
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Cardiovasc. Med. , 23 July 2024
Sec. Coronary Artery Disease
Volume 11 - 2024 | https://doi.org/10.3389/fcvm.2024.1437096
 HongYa Han1
HongYa Han1 XiaoLi Liu1
XiaoLi Liu1 Qi Zhao2
Qi Zhao2 ZhiJian Wang1Yan Sun1
ZhiJian Wang1Yan Sun1 Xiaoteng Ma1
Xiaoteng Ma1 MengChen Li1HanYing Ma3YuYang Liu1DongMei Shi1
MengChen Li1HanYing Ma3YuYang Liu1DongMei Shi1 YuJing Cheng1*
YuJing Cheng1* YuJie Zhou1*
YuJie Zhou1*
Background: The atherogenic index of plasma (AIP) and hyperuricemia (HUA) have been shown to be closely associated with morbidity and mortality of coronary artery disease. However, studies targeting predictive value of AIP and HUA for chronic total occlusion (CTO) lesions are still lacking.
Methods: In total, 5,238 patients meeting the eligibility criteria were recruited in this analysis. CTO was defined as the condition of lesions without forward blood flow and with over three months of occlusion time. AIP was calculated as log10 [triglycerides (mmol/L)/high-density lipoprotein cholesterol (mmol/L)]. HUA was defined based on sex-specific criteria: serum uric acid 420 and 360 μmol/L for males and females, respectively.
Results: CTO lesions were presented in 907 (17.3%) patients. Compared with patients showing lower AIP levels and non-HUA, the CTO lesion risks increased by 5.225 and 2.765 times in patients with higher AIP levels and HUA. Patients with AIP >0.15 and HUA exhibited the greatest CTO incidence (odds ratio 11.491; 95% confidence interval 9.019–14.641, P < 0.001). In addition, AIP combined with HUA had significantly increased effects (a 38.5% increase in CTO risk) relative to the sum of respective effects.
Conclusion: Patients having higher AIP levels and HUA exhibited the highest CTO incidence, in comparison with patients who have the increased single index. AIP combined with HUA displayed significant synergistic effect on the prediction of CTO lesion.
Chronic total occlusion (CTO) is a serious lesion-type of coronary artery disease (CAD), referring to thrombolysis in myocardial infarction (TIMI) 0 flow and lasting at least 3 months (1). It has been shown that CTO occurs in approximately16%–20% of patients with CAD who undergo coronary angiography (CAG) (2, 3). Studies have indicated that percutaneous coronary intervention (PCI) for CTO is characterized by lower success rate, higher complication incidence, longer procedural duration, higher cost, and uncertain clinical benefit (4, 5). As a result, it is vital to identify the CTO-related risk factors and formulate targeted intervention measures for delaying the progression of coronary lesion to CTO, which can thus improve cardiovascular prognosis.
The atherogenic index of plasma (AIP), which is obtained based on lipid profiles including triglycerides (TG) and high-density lipoprotein cholesterol (HDL-C), has been considered to be the alternative and simple marker for plasma atherogenicity; this may be superior to the standard atherosclerotic lipid profiles (6–8). AIP has been indicated to be significantly related to the development, progression, and prognosis of CAD (9–13). The homeostasis of uric acid (UA) depends on its production, excretion, and reabsorption, and disruption of either process may cause hyperuricemia (HUA) (14). Recently, many studies have revealed that HUA is closely associated with the morbidity and mortality of CAD (15–18).
However, currently, studies targeting the predictive value of AIP and HUA for CTO lesions are relatively few. In addition, no previous research is been performed to explore how AIP combined with HUA predicts CTO lesions in patients with CAD patients. Therefore, this study was performed to explore the significance of AIP and HUA for predicting CTO lesions in patients with CAD, as well as further evaluating their synergistic effect on predictive performance.
The study consecutively enrolled totally 5,728 patients undergoing CAG in Beijing Anzhen Hospital from August 2018 to February 2019, approved by the Ethics Review Committee of the hospital (approval no. 2018027). Informed consent was obtained from all participants. The patients were presented anonymously. This study included the following patients: (1) those diagnosed with CAD; (2) with age ≤75 and ≥18 years; and (3) receiving CAG. The following patients were excluded: (1) those without basic feature data; (2) using urate-lowering medications; (3) with cardiogenic shock, acute decompensated heart failure, advanced cancer, or chronic infectious disorders; (4) with kidney dysfunction [estimated glomerular filtration rate (eGFR) <30 ml/(min 1.73 m2)] or undergoing kidney replacement; and (5) with severe liver dysfunction and having aspartate transaminase and/or alanine transaminase ≥5 times the corresponding upper reference limits. Finally, a total of 5,238 patients were enrolled in this study (Figure 1).
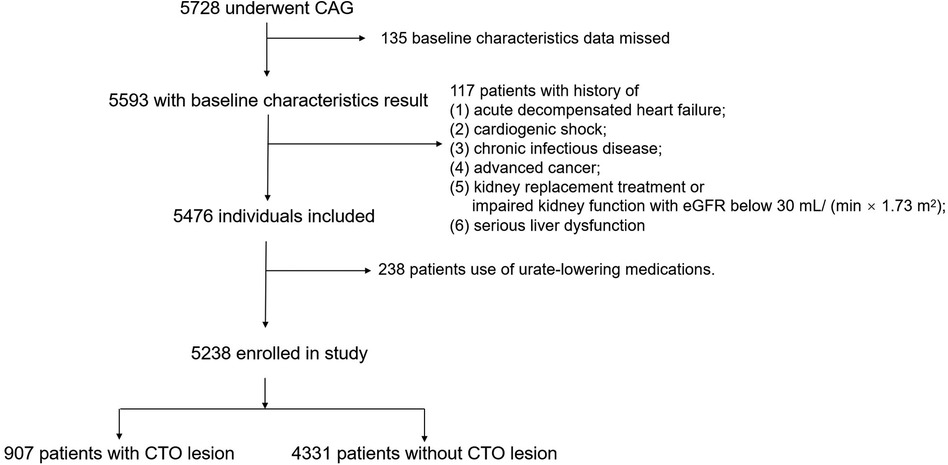
Figure 1 Flow of study participants.
After obtaining written informed consent from the patients, all demographic data and clinical information of the patents were obtained based on the hospital database. CTO lesions were judged by experienced cardiologists, with TIMI 0 forward blood flow of the occluded vessel segment, and with the occlusion lasting for over 3 months. Patients developing two to three-vessel disease were deemed to have multi-vessel disease, while patients developing ≥50% stenosis within the left main coronary artery were considered to have left main disease. The definition of hypertension was systolic blood pressure ≥140 mmHg and/or diastolic blood pressure ≥90 mmHg, or having antihypertensive medication. Diabetes mellitus can be defined as follows: (1) casual blood glucose ≥11.1 mmol/L, or (2) positive result of oral glucose tolerance test, or (3) fasting blood glucose ≥7.0 mmol/L. Smoking was deemed as cumulative (≥6 months) or continuous smoking during the lifetime, while hyperlipidemia as fasting total cholesterol (TC) > 5.17 mmol/L, TG > 1.69 mmol/L, HDL-C < 1.03 mmol/L, low-density lipoprotein cholesterol (LDL-C) > 3.36 mmol/L, and/or having lipid-lowering medication. HUA in adults was based on sex-specific criteria: serum uric acid ≥420 and 360 μmol/L for males and females, respectively. AIP was calculated according to TG and HDL-C: Log10 [TG (mmol/L)/HDL-C (mmol/L)].
The median of AIP (0.15) was taken as the optimum threshold based on AIP distribution. Basic patient data were depicted and analyzed following the optimum AIP threshold and diagnosis of HUA. Normally distributed continuous data were indicated by mean ± standard deviation (SD) and analyzed through the Student's t-test, as appropriate. Categorical data were indicated by number (percentage) and explored through chi-square tests.
The logistics regression was used to analyze the association of variables with CTO lesion. Three logistics regression models were constructed to evaluate the correlation between AIP/HUA and CTO lesion. Model 1 was adjusted for male gender and age. Variables of P < 0.05 upon univariate regression were incorporated into Model 2. Model 3 (the completely adjusted model) incorporated variables showing the univariate relation with adverse events or possible relation to clinical outcome, which included variables of Model 2 as well as age, smoking, and hypertension. To limit the impact of extreme observations, we standardized two interested variables to z score, a score indicating effect size of every unit SD increase. In addition, these two variables were incorporated into models as categorical variables according to median AIP (0.15) and sex-specific HUA criteria.
To evaluate the combined effect of AIP with HUA on predicting CTO lesion, patients were divided into four groups: AIP ≤ 0.15 and non-HUA (group 1), AIP > 0.15 and non-HUA (group 2), AIP ≤ 0.15 and HUA (group 3), or AIP > 0.15 and HUA (group 4). The completely adjusted logistic regression model was used to examine the combined effect on prediction. To explore the association of AIP with HUA, relative excess risk owing to interaction (RERI), synergy index (SI), and attributable proportion (AP) were determined. C-statistics, integrated discrimination improvement (IDI), and net reclassification improvement (NRI) were adopted for analyzing the synergistic prediction effect of AIP and HUA.
Table 1 displays basic patient characteristics that are classified according to median AIP. In total, this study enrolled totally 5,238 patients, among them, 75.4% were men (n = 3,947). Patients with higher AIP were younger and smoking, mostly men, and presented greater body mass index (BMI), heart rate, platelet, hemoglobin (HGB), glycosylated hemoglobin A1c (HbA1c), TC, LDL-C, and UA levels, but lower TG, HDL-C, and eGFR levels. There were more individuals who had acute coronary syndrome (ACS), multi-vessel disease, previous myocardial infarction (MI), PCI, diabetes mellitus, hyperlipidemia, hypertension, and received β-blocker and hypoglycemic therapy.

Table 1 Basic patient features based on AIP and UA level.
Patients were classified as HUA or non-HUA group (Table 1). Compared with the non-HUA subjects, HUA patients were younger, and presented greater BMI, TC, and AIP levels, with lower left ventricle ejection fraction (LVEF), HGB, HbA1c, and eGFR levels. In addition, there were more individuals who had previous MI, and diabetes mellitus, and were treated with aspirin, adenosine diphosphate (ADP) inhibitor, and hypoglycemic therapy.
In our study, CTO lesions were presented in 907 (17.3%) patients. The rate of CTO lesion was significantly higher in patients with higher AIP (P < 0.001). Patients with HUA had a significantly increased risk of CTO (P < 0.001) compared to those without HUA. Univariate logistics regression analysis showed that AIP and HUA were significantly associated with CTO lesion (Table 2). The predictive value of AIP and HUA remained significant after modifying for other cardiovascular risk factors (Table 3). Compared to patients with low levels of AIP and non-HUA, the risk of CTO lesion was 5.225 times higher for individuals with a high AIP and 2.765 times higher for individuals with HUA.
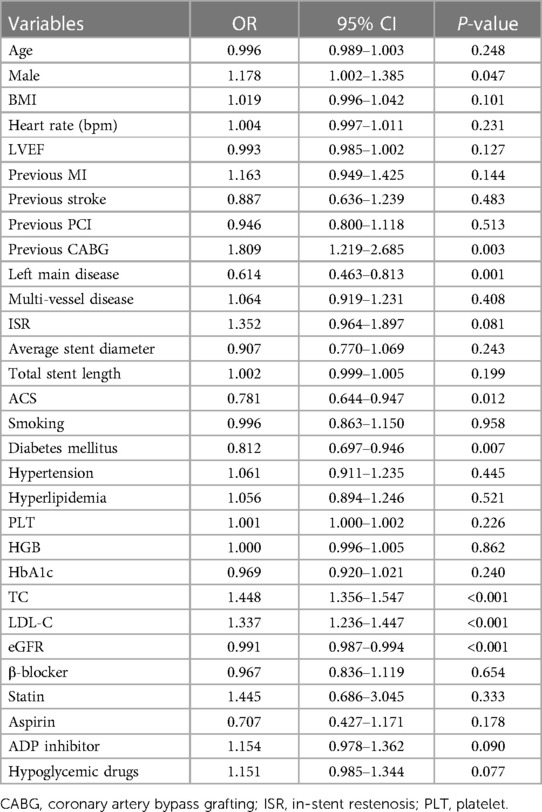
Table 2 Univariate logistics regression for CTO.
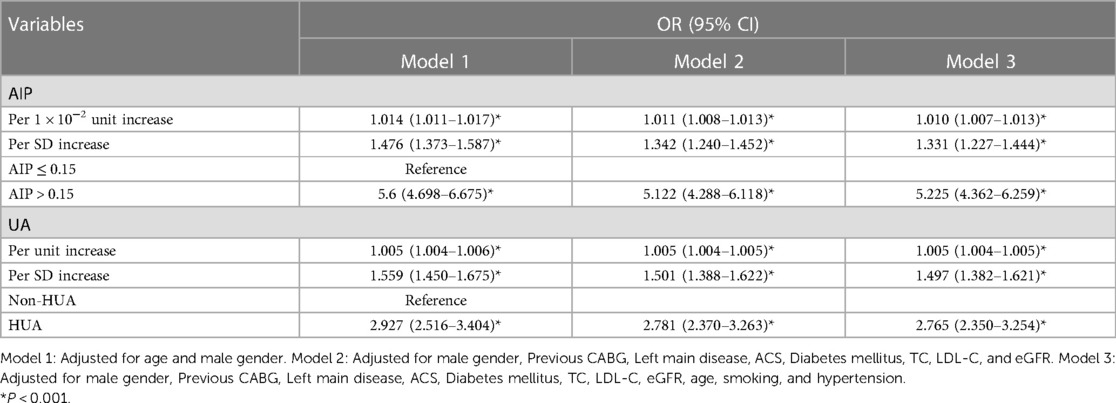
Table 3 Multivariate logistics regression for CTO.
All subjects were classified into one of four groups following median AIP and sex-specific HUA criteria. Logistics regression was performed to compare CTO lesion risk of the four groups (Table 4). Therefore, the greatest CTO lesion risk was determined in those having AIP > 0.15 and HUA, while the cumulative CTO lesion rate significantly decreased among patients having AIP ≤ 0.15 and without HUA (P < 0.001). The pooled significance of AIP and HUA for predicting CTO was confirmed through multivariate logistics regression. CTO risk was the highest in those having AIP > 0.15 and HUA [odds ratio (OR) = 11.491; 95% confidence interval (CI) 9.019–14.641, P < 0.001]. The adjusted OR for CTO was 1.938 (95% CI 1.373–2.735) in patients with AIP ≤ 0.15 and non-HUA, relative to patients of Group 1 (Table 4).
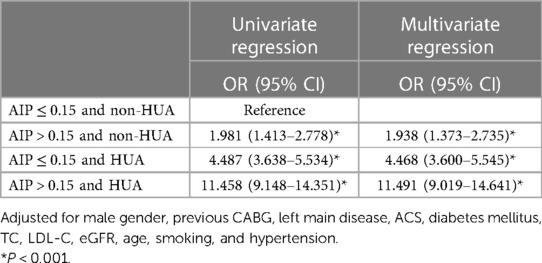
Table 4 Pooled effect of AIP and HUA on CTO.
Subgroup analyses stratified by age, sex, BMI, smoking, hypertension, diabetes mellitus, and hyperlipidemia were performed. Figure 2 presents the pooled relation between AIP/HUA and CTO lesion in different subgroups. In general, patients having higher AIP levels and HUA were significantly associated with CTO lesion, in all subgroups (Figure 2).
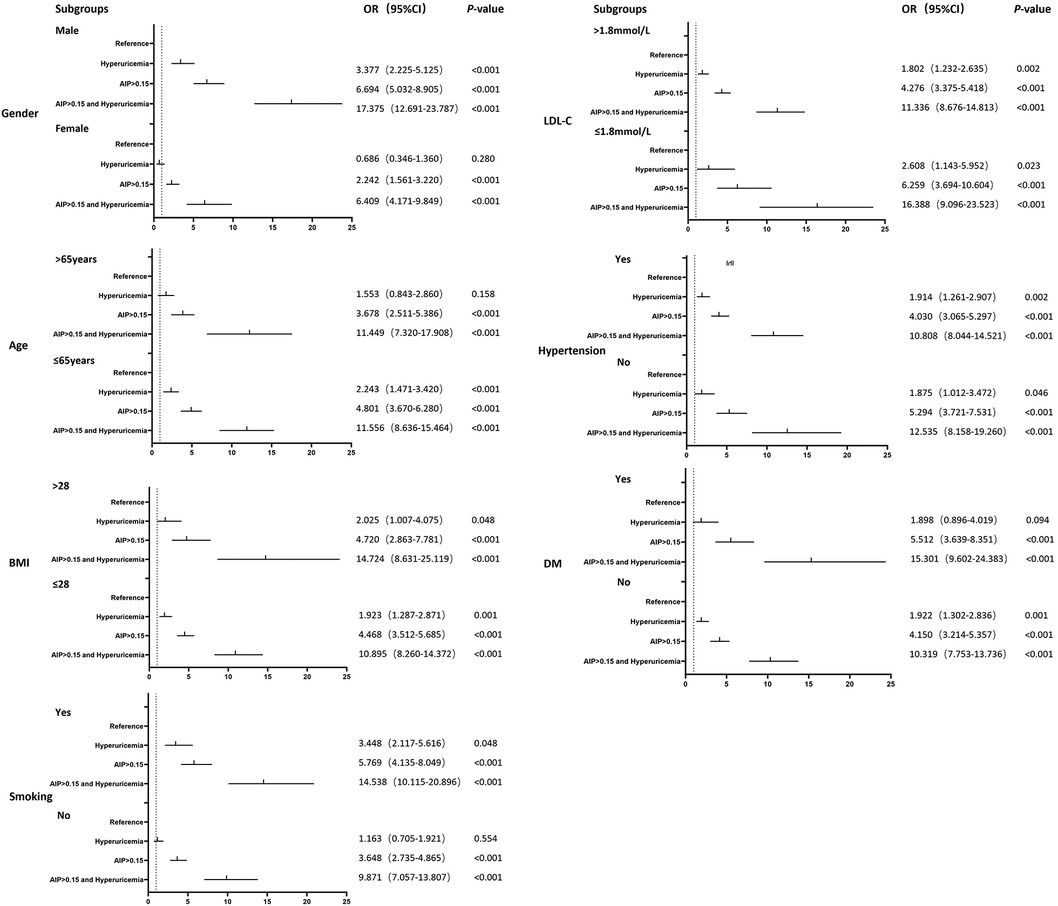
Figure 2 Subgroup analysis.
Based on interaction analysis, the pooled effect of AIP with HUA significantly increased relative to the respective single effects, with the CTO risk being increased by 38.5% (Table 5).
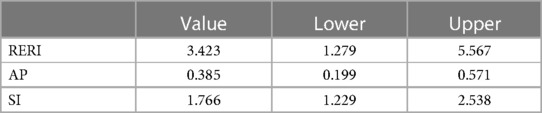
Table 5 Synergistic relation of AIP with HUA.
Based on C-statistic, continuous NRI, and IDI, adding AIP or HUA into the baseline model moderately but significantly improved the prediction effect. Afterward, both AIP and HUA were added into the baseline model to maximally improve model prediction. The addition of AIP and HUA markedly enhanced the discrimination and reclassification performance of the baseline model, with the category-free NRI and IDI being 0.411 and 0.027, respectively (P < 0.001) (Table 6).
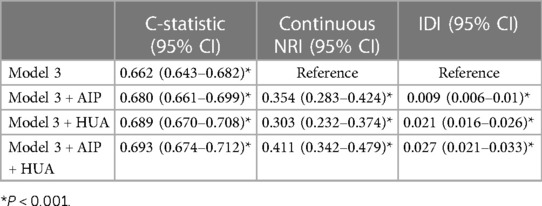
Table 6 C-statistic NRI and IDI for prediction significance of diverse models.
Recently, a novel cut-off value of hyperuricemia has been described that had a better relationship with cardiovascular diseases. The Uric acid Right for heArt Health (URRAH) study, a cross-sectional analysis including 26,971 individuals, had found a cut-off of 5.1 mg/dl for women and 5.6 mg/dl for men (19).
We made further analysis based on these criteria. Patients were also classified into the HUA or non-HUA group (Supplementary Table S1). Compared with non-HUA subjects, patients with HUA were mostly men, younger and smoking, and presented greater BMI, TG, HDL-C, AIP levels and average stent diameter, but lower LVEF, HGB, HbA1c, and eGFR levels. In addition, there were more individuals who had previous MI, diabetes mellitus, and hypertension, and were treated with hypoglycemic therapy.
Compared to patients with non-HUA, the risk of CTO lesion was 1.545 times higher for individuals with HUA (Supplementary Table S2). Patients were classified into one of four groups following median AIP and novel HUA criteria. CTO risk was the highest in those having AIP > 0.15 and HUA (OR = 5.882; 95% CI 4.581–7.552, P < 0.001) (Supplementary Table S3). The odds ratio was lower than the classic criteria. In subgroup analyses, patients with higher AIP levels and HUA were also significantly associated with CTO lesion, in all subgroups (Supplementary Figure S1).
Based on interaction analysis, the pooled effect of AIP with HUA increased relative to the respective single effects, with the CTO risk being increased by 34.9% (Supplementary Table S4), which was similar to that of the classic criteria. The category-free NRI and IDI had values of 0.750 and 0.073, respectively (P < 0.001), which had better improvement on the prediction effect.
The novel HUA cut-off showed excellent predictive value and is worth further exploration in future studies.
Our major results include the following: (1) Both high AIP and HUA showed significant independent association with CTO lesion. (2) Patients having high AIP levels and HUA exhibited the highest CTO risk in relation to an increased single index, no matter the subgroup. (3) The pooled effect of AIP with HUA significantly increased relative to the sum of the respective single effects. (4) The addition of AIP and HUA to the baseline model maximally improved risk prediction for CTO.
CTO lesions are mainly characterized by complete occlusion (TIMI flow grade 0) and duration greater than 3 months (1). Recently, the CTO lesion recanalization success rate through PCI steadily increased with the growth of operator experience, technological advancement, and technical development. However, the overall success rate of CTO lesion recanalization through PCI is low (20, 21). In addition, it was also shown that CTO-related PCI is associated with higher risk of complications including perforation, side branch occlusion, and myocardial infarction, when compared with PCI performed in non-CTO lesions (21–24). CTO-related PCI often takes a long time to operate on, which inevitably causes higher radiation doses for both the patient and the operator (25). Moreover, since CTO-related PCI procedures require more advanced consumables and auxiliary means (such as intravascular ultrasound, and optical coherence tomography), the cost is inevitably higher (5). More importantly, whether invasive strategies for CTO lesions can improve outcomes in patients with CAD is controversial (26–29). One recent meta-analysis including randomized controlled trials that compared the therapeutic effects of PCI with the optimal medical therapy alone demonstrated that CTO-related PCI did not improve long-time prognosis of patients with CAD (30).
Considering the lower success rate, higher complication incidence, longer procedural duration, higher cost, and uncertain clinical benefit, identifying the risk factors for CTO lesions and formulating targeted interventions as early as possible plays a crucial role in delaying the progression of coronary lesion to CTO and improving the prognosis of patients with CAD.
AIP, which is simply calculated from common lipid profiles including TG and HDL-C, is proposed to be the novel risk predictor of the development, progression, and prognosis of CAD. According to a case-control study from Cai et al. (11), it was concluded that AIP is closely related to CAD, indicating that it may be a useful risk predictor for CAD. According to the results from the Indian Atherosclerosis Research Study (31), the addition of family history and AIP into conventional cardiovascular risk factors improved risk discrimination for CAD (C-index: 0.864–0.873). Previous studies indicated a significant relationship of AIP with the progression of atheroma volume and coronary artery calcification determined with multi-detector computed tomography for participants free of cardiovascular disease at baseline (6, 32). Previous studies also revealed that there was a positive correlation between AIP and the synergy between PCI with taxus and cardiac surgery (SYNTAX) score (33). In a prospective cohort study including 2,676 middle-aged adults with a median follow-up of 7.8 years, when conventional risk factors were adjusted, an increase in AIP was a significant predictor of CAD development (10). The study of Qin et al. (13) further investigated the role of AIP in predicting adverse cardiovascular outcomes among patients with CAD, and the results showed that the increase of AIP showed significant relation to the higher incidence of major adverse cardiovascular/cerebrovascular events.
The relationship of HUA with the CAD morbidity and mortality is also well elucidated in previous studies. Niskanen et al. (34) prospectively recruited totally 1,423 middle-aged men initially free of cardiovascular disease and followed them for 11.9 years. The results demonstrated that HUA strongly predicted cardiovascular mortality among normal middle-aged men, regardless of other risk factors. In addition, another large-scale epidemiological study involving participants aged 25–74 years with an average of 16.4 years’ follow-up also indicated that HUA was significantly and independently associated with cardiovascular mortality risk (35). In addition, previous studies also demonstrated that HUA was significantly and independently related to 30-day and long-term mortality after acute myocardial infarction, and closely correlated with Killip class (36). The predictive value of HUA for the morbidity and mortality of CAD has been also verified by various meta-analyses (15–17). Even so, not all the studies on the relationship between HUA and CAD show a significant association. Previous studies found the absence of a role for HUA in determining CAD as well as left ventricular diastolic dysfunction, which indicated that HUA could act on the heart in an early phase of the disease, whereas other factors were involved in the advanced stages (37). This finding suggested that the question of how HUA impacts the progression of disease is worth further investigation.
Currently, studies targeting the predictive value of AIP and HUA for CTO lesions are few. Our study fills in the gaps of previous research, since it first revealed the significant association between AIP and HUA and the presence of CTO lesions. Then, it further provided the important evidence supporting the synergy of AIP with HUA for the prediction of CTO lesion risk.
AIP is suggested to show a positive relationship with serum malondialdehyde contents that reflect oxidative stress, and the latter is significantly related to coronary atherosclerosis (38). In addition, AIP is closely associated with epicardial adipose tissue (39), which has been shown to directly influence the progression of coronary atherosclerosis (40). AIP has also been demonstrated to exhibit direct and independent association with decreased arterial stiffness (41) and coronary flow reserve (42), both of which are vital risk factors inducing atherosclerosis. In addition, certain studies have indicated that HUA can enhance atherosclerosis development through inflammation, endothelial dysfunction, vascular smooth muscle cell proliferation, oxidative stress, and renin-angiotensin-aldosterone system activation (43–46). The above-mentioned factors may be important potential mechanisms that can mediate the atherogenic effect of AIP and HUA.
Previous studies have indicated that AIP is significantly related to various CAD-related risk factors including obesity, diabetes mellitus, and hypertension (10, 47, 48). The association of HUA with hypertension and metabolic syndrome was also verified by previous studies (49, 50). This may be another potential mechanism that can lead to atherosclerosis progression in response to AIP and HUA.
This study found a significant synergistic effect of AIP and HUA in predicting CTO lesions. The synergistic effect may be explained by insulin resistance. It has also been illustrated that insulin resistance is mainly characterized as hyperglycemia, hyperinsulinemia, central obesity, and dyslipidemia, particularly the elevated fasting TG and reduced HDL-C. Therefore, AIP, which is determined based on TG and HDL-C, indicates the level of insulin resistance to some extent. Insulin resistance can decrease UA excretion while promoting UA reabsorption. In addition, HUA exerts adverse influence on glucose absorption into skeletal muscle, and mediates oxidative alterations of adipocytes, resulting in insulin resistance (43, 44). They reinforce each other mutually, finally contributing to atherosclerosis development.
However, this study still has the following limitations. First, this is a single-center, retrospective observational study. The validation and generalizability of the findings in this cohort should be carried out based on independent validation samples. Second, all the subjects included in this study were Chinese. The model was created only from the patients who underwent coronary angiography and the severity of CTO was not recorded, probably causing selection bias. Third, despite the fact that subjects receiving urate-lowering drugs were excluded, medications including statins and hypoglycemic agents may have potential influences on evaluating AIP and UA. As is well known, diuretics have a significant impact on UA levels. The database in this study does not provide detailed records of diuretic use, which may have effect on the results. Although a previous study has shown that diuretic-related hyperuricemia carries a similar risk of cardiovascular events and all-cause mortality compared with patients with hyperuricemia in the absence of diuretic therapy (51), it is still unclear whether this result is applicable to the study with CTO lesions as the outcome. Additional data are required, and further research is necessary. Finally, dynamic changes from continuous monitoring of AIP and UA may provide more valuable information, but these were not covered in our study.
To conclude, both higher AIP and HUA are significantly related to CTO lesion. Patients who have higher AIP and HUA exhibit the highest CTO risk in comparison with those having an increased single index. AIP and HUA display a significant synergistic effect on predicting CTO lesions.
The original contributions presented in the study are included in the article/Supplementary Material, further inquiries can be directed to the corresponding authors.
The studies involving humans were approved by the Clinical Research Ethics Committee of Beijing Anzhen Hospital, Capital Medical University. The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
HH: Data curation, Investigation, Supervision, Writing – original draft, Writing – review & editing, Funding acquisition. XL: Data curation, Resources, Supervision, Writing – review & editing, Methodology. QZ: Data curation, Writing – review & editing. ZW: Data curation, Writing – review & editing, Methodology. YS: Data curation, Writing – review & editing. XM: Data curation, Writing – review & editing. ML: Data curation, Writing – review & editing. HM: Data curation, Writing – review & editing. YL: Data curation, Writing – review & editing. DS: Data curation, Writing – review & editing. YC: Data curation, Formal Analysis, Investigation, Project administration, Resources, Visualization, Methodology, Writing – review & editing. YZ: Data curation, Formal Analysis, Funding acquisition, Investigation, Project administration, Resources, Visualization, Methodology, Writing – review & editing.
The authors declare financial support was received for the research, authorship, and/or publication of this article.
This work was funded by the grant from National Key Research and Development Program of China (2022YFC3602500) and Beijing High-level Public Health Technical Talents Construction Project (Backbone-02-01; Academic leader-03-24; Academic leader-2022-2-008).
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fcvm.2024.1437096/full#supplementary-material
Supplementary Figure S1
Subgroup analysis.
CTO, chronic total occlusion; CAD, coronary artery disease; AIP, atherogenic index of plasma; HUA, hyperuricemia; TIMI, thrombolysis in myocardial infarction; TG, triglyceride; HDL-C, high-density lipoprotein cholesterol; SD, standard deviation; TC, total cholesterol; LDL-C, low-density lipoprotein cholesterol; UA, uric acid; PCI, percutaneous coronary intervention; BMI, body mass index; HGB, hemoglobin; HbA1c, glycosylated hemoglobin A1c; eGFR, estimated glomerular filtration rate; MI, myocardial infarction; OR, odds ratio; CI, confidence interval; NRI, net reclassification improvement; IDI, integrated discrimination improvement; SYNTAX, the synergy between PCI with taxus and cardiac surgery.
1. Brilakis ES, Mashayekhi K, Tsuchikane E, Abi Rafeh N, Alaswad K, Araya M, et al. Guiding principles for chronic total occlusion percutaneous coronary intervention: a global expert consensus document. Circulation. (2019) 140(5):420–33. doi: 10.1161/CIRCULATIONAHA.119.039797
2. Fefer P, Knudtson ML, Cheema AN, Galbraith PD, Osherov AB, Yalonetsky S, et al. Current perspectives on coronary chronic total occlusions: the Canadian multicenter chronic total occlusions registry. J Am Coll Cardiol. (2012) 59(11):991–7. doi: 10.1016/j.jacc.2011.12.007
3. Azzalini L, Jolicoeur EM, Pighi M, Millan X, Picard F, Tadros VX, et al. Epidemiology, management strategies, and outcomes of patients with chronic total coronary occlusion. Am J Cardiol. (2016) 118(8):1128–35. doi: 10.1016/j.amjcard.2016.07.023
4. Tajti P, Burke MN, Karmpaliotis D, Alaswad K, Werner GS, Azzalini L, et al. Update in the percutaneous management of coronary chronic total occlusions. JACC Cardiovasc Interv. (2018) 11(7):615–25. doi: 10.1016/j.jcin.2017.10.052
5. Azzalini L, Karmpaliotis D, Santiago R, Mashayekhi K, Di Mario C, Rinfret S, et al. Contemporary issues in chronic total occlusion percutaneous coronary intervention. JACC Cardiovasc Interv. (2022) 15(1):1–21. doi: 10.1016/j.jcin.2021.09.027
6. Won K-B, Heo R, Park H-B, Lee BK, Lin FY, Hadamitzky M, et al. Atherogenic index of plasma and the risk of rapid progression of coronary atherosclerosis beyond traditional risk factors. Atherosclerosis. (2021) 324:46–51. doi: 10.1016/j.atherosclerosis.2021.03.009
7. Dobiasova M, Frohlich J. The new atherogenic plasma index reflects the triglyceride and HDL-cholesterol ratio, the lipoprotein particle size and the cholesterol esterification rate: changes during Lipanor therapy. Vnitr Lek. (2000) 46(3):152–6.11048517
8. Quispe R, Manalac RJ, Faridi KF, Blaha MJ, Toth PP, Kulkarni KR, et al. Relationship of the triglyceride to high-density lipoprotein cholesterol (TG/HDL-C) ratio to the remainder of the lipid profile: the very large database of lipids-4 (VLDL-4) study. Atherosclerosis. (2015) 242(1):243–50. doi: 10.1016/j.atherosclerosis.2015.06.057
9. Frohlich J, Dobiasova M. Fractional esterification rate of cholesterol and ratio of triglycerides to HDL-cholesterol are powerful predictors of positive findings on coronary angiography. Clin Chem. (2003) 49(11):1873–80. doi: 10.1373/clinchem.2003.022558
10. Onat A, Can G, Kaya H, Hergenç G. “Atherogenic index of plasma” (log10 triglyceride/high-density lipoprotein−cholesterol) predicts high blood pressure, diabetes, and vascular events. J Clin Lipidol. (2010) 4(2):89–98. doi: 10.1016/j.jacl.2010.02.005
11. Cai G, Shi G, Xue S, Lu W. The atherogenic index of plasma is a strong and independent predictor for coronary artery disease in the Chinese Han population. Medicine (Baltimore). (2017) 96(37):e8058. doi: 10.1097/MD.0000000000008058
12. Wu T-T, Gao Y, Zheng Y-Y, Ma Y-T, Xie X. Atherogenic index of plasma (AIP): a novel predictive indicator for the coronary artery disease in postmenopausal women. Lipids Health Dis. (2018) 17:1–7. doi: 10.1186/s12944-018-0828-z
13. Qin Z, Zhou K, Li Y, Cheng W, Wang Z, Wang J, et al. The atherogenic index of plasma plays an important role in predicting the prognosis of type 2 diabetic subjects undergoing percutaneous coronary intervention: results from an observational cohort study in China. Cardiovasc Diabetol. (2020) 19:1–11. doi: 10.1186/s12933-020-0989-8
14. Maesaka JK, Fishbane S. Regulation of renal urate excretion: a critical review. Am J Kidney Dis. (1998) 32(6):917–33. doi: 10.1016/S0272-6386(98)70067-8
15. Li M, Hu X, Fan Y, Li K, Zhang X, Hou W, et al. Hyperuricemia and the risk for coronary heart disease morbidity and mortality a systematic review and dose-response meta-analysis. Sci Rep. (2016) 6(1):19520. doi: 10.1038/srep19520
16. Zuo T, Liu X, Jiang L, Mao S, Yin X, Guo L. Hyperuricemia and coronary heart disease mortality: a meta-analysis of prospective cohort studies. BMC Cardiovasc Disord. (2016) 16:1–10. doi: 10.1186/s12872-016-0379-z
17. Braga F, Pasqualetti S, Ferraro S, Panteghini M. Hyperuricemia as risk factor for coronary heart disease incidence and mortality in the general population: a systematic review and meta-analysis. Clin Chem Lab Med. (2016) 54(1):7–15. doi: 10.1515/cclm-2015-0523
18. Wu AH, Gladden JD, Ahmed M, Ahmed A, Filippatos G. Relation of serum uric acid to cardiovascular disease. Int J Cardiol. (2016) 213:4–7. doi: 10.1016/j.ijcard.2015.08.110
19. Maloberti A, Mengozzi A, Russo E, Cicero AFG, Angeli F, Agabiti Rosei E, et al. The results of the URRAH (Uric Acid Right for Heart Health) project: a focus on hyperuricemia in relation to cardiovascular and kidney disease and its role in metabolic dysregulation. High Blood Press Cardiovasc Prev. (2023) 30(5):411–25. doi: 10.1007/s40292-023-00602-4
20. Hannan EL, Zhong Y, Jacobs AK, Stamato NJ, Berger PB, Walford G, et al. Patients with chronic total occlusions undergoing percutaneous coronary interventions: characteristics, success, and outcomes. Circ Cardiovasc Interv. (2016) 9(5):e003586. doi: 10.1161/CIRCINTERVENTIONS.116.003586
21. Brilakis ES, Banerjee S, Karmpaliotis D, Lombardi WL, Tsai TT, Shunk KA, et al. Procedural outcomes of chronic total occlusion percutaneous coronary intervention: a report from the NCDR (National Cardiovascular Data Registry). JACC Cardiovasc Interv. (2015) 8(2):245–53. doi: 10.1016/j.jcin.2014.08.014
22. Patel SM, Menon RV, Burke MN, Jaffer FA, Yeh RW, Vo M, et al. Current perspectives and practices on chronic total occlusion percutaneous coronary interventions. J Invasive Cardiol. (2017) 30(2):43–50.29035846
23. Ojeda S, Pan M, Gutiérrez A, Romero M, Chavarría J, de Lezo JS, et al. Bifurcation lesions involved in the recanalization process of coronary chronic total occlusions: incidence, treatment and clinical implications. Int J Cardiol. (2017) 230:432–8. doi: 10.1016/j.ijcard.2016.12.088
24. Stetler J, Karatasakis A, Christakopoulos GE, Tarar MNJ, Amsavelu S, Patel K, et al. Impact of crossing technique on the incidence of periprocedural myocardial infarction during chronic total occlusion percutaneous coronary intervention. Catheter Cardiovasc Interv. (2016) 88(1):1–6. doi: 10.1002/ccd.26505
25. Maccia C, Malchair F, Gobert I, Louvard Y, Lefevre T. Assessment of local dose reference values for recanalization of chronic total occlusions and other occlusions in a high-volume catheterization center. Am J Cardiol. (2015) 116(8):1179–84. doi: 10.1016/j.amjcard.2015.07.026
26. Sapontis J, Salisbury AC, Yeh RW, Cohen DJ, Hirai T, Lombardi W, et al. Early procedural and health status outcomes after chronic total occlusion angioplasty: a report from the OPEN-CTO registry (outcomes, patient health status, and efficiency in chronic total occlusion hybrid procedures). JACC Cardiovasc Interv. (2017) 10(15):1523–34. doi: 10.1016/j.jcin.2017.05.065
27. Christakopoulos GE, Christopoulos G, Carlino M, Jeroudi OM, Roesle M, Rangan BV, et al. Meta-analysis of clinical outcomes of patients who underwent percutaneous coronary interventions for chronic total occlusions. Am J Cardiol. (2015) 115(10):1367–75. doi: 10.1016/j.amjcard.2015.02.038
28. Werner GS, Martin-Yuste V, Hildick-Smith D, Boudou N, Sianos G, Gelev V, et al. A randomized multicentre trial to compare revascularization with optimal medical therapy for the treatment of chronic total coronary occlusions. Eur Heart J. (2018) 39(26):2484–93. doi: 10.1093/eurheartj/ehy220
29. Lee S-W, Lee PH, Ahn J-M, Park D-W, Yun S-C, Han S, et al. Randomized trial evaluating percutaneous coronary intervention for the treatment of chronic total occlusion: the DECISION-CTO trial. Circulation. (2019) 139(14):1674–83. doi: 10.1161/CIRCULATIONAHA.118.031313
30. van Veelen A, Elias J, van Dongen IM, Hoebers LPC, Claessen B, Henriques JPS. Percutaneous coronary intervention versus medical therapy for chronic total coronary occlusions: a systematic review and meta-analysis of randomised trials. Neth Heart J. (2021) 29:30–41. doi: 10.1007/s12471-020-01503-0
31. Shanker J, Kakkar VV. Contribution of classical and emerging risk factors to coronary artery disease in Asian Indians. Int J Cardiol. (2016) 214:97–106. doi: 10.1016/j.ijcard.2016.03.012
32. Nam JS, Kim MK, Nam JY, Park K, Kang S, Ahn CW, et al. Association between atherogenic index of plasma and coronary artery calcification progression in Korean adults. Lipids Health Dis. (2020) 19:1–7. doi: 10.1186/s12944-020-01317-4
33. Wang L, Chen F, Xiaoqi C, Yujun C, Zijie L. Atherogenic index of plasma is an independent risk factor for coronary artery disease and a higher SYNTAX score. Angiology. (2021) 72(2):181–6. doi: 10.1177/0003319720949804
34. Niskanen LK, Laaksonen DE, Nyyssönen K, Alfthan G, Lakka H-M, Lakka TA, et al. Uric acid level as a risk factor for cardiovascular and all-cause mortality in middle-aged men: a prospective cohort study. Arch Intern Med. (2004) 164(14):1546–51. doi: 10.1001/archinte.164.14.1546
35. Fang J, Alderman MH. Serum uric acid and cardiovascular mortality: the NHANES I epidemiologic follow-up study, 1971-1992. JAMA. (2000) 283(18):2404–10. doi: 10.1001/jama.283.18.2404
36. Kojima S, Sakamoto T, Ishihara M, Kimura K, Miyazaki S, Yamagishi M, et al. Prognostic usefulness of serum uric acid after acute myocardial infarction (the Japanese Acute Coronary Syndrome Study). Am J Cardiol. (2005) 96(4):489–95. doi: 10.1016/j.amjcard.2005.04.007
37. Maloberti A, Bossi I, Tassistro E, Rebora P, Racioppi A, Nava S, et al. Uric acid in chronic coronary syndromes: relationship with coronary artery disease severity and left ventricular diastolic parameter. Nutr Metab Cardiovasc Dis. (2021) 31(5):1501–8. doi: 10.1016/j.numecd.2021.01.023
38. Amrita J, Mahajan M, Bhanwer AJS, Mohan G. Oxidative stress: an effective prognostic tool for an early detection of cardiovascular disease in menopausal women. Biochem Res Int. (2016) 2016:6157605. doi: 10.1155/2016/6157605
39. Erdur MF, Tonbul HZ, Ozbiner H, Ozcicek A, Ozcicek F, Akbas EM, et al. The relationship between atherogenic index of plasma and epicardial adipose tissue in hemodialysis and peritoneal dialysis patients. Ren Fail. (2013) 35(9):1193–8. doi: 10.3109/0886022X.2013.823826
40. Madonna R, Massaro M, Scoditti E, Pescetelli I, De Caterina R. The epicardial adipose tissue and the coronary arteries: dangerous liaisons. Cardiovasc Res. (2019) 115(6):1013–25. doi: 10.1093/cvr/cvz062
41. Choudhary MK, Eräranta A, Koskela J, Tikkakoski AJ, Nevalainen PI, Kähönen M, et al. Atherogenic index of plasma is related to arterial stiffness but not to blood pressure in normotensive and never-treated hypertensive subjects. Blood Press. (2019) 28(3):157–67. doi: 10.1080/08037051.2019.1583060
42. Kul Ş, Çalışkan Z, Güvenç TS, Güvenç RÇ, Çalışkan M. Plasma lipids in patients with inflammatory bowel disease: observations on the associations between lipid indices and coronary flow reserve. Wien Klin Wochenschr. (2020) 132:283–94. doi: 10.1007/s00508-020-01649-2
43. Sautin YY, Nakagawa T, Zharikov S, Johnson RJ. Adverse effects of the classic antioxidant uric acid in adipocytes: NADPH oxidase-mediated oxidative/nitrosative stress. Am J Physiol Cell Physiol. (2007) 293(2):C584–96. doi: 10.1152/ajpcell.00600.2006
44. Egli M, Vollenweider P, Burcelin R, Nicod P, Thorens B. Clustering of cardiovascular risk factors mimicking the human metabolic syndrome X in eNOS null mice. Swiss Med Wkly. (2003) 133(2526):360–3.12947532
45. Rao GN, Corson MA, Berk BC. Uric acid stimulates vascular smooth muscle cell proliferation by increasing platelet-derived growth factor A-chain expression. J Biol Chem. (1991) 266(13):8604–8. doi: 10.1016/S0021-9258(18)93017-6
46. Kang D-H, Park S-K, Lee I-K, Johnson RJ. Uric acid–induced C-reactive protein expression: implication on cell proliferation and nitric oxide production of human vascular cells. J Am Soc Nephrol. (2005) 16(12):3553–62. doi: 10.1681/ASN.2005050572
47. Varo N, Vicent D, Libby P, Nuzzo R, Calle-Pascual AL, Bernal MR, et al. Elevated plasma levels of the atherogenic mediator soluble CD40 ligand in diabetic patients: a novel target of thiazolidinediones. Circulation. (2003) 107(21):2664–9. doi: 10.1161/01.CIR.0000074043.46437.44
48. Song P, Xu L, Xu J, Zhang H-q, Yu C-x, Guan Q-b, et al. Atherogenic index of plasma is associated with body fat level in type 2 diabetes mellitus patients. Curr Vasc Pharmacol. (2018) 16(6):589–95. doi: 10.2174/1570161116666180103125456
49. Mazzali M, Hughes J, Kim Y-G, Jefferson JA, Kang D-H, Gordon KL, et al. Elevated uric acid increases blood pressure in the rat by a novel crystal-independent mechanism. Hypertension. (2001) 38(5):1101–6. doi: 10.1161/hy1101.092839
50. Nakagawa T, Hu H, Zharikov S, Tuttle KR, Short RA, Glushakova O, et al. A causal role for uric acid in fructose-induced metabolic syndrome. Am J Physiol Renal Physiol. (2006) 290(3):F625–31. doi: 10.1152/ajprenal.00140.2005
Keywords: coronary artery disease, chronic total occlusion, atherogenic index of plasma, hyperuricemia, prediction
Citation: Han H, Liu X, Zhao Q, Wang Z, Sun Y, Ma X, Li M, Ma H, Liu Y, Shi D, Cheng Y and Zhou Y (2024) The synergistic effect of the atherogenic index of plasma and hyperuricemia on the prediction of coronary chronic total occlusion lesion: an observational cross-sectional study. Front. Cardiovasc. Med. 11: 1437096. doi: 10.3389/fcvm.2024.1437096
Received: 23 May 2024; Accepted: 8 July 2024;
Published: 23 July 2024.
Edited by:
Rongjing Ding, Peking University, ChinaReviewed by:
Ruihai Zhou, University of North Carolina at Chapel Hill, United States© 2024 Han, Liu, Zhao, Wang, Sun, Ma, Li, Ma, Liu, Shi, Cheng and Zhou. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: YuJing Cheng, MTM0MjY0ODExOTNAMTYzLmNvbQ==; YuJie Zhou, YXp6eWoxMkAxNjMuY29t
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.