
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Cardiovasc. Med. , 07 March 2024
Sec. Sex and Gender in Cardiovascular Medicine
Volume 11 - 2024 | https://doi.org/10.3389/fcvm.2024.1308337
This article is part of the Research Topic Insights in Sex and Gender in Cardiovascular Medicine: 2023 View all 7 articles
 Mattia Giuliani1
Mattia Giuliani1 Giulia Santagostino Baldi2Nicolò Capra3
Giulia Santagostino Baldi2Nicolò Capra3 Alice Bonomi3
Alice Bonomi3 Chiara Marzorati4
Chiara Marzorati4 Valeria Sebri4
Valeria Sebri4 Paolo Guiddi1,4Piero Montorsi5Gabriella Pravettoni4,6Daniela Trabattoni2*
Paolo Guiddi1,4Piero Montorsi5Gabriella Pravettoni4,6Daniela Trabattoni2*
Introduction: Cardiovascular diseases are the leading cause of death among women. Prevention programmes underscore the need to address women-specific risk factors. Additionally, mental well-being is a significant aspect to consider when grappling with cardiovascular disease in women, particularly depression, anxiety, distress, and personality traits. This study aimed to create “at-risk” psychological profiles for women without prior cardiovascular disease history and to evaluate the association between anxiety, depression, distress, and Type-D personality traits with increased cardiovascular risk over 10 years.
Methods: 219 women voluntarily participated in the “Monzino Women's Heart Centre” project for primary prevention and early diagnosis of cardiovascular diseases. Psychological profiles were developed utilising cluster analysis.
Results: The primary finding indicating that belonging to the “at-risk” psychological cluster was associated with a surge in the 10-year cardiovascular risk prediction score, despite the number of comorbid risk factors (Psychological “at-risk” cluster: β = .0674; p = .006; Risk factors: β = .0199; p = .242).
Conclusions: This finding suggests that psychological well-being of women should be assessed from the very beginning of cardiovascular prevention programmes.
Cardiovascular diseases (CVD) is the primary cause of death for women, responsible for 35% of global mortality in 2019 (1). International calls for sex-specific cardiovascular research have been made due to disparities in CVD treatment and prognostic outcomes between sexes (1). In recent years, there has been a renewed impetus for investigating CVD in women and evidence on female-specific CVD risk factors has increased (2). A broader perspective is essential when it comes to women's health. Clinicians and researchers should consider psycho-social, economic, and cultural factors that contribute to the development, progression, and exacerbation of CVD. Unfortunately, such factors are still mostly ignored. In addition to the well-established CVD risk factors (hypertension, dyslipidemia, diabetes, obesity, unhealthy diet, sedentary lifestyle, and smoking), women also present sex-specific risk factors. These include menopause and premature menopause, pregnancy-related complications (gestational diabetes, hypertension and dyslipidemia during pregnancy, pre-eclampsia and preterm delivery), polycystic ovary syndrome, and systemic and autoimmune disorders (1, 2). Nonetheless, psychological symptoms and disorders, including depression, anxiety and distress, which are acknowledged risk factors for CVD (3–9), are more often detected in women than men (10, 11). According to the narrative review by Vlachopoulou et al. (12), depression in women is strongly linked to CVD. Depression is known to be a risk factor for fatal coronary heart disease (CHD) in women who have no baseline CHD, and a high risk for CHD in women with both Type 1 and Type 2 diabetes. Additionally, depression is independently predictive of coronary artery disease (CAD) in women, along with hypertension, waist-hip ratio and physical inactivity (12). The authors emphasized the role of anxiety, observing that women with high levels of phobic anxiety face a greater risk of fatal CHD, and that CVD events can be predicted in women with suspected myocardial ischemia who exhibit comorbid depression and anxiety symptoms (12). There is a wide and compelling evidence linking psychological distress with earlier onset of CVD, faster disease progression, worse prognosis, and an increased risk of mortality (13–17). Nonetheless, psychological distress is associated with stress-induced cardiomyopathy, which is also known as Takotsubo or “Broken Heart Syndrome”. This condition mainly affects postmenopausal women and is typically triggered by extreme physical or emotional events (18–20). In a recent study, Pimple et al. demonstrated that high psychological distress levels were linked to future cardiovascular events among female patients diagnosed with CAD (21). Psychological distress is the primary characteristic of “Type-D personality”, characterized by persistent negative emotions, such as anger, contempt, disgust, fear, guilt, nervousness, and low self-esteem (i.e., negative affectivity), alongside with social inhibition, a stable tendency to inhibit the expression of emotions and behaviours in social interaction (22). Type-D personality has a significant impact on various outcomes in cardiac patients. It is linked to poorer prognosis in patients with CAD—specifically, twice the risk of mortality and nonfatal myocardial infarction (MI). It is also a predictor of worse health status in CAD and heart failure (HF) patients, and is associated with worse quality of life in CAD patients undergoing rehabilitation. Type-D personality is linked to poor adherence to treatment and physicians’ prescriptions, and higher serum inflammatory marker (23). Based on the available evidence, it is crucial to identify and address women's specific psychological and cardiovascular risk factors in a timely manner for the improvement of their cardiovascular health (1). The aim of this study was to test the hypothesis that women without cardiovascular disease, but with a psychological profile deemed at risk –due to the presence of depressive, anxiety and distress symptoms and Type-D personality- may be more susceptible to a cardiovascular event within 10 years than those free from such psychological features. To our knowledge, this is the first study exploring such an association within healthy females.
219 women volunteered to participate in the “Monzino Women's Heart Centre” project for primary prevention and early diagnosis of cardiovascular disease, as described in Gili et al. (24). The participants were consecutively included in the sample and had to meet two criteria: they had to be women aged between 35 and 65 years, and had no history of overt or previous CVD. Furthermore, all participants provided a written informed consent, which was approved by the Centro Cardiologico Monzino Ethical Committee.
All the following questionnaires were used in their Italian validated versions (25–28).
The BDI-II is a self-report questionnaire containing 21 items that evaluate the severity of depressive symptoms in adults and adolescents (29). The patient rates each item on a Likert scale of 0–3. Then, the total score is calculated by summing the scores from all the items, which will determine the severity of the depressive symptoms into four levels: minimal depressive symptoms (from 0 to 13), mild depressive symptoms (from 14 to 19), moderate depressive symptoms (from 20 to 28) and severe depressive symptoms (from 29 to 63). The BDI-II has exhibited a high level of internal consistency (Cronbach α = .80), good convergent validity when compared with the Depression Questionnaire, and good test-retest reliability after one month (r = .76) (28).
The STAI-Y is a frequently used self-report inventory that evaluates both state and trait anxiety (30). The questionnaire contains 20 items that measure the level of state anxiety (STAI-S). State anxiety refers to anxiety experienced at the time of the evaluation, which is considered context-dependent and transient. Additionally, the STAI-Y comprises 20 further items that measure the levels of trait anxiety (STAI-T). Trait anxiety is usually experienced in day-to-day life and is thought to be a stable, context-independent condition. All items are rated on a 4-point scale with a total score ranging from 20 to 80 for both the state and trait anxiety subscales. The STAI-Y demonstrated a high level of internal consistency, with a Cronbach α of.93 for state anxiety and .90 for trait anxiety (31). Only the STAI-T scale was employed in this study.
The PSS is the most commonly used self-report measure for evaluating individuals’ distress perception (32). The questionnaire examines the frequency of feelings and thoughts related to distress perception over the past month. The responses range from 0 to 40, with higher scores corresponding to a greater level of perceived distress. Interpretation of the scores is based on three value categories: low distress perception (from 0 to 13); moderate distress perception (from 14 to 26); and high distress perception (from 27 to 40).
The DS-14 is a concise self-report survey that has been utilized globally for assessing negative affectivity (NA) and social inhibition (SI), associated with Type-D personality (22). The DS-14 comprises 14 items, each rated on a scale ranging from 0 (i.e., false) to 4 (i.e., true). This questionnaire provides distinct scales for both NA and SI, with scores ranging from 0 to 28. An individual with a score of ≥10 in the NA and/or SI scale is more likely to exhibit the correspondent personality trait.
Baseline clinical data were collected for all patients, encompassing biometric data, essential parameters including arterial blood pressure, conventional cardiovascular risk factors (i.e., smoking habit, familial history of cardiovascular disease, hypertension, dyslipidemia, diabetes mellitus, obesity/overweight), and cardiovascular risk factors specific to women. The participants’ medical records were thoroughly examined, including their past medical history, with a specific focus on endocrine, autoimmune, and gynecological disorders, as well as any instances of early or premature menopause, gestational diabetes and/or hypertension, eclampsia, or pre-term delivery. Each participant was provided with a conclusive summary detailing their estimated risk of cardiovascular event, calculated using the Progetto Cuore score: 10-year CV Risk PC (https://www.cuore.iss.it/valutazione/calc-rischio).
A k-means cluster analysis was conducted to identify subject subgroups with shared psychological characteristics, therefore using as clusterization variables the standardized scores of BDI-II, STAI-T, PSS, and both DS-14 NA and SI. The k-means algorithm was repeated 100 times with random initial centroids to ensure repeatability and stability of results, and the best configuration was selected. A scree plot was used to assess the Within-Cluster-Sum of Squares (WSS) trend based on the number of clusters, while the elbow method identified the optimal number. Mean ± standard deviation or median and [interquartile range] were used to express continuous variables, while categorical variables were presented as absolute numbers and percentages. Unpaired t-tests were used to compare clusters for normally distributed variables, while Wilcoxon rank sum tests were used for skewed variables. Categorical variables were analyzed using either Chi-square test or Fisher's exact test. To assess trends across clusters for categorical variables, the Mantel-Haenszel χ2-test was employed. Non-normally distributed variables were log-transformed. General linear models were used to investigate the association between estimated cardiovascular event risk, cluster membership, and number of conventional and female-specific CVD risk factors. Missing data were imputed using the PROC MI (Multiple imputation) procedure via the MCMC (Markov Chain Monte Carlo) method. One dataset was randomly selected out of the 25 imputed ones for the main analysis. To assess consistency, we calculated the percentage of times that the p-value was found to be significant or non-significant. We utilized the k-means package of RStudio (V. 4.0.3, RStudio, Boston, MA, USA) to perform k-means cluster analysis, while all other statistical analyses were conducted using SAS software package (V. 9.4, SAS Institute Inc., Cary, NC). All tests were two-sided, with a significance level of p ≤ .05.
Cluster analysis was utilized to categorize the 219 subjects into groups that share similar psychological characteristics. The elbow method applied to the scree plot (Figure 1) identified two as the most suitable number of clusters. As a result, the participants were divided into two subgroups: Cluster 1 or NPR (No Psychological Risk) cluster, consisting of 132 individuals, and Cluster 2 or PR (Psychological Risk) cluster, consisting of 87 individuals.
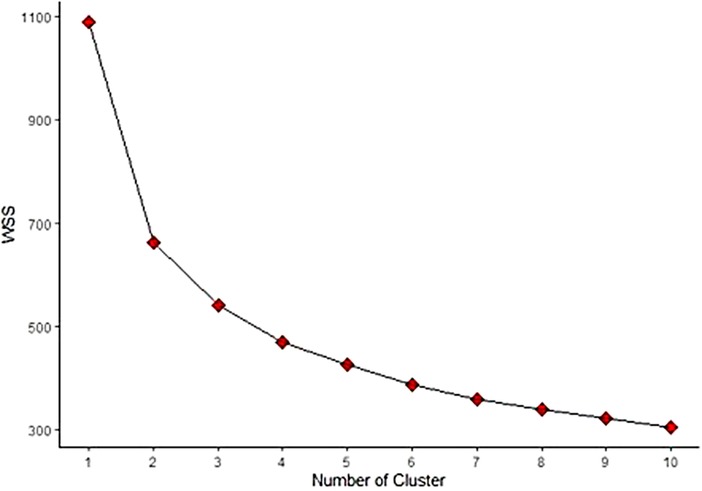
Figure 1. Scree plot for k-means clustering of psychological data. The scree plot shows how Within-Cluster-Sum of Squares (WSS) changes as a function of the number of clusters identified using the k-means algorithm. The elbow method identified an optimal number of clusters equal to two, the point at which the graph shows a distinct change in slope.
Table 1 displays the baseline characteristics of our population. Overall, both NPR and PR cluster participants were middle-aged and highly educated -with the majority having completed high school or attained a graduate degree- and a high proportion being married. No significant differences were observed between the two clusters.
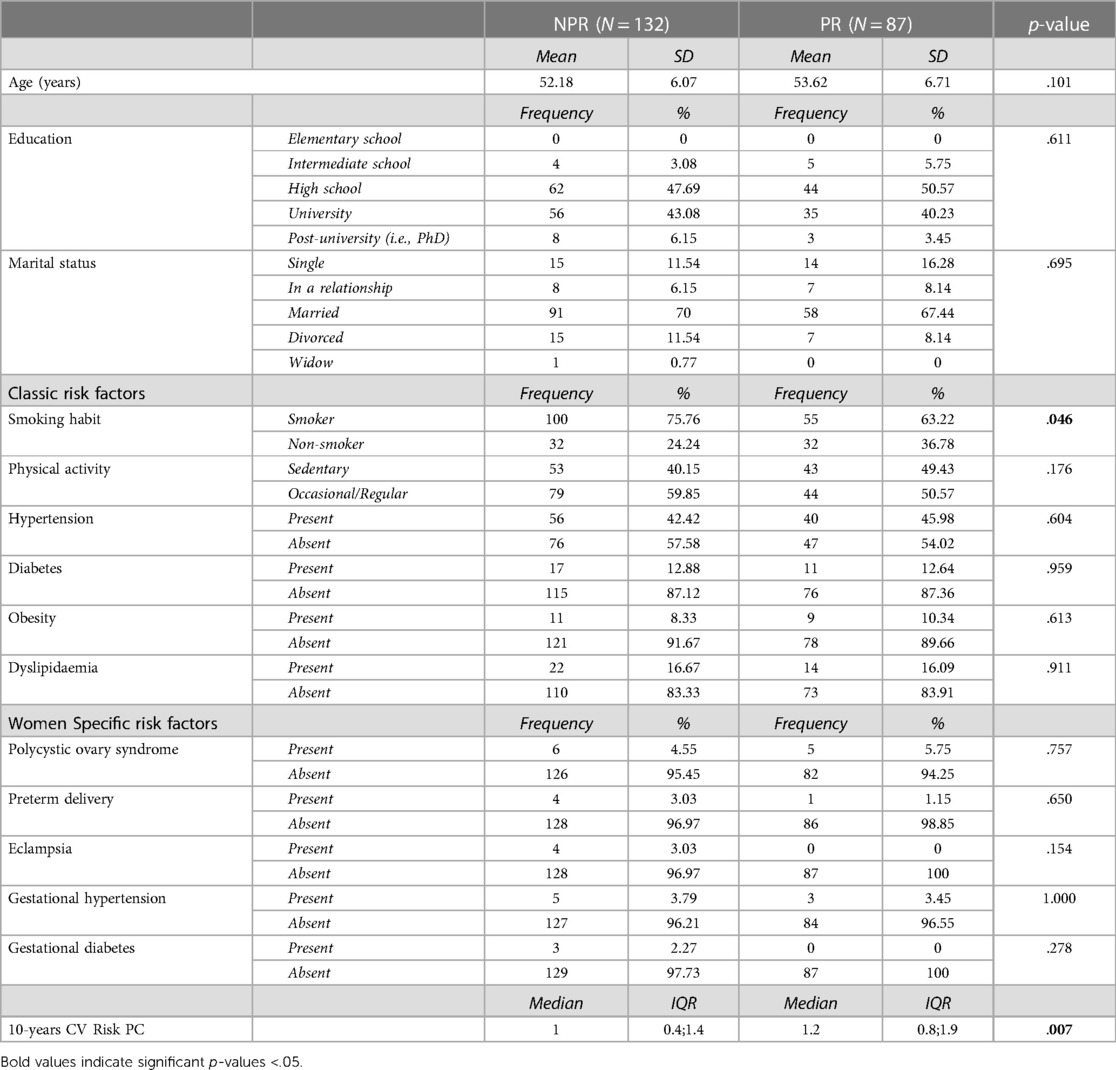
Table 1. NPR and PR clusters sociodemographic features.
Cigarette smoking was the most common modifiable traditional risk factor in both clusters, and the only one that showed a significant difference between them -NPR cluster displayed a higher percentage. Following this were hypertension and sedentary lifestyle, which were prevalent in both clusters. As for women-specific risk factors, polycystic ovary syndrome was the most common, but there was no significant difference between the two clusters. The 10-year CV Risk PC was generally low, but the PR cluster had a significantly higher score. These data are shown in Table 1.
The classic and gender-specific risk factors’ frequency increased significantly (p-trend = .04) in the PR compared to the NPR group (Figure 2). This result received validation in 24 out of 25 imputations (96%).
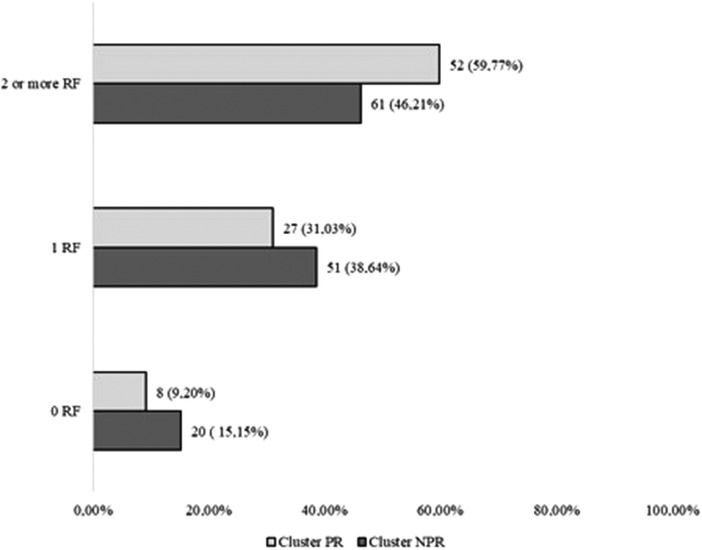
Figure 2. Classic and women specific RF trends in PR and NPR clusters.
The NPR cluster displayed low levels of anxiety symptoms, minimal depressive symptoms, and a low distress score. In contrast, the PR cluster demonstrated high levels of anxiety symptoms, mild depressive symptoms, and a moderate distress score. Additionally, the NPR cluster exhibited neither negative affectivity nor social inhibition, while the PR cluster showed clinically relevant levels of both personality traits. All these results are reported in Table 2.
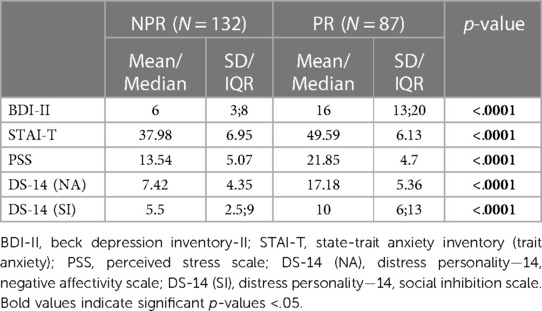
Table 2. NPR and PR clusters psychological features.
The principal finding of this analysis indicates that membership in the PR cluster characterized by an elevated psychological risk is linked to an elevation in 10-years CV Risk PC (expressed in logarithmic scale). This is regardless of the number of risk factors (both classic and women-specific) concurrently presented by subjects in comorbidity (Table 3). Our results were substantiated in all 25 imputations (100%).
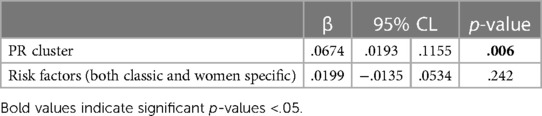
Table 3. Multivariate regression analysis on 10-years CV risk PC.
This study was the first to examine the association between a high 10-years CV risk and a psychological profile at risk, including the presence of anxiety, depressive and distress symptoms, and Type-D personality traits, within a cohort of healthy female participants. The primary finding showed that women with a psychological profile at risk scored higher in 10-years CV risk measure, irrespective of the number of comorbid risk factors. This evidence is of significance in the field of cardiovascular prevention for women as it indicates that addressing traditional psychological risk factors (such as anxiety, depression, distress and Type-D personality traits) for CVD is crucial from the earliest stage of prevention for women.
The study's theoretical background is based on two main models: Gordon's Operational Model (33) and Felner and Silverman's Antecedent Condition Model (34). We adopted the concept of “indicated interventions” from the Operational Model, which refers to screening programmes for specific subgroups of the population who present one or more specific risk conditions for the development of a disease. In this case, the subgroup consists of women who do not have an overt heart disease but may have sex-related risk factors for its development. The Antecedent Condition Model distinguishes between predisposing and precipitating factors for a specific clinical condition. In this case, sex and sex-specific factors for cardiovascular disease represent the predisposing factors, while the concomitant presence of cardiovascular risk factors and unfavourable psychological characteristics represent the precipitating factors. Both models recommend targeted interventions from the earliest stages of prevention to reduce diseases risk exposure.
Both clusters show no statistically significant difference in demographic composition. They comprise of married middle-aged women with medium to high levels of education, i.e., high school and university. Furthermore, there are no discernible differences in the frequency of classic, female-specific risk factors, except for smoking. The NPR cluster has a higher frequency of smokers than the PR cluster. However, it should be acknowledged that the borderline significance (p-value = .046) may be attributed to the smaller sample size of the PR cluster. We argue that it is highly probable that this significance may disappear with an increase in the sample size. Therefore, the two clusters can be considered similar in terms of demographic composition and risk factors. This information is crucial for interpreting the significant result regarding the effect of belonging to the psychological risk cluster on 10-year CV risk. Therefore, the primary interest lies in the role of psychological risk factors in increasing the 10-year risk of a cardiovascular event. In fact, anxiety, depression, distress, and Type-D personality were the only significant differences between the two clusters.
To the best of our knowledge, only one study has examined the relationship between depression in women and a widely-accepted lifetime CVD risk measure: the 10-year atherosclerotic CVD (ASCVD) (35). The researchers reported that, in women aged 40–79, the absolute risk of ASCVD was 6.0% for those without depression, 6.9% for those with mild depression, and 7.6% for those with major depression. They also found that among women aged 20–39, the prevalence of high lifetime CVD risk was 41.9% for those whitout depression, 53.2% for those with mild depression, and 66.5% for those with major depression. Our own findings align with these results, indicating an increasing trend in ASCVD risk with severity of depressive symptoms. The relationship between depression/depressive symptoms and CVD is a well-established issue. In 2008, the AHA consensus report in which it was clearly outlined that depression acts as an independent risk factor for CVD, and especially for CAD and MI (36). Nonetheless, to date, only a limited number of specialized hospitals have incorporated depression screening as part of their daily procedures (9). Currently, there is a lack of studies examining the relationship between anxiety and distress symptoms and the 10-year CVD risk in women. Consequently, we must refer to research investigating the relationship between anxiety, distress and overall cardiovascular risk to discuss our findings. According to Mosarla and Wood, anxiety symptoms heighten the risk of CVD in females, leading to a lower quality of life, and an increased cardiovascular morbidity, and mortality (37). Matthews et al. (38) conducted a study on a cohort of healthy postmenopausal women, which demonstrated that those who with higher levels of anger, hostility, and anxiety exhibited greater carotid thickening as assessed by IMT, even after a one-year follow-up period. In another prospective cohort study, researchers found that a one standard deviation increase in psychological distress was associated with a 44% elevated risk of cardiovascular events solely in women with CAD (21). Type-D personality traits, specifically NA and SI, are strongly correlated with both depression and anxiety (39). It is plausible to that Type-D personality traits may increase susceptibility to the development or worsening of anxiety and depressive symptoms, thereby contributing to an increased the risk of cardiovascular events. A fascinating investigation by Al-Qezweny et al. indicated that patients who underwent a percutaneous coronary intervention with type D personality had a 3.69-fold heightened risk of depression and a 2.72-fold heightened risk of anxiety at 10year of follow-up (40). The present study aligns with previous evidence. Anxiety symptoms and distress, akin to depressive symptoms, ought to receive appropriate screening and treatment from the early stages of cardiovascular prevention in women.
This paper has certain limitations; thus, the conclusions need to be interpreted with following elements in mind. First and foremost, the study exclusively involves Caucasians, and previous research indicates that cardiovascular risk is influenced by the participant's ethnic background (41). Secondly, the algorithm for calculating 10-year CVD risk requires consideration. The study utilized the 10-year CV risk PC algorithm, but it is crucial to examine whether the outcomes remain consistent with other algorithms employed in literature. Thirdly, one must also consider the psychological survey instruments employed in the present study. Validated instruments that are extensively used in literature to assess anxiety, depressive and distress symptoms, and Type-D personality traits were utilized. Nevertheless, these questionnaires are subject to limitations typical of all self-report measures and thus require further validation with other questionnaires that examined the same psychopathological constructs. A final point to consider is that the study sample consisted only of who were aware of the project and/or knew about the hospital, potentially introducing a sampling bias.
Gender disparity is a recognized concern in cardiovascular research, as women are frequently underrepresented in study samples and their specific characteristics, needs, and treatment within the cardiovascular field remain inadequately understood. This original research focuses on evaluating the potential impact of psychological well-being on the risk of developing cardiovascular disease in women who have no prior history of such conditions, over a ten-year period. Surprisingly, the findings indicate that psychological well-being is a stronger predictor than traditional cardiac risk factors (such as hypertension, diabetes, and smoking) for the development of cardiovascular disease within a decade, among women with no prior history of such disease. Although these results should be approached with caution, they lead to two primary considerations: (1) it is essential to evaluate the psychological well-being of patients from the earliest prevention stages; (2) while the link between anxiety, depression, perceived distress, personality traits and cardiovascular risk has been widely acknowledged in literature, this study confirms its strong association. To further investigate the focus of this research, future prospects will be considered: (1) to increase the sample size; (2) to include a cohort of men without any cardiovascular pathology to evaluate potential differences in the incidence of certain psychopathological traits and the role of psychological well-being on cardiovascular risk; (3) to include participants of different ethnicities to ensure a diverse sample; and (4) to collaborate with other hospitals that offer comparable services to “Monzino Women” to minimize sampling bias.
The datasets presented in this study can be found in online repositories. The names of the repository/repositories and accession number(s) can be found below: 10.5281/zenodo.5807307.
The studies involving humans were approved by Centro Cardiologico Monzino EC. The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
MG: Conceptualization, Data curation, Writing – original draft. GS: Data curation, Writing – review & editing. NC: Formal Analysis, Software, Writing – original draft. AB: Formal Analysis, Software, Writing – review & editing. CM: Writing – review & editing. VS: Writing – review & editing. PG: Writing – review & editing. PM: Writing – review & editing. GP: Writing – review & editing. DT: Conceptualization, Methodology, Supervision, Visualization, Writing – review & editing.
The author(s) declare financial support was received for the research, authorship, and/or publication of this article.
This research was supported by the Italian Ministry of Health-Ricerca Corrente to Centro Cardiologico Monzino IRCCS.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fcvm.2024.1308337/full#supplementary-material
1. Vogel B, Acevedo M, Appelman Y, Bairey Merz CN, Chieffo A, Figtree GA, et al. The lancet women and cardiovascular disease commission: reducing the global burden by 2030. Lancet. (2021) 397(10292):2385–438. doi: 10.1016/S0140-6736(21)00684-X
2. Elder P, Sharma G, Gulati M, Michos ED. Identification of female-specific risk enhancers throughout the lifespan of women to improve cardiovascular disease prevention. Am J Prev Cardiol. (2020) 2:100028. doi: 10.1016/j.ajpc.2020.100028
3. Allabadi H, Alkaiyat A, Alkhayyat A, Hammoudi A, Odeh H, Shtayeh J, et al. Depression and anxiety symptoms in cardiac patients: a cross-sectional hospital-based study in a Palestinian population. BMC Public Health. (2019) 19(1):232. doi: 10.1186/s12889-019-6561-3
4. Celano CM, Villegas AC, Albanese AM, Gaggin HK, Huffman JC. Depression and anxiety in heart failure: a review. Harv Rev Psychiatry. (2018) 26:175–84. doi: 10.1097/HRP.0000000000000162
5. Celano CM, Shapter C, Styra R, Czick M. Depression and anxiety in cardiac disease. Psychiatr Times. (2016) 33(12):4.
6. Celano CM, Daunis DJ, Lokko HN, Campbell KA, Huffman JC. Anxiety disorders and cardiovascular disease. Curr Psychiatry Rep. (2016) 18. doi: 10.1007/s11920-016-0739-5
7. Cserép Z, Losoncz E, Balog P, Szili-Török T, Husz A, Juhász B, et al. The impact of preoperative anxiety and education level on long-term mortality after cardiac surgery. J Cardiothorac Surg. (2012) 7(1):86. doi: 10.1186/1749-8090-7-86
8. Gorini A, Giuliani M, Raggio L, Barbieri S, Tremoli E. Depressive and anxiety symptoms screening in cardiac inpatients: a virtuous Italian approach to psychocardiology. Int J Environ Res Public Health. (2020) 17(14):5007. doi: 10.3390/ijerph17145007
9. Jha MK, Qamar A, Vaduganathan M, Charney DS, Murrough JW. Screening and management of depression in patients with cardiovascular disease: JACC state-of-the-art review. J Am Coll Cardiol. (2019) 73:1827–45. doi: 10.1016/j.jacc.2019.01.041
10. Bucciarelli V, Caterino AL, Bianco F, Caputi CG, Salerni S, Sciomer S, et al. Depression and cardiovascular disease: the deep blue sea of women’s heart. Trends Cardiovasc Med. (2020) 30:170–6. doi: 10.1016/j.tcm.2019.05.001
11. Buckland SA, Pozehl B, Yates B. Depressive symptoms in women with coronary heart disease: a systematic review of the longitudinal literature. J Cardiovasc Nurs. (2019) 34(1):52–9. doi: 10.1097/JCN.0000000000000533
12. Vlachopoulou E, Vassou C, Panagiotakos DB. Psychological factors and atherosclerotic cardiovascular disease development in women: a narrative review. J Atheroscler Prev Treat. (2022) 13(2):74–84. doi: 10.53590/japt.02.1036
13. Richardson S, Shaffer JA, Falzon L, Krupka D, Davidson KW, Edmondson D. Meta-analysis of perceived stress and its association with incident coronary heart disease. Am J Cardiol. (2012) 110(12):1711–6. doi: 10.1016/j.amjcard.2012.08.004
14. Edmondson D, von Känel R. Post-traumatic stress disorder and cardiovascular disease. Lancet Psychiatry. (2017) 4(4):320–9. doi: 10.1016/S2215-0366(16)30377-7
15. Steptoe A, Kivimäki M. Stress and cardiovascular disease. Nat Rev Cardiol. (2012) 9(6):360–70. doi: 10.1038/nrcardio.2012.45
16. Kivimäki M, Steptoe A. Effects of stress on the development and progression of cardiovascular disease. Nat Rev Cardiol. (2017) 15(4):215–29. doi: 10.1038/nrcardio.2017.189
17. Dar T, Radfar A, Abohashem S, Pitman RK, Tawakol A, Osborne MT. Psychosocial stress and cardiovascular disease. Curr Treat Options Cardiovasc Med. (2019) 21(5):1–17. doi: 10.1007/s11936-019-0724-5
18. Galli F, Bursi F, Carugo S. Traumatic events, personality and psychopathology in takotsubo syndrome: a systematic review. Front Psychol. (2019) 10:27–42. doi: 10.3389/fpsyg.2019.02742
19. Gorini A, Galli F, Giuliani M, Pierobon A, Werba JP, Adriano EP, et al. Psychological characteristics of patients with takotsubo syndrome and patients with acute coronary syndrome: an explorative study toward a better personalized care. J Pers Med. (2022) 12(1):38. doi: 10.3390/jpm12010038
20. Amadio P, Porro B, Cavalca V, Barbieri SS, Eligini S, Fiorelli S, et al. Persistent long-term platelet activation and endothelial perturbation in women with takotsubo syndrome. Biomed Pharmacother. (2021) 136:111259. doi: 10.1016/j.biopha.2021.111259
21. Pimple P, Lima BB, Hammadah M, Wilmot K, Ramadan R, Levantsevych O, et al. Psychological distress and subsequent cardiovascular events in individuals with coronary artery disease. J Am Hear Assoc Cardiovasc Cerebrovasc Dis. (2019) 8(9):e011866. doi: 10.1161/JAHA.118.011866
22. Denollet J. DS14: standard assessment of negative affectivity, social inhibition, and type D personality. Psychosom Med. (2005) 67(1):89–97. doi: 10.1097/01.psy.0000149256.81953.49
23. Staniute M, Brozaitiene J, Burkauskas J, Kazukauskiene N, Mickuviene N, Bunevicius R. Type D personality, mental distress, social support and health-related quality of life in coronary artery disease patients with heart failure: a longitudinal observational study. Heal Qual Life Outcomes. (2015) 13(1):1–11. doi: 10.1186/s12955-014-0204-2
24. Gili S, Giuliani M, Santagostino Baldi G, Teruzzi G, Pravettoni G, Montorsi P, et al. Early detection of cardiovascular risk factors and definition of psychosocial profile in women through a systematic approach: the monzino women heart center’s experience. Front Cardiovasc Med. (2022) 9. doi: 10.3389/fcvm.2022.844563
25. Pedrabissi L, Santinello M. Verifica della validità dello STAI forma Y di spielberger. [verification of the validity of the STAI, form Y, by spielberger.]. Giunti Organ Spec. (1989):191–2. 11–4.
26. Mondo M, Sechi C, Cabras C. Psychometric evaluation of three versions of the Italian perceived stress scale. Curr Psychol. (2019) 40(4):1884–92. doi: 10.1007/s12144-019-0132-8
27. Gremigni P, Sommaruga M. Personalità di tipo D, un costrutto rilevante in cardiologia. Studio preliminare di validazione del questionario italiano. Psicoter Cogn e Comport. (2005) 11(1):7–18. doi: 10.13140/2.1.2918.9765
28. Sica C, Ghisi M. The Italian versions of the beck anxiety inventory and the beck depression inventory-II: psychometric properties and discriminant power. Leading-edge Psychol Tests Test Res. (2007):27–50.
29. Beck AT, Steer RA, Brown GK. Manual for the Beck Depression Inventory-II. San Antonio, TX: Psychological Corporation (1996).
30. Spielberger CD. State-trait anxiety inventory. In: The Corsini Encyclopedia of Psychology. Hoboken, NJ, USA: John Wiley & Sons, Inc. (2010). p. 1–1. doi: 10.1002/9780470479216.corpsy0943 (cited May 11, 2020)
31. Spielberger C, Pedrabissi L, Santinello M. STAI: State-trait Anxiety Inventory: Forma Y: Manuale. Adattamento Italiano a Cura di Luigi Pedrabissi e Massimo Santaniello. (1996). Available online at: http://www.cbt.biblioteche.provincia.tn.it/oseegenius/resource?uri=6131914 (cited July 8, 2020)
32. Cohen S, Kamarck T, Mermelstein R. A global measure of perceived stress. J Health Soc Behav. (1983) 24(4):385–96. doi: 10.2307/2136404
33. Gordon RSJ. An operational classification of disease prevention. Public Health Rep. (1983) 98:107–9. PMID: 6856733; PMCID: PMC14244156856733
34. Silverman MM, Felner RD. Suicide prevention programs: issues of design, implementation, feasibility, and developmental appropriateness. Suicide Life Threat Behav. (1995) 25(1):92–104. doi: 10.1111/j.1943-278X.1995.tb00395.x
35. Barger SD, Struve GC. Association of depression with 10-year and lifetime cardiovascular disease risk among US adults, national health and nutrition examination survey, 2005–2018. Prev Chronic Dis. (2022) 19:E28. doi: 10.5888/pcd19.210418
36. Lichtman JH, Bigger JT, Blumenthal JA, Frasure-Smith N, Kaufmann PG, Lespérance F, et al. Depression and coronary heart disease: recommendations for screening, referral, and treatment—a science advisory from the American heart association prevention committee of the council on cardiovascular nursing, council on clinical cardiology, council on epidemiology and prevention, and interdisciplinary council on quality of care and outcomes research. Circulation. (2008) 118:1768–75. doi: 10.1161/CIRCULATIONAHA.108.190769
37. Mosarla RC, Wood M. The impact of depression and anxiety on cardiovascular disease risk and outcomes in women. Curr Treat Options Cardiovasc Med. (2021) 23(2):1–12. doi: 10.1007/s11936-020-00889-9
38. Matthews K, Owens J, Kuller L, Sutton-Tyrrell K, Jansen-McWilliams L. Are hostility and anxiety associated with carotid atherosclerosis in healthy postmenopausal women? Psychosom Med. (1998) 60(5):633–8. doi: 10.1097/00006842-199809000-00021
39. Mols F, Denollet J. Type D personality in the general population: a systematic review of health status, mechanisms of disease, and work-related problems. Health Qual Life Outcomes. (2010) 8(1):9. doi: 10.1186/1477-7525-8-9
40. Al-Qezweny MNA, Utens EMWJ, Dulfer K, Hazemeijer BAF, Van Geuns RJ, Daemen J, et al. The association between type D personality, and depression and anxiety ten years after PCI. Netherlands Hear J. (2016) 24(9):538–43. doi: 10.1007/s12471-016-0860-4
41. Vasan RS, van den Heuvel E. Differences in estimates for 10-year risk of cardiovascular disease in black versus white individuals with identical risk factor profiles using pooled cohort equations: an in silico cohort study. Lancet Digit Heal. (2022) 4(1):e55–63. doi: 10.1016/S2589-7500(21)00236-3
Keywords: anxiety, depression, distress, Type-D personality, gender medicine, cardiovascular prevention
Citation: Giuliani M, Santagostino Baldi G, Capra N, Bonomi A, Marzorati C, Sebri V, Guiddi P, Montorsi P, Pravettoni G and Trabattoni D (2024) The heart-mind relationship in women cardiovascular primary prevention: the role of depression, anxiety, distress and Type-D personality in the 10-years cardiovascular risk evaluation. Front. Cardiovasc. Med. 11:1308337. doi: 10.3389/fcvm.2024.1308337
Received: 6 October 2023; Accepted: 22 February 2024;
Published: 7 March 2024.
Edited by:
Pensée Wu, Keele University, United KingdomReviewed by:
Clementine Labrosciano, University of Adelaide, Australia© 2024 Giuliani, Santagostino Baldi, Capra, Bonomi, Marzorati, Sebri, Guiddi, Montorsi, Pravettoni and Trabattoni. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Daniela Trabattoni ZGFuaWVsYS50cmFiYXR0b25pQGNjZm0uaXQ=
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.