
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Cardiovasc. Med. , 17 May 2024
Sec. Coronary Artery Disease
Volume 11 - 2024 | https://doi.org/10.3389/fcvm.2024.1388164
 Chunlu Liu1,†Haijun Zhang1,†Liming Yang2Lihua Chen1Changhao Zu1Fangfang Wang1Yunjia Dai1
Chunlu Liu1,†Haijun Zhang1,†Liming Yang2Lihua Chen1Changhao Zu1Fangfang Wang1Yunjia Dai1 Haiyan Zhao1*
Haiyan Zhao1*
Background: This study aimed to explore the knowledge and attitude (KA) toward postoperative antithrombotic management and prevention among coronary artery disease (CAD) patients who underwent coronary revascularization.
Methods: This cross-sectional study enrolled CAD outpatients and inpatients between May and December 2023 at Kailuan Medical Group at Tangshan. Basic demographic characteristics and KA scores were collected through a self-made questionnaire.
Results: This study included 523 valid questionnaires. The mean knowledge and attitude scores were 13.20 ± 6.20 (range: 0–26) and 43.68 ± 6.01 (range: 21–50), respectively, indicating poor knowledge and favorable attitude. Multivariable logistic regression analysis showed that junior high school education (OR = 2.160, P = 0.035), high school or technical school education (OR = 2.356, P = 0.039), and monthly average income >5,000 RMB (OR = 3.407, P = 0.002) were independently associated with knowledge. Knowledge (OR = 1.095, P = 0.002), BMI ≥ 24.0 kg/m2 (OR = 0.372, P = 0.011), junior high school (OR = 3.699, P = 0.002), high school or technical school (OR = 2.903, P = 0.028), high associate degree or above education (OR = 6.068, P = 0.014), monthly average income 3,000–5,000 RMB (OR = 0.296, P = 0.005), monthly average income > 5,000 RMB (OR = 0.225, P = 0.021), with hypertension (OR = 0.333, P = 0.003), blood tests every 2–3 weeks (OR = 10.811, P = 0.011), blood tests every month (OR = 4.221, P = 0.024), and blood tests every 2–3 months (OR = 3.342, P = 0.033) were independently associated with attitude.
Conclusion: CAD patients who underwent coronary revascularization had poor knowledge but favorable attitudes toward postoperative antithrombotic management and prevention. The study underscores the need for targeted education, especially for individuals with lower education and income levels, ultimately improving patient compliance and cardiovascular outcomes.
Acute coronary syndromes (ACS) includes a spectrum of conditions associated with acute myocardial ischemia and/or necrosis, usually secondary to a reduction in coronary blood flow, including unstable angina (UA), non-ST-elevation myocardial infarction (NSTEMI), and ST-elevation myocardial infarction (STEMI) (1). The most common cause of ACS is plaque rupture in the setting of underlying coronary artery disease (CAD) (2). The common risk factors for CAD include tobacco abuse, dyslipidemia, hypertension, diabetes mellitus, and a family history of CAD (3). Revascularization of CAD can be performed electively or urgently when stenosis is significant (>50% stenosis) (4–7), and the most common type of surgery includes percutaneous coronary intervention (PCI) and coronary artery bypass grafting (CABG). CABG is a cardiac surgery in which a blood vessel segment, an artery or vein, is grafted from the aorta to bypass a blockage in a coronary artery, creating a new conduit to enhance blood flow to the heart (8), while PCI involves balloon dilation and stent implantation (9), and they both improve patients' survival outcome (10).
Antiplatelet therapy is recommended after CABG or PCI and is an important factor in improving patients' outcomes. Indeed, antiplatelet therapy decreases the risk of vein graft failure and major adverse cardiovascular events (MACE) (11) but at the expense of an increased bleeding risk (12). The antiplatelet therapies are mainly oral drugs that are taken at home without supervision. Hence, compliance with treatment is an important factor affecting the prognosis of coronary revascularization. Compliance with guideline-directed medical therapy following CABG or PCI was reported to be 67% at 1 year and 53% at 5 years (13). It is worth emphasizing that patient adherence to treatment is crucial and depends on the individual's understanding of medication purposes, recognizing warning signs, being aware of potential side effects, and having a positive attitude toward the treatment (14, 15). Postoperative antithrombotic therapy plays a crucial role in preventing thrombotic events and ensuring successful outcomes in patients undergoing coronary revascularization. Patient knowledge and attitude toward antithrombotic management are essential factors influencing treatment adherence and effectiveness. However, existing literature lacks a comprehensive understanding of the specific gaps in patient knowledge and attitude regarding postoperative antithrombotic therapy, particularly in the context of coronary revascularization.
Hence, evaluating the knowledge and attitude (KA) of antiplatelet therapy after coronary revascularization could provide important data about the gaps, misconceptions, and misunderstandings that could constitute barriers to optimal treatments (16, 17). Although several studies reported viewpoints of healthcare providers on antiplatelet therapy (18, 19), there were no related studies discussing KA toward postoperative antithrombotic management and prevention in patients with coronary revascularization. Assessing knowledge and attitude (KA) could allow the design of educational and motivational interventions to improve the practice of patients with CAD toward antiplatelet drugs, possibly improving patient outcomes. Therefore, this study aimed to investigate the KA toward postoperative antiplatelet management and prevention among CAD patients after coronary revascularization.
This cross-sectional study enrolled CAD outpatients and inpatients between May and December 2023 at Kailuan Medical Group in Tangshan, Hebei Province, China. The inclusion criteria were: (1) clinically diagnosed with CAD or underwent PCI or CABG due to CAD, and (2) were well-informed about the study and voluntarily participated in this study. The exclusion criteria were: (1) consciousness, mental, or cognitive impairments, (2) malignant tumors, (3) severe systemic infectious diseases, or (4) immune system disorders. The research protocol was approved by the ethics committee of Kailuan General Hospital. Informed consents were obtained from the participants before they completed the survey. This study is reported according to the CROSS statement (20).
The questionnaire design was based on the 2021 ACC/AHA/SCAI Guidelines for Coronary Revascularization (11) and the relevant literature (1, 10, 12, 13, 21). After the initial design, feedback from three experts, including two specialists in cardiovascular medicine and one in epidemiology, was sought and used to refine the questionnaire. Forty individuals were enrolled for a pretest to assess the reliability and validity of the questionnaire. The pretest reliability analysis showed that the Cronbach's α coefficients for knowledge, attitude, and overall were 0.892, 0.621, and 0.865, respectively, indicating good internal consistency. The overall data analysis showed that the Cronbach's α coefficients for knowledge, attitude, and overall were 0.838, 0.953, and 0.886, indicating good internal consistency. The Kaiser-Meyer-Olkin (KMO) measure was 0.924, suggesting good validity.
The final questionnaire was in Chinese and encompassed three parts: basic demographic characteristics, knowledge dimension, and attitude dimension. The basic demographic characteristics section comprised 14 questions on demographic and socioeconomic characteristics. The knowledge dimension consisted of 14 questions, with responses categorized into “Aware”, “Moderately aware”, and “Unaware”, scored 2, 1, and 0 points, respectively. The total score range was from 0 to 26 points. The 14th question investigated the sources of knowledge about antithrombotic management, without assigning scores. The attitude dimension comprised 10 questions and employed a 5-point Likert scale. For positively framed questions, responses ranged from “Strongly agree” to “Strongly disagree” scored from 5 to 1. Conversely, negatively framed questions are scored in reverse. The attitude score range was 10–50 points. Knowledge was deemed sufficient, and attitude was considered positive if the score exceeded 75% of the total score in the attitude dimension (22).
The survey questionnaires were distributed to the study participants through two channels: WeChat groups and face-to-face interactions in clinical examination rooms. The WeChat groups were created by the clinic to advertise medical information and news to patients. The study was simply advertised, and those interested in participating could participate. The patients have also proposed the study during routine medical examinations. Trained research team members checked all questionnaires for validity. Incomplete questionnaires, the questionnaires that took <30 s or >480 s to complete, had obvious logical errors [e.g., impossible age or body mass index (BMI, kg/m2)] or were completed using all the same options (e.g., all first choices) and were considered invalid.
The sample size was calculated using the formula for cross-sectional studies: , the assumed degree of variability of p = 0.5 maximizes the required sample size, and δ is an admissible error (which was 5% here). The theoretical sample size was 480, which included an extra 20% to allow for subjects to be lost during the study.
Data analysis was performed using SPSS 22.0 (IBM, Armonk, NY, USA). They were tested for normal distribution using the Kolmogorov-Smirnov test. Continuous data with a normal distribution were described as means ± standard deviation (SD) and analyzed using Student's t-test; otherwise, they were presented as medians (interquartile range, IQR) and analyzed using the Wilcoxon rank-sum test. Univariable and multivariable logistic regression analyses were used to analyze the covariates independently associated with knowledge and attitude. Variables with P < 0.05 in the univariable analyses were included in the multivariable analyses (enter method). A two-sided P-value < 0.05 was considered statistically significant.
Eleven questionnaires with an impossible BMI, one questionnaire from a participant reportedly under the age of 18, and two questionnaires with all responses in the knowledge and attitude dimension marked as “A” were excluded. Hence, 523 valid questionnaires were included in the analysis (validity rate of 97.39%). Most participants were >70 years old (30.02%), overweight (61.95%), male (68.07%), were urban residence (55.83%), with junior high school education (43.21%), earning monthly average income of 3,000–5,000 RMB (52.77%), not smoking (58.89%), not drinking (64.05%), not consuming coffee or tea (86.81%), with hypertension (69.98%), without diabetes (60.23%), without hyperlipidemia (78.01%), without a history of coronary heart disease (79.92%), >5 years since ACS (34.80%), underwent PCI (95.79%), taking antithrombotic medication (84.51%), and undergoing blood tests every 2–3 months (58.70%) (Table 1).

Table 1. Basic characteristics, knowledge and attitude scores.
The mean knowledge score was 13.20 ± 6.20 (range: 0–26), indicating poor knowledge. Higher knowledge scores were observed with higher education (P < 0.001), higher income (P < 0.001), consumption of coffee or tea (P = 0.042), those without hyperlipidemia (P = 0.021), and currently taking antithrombotic medication (P < 0.001) (Table 1). The items with the poorest knowledge scores were K9 [25.43%; “Novel oral anticoagulants (NOACs), mainly including apixaban, rivaroxaban, and dabigatran”] and K8 (31.40%; “Warfarin is the most commonly used anticoagulant therapy drug”). Hospital lectures and education were the primary sources of knowledge (47.42%) (Table 2).
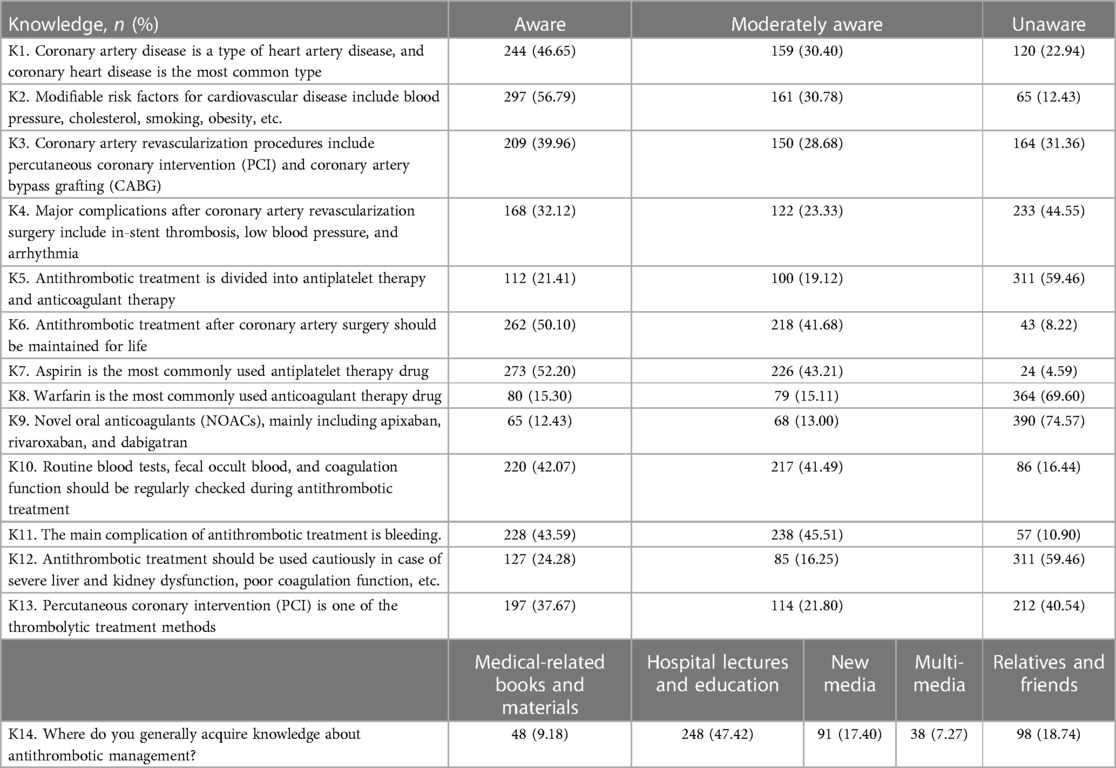
Table 2. Knowledge dimension.
The mean attitude score was 43.68 ± 6.01 (range: 21–50), indicating a favorable attitude. Higher attitude scores were observed with a smaller BMI (P = 0.021), rural residence (P = 0.023), no consumption of coffee or tea (P < 0.001), those without hyperlipidemia (P = 0.021), those with a family history of CAD (P < 0.001), currently taking antithrombotic medication (P = 0.002), and undergoing blood tests every 2–4 weeks (P = 0.002) (Table 1). Table 3 presents the distribution of the attitude of each item.
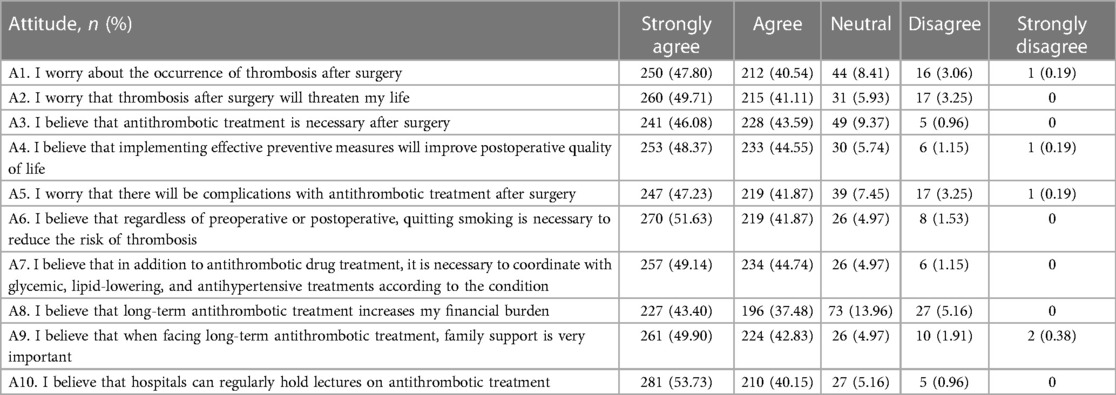
Table 3. Attitude dimension.
Multivariable logistic regression analysis found that junior high school (OR = 2.160, 95% CI: 1.058–4.411, P = 0.035), high school or technical school (OR = 2.356, 95% CI: 1.045–5.312, P = 0.039), and monthly average income >5,000 RMB (OR = 3.407, 95% CI: 1.619–7.166, P = 0.002) were independently associated with knowledge (Table 4). The knowledge (OR = 1.095, 95% CI: 1.032–1.160, P = 0.002), BMI ≥ 24.0 kg/m2 (OR = 0.372, 95% CI: 0.175–0.794, P = 0.011), junior high school (OR = 3.699, 95% CI: 1.615–8.473, P = 0.002), high school or technical school (OR = 2.903, 95% CI: 1.124–7.500, P = 0.028), high associate degree or above (OR = 6.068, 95% CI: 1.449–25.408, P = 0.014), monthly average income 3,000–5,000 RMB (OR = 0.296, 95% CI: 0.126–0.692, P = 0.005), monthly average income >5,000 RMB (OR = 0.225, 95% CI: 0.063–0.799, P = 0.021), with hypertension (OR = 0.333, 95% CI: 0.160–0.693, P = 0.003), blood tests every 2–3 weeks (OR = 10.811, 95% CI: 1.732–67.487, P = 0.011), blood tests every month (OR = 4.221, 95% CI: 1.213–14.691, P = 0.024), and blood tests every 2–3 months (OR = 3.342, 95% CI: 1.105–10.109, P = 0.033) were independently associated with attitude (Table 5).
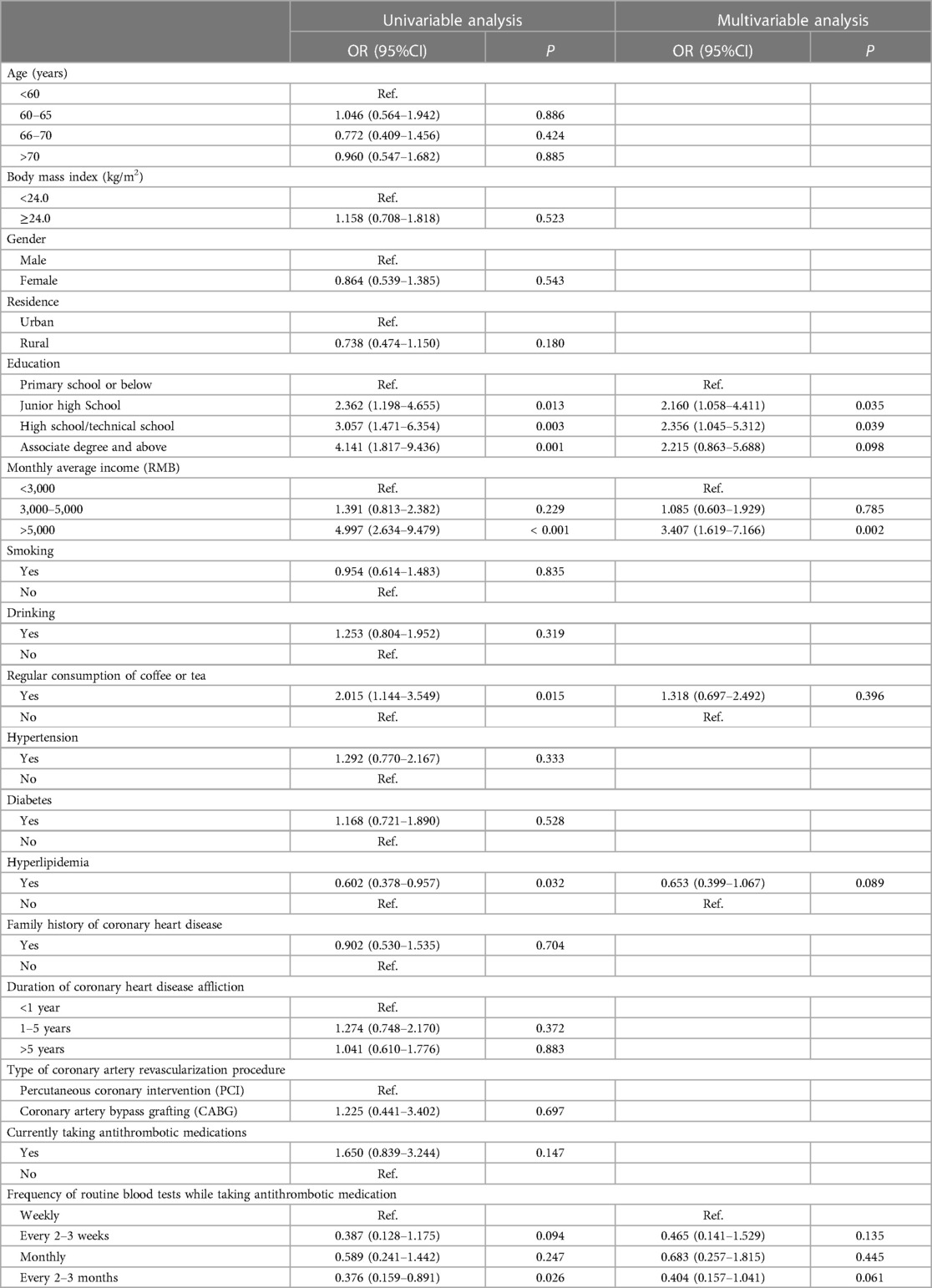
Table 4. Univariable and multivariable logistic regression analysis of knowledge.
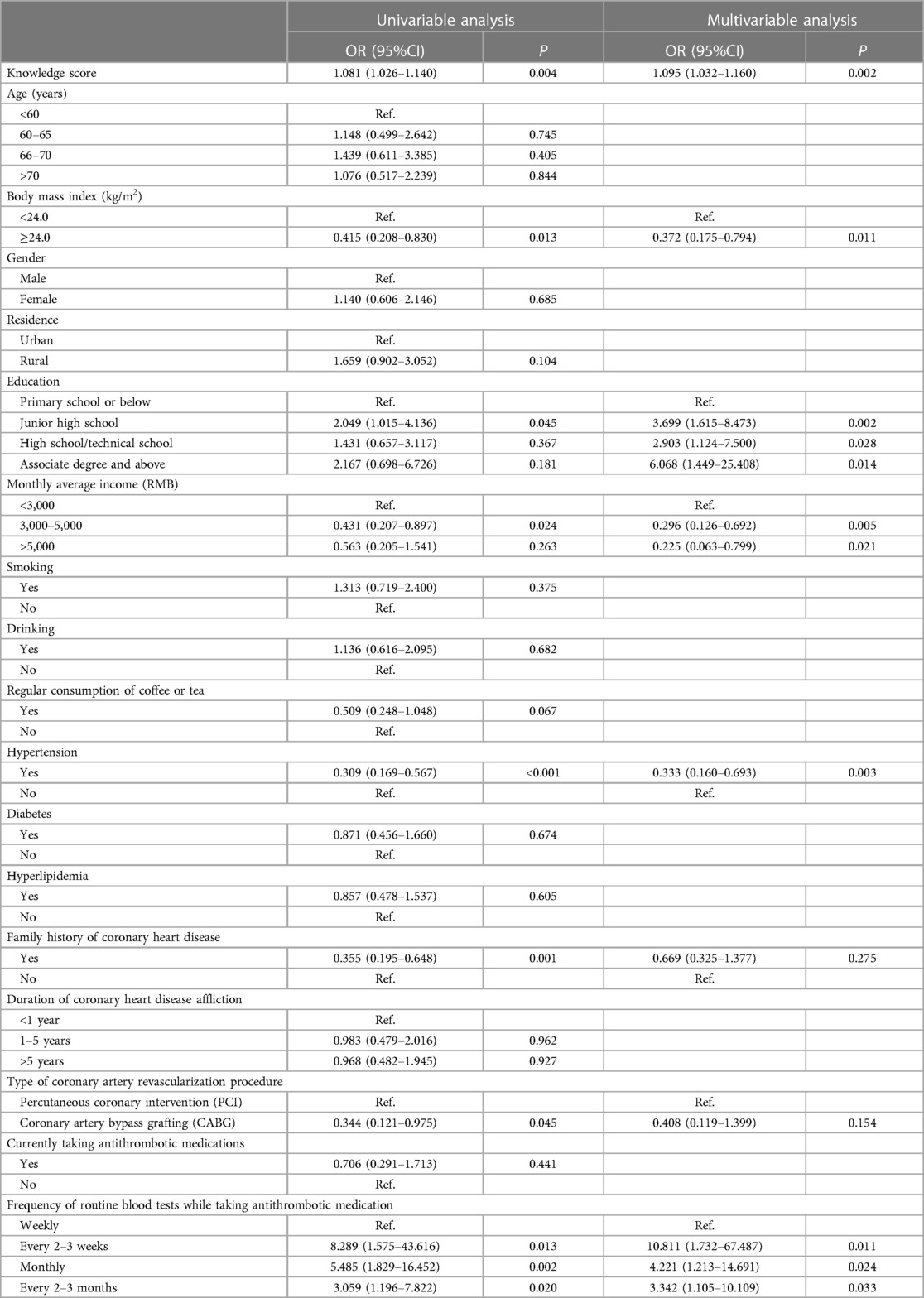
Table 5. Univariable and multivariable logistic regression analysis of attitude.
This study found that patients with CAD who underwent coronary revascularization have poor knowledge but favorable attitudes toward postoperative antithrombotic management and prevention. The questionnaire covered several aspects of antithrombotic management, but the patterns of poor knowledge were different among the participants. In addition, categories of patients were identified as associated with poorer knowledge, underscoring the importance of tailored patient education programs aimed at improving knowledge levels, particularly among individuals with lower education and income.
In this study, most patients with CAD were above 60 years old, which is consistent with the epidemiology of ACS (1, 2, 10, 23). The participants in the present study were older than in two previous KAP studies in patients with CAD (24, 25), suggesting a small likelihood of selection bias in the present study. The smoking rate in this study was lower than that in the other two previous studies (24, 26). Two previous studies reported that 97% (24) and 71% (25) of the participants could name the symptoms of CAD. Akshay et al. (24) reported that 50% of participants knew what CAD is, and 66.1% knew that the patients should follow a specific diet. Mohammad et al. (27) reported that about 50% of their participants could correctly answer general CAD questions. Similar results were observed in the present study. The questionnaire covered knowledge areas like the nature of CAD, the risk factors for CAD, the management of CAD, complications after CAD surgery, antithrombotic types, the length of antithrombotic therapy, the antithrombotic drugs available, examinations to perform during antithrombotic treatment, and the complications of antithrombotic treatment. Still, the patterns of incorrect responses were different among participants. A future study should examine whether the questionnaire developed here could be used to identify the KA areas to be improved and provide tailored educational and motivational interventions to the patients.
In the present study, higher education and higher income were both associated with higher knowledge scores. It is well known that a more favorable socioeconomic status is associated with better health literacy (28). Similar results were also observed previously (24, 29). Higher BMI was associated with lower attitudes, possibly because they tended to have poorer lifestyle habits and low willingness to change them. Higher education was also associated with a more favorable attitude. Surprisingly, higher income was associated with a less favorable attitude. It could be because patients with lower incomes are more willing to cultivate a good attitude toward therapy to avoid MACE, complications, and additional medical expenses. Less frequent blood examinations were also associated with a more favorable attitude, possibly because of saved time and money. Hence, these results suggest that although all patients would benefit from educational interventions, those with a lower socioeconomic status could profit even more.
This study also found that knowledge was independently associated with attitude, indicating that improving knowledge through education should also improve the attitude. This study showed that all patients would benefit from education, but those with low education and low income, i.e., those with lower socioeconomic status, would benefit the most. Still, available data in the literature suggested that healthcare providers have moderate knowledge of antiplatelet therapy (18, 19). Considering that healthcare providers are a primary source of reliable health information, as in the present study, their knowledge of antiplatelet therapy should be improved.
However, this study still had several limitations. The study was performed at a single center, resulting in a relatively small sample size. In addition, the participants were all from the same geographical area, limiting the generalizability of the results to other areas. The questionnaire was designed by the investigators according to the literature and local practice, policies, and reality. Hence, the questionnaire has limited exportability, and the results could lack generalizability. The items about the clinical characteristics of the participants were self-reported, and the results could be biased. In the present study, the practice was not evaluated because compliance, as the main practice indicator, could not be determined reliably. Finally, all KAP studies are at risk of the social desirability bias (30, 31), but considering that knowledge was poor, that bias has a low likelihood.
In conclusion, this study underscored the importance of tailored patient education programs aimed at improving knowledge levels, particularly among individuals with lower education and income. Addressing these gaps in understanding may enhance overall patient compliance and contribute to better cardiovascular outcomes following coronary revascularization. Future interventions should consider these factors to optimize postoperative antithrombotic management and prevention strategies among CAD patients.
The original contributions presented in the study are included in the article/Supplementary Material, further inquiries can be directed to the corresponding author.
The studies involving humans were approved by Kailuan General Hospital (No. 2020031). The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
CL: Conceptualization, Data curation, Investigation, Writing – original draft, Writing – review & editing. HZ: Formal Analysis, Investigation, Writing – original draft. LY: Data curation, Investigation, Writing – original draft. LC: Data curation, Investigation, Writing – original draft. CZ: Data curation, Investigation, Writing – original draft. FW: Data curation, Investigation, Writing – original draft. YD: Data curation, Investigation, Writing – original draft. HZ: Conceptualization, Data curation, Writing – original draft, Writing – review & editing.
The author(s) declare that no financial support was received for the research, authorship, and/or publication of this article.
We thank the other staff of the Department of Cardiology, Kailuan General Hospital, for their support in data collection.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fcvm.2024.1388164/full#supplementary-material
1. Amsterdam EA, Wenger NK, Brindis RG, Casey DE Jr, Ganiats TG, Holmes DR Jr, et al. 2014 AHA/ACC guideline for the management of patients with non-ST-elevation acute coronary syndromes: a report of the American College of Cardiology/American Heart Association Task Force on practice guidelines. Circulation. (2014) 130(25):e344–426. doi: 10.1161/CIR.0000000000000134
2. Ibanez B, James S, Agewall S, Antunes MJ, Bucciarelli-Ducci C, Bueno H, et al. 2017 ESC guidelines for the management of acute myocardial infarction in patients presenting with ST-segment elevation: the task force for the management of acute myocardial infarction in patients presenting with ST-segment elevation of the European Society of Cardiology (ESC). Eur Heart J. (2018) 39(2):119–77. doi: 10.1093/eurheartj/ehx393
3. M. Authors/Task Force, Piepoli MF, Hoes AW, Agewall S, Albus C, Brotons C. 2016 European guidelines on cardiovascular disease prevention in clinical practice: the sixth joint task force of the European Society of Cardiology and other societies on cardiovascular disease prevention in clinical practice (constituted by representatives of 10 societies and by invited experts): developed with the special contribution of the European Association for Cardiovascular Prevention & Rehabilitation (EACPR). Eur J Prev Cardiol. (2016) 23(11):NP1–96. doi: 10.1177/2047487316653709
4. Levine GN, Bates ER, Blankenship JC, Bailey SR, Bittl JA, Cercek B, et al. 2011 ACCF/AHA/SCAI guideline for percutaneous coronary intervention: a report of the American College of Cardiology Foundation/American Heart Association Task Force on practice guidelines and the society for cardiovascular angiography and interventions. Circulation. (2011) 124(23):e574–651. doi: 10.1161/CIR.0b013e31823ba622
5. Hillis LD, Smith PK, Anderson JL, Bittl JA, Bridges CR, Byrne JG, et al. 2011 ACCF/AHA guideline for coronary artery bypass graft surgery: a report of the American College of Cardiology Foundation/American Heart Association Task Force on practice guidelines. Circulation. (2011) 124(23):e652–735. doi: 10.1161/CIR.0b013e31823c074e
6. Patel MR, Dehmer GJ, Hirshfeld JW, Smith PK, Spertus JA, American College of Cardiology Foundation Appropriateness Criteria Task, et al. 2009 appropriateness criteria for coronary revascularization: a report by the American College of Cardiology Foundation appropriateness criteria task force, society for cardiovascular angiography and interventions, society of thoracic surgeons, American association for thoracic surgery, American heart association, and the American society of nuclear cardiology endorsed by the American society of echocardiography, the heart failure society of America, and the society of cardiovascular computed tomography. J Am Coll Cardiol. (2009) 53(6):530–53. doi: 10.1016/j.jacc.2008.10.005
7. Fihn SD, Blankenship JC, Alexander KP, Bittl JA, Byrne JG, Fletcher BJ, et al. 2014 ACC/AHA/AATS/PCNA/SCAI/STS focused update of the guideline for the diagnosis and management of patients with stable ischemic heart disease: a report of the American College of Cardiology/American Heart Association Task Force on practice guidelines, and the American association for thoracic surgery, preventive cardiovascular nurses association, society for cardiovascular angiography and interventions, and society of thoracic surgeons. Circulation. (2014) 130(19):1749–67. doi: 10.1161/CIR.0000000000000095
8. Diodato M, Chedrawy EG. Coronary artery bypass graft surgery: the past, present, and future of myocardial revascularisation. Surg Res Pract. (2014) 2014:726158. doi: 10.1155/2014/726158
9. Ahmad M, Mehta P, Reddivari AKR, Mungee S. Percutaneous coronary intervention. In: StatPearls. Treasure Island, FL: Ineligible Companies (2023). Disclosure: Parth Mehta declares no relevant financial relationships with ineligible companies. Disclosure: Anil Kumar Reddy Reddivari declares no relevant financial relationships with ineligible companies. Disclosure: Sudhir Mungee declares no relevant financial relationships with ineligible companies. PMID: 27478119
10. Braunwald E. Unstable angina and non-ST elevation myocardial infarction. Am J Respir Crit Care Med. (2012) 185(9):924–32. doi: 10.1164/rccm.201109-1745CI
11. M. Writing Committee, Lawton JS, Tamis-Holland JE, Bangalore S, Bates ER, Beckie TM, et al. 2021 ACC/AHA/SCAI guideline for coronary artery revascularization: a report of the American College of Cardiology/American Heart Association joint committee on clinical practice guidelines. J Am Coll Cardiol. (2022) 79(2):e21–129. doi: 10.1016/j.jacc.2021.09.006
12. Sandner S, Redfors B, Gaudino M. Antiplatelet therapy around CABG: the latest evidence. Curr Opin Cardiol. (2023) 38(6):484–9. doi: 10.1097/HCO.0000000000001078
13. Pinho-Gomes AC, Azevedo L, Ahn JM, Park SJ, Hamza TH, Farkouh ME, et al. Compliance with guideline-directed medical therapy in contemporary coronary revascularization trials. J Am Coll Cardiol. (2018) 71(6), 591–602. doi: 10.1016/j.jacc.2017.11.068
14. Jimmy B, Jose J. Patient medication adherence: measures in daily practice. Oman Med J. (2011) 26(3):155–9. doi: 10.5001/omj.2011.38
15. Martin LR, Williams SL, Haskard KB, Dimatteo MR. The challenge of patient adherence. Ther Clin Risk Manag. (2005) 1(3):189–99.18360559
16. Andrade C, Menon V, Ameen S, Kumar Praharaj S. Designing and conducting knowledge, attitude, and practice surveys in psychiatry: practical guidance. Indian J Psychol Med. (2020) 42(5):478–81. doi: 10.1177/0253717620946111
17. World Health Organization. Advocacy, Communication and Social Mobilization for TB Control: a Guide to Developing Knowledge, Attitude and Practice Surveys. (2008). Available online at: http://whqlibdoc.who.int/publications/2008/9789241596176_eng.pdf (accessed November 22, 2022).
18. Rai R, Mohan B, Babbar V, Dang N. Practices and perceptions of doctors for patients on anti-platelets during dental surgery: a national survey. J Maxillofac Oral Surg. (2014) 13(3):249–52. doi: 10.1007/s12663-013-0523-6
19. Al-Mohaissen MA, Al-Mehisen R, Lee T, Al-Madi EM. Managing cardiac patients: dentists’ knowledge, perceptions, and practices. Int Dent J. (2022) 72(3):296–307. doi: 10.1016/j.identj.2021.04.006
20. Sharma A, Minh Duc NT, Luu Lam Thang T, Nam NH, Ng SJ, Abbas KS, et al. A consensus-based checklist for reporting of survey studies (CROSS). J Gen Intern Med. (2021) 36(10):3179–87. doi: 10.1007/s11606-021-06737-1
21. Fox KA, Mehta SR, Peters R, Zhao F, Lakkis N, Gersh BJ, et al. Clopidogrel in unstable angina to prevent recurrent ischemic events: benefits and risks of the combination of clopidogrel and aspirin in patients undergoing surgical revascularization for non-ST-elevation acute coronary syndrome: the clopidogrel in unstable angina to prevent recurrent ischemic events (CURE) trial. Circulation. (2004) 110(10):1202–8. doi: 10.1161/01.CIR.0000140675.85342.1B
22. Obagha EC, Ajayi I, Abdullahi GA, Umeokonkwo CD. Clients’ satisfaction with preventive services for malaria during pregnancy in Anambra state, Nigeria. BMC Public Health. (2020) 20(1):1660. doi: 10.1186/s12889-020-09767-2
23. O’Gara PT, Kushner FG, Ascheim DD, Casey DE Jr, Chung MK, de Lemos JA, et al. 2013 ACCF/AHA guideline for the management of ST-elevation myocardial infarction: a report of the American College of Cardiology Foundation/American Heart Association Task Force on practice guidelines. Circulation. (2013) 127(4):e362–425. doi: 10.1161/CIR.0b013e3182742cf6
24. Akshay TV, Shruthilaya CK, Rafiyath VV, Rajesh KS, Subrahmanyam K, Kumart RR. Knowledge, attitude and practice of ischemic heart disease patients towards their medication. H Pharma Res Intl. (2021) 33(58A):256–62. doi: 10.9734/jpri/2021/v33i58A34114
25. Mirza AS, Aslam S, Perrin K, Curtis T, Stenback J, Gipson J, et al. Knowledge, attitudes and practices among patients with coronary artery disease in Dhaka, Bangladesh. Intl J Communit Med Publ Aff. (2016) 3(10):2740–8. doi: 10.18203/2394-6040.ijcmph20163355
26. Yahya R, Muhamad R, Yusoff HM. Association between knowledge, attitude and practice on cardiovascular disease among women in Kelantan, Malaysia. IJCRIMPH. (2012) 4:82–98.
27. Mohammad NB, Rahman NAA, Haque M. Knowledge, attitude, and practice regarding the risk of cardiovascular diseases in patients attending outpatient clinic in Kuantan, Malaysia. J Pharm Bioallied Sci. (2018) 10(1):7–14. doi: 10.4103/jpbs.JPBS_227_17
28. Svendsen MT, Bak CK, Sorensen K, Pelikan J, Riddersholm SJ, Skals RK, et al. Associations of health literacy with socioeconomic position, health risk behavior, and health status: a large national population-based survey among Danish adults. BMC Public Health. (2020) 20(1):565. doi: 10.1186/s12889-020-08498-8
29. Hertz JT, Sakita FM, Manavalan P, Mmbaga BT, Thielman NM, Staton CA. Knowledge, attitudes, and preventative practices regarding ischemic heart disease among emergency department patients in northern Tanzania. Public Health. (2019) 175:60–7. doi: 10.1016/j.puhe.2019.06.017
30. Bergen N, Labonte R. “Everything is perfect, and we have no problems”: detecting and limiting social desirability bias in qualitative research. Qual Health Res. (2020) 30(5):783–92. doi: 10.1177/1049732319889354
Keywords: myocardial infarction, knowledge, attitude, antiplatelet drugs, cross-sectional study
Citation: Liu C, Zhang H, Yang L, Chen L, Zu C, Wang F, Dai Y and Zhao H (2024) Knowledge and attitude toward postoperative antithrombotic management and prevention in patients with coronary revascularization: a cross-sectional study. Front. Cardiovasc. Med. 11:1388164. doi: 10.3389/fcvm.2024.1388164
Received: 29 February 2024; Accepted: 8 May 2024;
Published: 17 May 2024.
Edited by:
Lorenzo Menicanti, IRCCS San Donato Polyclinic, ItalyReviewed by:
Rosario Caruso, University of Milan, Italy© 2024 Liu, Zhang, Yang, Chen, Zu, Wang, Dai and Zhao. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Haiyan Zhao, aGFueWFuNzkyMkAxNjMuY29t
†These authors have contributed equally to this work
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.