 Ying Wang1,†
Ying Wang1,† Carolin Ertl1,2,†
Carolin Ertl1,2,† Christina Schmitt1
Christina Schmitt1 Linda Hammann3
Linda Hammann3 Rafaela Kramer4
Rafaela Kramer4 Ulrich Grabmaier5
Ulrich Grabmaier5 Florian Schöberl6,7David Anz3,8
Florian Schöberl6,7David Anz3,8 Ignazio Piseddu3,8Giulia Pesch1
Ignazio Piseddu3,8Giulia Pesch1 Julio Vera4Waltraud Froehlich3
Julio Vera4Waltraud Froehlich3 Ludwig Weckbach5
Ludwig Weckbach5 Dirk Tomsitz1Carmen Loquai9
Dirk Tomsitz1Carmen Loquai9 Lisa Zimmer10Johanna Mangana11
Lisa Zimmer10Johanna Mangana11 Reinhard Dummer11Ralf Gutzmer12Kai-Christian Klespe13Henner Stege14
Reinhard Dummer11Ralf Gutzmer12Kai-Christian Klespe13Henner Stege14 Frank Meiss15Kai-Martin Thoms16
Frank Meiss15Kai-Martin Thoms16 Patrick Terheyden17
Patrick Terheyden17 Paul J. Bröckelmann18
Paul J. Bröckelmann18 Douglas B. Johnson19Lars E. French1,20
Douglas B. Johnson19Lars E. French1,20 Lucie Heinzerling1,2,4*
Lucie Heinzerling1,2,4*
- 1Department of Dermatology and Allergy, University Hospital, LMU Munich, Munich, Germany
- 2SERIO Registry, Munich, Germany
- 3Division of Clinical Pharmacology, Klinikum der Universität München, Munich, Germany
- 4Department of Dermatology, Friedrich-Alexander University Erlangen-Nürnberg (FAU) and University Hospital Erlangen (UKER), Deutsches Zentrum Immuntherapie (DZI) and Comprehensive Cancer Center Erlangen-European Metropolitan Area of Nürnberg (CCC-ER-EMN), Erlangen, Germany
- 5Department of Medicine I, LMU University Hospital, LMU Munich, Munich, Germany
- 6Department of Neurology, LMU University Hospital, LMU Munich, Munich, Germany
- 7German Center for Vertigo and Balance Disorders (DSGZ), LMU University Hospital, LMU Munich, Munich, Germany
- 8Department of Medicine II, LMU University Hospital, LMU Munich, Munich, Germany
- 9Department of Dermatology, Klinikum Bremen-Ost, Gesundheit Nord gGmbH, Bremen, Germany
- 10Department of Dermatology, University Hospital Essen & German Cancer Consortium (DKTK), Partner Site Essen/Duesseldorf, & National Center for Tumor Diseases (NCT)-West, Campus Essen, & Research Alliance Ruhr, Research Center One Health, University Duisburg-Essen, Essen, Germany
- 11Department of Dermatology, University Hospital Zurich, Zurich, Switzerland
- 12Department of Dermatology, Johannes Wesling Medical Center, Mühlenkreiskliniken (MKK), Ruhr University Bochum, Minden, Germany
- 13Skin Cancer Center Hannover, Department of Dermatology and Allergy, Hannover Medical School, Hannover, Germany
- 14Department of Dermatology, University Medical Center of the Johannes Gutenberg University Mainz, Mainz, Germany
- 15Faculty of Medicine, Department of Dermatology, Medical Center—University of Freiburg, Freiburg, Germany
- 16Department of Dermatology, University Medical Center Goettingen, Georg-August-University, Goettingen, Germany
- 17Department of Dermatology, University of Lübeck, Lübeck, Germany
- 18Department I of Internal Medicine, Center for Integrated Oncology Aachen Bonn Cologne Duesseldorf, University of Cologne, Cologne, Germany
- 19Department of Medicine, Vanderbilt University Medical Center, Nashville, TN, United States
- 20Dr. Philip Frost, Department of Dermatology and Cutaneous Surgery, University of Miami Miller School of Medicine, Miami, FL, United States
Background: Immune checkpoint inhibitor (ICI)-induced myocarditis is a rare immune-related adverse event (irAE) with a fatality rate of 40%–46%. However, irMyocarditis can be asymptomatic. Thus, improved monitoring, detection and therapy are needed. This study aims to generate knowledge on pathogenesis and assess outcomes in cancer centers with intensified patient management.
Methods: Patients with cardiac irAEs from the SERIO registry (www.serio-registry.org) were analyzed for demographics, ICI-related information (type of ICI, therapy line, combination with other drugs, onset of irAE, and tumor response), examination results, irAE treatment and outcome, as well as oncological endpoints. Cardiac biopsies of irMyocarditis cases (n = 12) were analyzed by Nanostring and compared to healthy heart muscle (n = 5) and longitudinal blood sampling was performed for immunophenotyping of irMyocarditis-patients (n = 4 baseline and n = 8 during irAE) in comparison to patients without toxicity under ICI-therapy (n = 4 baseline and n = 7 during ICI-therapy) using flow cytometry.
Results: A total of 51 patients with 53 cardiac irAEs induced by 4 different ICIs (anti-PD1, anti-PD-L1, anti-CTLA4) were included from 12 centers in 3 countries. Altogether, 83.0% of cardiac irAEs were graded as severe or life-threatening, and 11.3% were fatal (6/53). Thus, in centers with established consequent troponin monitoring, work-up upon the rise in troponin and consequent treatment of irMyocarditis with corticosteroids and –if required–second-line therapy mortality rate is much lower than previously reported. The median time to irMyocarditis was 36 days (range 4–1,074 days) after ICI initiation, whereas other cardiotoxicities, e.g. asystolia or myocardiopathy, occurred much later. The cytokine-mediated signaling pathway was differentially regulated in myocardial biopsies as compared to healthy heart based on enrichment Gene Ontology analysis. Additionally, longitudinal peripheral blood mononuclear cell (PBMC) samples from irMyocarditis-patients indicated ICI-driven enhanced CD4+ Treg cells and reduced CD4+ T cells. Immunophenotypes, particularly effector memory T cells of irMyocarditis-patients differed from those of ICI-treated patients without side effects. LAG3 expression on T cells and PD-L1 expression on dendritic cells could serve as predictive indicators for the development of irMyocarditis.
Conclusion: Interestingly, our cohort shows a very low mortality rate of irMyocarditis-patients. Our data indicate so far unknown local and systemic immunological patterns in cardiotoxicity.
1 Background
Immune checkpoint inhibitors (ICI) have revolutionized tumor therapy and are effective in multiple tumor entities (1, 2). However, they also induce a broad spectrum of immune-related toxicities, including colitis, hepatitis, pneumonitis, thyroiditis, myositis, hypophysitis, dermatitis, and cardiotoxicity (3–6). ICI-related myocarditis (irMyocarditis) emerged as a significant concern, occurring in 0.5%–1% of ICI recipients (7–10), with a median onset of 34 days post-treatment initiation (11). Alarmingly, irMyocarditis historically carried a mortality rate of 40%–46%, which is the highest of any irAE and 10-fold higher than myocarditis from other causes (12, 13). The clinical presentation of irMyocarditis ranges from asymptomatic troponin elevation to heart failure, with ventricular arrhythmia, severe conduction disorders, or cardiogenic shock and may co-occur with symptoms of myositis and myasthenia gravis (3, 14).
Even though, early, and high dose steroids seem to be associated with a lower risk of death, the outcome of cardiac irAE is often hard to predict (15, 16). To ensure diagnosis, current guidelines recommend conducting various examinations and, in case of cardiovascular complications, the referral to cardiology (6, 17, 18). Up to now, diagnostics, monitoring, and therapy for cardiac irAEs under immunotherapy are still largely based on experience or, if one exists, guided by the clinic's internal algorithm. Therefore, monitoring for cardiac events comes with a large burden of unnecessary assessments and a reliable evidence base for treatment options is still lacking. IrMyocarditis can be induced by activation of autoreactive T-lymphocytes directed against heart muscle (19). The target antigens may overlap with striated muscle and thus create an overlap of irMyocarditis, irMyositis and myasthenia-like syndrome (14). Recently, single-cell RNA sequencing coupled with T cell receptor analysis revealed the enrichment of cytotoxic T cells, inflammatory macrophages, and conventional dendritic cells in heart tissue biopsies from patients with irMyocarditis (13). Notably, cardiac and tumor infiltrates from melanoma patients with fatal irMyocarditis shared high-frequency T cell receptor sequences, suggesting potential tumor-expressed antigen triggers for ICI-induced myocarditis (20). Autopsy specimens from patients with irMyocarditis have demonstrated cardiac infiltration primarily by T-lymphocytes and macrophages, with notable absence of B cells or antibody deposits (20). Another study identified an increase of CD8+ effector memory T-cells re-expressing CD45RA (TEMRA) in peripheral blood of irMyocarditis patients based on time-of-flight mass cytometry (CyTOF) (21). This would suggest that targeting cytotoxic CD8+ T cells may be effective in treating fulminant myocarditis.
Tissue transcriptomics of irMyocarditis has rarely been reported to date. In one study, bulk RNA sequencing of myocardial tissue from patients with irMyocarditis indicated that irMyocarditis was associated with multiple inflammatory pathways, especially interferon responses. Several interferon-stimulated genes were upregulated, including CXCL9, MDK, and GBP521 (22). In a murine study, CD8+ T cells of mice with myocarditis demonstrated a unique transcriptional profile consisting of proinflammatory and cytotoxicity markers (GZMB, GNLY, CST7, NKG7, KLRB1, and IL32), and myocardial-tropic chemokines CCL5, CCL4, and CCL4L2 (21).
This study analyzed a multicenter cohort of patients with cardiac irAEs with respect to symptoms, outcome and longitudinal changes of immunophenotype in comparison to patients without irAEs. Additionally, gene expression analyses of the corresponding heart muscle biopsies were conducted.
2 Method and design
2.1 Study population and design
This retrospective multicenter study includes a total of 51 patients from 12 centers (Cologne, Erlangen, Essen, Freiburg, Goettingen, Hannover, Luebeck, Mainz, Minden, Munich, Nashville, Zurich) with confirmed cardiac irAE drawn from our SERIO-registry and was approved by the ethics committee of the LMU University Hospital Munich (No. 20-1122). The diagnosis of irMyocarditis was confirmed by cardiologists at the corresponding center, who assessed symptoms, ECG alterations, troponin levels, and functional or structural changes in cardiac imaging, alongside a confirmed temporal association with the administration of ICIs. Cardiac MRIs were conducted on 33 patients, revealing findings consistent with irMyocarditis, such as late gadolinium enhancement, myocardial edema, wall motility disorders, and/or ischemia. Furthermore, endomyocardial biopsy results from 18 patients showed evidence of toxic damage to myocardial cells, including interstitial fibrosis, degenerative changes, and increased infiltration of lymphocytes, especially T cells, and CD68-positive macrophages, further supporting the diagnosis. If available, we collected creatine kinase (CK), creatine phosphokinase-MB (CK-MB), troponin T, and N-terminal prohormone of brain natriuretic peptide (NT-proBNP) serum levels at peak, as well as examination results of electrocardiogram (ECG), echocardiography (Echo) with left ventricular ejection fraction (LVEF), cardiac magnetic resonance imaging (MRI), and coronary angiography.
Clinical data was gathered using the international web-based Side Effect Registry Immuno-Oncology (SERIO; www.serio-registry.org). It was initiated in cooperation with the Paul-Ehrlich-Institute, to document rare, complex, or therapy-refractory side effects induced by immunotherapies. Within SERIO patients’ demographics, tumor entity, ICI therapy applied, tumor outcome, as well as type of irAE, irAE onset, grade, treatment and outcome are documented. The grading of irAEs followed the Common Terminology Criteria for Adverse Events (CTCAE) version 5.0. IrAE outcome was classified as resolved, improved, resolved with sequelae, or ongoing. The classification of completely “resolved” cardiac irAEs refers to cases where all cardiac symptoms and abnormalities associated with the irAE have disappeared. “Improved” defines irAE cases where there is a noticeable enhancement in cardiac irAE symptoms and/or abnormalities but which haven't entirely disappeared. “Resolved with sequelae” indicates that while the symptoms have subsided, there are residual effects or complications of the cardiac irAE, e.g., elevated troponin levels, remaining. “Ongoing” signifies cardiac irAE cases where symptoms and abnormalities persist without any significant improvement or resolution. Ethical approval for analyses from the SERIO registry was granted (Erlangen Nr. 2_20 B, Erlangen Nr. 17_16 Bc). SERIO was queried for cases of cardiac irAEs in February 2024.
For lab investigations participants gave their informed written consent prior to analysis. In total, peripheral blood mononuclear cells (PBMCs) from 19 patients were analyzed longitudinally for immunophenotyping at baseline and during ICI-therapy or during irAE. PBMCs from irMyocarditis patients (n = 4 baseline and n = 8 during irAE) were compared to patients without toxicity under ICI-therapy (n = 4 baseline and n = 7 during ICI-therapy). Heart muscle biopsies included irMyocarditis patients from Erlangen, Luebeck, Munich (D), and Zuerich (CH) (n = 11 available for lab investigations). Healthy heart muscle biopsies were obtained from pediatric cardiac surgery (n = 5). The healthy muscle was from a biobank that captured heart muscle from patients with valve reconstruction.
2.2 Blood sample processing and flow cytometry
PBMCs were isolated from lithium heparin blood samples by density gradient centrifugation with Ficoll-Paque density-gradient centrifugation followed by a cryopreservation with X-VIVO medium (Lonza) enriched with 20% fetal bovine serum (FBS, Pan Biotech) as well as with 10% DMSO (Thermo Fisher) and stored in liquid nitrogen. PBMCs were obtained from 8 patients with irMyocarditis and 11 ICI-patients without development of toxicities.
Thawed PBMCs were rested for one hour in RPMI medium + 10% FCS + 1% Pen/Strep + 1% L-Glutamine. Prior to staining, cells were incubated with human TrueStain Fc blocking reagent (Biolegend). Cells were then incubated (30 min, 4 °C) with eBioscience Fixable Viability Dye eFluor506 (Invitrogen) and the surface antibody mix (Table 1) in PBS. After fixation and permeabilization with eBioscience fixation/permeabilization reagent (Invitrogen; 30 min, 4 °C) and washing, cells were incubated (30 min, 4 °C) with the intracellular/intranuclear antibody mix (Table 1) and then measured the same day on an LSR Fortessa Cell Analyzer (BD Biosciences). FlowJo software (10.10.1) (BioSciences) was used for analysis.
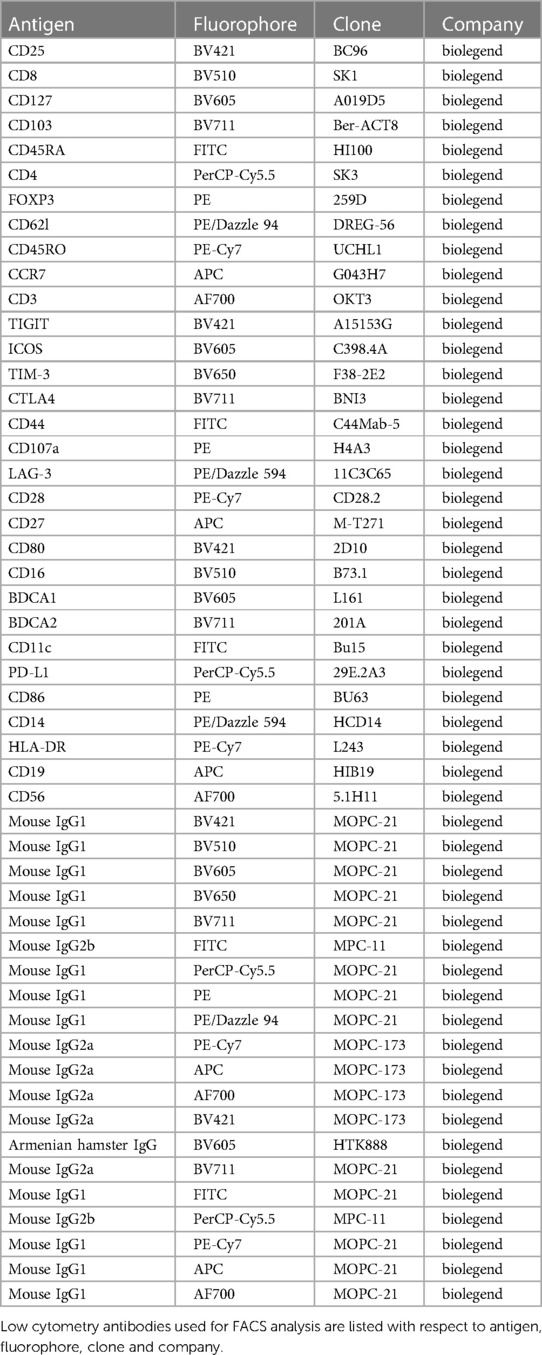
Table 1. The list of FACS antibodies used for PBMC.
2.3 RNA isolation
Total RNA was isolated from heart muscle specimens using TRIzol™ Reagent (Thermo Fisher Scientific, Germany) according to the manufacturer's instructions.
2.4 Nanostring analysis
Gene expression was analyzed using the nCounter PanCancer Immune Profiling Panel™ (human) (Nanostring, XT-CSO-HIP1–12). Sample detection and analysis were completed on a nCounter® Digital Analyzer. RNA gene expression analysis was performed using the nCounter SPRINT Profiler and the nCounter MAX Analysis System (NanoString Technologies, Inc.). Statistical analysis of gene expression results was implemented with the nSolver Analysis Software (NanoString Technologies, Inc.) and ROSALIND® (ROSALIND, Inc., San Diego, CA) (https://rosalind.bio/). Pathway analysis was conducted using EnrichR and EnrichR-KG, applying the databases KEGG 2021 Human and GO Biological Process 2021.
2.5 Unsupervised and statistical analysis
Raw data processing, quality control and normalization were performed using the NanoStringQCPro package for the R (version 4.1.0) environment. Quality control (QC) was performed with an imaging QC of >80% field of view registration, binding density QC within 0.05–2.25 range, and positive control scaling factors within a range of 0.3–3. In the differential expression analysis, a false discovery rate (FDR, Benjamini and Hochberg) adjusted p-value of ≤0.05 was applied as cutoff. One sample two-tailed unpaired Student's t-test, one sample Wilcoxon test and Mann–Whiney U-test were used to test statistical significance. *: p ≤ 0.05, **: p ≤ 0.01, and ***: p ≤ 0.001.
3 Results
In total, 51 patients (19 female—32 male patients; 37.2%–62.7%) with various tumor entities (Table 2) were included in this study investigating cardiac irAE. Most patients were diagnosed with cutaneous melanoma (31/51; 60.7%), followed by uveal melanoma (4/53; 7.8%) and melanoma of unknown primary (MUP) (3/51; 5.9%). Other reported tumor entities included, but were not limited to, head and neck carcinoma (2/51; 3.9%), neuroendocrine bladder cancer (5/51; 3.9%); breast cancer (1/51; 2.0%) and renal cell carcinoma (1/51; 2.0%). Applied checkpoint inhibitors included anti-cytotoxic T lymphocyte antigen 4 (CTLA-4), anti-programmed cell death 1 (PD-1), and anti-programmed cell death 1 ligand 1 (PD-L1) antibodies. Most frequently applied ICI regimens were combined therapy with ipilimumab and nivolumab (21/53; 39.6%), pembrolizumab (15/53; 28.3%) and nivolumab (11/53; 20.8%) in monotherapy. Reported cardiac irAEs included myocarditis (48/53; 90.5%), myocardiopathy (1/53; 1.9%), myocardial fibrosis (1/53; 1.9%), pericarditis (1/53; 1.9%), ventricular arrhythmia (1/53; 1.9%) and asystolia (1/53; 1.9%). Altogether, 53 cardiac irAE were documented, since 2 of 51 patients developed a second cardiac irAE. Three quarter of patients showed another irAE (72.5%; 37/51) with irMyositis (15/52; 28.8%) and irHepatitis (13/52; 24.5%) being the most frequently reported ones. According to CTCAE grading, 83.0% of cardiac irAEs were severe or life-threating (Grade ≥ 3 adverse events) (Figure 1) and 11.3% were fatal (6/53). IrMyocarditis, in particular, was fatal in 8.3% of cases (4/48). Death due to tumor progression occurred in 31.4% (16/51) of patients upon longitudinal analysis.
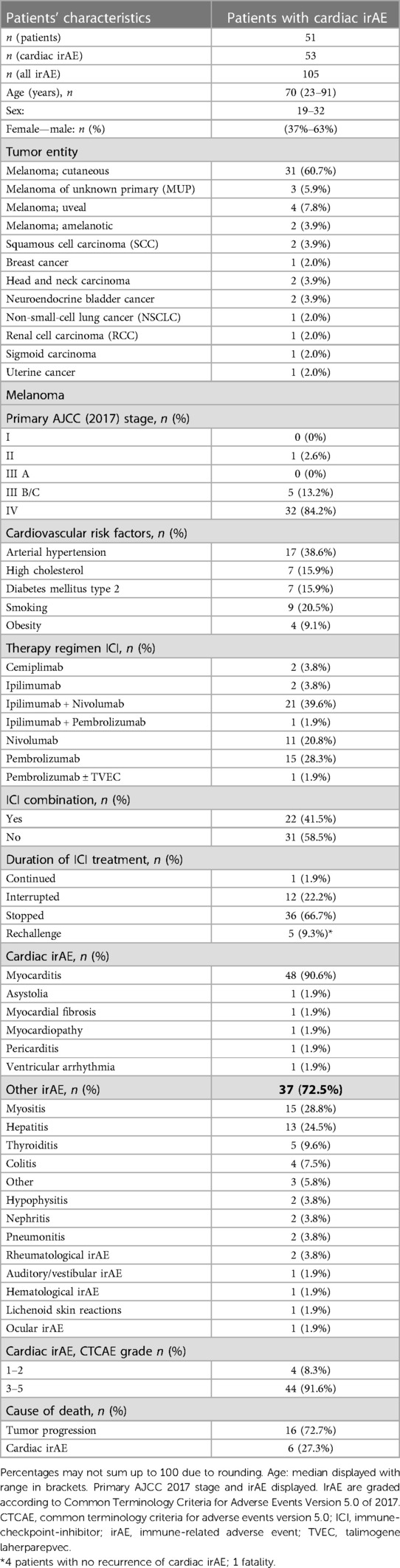
Table 2. Baseline characteristics of patients with immune-related cardiac adverse events associated with immunotherapy.
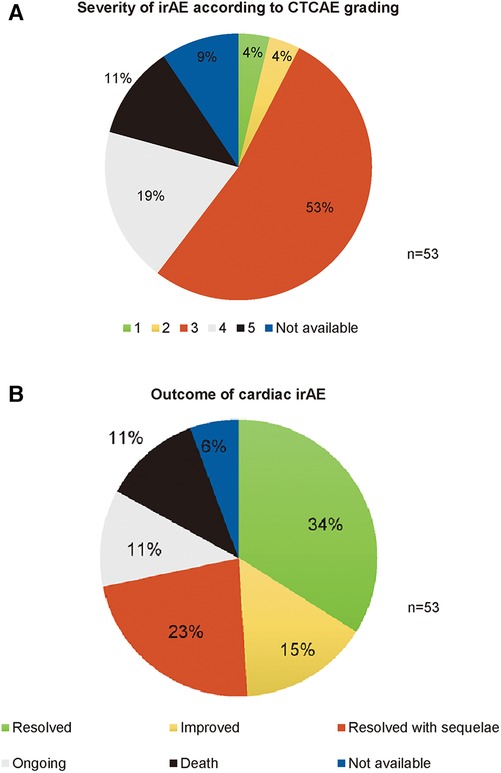
Figure 1. Documented cardiac irAE severity and outcome within the side effect registry immuno-oncology (SERIO). (A) Severity of irAE (grade 1-5 CTCAE). Data was available for 90.6% (48/53) of cases. (B) Outcome of irAE. Outcome data was available for 94.3% (50/53) of cases. CTCAE, common terminology criteria for adverse events version 5.0; IrAE, immune-related adverse event.
3.1 Signs and symptoms
The median time from initiation of ICI therapy to onset of cardiac irAEs was 37 days with a wide range (4–1,074 days). The time to onset of irMyocarditis significantly differed from other cardiac irAEs. In total, irMyocarditis occurred early after ICI initiation with a median time to onset of 36 days (range 4–1,074 days), whereas other cardiac irAEs had a median time to onset of 101 days (range 28–119 days). More than half of all patients (58.8%; 30/51) initially presented with symptoms like dyspnea (63.3%; 19/30) or chest pain (23.3%; 7/30) while 41.2% were asymptomatic. In over 50.0% of irAE cases, which ultimately resolved completely, elevated laboratory parameters (Troponin T, CK, CK-MB, and NT-proBNP) were initially observed (Table 3). In those patients that fully recovered, echocardiographic findings were predominantly within the normal range (92.9%; 13/14) and coronary angiographies presented with no signs of stenosis (75.0%; 9/12). The results of ECG and cardiac MRI in this cohort were nonspecific, showing a distribution of 50.0% abnormal and 50.0% normal results. Notably, biopsies of the myocardium of patients who fully recovered were indicative of myocarditis in 7 out of 8 cases (87.5%). Interestingly, in the cohort that ultimately led to fatality, cardiac diagnostic assessments were not performed in more than 50.0% of cases. Upon conducting the investigations in this cohort, abnormalities were observed in ECG (100.0%; 3/3) and coronary angiography (100.0%; 2/2), whereas the echocardiogram (66.7%; 2/3), LVEF (100.0%; 3/3), and MRI (100.0%; 1/1) findings were predominantly within the normal range (Table 3).
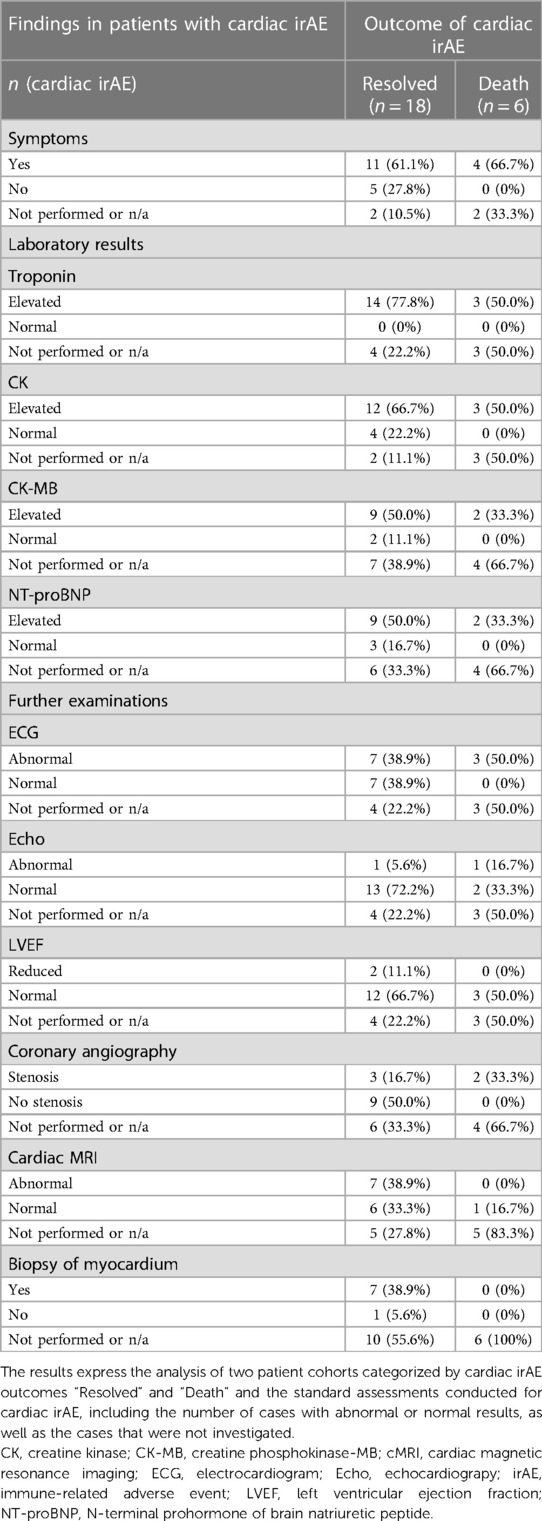
Table 3. Findings in patients with cardiac irAE.
3.2 IrAE treatment and outcome
In total, 92.5% (49/53) of patients with cardiac irAE were treated with systemic steroids, 5.7% (3/53) were solely treated with symptomatic therapies such as beta blockers and antihypertensive drugs, and 17.0% (9/53) required second-line therapy for steroid-refractory or steroid-dependent cardiac irAEs. As second-line immunosuppressants, intravenous immunoglobulins (IVIG), infliximab, anti-thymocyte globulin (ATG), mycophenolate mofetil (MMF) were applied. Optimal response rates of 90.0% (4/5) were attained through the administration of IVIG. In total, 72.5% (37/51) of patients required hospitalization.
Data evaluation of cardiac irAE outcomes indicated that 34.0% (18/53) of cases completely resolved, 15.1% (8/53) significantly improved, while 22.6% (12/53) resolved with relevant sequelae and 11.3% (6/53) were still ongoing, with an overall irAE response rate of 71.7% (Figure 1). In 11.3% (6/53) of cases, cardiac irAEs led to death (Figure 1). In our study, 5 patients received ICI rechallenge after cardiac irAE. In 80.0% (4/5) of cases ICI was successfully applied without recurrence of cardiac toxicities, while in one case the patient died early after ICI re-initiation due to exacerbated cardiac symptoms. In one case, ICI rechallenge was successfully administered with prophylactic steroid treatment. Tumor response in patients with cutaneous melanoma was assessed at the time of irAE: Complete response was reported in 5.9% (2/34), partial response in 8.8% (3/34), stable disease in 20.6% (7/34) and progressive disease in 32.4% (11/34) of patients (RECIST 1.1). Patients showed a median PFS of 8 months (range 0–60 months) and a median overall survival (OS) of 17 months (range 0–130 months). In total, 11.8% (4/34) of patients were treated in an adjuvant setting with recurrence-free survival between 1 and 13 months.
3.3 Gene expression analysis reveals substantial differences in cytokine pathways between irMyocarditis and healthy controls
To elucidate the gene expression signatures of irMyocarditis, heart tissue of 12 irMyocarditis patients was compared to heart tissue of 5 healthy controls using nCounter® Digital Analyzer. After normalizing the raw data, with a ratio >1.5 or <1.5 and p < 0.05 as the screening criteria for differential expression genes (DEG), the DEGs analysis identified a set of 113 differentially regulated genes in irMyocarditis compared to healthy controls, of which 99 genes were upregulated and 14 were downregulated (Figure 2A). The top five upregulated genes in irMyocarditis were IL6R (logFC 2.1, adjusted p-value 3.34 × 10−5), HLA-C (logFC 3.62, adjusted p-value 6.31 × 10−4), HLA-E (logFC 3.58, adjusted p-value 7.19 × 10−4), STAT2 (logFC 2.64, adjusted p-value 8.25 × 10−4) and IKBKB (logFC 2.41, adjusted p-value 9.22 × 10−4). The top five downregulated genes in irMyocarditis were DDX43 (logFC −10.04, adjusted p-value 3.01 × 10−4), HMGB1 (logFC −2.75, adjusted p-value 1.90 × 10−3), SYT17 (logFC −5.17, adjusted p-value 3.64 × 10−3), S100A12 (logFC −7.79, adjusted p-value 5.43 × 10−3) and IL13RA2 (logFC −9.45, adjusted p-value 9.85 × 10−3). The 113 DEGs were investigated using gene set enrichment and pathway analysis (Figure 2B), demonstrating the most significant pathways of the DEGs: (1) Cytokine-mediated signaling pathway (p = 6.6445 × 10−37), (2) Cellular response to cytokine production (p = 5.5129 × 10−32), (3) Positive regulation of cytokine production (p = 1.4357 × 10−30), (4) Hematopoietic cell lineage (p = 1.4458 × 10−22), (5) Epstein-Barr virus infection (p = 2.5618 × 10−22), (6) Cell adhesion molecules (p = 2.858 × 10−22), (7) Th17 cell differentiation (p = 2.6598 × 10−20), (8) Human T-cell leukemia virus 1 infection (p = 3.6892 × 10−20), (9) Regulation of interleukin-6 production (p = 1.724 × 10−15), (10) Innate immune response (p = 6.7096 × 10−15). Thus, the regulation of cytokines, especially type I IFNs and NFkB signaling was differently shaped in irMyocarditis compared to healthy control, indicating might also be relevant—IL-6 can be therapeutically inhibited.
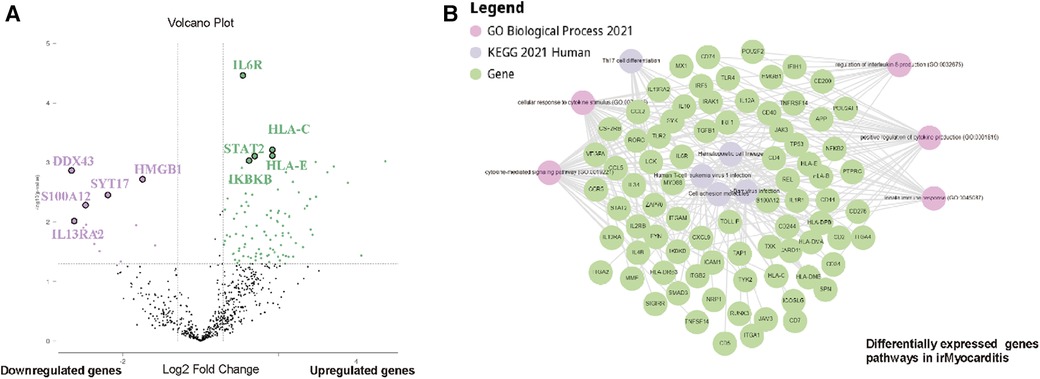
Figure 2. Bulk RNAseq reveals substantial differences in cytokine production pathways between irMyocarditis and healthy control. (A) Volcano plot shows 14 genes significantly downregulated in in irMyocarditis cohort and healthy heart cohort (violet) and 99 genes significantly upregulated in irMyocarditis compared to healthy control (green) (Log2 fold change ≤−1.5 or ≥1.5, p-value ≤0.05). Statistics were performed using Rosalind® software. (B) Enriched pathway analysis of significantly differentially expressed genes performed with STRING®, gene ontology and KEGG® reveals networks of enriched genes in irMyocarditis cohort and healthy heart cohort.
3.4 Enhanced activation of Treg cells and dendritic cells related to irMyocarditis development
Based on the analyzed gene expression patterns of immune response mechanisms, we next focused on characterization of the profile of the systemic immune response. We performed longitudinal analysis of PBMCs from irMyocarditis patients (baseline and time of adverse event). In longitudinal analysis, PBMCs of patients during irMyocarditis (ae) demonstrated significantly decreased frequencies of CD103+ activated CD4+ T cells and increased CD103+ activated CD4+ Treg cells compared to baseline (bl) whereas activated T cells as well as Treg cells showed no significant difference between bl and ae. Furthermore, no significant difference in CD103+ activated CD8+ T cells and activated CD8+ Treg cells was observed. Integrin CD103 is related to tissue residency in the context of inflammation and cancer (Figures 3A,B). The peripheral T cell compartment was investigated to determine the relative abundance of various T cell phenotypes, including effector-like T cells (Teff), effector memory-like T cells (Tem), central memory-like T cells (Tcm), and naïve T cells (Tn). This analysis utilized established markers such as CD45RA, CD45RO, CD62l, CCR7, and CD127. The frequency of Tn, Tcm, Tem, and Teff showed no significant difference neither in CD4+ nor in CD8+ T cells (Supplementary Figures S1A,B). Furthermore, markers associated with T cell activation (CD44, CD27, CD28, ICOS, and CD107a) and exhaustion (CTLA4, LAG3, TIM3, and TIGIT) were examined to gain further functional insights into differences in systemic T cell immunity. The CD8+ T cells showed an increased expression of CD44 which was not observed on CD4+ T cells (Figure 3C). Furthermore, we focused on the function and phenotype of antigen-presenting cells (APCs). We determined three different DC subsets in peripheral blood including BDCA1- cDC, BDCA1+ cDC, and monocyte-derived DC (moDC) based on the markers CD11c, CD19, CD56, CD14, BDCA1, and HLA-DR and determined the expression of the activation markers CD80, CD86 and HLA-DR as well as the inhibitory molecule PD-L1. Regarding DC, we found significantly higher frequencies of activated DC during the adverse event compared to baseline in irMyocarditis patient's PBMC as determined by the expression of the costimulatory molecule CD80 (Figure 3D). Besides, for DC subsets, the expression of the coinhibitory molecule PD-L1 on BDCA1- cDC was significantly reduced in ae compared to bl, indicating the effect might be related to the development of irMyocarditis (Figure 3E). The expression of CD80, CD86, and the MHC class II molecule HLA-DR on BDCA1- cDC, BDCA1+ cDC, and moDC showed no significant difference between ae and bl (Supplementary Figures S1C–E). To summarize, the peripheral T cell compartment of irMyocarditis patients showed ICI-driven enhanced levels of activated CD4+ Treg cells, CD44, CD80, PD-L1 expression on DC, and reduced levels of activated CD4+ T cells.
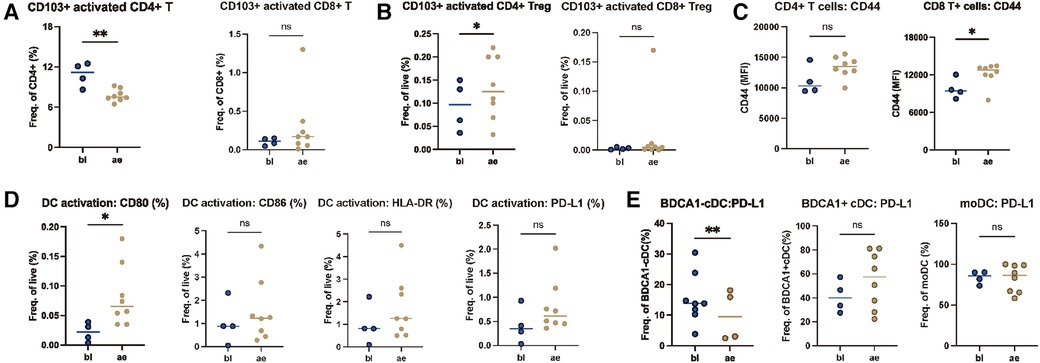
Figure 3. Enhanced activated Treg cells driven by ICI in irMyocarditis patient. PBMCs of patients with ae-irMyocarditis (n = 8) and bl (n = 4) were analyzed via flow cytometry. Distribution of activated T cells, Treg cells and other T cell phenotypes (Tn = naive T cells, Tcm = central memory T cells, Tem = effector memory T cells, Teff = effector T cells) in CD4+ and CD8+ T cells was determined. CD4+ and CD8+ T cells were also analyzed for expression of activation (CD27, CD28, ICOS, CD107a, CD44) and exhaustion (CTLA4, TIM-3, TIGIT, LAG3) markers using FACS. The abundance and activation of dendritic cell (DC) subsets was analyzed [activated DC, BDCA1- DC, BDCA1+ DC and monocyte derived DC (moDC)] using flow cytometry. (A) The frequencies of CD4+ and CD8+ in CD103+ activated CD4+ T cells and CD103+ activated CD8+ T cell. (B) The frequencies of live cells in CD103+ activated CD4+ Treg cells and CD103+ activated CD8+ Treg cells. (C) CD4+ and CD8+ T cells were analyzed for expression of activation CD44 markers using FACS. (D) The frequencies of live cells in CD80+, CD86+, HLA-DR, PD-L1 activated DC cells. (E) The frequencies of BDCA1- DC in PD-L1+ BDCA1- DC, PD-L1+ BDCA1+ DC and PD-L1+ moDC. IrAE, immune-related adverse event; bl, baseline.
3.5 Tem cell and exhaustion markers dominate in irMyocarditis compared to patients without toxicity
Following the longitudinal immunophenotype changes in irMyocarditis patients from baseline to adverse event, we analyzed the irMyocarditis patients during the adverse events in comparison to patients who did not develop toxicities while undergoing ICI-therapy toxicities (Ø tox ICI-patients). PBMCs of irMyocarditis patients showed significantly higher frequencies of CD4+ Treg cells and higher levels of activated CD8+ T cells compared to Ø tox ICI-patients (Figure 4A). Interestingly, different from previous results, irMyocarditis patients showed significantly higher frequencies of CD4+ Tcm cells and CD4+ Teff cells compared to Ø tox ICI-patients. Furthermore, we observed a significant decrease in CD4+ Tem cells and CD8+ Tem cells in irMyocarditis compared to Ø tox ICI-patients (Figure 4B), whereas no significant alterations of CD4+ naïve T cells and CD8+ naïve T cells could be observed (Supplementary Figure S2A). Noticeably, among the tested functional markers only CD28 of CD4+ T cells was elevated in Ø tox ICI-patients (Supplementary Figures S2B,C). Of note, both CD4+ as well as CD8+ T cells of irMyocarditis patients showed significantly increased expression of the T cell exhaustion marker TIGIT, however a decrease of TIM-3 expression on CD8+ T cells (Figure 4C). For other T cell exhaustion markers, the expression of LAG3 was elevated in CD4+ T cells but not in CD8+ T cells in irMyocarditis compared to Ø tox ICI-patients (Supplementary Figure S2D). The expression of CTLA4, however, was not different in irMyocarditis and Ø tox ICI-patients neither in CD4+ nor in CD8+ T cells (Supplementary Figure S2E). Further analysis of APC cells showed significantly higher expression of CD86 on activated DC, BDCA1- cDC, BDCA1+ cDC, and moDC (Figure 4D). Regarding other costimulatory molecules, we found significantly higher frequencies of CD80 on BDCA1- DC as well as the HLA-DR on BDCA1- cDC, BDCA1+ cDC in irMyocarditis patients, pointing towards an increase in cDC activation potentially induced by irMyocarditis (Figures 4E,F). The expression of CD80 markers on activated DC, BDCA1+ DC, and moDC, and the expression of HLA-DR on moDC and activated DC, however, was not statistically different between irMyocarditis and Ø tox ICI-patients (Supplementary Figures S2F,G). Strikingly, the expression of PD-L1 showed a significant increase in all DC subsets in irMyocarditis patients (Figure 4G). Furthermore, in our irMyocarditis cohort, circulating B cells were significantly less abundant than in Ø tox ICI-patients (Supplementary Figure S2H). Lastly, a difference between CD56high/CD16- NK cells and CD56low/CD16+ NK cells could not be detected between irMyocarditis and Ø tox ICI-patients, which indicated the cardiotoxicity might not be related to NK cell-mediated cytotoxicity (Supplementary Figure S2I). Taken together, these data suggest that irMyocarditis is characterized by activation of T cells, particularly Tem cells, additionally the exhaustion markers TIGIT, TIM and LAG3 were identified to be of greater importance in irMyocarditis patients.
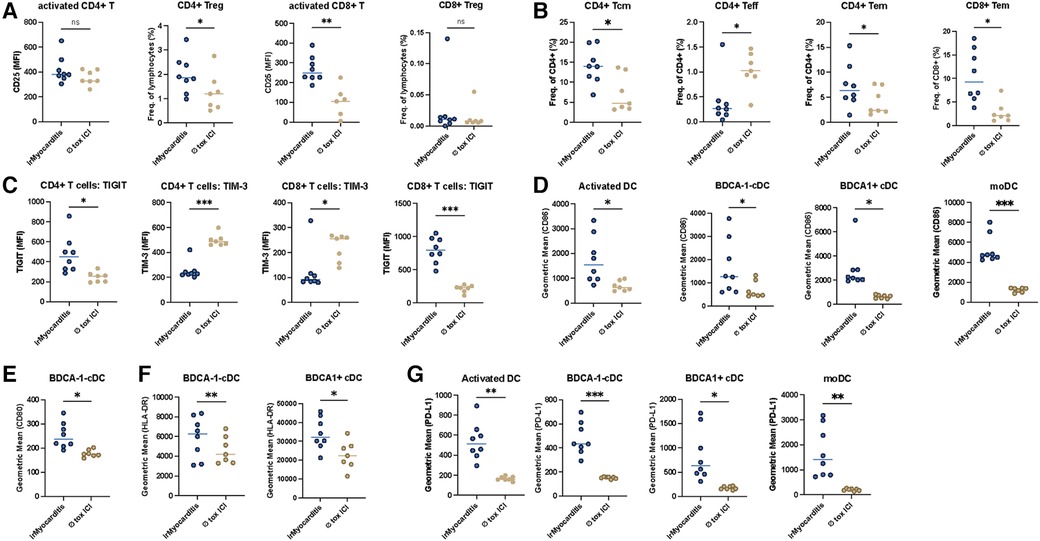
Figure 4. Tem cell and exhaustion markers dominate in the induction of cardiotoxicity in irMyocarditis patients. PBMCs of patients with irMyocarditis (n = 8) and patients undergoing checkpoint-inhibitor therapy without development of toxicities (Ø tox ICI, n = 7) were analyzed via flow cytometry. Distribution of activated T cells, Treg cells, Tn, Tcm, Tem, Teff in CD4+ and CD8+ T cells was determined. CD4+ and CD8+ T cells were also analyzed for expression of activation (CD27, CD28, ICOS, CD107a, CD44) and exhaustion (CTLA4, TIM-3, TIGIT, LAG3) markers using FACS. The abundance and activation of dendritic cell (DC) subsets were analyzed using FACS. (A) The expression level of CD25 in activated CD4+, CD8+ T cell and the frequencies of lymphocytes of CD4+ Treg, CD8+ Treg cells (B) The frequencies of CD4 in CD4+ Tcm, CD4+ Teff, CD4+ Tem, and CD8+ Tem. (C) The expression level of TIGIT, TIM3 in CD4+ and CD8+ T cells. (D) The expression level of CD86 in activated DC, BDCA1- DC, BDCA1+ DC cells. (E) The expression level of CD80 of BDCA1- DC. (F) The expression level of HLA-DR of BDCA1- DC, BDCA1+ DC. (G) The frequencies of PD-L1 in activated DC, BDCA1- DC, BDCA1+ DC and moDC.
3.6 LAG3 and PD-L1 as potential indicators to predict the occurrence of irMyocarditis
Furthermore, we aimed to analyze the baseline immunophenotype of PBMC of irMyocarditis patients in comparison to Ø tox ICI-patients before initiation of ICI-therapy. First, we determined the frequencies of activated T cells in peripheral blood. Here, CD103+ activated CD4+ T cells and CD103+ activated CD4+ Treg cells showed significant expansion in bl-irMyocarditis compared to bl-Ø tox ICI-patients,. whereas the abundance of CD103+ activated CD8+ T cell CD103+ activated CD8+ Treg cell were unaltered (Figures 5A,B). Regarding other phenotypes of T cells, we found no difference in frequencies of Tn, Tcm, Tem, and Teff neither in CD4+ nor in CD8+ T cells between bl-irMyocarditis patients and bl-Ø tox ICI-patients (Supplementary Figures S3A,B). To gain additional functional insights, we analyzed activation and exhaustion markers of the T cells. Interestingly, most activation markers showed significantly higher levels in bl-irMyocarditis, such as CD107a in CD8+ T cells, and ICOS in both CD4+ and CD8+ T cells, however CD28 was significantly higher in CD4+ T cells in bl-Ø tox ICI-patients compared to bl-irMyocarditis (Figure 5C). Expression of CD44, as well as CD27, showed no difference between bl-irMyocarditis and bl-Ø tox ICI-patients (Supplementary Figures S3C,D). Markedly, expression of the exhaustion marker LAG3 was highly elevated in both CD4+ and CD8+ T cells in bl-irMyocarditis. Significantly enhanced expression of CTLA4 in CD4+ T cells and TIGIT in CD8+ T cells, however a significant decrease of TIM-3 in CD4+, respectively, was detected in bl-irMyocarditis compared to bl-Ø tox ICI-patients (Figure 5D). In DC subsets, we observed an increased expression of PD-L1 on activated DC, BDCA1- cDC, BDCA1+ cDC, and moDC in bl-irMyocarditis patients (Figure 5E). Additionally, in our bl-irMyocarditis cohort, circulating B cells were significantly lower abundant than in bl-Ø tox ICI-patients. A significantly higher amount of moDC could be detected in the bl-irMyocarditis cohort compared to bl-Ø the tox ICI cohort (Figure 5F). To summarize, these data suggest that expression of exhaustion markers, particularly LAG3 on T cells and PD-L1 on DCs at baseline could be used as indicators to predict the occurrence of irMyocarditis.
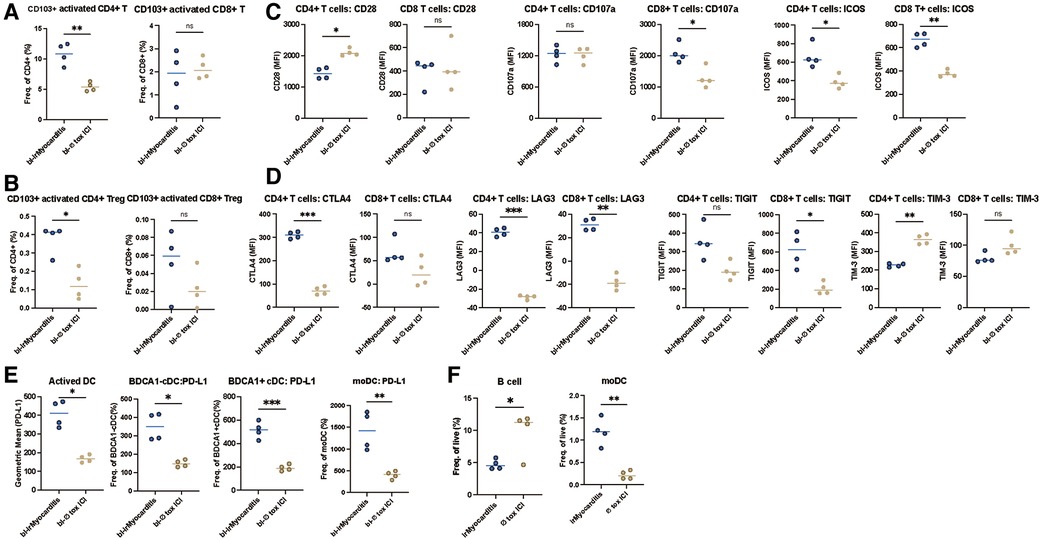
Figure 5. LAG3 and PD-L1 can be used as indicators to predict the occurrence of irMyocarditis. PBMCs of patients with bl-irMyocarditis (n = 4) and bl-tox ICI (n = 4) were analyzed via flow cytometry. Distribution of activated T cells, Treg cells, Tn, Tcm, Tem, Teff in CD4+ and CD8+ T cells was determined. CD4+ and CD8+ T cells were also analyzed for expression of activation (CD27, CD28, ICOS, CD107a, CD44) and exhaustion (CTLA4, TIM-3, TIGIT, LAG3) markers using FACS. The abundance and activation of dendritic cell (DC) subsets were analyzed using FACS. (A) The frequencies of CD4, CD8 in activated CD4+, CD8+ T cells. (B) The frequencies of CD4, CD8 in CD103+ activated CD4+ Treg, CD8+ Treg cells (C) The expression level of CD28, CD107a, and ICOS in CD4+ and CD8+ T cells. (D) The expression level of CTLA4, LAG3, TIGIT, and TIM3 in CD4+ and CD8+ T cells. (E) The expression level of PD-L1 in activated DC, BDCA1- DC, BDCA1+ DC, and moDC cells. (F) The frequencies of live cells of B cells and moDC.
4 Discussion
In recent years, the use of ICIs has been expanding due to their effectiveness in various tumor entities and even early tumor stages. Cardiotoxicity is a rare but often fatal side effect that is difficult to diagnose and hard to predict (23). Therefore, we aimed to investigate options for better patient monitoring including knowledge of pathogenesis and outcome under intensified management and to unravel potential immunophenotypes including suggestions for predictive signatures and transcriptomic pathways associated with development of cardiotoxicity.
In this multicenter study, we report on 51 patients with cardiac irAE induced by checkpoint inhibitor therapy. The analysis of laboratory results revealed elevated cardiac markers (Troponin, CK, CK-MB, NT-proBNP) in the majority of cardiac irAE patients. Subsequent examinations, such as ECG, Echo, LVEF, and cardiac MRI, commonly considered in the diagnostic work-up, were often nonspecific. But, as shown in Table 3, omission to perform further investigations is highly associated with an elevated mortality rate. Noteworthy changes were predominantly shown in cardiac biopsies. Since myocarditis is often a focal process in the myocardium especially in the early stages and due to the challenging procedure (24), we emphasize the need to be cautious of false-negative results. To further strengthen the validity of biopsy results and to minimize the risk of complications, those should be performed based on MRI [including late gadolinium enhancement (LGE)] findings.
In accordance with other reports with an onset of 30 days (25), irMyocarditis occurred early after ICI initiation, i.e., with a median of 36 days. Interestingly, in over 72% of patients another irAE occurred at the same time as the cardiac event. When cardiac irAEs are diagnosed, early initiation of high-dose steroids is of crucial importance (15). Patients with steroid-resistant irMyocarditis historically have the highest mortality rate of up to 43.7% (16). Treatment of steroid-refractory irAEs is largely based on expert opinions, which emphasizes the need for clinical studies. In our cohort, IVIGs were successfully applied as second-line immunosuppressants for cardiac irAE recalcitrant to steroids and led to high response rates as reported previously by Norwood et al. (26). While there are varying results on ICI rechallenge in cardiac irAE, with one case without recurrence of irAE, and another case, that resulted in mortality (3, 27), in 4 out of 5 patients from our cohort, re-initiation of ICIs after irAE resolution was feasible, while one patient died due to cardiac irAE upon ICI rechallenge. Nevertheless, better information including predictive markers in the challenging clinical setting of ICI rechallenge after cardiac irAE is still lacking.
Prior studies describe high fatality rates of over 39% for cardiac irAE (23). Our multi-center analysis, comparing different clinics’ approaches and the outcome of cardiac irAE, revealed that optimized management significantly reduces the mortality to 11.3% in our cohort. Therefore, we call for a standardized workflow in each center for the proactive, diagnostic, and therapeutic management of cardiac side effects, as prompt diagnosis and stringent monitoring significantly contribute to favorable outcomes. Shown in Supplementary Figure S4, we established an algorithm that could be applied across centers.
By comparing gene expression in cardiac biopsies of irMyocarditis patients to healthy heart muscle, we demonstrated an enrichment of inflammatory genes in irMyocarditis, especially highly significant for IL6R and STAT2. IL-6 has been described to increase during irAE and anti-IL-6 antibodies like tocilizumab have shown efficacy in treatment of irAE (28). Interestingly, this indicates potential parallels and might show validation on transcriptomic level for previous case reports with successful application of tocilizumab as anti-IL6R (29, 30) and of JAK-STAT-inhibitors (8, 16, 31) in severe cases with irMyocarditis. Additionally, we showed an upregulation of pathways related to cytokine-mediation, -response and -production in irMyocarditis patients. Since we also found an upregulation of the pathway of Epstein-Barr virus infection, we think this viral infection should be investigated as a potential risk factor for irMyocarditis development in future studies. Overall, our transcriptomic findings indicate as a distinct activation of the immune response in irMyocarditis with a need for further evaluation of especially anti-IL6R and JAK-inhibitor treatment.
Furthermore, we investigated immunophenotyping changes potentially related to irMyocarditis development. First of all, we demonstrated a higher activation of Treg cells and DCs in relation to the longitudinally observed development of irMyocarditis, explicitly shown by increased activated CD4+ Treg cells, enhanced level of PD-L1, and reduced levels of activated CD4+ T cells. Secondly, in comparison to patients without irAE undergoing ICI-therapy, patients with irMyocarditis showed a significant increase of activated Tem cells, with a higher expression of exhaustion markers (Supplementary Figure S5). There is a growing consensus that the response to ICI-therapy is achieved by modulating immunosuppressive cells such as Tregs (32). Recently, research demonstrated that Treg frequencies show a weak but statistically significant correlation with irAE severity (33). It also has been reported that patients with thymic epithelial tumor and non-small cell lung cancer show a strong increase of Tregs during anti-PD-1 therapy (34). Herein, patients with irMyocarditis show a higher frequency of Tregs compared to ICI-treated patients without toxicity. In the context of previous studies, our results of Tem cells might show parallels to the findings of Lozano et al. In this retrospective study, a strong correlation between the development of irAE and CD4+ Tem cells was identified (35). On the other hand, Tem (both CD4 and CD8) trended down in patients with irAE in a study investigated by Manfred, et al. (36). Additional work is needed to determine whether these different patterns represent mechanistic differences among different organ-specific irAE. Although the mechanisms of irMyocarditis are complex and incompletely understood, it is well established that irMyocarditis is mediated by the delicate regulation of the adaptive immune system. As their lineages of immune cells are interconnected, modulating the balance of their correlated T cell differentiation is a promising method for improving irMyocarditis.
The greatest challenges in the field of irMyocarditis surround monitoring, diagnosis and management, as well as the risks associated with re-challenge since decisions are based on expert opinion or retrospective data. Given the high mortality rate of irMyocarditis, an area of growing interest is biomarkers to predict irMyocarditis, like e.g., the composite biomarker score that includes the frequency of CD4 Tem cells in peripheral blood (35). Other biomarkers including cytokines, serum and other biological fluid proteins, genetic variations and gene profiles have been described as potential irMyocarditis predictors (22, 37–39). Our third finding regarding immunophenotyping indicated that T cell abundance could not serve as predictor for the development of cardiotoxicity. However, we observed LAG3 expression on T cells and PD-L1 expression on DC cells as potential predictive indicators for the occurrence of irMyocarditis comparing baseline immunophenotypes of irMyocarditis with patients without toxicity. Further studies will be needed to validate these proposed biomarkers.
5 Conclusion
The very low mortality rate of 11.3% for cardiac irAE in this cohort is remarkable and might be due to stringent monitoring since patients without troponin measurement were far more likely to die of the irAE. Our gene expression analyses imply an upregulation of IL6R and STAT2 and would thus suggest a more targeted therapy of the irAE with tocilizumab, or JAK-inhibitors, especially in steroid refractory irMyocarditis. Immunophenotyping of PBMC could enable early diagnosis of at risk groups that were characterized by enhanced Treg, Tem cells.
Data availability statement
The datasets presented in this study can be found in online repositories. The names of the repository/repositories and accession number(s) can be found in the article/Supplementary Material.
Ethics statement
The studies involving humans were approved by the ethics commission in Erlangen (17_16_Bc; 2_20_B) and Munich (20–1,122), and the study followed the declaration of Helsinki. For patients enrolled elsewhere, each cancer center had approval or exemption of the respective institutional review board. All centers were acting according to their regulatory requirements. The studies were conducted in accordance with the local legislation and institutional requirements. Written informed consent for participation in this study was provided by the participants’ legal guardians/next of kin.
Author contributions
YW: Writing – original draft, Writing – review & editing, Conceptualization, Data curation, Formal Analysis, Funding acquisition, Investigation, Methodology, Project administration, Resources, Software, Validation, Visualization. CE: Conceptualization, Data curation, Formal Analysis, Funding acquisition, Investigation, Methodology, Project administration, Resources, Software, Validation, Visualization, Writing – original draft, Writing – review & editing. CS: Conceptualization, Data curation, Funding acquisition, Investigation, Resources, Validation, Writing – review & editing. LH: Data curation, Investigation, Validation, Writing – review & editing. RK: Data curation, Investigation, Validation, Writing – review & editing. UG: Data curation, Investigation, Validation, Writing – review & editing. FS: Data curation, Investigation, Validation, Writing – review & editing. DA: Data curation, Investigation, Validation, Writing – review & editing. IP: Data curation, Investigation, Validation, Writing – review & editing. GP: Data curation, Investigation, Validation, Writing – review & editing. JV: Data curation, Investigation, Validation, Writing – review & editing. WF: Data curation, Investigation, Validation, Writing – review & editing. LW: Data curation, Investigation, Validation, Writing – review & editing. DT: Data curation, Investigation, Validation, Writing – review & editing. CL: Data curation, Investigation, Validation, Writing – review & editing. LZ: Data curation, Investigation, Validation, Writing – review & editing. JM: Data curation, Investigation, Validation, Writing – review & editing. RD: Data curation, Investigation, Validation, Writing – review & editing. RG: Data curation, Investigation, Validation, Writing – review & editing. K-CK: Data curation, Investigation, Validation, Writing – review & editing. HS: Data curation, Investigation, Validation, Writing – review & editing. FM: Data curation, Investigation, Validation, Writing – review & editing. K-MT: Data curation, Investigation, Validation, Writing – review & editing. PT: Data curation, Investigation, Validation, Writing – review & editing. PB: Data curation, Investigation, Validation, Writing – review & editing. DJ: Data curation, Investigation, Validation, Writing – review & editing. LF: Data curation, Investigation, Validation, Writing – review & editing. LH: Data curation, Investigation, Validation, Writing – review & editing, Conceptualization, Formal Analysis, Funding acquisition, Methodology, Project administration, Resources, Software, Supervision, Visualization, Writing – original draft.
Funding
The authors declare financial support was received for the research, authorship, and/or publication of this article.
The SERIO registry is supported by the German Foundation immuno-oncology (Stiftung Immunonkologie) (FA-21-002) and the Verein zur Förderung des Tumorzentrums der Universität Erlangen-Nürnberg e.V. This work was also supported by the German Federal Ministry of Education and Research (BMBF) as part of the project emed:MelAutim (01ZX1905E to LH). Further funding was provided to I.P. by the Bavarian Cancer Research Center (BZKF) for personal costs and to D.A. by the German Research Foundation (DFG AN 801/4-1 and SFB TRR355). The Deutsche Gesellschaft für Muskelkranke (DGM) e.V. and the German Cancer Consortium (DKTK), Partner Site Charité Berlin, supported the study. PJB is supported by an Excellence Stipend of the Else Kröner-Fresenius-Foundation (EKFS). The study's funders had no role in study design, data collection, analysis, and interpretation of data, or in the writing of the manuscript and the decision to submit the paper for publication.
Conflict of interest
LH received speaker and consultancy fees from BiomeDx, BMS, Immunocore, Kyowa Kirin, Merck, MSD, Myoncare, Novartis, Pieris, Pierre-Fabre, Roche, Sanofi, Stemline Therapeutics, SUN and Therakos. The LMU received research grants or clinical study grants from Agenus, AstraZeneca Inc., BMS, Hoffmann-La Roche AG, Huya Bioscience, Immunocore, IO Biotech, Merck, Merck Sharp & Dome GmbH, Miltenyi Biomedicine GmbH, Novartis, Pfizer, Pierre Fabre, Regeneron, Replimune, and Sanofi Aventis. CE reports on speaker fees from BristolMyers Squibb, GSK, Immunocore, Kyowa Kirin, MSD CL received honoraria (lectures, presentations, speakers bureaus, manuscript writing or educational events) and travel support from: BMS, MSD Merck, Pierre-Fabre, Biontech, Almirall Hermal, Sun Pharma, KyowaKirin, Immunocore, Sanofi, Novartis. DT reports consultancy, speaker fees or travel grants: BMS, Roche, Novartis, Sanofi, Recordati, Kyowa Kirin, Sun Pharma and Pierre Fabre. LZ served as consultant and has received honoraria from BMS, MSD, Novartis, Pierre Fabre, Sanofi, and Sunpharma and travel support from MSD, BMS, Pierre Fabre, Sanofi, Sunpharma and Novartis, outside the submitted work. PJB reports research funding (inst) by BeiGene, BMS, MSD and Takeda; an advisory role to BeiGene, BMS, MSD, Need Inc., Stemline and Takeda; honoraria from BeiGene, BMS, Celgene, MSD, Need Inc., Stemline and Takeda and stock options from Need Inc. RG received honoraria for advice and lectures from BristolMyers Squibb, Roche Pharma, MerckSharpDohme, Novartis, Merck-Serono, Amgen, Almirall Hermal, Pierre-Fabre, Sun Pharma, Immunocore, 4SC, Delcath, Sanofi/Regeneron. Ralf Gutzmer received travel support from SUN Pharma, Boehringer Ingelheim and PierreFabre. Ralf Gutzmer received research grants from Novartis, Sanofi/Regeneron, Merck Serono, Amgen, SUN Pharma, KyowaKirin, Admiral Hermal. RD has intermittent, project focused consulting and/or advisory relationships with Novartis, Merck Sharp & Dhome (MSD), Bristol-Myers Squibb (BMS), Roche, Amgen, Takeda, Pierre Fabre, Sun Pharma, Sanofi, Catalym, Second Genome, Regeneron, Alligator, T3 Pharma, MaxiVAX SA, Pfizer, Simcere and touchIME outside the submitted work. All remaining authors have declared no conflicts of interest.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fcvm.2024.1408586/full#supplementary-material
References
1. Vukadin S, Khaznadar F, Kizivat T, Vcev A, Smolic M. Molecular mechanisms of resistance to immune checkpoint inhibitors in melanoma treatment: an update. Biomedicines. (2021) 9(7):835. doi: 10.3390/biomedicines9070835
2. Khair DO, Bax HJ, Mele S, Crescioli S, Pellizzari G, Khiabany A, et al. Combining immune checkpoint inhibitors: established and emerging targets and strategies to improve outcomes in melanoma. Front Immunol. (2019) 10:453. doi: 10.3389/fimmu.2019.00453
3. Heinzerling L, Ott PA, Hodi FS, Husain AN, Tajmir-Riahi A, Tawbi H, et al. Cardiotoxicity associated with CTLA4 and PD1 blocking immunotherapy. J Immunother Cancer. (2016) 4:50. doi: 10.1186/s40425-016-0152-y
4. Zhang L, Zlotoff DA, Awadalla M, Mahmood SS, Nohria A, Hassan MZO, et al. Major adverse cardiovascular events and the timing and dose of corticosteroids in immune checkpoint inhibitor-associated myocarditis. Circulation. (2020) 141(24):2031–4. doi: 10.1161/CIRCULATIONAHA.119.044703
5. Hu JR, Florido R, Lipson EJ, Naidoo J, Ardehali R, Tocchetti CG, et al. Cardiovascular toxicities associated with immune checkpoint inhibitors. Cardiovasc Res. (2019) 115(5):854–68. doi: 10.1093/cvr/cvz026
6. Schneider BJ, Naidoo J, Santomasso BD, Lacchetti C, Adkins S, Anadkat M, et al. Management of immune-related adverse events in patients treated with immune checkpoint inhibitor therapy: ASCO guideline update. J Clin Oncol. (2021) 39(36):4073–126. doi: 10.1200/JCO.21.01440
7. Lehmann LH, Cautela J, Palaskas N, Baik AH, Meijers WC, Allenbach Y, et al. Clinical strategy for the diagnosis and treatment of immune checkpoint inhibitor-associated myocarditis: a narrative review. JAMA Cardiol. (2021) 6(11):1329–37. doi: 10.1001/jamacardio.2021.2241
8. Salem JE, Bretagne M, Abbar B, Leonard-Louis S, Ederhy S, Redheuil A, et al. Abatacept/ruxolitinib and screening for concomitant respiratory muscle failure to mitigate fatality of immune-checkpoint inhibitor myocarditis. Cancer Discov. (2023) 13(5):1100–15. doi: 10.1158/2159-8290.CD-22-1180
9. Lehmann LH, Heckmann MB, Bailly G, Finke D, Procureur A, Power JR, et al. Cardiomuscular biomarkers in the diagnosis and prognostication of immune checkpoint inhibitor myocarditis. Circulation. (2023) 148(6):473–86. doi: 10.1161/CIRCULATIONAHA.123.062405
10. Fenioux C, Abbar B, Boussouar S, Bretagne M, Power JR, Moslehi JJ, et al. Thymus alterations and susceptibility to immune checkpoint inhibitor myocarditis. Nat Med. (2023) 29(12):3100–10. doi: 10.1038/s41591-023-02591-2
11. Mahmood SS, Fradley MG, Cohen JV, Nohria A, Reynolds KL, Heinzerling LM, et al. Myocarditis in patients treated with immune checkpoint inhibitors. J Am Coll Cardiol. (2018) 71(16):1755–64. doi: 10.1016/j.jacc.2018.02.037
12. Ma P, Liu J, Qin J, Lai L, Heo GS, Luehmann H, et al. Expansion of disease specific cardiac macrophages in immune checkpoint inhibitor myocarditis. bioRxiv (2023).
13. Blum SM, Zlotoff DA, Smith NP, Kernin IJ, Ramesh S, Zubiri L, et al. Immune responses in checkpoint myocarditis across heart, blood, and tumor. bioRxiv (2023).
14. Moreira A, Loquai C, Pföhler C, Kähler KC, Knauss S, Heppt MV, et al. Myositis and neuromuscular side-effects induced by immune checkpoint inhibitors. Eur J Cancer. (2019) 106:12–23. doi: 10.1016/j.ejca.2018.09.033
15. Puzanov I, Diab A, Abdallah K, Bingham CO 3rd, Brogdon C, Dadu R, et al. Managing toxicities associated with immune checkpoint inhibitors: consensus recommendations from the society for immunotherapy of cancer (SITC) toxicity management working group. J Immunother Cancer. (2017) 5(1):95. doi: 10.1186/s40425-017-0300-z
16. Wang C, Lin J, Wang Y, Hsi DH, Chen J, Liu T, et al. Case series of steroid-resistant immune checkpoint inhibitor associated myocarditis: a comparative analysis of corticosteroid and tofacitinib treatment. Front Pharmacol. (2021) 12:770631. doi: 10.3389/fphar.2021.770631
17. Haanen J, Obeid M, Spain L, Carbonnel F, Wang Y, Robert C, et al. Management of toxicities from immunotherapy: ESMO clinical practice guideline for diagnosis, treatment and follow-up. Ann Oncol. (2022) 33(12):1217–38. doi: 10.1016/j.annonc.2022.10.001
18. Thompson JA, Schneider BJ, Brahmer J, Achufusi A, Armand P, Berkenstock MK, et al. Management of immunotherapy-related toxicities, version 1.2022, NCCN clinical practice guidelines in oncology. J Natl Compr Canc Netw. (2022) 20(4):387–405. doi: 10.6004/jnccn.2022.0020
19. Tajiri K, Aonuma K, Sekine I. Immune checkpoint inhibitor-related myocarditis. Jpn J Clin Oncol. (2017) 48(1):7–12. doi: 10.1093/jjco/hyx154
20. Johnson DB, Balko JM, Compton ML, Chalkias S, Gorham J, Xu Y, et al. Fulminant myocarditis with combination immune checkpoint blockade. N Engl J Med. (2016) 375(18):1749–55. doi: 10.1056/NEJMoa1609214
21. Zhu H, Galdos FX, Lee D, Waliany S, Huang YV, Ryan J, et al. Identification of pathogenic immune cell subsets associated with checkpoint inhibitor-induced myocarditis. Circulation. (2022) 146(4):316–35. doi: 10.1161/CIRCULATIONAHA.121.056730
22. Finke D, Heckmann MB, Salatzki J, Riffel J, Herpel E, Heinzerling LM, et al. Comparative transcriptomics of immune checkpoint inhibitor myocarditis identifies guanylate binding protein 5 and 6 dysregulation. Cancers. (2021) 13(10):2498. doi: 10.3390/cancers13102498
23. Wang DY, Salem JE, Cohen JV, Chandra S, Menzer C, Ye F, et al. Fatal toxic effects associated with immune checkpoint inhibitors: a systematic review and meta-analysis. JAMA Oncol. (2018) 4(12):1721–8. doi: 10.1001/jamaoncol.2018.3923
24. Laissy JP, Messin B, Varenne O, Iung B, Karila-Cohen D, Schouman-Claeys E, et al. MRI of acute myocarditis: a comprehensive approach based on various imaging sequences. Chest. (2002) 122(5):1638–48. doi: 10.1378/chest.122.5.1638
25. Salem JE, Manouchehri A, Moey M, Lebrun-Vignes B, Bastarache L, Pariente A, et al. Cardiovascular toxicities associated with immune checkpoint inhibitors: an observational, retrospective, pharmacovigilance study. Lancet Oncol. (2018) 19(12):1579–89. doi: 10.1016/S1470-2045(18)30608-9
26. Norwood TG, Westbrook BC, Johnson DB, Litovsky SH, Terry NL, McKee SB, et al. Smoldering myocarditis following immune checkpoint blockade. J Immunother Cancer. (2017) 5(1):91. doi: 10.1186/s40425-017-0296-4
27. Tajmir-Riahi A, Bergmann T, Schmid M, Agaimy A, Schuler G, Heinzerling L. Life-threatening autoimmune cardiomyopathy reproducibly induced in a patient by checkpoint inhibitor therapy. J Immunother. (2018) 41(1):35–8. doi: 10.1097/CJI.0000000000000190
28. Husain B, Kirchberger MC, Erdmann M, Schüpferling S, Abolhassani AR, Fröhlich W, et al. Inflammatory markers in autoimmunity induced by checkpoint inhibitors. J Cancer Res Clin Oncol. (2021) 147(6):1623–30. doi: 10.1007/s00432-021-03550-5
29. Doms J, Prior JO, Peters S, Obeid M. Tocilizumab for refractory severe immune checkpoint inhibitor-associated myocarditis. Ann Oncol. (2020) 31(9):1273–5. doi: 10.1016/j.annonc.2020.05.005
30. Fa'ak F, Buni M, Falohun A, Lu H, Song J, Johnson DH, et al. Selective immune suppression using interleukin-6 receptor inhibitors for management of immune-related adverse events. J Immunother Cancer. (2023) 11(6):e006814. doi: 10.1136/jitc-2023-006814
31. Liu Y, Jiang L. Tofacitinib for treatment in immune-mediated myocarditis: the first reported cases. J Oncol Pharm Pract. (2020) 27:739–46.
32. González-Navajas JM, Fan DD, Yang S, Yang FM, Lozano-Ruiz B, Shen L, et al. The impact of Tregs on the anticancer immunity and the efficacy of immune checkpoint inhibitor therapies. Front Immunol. (2021) 12:625783. doi: 10.3389/fimmu.2021.625783
33. Lepper A, Bitsch R, Özbay Kurt FG, Arkhypov I, Lasser S, Utikal J, et al. Melanoma patients with immune-related adverse events after immune checkpoint inhibitors are characterized by a distinct immunological phenotype of circulating T cells and M-MDSCs. Oncoimmunology. (2023) 12(1):2247303. doi: 10.1080/2162402X.2023.2247303
34. Kim KH, Hur JY, Cho J, Ku BM, Koh J, Koh JY, et al. Immune-related adverse events are clustered into distinct subtypes by T-cell profiling before and early after anti-PD-1 treatment. Oncoimmunology. (2020) 9(1):1722023. doi: 10.1080/2162402X.2020.1722023
35. Lozano AX, Chaudhuri AA, Nene A, Bacchiocchi A, Earland N, Vesely MD, et al. T cell characteristics associated with toxicity to immune checkpoint blockade in patients with melanoma. Nat Med. (2022) 28(2):353–62. doi: 10.1038/s41591-021-01623-z
36. Reschke R, Gussek P, Boldt A, Sack U, Köhl U, Lordick F, et al. Distinct immune signatures indicative of treatment response and immune-related adverse events in melanoma patients under immune checkpoint inhibitor therapy. Int J Mol Sci. (2021) 22(15):1167–74. doi: 10.3390/ijms22158017
37. Les I, Martínez M, Pérez-Francisco I, Cabero M, Teijeira L, Arrazubi V, et al. Predictive biomarkers for checkpoint inhibitor immune-related adverse events. Cancers (Basel). (2023) 15(5):1629. doi: 10.3390/cancers15051629
38. Takai R, Funakoshi Y, Suto H, Nagatani Y, Imamura Y, Toyoda M, et al. Serum soluble interleukin-2 receptor as a potential biomarker for immune-related adverse events. Anticancer Res. (2021) 41(2):1021–6. doi: 10.21873/anticanres.14857
39. Shahabi V, Berman D, Chasalow SD, Wang L, Tsuchihashi Z, Hu B, et al. Gene expression profiling of whole blood in ipilimumab-treated patients for identification of potential biomarkers of immune-related gastrointestinal adverse events. J Transl Med. (2013) 11:75. doi: 10.1186/1479-5876-11-75
Keywords: checkpoint inhibitor, melanoma, immunotherapy, myocarditis, cardiovascular toxicity
Citation: Wang Y, Ertl C, Schmitt C, Hammann L, Kramer R, Grabmaier U, Schöberl F, Anz D, Piseddu I, Pesch G, Vera J, Froehlich W, Weckbach L, Tomsitz D, Loquai C, Zimmer L, Mangana J, Dummer R, Gutzmer R, Klespe K-C, Stege H, Meiss F, Thoms K-M, Terheyden P, Bröckelmann PJ, Johnson DB, French LE and Heinzerling L (2024) Stringent monitoring can decrease mortality of immune checkpoint inhibitor induced cardiotoxicity. Front. Cardiovasc. Med. 11:1408586. doi: 10.3389/fcvm.2024.1408586
Received: 28 March 2024; Accepted: 14 May 2024;
Published: 10 June 2024.
Edited by:
Ippei Shimizu, Juntendo University, JapanReviewed by:
Kazuko Tajiri, National Cancer Center Hospital East, JapanNikhil Agrawal, University of Texas Health Science Center at Houston, United States
© 2024 Wang, Ertl, Schmitt, Hammann, Kramer, Grabmaier, Schöberl, Anz, Piseddu, Pesch, Vera, Froehlich, Weckbach, Tomsitz, Loquai, Zimmer, Mangana, Dummer, Gutzmer, Klespe, Stege, Meiss, Thoms, Terheyden, Bröckelmann, Johnson, French and Heinzerling. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Lucie Heinzerling, bHVjaWUuaGVpbnplcmxpbmdAbWVkLnVuaS1tdWVuY2hlbi5kZQ==
†These authors have contributed equally to this work and share first authorship