 Ibrahim Antoun1*
Ibrahim Antoun1* Xin Li2
Xin Li2 Ahmed Kotb3Joseph Barker3Akash Mavilakandy3
Ahmed Kotb3Joseph Barker3Akash Mavilakandy3 Ivelin Koev1Zakariyya Vali1Riyaz Somani1,3
Ivelin Koev1Zakariyya Vali1Riyaz Somani1,3 G. André Ng1,3,4
G. André Ng1,3,4
- 1Department of Cardiology, University Hospitals of Leicester NHS Trust, Glenfield Hospital, Leicester, United Kingdom
- 2Department of Engineering, University of Leicester, Glenfield Hospital, Leicester, United Kingdom
- 3Department of Cardiovascular Sciences, Clinical Science Wing, University of Leicester, Glenfield Hospital, Leicester, United Kingdom
- 4Department of Research, National Institute for Health Research Leicester Research Biomedical Centre, Leicester, United Kingdom
Background: Direct current cardioversion (DCCV) is used as elective and emergency rhythm control for atrial fibrillation (AF). We aimed to explore the role of P-wave parameters measured during sinus rhythm using body surface mapping (BSM) in predicting successful DCCV for persistent atrial fibrillation (persAF) at 12 months.
Methods: This case–control study included 56 males >18 years old who underwent DCCV for persAF. P-wave parameter collection after DCCV for AF was done using 128 unipolar leads. A band-pass filter of 1–50 Hz was utilised. Corrected P-wave duration (PWDc), P-wave amplitude, and P-wave dispersion were measured to predict 12-month outcomes and time of recurrence.
Results: The mean age was 64 ± 4 years, and 23 patients (44%) were on amiodarone. The 12-month success rate was 44% (n = 23), while the rest reverted to AF after 2.6 ± 0.4 months. The parameters were comparable between successful and failed DCCV in the entire cohort and patients not on amiodarone. In patients on amiodarone, patients with failed arms had higher PWDc than those with successful arms (188 vs. 150 ms, P = 0.04). Receiver operator characteristic curve analysis for PWDc in the amiodarone cohort showed an area under the curve (AUC) of 0.75 and P = 0.049. A recurrence cut-off >161 ms had a sensitivity of 69% and a specificity of 100%, with a hazard ratio of 10.7, P = 0.004. The parameters were not predictive of the time of recurrence.
Conclusion: In patients on amiodarone, increased PWDc measured using BSM was associated with higher AF recurrence at 12 months following DCCV for persAF.
Introduction
Atrial fibrillation (AF) is the most common sustained arrhythmia worldwide, increasing the risk of stroke and mortality (1, 2). AF could be caused by triggers or substrate driven by electrical or structural remodelling. The recent European Society of Cardiology guidelines suggested a rate or rhythm control approach to manage AF (3). Rhythm control options include anti-arrhythmic drugs, catheter ablation, and direct current cardioversion (DCCV). DCCV is particularly useful when the patient is hemodynamically unstable or there is an urgency to resume sinus rhythm (SR). The mechanism of DCCV was proposed to prevent the maintenance of re-entrant tachycardia by the remaining myocardial tissue after depolarisation of a critical mass (4). The 1-year success rate of external DCCV for AF varied between 15% and 47% (5–8). Predicting DCCV outcome after reversion to SR has been explored in the literature. Symptom monitoring was unreliable in predicting DCCV outcomes due to asymptomatic AF (9). Predictors of DCCV outcomes in the literature include demographics, the use of anti-arrhythmic medication (10), cardiac imaging (11), and P-wave analysis (12).
P-wave represents the spatiotemporal convolution of the depolarisation wavefront in the atria as collected in the torso. P-wave parameters provide insights into atrial electrophysiology and essential information regarding atrial remodelling, which triggers and maintains AF (13). These parameters utilised 12-lead ECG and signal-averaged ECG (SAEG) following initial successful cardioversion to predict freedom of arrhythmia rate (Table 1). However, these studies have yet to utilise body surface mapping (BSM) to assess the same hypothesis. This study aimed at determining the value of 128-lead BSM of P-waves in SR in predicting 12-month freedom from arrhythmia rate after initially successful DCCV for AF.
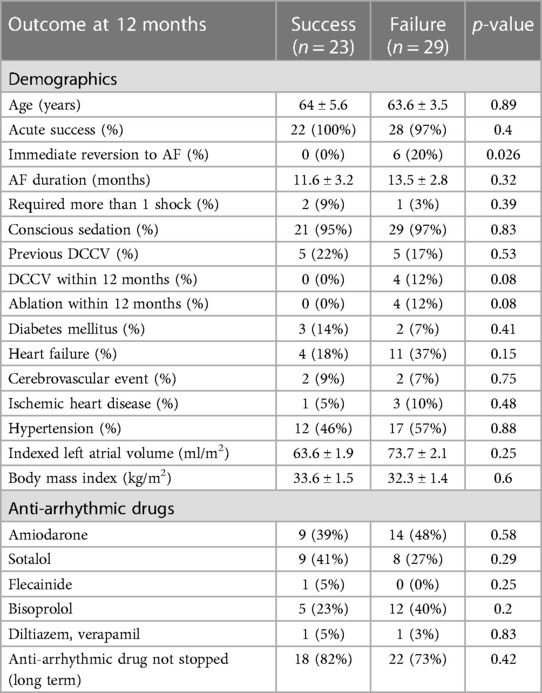
Table 1 Demographics, clinical outcomes, and medication details of study cohort.
Methods
This case–control study included 56 patients who underwent DCCV for AF between October 2013 and May 2015. DCCV acute success was defined as the immediate return to SR. Long-term DCCV success was determined by the lack of AF or atrial flutter up to 1 year following DCCV. P-wave parameters measured using BSM were used to predict DCCV outcome at 12 months and recurrence time. Clinical details of DCCV, follow-ups, and medication were obtained by retrospective analysis of clinical paper records. This study was a part of the USURP-AF II study approved by the East Midlands–Leicester Central Research Ethics Committee. REC reference: 19/EM/003
The selection criteria included the following:
1. Patients with persistent atrial fibrillation (persAF) who underwent external DCCV in Glenfield Hospital, Leicester, UK, between January 2013 and May 2015
2. Patients >18 years old and who consented to the study
3. Planting anterior leads around the breast tissue in females could be challenging. Therefore, only male patients were selected.
4. Patients who had ECG-documented AF directly before DCCV
5. Patients who were adequately anti-coagulated for 4 weeks before DCCV [therapeutic international normalised ratio (INR)].
P-wave parameter collection after DCCV for AF was done using 128 unipolar leads with 64 leads on the front and back of the torso (Figure 1). The vest utilised electrodes from Biosemi (Amsterdam, The Netherlands). The electrodes record digital ECGs before, during, and after DCCV. If DCCV was acutely successful, SR resumption would allow recording digital P-waves following DCCV. A MATLAB code was then applied to the digital BSM data using a band-pass filter of 1–50 Hz. It anointed the isoelectric line and P-wave peak to measure the P-wave duration (PWD) and amplitude. Also, it allowed the measurement of the P-wave manually by adjusting its start and end. The first four identifiable P-waves were measured and averaged in each lead. The parameters measured include the following:

Figure 1 Demonstration of real-time body surface mapping.
The following P-wave parameters were produced:
1. PWD: Distance from P-wave onset to offset. It demonstrates a marker of atrial conduction.
2. P-wave amplitude (PWA): The area under the P-wave was estimated using the trapezoidal method by integrating the total area into a little trapezoid. It demonstrates atrial voltage. Regarding biphasic P-waves, the highest PWA absolute value between the positive and negative phases was accepted.
3. P-wave dispersion (PWDisp): The maximum difference between P-wave durations. It demonstrates atrial depolarisation heterogeneity.
Each measurement was averaged in all 128 leads to produce one number representing a P-wave measurement in each patient (Figure 2).
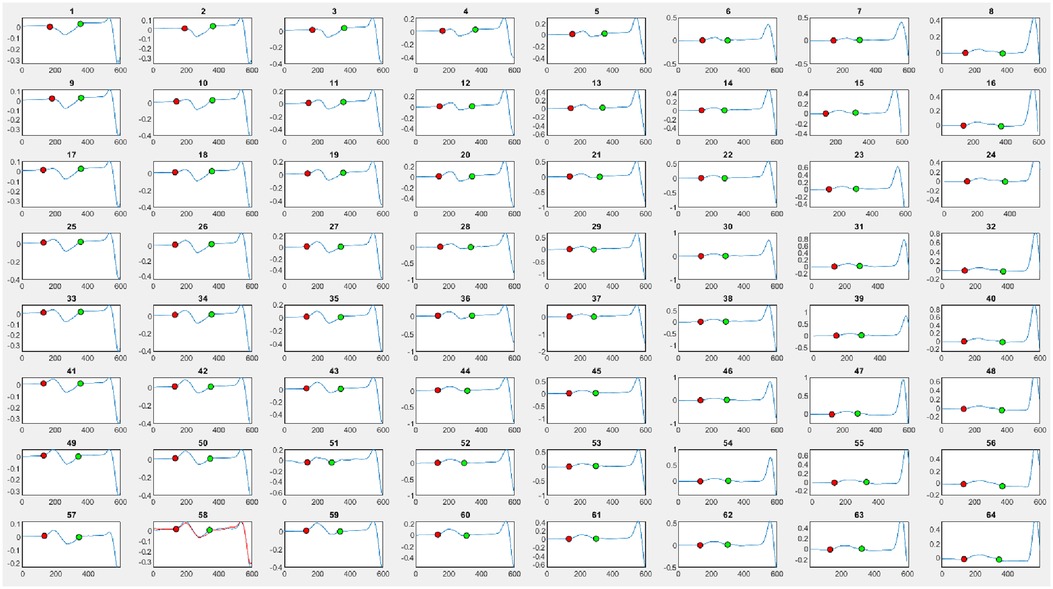
Figure 2 Demonstration of P-wave parameters anointing using body surface mapping at the front 64 leads. The resulting parameters are P-wave duration, amplitude, and dispersion. The red dot represents the beginning of the P-wave, while the green dot represents the end of the P-wave.
In patients with immediate reversion to AF with <4 sinus beats, P-waves were measured until AF reversion. Heart rate (HR) was also noted in every ECG. Amiodarone is known to adjust P-wave morphology (14). Therefore, P-wave analysis was done after stratifying the patients based on amiodarone. It is well recognised that changes in HR and cycle length may affect P-wave morphology (15, 16). Previous studies have tried to tackle this by adjusting P-wave parameters to heart rate in regression analysis, a method that was not utilised in this study (17). As there are no current verified formulae to correct PWD for heart rate, we utilised a QT correcting formula to address this issue. Out of the formulae used in the literature, the Hodges formula has been proposed to be the most reliable and was therefore utilised in this study to correct PWD for heart rate, producing corrected P-wave duration (PWDc) (18). The intra-observer variability test anonymously analysed 20 BSMs on 2 days.
Statistical analysis
Statistical analysis was conducted using GraphPad Prism V9.3 (San Diego, CA, USA). Categorical variables were expressed as frequency and percentage. The mean ± standard error of the mean was adopted to describe continuous parametric data. Unpaired t-tests or Mann–Whitney U tests were utilised to analyse unmatched data depending on the normality of the distribution. Gubbs’ test was conducted to identify outlier measurements. The cut-off of P-wave parameters for the DCCV outcome was analysed using receiver operator curve (ROC) analysis. The detected cut-off was used in a Kaplan–Meier survival analysis to use the proposed cut-off in predicting DCCV outcomes. P-value ≤0.05 represented statistical significance.
Results
The mean age was 64 ± 4 years. Three of the 56 patients involved were in SR at their DCCV appointment and were excluded. One patient was also excluded due to the lack of follow-up at 12 months (Figure 3). The 12-month success rate was 44% (n = 23), while the rest reverted to AF after 2.6 ± 0.4 months. Patients’ clinical details and demographics are provided in Table 2. Intra-observer variability was highest in PWA at 10% (0.05 mV), followed by PWDisp at 8% (9.5 ms) and PWD at 5% (8.4 ms). Gubbs’ test did not yield outlier values.
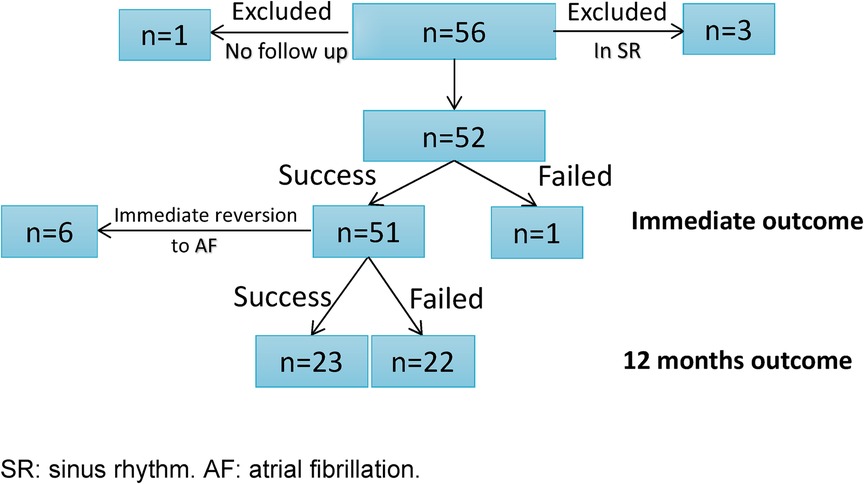
Figure 3 Clinical outcomes of the cohort.
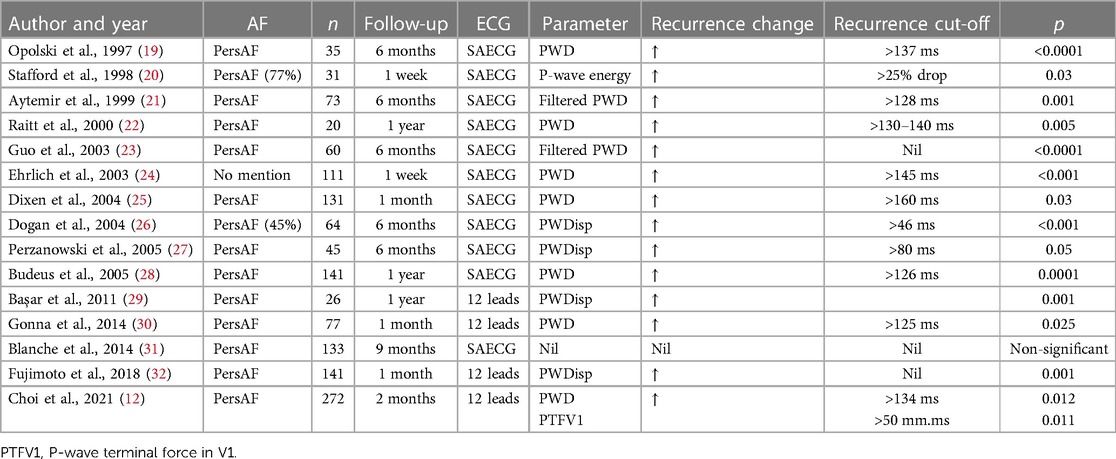
Table 2 Studies that correlated P-wave parameter with direct current cardioversion outcome.
P-wave parameters were compared between successful and failed arms (PWDc: 163 vs. 178 ms, P = 0.29. PWA: 0.33 vs. 0.38 mV, P = 0.1. PWDisp: 24 vs. 27 ms, P = 0.35).
After stratifying for amiodarone, the success rates in the amiodarone and non-amiodarone cohorts were 39% vs. 48%, P = 0.58, respectively. P-wave parameters were comparable in the non-amiodarone cohort (172 vs. 167 ms, P = 0.82; PWA: 0.34 vs. 0.41 mV, P = 0.2; PWDisp: 26 vs. 24 ms, P = 0.58). In patients on amiodarone, those who had failed arms had higher PWDc than those with successful arms (188 vs. 150 ms, P = 0.04), while PWA and PWDisp were comparable between both arms (0.3 vs. 0.4 mV, P = 0.09, and 21 vs. 20 ms, P = 0.94, respectively). ROC curve analysis for PWDc in the amiodarone cohort showed an area under the curve (AUC) of 0.75 and P = 0.049. A recurrence cut-off >161 ms had a sensitivity of 69% and a specificity of 100%. The Kaplan–Meier survival analysis using a PWDc cut-off of 161 ms in the amiodarone cohort indicated a hazard ratio of 10.7, P = 0.004. By contrast, the non-amiodarone and full cohorts did not show a difference between cut-off and 12-month DCCV outcomes (Figure 4). There was no correlation between P-wave parameters and AF recurrence time in the entire cohort (PWDc: r = −0.23, P = 0.24; PWA: r = 0.33, P = 0.09; PWDisp: r = −0.13, P = 0.52), the amiodarone cohort (PWDc: r = −0.02, P = 0.95; PWA: r = 0.5, P = 0.07; PWDisp: r = –0.23, P = 0.45), and the non-amiodarone cohort (PWDc: r = −0.36, P = 0.24; PWA: r = −0.1, P = 0.74; PWDisp: r = −0.12, P = 0.71).
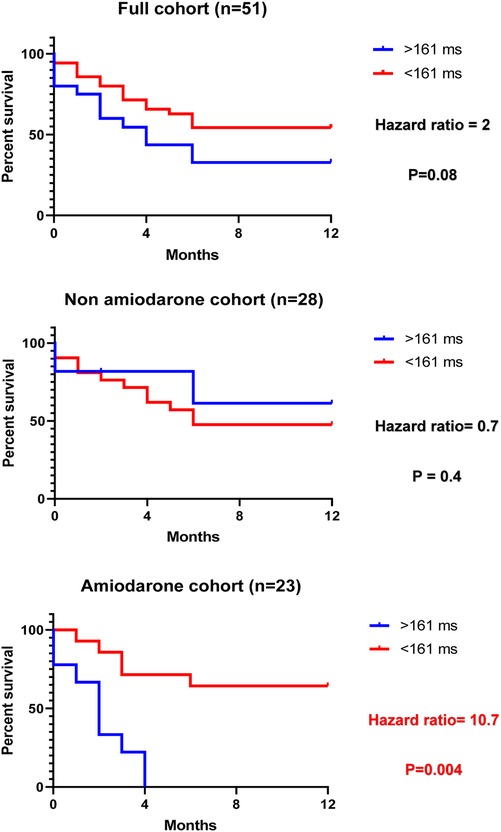
Figure 4 Kaplan–Meier survival analysis for the corrected P-wave duration cut-off in all cohorts.
Discussion
Although other studies correlated P-wave parameters after DCCV with outcome using signal-averaged ECG or 12-lead ECG (summarised in Table 2), this is the first study to perform this using BSM of P-waves. The 1-year success rate in our cohort falls into the higher range of previous studies demonstrating relatively good outcomes in our centre. However, the inclusion of males might have positively affected the one-year success rate (33). Unlike former studies, demographics in this cohort were not predictive of the outcome (34, 35). One would expect a positive correlation of AF risk factors with AF recurrence after DCCV. It was noted that this cohort only involved male patients. This could cause selection bias and affect the rest of the demographics. Therefore, further studies with a random selection of subjects would be advised to investigate predictive factors (36, 37).
Regarding P-wave analysis, to the best of our knowledge, no previous study has correlated P-wave BSM with 12 months of DCCV outcome and assessed recurrence time. Stratification by being on amiodarone was conducted to address its effects on P-wave parameters. Increased PWDc after DCCV in the amiodarone cohort was associated with 12-month failure with high specificity. This was in keeping with previous studies in Table 2. This can be explained by left atrium (LA) remodelling, fibrosis, and intra-atrial conduction delay in patients prone to AF recurrence (38). Furthermore, a previous study demonstrated shorter PWD in patients with AF successfully treated with amiodarone (14). These results were not evident in patients who were not on amiodarone. The reason behind this finding is unclear. One reason could be that patients did not have refractory AF significant enough to be on amiodarone, leading to the lack of LA conduction delay. This may be possible to detect with imaging modalities and is advised in future studies. Another reason could be the potential small size to detect a significant effect. As for PWA, one would expect a correlation between low PWA (caused by fibrosis) and DCCV 1-year failure. This corresponded to the PVI studies that proposed this (39, 40). Although only one study correlated reduced PWA with AF recurrence after internal cardioversion (17), DCCV (external) was used in this study, and all studies in Table 2 did not show similar findings. It was unclear why PWA was predictive of outcome in internal DCCV but not external DCCV. However, one theory is that external cardioversion could have caused lower atrial stunning, not affecting PWA, unlike internal cardioversion (41). Further randomised trials would be beneficial in establishing a mechanism.
PWDisp reflects inhomogeneous atrial refractoriness and AF vulnerability (42). It was not correlated to the DCCV 12-month outcome in this cohort. According to previous studies, amiodarone decreases PWDisp because of increased atrial repolarisation (14, 43). Following the hypothesis that the amiodarone cohort had more LA remodelling, it is possible that the increased PWDisp from remodelling was decreased to normal by the amiodarone effect. Patients not on amiodarone did not have enough remodelling to cause a notable PWDisp effect predictive of DCCV outcomes per previous studies (Table 2). These results warrant further investigation into predicting DCCV outcomes in patients on and off amiodarone. Further studies should directly compare BSM, signal-averaged electrocardiogram (SAECG), and 12-lead ECG in utilising P-wave parameters to predict 12-month DCCV outcome for AF.
Conclusion
Predicting DCCV outcome using P-wave parameters measured in SR using BSM was only feasible in patients on amiodarone. In this cohort, increased PWDc in SR directly following DCCV was associated with failed DCCV at 12 months. PWDc >161 ms was 100% specific for AF recurrence by 12 months after initial successful DCCV. This could serve as a marker for considering an early rate control strategy.
Limitations
This is a single-centre retrospective study with AF recurrence detected using 12-lead ECG or Holter monitoring. Long-term monitoring was not done, and the AF burden was not evaluated. This could have missed sub-clinical and micro-AF episodes. The relatively low sample size with post-hoc power analysis of 67% and 71% in the full cohort and amiodarone cohort to detect a significant difference in PWDc may lead to a type-2 error. Therefore, future studies using BSM with a higher number and pre-study sample size calculation are advised. Direct comparison between BSM, 12-lead ECG, and SAECG was not conducted and is suggested in future studies. This study only included male patients, which can cause selection bias. Although not impossible, including female patients would require the adjustment of lead positions, making comparisons challenging. Flecainide and sotalol used in our cohort affected PWD (44, 45). Furthermore, patients stopping their anti-arrhythmic drugs were included in the analysis. Future studies matching patients by anti-arrhythmic drugs and their cessation are needed to limit confounding. The Hodges formula is currently not verified as a methodology in the literature to correct PWD for HR. A future dedicated study would be useful to confirm the utility of this formula for the benefit of future studies utilising PWD. One of the main limitations of this study is the age of the data utilised. The data were collected between 2013 and 2015, which may affect the applicability of the findings to current clinical practice. In future studies, incorporating recent data with longer follow-ups is advised. This study did not measure potential relevant pre-DCCV parameters, including AF cycle length and AF coarseness. The study did not utilise magnetic resonance imaging to evaluate LA fibrosis, which is recommended for future studies.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors without undue reservation.
Ethics statement
The studies involving humans were approved by the Leicester Central Research Ethics Committee. The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
Author contributions
IA: Writing – original draft, Writing – review & editing. XL: Software, Writing – review & editing. AK: Writing – review & editing. JB: Writing – review & editing. AM: Writing – review & editing. IK: Writing – review & editing. ZV: Writing – review & editing. RS: Writing – review & editing. GA: Supervision, Writing – review & editing.
Funding
The authors declare that no financial support was received for the research, authorship, and/or publication of this article.
Acknowledgements
This study is part of the research portfolio supported by the Leicester National Institute for Health and Care Biomedical Research Centre's cardiovascular theme.
Conflict of interest
AK is supported with a clinical research fellowship from Abbott. GAN is supported by a British Heart Foundation Programme Grant (RG/17/3/32,774) and the Medical Research Council Biomedical Catalyst Developmental Pathway Funding Scheme (MR/S037306/1). GAN also discloses consultancy fees, speaker honorarium fellow support from Biosense Webster, research fellow funding from Abbott, and consultancy fees from Catheter Precision.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Wolf PA, Mitchell JB, Baker CS, Kannel WB, D'Agostino RB. Impact of atrial fibrillation on mortality, stroke, and medical costs. Arch Intern Med. (1998) 158(3):229–34. doi: 10.1001/archinte.158.3.229
2. Wyndham CR. Atrial fibrillation: the most common arrhythmia. Tex Heart Inst J. (2000) 27(3):257.11093410
3. Hindricks G, Potpara T, Dagres N, Arbelo E, Bax JJ, Blomström-Lundqvist C, et al. 2020 ESC guidelines for the diagnosis and management of atrial fibrillation developed in collaboration with the European Association for Cardio-Thoracic Surgery (EACTS): the task force for the diagnosis and management of atrial fibrillation of the European Society of Cardiology (ESC) developed with the special contribution of the European Heart Rhythm Association (EHRA) of the ESC. Eur Heart J. (2021) 42(5):373–498. doi: 10.1093/eurheartj/ehaa612
4. Zipes DP, Fischer J, King RM, Nicoll A, Jolly WW. Termination of ventricular fibrillation in dogs by depolarizing a critical amount of myocardium. Am J Cardiol. (1975) 36(1):37–44. doi: 10.1016/0002-9149(75)90865-6
5. Van Gelder IC, Crijns HJ, Tieleman RG, Brügemann J, De Kam PJ, Gosselink AM, et al. Chronic atrial fibrillation: success of serial cardioversion therapy and safety of oral anticoagulation. Arch Intern Med. (1996) 156(22):2585–92. doi: 10.1001/archinte.1996.00440210109011
6. Tabery S, Bouwels L, Uijen G, Uppelschoten A, Verheugt F. Factors influencing immediate and long-term outcome of electrical cardioversion of persistent atrial fibrillation and flutter. Neth Heart J. (2001) 9(1):16.25696689
7. Kuppahally SS, Foster E, Shoor S, Steimle AE. Short-term and long-term success of electrical cardioversion in atrial fibrillation in managed care system. Int Arch Med. (2009) 2:1–9. doi: 10.1186/1755-7682-2-39
8. Castrichini M, Restivo L, Fabris E, Massa L, Di Meola R, Beltrame D, et al. Prevalence and predictors of persistent sinus rhythm after elective electrical cardioversion for atrial fibrillation. J Cardiovasc Med. (2021) 22(8):626–30. doi: 10.2459/JCM.0000000000001182
9. Fetsch T, Bauer P, Engberding R, Koch HP, Lukl J, Meinertz T, et al. Prevention of atrial fibrillation after cardioversion: results of the PAFAC trial. Eur Heart J. (2004) 25(16):1385–94. doi: 10.1016/j.ehj.2004.04.015
10. Lafuente-Lafuente C, Valembois L, Bergmann JF, Belmin J. Antiarrhythmics for maintaining sinus rhythm after cardioversion of atrial fibrillation. Cochrane Database Syst Rev. (2019) 9:CD005049. doi: 10.1002/14651858.CD005049.pub5
11. Luong C, Thompson DJ, Bennett M, Gin K, Jue J, Barnes ME, et al. Right atrial volume is superior to left atrial volume for prediction of atrial fibrillation recurrence after direct current cardioversion. Can J Cardiol. (2015) 31(1):29–35. doi: 10.1016/j.cjca.2014.10.009
12. Choi J-H, Kwon H-J, Kim HR, Park S-J, Kim JS, On YK, et al. Electrocardiographic predictors of early recurrence of atrial fibrillation. Ann Noninvasive Electrocardiol. (2021) 26(6):e12884. doi: 10.1111/anec.12884
13. Nielsen JB, Kühl JT, Pietersen A, Graff C, Lind B, Struijk JJ, et al. P-wave duration and the risk of atrial fibrillation: results from the Copenhagen ECG study. Heart Rhythm. (2015) 12(9):1887–95. doi: 10.1016/j.hrthm.2015.04.026
14. Banasiak W, Telichowski A, Anker SD, Fuglewicz A, Kalka D, Molenda W, et al. Effects of amiodarone on the P-wave triggered signal-averaged electrocardiogram in patients with paroxysmal atrial fibrillation and coronary artery disease. Am J Cardiol. (1999) 83(1):112–4. doi: 10.1016/S0002-9149(98)00792-9
15. Boineau JP, Schuessler RB, Mooney CR, Wylds A, Miller C, Hudson R, et al. Multicentric origin of the atrial depolarization wave: the pacemaker complex. Relation to dynamics of atrial conduction, P-wave changes and heart rate control. Circulation. (1978) 58(6):1036–48. doi: 10.1161/01.CIR.58.6.1036
16. Forester J, Bo H, Sleigh J, Henderson J. Variability of RR, P wave-to-R wave, and R wave-to-T wave intervals. Am J Physiol Heart Circ Physiol. (1997) 273(6):H2857–60. doi: 10.1152/ajpheart.1997.273.6.H2857
17. Magnani JW, Zhu L, Lopez F, Pencina MJ, Agarwal SK, Soliman EZ, et al. P-wave indices and atrial fibrillation: cross-cohort assessments from the Framingham Heart Study (FHS) and Atherosclerosis Risk in Communities (ARIC) study. Am Heart J. (2015) 169(1):53–61.e1. doi: 10.1016/j.ahj.2014.10.009
18. Chiladakis J, Kalogeropoulos A, Arvanitis P, Koutsogiannis N, Zagli F, Alexopoulos D. Preferred QT correction formula for the assessment of drug-induced QT interval prolongation. J Cardiovasc Electrophysiol. (2010) 21(8):905–13. doi: 10.1111/j.1540-8167.2010.01738.x
19. Opolski G, Ścisło P, Stanisławska J, Górecki A, Steckiewicz R, Torbicki A. Detection of patients at risk for recurrence of atrial fibrillation after successful electrical cardioversion by signal-averaged P-wave ECG. Int J Cardiol. (1997) 60(2):181–5. doi: 10.1016/S0167-5273(97)02982-3
20. Stafford PJ, Kamalvand K, Tan K, Vincent R, Sulke N. Prediction of maintenance of sinus rhythm after cardioversion of atrial fibrillation by analysis of serial signal-averaged P waves. Pacing Clin Electrophysiol. (1998) 21(7):1387–95. doi: 10.1111/j.1540-8159.1998.tb00209.x
21. Aytemir K, Aksoyek S, Yildirir A, Ozer N, Oto A. Prediction of atrial fibrillation recurrence after cardioversion by P wave signal-averaged electrocardiography. Int J Cardiol. (1999) 70(1):15–21. doi: 10.1016/S0167-5273(99)00038-8
22. Raitt MH, Ingram KD, Thurman SM. Signal-averaged P wave duration predicts early recurrence of atrial fibrillation after cardioversion. Pacing Clin Electrophysiol. (2000) 23(2):259–65. doi: 10.1111/j.1540-8159.2000.tb00808.x
23. Guo XH, Gallagher MM, Poloniecki J, Yi G, Camm AJ. Prognostic significance of serial P wave signal-averaged electrocardiograms following external electrical cardioversion for persistent atrial fibrillation: a prospective study. Pacing Clin Electrophysiol. (2003) 26(1p2):299–304. doi: 10.1046/j.1460-9592.2003.00037.x
24. Ehrlich J, Schadow K, Steul K, Zhang G, Israel C, Hohnloser S. Prediction of early recurrence of atrial fibrillation after external cardioversion by means of P wave signal-averaged electrocardiogram. Z Kardiol. (2003) 92(7):540–6. doi: 10.1007/s00392-003-0940-5
25. Dixen U, Joens C, Parner J, Rasmussen V, Pehrson S, Jensen G. Prolonged signal-averaged P wave duration after elective cardioversion increases the risk of recurrent atrial fibrillation. Scand Cardiovasc J. (2004) 38(3):147–51. doi: 10.1080/14017430410028645
26. Dogan A, Avsar A, Ozturk M. P-wave dispersion for predicting maintenance of sinus rhythm after cardioversion of atrial fibrillation. Am J Cardiol. (2004) 93(3):368–71. doi: 10.1016/j.amjcard.2003.09.064
27. Perzanowski C, Ho AT, Jacobson AK. Increased P-wave dispersion predicts recurrent atrial fibrillation after cardioversion. J Electrocardiol. (2005) 38(1):43–6. doi: 10.1016/j.jelectrocard.2004.09.008
28. Budeus M, Hennersdorf M, Perings C, Wieneke H, Erbel R, Sack S. Prediction of the recurrence of atrial fibrillation after successful cardioversion with P wave signal-averaged ECG. Ann Noninvasive Electrocardiol. (2005) 10(4):414–9. doi: 10.1111/j.1542-474X.2005.00059.x
29. Başar N, Malçok Gürel O, Ozcan F, Ozlü MF, Biçer Yeşilay A, Cağlı K, et al. Diagnostic accuracy of P-wave dispersion in prediction of maintenance of sinus rhythm after external cardioversion of atrial fibrillation. Anadolu Kardiyol Derg. (2011) 11(1):34–8. doi: 10.5152/akd.2011.006
30. Gonna H, Gallagher MM, Guo XH, Yap YG, Hnatkova K, Camm AJ. P-wave abnormality predicts recurrence of atrial fibrillation after electrical cardioversion: a prospective study. Ann Noninvasive Electrocardiol. (2014) 19(1):57–62. doi: 10.1111/anec.12087
31. Blanche C, Tran N, Carballo D, Rigamonti F, Burri H, Zimmermann M. Usefulness of P-wave signal averaging to predict atrial fibrillation recurrences after electrical cardioversion. Ann Noninvasive Electrocardiol. (2014) 19(3):266–72. doi: 10.1111/anec.12131
32. Fujimoto Y, Yodogawa K, Maru Y-j, Oka E, Hayashi H, Yamamoto T, et al. Advanced interatrial block is an electrocardiographic marker for recurrence of atrial fibrillation after electrical cardioversion. Int J Cardiol. (2018) 272:113–7. doi: 10.1016/j.ijcard.2018.07.135
33. Suttorp MJ, Kingma JH, Koomen EM, van't Hof A, Tijssen JG, Lie KI. Recurrence of paroxysmal atrial fibrillation or flutter after successful cardioversion in patients with normal left ventricular function. Am J Cardiol. (1993) 71(8):710–3. doi: 10.1016/0002-9149(93)91015-A
34. Alt E, Ammer R, Lehmann G, Pütter K, Ayers GM, Pasquantonio J, et al. Patient characteristics and underlying heart disease as predictors of recurrent atrial fibrillation after internal and external cardioversion in patients treated with oral sotalol. Am Heart J. (1997) 134(3):419–25. doi: 10.1016/S0002-8703(97)70076-0
35. Soran H, Younis N, Currie P, Silas J, Jones I, Gill G. Influence of diabetes on the maintenance of sinus rhythm after a successful direct current cardioversion in patients with atrial fibrillation. QJM. (2008) 101(3):181–7. doi: 10.1093/qjmed/hcm123
36. Mercuro G, Deidda M, Piras A, Dessalvi CC, Maffei S, Rosano GM. Gender determinants of cardiovascular risk factors and diseases. J Cardiovasc Med. (2010) 11(3):207–20. doi: 10.2459/JCM.0b013e32833178ed
37. Andersen KK, Andersen ZJ, Olsen TS. Age-and gender-specific prevalence of cardiovascular risk factors in 40,102 patients with first-ever ischemic stroke: a nationwide Danish study. Stroke. (2010) 41(12):2768–74. doi: 10.1161/STROKEAHA.110.595785
38. Papageorgiou P, Monahan K, Boyle NG, Seifert MJ, Beswick P, Zebede J, et al. Site-dependent intra-atrial conduction delay: relationship to initiation of atrial fibrillation. Circulation. (1996) 94(3):384–9. doi: 10.1161/01.CIR.94.3.384
39. Vlachos K, Efremidis M, Letsas KP, Bazoukis G, Martin R, Kalafateli M, et al. Low-voltage areas detected by high-density electroanatomical mapping predict recurrence after ablation for paroxysmal atrial fibrillation. J Cardiovasc Electrophysiol. (2017) 28(12):1393–402. doi: 10.1111/jce.13321
40. Huang D, Li J-b, Zghaib T, Ipek EG, Balouch M, Spragg DD, et al. The extent of left atrial low-voltage areas included in pulmonary vein isolation is associated with freedom from recurrent atrial arrhythmia. Can J Cardiol. (2018) 34(1):73–9. doi: 10.1016/j.cjca.2017.10.012
41. Gorenek B, Birdane A, Kudaiberdieva G, Goktekin O, Cavusoglu Y, Unalir A, et al. P wave amplitude and duration may predict immediate recurrence of atrial fibrillation after internal cardioversion. Ann Noninvasive Electrocardiol. (2003) 8(3):215–8. doi: 10.1046/j.1542-474X.2003.08308.x
42. Li Z, Hertervig E, Carlson J, Johansson C, Olsson SB, Yuan S. Dispersion of refractoriness in patients with paroxysmal atrial fibrillation: evaluation with simultaneous endocardial recordings from both atria. J Electrocardiol. (2002) 35(3):227–34. doi: 10.1054/jelc.2002.33973
43. Boriani G, Diemberger I, Biffi M, Camanini C, Valzania C, Corazza I, et al. P wave dispersion and short-term vs. late atrial fibrillation recurrences after cardioversion. Int J Cardiol. (2005) 101(3):355–61. doi: 10.1016/j.ijcard.2004.03.039
44. Telichowski A, Banasiak W, Wiech K, Zeborowski J, Pierog M, Ponikowski P, et al. The effect of sotalol hydrochloride therapy on atrial signal-averaged ECG in patients with paroxysmal atrial fibrillation. Pol Merkur Lekarski. (1996) 1(5):303–9.9273201
Keywords: atrial fibrillation, body surface mapping, p-waves, cardioversion, electrical cardioversion
Citation: Antoun I, Li X, Kotb A, Barker J, Mavilakandy A, Koev I, Vali Z, Somani R and Ng GA (2024) Body surface mapping of P-waves in sinus rhythm to predict recurrence following cardioversion for atrial fibrillation. Front. Cardiovasc. Med. 11: 1417029. doi: 10.3389/fcvm.2024.1417029
Received: 13 April 2024; Accepted: 15 July 2024;
Published: 25 July 2024.
Edited by:
Kyungmoo Paul Ryu, Abbott, United StatesReviewed by:
Vassilios Vassilikos, Aristotle University of Thessaloniki, GreeceChristopher Aldo Rinaldi, St Thomas’ Hospital, United Kingdom
© 2024 Antoun, Li, Kotb, Barker, Mavilakandy, Koev, Vali, Somani and Ng. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Ibrahim Antoun, aWEyNzdAbGVpY2VzdGVyLmFjLnVr