 Raquel López-Vilella1,2*
Raquel López-Vilella1,2* Borja Guerrero Cervera2Víctor Donoso Trenado1,2
Borja Guerrero Cervera2Víctor Donoso Trenado1,2 Luis Martínez Dolz2,3Luis Almenar Bonet1,2,3
Luis Martínez Dolz2,3Luis Almenar Bonet1,2,3
- 1Heart Failure and Transplant Unit, Hospital Universitari i Politècnic La Fe, Valencia, Spain
- 2Cardiology Department, Hospital Universitari i Politècnic La Fe, Valencia, Spain
- 3Centro de Investigación Biomédica en Red de Enfermedades Cardiovasculares (CIBERCV), Instituto de Salud Carlos III, Madrid, Spain
Background: In heart failure (HF), not all episodes of decompensation are alike. The study aimed to characterize the clinical groups of decompensation and perform a survival analysis.
Methods: A retrospective study was conducted on patients consecutively admitted for HF from 2018 to 2023. Patients who died during admission were excluded (final number 1,668). Four clinical types of HF were defined: low cardiac output (n:83), pulmonary congestion (n:1,044), mixed congestion (n:353), and systemic congestion (n:188).
Results: The low output group showed a higher prevalence of reduced left ventricular ejection fraction (93%) and increased biventricular diameters (p < 0.01). The systemic congestion group exhibited a greater presence of tricuspid regurgitation with dilatation and right ventricular dysfunction (p:0.0001), worse renal function, and higher uric acid and CA125 levels (p:0.0001). Diuretics were more commonly used in the mixed and, especially, systemic congestion groups (p:0.0001). The probability of overall survival at 5 years was 49%, with higher survival in pulmonary congestion and lower in systemic congestion (p:0.002). Differences were also found in survival at 1 month and 1 year (p:0.0001).
Conclusions: Mortality in acute HF is high. Four phenotypic profiles of decompensation differ clinically, with distinct characteristics and varying prognosis in the short, medium, and long term.
Introduction
Heart failure (HF) can be considered a severe and chronic disease (1). However, far from remaining stable over time, it exhibits a clear tendency to progress towards clinical deterioration in affected patients (2). In this clinical evolution, the natural history of the disease shows that there are, with varying frequency, episodes of exacerbation and decompensation that necessitate hospitalization (3). Not all episodes of instability are the same, with different forms of decompensation ranging from scenarios of low cardiac output to clinical pictures of pulmonary or systemic congestion, or both (4). Each of these has a distinct clinical-analytical profile, requiring a different therapeutic approach and the adoption of a personalized prognostic evolutionary perspective (5, 6). Some of these clinical patterns have traditionally been associated with a worse prognosis (low output) (7). However, the clinical and analytical characterization, as well as the prescribed treatment at discharge, have not been clearly defined for all these profiles, revealing a lack of typification and analysis of the specificities of each. On the other hand, differences in survival among types of clinical decompensation have not been thoroughly investigated. The hypothesis when formulating this study was that since the clinical decompensation profile of HF patients admitted for HF is different, clinical characteristics, analytical alterations, prescribed treatment at discharge, and medium to long-term survival could also differ. Thus, the primary objective of the study was to analyze the clinical and analytical characteristics of patients admitted for heart failure according to the clinical decompensation profile. The secondary objective was to conduct a comparative analysis of overall survival and each group's long-term survival (5 years).
Materials and methods
Retrospective longitudinal study based on patient data admitted to the Cardiology Department of a referral hospital. The study enrolled consecutive patients diagnosed with HF, including those with low cardiac output, pulmonary congestion, mixed congestion, and systemic congestion. The inclusion period spanned five years (June 2018–June 2023). Patients who died during hospitalization (n: 59) were excluded, as the primary goal was to understand the treatment that improved the patient's condition and enabled hospital discharge. The total number of patients included in the study was 1,668. The diagnosis was made following the criteria of the 2021 European Heart Failure Guidelines (8).
Variable definitions were established prior to the initiation of the database. (a) Low output: presence of hypotension (defined as a systolic blood pressure less than 90 mmHg) and hypoperfusion [defined as with peripheral coldness, oliguria (urine output <500 ml in 24 h), requiring inotropic support (dobutamine alone or with noradrenaline) for clinical stabilization]. (b) Pulmonary congestion: crackles in both lung fields and/or chest x-ray with pleural effusion and/or alveolar, interstitial, or mixed pattern without peripheral or minimal edema. Patients in whom congestion was confirmed by lung ultrasound also entered this group, although lung ultrasound was not a mandatory requirement for diagnosis. (c) Mixed congestion: pulmonary congestion defined as stated above plus significant edema in lower limbs (at least moderate degree) and/or abdomen with ascites. (d) Systemic congestion: Significant edema in lower limbs (at least moderate degree) and/or abdomen with ascites and/or hepatojugular reflux/hepatomegaly but without pulmonary congestion. Patients in whom congestion was confirmed by ultrasound (VExUS, venous excess ultrasound score) also entered this group, although VExUS was not performed routinely on all patients and this examination was not a mandatory requirement for diagnosis.
Ejection fraction was considered preserved when equal to or greater than 50% and reduced when below this threshold in the echocardiographic study conducted during the early days of hospital admission.
Medical history, echocardiographic parameters, admission laboratory results, and prescribed treatment at hospital discharge were analyzed and compared. Overall survival and survival within each subgroup were also compared during the study period (5 years).
Data entry into the database was completed on the day of hospital discharge. To minimize errors, data collection and entry were performed by personnel experienced in managing these patients, specifically by the same cardiologists belonging to the HF Unit.
The study received approval from the Biomedical Research Ethics Committee of the hospital, adhering to the ethical principles for medical research in human subjects as defined by the Declaration of Helsinki.
Statistical analysis
Qualitative variables were expressed as numbers and percentages, and quantitative variables as median and interquartile range (non-normal distribution, p < 0.05 in the Kolmogorov–Smirnov test). Comparison between quantitative variables was performed using the Kruskal–Wallis ANOVA. For comparative analysis between qualitative variables, Pearson's χ2 test was applied. Survival curves were calculated using the Kaplan–Meier method, and comparisons were made using the Log Rank test. The multivariate analysis was conducted using Cox regression (Hazard Ratio), with the dependent variable being mortality and the independent variables being those considered of interest; the method employed was “Enter”. A p-value of <0.05 was considered significant. Statistical analysis utilized SPSS Statistics Version 27® software and Stata Statistics/Data Analysis 16.1, serial number 501606323439. Graphs were created using the SPSS program and modified with PowerPoint. The database was designed with Access and completed at the patient's discharge, excluding survival follow-up. Both programs are part of the Microsoft Office Professional Plus 2019 statistical package.
Results
Baseline characteristics
Some differences were found in the clinical profile among the study groups, particularly in the low output group, where younger males were more prevalent (p: 0.0001). Among the congestive groups, younger male patients were predominantly in the systemic congestion group (p: 0.0001). The most prevalent underlying heart condition in the low output group was ischemic heart disease, followed by idiopathic dilated cardiomyopathy. In the other groups, valvulopathies and ischemic heart disease were predominant (p: 0.0001). Relevant medical history (renal dysfunction and atrial fibrillation) was mostly present in the mixed and systemic congestion group (p < 0.01). These data can be observed in Table 1.
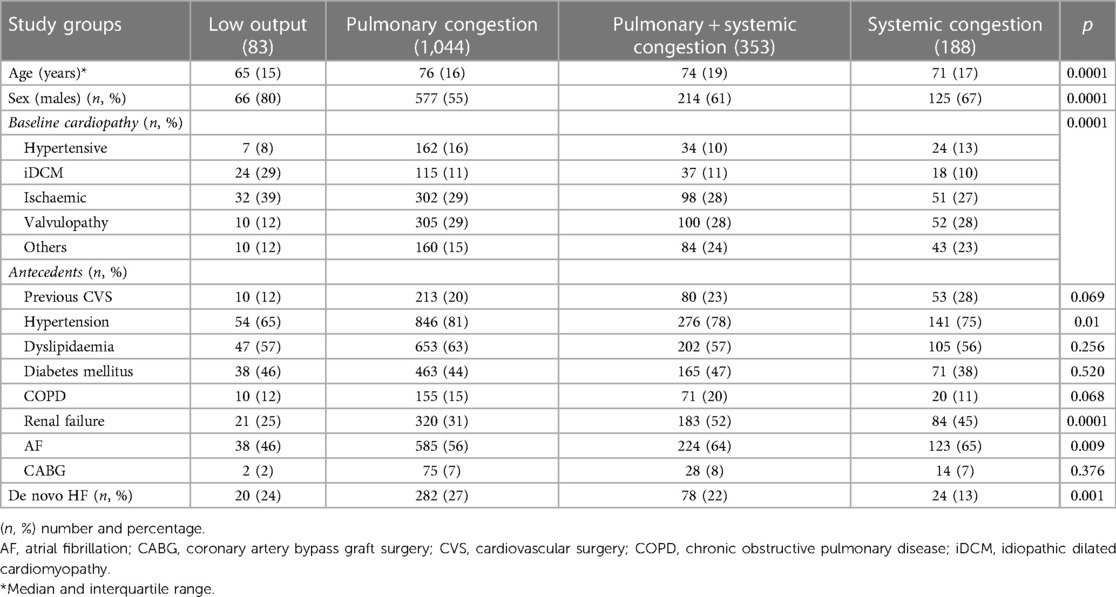
Table 1. Baseline characteristics by profile.
Echocardiographic and analytical parameters
Many differences were identified. The low output group was markedly different from the others, with a significant proportion of patients having reduced left ventricular ejection fraction [LVEF] (93%) and larger biventricular diameters (p < 0.01). Among the other three groups, the systemic congestion group showed a higher incidence of significant tricuspid regurgitation (TR) with dysfunction and dilation of the right ventricle [RV] (p: 0.0001). Regarding analytical parameters, the low output group exhibited the most significant clinical differences, particularly with a higher elevation of hepatic biomarkers, troponin, NT-ProBNP, and ferritin (p < 0.001). In the other groups, the most relevant clinical differences were a progressive increase in plasma levels of creatinine, uric acid, and CA 125 among the pulmonary congestion, mixed congestion, and systemic congestion groups (Table 2).
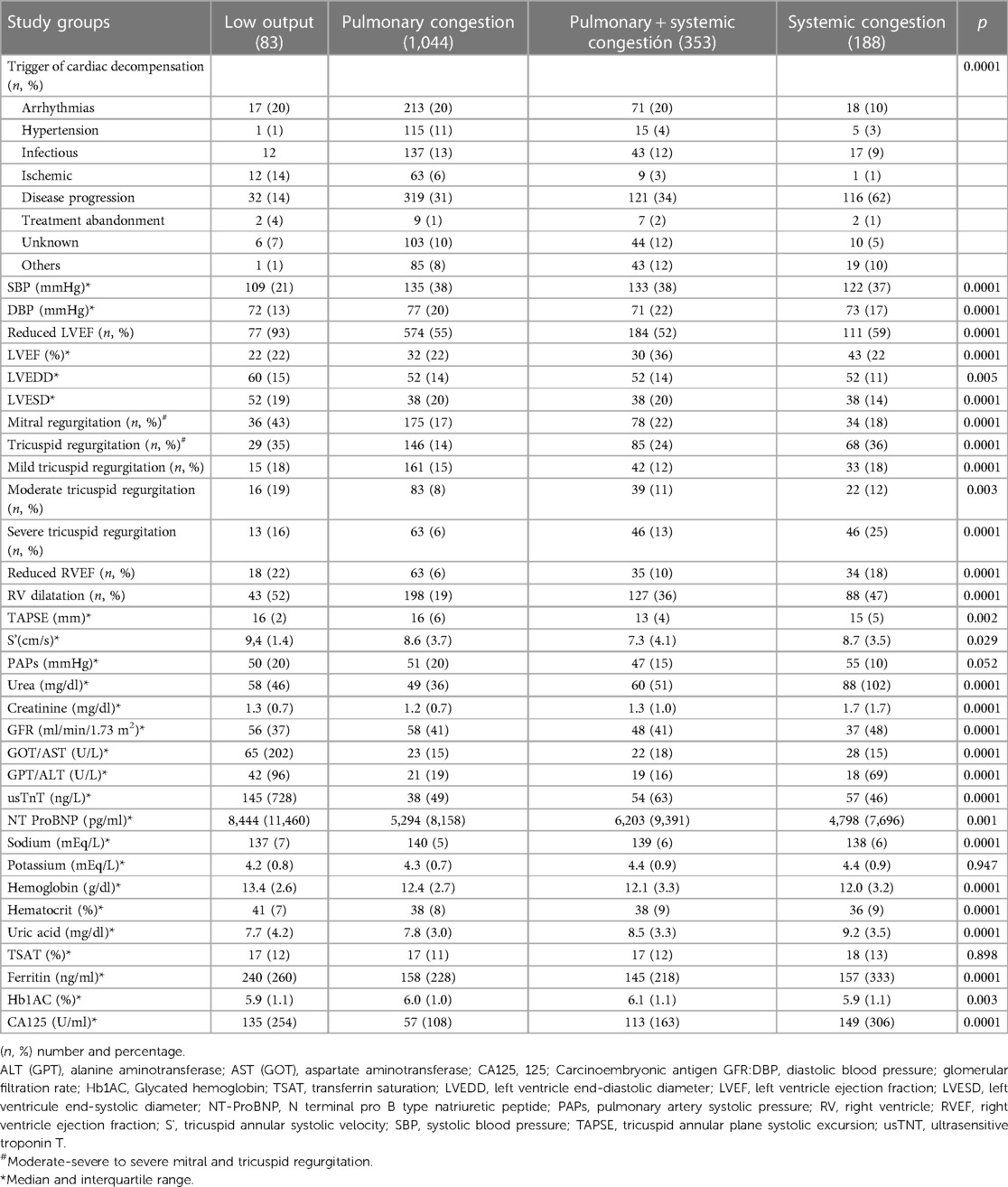
Table 2. Clinical, echocardiographic and analytical parameters by profile.
Discharge treatment
The most apparent differences included a higher use of diuretics in the mixed and, especially, systemic congestion groups (p: 0.0001). Detailed comparative analysis can be observed in Table 3.

Table 3. Discharge treatment by profile.
Survival analysis
Mortality during the entire follow-up exceeded 50% at 5 years, with a gradual decrease from admission due to decompensation and an average survival of 1,213 days (Figure 1A). When comparing survival function by groups, it was evident that they were not all equal. Thus, the best survival was observed in the pulmonary congestion group and the lowest in the systemic congestion group, even below that of the low output group. The differences found were between pulmonary congestion vs. low output (p: 0.01) and vs. systemic congestion (p: 0.001) (Figure 1B). The comparison at different periods (1 month, 1 year, and 5 years) of the probability of survival by groups was different (p < 0.05), with lower survival at one month and one year in the low output group. There were also differences in the percentage of deceased individuals in each group (p: 0.0001) (Table 4 and Figure 2). In the multivariate analysis, age, systemic congestion, low cardiac output, renal dysfunction, and right ventricular dysfunction were found to be independent predictors of mortality (Figure 3).

Figure 1. Overall and study group survival function. (A) Probability of survival for the entire series. (B) Probability of survival by study groups. Median survival: Low output group: 1,113 days, 95% CI: 845–1,382. Pulmonary congestion group: 1,288 days, 95% CI: 1,214–1,362. Mixed congestion group: 1,191 days, 95% CI: 1,064–1,317. Systemic congestion group: 990 days, 95% CI: 832–1,148. CI, confidence interval.
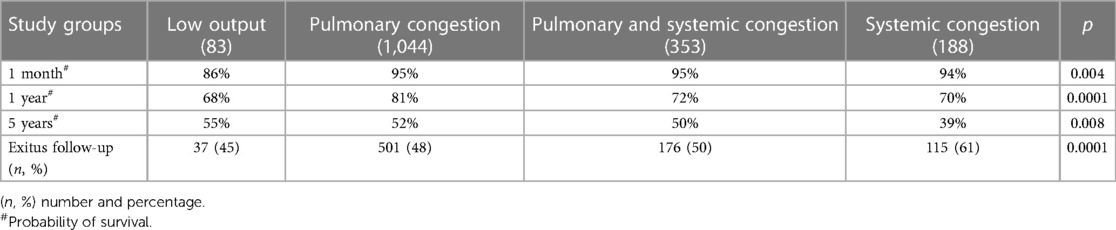
Table 4. Probability of survival and number of exitus during follow-up.
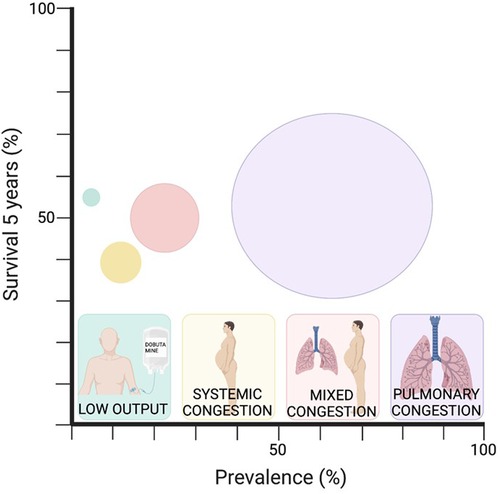
Figure 2. Circles size is proportional to the prevalence of each profile.
Discussion
Admissions due to decompensation in HF reduce patients' quality of life and shorten their survival probability (1–3, 7). However, the clinical picture of HF decompensation does not have a unique phenotypic profile; it can vary, leading to different clinical characteristics and prognoses (4). Currently, it is essential, for personalized precision medicine, to identify clinical phenotypes within the heart failure framework that help us correctly identify patients admitted for decompensation. This aids in conducting a functional and prognostic assessment, allowing for the establishment of individualized therapeutic and follow-up goals by identifying the risk related to the decompensation reason and, consequently, the evolutionary prognosis. This study aimed to identify the four clinical profiles that patients present upon admission for decompensations to understand their overall clinical characteristics and the probability of survival over a 5-year period.
It has been confirmed that there are four different clinical profiles into which all patients can be categorized. These profiles differ in terms of clinical characteristics, analytical parameters, echocardiographic studies, and differences in the prescription of cardioactive drugs at discharge. Additionally, there are differences in survival, with the highest in pulmonary congestion and the lowest in systemic congestion. In this study, we selected the four profiles that we believe encompass all clinical presentations of heart failure decompensation. These profiles are easily identifiable, both through analytical parameters (NT-ProBNP, CA 125) and clinical indicators (6), in a more objective manner than the classic determination of wet/dry or cold/hot. This classic determination is much more variable over time and examiner-dependent (9, 10). It also allows the exclusion of ejection fraction from the classification, which, in many cases, does not correspond to the clinical presentation. Additionally, we incorporated the mixed congestion pattern (systemic and pulmonary), not explicitly reflected in guidelines (8) or in most studies in this field (5, 11–13). However, in our study, it has a prevalence of 21.1% and presents characteristics regarding survival, evolution, and clinical features distinct from other congestion patterns and the low-output pattern.
It is important to note that in other studies, clinical profiles are classified as cold or hot based on perfusion status and as wet or dry based on congestion status (10, 13, 14). In this series, the low-output group includes patients who are also congestive (cold and wet). This distinction is crucial since the medical management of these patients classified in the same group will be different and includes the use of diuretics.
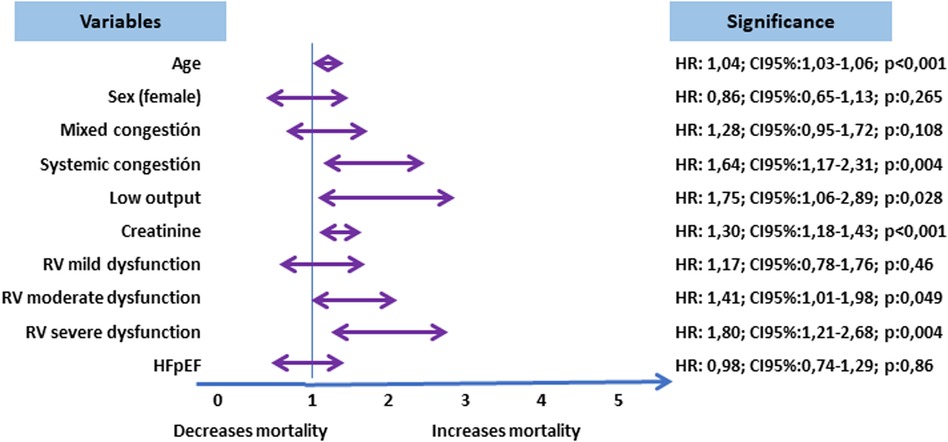
Figure 3. Multivariate analysis. Cox regression (Hazard Ratio). The congestion profiles are analyzed with respect to the pattern of pulmonary congestion. Right ventricular dysfunction is analyzed in relation to normal right ventricular function.
Among the baseline characteristics, differences exist between the groups, as reflected in other large studies on clinical profiles such as the EHFS II study [3,580 patients] (15) or the ESC-EORP-HFA Registry [7,865 patients] (16). In these studies, the average age of patients was around 70 years, with a male predominance (higher prevalence in the low-output group), coinciding with the findings of the present study. The most prevalent underlying heart condition in the low-output group was ischemic heart disease in both studies, whereas in the other groups, valvular heart disease was more prevalent in EHFS II, and ischemic heart disease was also prevalent in ESC-EORP-HFA. In ESC-EORP-HFA, renal dysfunction and atrial fibrillation were predominant in congestive patients, aligning with the results of this analysis.
Regarding echocardiographic characteristics, in the European ESC-HF-LT registry with 6,629 patients, the cardiogenic shock group showed the highest percentage of patients with reduced left ventricular ejection fraction (LVEF) and severe mitral regurgitation, similar to these results. Additionally, a certain percentage of patients (14.7%) presented with preserved LVEF. This finding can be justified by concurrent valvular diseases (mitral regurgitation and/or aortic stenosis), situations of hypovolemia (third space), diastolic dysfunction, or severe right ventricular dysfunction (10, 13, 17). Right ventricular dysfunction is more prevalent in low output and systemic congestion groups. This is due to the determining role that the RV plays physiopathologically in both conditions. Right ventricular dysfunction begins with initial myocardial injury, with the most common cause being left HF. The mechanism that causes right-sided failure initiates initial dyssynchrony, dilation, increased wall tension, and oxygen consumption, leading to a decrease in right ventricular contractile function. The interventricular septum shifts leftward due to ventricular interdependence, reducing left ventricular preload and afterload, leading to decreased cardiac output. The decrease in cardiac output limits coronary flow, which exacerbates right ventricular dysfunction, whose dysfunction causes systemic congestion due to increased central venous pressures; this causes more organ damage than the decrease in cardiac output alone. In this sense, right ventricular dysfunction has been associated with worse prognosis, consistent with the results of the present study. In acute HF, right dysfunction is associated with a higher risk of recurrent admissions (18), especially in HF with preserved ejection fraction (18, 19). No differences were found in our study regarding estimated pulmonary systolic pressure by echocardiography, although previous studies had reported a relationship between higher pulmonary systolic pressure values and poor prognosis in acute HF (19, 20). Finally, in the echocardiographic characteristics of the 4 study groups, it can be observed how severe TR is more frequent in the systemic congestion group, which is consistent with worse prognosis in this group, with TR being a known factor associated with poor prognosis and worse survival in acute HF, regardless of the presence of pulmonary hypertension (21). In relation to other types of ultrasound, it should be noted that in this study, ultrasound was not systematically conducted on patients to assess the degree of congestion. Although ultrasound is not typically employed routinely in the context of acute heart failure, it is undeniably an increasingly utilized tool. It is recognized that clinical and ultrasound indicators of congestion are highly prevalent in patients with acute heart failure, and that their combined assessment enhances risk stratification (22–24).
In reference to analytical values, it is consistent with the pathophysiology of each profile that higher levels of CA 125 and worse renal function are found in the systemic congestion group (6). According to current scientific literature, levels of the carbohydrate antigen CA 125 have been widely associated with the state of congestion, increasing with its severity (25). Furthermore, the elevation of this molecule has been linked to higher rates of readmission and adverse clinical outcomes (26, 27). Unfortunately, major series analyzing patients based on their HF profile do not include this value in their results. This study represents the first European series to analyze this parameter within the specific clinical profiles of HF selected for this research (10, 13–15). Notably, the results highlight a progression within the congestive groups, where renal function deteriorates progressively, and CA 125 increases from the pulmonary congestion group, through mixed congestion, and finally to systemic congestion. These findings align with the pathophysiology of CA-125 and its association with clinical progression and survival, as demonstrated in the results (28).
Regardless of the analyzed HF profile, the mortality throughout the series was high, exceeding 50% at 5 years, with a gradual decrease from the decompensation admission and a mean survival of 1,213 days. These figures align with other large studies. The ECHOES study, involving 3,960 patients with a 5-year follow-up, reported survival rates around 50% (29). A Spanish study showed mortality values exceeding 40% at 5 years (30). Some studies even indicate mortality rates exceeding 70% at 5 years, regardless of the type of HF presented by patients (31, 32).
When analyzing survival by groups, the group with the lowest survival within the first month and the first year is the low output group. However, at a 5-year follow-up, the profile offering better survival is the pulmonary congestion group, while the systemic congestion group exhibits lower survival (with a median nearly 300 days less than the former), even with worse figures than the low output group. In the multivariate analysis, both systemic congestion and low cardiac output profile turned out to be independent predictors of mortality compared to the lower mortality profile (pulmonary congestion). It can be observed that the low output group experiences a rapid decline in survival initially but then stabilizes, whereas the systemic congestion group's curve shows a more gradual decline without stabilizing. In fact, its median survival is 123 days less than the low output group. In most reviewed series, the low output group initially presents higher mortality figures. However, when studying data beyond the first year, survival curves start to converge, and other clinical profiles equal or surpass the low output group, such as the systemic congestion group (28, 30). This may be justified by the fact that although the low output profile with systemic hypoperfusion has higher short-term mortality initially (32), follow-up has described congestion at discharge, renal dysfunction, and elevated proBNP and CA-125 levels as mortality predictors in HF patients (9, 23, 27). All of these factors are more prevalent in the systemic congestion group, which showed the worst 5-year survival.
The study's potential limitations are associated with inherent biases in retrospective studies. Routine ultrasound techniques were not used to classify patients in each group, although signs, symptoms and other complementary examinations were used. Drug prescriptions upon discharge depended on the attending physician during admission, introducing possible variability in medical criteria. However, clinical practice guidelines exist in the cardiology department, established by the HF Unit and utilized by all specialists treating HF patients. It was also not possible to assess whether the lack of prescription was due to side effects or additional comorbidities, introducing a potential measurement bias. Residual congestion at hospital discharge has also not been evaluated. Finally, patients who died during hospitalization were excluded, and this can be understood as a possible limitation. Nevertheless, the study involved a significant number of patients included over 5 consecutive years with predefined variables at the initial inclusion and in a single center, ensuring homogeneity in the assignment to a specific clinical group. Additionally, having hospitalized patients allowed for on-site necessary examinations to precisely define the decompensation pattern, avoiding selection biases. Both data collection from electronic records and input into the computer program were carried out by cardiologists from the HF Unit, enhancing data reliability by reducing methodological errors in transcription and interpretation, thereby avoiding information biases.
Conclusion
There are four clinical profiles among patients admitted for decompensated HF: low cardiac output, isolated pulmonary or systemic congestion, and mixed congestion. The differences between them are marked by clinical characteristics, analytical parameters, echocardiographic studies, and variations in the prescription of cardioactive drugs at discharge. There are significant differences in long-term survival between the profiles, such that cases of pulmonary congestion have a better prognosis, while cases of systemic congestion result in more fatalities during follow-up.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statement
The studies involving humans were approved by Instituto de Investigación Sanitaria La Fe. The studies were conducted in accordance with the local legislation and institutional requirements. The ethics committee/institutional review board waived the requirement of written informed consent for participation from the participants or the participants’ legal guardians/next of kin because the study is retrospective.
Author contributions
RL-V: Conceptualization, Data curation, Investigation, Methodology, Writing – original draft, Writing – review & editing. BG: Investigation, Writing – original draft, Writing – review & editing. VD: Data curation, Resources, Writing – review & editing. LM: Writing – review & editing. LA: Conceptualization, Formal Analysis, Investigation, Methodology, Project administration, Supervision, Writing – original draft, Writing – review & editing.
Funding
The authors declare that no financial support was received for the research, authorship, and/or publication of this article.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Truby LK, Rogers JG. Advanced heart failure: epidemiology, diagnosis, and therapeutic approaches. JACC Heart Fail. (2020) 8(7):523–36. doi: 10.1016/j.jchf.2020.01.014
2. Wachter R, Senni M, Belohlavek J, Straburzynska-Migaj E, Witte KK, Kobalava Z, et al. Initiation of sacubitril/valsartan in haemodynamically stabilised heart failure patients in hospital or early after discharge: primary results of the randomised TRANSITION study. Eur J Heart Fail. (2019) 21(8):998–1007. doi: 10.1002/ejhf.1498
3. Greene SJ, Bauersachs J, Brugts JJ, Ezekowitz JA, Lam CSP, Lund LH, et al. Worsening heart failure: nomenclature, epidemiology, and future directions. J Am Coll Cardiol. (2023) 81(4):413–24. doi: 10.1016/j.jacc.2022.11.023
4. Singer AJ, Skopicki H, Thode HC Jr, Peacock WF. Hemodynamic profiles of ED patients with acute decompensated heart failure and their association with treatment. Am J Emerg Med. (2014) 32(4):302–5. doi: 10.1016/j.ajem.2013.12.005
5. Mullens W, Damman K, Harjola VP, Mebazaa A, Brunner-La Rocca HP, Martens P, et al. The use of diuretics in heart failure with congestion—a position statement from the heart failure association of the European society of cardiology. Eur J Heart Fail. (2019) 21(2):137–55. doi: 10.1002/ejhf.1369
6. López-Vilella R, Jover Pastor P, Donoso Trenado V, Sánchez-Lázaro I, Martínez Dolz L, Almenar Bonet L. Clinical phenotypes according to diuretic combination in acute heart failure. Hellenic J Cardiol. (2023) 73:1–7. doi: 10.1016/j.hjc.2023.03.009
7. Gheorghiade M, Abraham WT, Albert NM, Greenberg BH, O’Connor CM, She L, et al. Systolic blood pressure at admission, clinical characteristics, and outcomes in patients hospitalized with acute heart failure. JAMA. (2006) 296(18):2217–26. doi: 10.1001/jama.296.18.2217
8. Mcdonagh TA, Metra M, Adamo M, Gardner RS, Baumbach A, Böhm M, et al. 2021 ESC guidelines for the diagnosis and treatment of acute and chronic heart failure. Eur Heart J. (2021):1–128. doi: 10.1093/eurheartj/ehab368
9. Gheorghiade M, Pang PS. Acute heart failure syndromes. J Am Coll Cardiol. (2009) 53:557–73. doi: 10.1016/j.jacc.2008.10.041
10. Javaloyes P, Miró Ò, Gil V, Martín-Sánchez FJ, Jacob J, Herrero P, et al. Clinical phenotypes of acute heart failure based on signs and symptoms of perfusion and congestion at emergency department presentation and their relationship with patient management and outcomes. Eur J Heart Fail. (2019) 21(11):1353–65. doi: 10.1002/ejhf.1502
11. de la Espriella R, Santas E, Zegri Reiriz I, Górriz JL, Cobo Marcos M, Núñez J. Quantification and treatment of congestion in heart failure: a clinical and pathophysiological overview. Nefrologia (Engl Ed). (2021):S0211-6995(21)00114-4. English, Spanish. doi: 10.1016/j.nefro.2021.04.006
12. Boorsma EM, Ter Maaten JM, Damman K, Dinh W, Gustafsson F, Goldsmith S, et al. Congestion in heart failure: a contemporary look at physiology, diagnosis and treatment. Nat Rev Cardiol. (2020) 17(10):641–55. doi: 10.1038/s41569-020-0379-7
13. Chioncel O, Mebazaa A, Harjola VP, Coats AJ, Piepoli MF, Crespo-Leiro MG, et al. Clinical phenotypes and outcome of patients hospitalized for acute heart failure: the ESC heart failure long-term registry. Eur J Heart Fail. (2017) 19(10):1242–54. doi: 10.1002/ejhf.890
14. Chioncel O, Parissis J, Mebazaa A, Thiele H, Desch S, Bauersachs J, et al. Epidemiology, pathophysiology and contemporary management of cardiogenic shock—a position statement from the heart failure association of the European society of cardiology. Eur J Heart Fail. (2020) 22(8):1315–41. doi: 10.1002/ejhf.1922
15. Nieminen MS, Brutsaert D, Dickstein K, Drexler H, Follath F, Harjola VP, et al. Euroheart failure survey II EHFS II): a survey on hospitalized acute heart failure patients: description of population. Eur Heart J. (2006) 27:2725–36. doi: 10.1093/eurheartj/ehl193
16. Chioncel O, Mebazaa A, Maggioni AP, Harjola VP, Rosano G, Laroche C, et al. Acute heart failure congestion and perfusion status—impact of the clinical classification on in-hospital and long-term outcomes; insights from the ESC-EORP-HFA heart failure long-term registry. Eur J Heart Fail. (2019) 21(11):1338–52. doi: 10.1002/ejhf.1492
17. D'Aloia A, Faggiano P, Aurigemma G, Bontempi L, Ruggeri G, Metra M, et al. Serum levels of carbohydrate antigen 125 in patients with chronic heart failure: relation to clinical severity, hemodynamic and Doppler echocardiographic abnormalities, and short-term prognosis. J Am Coll Cardiol. (2003) 41(10):1805–11. doi: 10.1016/s0735-1097(03)00311-5
18. Santas E, Miñana G, Palau P, Espriella R, Lorenzo M, Núñez G, et al. Right heart dysfunction and readmission risk across left ventricular ejection fraction status in patients with acute heart failure. J Card Fail. (2021) 27(10):1090–8. doi: 10.1016/j.cardfail.2021.06.020
19. Palazzuoli A, Cartocci A, Pirrotta F, Vannuccini F, Campora A, Martini L, et al. Different right ventricular dysfunction and pulmonary coupling in acute heart failure according to the left ventricular ejection fraction. Prog Cardiovasc Dis. (2023) 81:89–97. doi: 10.1016/j.pcad.2023.07.008
20. Bosch L, Lam CSP, Gong L, Chan SP, Sim D, Yeo D, et al. Right ventricular dysfunction in left-sided heart failure with preserved versus reduced ejection fraction. Eur J Heart Fail. (2017) 19(12):1664–71. doi: 10.1002/ejhf.873
21. Cocianni D, Stolfo D, Perotto M, Contessi S, Barbisan D, Savonitto G, et al. Association of tricuspid regurgitation with outcome in acute heart failure. Circ Cardiovasc Imaging. (2023) 16(7):566–76. doi: 10.1161/CIRCIMAGING.122.014988
22. Palazzuoli A, Ruocco G, Pellicori P, Gargani L, Coiro S, Lamiral Z, et al. Multi-modality assessment of congestion in acute heart failure: associations with left ventricular ejection fraction and prognosis. Curr Probl Cardiol. (2024) 49(3):102374. doi: 10.1016/j.cpcardiol.2024.102374
23. Palazzuoli A, Cartocci A, Pirrotta F, Tavera MC, Morrone F, Vannuccini F, et al. Usefulness of combined ultrasound assessment of E/e’ ratio, pulmonary pressure, and cava vein Status in patients with acute heart failure. Am J Cardiol. (2024) 213:36–44. doi: 10.1016/j.amjcard.2023.12.001
24. Gargani L, Girerd N, Platz E, Pellicori P, Stankovic I, Palazzuoli A, et al. Lung ultrasound in acute and chronic heart failure: a clinical consensus statement of the European association of cardiovascular imaging (EACVI). Eur Heart J Cardiovasc Imaging. (2023) 24(12):1569–82. doi: 10.1093/ehjci/jead169
25. Miñana Escrivá G, Núñez J, Sanchis J, Bodi V, Núnez E, Chorro FJ, et al. Mediciones seriadas de antígeno carbohidrato 125 tras un ingreso por insuficiencia cardíaca aguda y riesgo de reingreso precoz [Carbohydrate antigen 125 serial measurements after an admission for acute heart failure and risk of early readmission]. Med Clin (Barc). (2012) 139(11):479–86. Spanish. doi: 10.1016/j.medcli.2011.05.029
26. Núñez J, Bayés-Genís A, Revuelta-López E, Ter Maaten JM, Miñana G, Barallat J, et al. Clinical role of CA125 in worsening heart failure: a BIOSTAT-CHF study subanalysis. JACC Heart Fail. (2020) 8(5):386–97. doi: 10.1016/j.jchf.2019.12.005
27. Núñez J, Llàcer P, Bertomeu-González V, Bosch MJ, Merlos P, García-Blas S, et al. Carbohydrate antigen-125–guided therapy in acute heart failure: cHANCE-HF: a randomized study. JACC: Heart Failure. (2016) 4(11):833–43. doi: 10.1016/j.jchf.2016.06.007
28. Hobbs FDR, Roalfe AK, Davis RC, Davies MK, Hare R, The Midlands Research Practices Consortium (MidReC). Prognosis of all-cause heart failure and borderline left ventricular systolic dysfunction: 5 year mortality follow-up of the echocardiographic heart of England screening study (ECHOES). Eur Heart J. (2007) 28(9):1128–34. doi: 10.1093/eurheartj/ehm102
29. Pons F, Lupón J, Urrutia A, González B, Crespo E, Díez C, et al. Mortalidad y causas de muerte en pacientes con insuficiencia cardiaca: experiencia de una unidad especializada multidisciplinaria. Rev Esp Cardiol. (2010) 63(3):303–14. doi: 10.1016/S0300-8932(10)70089-0
30. Shah KS, Xu H, Matsouaka RA, Bhatt DL, Heidenreich PA, Hernandez AF, et al. Heart failure with preserved, borderline, and reduced ejection fraction: 5-year outcomes. J Am Coll Cardiol. (2017) 70(20):2476–86. doi: 10.1016/j.jacc.2017.08.074
31. Henkel DM, Redfield MM, Weston SA, Gerber Y, Roger VL. Death in heart failure. Circ Heart Fail. (2008) 1(2):91–7. doi: 10.1161/CIRCHEARTFAILURE.107.743146
32. González-Pacheco H, Álvarez-Sangabriel A, Martínez-Sánchez C, Briseño-Cruz JL, Altamirano-Castillo A, Mendoza-García S, et al. Clinical phenotypes, aetiologies, management, and mortality in acute heart failure: a single-institution study in Latin-America. ESC Heart Fail. (2020) 8(1):423–37. doi: 10.1002/ehf2.13092
Keywords: heart failure, clinical profiles, treatment, prognosis, survival
Citation: López-Vilella R, Guerrero Cervera B, Donoso Trenado V, Martínez Dolz L and Almenar Bonet L (2024) Clinical profiling of patients admitted with acute heart failure: a comprehensive survival analysis. Front. Cardiovasc. Med. 11:1381514. doi: 10.3389/fcvm.2024.1381514
Received: 3 February 2024; Accepted: 6 May 2024;
Published: 21 May 2024.
Edited by:
Erberto Carluccio, Heart Failure Unit, ItalyReviewed by:
Alberto Palazzuoli, University of Siena, ItalyMichele Ciccarelli, University of Salerno, Italy
Cinzia Zuchi, Hospital of Santa Maria della Misericordia in Perugia, Italy
© 2024 López-Vilella, Guerrero Cervera, Donoso Trenado, Martínez Dolz and Almenar Bonet. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Raquel López-Vilella, bG9wZXpfcmFxdmlsQGd2YS5lcw==