
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Cardiovasc. Med., 07 April 2025
Sec. Sex and Gender in Cardiovascular Medicine
Volume 12 - 2025 | https://doi.org/10.3389/fcvm.2025.1463439
This article is part of the Research TopicDisparities, controversies and unmet needs in the management of cardiomyopathiesView all 3 articles
 Michael Butzner1*
Michael Butzner1* Sanika Amonkar2
Sanika Amonkar2 Meiling Chen2Eros Papademetriou3Ravi Potluri3Xing Liu3
Meiling Chen2Eros Papademetriou3Ravi Potluri3Xing Liu3 Theodore Abraham2
Theodore Abraham2
Background: Previous studies of patients with symptomatic obstructive hypertrophic cardiomyopathy (oHCM) have reported worse clinical burden for female patients; whether this translates to an increase in healthcare resource use (HRU) and cost is unknown. Therefore, we evaluated the impact of sex on economic burden in symptomatic oHCM.
Methods: Medical and pharmacy claims data were assessed from 2016 to 2021 to identify (ICD-10 code) adult patients with symptomatic oHCM in the United States. Generalized linear models were used to estimate HCM-related cost and generalized estimating equations for HRU [both reported as mean per-person-per-year (PPPY)] for healthcare categories: inpatient, outpatient, emergency room (ER), urgent care, and pharmacy. Cox proportional hazard regressions were used to compare differences in male and female patients with symptomatic HCM.
Results: Among 9,490 patients with symptomatic oHCM, 5,309 (55.9%) were female. Female patients were older (64 ± 13 vs. 59 ± 14), with a higher Charlson Comorbidity Index (1.9 vs. 1.7) compared to males, respectively. After adjusting for patient characteristics, female patients had significantly greater number of HCM-related hospitalizations (0.24 vs. 0.20 PPPY, p = 0.0014), LOS (5.08 vs. 4.30 PPPY; p = 0.0235), number of outpatient visits (4.98 vs. 4.59 PPPY; p = 0.0387), and number of distinct drugs (0.59 vs. 0.55 PPPY; p = 0.0010), compared with males, respectively. In adjusted models, only HCM-related pharmacy costs were significant, with female patients having slightly higher costs compared to males ($70 vs. $61 PPPY; p = 0.0465). There were no significant differences in all-cause costs of care between male and female patients with oHCM.
Conclusions: Female patients with symptomatic oHCM experience greater rates of HCM-related and all-cause hospitalizations and number of prescriptions, and HCM-related length of stay, outpatient visits, and pharmacy costs compared to male patients.
Hypertrophic Cardiomyopathy (HCM) is a chronic, progressive myocardial disorder defined by LV hypertrophy (1). An ECG-based epidemiologic study showed a disease prevalence of 1 case per 500 people in the general population, but a higher prevalence (1 case per 200) can be calculated when both clinical and genetic diagnoses are considered (2, 3). Using population-based methods, the estimated average prevalence of HCM around the world varies from 1 in 1,250 people in the US to a range of 1 in 1,372 people to 1 in 3,195 people in European countries (4–7). Approximately two-thirds of diagnosed HCM cases are obstructive HCM (oHCM) (8), and an estimated 50% of patients with oHCM are symptomatic (9). Previous studies have outlined the economic burden for patients with oHCM (9–11), but no evidence exists on the impact of sex on economic burden in this disease. Because female sex is associated with a higher risk of HCM-related events, HCM-related death, major cardiovascular events, cardiovascular death, noncardiovascular death, and all-cause mortality (12), it is important to understand whether this translates to an increase in healthcare resource use (HRU) and cost. The objective of this study was to evaluate the impact of sex on HRU and costs in patients with symptomatic oHCM using a large, national database of medical and pharmacy administrative claims.
The study is a retrospective analysis of longitudinal medical and pharmacy claims data from Symphony Integrated Dataverse (IDV) database. The IDV is an open claims administrative health claims database that contains prescription, medical, and hospital claims across the US for all payment types, including commercial plans, Medicare Part D, cash, assistance programs, and Medicaid. The IDV contains over 10 billion deidentified prescriptions claims linked to over 280 million unique patients with an average of 5 years of prescription drug history. These prescription drug claims are linked to hospital and physician practices claims with medical procedure (i.e., current procedural terminology [CPT] and diagnosis codes [International Classification of Disease Tenth Revision (ICD-10)] for nearly 180 million patients. The full database includes claims from over 65,000 pharmacies, 1,500 hospitals, 800 outpatient facilities, and 80,000 physician practices across the US, capturing approximately 75% of the total prescriptions dispensed in the US. The IDV database was selected due to its longitudinal nature and comprehensive coverage of claims required to meet the study objectives. The distribution of Symphony Health patients across census regions is very similar to that of the US population.
Patients of interest were identified from January 1st, 2017 to April 30th, 2021, with a 12-month index period. The first relevant ICD-10 claim of HCM diagnosis was considered as the index diagnosis date. The date of first treatment with a beta-blocker, calcium channel blocker, disopyramide, or a procedure of interest (e.g., alcohol septal ablation, septal myectomy, pacemaker) after diagnosis date was considered as the index treatment date. Patient demographics and clinical characteristics were captured at baseline and costs and HRU were captured over the follow-up period. The data used in this study were de-identified in compliance with the Health Insurance Portability and Accountability Act.
The patient population for this study consisted of prevalent patients with oHCM identified from the IDV (Figure 1). Adult (Age ≥ 18 years at index treatment date) patients with oHCM who met the following criteria were included in this study (1) ≥two claims of oHCM (ICD-10 diagnosis code: I42.1) at least 30 days apart, or (2) one diagnosis of HCM (ICD-10 diagnosis code: I42.2) along with either a diagnosis of oHCM (ICD-10 diagnosis code: I42.1) at least 30 days apart or a septal reduction therapy procedure any time after HCM diagnosis. Patients were required to have 12 months of activity prior to index treatment date, 3 months of activity post index treatment date, and be symptomatic. Patients were categorized as symptomatic if they had a diagnosis for fatigue, chest pain, syncope, dyspnea, heart failure, palpitations, insertion of a pacemaker, or septal reduction therapy, in the 3 months before or after their index diagnosis date. We excluded patients with a diagnosis of Fabry disease, amyloidosis, and patients with HCM treatment in the 12 months prior to index treatment date (i.e., patients were treatment-naïve at index treatment date). Patients were followed from their index treatment date until the end of index treatment due to either (1) discontinuation, (2) treatment switch, (3) treatment augmentation, or (4) end of activity in the database.
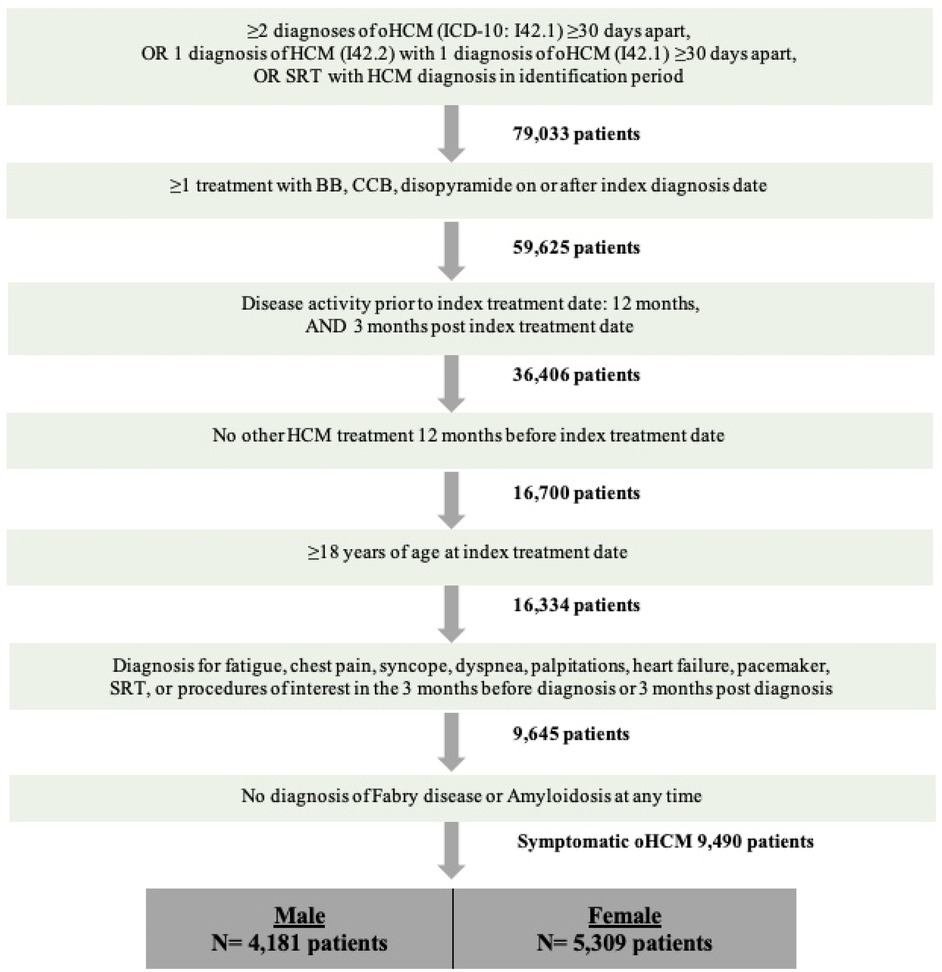
Figure 1. Patient selection criteria.
Patient demographics and comorbidities, included the Charlson Comorbidity Index, were calculated 12 months prior to index date (excluding index date). All-cause and HCM-related HRU and costs were evaluated. Healthcare resource utilization and costs were defined for inpatient admissions, outpatient visits, ER visits, urgent care visits, other visits, and pharmacy costs (HCM-related prescriptions and non-HCM related prescriptions). HCM-related outcome variables included in this analysis were predefined based on the AHA/ACC treatment guidelines and confirmed by clinical experts who care for patients with HCM (13). Regarding the financial data available in the IDV, final adjudicated costs were only available for all-cause related prescriptions. For all other cost categories including HCM-related prescriptions, the amount billed by the payer (charged amount) is reported.
Descriptive statistics were presented as means and standard deviation (SD), median and interquartile range (IQR) for continuous variables, and frequencies and proportions for categorical, and dichotomous variables. Baseline characteristics were compared with Chi-squared test for categorical variables or Kruskal–Wallis test for continuous variables. Systematic differences between sex were evaluated by Kruskal–Wallis for continuous variables and Chi-square tests for categorical variables. Generalized linear models with a gamma distribution and log link clustered on the patient was used to estimate per-person-per-year (PPPY) costs and generalized estimating equations with a negative binomial distribution clustered on the patient was used to estimation PPPY visits. The mean difference in PPPY costs/visits, 95% confidence intervals (CIs), and p-values were estimated for the patient cohort and by sex. These estimates were evaluated for each healthcare setting (inpatient, outpatient, ER, urgent care, other medical visits, and prescriptions).
An adjusted analysis of all-cause and HCM related HRU and costs was conducted. This included generalized linear models to estimate adjusted healthcare costs and generalized estimating equations to estimate adjusted healthcare visits. Covariates in the adjusted models were selected based on differences seen in a univariate analysis of baseline variables between males and females (Table 1). These included the baseline patient values of age, region, insurance type, hypertension, atrial fibrillation and flutter, heart failure, ventricular fibrillation, ventricular tachycardia, chronic pulmonary disease, obesity, valvular disease, stress cardiomyopathy, and coronary artery disease. Missing or unavailable data were not included in the analyses.
Among 9,490 patients with symptomatic oHCM, 5,309 (55.9%) were female and male patients had longer length of follow-up time (Table 1). Female patients were older (64 ± 13 vs. 59 ± 14; p < 0.0001) compared to males, respectively. Regardless of sex, the majority of patients in this cohort were 65 years of age or older (N = 4,726, 99.6%). Female patients also had a higher Charlson Comorbidity Index (1.9 vs. 1.7; p < 0.0001) compared to males, respectively. Baseline patient clinical characteristics for this cohort of patients with symptomatic oHCM are summarized in Table 2.
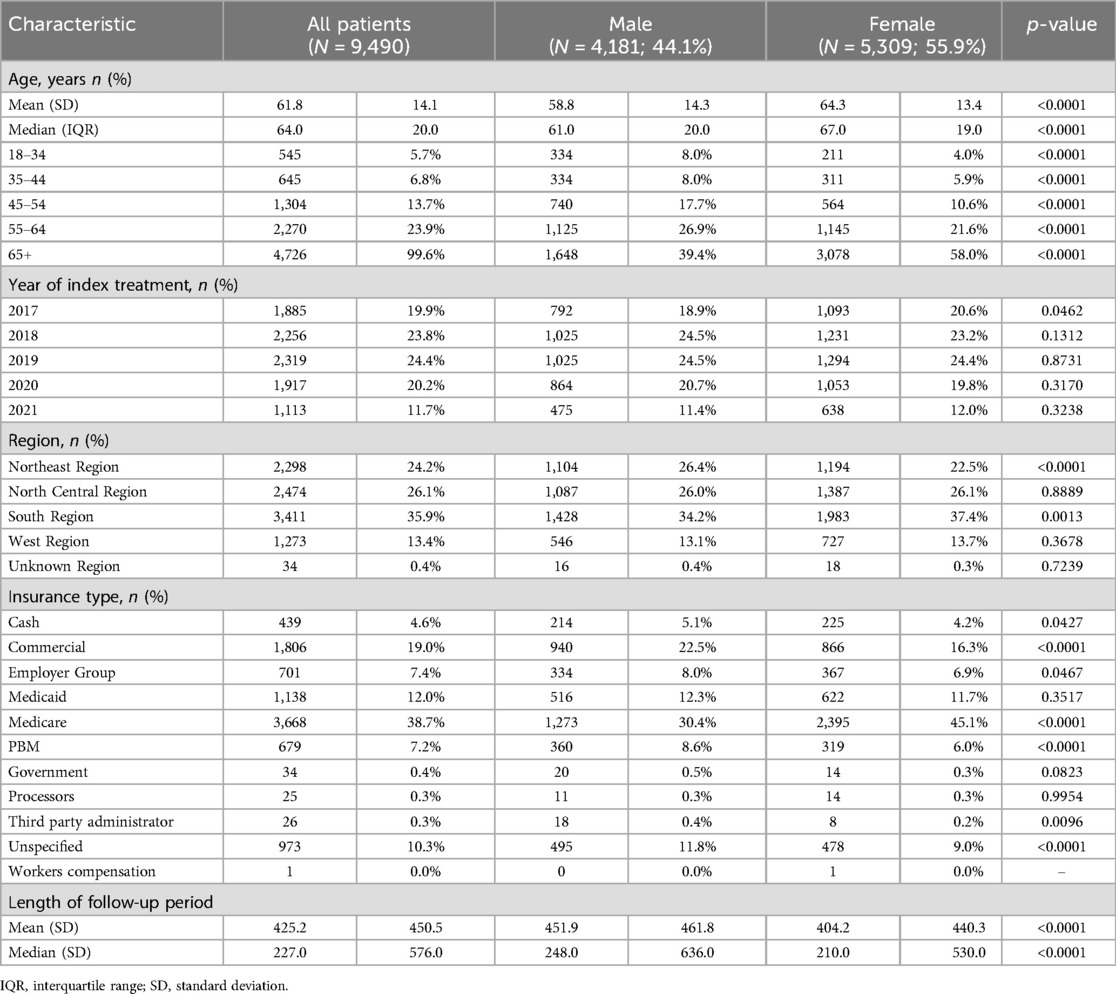
Table 1. Baseline patient demographics.
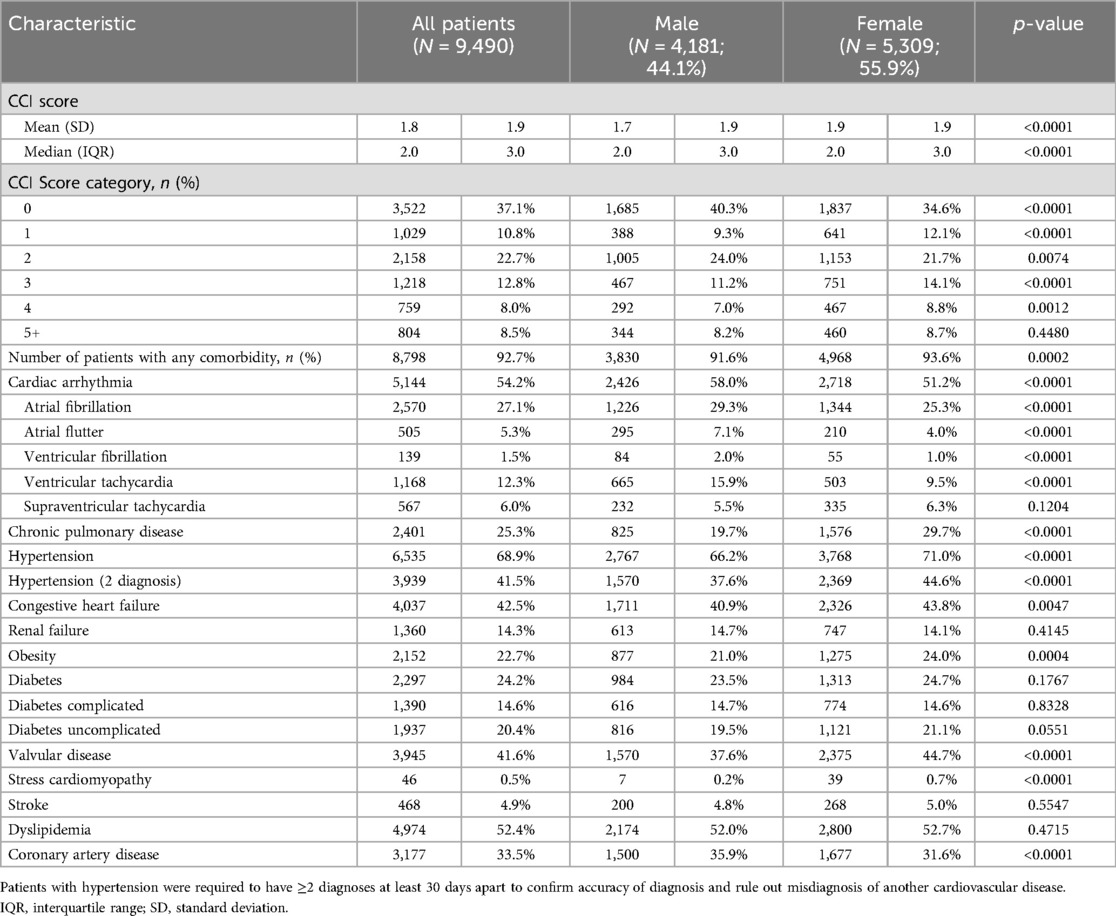
Table 2. Baseline patient clinical characteristics.
After adjusting for patient characteristics, female patients had significantly greater number of HCM-related hospitalizations (0.24 vs. 0.20 PPPY, p = 0.0014), LOS (5.08 vs. 4.30 PPPY; p = 0.0235), number of outpatient visits (4.98 vs. 4.59 PPPY; p = 0.0387), and number of distinct drugs (0.59 vs. 0.55 PPPY; p = 0.0010), compared with males, respectively (Table 3). Additionally, female patients had significantly greater number of all-cause hospitalizations (0.96 vs. 0.82 PPPY, p = 0.0002) and number of distinct drugs (7.34 vs. 6.31 PPPY; p < 0.0001), after adjusting for patient characteristics (Table 4). Unadjusted HCM-related and all-cause HRU are presented in Supplementary Table S1 and Supplementary Table S2, respectively.
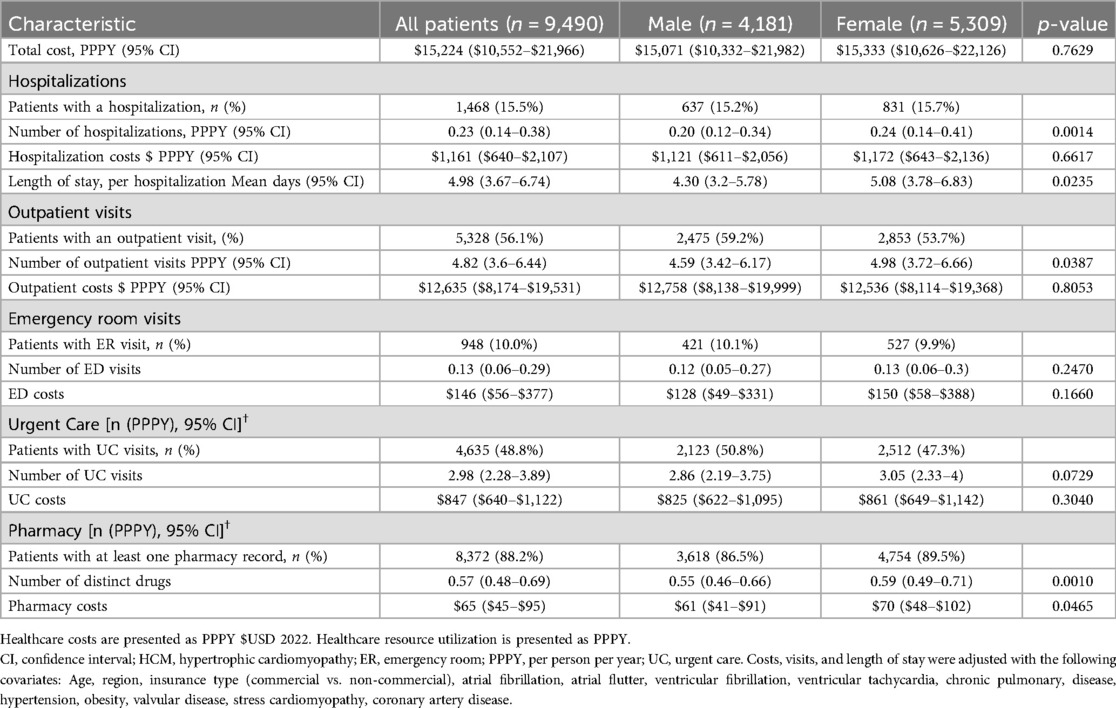
Table 3. Adjusted HCM-related healthcare resource utilization and costs.
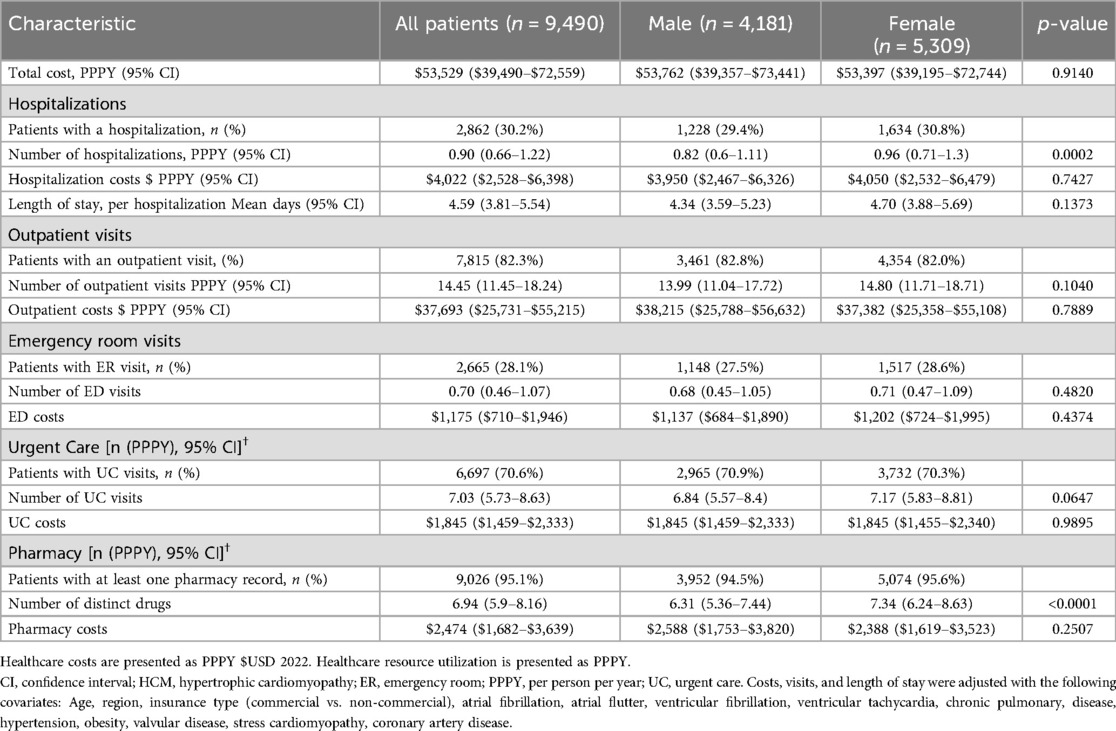
Table 4. Adjusted All-cause healthcare resource utilization and costs.
Among symptomatic oHCM patients, total all-cause costs were greater compared to HCM-related costs, respectively ($51,835 vs. $23,048). In adjusted models, only HCM-related pharmacy costs were significant, with female patients having slightly higher costs compared to males ($70 vs. $61 PPPY; p = 0.0465; Table 3). There were no significant differences in all-cause cost of care between male and female patients with oHCM (Table 4). Unadjusted HCM-related and all-cause costs are presented in Supplementary Table S1, and no significant differences in any all-cause costs categories between male and female patients with symptomatic oHCM (Supplementary Table S2).
To our knowledge, this is the first study to evaluate the impact of sex on HRU and costs in patients with symptomatic oHCM. Using a large, national database of medical and pharmacy administrative claims, we found that female patients with symptomatic oHCM, after adjusting for baseline patient characteristics, experience greater HCM-related and all-cause hospitalizations and prescriptions, and HCM-related length of stay and outpatient visits compared to male patients. Furthermore, female patients had greater HCM-related pharmacy costs, but there were no differences in all-cause costs of care by sex in symptomatic oHCM patient. Thus, suggesting that significant increases in costs of care for this cohort of patients may potentially be attributable to the specific nature of their symptomatic oHCM.
While previous investigations have analyzed the economic burden of patients with HCM (9, 10, 14), including invasive procedures like septal reduction therapy (11, 15–17), this is the first population-based study to evaluate the impact of sex on HRU and costs among patients with symptomatic oHCM. In a previous population-based study, Butzner et al. (2022) used a national medical and pharmacy claims database in the United States to evaluate HCM-related and all-cause economic burden for patients with oHCM (10). They found that costs related to oHCM increased from $5,968 to $20,290 at 1-year follow-up after oHCM diagnosis ($23,048 in the current analysis), driven mostly by inpatient hospitalizations and surgical costs (10). Additionally, in their cohort of oHCM patients, 27% had an inpatient hospitalization due to their HCM (10), compared to 15.5% of patients in the present study having an inpatient hospitalization. Our study extends upon these findings to show that when factoring in sex in adjusted models, female patients with symptomatic oHCM experience greater HRU compared to male counterparts.
Prior to this investigation, a single study used medical and pharmacy claims data to evaluate sex differences in oHCM treatment and cardiovascular outcomes among patients with oHCM (18). Regarding treatment, they found women were less likely to be prescribed HCM-related treatments including beta blockers and anticoagulants (18). In contrast, we found that female patients with symptomatic oHCM were more likely to have an HCM-related and all-cause prescription fill, with 89.5% of patients receiving a prescription to treat their oHCM. However, the present analysis evaluated HCM prescriptions as an inclusive category of all HCM prescriptions, without separating specific HCM medications to test differences. We extend upon these clinical differences among sex to report that after adjusting for baseline patient characteristics, female patients with symptomatic oHCM are prescribed more HCM-related and all-cause prescriptions to treat their disease compared with male patients.
The impact of comorbidities in oHCM (including by sex) is important to consider for the present analysis as female patients presented with greater comorbidity burden and increased HRU. For example, hemodynamic disruptions due to obstruction in HCM can be further exacerbated by systolic anterior motion of the mitral valve and are a critical component of disease development (19). Previous studies show that oHCM patients commonly have additional structural abnormalities of the sub-mitral valve (20, 21), with a significant difference in female and male patients (44.7% vs. 37.6, respectively) in the present analysis having valvular disease. Concomitant interventions to account for these additive comorbidities are associated with worse clinical outcomes including in- hospital death, adverse in-hospital events, and 30-day readmission (22). Further investigation is needed to understand whether differences in HRU and costs are driven primarily by oHCM or comorbidities, and if there are difference across sex.
It is also important to consider the present results in context of a contemporary population of HCM. In a recent study of a large, global registry of patients with HCM, Canepa et al. (2020) found that age of HCM diagnosis increased significantly over time with a stable male-to-female ratio, suggesting that evolving HCM populations include progressively greater representation of older patients (23). Socioeconomic factors, such as age, may impact patients' healthcare costs. While it is plausible to hypothesize that economic burden for patients increase with age, a retrospective analysis of 5,129 patients with oHCM found that being aged 18–39 years was associated with increased HCM-related healthcare costs (total, medical, office visit, outpatient visit, emergency room), compared to older categorical age groups (24). Additionally, the current findings must take into account a longer length of follow-up for male patients. Further investigation is needed to evaluate time-varying impact of both age and sex on costs of care and HRU in patients with HCM.
This study provides benchmark economic data on the impact of sex on the costs of care for patients with symptomatic oHCM. Female patients experienced greater HRU and pharmacy costs due to their HCM compared to male patients with symptomatic oHCM, after adjusting for patient characteristics. Healthcare costs and resource utilization have not been detailed in previous (13) and current (21) recommended guidelines for the management of patients with HCM, including the impact of sex on clinical and economic burden. The results from this analysis can be used to emphasize and bring awareness to sex differences in resource utilization and costs of care for symptomatic oHCM, highlighting the clinical importance of sex-based differences for diagnosis and management in HCM patients. Lastly, regarding economic differences in HCM prescription fills and increased utilization among female patients, the impact of emerging therapies, indicated for patients with symptomatic oHCM (25–28), on HRU and costs of care for patients with symptomatic oHCM should be evaluated.
This study is subject to several limitations, which are common across claims database analyses. The diagnoses, comorbidities, HRU and costs of patients with HCM were identified based on ICD-10-CM diagnosis code. The presence of a diagnosis code on a medical claim does not necessarily indicate a positive presence of disease because the medical record may have been incorrectly coded or included as a rule-out criterion rather than the actual disease. Also, diagnosis codes only signify the presence of the disease and do not detail the characteristics or the nature of the disease as you would find in electronic medical record data. This limitation was overcome by requiring eligible patients to have at least two claims with diagnosis codes for HCM. It was also ensured that generic codes, such as codes for “other cardiomyopathy” and “unspecified cardiomyopathy,” which could be used for HCM, were not included in the identification of HCM patients for the study.
Diagnosis codes were used to identify patients with symptomatic oHCM, and a combination of symptoms, comorbidities, and procedures was used to identify symptomatic oHCM in this study. Since the claims database does not have a record of all symptoms of a patient, and some of the symptoms could be attributed to comorbidities, there is the possibility of difference in actual proportion of patients with symptomatic oHCM and the estimates in this study. Additionally, due to restrictions of the database regarding HIPAA policies, we are unable to report separate costs for surgical procedures including septal reduction therapy. Furthermore, without patient level medical record data, the question remains whether these differences in HRU (including adjusted analyses) are driven primarily by HCM or the additive comorbidity burden. Lastly, the definition of costs in this analysis was charges, meaning the amount billed by the payer. This may not be reflective of what a patients pays for their cost of care, but what the charged amount is by the payer in the U.S. healthcare system.
In this large, national cohort of symptomatic oHCM patients, adjusted models report that female patients with symptomatic oHCM experienced greater rates of HCM-related and all-cause hospitalizations and number of prescriptions, and HCM-related length of stay, outpatient visits, and pharmacy costs compared to male patients. These findings highlight the clinical importance of sex-based differences for diagnosis and management in HCM patients and warrant inclusion in current HCM treatment guidelines. Future research on the impact of emerging therapies on HRU and cost of care for patients with symptomatic oHCM should be evaluated.
The original contributions presented in the study are included in the article/Supplementary Material, further inquiries can be directed to the corresponding author.
Ethical approval was not required for the study involving humans in accordance with the local legislation and institutional requirements. Written informed consent to participate in this study was not required from the participants or the participants' legal guardians/next of kin in accordance with the national legislation and the institutional requirements.
MB: Conceptualization, Funding acquisition, Investigation, Methodology, Project administration, Supervision, Validation, Visualization, Writing – original draft, Writing – review & editing. SA: Conceptualization, Methodology, Validation, Visualization, Writing – review & editing. MC: Conceptualization, Methodology, Validation, Visualization, Writing – review & editing. EP: Conceptualization, Data curation, Formal Analysis, Methodology, Project administration, Resources, Software, Supervision, Validation, Visualization, Writing – review & editing. RP: Conceptualization, Data curation, Methodology, Project administration, Software, Supervision, Validation, Visualization, Writing – review & editing. XL: Conceptualization, Data curation, Formal analysis, Methodology, Software, Validation, Visualization, Writing – review & editing. TA: Conceptualization, Investigation, Methodology, Supervision, Validation, Visualization, Writing – review & editing.
The author(s) declare that financial support was received for the research and/or publication of this article. This work was funded by Cytokinetics Incorporated.
MB was employed by the Cytokinetics Incorporated. EP, RP and XL were employed by the Putnam Associates, LLC.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fcvm.2025.1463439/full#supplementary-material
1. Authors/Task Force members, Elliott PM, Anastasakis A, Borger MA, Borggrefe M, Cecchi F, Charron P, Hagege AA, et al. 2014 ESC guidelines on diagnosis and management of hypertrophic cardiomyopathy: the task force for the diagnosis and management of hypertrophic cardiomyopathy of the European Society of Cardiology (ESC). Eur Heart J. (2014) 35(39):2733–79. doi: 10.1093/eurheartj/ehu284
2. Semsarian C, Ingles J, Maron MS, Maron BJ. New perspectives on the prevalence of hypertrophic cardiomyopathy. J Am Coll Cardiol. (2015) 65(12):1249–54. doi: 10.1016/j.jacc.2015.01.019
3. Maron BJ, Gardin JM, Flack JM, Gidding SS, Kurosaki TT, Bild DE. Prevalence of hypertrophic cardiomyopathy in a general population of young adults. Echocardiographic analysis of 4111 subjects in the CARDIA study. Coronary artery risk development in (young) adults. Circulation. (1995) 92(4):785–9. doi: 10.1161/01.cir.92.4.785
4. Butzner M, Maron M, Sarocco P, Rowin E, Teng CC, Tan H, et al. Clinical diagnosis of hypertrophic cardiomyopathy over time in the United States (A population-based claims analysis). Am J Cardiol. (2021) 159:107–12. doi: 10.1016/j.amjcard.2021.08.024
5. Maron MS, Hellawell JL, Lucove JC, Farzaneh-Far R, Olivotto I. Occurrence of clinically diagnosed hypertrophic cardiomyopathy in the United States. Am J Cardiol. (2016) 117(10):1651–4. doi: 10.1016/j.amjcard.2016.02.044
6. Magnusson P, Palm A, Branden E, Mörner S. Misclassification of hypertrophic cardiomyopathy: validation of diagnostic codes. Clin Epidemiol. (2017) 9:403–10. Published 2017 August 9. doi: 10.2147/CLEP.S139300
7. Husser D, Ueberham L, Jacob J, Heuer D, Riedel-Heller S, Walker J, et al. Prevalence of clinically apparent hypertrophic cardiomyopathy in Germany-an analysis of over 5 million patients. PLoS One. (2018) 13(5):e0196612. Published 2018 May 3. doi: 10.1371/journal.pone.0196612
8. Lu DY, Pozios I, Haileselassie B, Ventoulis I, Liu H, Sorensen LL, et al. Clinical outcomes in patients with nonobstructive, labile, and obstructive hypertrophic cardiomyopathy. J Am Heart Assoc. (2018) 7(5):e006657. Published 2018 February 25. doi: 10.1161/JAHA.117.006657
9. Jain SS, Li SS, Xie J, Sutton MB, Fine JT, Edelberg JM, et al. Clinical and economic burden of obstructive hypertrophic cardiomyopathy in the United States. J Med Econ. (2021) 24(1):1115–23. doi: 10.1080/13696998.2021.1978242
10. Butzner M, Maron M, Sarocco P, Teng CC, Stanek E, Tan H, et al. Healthcare resource utilization and cost of obstructive hypertrophic cardiomyopathy in a US population. Am Heart J Plus Cardiol Res Pract. (2022) 13:100089. doi: 10.1016/j.ahjo.2022.100089
11. Butzner M, Maron MS, Sarocco P, Teng CC, Stanek E, Tan H, et al. Costs and healthcare resource utilization for obstructive hypertrophic cardiomyopathy with septal reduction therapy. J Invasive Cardiol. (2022) 34(12):E866–72. doi: 10.25270/jic/22.00150
12. Zhao H, Tan Z, Liu M, Yu P, Ma J, Li X, et al. Is there a sex difference in the prognosis of hypertrophic cardiomyopathy? A systematic review and meta-analysis. J Am Heart Assoc. (2023) 12(11):e026270. doi: 10.1161/JAHA.122.026270
13. Ommen SR, Mital S, Burke MA, Day SM, Deswal A, Elliott P, et al. 2020 AHA/ACC guideline for the diagnosis and treatment of patients with hypertrophic cardiomyopathy: a report of the American College of Cardiology/American Heart Association joint committee on clinical practice guidelines [published correction appears in circulation. 2020 Dec 22;142(25):e633]. Circulation. (2020) 142(25):e558–631. doi: 10.1161/CIR.0000000000000937
14. Owens AT, Sutton MB, Gao W, Fine JT, Xie J, Naidu SS, et al. Treatment changes, healthcare resource utilization, and costs among patients with symptomatic obstructive hypertrophic cardiomyopathy: a claims database study. Cardiol Ther. (2022) 11(2):249–67. doi: 10.1007/s40119-022-00257-7
15. Chothani A, Panaich SS, Patel N, Patel NJ, Arora S, Deshmukh A, et al. Septal ablation and hypertrophic obstructive cardiomyopathy: 7 years US experience. J Interv Cardiol. (2016) 29(5):505–12. doi: 10.1111/joic.12319
16. Ando T, Adegbala O, Aggarwal A, Afonso L, Grines CL, Takagi H, et al. Unplanned thirty-day readmission after alcohol septal ablation for hypertrophic cardiomyopathy (from the nationwide readmission database). Am J Cardiol. (2020) 125(12):1890–5. doi: 10.1016/j.amjcard.2020.03.016
17. Panaich SS, Badheka AO, Chothani A, Mehta K, Patel NJ, Deshmukh A, et al. Results of ventricular septal myectomy and hypertrophic cardiomyopathy (from nationwide inpatient sample [1998–2010]). Am J Cardiol. (2014) 114(9):1390–5. doi: 10.1016/j.amjcard.2014.07.075
18. Butzner M, Leslie D, Cuffee Y, Hollenbeak CS, Sciamanna C, Abraham TP. Sex differences in clinical outcomes for obstructive hypertrophic cardiomyopathy in the USA: a retrospective observational study of administrative claims data. BMJ Open. (2022) 12(3):e058151. Published 2022 March 9. doi: 10.1136/bmjopen-2021-058151
19. Ommen SR, Ho CY, Asif IM, Balaji S, Burke MA, Day SM, et al. 2024 AHA/ACC/AMSSM/HRS/PACES/SCMR guideline for the management of hypertrophic cardiomyopathy: a report of the American Heart Association/American College of Cardiology Joint Committee on clinical practice guidelines [published correction appears in circulation. 2024 Aug 20;150(8):e198. doi: 10.1161/CIR.0000000000001277]. Circulation. (2024) 149(23):e1239–311. doi: 10.1161/CIR.0000000000001250
20. Maron MS, Olivotto I, Harrigan C, Appelbaum E, Gibson CM, Lesser JR, et al. Mitral valve abnormalities identified by cardiovascular magnetic resonance represent a primary phenotypic expression of hypertrophic cardiomyopathy. Circulation. (2011) 124(1):40–7. doi: 10.1161/CIRCULATIONAHA.110.985812
21. Sherrid MV, Balaram S, Kim B, Axel L, Swistel DG. The mitral valve in obstructive hypertrophic cardiomyopathy: a test in context. J Am Coll Cardiol. (2016) 67(15):1846–58. doi: 10.1016/j.jacc.2016.01.071
22. Altibi AM, Sapru A, Ghanem F, Zhao Y, Alani A, Cigarroa J, et al. Impact of concomitant surgical interventions on outcomes of septal myectomy in obstructive hypertrophic cardiomyopathy. Int J Cardiol. (2024) 400:131790. doi: 10.1016/j.ijcard.2024.131790
23. Canepa M, Fumagalli C, Tini G, Vincent-Tompkins J, Day SM, Ashley EA, et al. Temporal trend of age at diagnosis in hypertrophic cardiomyopathy: an analysis of the international sarcomeric human cardiomyopathy registry. Circ Heart Fail. (2020) 13(9):e007230. doi: 10.1161/CIRCHEARTFAILURE.120.007230
24. Reza N, Butzner M, Batra K, Amos Q, Buikema A, Anderson A, et al. Abstract 4137810: association of sociodemographic characteristics on costs of care in patients with obstructive hypertrophic cardiomyopathy. Circulation. (2024) 150(1):Suppl_1. doi: 10.1161/circ.150.suppl_1.4137810
25. Maron MS, Masri A, Choudhury L, Olivotto I, Saberi S, Wang A, et al. Phase 2 study of aficamten in patients with obstructive hypertrophic cardiomyopathy. J Am Coll Cardiol. (2023) 81:34–45. doi: 10.1016/j.jacc.2022.10.020
26. Coats CJ, Maron MS, Abraham TP, Olivotto I, Lee MMY, Arad M, et al. Exercise capacity in patients with obstructive hypertrophic cardiomyopathy: SEQUOIA-HCM baseline characteristics and study design. JACC Heart Fail. (2024) 12(1):199–215. doi: 10.1016/j.jchf.2023.10.004
27. Cytokinetics. Cytokinetics Annouces Postivie Results From SEQUOIA-HCM, the Pivotal Phase 3 Clinical Trial of Aficamten in Patients With Obstructive Hypertrhophic Cardiomyopathy. Available online at: https://ir.cytokinetics.com/news-releases/news-release-details/cytokinetics-announces-positive-results-sequoia-hcm-pivotal (accessed January 20, 2024).
28. Cytokinetics. A Phase 3, Multi-center, Randomized, Double-blind Trial to Evaluate the Efficacy and Safety of Aficamten Compared to Metoprolol in Adults With Symptomatic Obstructive Hypertrophic Cardiomyopathy (MAPLE-HCM). Available online at: https://www.clinicaltrials.gov/study/NCT05767346 (accessed January 5, 2024).
Keywords: economic burden, hypertrophic cardiomyopathy, obstructive, sex differences, real-world evidence
Citation: Butzner M, Amonkar S, Chen M, Papademetriou E, Potluri R, Liu X and Abraham T (2025) Associations of sex on economic burden in patients with symptomatic obstructive hypertrophic cardiomyopathy: results from medical and pharmacy claims data. Front. Cardiovasc. Med. 12:1463439. doi: 10.3389/fcvm.2025.1463439
Received: 11 July 2024; Accepted: 12 March 2025;
Published: 7 April 2025.
Edited by:
Sri Harsha Patlolla, Mayo Clinic, United StatesReviewed by:
Giacomo Tini, Sapienza University of Rome, ItalyCopyright: © 2025 Butzner, Amonkar, Chen, Papademetriou, Potluri, Liu and Abraham. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Michael Butzner, bWJ1dHpuZXJAY3l0b2tpbmV0aWNzLmNvbQ==
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.