 Bupe Amon Kyelu
Bupe Amon Kyelu Phillip Taderera Bwititi2
Phillip Taderera Bwititi2 Ezekiel Uba Nwose
Ezekiel Uba Nwose- 1School of Health and Medical Science, University of Southern Queensland, Toowoomba, QLD, Australia
- 2School of Dentistry and Biomedical Sciences, Charles Sturt University, Wagga Wagga, NSW, Australia
A commentary on
By Liu J, Xiao G, Liang Y, He S, Lyu M and Zhu Y (2024). Front. Cardiovasc. Med. 11:1304864. doi: 10.3389/fcvm.2024.1304864
Introduction
In the paper, “Heart-brain interaction in cardiogenic dementia: pathophysiology and therapeutic potential” (1), it is acknowledged that heart failure (HF) may constitute the greatest burden of cardiovascular disease (CVD), which is a major public health issue globally. The authors draw attention to CVD physiology as well as the implications for cardiovascular medicine and also articulate and update three themes – risk factors, effects on cerebral blood flow (CBF) and preventive management – of cognitive impairment theory and mental health areas with a focus on dementia.
From a laboratory medicine perspective, the term “blood flow” is mentioned 5 times, and “platelet” 3 times. However, neither “blood test” for blood flow nor “viscosity” were indicated. Hence, from laboratory or evidence-base medicine perspective, there is opportunity to advance blood viscosity concept in dementia management. In this paper, the risk factors (atrial fibrillation, coronary artery disease, heart failure, myocardial infarction, and valvular heart disease) of cardiogenic dementia that can be associated with increased blood viscosity, are discussed. Further, the authors have elucidated on the mechanism to involve hypoperfusion and oxidative stress both leading to hyperviscosity, as well as prevention therapies to reduce blood viscosity (Table 1).
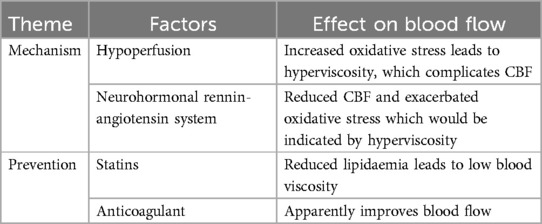
Table 1. Rearticulation of blood viscosity in cardiogenic dementia pathophysiology.
Antiplatelet management of hyperviscosity and implication for laboratory testing
Hyperviscosity constitutes a cardiovascular phenomenon, which connotes stasis (2), and the management of stasis in clinical practice involves antiplatelet drugs such as aspirin (3, 4). What is probably arguable is the practice of evidence-base monitoring of the therapeutic effectiveness. That is, the extent that the antiplatelet drugs such as aspirin and clopidogrel reduce the hyperviscosity being managed by laboratory monitoring methods. This therefore brings to the fore the concept of measuring blood viscosity in clinical practice. Perhaps, a second question is awareness of availability and utility of blood viscosity measurement.
There have been alternative tests for plasma viscosity and whole blood viscosity (5–8), which were limited to reference laboratory, but are no longer available. There is also the option of estimated or extrapolated whole blood viscosity (eWBV) (8), which is applicable in cardiovascular medicine (9, 10), including metabolic syndrome and mental health services but not yet adopted in clinical practice presumably due to lack of awareness.
Discussion: antiplatelet drug monitoring in cardiovascular medicine
This commentary advances the discourse of cardiogenic dementia to highlight a gap in knowledge and practice of mental health service. The implication of hyperviscosity in the pathophysiology and therapeutic potentials (1), means that laboratory evidence-base determination would need to studied to understand the course of hyperviscosity in pathophysiology and its response to treatment of various disorders.
It is pertinent to emphasize that the option of eWBV has been known for a long time and applicable in mental health management (8), and investigation of possible cardiovascular outcomes (5, 10), as well as antiplatelet therapy monitoring in diabetes (11). That is, blood viscosity evaluation including the eWBV option, is well established in clinical research, but there has been retrogress in clinical practice (9). Cardiogenic dementia has been recognised for over three decades (12), but there has been a lack of movement/research, which is evidenced by dearth or clinical trial or meta-analysis on the subject.
To expatiate a bit more on antiplatelet drug monitoring: it is noteworthy that patients deemed for antiplatelet therapy are supposed to be assessed against risk of bleeding prior to treatment (13). However, this is rarely done, most probably because the pathology is deemed unavailable, whereas eWBV is a useful tool (11). The methodology of eWBV is simple algorithm using haematocrit (packed cell volume) and serum protein from routine haematology and liver function tests, respectively (10, 11). Clinical guidelines for practical implementation are essentially the two opposite sides of haemostasis imbalance which often requires monitoring (3). That is, where bleeding risk or thrombosis would be identified with hypo-viscosity or hyper-viscosity, respectively.
Therefore, it is important to note that Liu and colleagues advanced the discourse on cardiogenic pathophysiology, and research can now review the aspect of laboratory evidence-base medicine. Further, the idea of monitoring rheological variables with laboratory tests is known but often limited to routine haematology including blood cell counts (14). This commentary advances the concept eWBV, which is at no additional “cost-of-production” to the health service providers.
It is also pertinent to emphasize that blood viscosity test in clinical practice used to be performed albeit in reference laboratories thus, limited access, by most clinicians, especially the remote and rural healthcare providers. This has resulted in under-utilisation of this important diagnostic test that is affordable since it can be estimated from routine lab results (9). Current testing provides a valid result only if immediate access to pathology services is available since transporting the sample for long distance can result in the deterioration. The newly-developed algorithm for estimating WBV from haematocrit and total serum protein levels, which are routine blood tests, offers ready access to this important measure of WBV.
Implications for health services research
This new process for assessing WBV using results from routine blood tests such as haematocrit and total serum protein can be accessed without using advanced testing. This means it can be used for various common diseases that are associated with changes in WBV, such as stress, with outpatient mental health and alcohol & other drugs services, diabetes mellitus, cardiovascular and kidney diseases (15). Further, this medical assessment does not require clients to be hospitalized or to travel to reference facility. Requests for WBV testing e.g., for a mental health client's evaluation of stress levels or for an individual living with cardiovascular disease can be done by a GP or primary healthcare provider (16–19), without the client needing to travel.
There has been the question whether blood flow changes with mood (20) and studies have reported that this can be the case. For instance, it is established that physical restraint of client can cause blood flow stasis leading to development of thrombosis complications (21). Therefore, suffice to conclude that there is reasonable justification to advance the laboratory evidence-base of cardiogenic mental health.
Author contributions
BK: Conceptualization, Writing – original draft, Writing – review & editing. PB: Supervision, Writing – original draft, Writing – review & editing. KK: Supervision, Writing – original draft, Writing – review & editing. EN: Conceptualization, Supervision, Writing – original draft, Writing – review & editing.
Funding
The author(s) declare that no financial support was received for the research, authorship, and/or publication of this article.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Liu J, Xiao G, Liang Y, He S, Lyu M, Zhu Y. Heart-brain interaction in cardiogenic dementia: pathophysiology and therapeutic potential. Front Cardiovasc Med. (2024) 11:1304864. doi: 10.3389/fcvm.2024.1304864
2. Zarkovic M, Kwaan HC. Correction of hyperviscosity by apheresis. Semin Thromb Hemost. (2003) 29(5):535–42. doi: 10.1055/s-2003-44560
3. Lee CH, Jung KH, Cho DJ, Jeong SK. Effect of warfarin versus aspirin on blood viscosity in cardioembolic stroke with atrial fibrillation: a prospective clinical trial. BMC Neurol. (2019) 19(1):82. doi: 10.1186/s12883-019-1315-5
4. Rosenson RS, Chen Q, Najera SD, Krishnan P, Lee ML, Cho DJ. Ticagrelor improves blood viscosity-dependent microcirculatory flow in patients with lower extremity arterial disease: the hema-kinesis clinical trial. Cardiovasc Diabetol. (2019) 18(1):77. doi: 10.1186/s12933-019-0882-5
5. Waksman O, Choi D, Mar P, Chen Q, Cho DJ, Kim H, et al. Association of blood viscosity and device-free days among hospitalized patients with COVID-19. J Intensive Care. (2023) 11(1):17. doi: 10.1186/s40560-023-00665-4
6. Celik T, Yilmaz MI, Balta S, Ozturk C, Unal HU, Aparci M, et al. The relationship between plasma whole blood viscosity and cardiovascular events in patients with chronic kidney disease. Clin Appl Thromb Hemost. (2017) 23(6):663–70. doi: 10.1177/1076029616634888
7. Carallo C, Irace C, De Franceschi MS, Coppoletta F, Tiriolo R, Scicchitano C, et al. The effect of aging on blood and plasma viscosity. An 11.6 years follow-up study. Clin Hemorheol Microcirc. (2011) 47(1):67–74. doi: 10.3233/CH-2010-1367
8. Muldoon MF, Herbert TB, Patterson SM, Kameneva M, Raible R, Manuck SB. Effects of acute psychological stress on serum lipid levels, hemoconcentration, and blood viscosity. Arch Intern Med. (1995) 155(6):615–20. doi: 10.1001/archinte.1995.00430060077009
9. Celik T, Balta S, Ozturk C, Iyisoy A. Whole blood viscosity and cardiovascular diseases: a forgotten old player of the game. Med Princ Pract. (2016) 25(5):499–500. doi: 10.1159/000446916
10. Tamariz LJ, Young JH, Pankow JS, Yeh H-C, Schmidt MI, Astor B, et al. Blood viscosity and hematocrit as risk factors for type 2 diabetes mellitus: the atherosclerosis risk in communities (ARIC) study. Am J Epidemiol. (2008) 168(10):1153–60. doi: 10.1093/aje/kwn243
11. Nwose EU, Butkowski EG. Algorithm for whole blood viscosity: implication for antiplatelet bleeding risk assessment. Austr J Med Sc. (2013) 34(2):50–5. doi: 10.3316/INFORMIT.426995725367787
12. Lane RJ. ‘Cardiogenic dementia’ revisited. J R Soc Med. (1991) 84(10):577–9. doi: 10.1177/014107689108401002
13. Iqbal AM, Lopez RA, Hai O. Antiplatelet medications. In: StatPearls. Treasure Island, FL: StatPearls Publishing (2022).
14. von Tempelhoff GF, Heilmann L, Pollow K, Hommel G. Monitoring of rheologic variables during postoperative high-dose brachytherapy for uterine cancer. Clin Appl Thromb Hemost. (2004) 10(3):239–48. doi: 10.1177/107602960401000306
15. Sercelik A, Besnili AF. The contribution of whole blood viscosity to the process of aortic valve sclerosis. Med Princ Pract. (2018) 27(2):173–8. doi: 10.1159/000487509
16. Jerome GJ, Goldsholl S, Dalcin AT, Gennusa Rd JV, Yuan CT, Brown K, et al. Comparing implementation strategies for an evidence-based weight management program delivered in community mental health programs: protocol for a pilot randomized controlled trial. JMIR Res Protoc. (2023) 12:e45802. doi: 10.2196/45802
17. Smith SM, Wallace E, O'Dowd T, Fortin M. Interventions for improving outcomes in patients with multimorbidity in primary care and community settings. Cochrane Database Syst Rev. (2016) 3(3):Cd006560. doi: 10.1002/14651858.CD006560.pub326976529
18. Azzopardi PS, Willenberg L, Wulan N, Devaera Y, Medise B, Riyanti A, et al. Direct assessment of mental health and metabolic syndrome amongst Indonesian adolescents: a study design for a mixed-methods study sampled from school and community settings. Glob Health Action. (2020) 13(1):1732665. doi: 10.1080/16549716.2020.1732665
19. Sun MJ. Jang MH: risk factors of metabolic syndrome in community-dwelling people with schizophrenia. Int J Environ Res Public Health. (2020) 17(18):6700. doi: 10.3390/ijerph17186700
20. Kalelioglu T, Kocabiyik M, Kok B, Unalan P, Sozen S, Yuksel O, et al. Does blood flow change according to mood? Blood rheology in bipolar disorder. Clin Psychopharmacol Neurosci. (2018) 16(3):310–5. doi: 10.9758/cpn.2018.16.3.310
Keywords: mental health, cardiovascular disease, pathology evaluation, routine laboratory indicators, evidence-base medicine, blood viscosity
Citation: Kyelu BA, Bwititi PT, Kauter K and Nwose EU (2025) Commentary: Heart–brain interaction in cardiogenic dementia: pathophysiology and therapeutic potential. Front. Cardiovasc. Med. 11:1479675. doi: 10.3389/fcvm.2024.1479675
Received: 12 August 2024; Accepted: 3 December 2024;
Published: 10 January 2025.
Edited by:
Leonardo Roever, Brazilian Evidence-Based Health Network, BrazilReviewed by:
Akhmetzhan Galimzhanov, Semey State Medical University, KazakhstanCopyright: © 2025 Kyelu, Bwititi, Kauter and Nwose. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Bupe Amon Kyelu, YnVwZS5reWVsdUB1bmlzcS5lZHUuYXU=