
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Cardiovasc. Med. , 03 September 2024
Sec. Hypertension
Volume 11 - 2024 | https://doi.org/10.3389/fcvm.2024.1449506
 Désirée Carmine1,2
Désirée Carmine1,2 Stefanie Aeschbacher1,2
Stefanie Aeschbacher1,2 Michael Coslovsky1,3
Michael Coslovsky1,3 Elisa Hennings1,2
Elisa Hennings1,2 Rebecca E. Paladini1,2
Rebecca E. Paladini1,2 Raffaele Peter1,2
Raffaele Peter1,2 Melanie Burger1,2
Melanie Burger1,2 Tobias Reichlin4
Tobias Reichlin4 Nicolas Rodondi5,6Andreas S. Müller7Peter Ammann8Giulio Conte9Angelo Auricchio9Giorgio Moschovitis9Julia B. Bardoczi5,6Annina Stauber7Maria Luisa De Perna9Christine S. Zuern1,2Tim Sinnecker10,11
Nicolas Rodondi5,6Andreas S. Müller7Peter Ammann8Giulio Conte9Angelo Auricchio9Giorgio Moschovitis9Julia B. Bardoczi5,6Annina Stauber7Maria Luisa De Perna9Christine S. Zuern1,2Tim Sinnecker10,11 Patrick Badertscher1,2
Patrick Badertscher1,2 Christian Sticherling1,2Leo H. Bonati12
Christian Sticherling1,2Leo H. Bonati12 David Conen13
David Conen13 Philipp Krisai1,2Stefan Osswald1,2
Philipp Krisai1,2Stefan Osswald1,2 Michael Kühne1,2* for the Swiss-AF Investigators
Michael Kühne1,2* for the Swiss-AF Investigators
Background: The influence of atrial fibrillation (AF) and blood pressure (BP) on brain lesions and cognitive function is unclear. We aimed to investigate the association of BP with different types of brain lesions and cognitive decline in patients with AF.
Methods: Overall, 1,213 AF patients underwent standardized brain magnetic resonance imaging at baseline and after 2 years, as well as yearly neurocognitive testing. BP was measured at baseline and categorized according to guidelines. New lesions were defined as new or enlarged brain lesions after 2 years. We defined cognitive decline using three different neurocognitive tests. Logistic and Cox regression analyses were performed to examine the associations of BP with new brain lesions and cognitive decline.
Results: The mean age was 71 ± 8.4 years, 74% were male and mean BP was 135 ± 18/79 ± 12 mmHg. New ischemic lesions and white matter lesions were found in 5.4% and 18.4%, respectively. After multivariable adjustment, BP was not associated with the presence of new brain lesions after 2 years. There was no association between BP and cognitive decline over a median follow-up of 6 years when using the Montreal Cognitive Assessment or Digit Symbol Substitution Test. However, BP categories were inversely associated with cognitive decline using the Semantic Fluency Test, with the strongest association in patients with hypertension grade 1 [Hazard Ratio (95% Confidence Interval) 0.57(0.42 to 0.77)], compared to patients with optimal BP (p for linear trend: 0.025).
Conclusions: In a large cohort of AF patients, there was no association between BP and incidence of brain lesions after 2 years. Also, there was no consistent association between BP and cognitive decline over a follow-up of 6 years.
Clinical Trial Registration: https://clinicaltrials.gov/study/NCT02105844, Identifier (NCT02105844).
The global number of individuals affected by atrial fibrillation (AF) and arterial hypertension is continuously increasing and is expected to further rise due to increasing life expectancy (1, 2). AF and hypertension often coexist. First, they are both associated with age (3, 4). Second, elevated blood pressure (BP) levels contribute to a higher risk of developing left ventricular hypertrophy and left atrial dilatation, which are predisposing conditions for AF (5, 6).
In comparison to the general population, patients with AF face an elevated risk of clinical stroke, covert brain lesions and dementia (7–11), which is responsible for years lived with disability and causes important costs to society (12, 13). Within the Swiss Atrial Fibrillation study (Swiss-AF), we identified a high prevalence of ischemic brain infarcts, white matter lesions (WML), and microbleeds (Mb) (11). Moreover, we demonstrated a relevant incidence of new brain lesions over a period of 2 years, despite a high rate of oral anticoagulation (14).
Hypertension, ischemic brain lesions, and WML have been shown to be associated with impaired cognitive function in the general population (15). In patients with AF, a cross-sectional analysis within the Swiss-AF study described an association between hypertension and the presence of different types of brain lesions, mainly WML (16).
A previous study, which is based on health insurance data, investigated time-updated BP levels and risk of dementia in midlife patients with AF and suggests that BP of 120–129/80–84 mm Hg might reduce the risk of dementia (17). Furthermore, they assume that lower BP might increase the risk of Alzheimer dementia, and higher BP might promote vascular dementia (17).
Considering the high burden of both AF and hypertension, and the increasing global prevalence of dementia (12), a better understanding of their association is of high relevance. We therefore aimed to investigate the influence of BP levels and hypertension on incidence, type, and volume of new brain lesions in AF patients after a 2-year follow-up. Furthermore, we aimed to evaluate the association between BP levels and cognitive decline over a follow-up period of up to 8 years.
This analysis was conducted using data from the ongoing, prospective, multicenter Swiss-AF study. Patients aged ≥65 years with documented AF were enrolled in 14 different centers across Switzerland between 2014 and 2017. Additionally, a smaller sample (10%) of patients aged between 45 and 65 years was also included to study socioeconomic aspects. The detailed study design was published previously (ClinicalTrials.gov: NCT02105844) (18). Exclusion criteria were the lack of a written informed consent, short transient forms of AF due to reversible causes (e.g., surgery or infection) and the presence of any acute disease in the previous month. At baseline, all patients had a personal visit at their respective study center. Yearly follow-up visits were done either personally or by phone. The Swiss-AF study follows the Declaration of Helsinki, and the protocol was accepted by the responsible ethics committees.
The patient selection process is presented in Figure 1. Of the 2,415 patients enrolled in the Swiss-AF study, 16 patients were excluded due to missing BP measurement at baseline. Additionally, we excluded 662 patients with missing brain MRI at baseline (mainly due to a cardiac device or claustrophobia), and 370 patients with a missing brain MRI after 2 years. Finally, we had to exclude 22 patients with incomplete baseline cognitive assessment, and 132 patients with no follow-up assessment of cognitive functions, resulting in 1,213 participants for the current analysis.
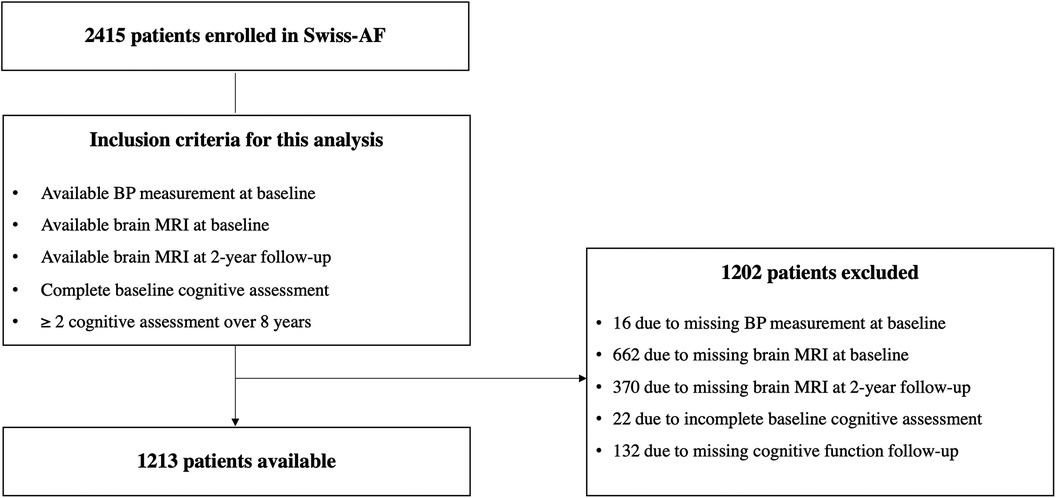
Figure 1. Flow chart patient enrollment. AF, atrial fibrillation; BP, blood pressure; MRI, magnetic resonance imaging.
At baseline and during yearly follow-up visits, we collected detailed information about patient characteristics, educational status, medication, and medical history. History of hypertension was self-reported and confirmed through medical reports. Study patients had to complete standardized case report forms, containing questions about eating habits, physical activity, and smoking status. Regular physical activity was defined as patients performing sports at least once a week. Additionally, the geriatric depression scale (GDS) (19) was administered. Weight and height were measured, and the body mass index (BMI) was calculated by dividing weight in kilograms by height in meters squared. We recorded a resting 12-lead surface electrocardiogram (ECG) for 5 min and the rhythm was determined by board-certified cardiologists. At baseline we took blood samples, and we measured the levels of total cholesterol, and low-density lipoprotein-cholesterol (LDL-C). We defined hypercholesterolemia as either a total cholesterol level ≥200 mg/dl (5.2 mmol/dl) and/or LDL-C ≥ 190 mg/dl (4.9 mmol/dl).
We measured BP with validated devices three times in sitting or supine position after a resting period of 5 min. We then calculated the mean of the three consecutive BP measurements. For these analyses, we categorized the BP values into BP categories, according to the current guidelines of the European Society of Hypertension (20) (Supplementary Table S1).
A standardized brain MRI was conducted at baseline and after 2 years of follow-up. Every participating study center performed pre-specified, standardized brain MRI protocols with either 1.5 or 3 Tesla scanners and without contrast agents. The images were first locally evaluated for incidental findings, and then centrally analyzed at the Medical Image Analyses Center (MIAC AG) in Basel, Switzerland. Blinded expert raters and board-certified neuroradiologists performed standardized analyses and ratings.
We performed fluid attenuated inversion recovery (FLAIR) and susceptibility-weighted images (SWI), as well as T2*-weighted imaging. Non-cortical infarcts were defined as lesions that do not involve the cortex and show hyperintensity on axial section on FLAIR sequences. If the lesions presented a diameter of ≤20 mm, they were classified as small non-cortical infarcts (SNCI), otherwise as large non-cortical infarcts (LNCI) (21). Lesions that involve the cortex and typically showing hyperintensity in FLAIR were defined as cortical infarcts. We combined large non-cortical infarcts and any cortical infarct into one category (LNCCI). Ischemic lesions were defined as either LNCCI and/or SNCI. We defined WML as hyperintense lesions in T2*-weighted and FLAIR involving the periventricular or deep white matter. We also described the presence of Mb as nodular lesions, with strong hypointense signal on T2*-weighted or SWI. A composite endpoint for microvascular damage was defined including the presence of WML, Mb or SNCI. New lesions were defined as either lesions that appeared between the baseline and the 2-year follow-up or pre-existing lesions from the baseline that demonstrated an increase in volume after 2 years.
Neurocognitive testing was performed on a yearly basis using the Montreal Cognitive Assessment (MoCA), the Semantic Fluency Test (SFT), and the Digit Symbol Substitution Test (DSST). The complete test battery was done at in-person visits. During phone visits, only the SFT was used. In brief, the MoCA test is a screening instrument for mild cognitive dysfunction and aims to assess the global cognitive function, including tests for executive functions, visuoconstructional skills, attention, and memory (22). The maximum and best score is 30 points, the worst 0 points. Patients reporting an education of <12 years receive an additional point if they reach <30 points. The SFT is a brief test that assesses verbal ability and executive control (23). During the test, patients are given 60 s to list as many words as possible belonging to a specific category, such as animals (23). The DSST is a widely used cognitive test that requires patients to match symbols to numbers within a 120-second timeframe, with a maximum achievable score of 135 points (24). Motor speed, attention, and visuoperceptual functions are crucial factors that significantly influence performance in this task (24). Our main outcome was cognitive decline defined as a change of more than −1 standard deviation (SD) of the age-education standardized baseline population of the MoCA test, SFT and DSST, compared with individual baseline levels (25, 26). A drop of 1 SD in the standardized scores is equivalent to 3 MoCA points, 5 SFT score units, and 12 DSST score units.
Continuous variables are presented as mean (±SD) or median [interquartile range (IQR)] and categorical variables as numbers (percentage). Continuous systolic BP (SBP), continuous diastolic BP (DBP), and BP categories were considered as the main predictor variables. New brain lesions (occurrence and volume) and cognitive function were stratified by BP categories and were compared using the appropriate test (Chi-square test or Kruskal-Wallis-Test).
To assess the association of continuous SBP, continuous DBP and BP categories with presence of new brain lesions, multivariable adjusted logistic regression analyses were performed using, in turn, new ischemic infarcts, WML, Mb and a composite (SNCI, Mb and WML) as the outcome variables. Linear regression analyses were done to assess the association of BP and BP categories with new lesions’ volume. To improve the normality of the distribution, the volume of the brain lesions was log-transformed. We calculated p for linear and quadratic trends, and we performed interaction analysis to examine potential effect modification of AF type (paroxysmal vs. non-paroxysmal) and baseline heart rhythm (AF and atrial flutter vs. sinus rhythm) on the association of BP with the incidence of new ischemic lesions and new WML.
All regression models were adjusted for potential confounders, pre-chosen based on expert knowledge. The first model was adjusted for sex and age. A second model was additionally adjusted for educational status, BMI, smoking status, previous stroke, or transient ischemic attack (TIA), history of diabetes, history of heart failure, history of coronary heart disease, AF type, oral anticoagulation, antithrombotic treatment, and antihypertensive treatment.
To assess the associations of continuous BP and BP categories with cognitive decline over a time period of up to 8 years, we performed multivariable adjusted Cox proportional hazard regression analyses. We used age-education adjusted standardized scores for all cognitive outcomes of interest. To determine person-years of follow-up, we measured the time from baseline to either cognitive decline, the last visit, or the last visit preceding study termination due to drop-outs, death, or loss to follow-up.
We adjusted the first model for sex, age, and educational status. The second model was additionally adjusted for GDS, BMI, smoking status, previous stroke or TIA, diabetes, heart failure, coronary heart disease, AF type, oral anticoagulation, antithrombotic treatment, and antihypertensive treatment.
Since loss of patients due to death may generate an attrition bias on the estimates, we conducted a sensitivity analysis by repeating the Cox regression analyses without patients who died during the course of the study. As additional sensitivity analysis, we reanalyzed the association of BP with cognitive decline, by using our dataset together with initially excluded patients due to missing MRI data (n = 2,124). Another sensitivity analysis was performed by adding regular physical activity and hypercholesterolemia as covariates (Model 3). Furthermore, to investigate the association of baseline BP with cognitive function scores as continuous variable, we performed mixed effects linear models. Time since the first measurement (random slope) and patient number nested within center (random intercepts) were added to both models. As fixed effects we included the same adjusting variables as described for models 1 and 2, alongside interaction terms between time and BP.
We considered a two-sided p-value <0.05 as statistically significant; no correction was done for multiple testing. All statistical analyses were performed using R version 4.2.2 (Foundation for Statistical Computing, Vienna, Austria).
Baseline characteristics are presented in Table 1 and a comparison of the final patient population with patients without complete MRI data is shown in Supplementary Table S2. Mean (SD) age of the 1,213 included patients was 71.4 (±8.4) years and 897 (73.9%) patients were male. Mean systolic/diastolic BP was 135/79 (±18/12) mmHg and mean CHA2DS2-VASc score was 3.1 (±1.7) points. Most patients were in sinus rhythm at the baseline visit (n = 673, 55.7%) and 46.7% (n = 567) had paroxysmal AF. A history of hypertension was reported by 821 (67.7%) patients, 792 (65.3%) were already on antihypertensive medication, and 47.1% required ≥3 antihypertensive drugs. Overall, 89.5% (n = 1,086) were prescribed oral anticoagulation, while 17.2% (n = 208) received antiplatelet therapy.

Table 1. Baseline characteristics.
When considering the measured BP at the baseline visit, 211 patients (17.4%) showed optimal BP (SBP <120 and DBP <80 mmHg), 249 (20.5%) normal BP (SBP 120–129 and/or DBP 80–84 mmHg), and 265 (21.8%) high normal BP levels (SBP 130–139 and/or DBP 85–89 mmHg). Most patients (n = 348, 28.7%) had hypertension grade 1 (SBP 140–159 and/or DBP 90–99 mmHg), and 140 (11.5%) patients had hypertension grade 2 or 3 (SBP ≥160 and/or DBP ≥100 mmHg).
At baseline, ischemic brain lesions were present in 428 (35.4%) patients, 1,195 (98.9%) patients had WML, and Mb were present in 238 (20.3%) patients. The overall median MoCA score was 26 [24, 28] points, the median SFT was 20 [16, 23] points, and the median DSST 47 [37, 56] points. The cognitive test scores did not differ among different BP categories (Supplementary Table S3).
The overall incidence of new ischemic lesions after 2-years follow-up was 5.4%, with a new median volume of 278 [116, 653] mm3. New or enlarged WML were present in 223 (18.4%) patients with a median volume of 108 [45, 284] mm3. Mb and the composite outcome of microvascular damage were present in 11.5% and 28% of patients, respectively (Table 2, Figure 2). There were no significant differences in the incidence or volume of brain lesions across the various BP categories.
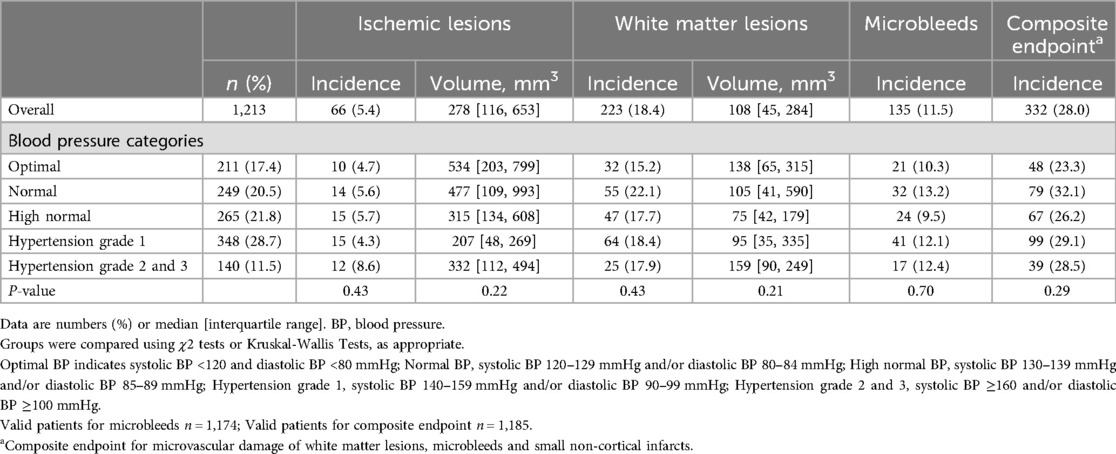
Table 2. Incidence and volume of new brain lesions on brain magnetic resonance imaging after 2 years of follow-up, overall and in blood pressure categories.
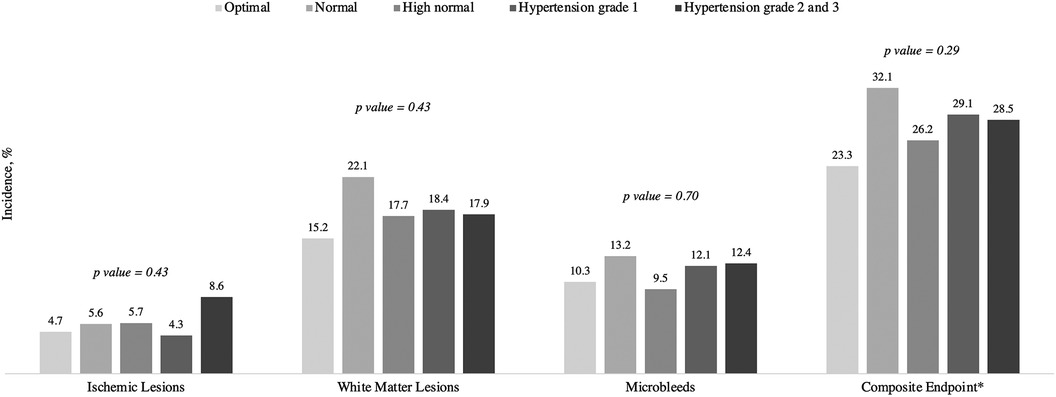
Figure 2. Incidence of new brain lesions by blood pressure categories. Data are %. P-value was calculated using the χ2 tests or Kruskal-Wallis Tests, as appropriate. *Composite endpoint for microvascular damage of white matter lesions, microbleeds and small non-cortical infarcts. BP, blood pressure. Optimal BP indicates systolic BP <120 and diastolic BP <80 mmHg; Normal BP, systolic BP 120–129 mmHg and/or diastolic BP 80–84 mmHg; High normal BP, systolic BP 130-139 mmHg and/or diastolic BP 85-89 mmHg; Hypertension grade 1, systolic BP 140-159 mmHg and/or diastolic BP 90-99 mmHg; Hypertension grade 2 and 3, systolic BP ≥160 and/or diastolic BP ≥100 mmHg.
The results of the association analyses between BP and different types of brain lesions are presented in Figure 3, Supplementary Tables S4, and S5. After adjusting for a comprehensive set of variables, the incidence and volume of ischemic lesions were not associated with BP categories. Per 10 mmHg increase in SBP and DBP the adjusted odds ratio (OR) [95% confidence interval (CI)] for new ischemic lesions were 1.10 (0.95–1.27; p = 0.21) and 1.23 (0.99–1.52, p = 0.06), respectively. The adjusted β-coefficients (95% CI) for the association of continuous SBP and DBP with the volume of ischemic lesions were 0.11 (−0.13 to 0.35, p = 0.37), and −0.01 (−0.34 to 0.32, p = 0.94).
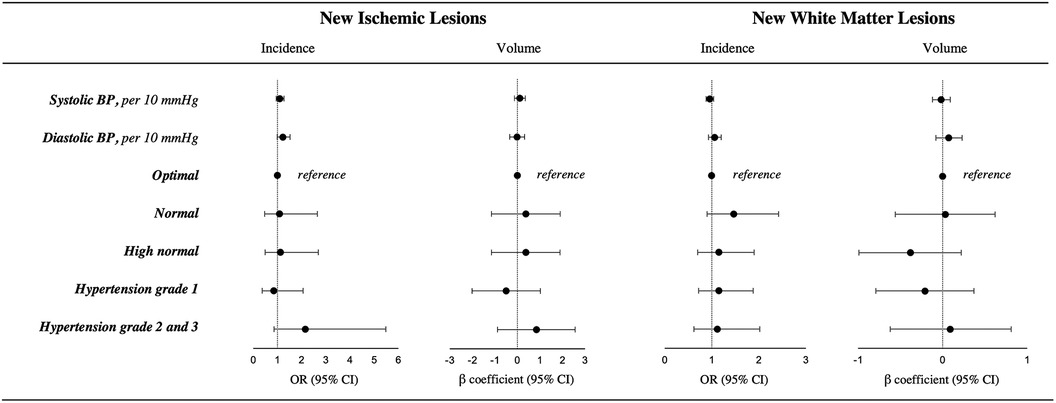
Figure 3. Results of the multivariable adjusted logistic and linear regression model of the association between blood pressure and the incidence and volume of new ischemic infarcts and new white matter lesions. Models are adjusted for age, sex, education, body mass index, smoking status, previous stroke or transient ischemic attack, history of diabetes, history of heart failure, history of coronary heart disease, atrial fibrillation type, oral anticoagulation, antithrombotic treatment, and antihypertensive treatment. BP, blood pressure; CI, confidence interval; and OR, odds ratio. Optimal BP indicates systolic BP <120 and diastolic BP <80 mmHg; Normal BP, systolic BP 120–129 mmHg and/or diastolic BP 80–84 mmHg; High normal BP, systolic BP 130–139 mmHg and/or diastolic BP 85–89 mmHg; Hypertension grade 1, systolic BP 140-159 mmHg and/or diastolic BP 90-99 mmHg; Hypertension grade 2 and 3, systolic BP ≥160 and/or diastolic BP ≥100 mmHg. Valid n for incidence for all patients = 1,213. Valid n for volume of new ischemic lesions = 66. Valid n for volume of new white matter lesions = 223.
When investigating the association of BP with the occurrence of new WML, there was no trend across BP categories (p for linear trend = 0.99, p for quadratic trend = 0.43). Per 10 mmHg increase in SBP and DBP the adjusted OR for incidence of WML were 0.96 (0.88 to 1.04; p = 0.32) and 1.06 (0.93 to 1.20, p = 0.40). Similarly, there was no association between BP and the volume of new WML. The results of the association of BP with new Mb and the composite outcome are presented in Supplementary Table S5 and Figure S1. None of the associations were significant.
Subgroup and interaction analyses of the association between SBP, ischemic lesions and WML are presented in Supplementary Table S6. AF type (paroxysmal vs. non-paroxysmal) and heart rhythm (AF and atrial flutter vs. sinus rhythm) did not show any interaction effect on the association between continuous SBP and the incidence of new ischemic lesions or WML.
The results of the association between BP and cognitive decline are presented in Table 3. The median follow-up time for the MoCA or DSST was 4 years and 6 years for the SFT. The incidence rate per 100 person years for cognitive decline was 2.50 when using the MoCA score, 6.20 for the SFT, and 2.31 for the DSST. Per 10 mmHg increase in SBP, the adjusted hazard ratio (HR) for cognitive decline was 0.94 (0.85–1.04, p = 0.23) using the MoCA score, 0.94 (0.89–1.00, p = 0.06) using the SFT, and 0.94 (0.84–1.05, p = 0.27) when using the DSST. Across increasing BP categories, we could not find any significant association between BP categories and cognitive decline using the MoCA Score (p for linear trend = 0.38, p for quadratic trend = 0.57) or using the DSST (p for linear trend = 0.52, p for quadratic trend = 0.99). However, using the SFT and considering optimal BP as reference, adjusted HR (95% CI) for cognitive impairment was 0.75 (0.55–1.03, p = 0.07) for normal BP, 0.63 (0.46–0.87, p = 0.005) for high normal BP, 0.57 (0.42–0.77, p < 0.001) for hypertension grade 1, and 0.72 (0.49–1.05, p = 0.09) for hypertension grade 2 and 3; with p for linear trend = 0.025 and p for quadratic trend = 0.020. The results of our sensitivity analysis excluding patients who died during the study period were consistent with the results of our main analysis (Supplementary Table S7).
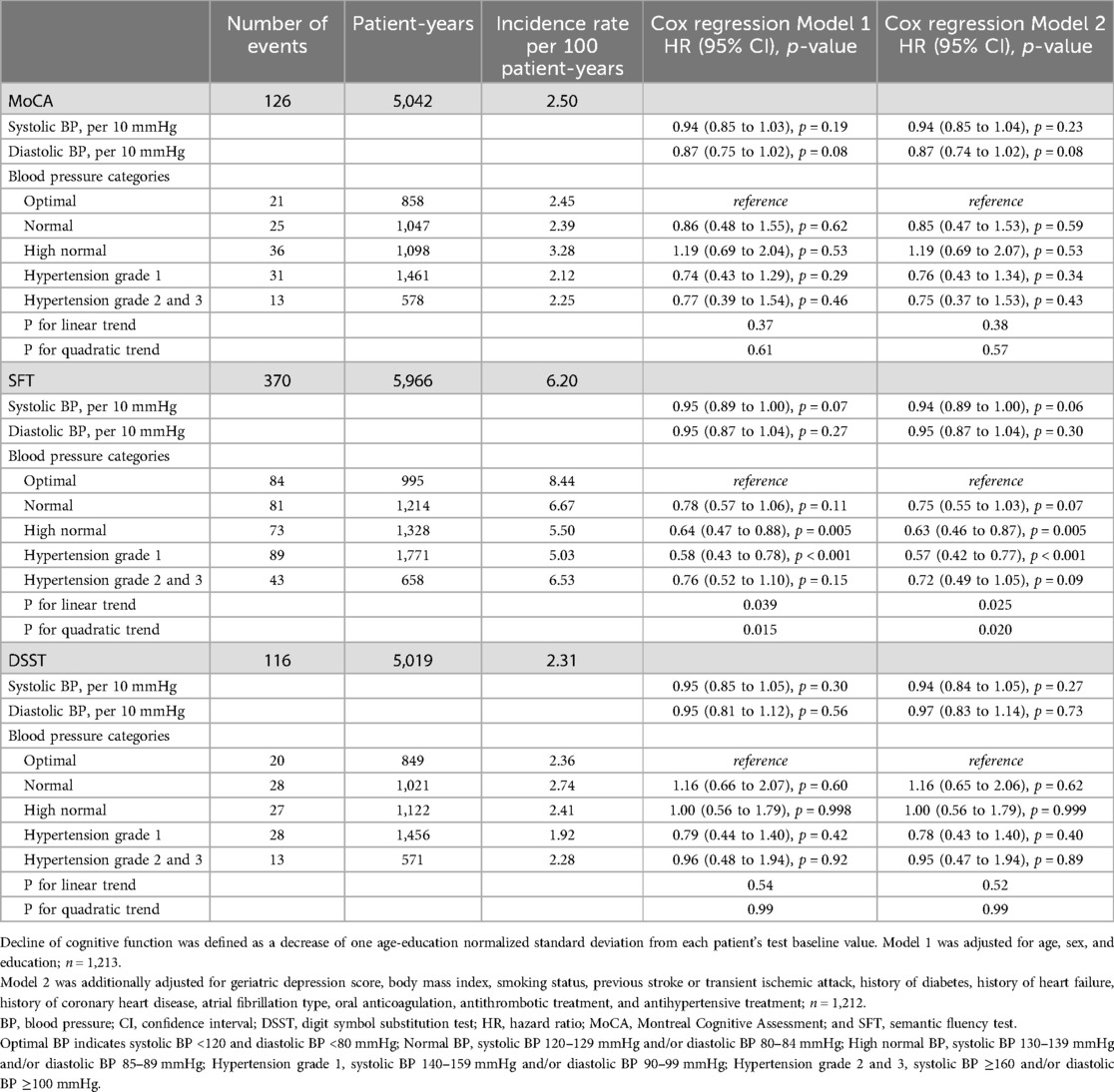
Table 3. Association of blood pressure and hypertension categories with new cognitive decline by using Cox regression analysis.
A sensitivity analysis of 2,124 patients, also including patients without MRI data, showed significant associations between continuous DBP and cognitive decline by using the MoCa score, as well as between continuous BP and BP categories with cognitive decline by using the SFT (Supplementary Table S8). The sensitivity analysis considering physical activity and hypercholesterolemia as possible confounders (Supplementary Table S9) showed consistent results to our main analysis. Results of the mixed effects linear models did not show any significant interactions between BP and time, thus do not support a change in cognition over time to depend on BP (Supplementary Table S10).
In this large cohort of AF patients, we investigated the associations of BP with new brain lesions after 2 years and cognitive decline over a time period of up to 8 years (median 6 years). The main findings are the following: first, nearly 68% of our patients had a prior history of hypertension at baseline. Second, after 2 years, there was no substantial association observed between BP and the occurrence and extent of new brain lesions on brain MRI. Third, BP was not consistently associated with cognitive decline during a median follow-up of 6 years.
Although we had observed a significant association between BP and brain lesions in a cross-sectional study (16), we found no strong evidence of an association between BP and new brain lesions after a mid-term follow-up of 2 years. Several factors might account for these findings. First, the limited number of ischemic and hemorrhagic events, potentially due to the high percentage of patients on oral anticoagulation and antihypertensive treatment (27–29). Second, considering the number of patients with pre-existing brain lesions at baseline, it is plausible that the observation period of 2 years might be insufficient to see relevant changes in the occurrence and volume of new lesions, despite high BP levels in some patients. Furthermore, the possible dynamic nature of brain lesions and the sensitivity of brain MRI warrants consideration, as it may have led to failure to detect brain lesions and subsequent underestimation of new lesions (30, 31). A longer term analysis may be able to uncover an association between BP levels and brain lesions, considering the potential rise in event rates over time. Moreover, it could enhance our understanding of how the impact of BP levels evolves over time (midlife vs. late-life) in patients with AF.
In our analysis, the association between BP and cognitive decline was inconsistent and depended on the type of cognitive test examined. We found some support for a possible association of cognitive decline in SFT with BP, but no evidence for this in the other two cognitive tests. The MoCa score is a relevant clinical screening tool to identify mild dementia and mild cognitive impairment (32). It includes the evaluation of executive function, visuospatial abilities, short-term and working memory, naming, language, attention, concentration, verbal abstraction, and orientation (22, 32). As the MoCa score covers various cognitive functions, it is a more global cognitive assessment tool. Thus, it might be possible that strengths in some functions can compensate weaknesses in others. This could result in a reduced event rate (compared to more specific cognitive assessments) and could potentially explain the lack of significant associations observed in our analysis.
The DSST has also been shown to measure various cognitive operations [such as attention, visuoperceptual functions, associative learning, working memory and motor speed (24)]. Though it is a useful and sensitive test to monitor cognitive dysfunction. However, it has a low specificity to identify which specific cognitive domain is affected (24) and a slight impairment in a specific cognitive function might be compensated by strengths in others. Such a compensation may be less likely in the SFT, as it assesses fewer cognitive functions [namely semantic memory and executive function (33, 34)]. However, considering the potential impact of the number of events and the larger sample size for the SFT on statistical power, it is not clear whether there is indeed a specific influence of BP on the SFT, or whether the differences compared to the other neurocognitive tests are real or a chance-finding.
Though the statistical significance level were not reached, the Cox regression analysis showed lower HRs in patients with higher BP (compared to patients with optimal BP), suggesting that increased BP levels may play an active role in the development of cognitive impairment. Recent findings in the general population are comparable with our data, possibly underlining the importance of maintaining an adequate level of DBP in patients affected with AF (35). Current literature suggests that cerebral perfusion might play a key role in cognitive function (36). Studies have shown a link between higher cerebral perfusion and better cognitive performance (37), as well as cerebral hypoperfusion with cognitive impairment (38). A history of coronary heart disease was reported by 25.7% of the patients, and 5.3% had peripheral artery disease. In our cohort of patients mainly over 65 years, arterial stiffness and vascular calcification was not systematically assessed, but may be present in a majority of patients. Considering that these conditions lead to impaired brain perfusion, the higher BP levels which may have contributed to vascular damages in midlife, may permit a sufficient and better perfusion, leading to better cognitive performance later (39, 40). A further possible explanation could be hidden behind the increased beat-to-beat variation in AF, which leads to intermittent cerebral hypoperfusion (41). The slightly elevated BP levels may permit the counteraction of the reduction in cerebral blood flow and maintain the perfusion more stable.
The findings of the cognitive tests could be influenced by the specific brain regions involved in each task. The SFT relies on areas like the temporal and frontal regions (particularly the prefrontal cortex), which are crucial for executive functions (42, 43). It is conceivable that patients with AF who are at higher risk for brain lesions, embolic events, and comorbidities (10, 44, 45), might benefit from slightly elevated BP levels, which improve blood flow in these regions. Advanced brain MRI protocols, which include the estimation of brain perfusion, could be helpful to better investigate this association in patients with AF.
Furthermore, several studies have underlined the importance of age, which may strongly influence the association between BP and cognitive function (39, 40, 46). BP levels and hypertension might have their greatest and negative influence on cognitive function during midlife (48–67 years) (47). Considering that our study population had a mean age of 72 years, and was mainly aged over 65 years, we may have missed the patient categories in which potential effects on neurocognitive function later in life might be significant.
For our analysis, we mainly focused on the BP measured at baseline, regardless of whether patients had diagnosed hypertension or if they were on antihypertensive therapy. However, the time point of the hypertension diagnosis, the persistence and a sufficient duration of high BP levels also play an important role in order to detect significant influence on cognitive function and cognitive decline (40).
The SPRINT (48) and the SPRINT-MIND (49) study provided important results regarding intensive BP control (target SBP of ≤120 mmHg) and the association with cardiovascular events, dementia and mild cognitive impairment (MCI). Compared to our analysis, the SPRINT-MIND study did not find any significant effects on incidence of dementia. However, they found benefits regarding the progression of WML and a lower risk of MCI. A post-hoc analysis in patients with AF showed a positive association of intensive BP treatment on the risk of dementia but no significant associations with MCI or probable dementia (50). In our study population, nearly 97% of patients with history of hypertension were on antihypertensive treatment. The question concerning the potential benefit of antihypertensive treatment and the best therapeutic goal for elderly AF patients with a high burden of cardiovascular disease thus remains unanswered. Considering the high prevalence of AF and the increasing rate of dementia, further study of this topic may be of relevant public interest.
The strengths of our study include the detailed information concerning patient characteristics and the large sample of AF patients with brain MRI data. We performed systematic and standardized brain MRI and cognitive assessment, which increases the reliability and comparability of the results over up to 8 years and across 14 centers in the three main language regions in Switzerland. However, certain limitations should be considered when interpreting the results. First, the generalizability of our results to other patient populations is unclear as we mainly included patients of European origin. Similarly, our findings are limited to patients who were able to undergo brain MRI. Second, the follow-up duration of 2 years for the MRI analysis and up to 8 years for the cognitive decline analysis might be too short and may represent a limitation of the analysis. Third, due to the limited number of patients with ischemic lesions after 2 years, we could not analyze LNCCI and SNCI separately. We combined them as ischemic infarcts instead. The merging of the two categories could have caused some noise, as these entities likely have different pathophysiological backgrounds (11, 21). The limited event rate may also affect the statistical power of our analyses. Finally, Swiss-AF is an observational study. Although potential confounders were included in our models as adjusting variables, residual confounding may have influenced our results.
In a well-characterized cohort of AF patients, we did not find compelling evidence for an association between BP and incidence or volume of new brain lesions after a follow-up of 2 years. The results of certain BP categories and a specific cognitive test indicate a potential risk reduction for cognitive decline; however, BP was not consistently associated with cognitive decline during a median follow-up of 6 years.
The data analyzed in this study is subject to the following licenses/restrictions: the datasets presented in this article are not publicly available due to restrictions by the Ethics Committee. Requests to access these datasets should be directed to Michael Kühne,bWljaGFlbC5rdWVobmVAdXNiLmNo.
The studies involving humans were approved by Ethics Committee Nordwest- und Zentralschweiz, Switzerland and all local Ethics Committees at the study sites. The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
DeC: Conceptualization, Formal Analysis, Methodology, Software, Validation, Visualization, Writing – original draft, Writing – review & editing. SA: Data curation, Formal Analysis, Project administration, Software, Writing – review & editing, Visualization. MC: Data curation, Methodology, Software, Writing – review & editing. EH: Conceptualization, Visualization, Writing – review & editing. REP: Data curation, Project administration, Writing – review & editing. RP: Conceptualization, Software, Writing – review & editing. MB: Writing – review & editing. TR: Writing – review & editing. NR: Writing – review & editing. ASM: Writing – review & editing. PA: Writing – review & editing. GC: Writing – review & editing. AA: Writing – review & editing. GM: Writing – review & editing. JBB: Writing – review & editing. AS: Writing – review & editing. MLDP: Writing – review & editing. CSZ: Writing – review & editing. TS: Writing – review & editing, Data curation, Investigation. PB: Writing – review & editing. CS: Writing – review & editing. LHB: Funding acquisition, Writing – review & editing. DC: Funding acquisition, Writing – review & editing. PK: Writing – review & editing. SO: Funding acquisition, Writing – review & editing. MK: Conceptualization, Funding acquisition, Methodology, Supervision, Visualization, Writing – original draft, Writing – review & editing.
The author(s) declare financial support was received for the research, authorship, and/or publication of this article. The Swiss-AF study is supported by grants of the Swiss National Science Foundation (grant numbers 33CS30_148474, 33CS30_177520, 32473B_176178, and 32003B_197524), the Swiss Heart Foundation, the Foundation for Cardiovascular Research Basel (FCVR), and the University of Basel.
AA has received consulting fees from Boston Scientific, Cairdac, EP Solutions, Medtronic, Philips, Radcliffe Publishers, and XSpline and payment or honoraria from Boston Scientific, Medtronic, Microport CRM, and Philips and has patents with Boston Scientific, Biosense Webster, and Microport CRM. ASM reports fellowship and training support from Biotronik, Boston Scientific, Medtronic, Abbott/St. Jude Medical, and Biosense Webster. Speaker honoraria from Biosense Webster, Medtronic, Abbott/St. Jude Medical, AstraZeneca, Daiichi Sankyo, Biotronik, MicroPort, Novartis. Consultant for Biosense Webster, Medtronic, Abbott/St. Jude Medical, and Biotronik (all outside of the current work). CS has received speaker honoraria from Biosense Webster and Medtronic and research grants from Biosense Webster, Daiichi Sankyo and Medtronic. CSZ reports a research grant from Medtronic and speaker fees from Vifor Pharma and Novartis. DC received speaker fees from Servier, and consulting fees from Roche Diagnostics and Trimedics, all outside of the current work. GC reports a research grant from the Swiss National Science Foundation, and research grants from Boston Scientific Inc. GM has received advisory board or speaker’s fees from Astra Zeneca, Bayer, Boehringer Ingelheim, Daiichi Sankyo, Gebro Pharma, Novartis and Vifor, all outside of the submitted work. LHB received grants from the Swiss National Science Foundation (PBBSB-116873, 33CM30-124119, 32003B-156658, 32003B-197524); Berne, Switzerland), The Swiss Heart Foundation (Berne, Switzerland, the University of Basel (Basel, Switzerland), and the “Stiftung zur Förderung der gastroenterologischen und allgemeinen klinischen Forschung sowie der medizinischen Bildauswertung” (Basel, Switzerland). LHB has received an unrestricted research grant from Astra Zeneca, and consultancy or advisory board fees or speaker’s honoraria from Amgen, Bayer, Bristol-Myers Squibb, and Claret Medical, and travel grants from AstraZeneca and Bayer. MK reports grants from the Swiss National Science Foundation (Grant numbers 33CS30_148474, 33CS30_177520, 32473B_176178, 32003B_197524), the Swiss Heart Foundation, the Foundation for Cardiovascular Research Basel and the University of Basel, grants from Bayer, grants from Pfizer, grants from Boston Scientific, grants from BMS, grants from Biotronik, grants and personal fees from Daiichi Sankyo. NR received a grant from the Swiss Heart Foundation. PK reports speaker fees BMS/Pfizer. Grants from the Swiss Heart Foundation, Foundation for Cardiovascular Research Basel, Machaon Foundation. SA received speaker fee from Roche Diagnostics. SO received grants from the Swiss National Science Foundation for Swiss-AF studies, research support from Roche (biomarker measurements), and is president of the Swiss Heart Foundation. TR has received research grants from the Swiss National Science Foundation, the Swiss Heart Foundation, the European Union [Eurostars 9799 – ALVALE), and the Cardiovascular Research Foundation Basel, all for work outside the submitted study. He has received speaker/consulting honoraria or travel support from Abbott/SJM, Astra Zeneca, Brahms, Bayer, Biosense-Webster, Biotronik, Boston-Scientific, Daiichi Sankyo, Medtronic, Pfizer-BMS, and Roche, all for work outside the submitted study. He has received support for his institution’s fellowship program from Abbott/SJM, Biosense-Webster, Biotronik, Boston-Scientific, and Medtronic, for work outside the submitted study.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The author(s) declared that they were an editorial board member of Frontiers, at the time of submission. This had no impact on the peer review process and the final decision.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fcvm.2024.1449506/full#supplementary-material
AF, atrial fibrillation; BMI, body mass index; BP, blood pressure; CI, confidence interval; DBP, diastolic blood pressure; DSST, digit symbol substitution test; ECG, electrocardiogram; FLAIR, fluid attenuated inversion recovery; GDS, geriatric depression scale; HR, hazard ratio; IQR, interquartile range; LDL-C, Low-density lipoprotein-cholesterol; LNCI, large non-cortical infarcts; LNCCI, large non-cortical infarcts and any cortical infarct; MAP, mean arterial pressure; Mb, microbleeds; MCI, mild cognitive impairment; MoCA, montreal cognitive assessment; MRI, magnetic resonance imaging; OR, odds ratio; OSAS, obstructive sleep apnea syndrome; SBP, systolic blood pressure; SD, standard deviation; SFT, semantic fluency test; SNCI, small non-cortical infarcts; SVD, small vessel disease; SWI, susceptibility-weighted images; Swiss-AF, swiss atrial fibrillation study; TIA, transient ischemic attack; WML, white matter lesions.
1. Krijthe BP, Kunst A, Benjamin EJ, Lip GYH, Franco OH, Hofman A, et al. Projections on the number of individuals with atrial fibrillation in the European Union, from 2000 to 2060. Eur Heart J. (2013) 34(35):2746–51. doi: 10.1093/eurheartj/eht280
2. Buford TW. Hypertension and aging. Ageing Res Rev. (2016) 26:96–111. doi: 10.1016/j.arr.2016.01.007
3. Unger T, Borghi C, Charchar F, Khan NA, Poulter NR, Prabhakaran D, et al. 2020 International Society of Hypertension Global Hypertension Practice Guidelines. Hypertension. (2020) 75(6):1334–57. doi: 10.1161/HYPERTENSIONAHA.120.15026
4. Middeldorp ME, Ariyaratnam JP, Kamsani SH, Albert CM, Sanders P. Hypertension and atrial fibrillation. J Hypertens. (2022) 40(12):2337–52. doi: 10.1097/HJH.0000000000003278
5. Kallistratos MS, Poulimenos LE, Manolis AJ. Atrial fibrillation and arterial hypertension. Pharmacol Res. (2018) 128:322–6. doi: 10.1016/j.phrs.2017.10.007
6. Benjamin EJ, Levy D, Vaziri SM, D'Agostino RB, Belanger AJ, Wolf PA, et al. Independent risk factors for atrial fibrillation in a population-based cohort: the Framingham Heart study. JAMA. (1994) 271(11):840–4. doi: 10.1001/jama.1994.03510350050036
7. Koh YH, Lew LZW, Franke KB, Elliott AD, Lau DH, Thiyagarajah A, et al. Predictive role of atrial fibrillation in cognitive decline: a systematic review and meta-analysis of 2.8 million individuals. Europace. (2022) 24(8):1229–39. doi: 10.1093/europace/euac003
8. Kalantarian S, Stern TA, Mansour M, Ruskin JN. Cognitive impairment associated with atrial fibrillation: a meta-analysis. Ann Intern Med. (2013) 158(5 Pt 1):338–46. doi: 10.7326/0003-4819-158-5-201303050-00007
9. Conen D, Chae CU, Glynn RJ, Tedrow UB, Everett BM, Buring JE, et al. Risk of death and cardiovascular events in initially healthy women with new-onset atrial fibrillation. JAMA. (2011) 305(20):2080–7. doi: 10.1001/jama.2011.659
10. Lubitz SA, Moser C, Sullivan L, Rienstra M, Fontes JD, Villalon ML, et al. Atrial fibrillation patterns and risks of subsequent stroke, heart failure, or death in the community. J Am Heart Assoc Cardiovasc Cerebrovasc Dis. (2013) 2(5):e000126. doi: 10.1161/JAHA.113.000126
11. Conen D, Rodondi N, Müller A, Beer JH, Ammann P, Moschovitis G, et al. Relationships of overt and silent brain lesions with cognitive function in patients with atrial fibrillation. J Am Coll Cardiol. (2019) 73(9):989–99. doi: 10.1016/j.jacc.2018.12.039
12. Prince M, Wimo A, Guerchet M, Ali GC, Wu YT, Prina M, et al. World Alzheimer Report 2015: the global impact of dementia: an analysis of prevalence, incidence, cost and trends. Alzheimer’s Disease International. (2015).
13. Gauthier S, Rosa-Neto P, Morais JA, Webster C. World Alzheimer Report 2021: journey through the diagnosis of dementia. Alzheimer’s Disease International. (2021). Available online at: https://www.alzint.org/resource/world-alzheimer-report-2021/ (cited August 5, 2023)
14. Kühne M, Krisai P, Coslovsky M, Rodondi N, Müller A, Beer JH, et al. Silent brain infarcts impact on cognitive function in atrial fibrillation. Eur Heart J. (2022) 43(22):2127–35. doi: 10.1093/eurheartj/ehac020
15. Levine DA, Galecki AT, Langa KM, Unverzagt FW, Kabeto MU, Giordani B, et al. Blood pressure and cognitive decline over 8 years in middle-aged and older black and white Americans. Hypertension. (2019) 73(2):310–8. doi: 10.1161/HYPERTENSIONAHA.118.12062
16. Aeschbacher S, Blum S, Meyre PB, Coslovsky M, Vischer AS, Sinnecker T, et al. Blood pressure and brain lesions in patients with atrial fibrillation. Hypertension. (2021) 77(2):662–71. doi: 10.1161/HYPERTENSIONAHA.120.16025
17. Kim D, Yang PS, Jang E, Tae Yu H, Kim TH, Uhm JS, et al. Blood pressure control and dementia risk in midlife patients with atrial fibrillation. Hypertension. (2020) 75(5):1296–304. doi: 10.1161/HYPERTENSIONAHA.119.14388
18. Conen D, Rodondi N, Mueller A, Beer J, Auricchio A, Ammann P, et al. Design of the Swiss atrial fibrillation cohort study (Swiss-AF): structural brain damage and cognitive decline among patients with atrial fibrillation. Swiss Med Wkly. (2017) 147:w14467. doi: 10.4414/smw.2017.14467
19. Yesavage JA, Brink TL, Rose TL, Lum O, Huang V, Adey M, et al. Development and validation of a geriatric depression screening scale: a preliminary report. J Psychiatr Res. (1982) 17(1):37–49. doi: 10.1016/0022-3956(82)90033-4
20. Mancia G, Kreutz R, Brunström M, Burnier M, Grassi G, Januszewicz A, et al. 2023 ESH guidelines for the management of arterial hypertension the task force for the management of arterial hypertension of the European Society of Hypertension: Endorsed by the International Society of Hypertension (ISH) and the European Renal Association (ERA). J Hypertens. (2023) 41(12):1874–2071. doi: 10.1097/HJH.0000000000003480
21. Wardlaw JM, Smith EE, Biessels GJ, Cordonnier C, Fazekas F, Frayne R, et al. Neuroimaging standards for research into small vessel disease and its contribution to ageing and neurodegeneration. Lancet Neurol. (2013) 12(8):822–38. doi: 10.1016/S1474-4422(13)70124-8
22. Nasreddine ZS, Phillips NA, Bédirian V, Charbonneau S, Whitehead V, Collin I, et al. The Montreal cognitive assessment, MoCA: a brief screening tool for mild cognitive impairment. J Am Geriatr Soc. (2005) 53(4):695–9. doi: 10.1111/j.1532-5415.2005.53221.x
23. Shao Z, Janse E, Visser K, Meyer AS. What do verbal fluency tasks measure? Predictors of verbal fluency performance in older adults. Front Psychol. (2014) 5:772. doi: 10.3389/fpsyg.2014.00772
24. Jaeger J Digit symbol substitution test: the case for sensitivity over specificity in neuropsychological testing. J Clin Psychopharmacol. (2018) 38(5):513–9. doi: 10.1097/JCP.0000000000000941
25. Palmer K, Fratiglioni L, Winblad B. What is mild cognitive impairment? Variations in definitions and evolution of nondemented persons with cognitive impairment. Acta Neurol Scand. (2003) 107:14–20. doi: 10.1034/j.1600-0404.107.s179.2.x
26. Wueest AS, Zuber P, Coslovsky M, Rommers N, Rodondi N, Gencer B, et al. Mid-term changes in cognitive functions in patients with atrial fibrillation: a longitudinal analysis of the Swiss-AF cohort. Front Cardiovasc Med. (2023) 10:1212587. doi: 10.3389/fcvm.2023.1212587
27. Hart RG, Pearce LA, Aguilar MI. Meta-analysis: antithrombotic therapy to prevent stroke in patients who have nonvalvular atrial fibrillation. Ann Intern Med. (2007) 146(12):857–67. doi: 10.7326/0003-4819-146-12-200706190-00007
28. Ruff CT, Giugliano RP, Braunwald E, Hoffman EB, Deenadayalu N, Ezekowitz MD, et al. Comparison of the efficacy and safety of new oral anticoagulants with warfarin in patients with atrial fibrillation: a meta-analysis of randomised trials. Lancet Lond Engl. (2014) 383(9921):955–62. doi: 10.1016/S0140-6736(13)62343-0
29. Sörös P, Whitehead S, Spence JD, Hachinski V. Antihypertensive treatment can prevent stroke and cognitive decline. Nat Rev Neurol. (2013) 9(3):174–8. doi: 10.1038/nrneurol.2012.255
30. Aben HP, Luijten L, Jansen BP, Visser-Meily JM, Spikman JM, Biessels GJ, et al. Absence of an infarct on MRI is not uncommon after clinical diagnosis of ischemic stroke. J Stroke Cerebrovasc Dis Off J Natl Stroke Assoc. (2020) 29(8):104979. doi: 10.1016/j.jstrokecerebrovasdis.2020.104979
31. Alberts MJ, Faulstich ME, Gray L. Stroke with negative brain magnetic resonance imaging. Stroke. (1992) 23(5):663–7. doi: 10.1161/01.STR.23.5.663
32. Dautzenberg G, Lijmer J, Beekman A. Diagnostic accuracy of the Montreal cognitive assessment (MoCA) for cognitive screening in old age psychiatry: determining cutoff scores in clinical practice. Avoiding spectrum bias caused by healthy controls. Int J Geriatr Psychiatry. (2020) 35(3):261–9. doi: 10.1002/gps.5227
33. Lopes M, Brucki SMD, Giampaoli V, Mansur LL. Semantic verbal fluency test in dementia: preliminary retrospective analysis. Dement Neuropsychol. (2009) 3(4):315–20. doi: 10.1590/S1980-57642009DN30400009
34. Oh SJ, Sung JE, Choi SJ, Jeong JH. Clustering and switching patterns in semantic fluency and their relationship to working memory in mild cognitive impairment. Dement Neurocognitive Disord. (2019) 18(2):47–61. doi: 10.12779/dnd.2019.18.2.47
35. Zhu Y, Li C, Gao D, Huang X, Zhang Y, Ji M, et al. Associations of blood pressure trajectories with subsequent cognitive decline, dementia and mortality. J Prev Alzheimers Dis. (2024). doi: 10.14283/jpad.2024.91
37. Leeuwis AE, Smith LA, Melbourne A, Hughes AD, Richards M, Prins ND, et al. Cerebral blood flow and cognitive functioning in a community-based, multi-ethnic cohort: the SABRE study. Front Aging Neurosci. (2018) 10:279. doi: 10.3389/fnagi.2018.00279
38. Wolters FJ, Zonneveld HI, Hofman A, van der Lugt A, Koudstaal PJ, Vernooij MW, et al. Cerebral perfusion and the risk of dementia: a population-based study. Circulation. (2017) 136(8):719–28. doi: 10.1161/CIRCULATIONAHA.117.027448
39. Qiu C, Winblad B, Fratiglioni L. The age-dependent relation of blood pressure to cognitive function and dementia. Lancet Neurol. (2005) 4(8):487–99. doi: 10.1016/S1474-4422(05)70141-1
40. Power MC, Tchetgen Tchetgen EJ, Sparrow D, Schwartz J, Weisskopf MG. Blood pressure and cognition:factors that may account for their inconsistent association. Epidemiol Camb Mass. (2013) 24(6):886–93. doi: 10.1097/EDE.0b013e3182a7121c
41. Gardarsdottir M, Sigurdsson S, Aspelund T, Rokita H, Launer LJ, Gudnason V, et al. Atrial fibrillation is associated with decreased total cerebral blood flow and brain perfusion. Europace. (2018) 20(8):1252–8. doi: 10.1093/europace/eux220
42. Biesbroek JM, van Zandvoort MJE, Kappelle LJ, Velthuis BK, Biessels GJ, Postma A. Shared and distinct anatomical correlates of semantic and phonemic fluency revealed by lesion-symptom mapping in patients with ischemic stroke. Brain Struct Funct. (2016) 221(4):2123–34. doi: 10.1007/s00429-015-1033-8
43. Baldo JV, Schwartz S, Wilkins D, Dronkers NF. Role of frontal versus temporal cortex in verbal fluency as revealed by voxel-based lesion symptom mapping. J Int Neuropsychol Soc. (2006) 12(6):896–900. doi: 10.1017/S1355617706061078
44. Hindricks G, Potpara T, Dagres N, Arbelo E, Bax JJ, Blomström-Lundqvist C, et al. 2020 ESC guidelines for the diagnosis and management of atrial fibrillation developed in collaboration with the European Association for Cardio-Thoracic Surgery (EACTS): the Task Force for the diagnosis and management of atrial fibrillation of the European Society of Cardiology (ESC) Developed with the special contribution of the European Heart Rhythm Association (EHRA) of the ESC. Eur Heart J. (2021) 42(5):373–498. doi: 10.1093/eurheartj/ehaa612
45. Frost L, Engholm G, Johnsen S, Møller H, Henneberg EW, Husted S. Incident thromboembolism in the aorta and the renal, mesenteric, pelvic, and extremity arteries after discharge from the hospital with a diagnosis of atrial fibrillation. Arch Intern Med. (2001) 161(2):272–6. doi: 10.1001/archinte.161.2.272
46. Forte G, De Pascalis V, Favieri F, Casagrande M. Effects of blood pressure on cognitive performance: a systematic review. J Clin Med. (2019) 9(1):34. doi: 10.3390/jcm9010034
47. Gottesman RF, Schneider ALC, Albert M, Alonso A, Bandeen-Roche K, Coker L, et al. Midlife hypertension and 20-year cognitive change: the atherosclerosis risk in communities neurocognitive study. JAMA Neurol. (2014 ) 71(10):1218–27. doi: 10.1001/jamaneurol.2014.1646
48. The SPRINT Research Group. A randomized trial of intensive versus standard blood-pressure control. N Engl J Med. (2015) 373(22):2103–16. doi: 10.1056/NEJMoa1511939
49. SPRINT MIND Investigators for the SPRINT Research Group; Williamson JD, Pajewski NM, Auchus AP, Bryan RN, Chelune G, Cheung AK, et al. Effect of intensive vs standard blood pressure control on probable dementia: a randomized clinical trial. JAMA. (2019) 321(6):553–61. doi: 10.1001/jama.2018.21442
Keywords: atrial fibrillation, blood pressure, hypertension, brain lesions, cognitive decline
Citation: Carmine D, Aeschbacher S, Coslovsky M, Hennings E, Paladini RE, Peter R, Burger M, Reichlin T, Rodondi N, Müller AS, Ammann P, Conte G, Auricchio A, Moschovitis G, Bardoczi JB, Stauber A, De Perna ML, Zuern CS, Sinnecker T, Badertscher P, Sticherling C, Bonati LH, Conen D, Krisai P, Osswald S and Kühne M (2024) Blood pressure, brain lesions and cognitive decline in patients with atrial fibrillation. Front. Cardiovasc. Med. 11:1449506. doi: 10.3389/fcvm.2024.1449506
Received: 15 June 2024; Accepted: 7 August 2024;
Published: 3 September 2024.
Edited by:
Elise Peery Gomez-Sanchez, University of Mississippi Medical Center, United StatesReviewed by:
Aadhavi Sridharan, Banner—University Medical Center Tucson, Banner Health, United StatesCopyright: © 2024 Carmine, Aeschbacher, Coslovsky, Hennings, Paladini, Peter, Burger, Reichlin, Rodondi, Müller, Ammann, Conte, Auricchio, Moschovitis, Bardoczi, Stauber, De Perna, Zuern, Sinnecker, Badertscher, Sticherling, Bonati, Conen, Krisai, Osswald and Kühne. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Michael Kühne, TWljaGFlbC5LdWVobmVAdXNiLmNo
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.