
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
STUDY PROTOCOL article
Front. Cardiovasc. Med. , 29 January 2024
Sec. Cardiac Rhythmology
Volume 11 - 2024 | https://doi.org/10.3389/fcvm.2024.1303540
 Ruowu Qiu1,2,†
Ruowu Qiu1,2,† Qingqing Ni1,2,†
Qingqing Ni1,2,† Muli Wu1,3,†
Muli Wu1,3,† Zhongbo Xiao1,3,†Jiaxin Xiao1,3Weizhao Lin4Weipeng Huang5
Zhongbo Xiao1,3,†Jiaxin Xiao1,3Weizhao Lin4Weipeng Huang5 Yequn Chen1,3Chang Chen1,3*Liekai Hong1,2,3*
Yequn Chen1,3Chang Chen1,3*Liekai Hong1,2,3*
Introduction: A high recurrence rate of atrial fibrillation was monitored after catheter ablation for persistent atrial fibrillation. Sacubitril/valsartan can improve outcomes for patients with heart failure and ventricular tachycardia, but few studies examined whether it can reduce recurrence or improve cardiovascular outcomes in patients with persistent atrial fibrillation after catheter ablation. In this study, we will assess the effect of sacubitril/valsartan on sinus rhythm maintenance and incidence of major adverse cardiovascular events (MACE) in patients with persistent atrial fibrillation after catheter ablation through a randomized controlled trial (RCT).
Methods: This is a multi-center, randomized, controlled, open-label, superiority clinical trial involving 462 patients without reduced ejection fraction heart failure after catheter ablation of persistent atrial fibrillation. Patients will be randomized to (1) receive the standard treatment strategy plus sacubitril/valsartan titration, or (2) receive the standard treatment strategy without taking sacubitril/valsartan. The primary outcome will be sinus rhythm maintenance rate over 12 months, monitored by random electrocardiogram and 24-h Holter electrocardiogram.
Discussion: This study is designed to evaluate the effect of sacubitril/valsartan on sinus rhythm maintenance and incidence of major adverse cardiovascular events (MACE) in patients with persistent atrial fibrillation after catheter ablation. The results will evaluate sacubitril/valsartan as a novel treatment for improving prognosis and a complement to conventional drug therapy.
Trial Registration: Registered with Chinese Clinical Trials Registry on 27 August 2022, identifier: ChiCTR2200062995.
Atrial fibrillation (AF) now has become a common clinical arrhythmia and refers to the loss of ordered electrical activity in the atria. In China, the available evidence infers that the prevalence of AF in China is 2.32% among people over 65 years old (1–4). The incidence of AF has increased continuously over the past decades, and the rates of hospitalization and fatality are also increasing (5). Based on the duration of AF, AF can be divided into five categories: first diagnosed AF (AF not previously diagnosed), paroxysmal AF (duration < 7 days), persistent AF (duration > 7 days), long-standing persistent AF (duration > 1 year), and permanent AF (diagnosed as AF, patient and doctor have reached an agreement and will no longer attempt to restore sinus rhythm). The sustained onset of atrial fibrillation significantly increases the risk of cardiovascular and cerebrovascular accidents, affecting quality of life and survival of patients. A cohort study showed that the proportion of HF patients with AF is as high as 24.4%, and HF can make further efforts to induce AF (6). Chronic heart failure and persistent atrial fibrillation can promote each other, thus entering a vicious cycle (7, 8).
The therapy of atrial fibrillation has become an increasingly great challenge in the cardiovascular field. Catheter ablation has been confirmed to be an effective way to treat atrial fibrillation, and it has become the most recommended treatment option for symptomatic atrial fibrillation (9). Cochrane systematic reviews have also shown that ablation of persistent AF had a greater advantage in prognosis than anti-arrhythmic drug treatment in eliminating atrial arrhythmias, reducing the need for cardioversion and the risk of hospitalization for cardiac reasons (10). However, the recurrence rate of AF still remained high in patients after catheter ablation, with incidence of early postoperative recurrence (3–12 months) being 25%–40% (11). The CABANA clinical study showed a recurrence rate of 49.9% in the AF ablation group during a long period of follow-up (12). After undergoing catheter ablation, the recurrence rate of persistent AF is higher compared to paroxysmal AF (11). Reducing the recurrence of atrial fibrillation can effectively improve the prognosis of catheter ablation.
Sacubitril/valsartan is the first angiotensin receptor-neprilysin inhibitor (ARNI) with a dual-target inhibitory effect. Studies have shown that AF patients with HF, treated with ARNI, tended to reduce the risk of hospitalization, reversal of cardiac remodeling, and corrected cardiac function after catheter ablation of AF (13–15). However, there is a lack of randomized controlled trials (RCT) to show a therapeutic effect of ARNI in patients with persistent AF after catheter ablation. We will evaluate the effect of ARNI on sinus rhythm maintenance rate and incidence of MACE in patients with persistent AF after catheter ablation in this study through a randomized controlled trial.
This prospective trial is a multi-center, randomized, controlled, open-label, superiority trial with a 1:1 ratio of trial and controls. A total of 462 patients with persistent atrial fibrillation after catheter ablation will be recruited in three centers (the First Affiliated Hospital of Shantou University Medical College, Second Affiliated Hospital of Shantou University Medical College, and Jieyang People's Hospital) from August 2022 through August 2025. This protocol is designed according to the Standard Protocol Items: Recommendations for Interventional Trials (SPIRIT) 2013 Statement (16).
The overall expectation is that patients taking sacubitril/valsartan with persistent atrial fibrillation after catheter ablation will have better sinus rhythm maintenance and cardiovascular outcomes within 12 months than those not taking. This prediction will be tested with the following three objectives. The primary objective will be to evaluate the efficacy of sacubitril/valsartan on sinus rhythm maintenance after ablation of persistent AF patients in this trial. Whether sacubitril/valsartan decreases the incidence of MACE and improves structural indices of the atrium in patients with AF is the secondary objective of this study. The third objective will be to determine the efficacy of sacubitril/valsartan on re-hospitalization rates for cardiovascular causes.
Patients will be recruited at The First Affiliated Hospital of Shantou University Medical College, The Second Affiliated Hospital of Shantou University Medical College, and Jieyang People's Hospital, three medical centers in Guangdong province. A well-trained research team composed of clinicians familiar with the diagnosis and treatment of atrial fibrillation was set up to screen patients who may meet the research criteria.
Ethical approval was obtained before the start of this study from the Committee of Ethics of the First Affiliated Hospital of Shantou University Medical College (Number: B-2022-170-XZ1).
(1) Adult (age ≥ 18), male or female
(2) Physical condition allows oral medication
(3) Patients without HFrEF (heart failure with LVEF ≤ 40%)
(4) Patients who have a clinical diagnosis of persistent AF (AF lasting >7 days, Holter ECG >24 h will be completed before procedure) and have undergone catheter ablation (successful conversion of rhythm and immediately complete electrocardiogram after procedure)
(5) Understand the purpose of the trial and agree to all the study steps, voluntarily sign the informed consents, and be willing to undergo follow-up.
(1) Pregnant and lactating women
(2) Patients with previous ablations (percutaneous or surgical)
(3) Acute coronary syndrome (including myocardial infarction), acute stroke, or emergency coronary intervention within 3 months prior to enrollment
(4) Heart failure: a clinical diagnosis of heart failure, and transthoracic heart color ultrasound indicates that the left ventricular ejection fraction is 40% or less
(5) Patients with acute infectious diseases, important organ injuries, malignant tumors
(6) Severe liver insufficiency (Child-Pugh level C) and severe renal insufficiency (eGFR <30 ml/min/L.73 m2)
(7) The average blood pressure of the three postoperative measurements is lower than 90/60 mmHg
(8) Abnormal coagulation mechanism and immune function
(9) The subject is currently taking part in another clinical study
(10) The investigator considers that the subject is unable to follow the protocol requirements or for any reason considers that the subject is not eligible for the study
(11) Allergic to the active ingredient of sacubitril/valsartan or any excipients.
Patients can voluntarily withdraw from this clinical trial at any time. Patients who experience the following conditions will also withdraw from the trial:
(1) Serious adverse events (AEs) occurred throughout the entire trial process
(2) Unable to continue cooperating with clinical examinations and follow-up due to unexpected reasons.
Throughout the entire trial enrollment process, patients who have been assessed as eligible for enrollment will be introduced to the research content and specific process by trained researchers, ensuring that patients fully understand the benefits and potential risks of the trial. At the same time, patients will be informed that whether they participate or not will not affect their normal treatment and all participants' personal information will always be kept confidential. Patients will have 24 h to consider and make decisions. All participating patients must sign the informed consent.
Patients who meet the inclusion criteria, successfully converted to sinus rhythm and were confirmed by electrocardiogram immediately after ablation will be enrolled. Randomization will be performed after the ablation. After eligible patients sign the informed consent, baseline information will be collected, including basic information, medical history, preoperative medication history, electrocardiogram and laboratory results. Researchers will randomly allocate eligible patients at a 1:1 ratio to receive sacubitril/valsartan or not. This trial will be randomized using a dynamic stratified block group randomization method. The R package blockrand (R version 4.1.2) was used to generate a randomization table with a specified sample size, and the block sizes were randomized among 4, 6, and 8 to form the randomization pool for this trial. The trial was stratified by research centers, each of which was assigned random numbers for a block unit by “first-come, first-served”, and the random number for the next block was available in the randomization pool only when the random number for that block was used up. The process of generating the randomization table and assigning randomized numbers for this study was carried out by an independent researcher who was not involved in recruitment and subsequent interventions. After a subject had consented to participate in the trial, the recruiting physician queried the randomization number from the investigator in charge of randomization, who provided the patient's treatment allocation plan based on the participant's center and order of inclusion, as well as marked the grouping on the randomization table.
For all patients enrolled, if they are taking ACEI drugs, they will be given the trial drug starting 36 h after discontinuation of ACEI drugs. The control group will be given conventional perioperative medications according to guidelines of atrial fibrillation, and the trial group will receive conventional perioperative drug therapy plus sacubitril/valsartan (Beijing Novartis Pharmaceutical Company, J20171054). The test drug will be titrated according to Figure 1. The target maintenance dose is 100 mg twice per day. Based on the patient tolerance, drug dosage will be doubled every 2 weeks. If the patient cannot tolerate the maximum dose, the dose will be reduced to the maximum dose tolerated by the patient. In order to increase patient medication compliance, patients will be reminded to take drugs on time by WeChat. When patients change the dose, patients will be required to bring the packaging box of the drugs. Blood pressure, blood potassium and renal function examination will be performed at each follow-up period. If hypotension or symptomatic hypotension occurs, the dose will be adjusted.
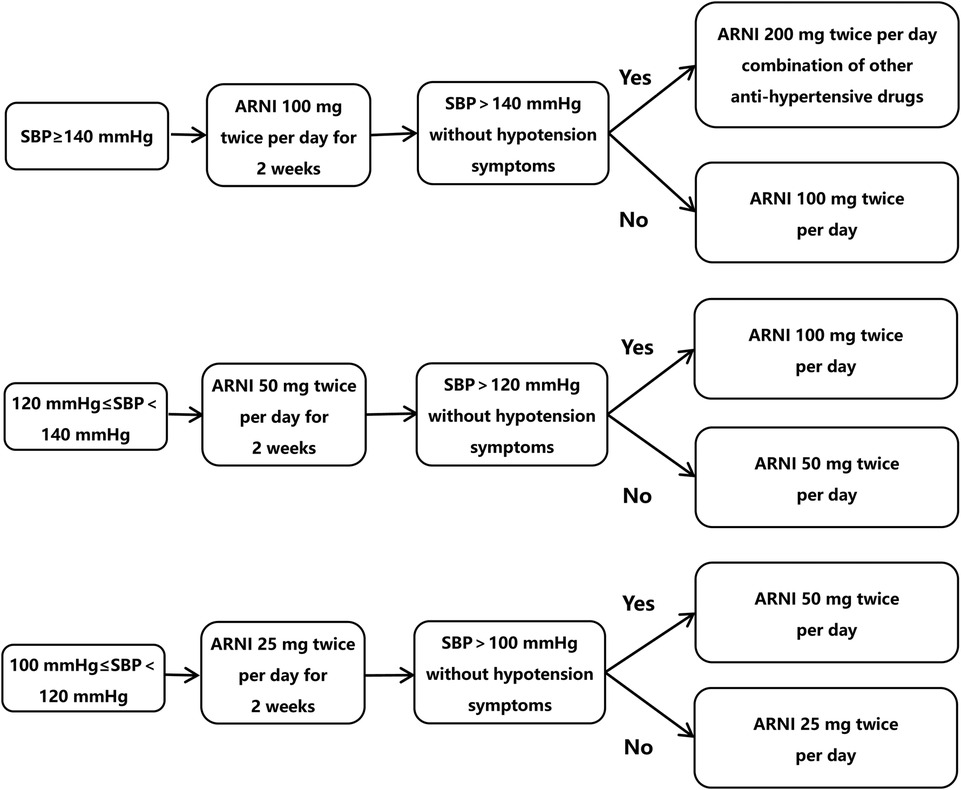
Figure 1. Drug dose titration.
All patients will underwent pulmonary vein isolation (PVI) using radiofrequency energy and a three-dimensional electroanatomical mapping system (CARTO, Biosense Webster). Additional ablation lines (roof line of the LA, mitral isthmus line, or cavo-tricuspid isthmus line) or ablation of complex fractioned electrograms would not be performed during procedure for enrolling patients.. The endpoint for complex fractionated atrial electrogram ablation is a complete abatement of potentials at these sites.
Patients will be treated by standard treatment according to current guidelines (11). They will be on an uninterrupted anticoagulation regimen during the perioperative period. Uninterrupted oral anticoagulation will be taken based on stroke/thromboembolic risk during the perioperative period of AF catheter ablation for enrolling patients (9). Patients can use antiarrhythmic drugs such as Class III drugs (amiodarone) when appropriate based on the judgment of the responsible physician during the 3-month blanking period.
This trial is designed as an open label. Trial participants and care givers will not be blinded to the group assignment while the investigator or other relevant personnel will not be made aware of the information about the treatment subgroup to which they are assigned until the order of enrollment/randomization of the subjects has been confirmed. Data analysts and outcome evaluator will remain blinded to minimize trial bias.
The primary endpoint of the study will be the sinus rhythm maintenance rate within 12 months determined by at least the 24-hour Holter electrocardiogram. Patients will be given the Holter electrocardiogram at 3, 6 months and 12 months.
The secondary endpoint will be the sinus rhythm maintenance rate at 3 and 6 months and incidence of MACE at 3, 6, and 12 months. Cardiovascular re-hospitalization at 3, 6, and 12 months will be aggregated in HFpEF patients with AF and patients with AF and otherwise normal cardiac function. Changes in cardiac structural function indicators will be observed at 3, 6, and 12 months. Echocardiographic parameters such as LAD, LAVi, LAEF will be recorded or calculated.
This study will also analyze the safety profile focusing on the incidence of adverse events at months 3, 6, and 12. Blood pressure will be measured and potassium and renal function will be tested during follow-up period. The main adverse events will include hypotension, hyperkalemia and renal function impairment that cannot be improved by dose reduction. Hyperkalemia (blood potassium > 5.5 mmol/L), hypotension (SBP < 90 mmHg or DBP < 60 mmHg), symptomatic hypotension (SBP ≥ 90 mmHg and dizziness, nausea, fatigue, syncope), and creatinine increase more than 50% will be considered as adverse reactions.
This study differentiate different cardiovascular causes for re-hospitalization into cardioversion, repeat ablation, heart failure, acute coronary syndrome, stroke or transient ischemic attack, or other cardiovascular-related diseases.
MACE are defined as heart failure, myocardial infarction, stroke, malignant arrhythmia and cardiac death. The specific definitions are as follows:
(1) Definition of heart failure: patients who had a history of HF-plausible symptoms, physical examination changes, electrocardiogram changes, cardiac ultrasound changes, and elevated serological markers of heart failure (NT-proBNP > 125 pg/ml or BNP ≥ 35 pg/ml) will be clinically diagnosed as heart failure according to the 2022 AHA/ACC/HFSA Guidelines: Management of Heart Failure. Heart failure with reduced ejection fraction (HFrEF) is classified as an LVEF ≤ 40% (17).
(2) Definition of acute coronary syndrome: includes ST-segment elevation myocardial infarction (STEMI), non-ST-segment elevation myocardial infarction (NSTEMI), and unstable angina (UA) according to the guidelines for rapid diagnosis and treatment of acute coronary syndromes in emergency medicine (18).
(3) The diagnosis of malignant arrhythmia (MA) refers to the diagnostic criteria for malignant arrhythmia in the 2020 American Heart Association Guidelines for Resuscitation and Emergency Cardiovascular Care (19). MA includes ventricular arrhythmias (ventricular tachycardia and ventricular fibrillation) and grade II or III atrioventricular block. Each type of MA may occur alone or in combination with other types at the same time.
After randomization, subjects will have follow-up after 3, 6 and 12 months, mainly in the outpatient clinic according to Figure 2.
(1) The survival status will be confirmed and rehospitalization and occurrence of MACE events will be requested by telephone
(2) Holter electrocardiogram (>24 h), transthoracic heart color ultrasound, blood test of blood potassium and kidney function will be performed in the outpatient clinic
(3) Adverse event assessment, the main adverse reactions assessed will be: hypotension, high blood potassium, impairment of renal function, as determined in the outpatient clinic
(4) Medication consumption in the past will be requested by telephone;
(5) Drug bottles will be collected, and the subject reminded of the importance of study medication compliance by the outpatient clinic.
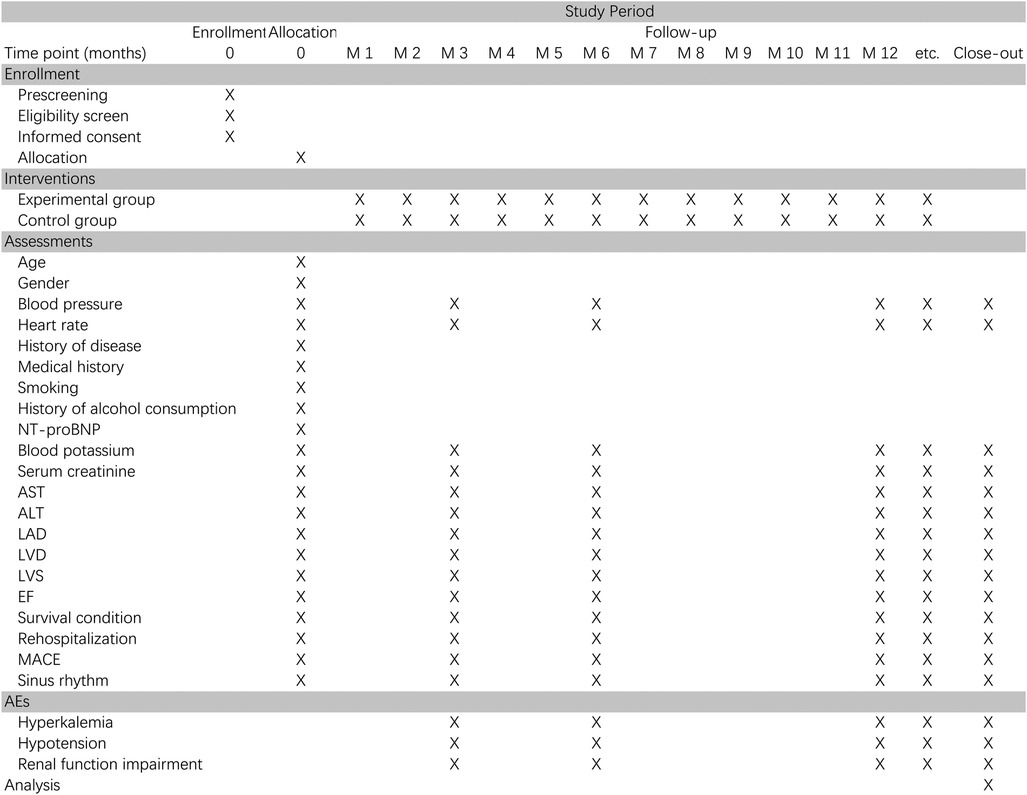
Figure 2. Schedule of enrollment, interventions and assessments for the trial.
The determination of the sample size in this study will be driven by the need of the above strategy to detect sacubitril/valsartan over conventional drugs.
The recurrence rate of atrial fibrillation after 12 months in patients with persistent AF is approximately 42% (15), and we expect a 20% decrease in the incidence of primary endpoint events taking ARNI after catheter ablation in patients with persistent AF. Under the assumption based on the exponential distribution, the risk ratio is 0.46.
Based on the above assumptions, the expected enrollment time is 24 months, without considering the mid-term analysis, and the minimum follow-up time is 12 months. Assuming a 20% missing visit in each of the control and trial groups, the study requires 450 participants (225 trial group, 225 control group) to obtain 90% difference at a significance level of a = 0.05 (unilateral). The sample size is calculated by PASS15.0 software. The interim analyses is set up by the O'Brien-Fleming method to control the overall Type I error below 0.05. The final sample size will be 462 cases (231 trial group, 231 control group).
Blank case report forms (CRFs) that has been ethically approved will be used to record data for all participants. Each enrolled patient corresponds to a complete CRF, and unrecorded data will be labeled and justified. The CRFs will be entered into the scientific research platform of the First Affiliated Hospital of Shantou University Medical School in a double-entry manner by researchers. Researchers are responsible for the completeness and accuracy of the records. A CRF will include:
(1) Medical history or medical examination data
(2) Informed consent of the subjects and the randomization number of this trial
(3) Time of each follow-up visit and signed notes
(4) Reported adverse events and their resolution or absence, including documentation such as hospitalization records, discharge summary, ECG, etc
(5) Record of the medication use of the test subjects during the trial
The statistical analysis will be along with the intention-to-treat (ITT) principles. The ITT population will include patients who meet the criteria, are randomized, and take at least one dose of drugs after being enrolled. For statistical description, continuous variables are described by using mean and standard deviation if they satisfy a normal distribution, skewed distributions are described by medians and quartiles, while categorical variables will be presented as frequency or percentage in each category. For the baselines, the t-test is used to compare the differences for quantitative variable if the data meets the normality test, otherwise, the data will be transformed or rank sum test. Categorical variables such as disease history and smoking history can be tested using chi-square test or rank sum test. For outcomes such as 239sinus rhythm maintenance rate, all-cause death, re-hospitalization rate for cardiovascular causes and MACE, Kaplan-Meier curves will be used to characterize how the probability of an endpoint event changes with survival time, and comparisons between survival curves will be carried out using log-rank tests. We used cox proportional hazards models to estimate hazard ratios and 95% confidence intervals. Cardiac structural function indicators will be described by mean value (±SD) or median and quartiles, and the sphericity of the covariance array will be tested by the Mauchly method. If the data satisfies the sphericity of the covariance array, the analysis of variance with repeated measures data will be used for group comparisons of each indicator. If it is not satisfied, the Greenhouse-Geisser method will be used for comparison of differences. Missing observations will be accounted for using the predictive mean matching (PMM) method. If the missing data is numerical, it will be filled by predictive mean matching; meanwhile if the missing data is non-numerical, logistic regression and discriminant functions will be used to fill it. The p-value threshold is 0.05(p < 0.05), and when it is below this threshold, indicating that the difference is statistical significant. SPSS statistical software (SPSS Inc, Chicago, IL, USA, version 23) will be used to analyse data.
Interim analyses of key safety and endpoint metrics will be conducted periodically during the course of the trial. Two interim analyses will be conducted when 33% and 67% of the total number of planned primary endpoint events have been reached. Interim analyses will be performed using the O'Brien-Fleming method to maintain an overall significance level of 0.05. The significance level alpha for the two interim and final analyses is 0.0015, 0.0172, and 0.0313, respectively. The independent Data Monitoring Committee will review the safety and efficacy of the trial based on interim analysis results.
The trial will be conducted following the approved protocol. An independent committee of data and safety monitoring has been established to oversee the trial. Five chairpersons will be set up in the committee composed of independent researchers, while ensuring that committee members are not involved in the trial operation and have no conflicts of interest with this study. The data and safety monitoring committee will review and supervise the reliability and completeness of research data on the basis of ensuring the physical safety and data security of participants.
Events that are fatal, life-threatening, disabling or incapacitating, or leading to prolonged hospital stay or malformation are defined as serious adverse events in this trial.
The patient blood pressure will be observed by follow-up, and blood samples will be tested for potassium and renal function. The main adverse events will include hypotension, hyperkalemia and renal function impairment that cannot be improved by dose reduction. Adverse reaction criteria: hyperkalemia (blood potassium > 5.5 mmol/L), hypotension (SBP < 90 mmHg or DBP < 60 mmHg), symptomatic hypotension (SBP ≥ 90 mmHg and dizziness, nausea, fatigue, syncope), and creatinine increase more than 50% will be considered as adverse events.
A detailed report will be submitted to the Medicines and Healthcare Products Regulatory Agency in a timely manner when unexpected serious adverse events occur. All patients participating in the trial will receive insurance, including additional healthcare, compensation, or damages. All adverse events which may possibly related to the trial will be recorded in the CRFs.
During the course of the study, representatives of the ethics committee will conduct reviews in accordance with national regulations. If there is a need to make changes to the protocol, an application will be submitted in advance to the ethics committee and regulatory agencies for approval, then recorded in the form of an amendment to the protocol.
There was no public or patient involvement in the conceptualization of the study. The research results will be analyzed and be part of written article for publication.
This is a randomized, controlled, open-label, superiority clinical trial designed to explore the efficacy of sacubitril/valsartan on sinus rhythm maintenance in patients with persistent AF after catheter ablation. As a common cardiac arrhythmia worldwide, atrial fibrillation is closely related to various adverse outcomes and economic burden. It has been shown that persistent AF as an independent influencing factor is more significantly associated with increased mortality or all-cause hospitalization compared with paroxysmal AF or first diagnosed AF (20, 21). Cardiac electrical remodeling, due to cardiac reconstruction, left atrial volume enlargement, and atrial fibrosis, is important to the development and progression of atrial fibrillation. Especially in persistent atrial fibrillation patients, long-term arrhythmia further aggravate the electrical remodeling of the heart, while the chances of heart failure attacks are greatly increased. Otherwise, heart failure can cause atrial dilatation, which leads to cardiac damage and fibrosis (22, 23). All of these significantly contribute to the deterioration of AF patients. Catheter ablation of AF is an effective therapy and has become the first choice of treatment for symptomatic atrial fibrillation (9). However, patients with persistent AF after catheter ablation still remain a significant recurrence rate, which may be associated with heart reconstruction, partial myocardial fibrosis and structural changes that cannot be completely reversed by the procedure. Reducing the recurrence of atrial fibrillation can effectively improve the prognosis of catheter ablation.
Sacubitril/valsartan is the first angiotensin receptor-neprilysin inhibitor (ARNI) with a dual-target inhibitory effect. The mechanism of action is to reduce myocardial fibrosis and improve cardiac remodeling by inhibiting the RAAS system, modulating the natriuretic peptide system, and restoring neurohumoral homeostasis (24). The PARADIGM study and the PARAMOUNT study both showed good efficacy of ARNI (25, 26), which became the recommended drug in the guidelines for HF with reduced ejection fraction (17, 27). However, the PARAGON-HF study presented at the 2019 European Cardiovascular Congress ESC suggested that the trial and control groups of patients with preserved ejection heart failure (HFpEF) did not show a statistical difference, and the effect of ARNI in patients with non-reduced ejection fraction HF remains controversial (28). So, patients with reduced ejection fraction HF will be excluded in this trial to avoid ethical conflicts.
The anti-arrhythmic efficacy of sacubitril/valsartan is also being noticed by researchers. ARNI can reduce atrial arrhythmic events in HF with reduced ejection fraction. It is shown that a trend toward a reduction in the frequency of atrial arrhythmia events after nine months of taking ARNI, suggesting a possible link between ARNI and atrial arrhythmia (24). Sacubitril acts synergistically by modulating the natriuretic peptide system, thus allowing ARNI to make greater contributions in reversing atrial remodeling. So, it is reasonable to postulate that the use of ARNI after catheter ablation of atrial fibrillation reverses left atrial electrical remodeling and positively contributes to sinus rhythm maintenance after catheter ablation. Okutucu from Turkey found that the P-wave dispersion and maximum P-wave time frame improved by using ARNI in 28 patients with reduced ejection fraction HF, suggesting that ARNI may have reversed left atrial remodeling in patients with reduced ejection fraction HF (29). Also, DeVecchis published a retrospective cohort study showing that patients with HF combined with atrial fibrillation had an increasing peak atrial longitudinal strain (PALS) after ARNI treatment, which also reduced the risk of atrial fibrillation recurrence in such patients (30). Li from China found that rabbits with heart failure experienced prolongation of the effective atrial and ventricular induction periods and altered calcium channel proteins in a rabbit model of AF. These results suggest that ARNI improves atrial electrical and structural remodeling in AF (31). We surmise that Sacubitril/valsartan can reverse cardiac remodeling and reduce myocardial fibrosis, so as to reduce the recurrence of AF and the incidence of adverse cardiovascular outcomes in order to improve the prognosis of catheter ablation.
ARNI also has been approved for the therapy of hypertension and has a strong anti-hypertensive effect. In clinical practice, hypertension is a high-risk factor for HF in atrial fibrillation patients. The anti-hypertensive function of ARNI may contribute to reduce the incidence of adverse cardiovascular events after catheter ablation of AF (32).
In conclusion, ARNI may reduce the recurrence of AF and the incidence of cardiovascular adverse events due to reduction of myocardial fibrosis, reversing cardiac remodeling and controlling blood pressure. However, there lack multi-center randomized controlled clinical trials showing the effect of ARNI in patients with persistent AF after catheter ablation. Therefore, we will confirm the effect of ARNI on the prognosis of patients with persistent AF after catheter ablation through a RCT by evaluating sinus rhythm maintenance rate and incidence of MACE in patients. The results of this trial will further explore the application scope of ARNI and the possibility of improving prognosis after catheter ablation.
Firstly, this is an open-label clinical trial and the results can not represent all AF patients. Secondly, lack of continuous ECG monitoring (such as a handheld smartphone ECG device) at patient follow-up allows for the possibility that some atrial arrhythmias are not monitored, and the chance of false negatives is increased.
The recruitment date is from 2022/08/30 To 2025/08/30. The trial is currently recruiting patients.
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
The studies involving humans were approved by the Committee of Ethics of the First Affiliated Hospital of Shantou University Medical College. The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
RQ: Writing – original draft, Writing – review & editing. QN: Writing – review & editing. MW: Writing – review & editing. ZX: Writing – review & editing. JX: Writing – review & editing. WL: Writing – review & editing. WH: Writing – review & editing. YC: Writing – review & editing. CC: Writing – original draft, Writing – review & editing. LH: Writing – original draft, Writing – review & editing.
The author(s) declare financial support was received for the research, authorship, and/or publication of this article.
This work is supported by the following funding bodies: 1. Supported by 2021 Special Fund Project for Science and Technology Innovation Strategy of Guangdong Province (2021-88-53); 2. Supported by 2022 Special Fund Project for Science and Technology Innovation Strategy of Guangdong Province (2022-124-6).
We appreciate the efforts of all research staff participating in this trial. We also acknowledge the helpful support from all participants.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Zoni-Berisso M, Lercari F, Carazza T, Domenicucci S. Epidemiology of atrial fibrillation: European perspective. Clin Epidemiol. (2014) 6:213–20. doi: 10.2147/CLEP.S47385
2. Schnabel RB, Yin X, Gona P, Larson MG, Levy D. 50 Year trends in atrial fibrillation prevalence, incidence, risk factors, and mortality in the Framingham heart study: a cohort study. Lancet. (2015) 386(9989):154–62. doi: 10.1016/S0140-6736(14)61774-8
3. Xuejuan J, Jingmin Z. The coexistence of heart failure and atrial fibrillation: progress in epidemiology and related clinical research. Journal of Clinical Cardiology. (2019) 35(3):199–202. doi: 10.13201/j.issn.1001-1439.2019.03.002
4. Khan MA, Neyses L, Mamas MA. Atrial fibrillation in heart failure: an innocent bystander? Curr Cardiol Rev. (2012) 8(4):273–80. doi: 10.2174/157340312803760839
5. Kornej J, Borschel CS, Benjamin EJ, Schnabel RB. Epidemiology of atrial fibrillation in the 21st century: novel methods and new insights. Circ Res. (2020) 127(1):4–20. doi: 10.1161/CIRCRESAHA.120.316340
6. Anter E, Jessup M, Callans DJ. Atrial fibrillation and heart failure: treatment considerations for a dual epidemic. Circulation. (2009) 119(18):2516–25. doi: 10.1161/CIRCULATIONAHA.108.821306
7. Richter S, Di Biase L, Hindricks G. Atrial fibrillation ablation in heart failure. Eur Heart J. (2019) 40(8):663–71. doi: 10.1093/eurheartj/ehy778
8. Skanes AC, Tang ASL. Atrial fibrillation and heart failure: untangling a modern Gordian knot. Can J Cardiol. (2018) 34(11):1437–48. doi: 10.1016/j.cjca.2018.07.483
9. Hindricks G, Potpara T, Dagres N, Arbelo E, Bax JJ, Blomstrom-Lundqvist C, et al. 2020 ESC guidelines for the diagnosis and management of atrial fibrillation developed in collaboration with the European association for cardio-thoracic surgery (EACTS): the task force for the diagnosis and management of atrial fibrillation of the European society of cardiology (ESC) developed with the special contribution of the European heart rhythm association (EHRA) of the ESC. Eur Heart J. (2021) 42(5):373–498. doi: 10.1093/eurheartj/ehaa612
10. Margulescu AD, Mont L. Persistent atrial fibrillation vs paroxysmal atrial fibrillation: differences in management. Expert Rev Cardiovasc Ther. (2017) 15(8):601–18. doi: 10.1080/14779072.2017.1355237
11. Electrophysiology CSoPa, Arrhythmias CSo, China AFCUo. Current knowledge and management of atrial fibrillation: consensus of Chinese experts 2021. Chin J Cardiac Arrhythmias. (2022) 26(1):74. doi: 10.3760/cma.j.cn113859-20211224-00264
12. Packer DL, Mark DB, Robb RA, Monahan KH, Bahnson TD, Poole JE, et al. Effect of catheter ablation vs antiarrhythmic drug therapy on mortality, stroke, bleeding, and cardiac arrest among patients with atrial fibrillation: the CABANA randomized clinical trial. JAMA. (2019) 321(13):1261–74. doi: 10.1001/jama.2019.0693
13. Kaplinsky E. Sacubitril/valsartan in heart failure: latest evidence and place in therapy. Ther Adv Chronic Dis. (2016) 7(6):278–90. doi: 10.1177/2040622316665350
14. Suo Y, Yuan M, Li H, Zhang Y, Li Y, Fu H, et al. Sacubitril/valsartan improves left atrial and left atrial appendage function in patients with atrial fibrillation and in pressure overload-induced mice. Front Pharmacol. (2019) 10:1285. doi: 10.3389/fphar.2019.01285
15. Wang Q, Zhuo C, Xia Q, Jiang J, Wu B, Zhou D, et al. Sacubitril/valsartan can reduce atrial fibrillation recurrence after catheter ablation in patients with persistent atrial fibrillation. Cardiovasc Drugs Ther. (2023) 37(3):549–60. doi: 10.1007/s10557-022-07315-1
16. Chan AW, Tetzlaff JM, Gotzsche PC, Altman DG, Mann H, Berlin JA, et al. SPIRIT 2013 explanation and elaboration: guidance for protocols of clinical trials. Br Med J. (2013) 8(346):e7586. doi: 10.1136/bmj.e7586
17. Heidenreich PA, Bozkurt B, Aguilar D, Allen LA, Byun JJ, Colvin MM, et al. 2022 AHA/ACC/HFSA guideline for the management of heart failure: a report of the American College of Cardiology/American Heart Association Joint Committee on clinical practice guidelines. Circulation. (2022) 145(18):e895–e1032. doi: 10.1161/CIR.0000000000001063
18. Xinchao Z, Xuezhong Y, Fengying C, 朱华栋 . Emergency rapid diagnosis and treatment of guidelines acute coronary syndrome. Chin J Emerg Med. (2019) 28(4):10 doi: 10.13201/j.issn.1009-5918.2019.04.001
19. McCarthy JJ, Carr B, Sasson C, Bobrow BJ, Callaway CW, Neumar RW, et al. Out-of-hospital cardiac arrest resuscitation systems of care: a scientific statement from the American Heart Association. Circulation. (2018) 137(21):e645–e60. doi: 10.1161/CIR.0000000000000557
20. Baroutidou A, Kartas A, Samaras A, Papazoglou AS, Vrana E, Moysidis DV, et al. Associations of atrial fibrillation patterns with mortality and cardiovascular events: implications of the MISOAC-AF trial. J Cardiovasc Pharmacol Ther. (2022) 27:10742484211069422. doi: 10.1177/10742484211069422
21. Ren J, Yang Y, Zhu J, Wu S, Wang J, Zhang H, et al. Type of atrial fibrillation and outcomes in patients without oral anticoagulants. Clin Cardiol. (2021) 44(2):168–75. doi: 10.1002/clc.23519
22. Chaofeng H, Junwen X, Fenglin S. Clinical characteristics and risk factors of atrial fibrillation in elderly patients. Chin J Geriatr. (2020) 39(8):4. doi: 10.3760/cma.j.issn.0254-9026.2020.08.004
23. Maisel WH, Stevenson LW. Atrial fibrillation in heart failure: epidemiology, pathophysiology, and rationale for therapy. Am J Cardiol. (2003) 91(6A):2D–8D. doi: 10.1016/s0002-9149(02)03373-8
24. de Diego C, Gonzalez-Torres L, Nunez JM, Centurion Inda R, Martin-Langerwerf DA, Sangio AD, et al. Effects of angiotensin-neprilysin inhibition compared to angiotensin inhibition on ventricular arrhythmias in reduced ejection fraction patients under continuous remote monitoring of implantable defibrillator devices. Heart Rhythm. (2018) 15(3):395–402. doi: 10.1016/j.hrthm.2017.11.012
25. Solomon SD, Claggett B, Desai AS, Packer M, Zile M, Swedberg K, et al. Influence of ejection fraction on outcomes and efficacy of sacubitril/valsartan (LCZ696) in heart failure with reduced ejection fraction: the prospective comparison of ARNI with ACEI to determine impact on global mortality and morbidity in heart failure (PARADIGM-HF) trial. Circ Heart Fail. (2016) 9(3):e002744. doi: 10.1161/CIRCHEARTFAILURE.115.002744
26. Solomon SD, Zile M, Pieske B, Voors A, Shah A, Kraigher-Krainer E, et al. The angiotensin receptor neprilysin inhibitor LCZ696 in heart failure with preserved ejection fraction: a phase 2 double-blind randomised controlled trial. Lancet. (2012) 380(9851):1387–95. doi: 10.1016/S0140-6736(12)61227-6
27. McDonagh TA, Metra M, Adamo M, Gardner RS, Baumbach A, Bohm M, et al. 2021 ESC guidelines for the diagnosis and treatment of acute and chronic heart failure. Eur Heart J. (2021) 42(36):3599–726. doi: 10.1093/eurheartj/ehab368
28. Solomon SD, Rizkala AR, Gong J, Wang W, Anand IS, Ge J, et al. Angiotensin receptor neprilysin inhibition in heart failure with preserved ejection fraction: rationale and design of the PARAGON-HF trial. JACC Heart Fail. (2017) 5(7):471–82. doi: 10.1016/j.jchf.2017.04.013
29. Okutucu S, Fatihoglu SG, Sabanoglu C, Bursa N, Sayin BY, Aksoy H, et al. Effects of angiotensin receptor neprilysin inhibition on P-wave dispersion in heart failure with reduced ejection fraction. Herz. (2021) 46(Suppl 1):69–74. doi: 10.1007/s00059-019-04872-4
30. De Vecchis R, Paccone A, Di Maio M. Favorable effects of sacubitril/valsartan on the peak atrial longitudinal strain in patients with chronic heart failure and a history of one or more episodes of atrial fibrillation: a retrospective cohort study. J Clin Med Res. (2020) 12(2):100–7. doi: 10.14740/jocmr4076
31. Li LY, Lou Q, Liu GZ, Lv JC, Yun FX, Li TK, et al. Sacubitril/valsartan attenuates atrial electrical and structural remodelling in a rabbit model of atrial fibrillation. Eur J Pharmacol. (2020) 881:173120. doi: 10.1016/j.ejphar.2020.173120
32. Li X, Zuo C, Chen C, Tian D, Li J, Fan L, et al. Effectiveness and safety evaluation of sacubitril/valsartan in blood pressure control and clinical outcomes for elderly patients with heart failure and hypertension: a prospective cohort study. Int J Cardiol. (2023) 371:244–51. doi: 10.1016/j.ijcard.2022.09.050
Keywords: sacubitril/valsartan, persistent atrial fibrillation, catheter ablation, sinus rhythm maintenance, major adverse cardiovascular events
Citation: Qiu R, Ni Q, Wu M, Xiao Z, Xiao J, Lin W, Huang W, Chen Y, Chen C and Hong L (2024) Effect of sacubitril/valsartan on sinus rhythm maintenance after catheter ablation in patients with persistent atrial fibrillation without reduced ejection fraction heart failure: a study protocol for a multi-center, open-label, randomized, controlled, superiority clinical trial. Front. Cardiovasc. Med. 11:1303540. doi: 10.3389/fcvm.2024.1303540
Received: 28 September 2023; Accepted: 15 January 2024;
Published: 29 January 2024.
Edited by:
Frank Heinzel, Charité University Medicine Berlin, GermanyReviewed by:
Andreas Metzner, University Heart and Vascular Center, University Medical Center Hamburg-Eppendorf, Germany© 2024 Qiu, Ni, Wu, Xiao, Xiao, Lin, Huang, Chen, Chen and Hong. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Chang Chen c3RfY2hhbmdAcXEuY29t Liekai Hong aG9uZ2xpZWthaUAxNjMuY29t
†These authors have contributed equally to this work
Abbreviations ACEI, angiotensin-converting enzyme inhibitor; ACS, acute coronary syndrome; AE, serious adverse event; AF, atrial fibrillation; ARNI, angiotensin receptor-neprilysin inhibitor; CRF, case report form; DBP, diastolic blood pressure; ECG, electrocardiogram; HF, heart failure; LAAD, left atrial anteroposterior diameter; LVEF, left ventricular ejection fraction; MACE, major adverse cardiovascular events; RAAS, renin-angiotensin-aldosterone system; RCT, randomized controlled trial; SBP, systolic blood pressure.
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.