamamoto N, Irie T, Takaki S, Yamaguchi O, Goto T. Predictors of severe postoperative hyperglycemia after cardiac surgery in infants: a single-center, retrospective, observational study. J Anesth. (2018) 32:160–6. doi: 10.1007/s00540-017-2444-x
34. Zhang Y, Cai S, Xiong X, Zhou L, Shi J, Chen D. Intraoperative glucose and kidney injury after on-pump cardiac surgery: a retrospective cohort study. J Surg Res. (2024) 300:439–47. doi: 10.1016/j.jss.2024.04.080
35. Choi H, Park CS, Huh J, Koo J, Jeon J, Kim E, et al. Intraoperative glycemic variability and mean glucose are predictors for postoperative delirium after cardiac surgery: a retrospective cohort study. Clin Interv Aging. (2022) 17:79–95. doi: 10.2147/CIA.S338712
36. Shah NJ, Leis A, Kheterpal S, Englesbe MJ, Kumar SS. Association of intraoperative hyperglycemia and postoperative outcomes in patients undergoing non-cardiac surgery: a multicenter retrospective study. Bmc Anesthesiol. (2020) 20:106. doi: 10.1186/s12871-020-01022-w
37. Wahba A, Milojevic M, Boer C, De Somer F, Gudbjartsson T, van den Goor J, et al. 2019 EACTS/EACTA/EBCP guidelines on cardiopulmonary bypass in adult cardiac surgery. Eur J Cardiothorac Surg. (2020) 57:210–51. doi: 10.1093/ejcts/ezz267
38. Wan S, LeClerc JL, Vincent JL. Cytokine responses to cardiopulmonary bypass: lessons learned from cardiac transplantation. Ann Thorac Surg. (1997) 63(1):269–76. doi: 10.1016/s0003-4975(96)00931-9
39. Greco G, Ferket BS, D'Alessandro DA, Shi W, Horvath KA, Rosen A, et al. Diabetes and the association of postoperative hyperglycemia with clinical and economic outcomes in cardiac surgery. Diabetes Care. (2016) 39:408–17. doi: 10.2337/dc15-1817
40. Marin-Vivas RR, Saldivar-Muller CE, Sanchez-Banuelos CC, Flores-Lujano J, Nunez-Enriquez JC. Prognostic factors of postoperative severe hyperglycemia after cardiac surgery in pediatric patients. Rev Med Inst Mex Seguro Soc. (2017) 55:324–9.28440986
41. Jones KW, Cain AS, Mitchell JH, Millar RC, Rimmasch HL, French TK, et al. Hyperglycemia predicts mortality after CABG: postoperative hyperglycemia predicts dramatic increases in mortality after coronary artery bypass graft surgery. J Diabetes Complications. (2008) 22:365–70. doi: 10.1016/j.jdiacomp.2007.05.006
Keywords: cardiac surgery, cardiopulmonary bypass, postoperative hyperglycemia, risk factors, clinical outcomes
Citation: Xiang Y, Luo T and Zeng L (2025) Risk factors and clinical outcome of postoperative hyperglycemia after cardiac surgery with cardiopulmonary bypass. Front. Cardiovasc. Med. 12:1479922. doi: 10.3389/fcvm.2025.1479922
Received: 13 August 2024; Accepted: 12 March 2025;
Published: 7 April 2025.
Edited by:
Enyi Shi, China Medical University, ChinaReviewed by:
Eric Jeng, University of Florida, United StatesCopyright: © 2025 Xiang, Luo and Zeng. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Ling Zeng, emVuZ2xpbmc1MTBAMTYzLmNvbQ==
†These authors have contributed equally to this work
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.