 Christian Jøns1*‡
Christian Jøns1*‡ Poul Erik Bloch Thomsen2,‡
Poul Erik Bloch Thomsen2,‡ Sam Riahi2,‡Tom Smilde3,‡Ulrich Bach4,‡Peter Karl Jacobsen1,‡
Sam Riahi2,‡Tom Smilde3,‡Ulrich Bach4,‡Peter Karl Jacobsen1,‡ Miloš Táborský5,‡Jozsef Faluközy6Marcus Wiemer7,‡Per Dahl Christensen8,‡Attila Kónyi9,‡Dan Schelfaut10,‡
Miloš Táborský5,‡Jozsef Faluközy6Marcus Wiemer7,‡Per Dahl Christensen8,‡Attila Kónyi9,‡Dan Schelfaut10,‡ Alan Bulava11,‡Marcin Grabowski12,‡Béla Merkely13,‡Dieter Nuyens14,‡Rajiv Mahajan15,‡Patrick Nagel16,‡Roland Tilz17,‡Jerzy Malczynski18Clemens Steinwender19,‡
Alan Bulava11,‡Marcin Grabowski12,‡Béla Merkely13,‡Dieter Nuyens14,‡Rajiv Mahajan15,‡Patrick Nagel16,‡Roland Tilz17,‡Jerzy Malczynski18Clemens Steinwender19,‡ Johannes Brachmann20,‡Harvey Serota21
Johannes Brachmann20,‡Harvey Serota21 Jürgen Schrader22,‡Steffen Behrens23,†,‡Peter Søgaard2,†,‡on behalf of the BIO|GUARD-MI study group
Jürgen Schrader22,‡Steffen Behrens23,†,‡Peter Søgaard2,†,‡on behalf of the BIO|GUARD-MI study group
- 1Department of Cardiology, Rigshospitalet, University of Copenhagen, Copenhagen, Denmark
- 2Department of Cardiology, Aalborg University Hospital, Aalborg, Denmark
- 3Department of Cardiology, Scheperziekenhuis, Treant Zorggroep, Emmen, Netherlands
- 4Department of Cardiology, Vivantes Humboldt-Klinikum, Berlin, Germany
- 5Department of Cardiology, Fakultní Nemocnice Olomouc, Olomouc, Czech Republic
- 6National Hospital of Cardiology, Balatonfüred, Hungary
- 7Department of Cardiology, Johannes Wesling Universitätsklinik, Minden, Germany
- 8Department of Cardiology, Viborg Regional Hospital, Viborg, Denmark
- 9Heart Institute, The University of Pécs, Pécs, Hungary
- 10Cardiovascular Centre, Onze Lieve Vrouw Clinic Aalst, Aalst, Belgium
- 11Department of Cardiology, České Budějovice Hospital and Faculty of Health and Social Sciences, University of South Bohemia, České Budějovice, Czech Republic
- 12First Department of Cardiology, Medical University of Warsaw, Warsaw, Poland
- 13Heart and Vascular Centre, Semmelweis University, Budapest, Hungary
- 14Ziekenhuis Oost-Limburg, Genk, Belgium
- 15Department of Cardiology, Lyell McEwin Hospital, and Adelaide Medical School, The University of Adelaide, Adelaide, SA, Australia
- 16Department of Cardiology, Charité Universitätsmedizin Berlin, Berlin, Germany
- 17Department of Cardiology, Universitätsklinikum Schleswig-Holstein - Campus Lübeck, Lübeck, Germany
- 18Herning Hospital, Herning, Denmark
- 19Department of Cardiology, Kepler University Hospital Linz, Linz, Austria
- 20Department of Cardiology, Klinikum Coburg, Coburg, Germany
- 21Department of Cardiology, St. Louis Heart and Vascular, Bridgeton, MO, United States
- 22Biotronik SE & Co. KG, Berlin, Germany
- 23Department of Cardiology, Vivantes Humboldt-Klinikum and Klinikum Spandau, Berlin, Germany
Objectives: Cardiac arrhythmias predict poor outcome after myocardial infarction (MI). We studied if arrhythmia monitoring with an insertable cardiac monitor (ICM) can improve treatment and outcome.
Design: BIO|GUARD-MI was a randomized, international open-label study with blinded outcome assessment.
Setting: Tertiary care facilities monitored the arrhythmias, while the follow-up remained with primary care physicians.
Participants: Patients after ST-elevation (STEMI) or non-ST-elevation MI with an ejection fraction >35% and a CHA2DS2-VASc score ≥4 (men) or ≥5 (women).
Interventions: Patients were randomly assigned to receive or not receive an ICM in addition to standard post-MI treatment. Device-detected arrhythmias triggered immediate guideline recommended therapy changes via remote monitoring.
Main outcome measures: MACE, defined as a composite of cardiovascular death or acute unscheduled hospitalization for cardiovascular causes.
Results: 790 patients (mean age 71 years, 72% male, 51% non-STEMI) of planned 1,400 pts were enrolled and followed for a median of 31.6 months. At 2 years, 39.4% of the device group and 6.7% of the control group had their therapy adapted for an arrhythmia [hazard ratio (HR) = 5.9, P < 0.0001]. Most frequent arrhythmias were atrial fibrillation, pauses and bradycardia. The use of an ICM did not improve outcome in the entire cohort (HR = 0.84, 95%-CI: 0.65–1.10; P = 0.21). In secondary analysis, a statistically significant interaction of the type of infarction suggests a benefit in the pre-specified non-STEMI subgroup. Risk factor analysis indicates that this may be connected to the higher incidence of MACE in patients with non-STEMI.
Conclusions: The burden of asymptomatic but actionable arrhythmias is large in post-infarction patients. However, arrhythmia monitoring with an ICM did not improve outcome in the entire cohort. Post-hoc analysis suggests that it may be beneficial in non-STEMI patients or other high-risk subgroups.
Clinical Trial Registration: [https://www.clinicaltrials.gov/ct2/show/NCT02341534], NCT02341534.
Strengths of this study
• Our study investigates the effect of continuous monitoring of arrhythmias in post-MI patients
• Because the target population is large and their risk of acute deteriorations is high, a clinical benefit might be very meaningful
• The methods are clinically applicable
Limitations of this study
• Blinding was impossible and unbiased collection of clinical events was challenging
Introduction
Ischemic heart disease (IHD) is a leading cause of death and disability worldwide (1). Patients with chronic IHD are under a considerable risk to experience major adverse cardiac events (MACE) such as myocardial (re-) infarction, stroke, or acute worsening of heart failure. After cardiac rehabilitation, bi-annual evaluations by a general practitioner or cardiologist are recommended in the first year (2), but follow-up may be too infrequent to detect an acute deterioration of the patient's status and thereby prevent future events. In patients with an implantable cardioverter-defibrillator (ICD), continuous remote monitoring of cardiac arrhythmias shortens the time to clinical decision and subsequently improves prognosis in some studies (3–7), though results are conflicting (8).
The CARISMA and SMART-MI trials have shown that post-infarction patients without an indication for an ICD suffer from a significant burden of arrhythmias as documented using an implantable cardiac monitor (ICM) (9, 10). In CARISMA, asymptomatic arrhythmias preceeded MACE in the majority of patients (9, 11, 12). However, no randomized trial has tested whether monitoring and responding to arrhythmias detected on an ICD improves prognosis in high-risk post-infarction patients.
In the present randomized controlled trial, we compared the clinical outcome of standard treatment without ICM against an ICM-based treatment with remote monitoring in high-risk patients after myocardial infarction (MI). The hypothesis was that a fast response to ICM-detected arrhythmias using a predefined investigational algorithm to guide diagnosis and treatment would result in a reduction a combined endpoint of cardiovascular death and hospitalization (13).
Material and methods
Study design
BIO|GUARD-MI (Biomonitoring in Patients with Preserved Left Ventricular Function after Diagnosed Myocardial Infarction) was an international, randomized, parallel group, open-label study with a blinded outcome assessment and an event-driven design. The investigational sites were 60 tertiary clinical centers in Europe, the USA, and Australia (see Supplemental Material). Details of the trial design have been published previously (13). A Steering Committee developed the study concept, designed and oversaw the study, had full access to all data, supervised the analysis, and had final responsibility for the decision to submit for publication. An independent Data and Safety Monitoring Board (DSMB) guided the study (Supplemental Material).
Patients
Patients were enrolled if they had a history of MI and a CHA2DS2-VASc score ≥4 (men) or ≥5 (women). Although originally constructed to estimate the risk of stroke, we used the CHA2DS2-VASc score as a simple tool to identify patients with a higher risk for primary endpoints and thereby reduce the number of required patients (13). Further, a left ventricular ejection fraction >35% was required excluding patients eligible for an implantable cardioverter/defibrillator (ICD). Patients with oral anticoagulation therapy, Parkinson's disease, hemorrhagic diathesis, chronic renal dialysis, or a cardiac implantable electronic device were excluded (13).
Randomization and masking
The patients were randomly assigned in a 1:1 ratio to receive an ICM with remote monitoring (ICM group) or no ICM (control group), in addition to standard post-MI treatment. The randomization was generated through a centralized, concealed process implemented by the sponsor and stratified by site and by the presence (STEMI) or absence (NSTEMI) of ST-segment elevation at the index infarction. Neither patients nor investigators were blinded to the group assignment, because a sham implantation of an inactive device was considered too risky and inconvenient for control group patients.
Procedures
Patients randomized to the ICM group received a BioMonitor 2-AF or BIOMONITOR III device (Biotronik SE & Co. KG, Germany) (14, 15). After subcutaneous insertion, the ICM records 1-minute ECGs for atrial fibrillation, bradycardia, high ventricular rate, or asystole episodes and automatically transmits up to six ECGs per day to the secure Biotronik Home Monitoring website (16). The suggested device programming is available in the design paper (13).
ICM-detected ECGs were screened every working day by the Central ECG Monitoring Board (see Supplemental Material). ECGs that were not caused by over- or undersensing were entered into the study database. Investigators were required, within 7 days, to adjudicate the rhythm, decide on the clinical relevance, and report whether they would contact the patient. Decisions about subsequent changes of therapy were in the responsibility of the investigator who followed prespecified recommendations based on current guidelines (13). The investigator implemented them or delegated them to the patient's general practitioner or cardiologist.
Because follow-up in tertiary care centers is not standard of care in post-MI patients, study subjects were advised to undergo regular follow-up by their general practitioner or cardiologist, according to local standard post-MI practice. Because ICMs do not need regular follow-up by the device clinic (in contrast to therapeutic devices such as pacemakers or ICDs), no study visits were scheduled in either arm. Patients were explicitly instructed not to visit or contact the investigational site on their own initiative, but to refer to their personal physician in case of symptoms. Investigators contacted patients only after arrhythmia detection by the ICM. No contacts were required to manage remote monitoring transmissions.
The lack of regular follow-up visits in the investigational site made adverse event reporting challenging. All patients were called by telephone every 6 months by an interviewer of a contract research organization who asked them about adverse events from the preceding period. These interviewers did not interfere in the medical treatment or give advice in any way. If the patient reported any hospitalization or other medical occurrence, the study investigators were informed. The interviewer also supported the provision of discharge letters, death certificates or other documentation of the event. For every adverse event, it was reported whether an arrhythmia was involved that required a change in therapy according to current guidelines (13).
Outcomes
The primary endpoint was MACE, defined as a composite of cardiovascular death, urgent visit for acute worsening of heart failure, or acute unscheduled hospitalization due to arrhythmia, acute coronary syndrome, heart failure, stroke, systemic embolism, or major bleeding (included to capture side effects of anticoagulation treatment). Events resulting from ICM detection were considered scheduled and were not counted as endpoints. An independent blinded Endpoint and Adverse Event Committee adjudicated all adverse events that fulfilled predefined criteria. The major secondary endpoint was the time to the first arrhythmia that resulted in a therapeutic change. Further secondary endpoints were all-cause mortality, components of the composite primary endpoint, the time to the first arrhythmia, and quality of life.
Adverse event reporting bias and premature termination
Based on the unblinded results of the first interim analysis, the DSMB detected an increased incidence of adverse events in the ICM group. They assumed that this was probably attributable to a reporting bias resulting from the unblinded trial design and informed the steering committee, although the formal futility criterion was not fulfilled. A small unblinded team of sponsor personnel involved external independent experts to judge whether a bias in the clinical event reporting existed and to suggest corrective measures. The quality of adverse events reporting was compared between the study groups using the time to the first non-cardiovascular adverse event because ICMs should not modify this event type. A significantly lower non-cardiovascular adverse event rate in the control group was found. Based on the fact that the group allocation was randomized and the assumption that the ICM cannot cause non-cardiovascular events, this result was interpreted as evidence of a more complete adverse event reporting in ICM patients. This bias appeared possible because ICM group patients knew of their device and may have seen reasons to contact the study site, even if they were explicitly asked not to do this; this could result in a higher chance of medical events getting attention of the investigational site staff. If a bias of the same amplitude was present also in primary endpoints, it was judged large enough to inevitably cause a negative study result.
Patient enrollment was stopped while follow-up continued. Efforts to get reports of all adverse events in both study groups were stepped up by re-training of the telephone interviewers, by additional telephone contacts to patients and by intensified source data verification. While these corrective measures reduced the bias, they did not resolve it completely after a considerable investment of time and effort. Thus, a protocol amendment was introduced which defined that all patients were to be invited to the investigational site and asked about all hospitalizations during the study, and then to exit the study. The trial was prematurely terminated after the last patient visit.
In the final data, the difference in the time to the first non-cardiovascular adverse events was not statistically significant between the study groups (HR = 1.08; P = 0.38). Thus, the analysis presented here assumes unbiased reporting. This assumption is conservative, since a hypothetical remaining bias would reduce the study effect.
Statistical analysis
It was initially planned to enroll and follow patients until 372 primary endpoints had occurred, with interim analyses after 124 and 248 primary events (a 3-stage adaptive group sequential test procedure according to O'Brian Fleming) (13). This gave an 80% power given an assumed hazard ratio (HR) of 0.7452. However, the group sequential design was abandoned because of the unblinding of limited sponsor personnel after the first interim analysis. The modified plan in the amended protocol was a final analysis based on all available data after premature study termination.
The primary hypothesis was tested with the log rank test stratified for NSTEMI/STEMI in all patients with follow-up, based on the intention-to-treat principle.
If non-fatal outcomes are frequent, the exclusion of recurrent events by the Kaplan-Meier method reduces the power to detect outcome differences (17). To compensate for the power lost due to the premature study termination, a post-hoc analysis including recurrent events was conducted using the Andersen-Gill method with robust estimates for the standard errors. The influence of predefined subgroups on the study effect was also tested including recurrent events.
Missing data were not imputed. Other time-to-event data than the primary endpoint were analyzed with the Cox-regression model and visualized with the Kaplan-Meier method.
To test post-hoc whether the apparent study benefit in the NSTEMI subgroup depends on the higher risk of NSTEMI patients, we used the multivariate Cox method and identified baseline variables linked with a higher incidence of the primary endpoint, including recurrent events. This was done in the control group because study treatment can modify the risk. As input variables, we selected all available baseline characteristics and comorbidities that affected between 10% and 90% of patients, except the STEMI/NSTEMI variable. Few missing values were imputed with the more frequent value. We tested whether the number of risk factors per patient showed statistical interaction with the study effect.
Quantitative variables are described as mean ± SD or as median and interquartile range (IQR). Continuous and ordinal data were compared with the non-parametric Mann–Whitney-Wilcoxon test, and nominal data with the exact Fisher test. A two-sided P-value <0.05 was considered statistically significant. All analyses were performed with SAS 9.4.
Results
Study population
Between August 2015 and April 2020, 802 patients were enrolled, of whom 790 were randomly assigned (Figure 1): 398 to the ICM group, 392 to the control group. Patient characteristics were well balanced between the two groups (Table 1). Mean age was 71.2 years (SD 8.1), and 568 (72%) patients were men. In the ICM group, 366 (92%) patients received an ICM, and in the control group, one patient mistakenly received an ICM; all patients were analysed in the group to which they were randomized. Of 790 randomized patients, 647 (82%) completed follow-up, 85 died (11%), and 58 (7%) terminated the study prematurely (Figure 1).
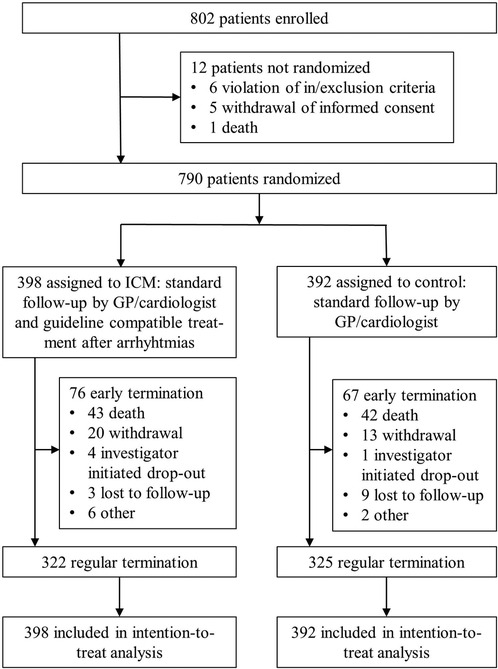
Figure 1. Trial profile. GP, general practitioner; ICM, implantable cardiac monitor.
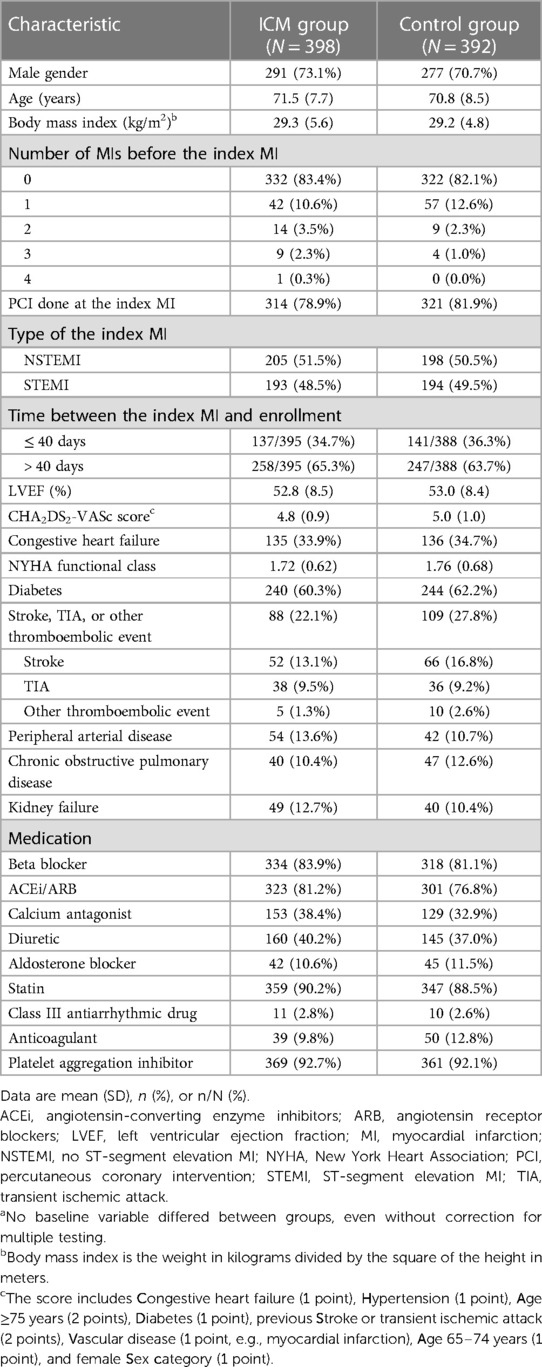
Table 1. Characteristics of the intention-to-treat population at baselinea.
The median length of follow-up was 31.6 months (IQR 21.8–45.4). Cumulative follow-up was 1,071 vs. 1,120 patient-years (ICM vs. control group).
Detection of arrhythmias and treatment
Of 2,548 arrhythmia notifications that were sent by the Central ECG Monitoring Board, 1,909 were classified as true arrhythmias. Divided by the study duration in the ICM group, this results in 1.8 true arrhythmias per patient-year. Most frequent were bradycardic events (48.4%, including sinus bradycardia, pause, and atrioventricular block) and atrial fibrillation (33.0%) (Table 2). For 482 arrhythmia notifications, a contact to the patient was planned. The median delay between arrhythmia and patient contact was 4 days (IQR 2–6 days). At 2 years, 67.3% of the ICM group had a first arrhythmia and 39.4% received a guideline required change in therapy, as compared to 6.7% of control patients (HR = 5.9, P < 0.0001; Figure 2). The number of adverse events with arrhythmias leading to therapy modification was 213 in the ICM group (affecting 161 patients) and 50 in the control group (36 patients). Within these adverse events, the most frequent arrhythmias were atrial fibrillation (N = 120), leading to oral anticoagulation initiation in 79.2% of cases, and bradycardic events (N = 103), leading to a pacemaker implantation (49.5%) or reduction of heart rate lowering drugs (45.6%). Less frequent were other supraventricular arrhythmias (N = 19) or ventricular tachycardias (N = 17). Overall, 11 implantable cardioverter-defibrillators and six catheter ablations were indicated.
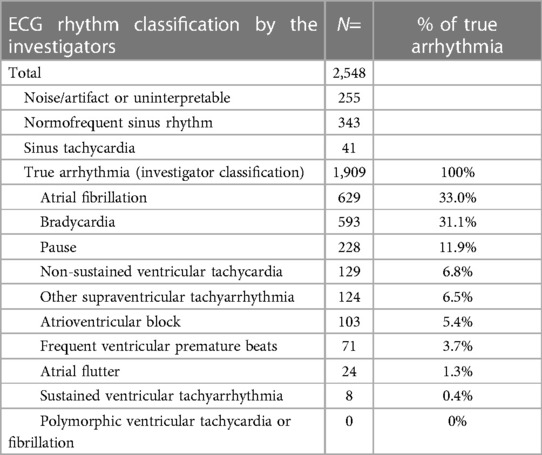
Table 2. ECG recordings sent to the investigational site.
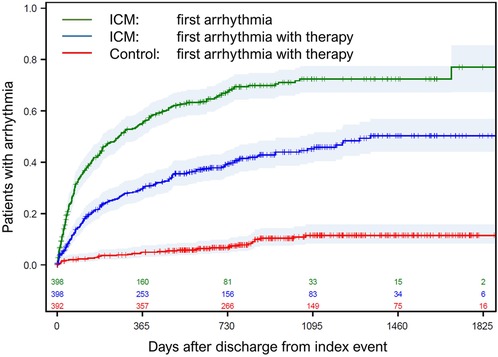
Figure 2. Time to first arrhythmia. Time to first ICM-detected arrhythmia (green line), time to first arrhythmia resulting in a therapy change in the ICM group (blue line), and time to first arrhythmia resulting in a therapy change in the control group (red line). Day 0 is the discharge from index hospitalization. ICM, implantable cardiac monitor.
The percentage of patients with oral anticoagulation treatment was increased at study termination compared to baseline in both study groups, but more in the ICM group (37.5%) than in the control group (25.1%; P = 0.0007). In NSTEMI patients, the use of ACEi/ARB at study termination was higher in the ICM group than in the control group (75.4% vs. 62.5%; P = 0.013), but in STEMI patients it was similar in both groups (74.4% vs. 70.8%; P = 0.47).
Clinical outcome
Primary result
A total of 336 primary endpoint events occurred in 218 patients. There was no statistically significant difference in primary endpoints between the study groups (HR = 0.84, 95%-CI 0.65–1.10; P = 0.21; Figure 3). Most frequent endpoints were hospitalizations for acute coronary syndrome and for worsening of heart failure (Table 3).
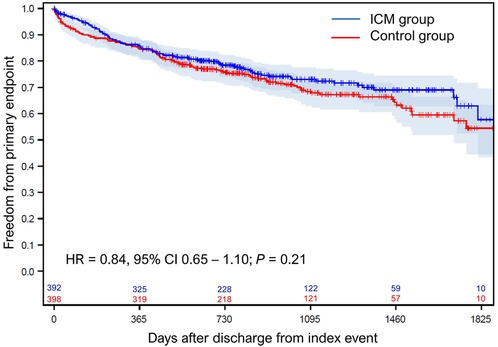
Figure 3. Freedom from primary endpoint. The probability of freedom from primary endpoint. Day 0 is the discharge from index hospitalization. CI, confidence interval; HR, hazard ratio; ICM, implantable cardiac monitor.
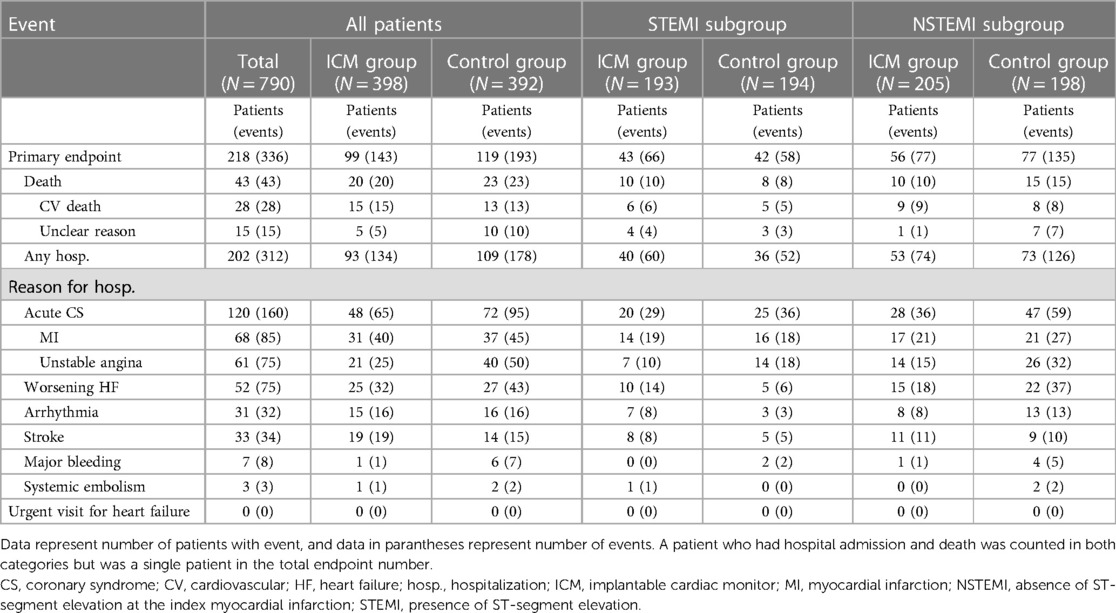
Table 3. Patients with primary endpoints.
Post-hoc analyses and subgroups
The post-hoc analysis including recurrent events according to Andersen-Gill utilized all 336 primary endpoint events from 218 patients. It confirmed the Kaplan-Meier result of no significant benefit (HR = 0.77, 95%-CI 0.57–1.03).
Of the prespecified subgroups, only the STEMI/NSTEMI variable showed significant interaction with the study effect (Figure 4). Patients with NSTEMI (N = 403; HR = 0.58, 95%-CI 0.40–0.83) appeared to have a benefit but patients with STEMI (N = 387; HR = 1.23; 95%-CI 0.76–1.97) did not (Pinteraction = 0.013).
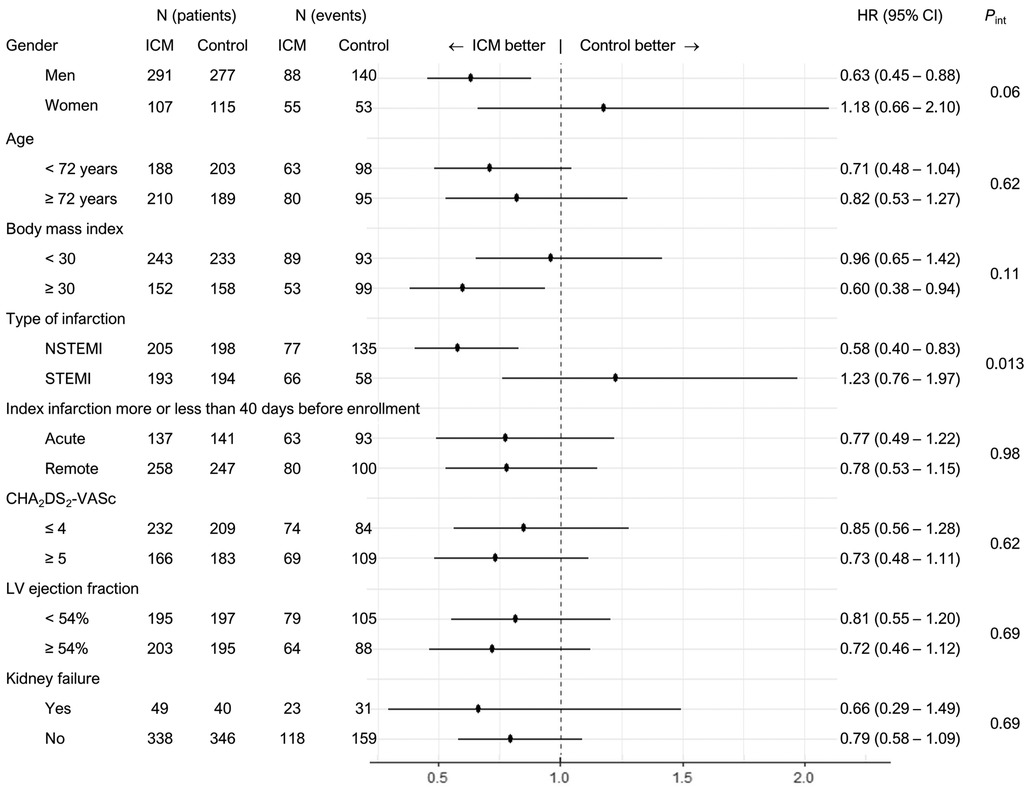
Figure 4. Predefined subgroup analyses of the primary endpoint. Only STEMI/NSTEMI showed significant interaction with the study effect. Subgroups with a study benefit were NSTEMI, male gender and BMI >30. For the definition of CHA2DS2-VASc, see Table 1. CI, confidence interval; HR, hazard ratio; ICM, implantable cardiac monitor group; Int, interaction; LV, left ventricular; NSTEMI, absence of ST-segment elevation; STEMI, presence of ST-segment elevation at the index myocardial infarction.
The incidence of primary endpoints was higher in the NSTEMI than STEMI subgroup of patients (HR = 1.78, P = 0.0002). To investigate whether the apparent benefit in the NSTEMI subgroup depends on the higher risk in these patients, we constructed a risk model. The included variables and their influence on the incidence of the primary endpoint in the control group are shown in Table 4. In multivariate analysis, we excluded the NSTEMI / STEMI variable because we were interested in the effect of other risk factors than this variable. Four variables remained as predictors: peripheral artery disease, kidney failure, body mass index >30 and MI within 40 days of enrollment. The number of risk factors per patient exerted a borderline significant effect on the study benefit (Pinteraction = 0.051), with a higher number of risk factors connected to a higher study benefit.
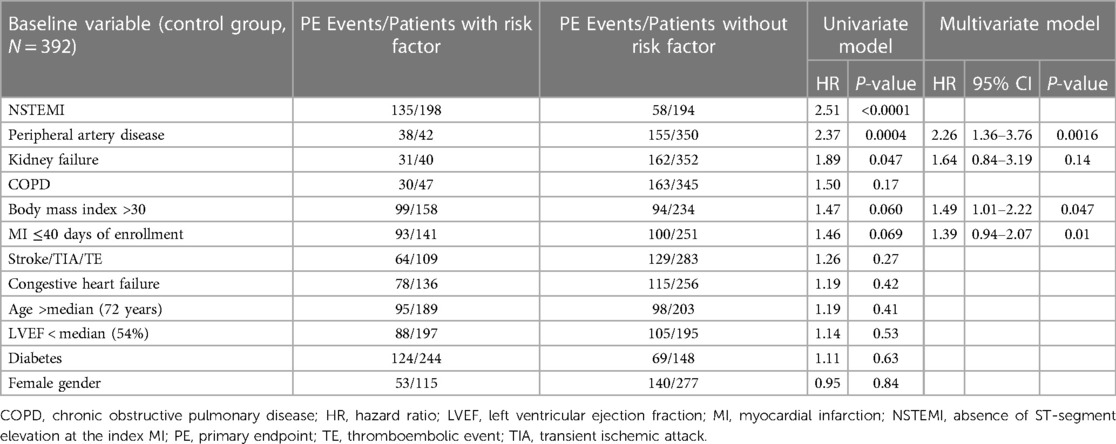
Table 4. Baseline variables linked with a higher incidence of primary endpoint, including recurrent events.
Discussion
In post-MI patients with a CHA2DS2-VASc score ≥4 (≥5 in women), continuous arrhythmia monitoring with an ICM leads to a considerable amount of guideline-directed therapy changes. The BIO|GUARD–MI trial confirms similar findings of CARISMA (9) and SMART-MI (10), but in contrast to these trials, it is the only trial so far designed to test if responding clinically to these arrhythmias has a clinical effect. Our study was terminated early due to difficulties with the unbiased collection of adverse events; the final analysis failed to prove that guideline-directed study treatments provide a clinical benefit in the total study population.
The inclusion of repeated events in patients who survived the first MACE provides a more accurate estimate of the effect size (17). This analyses included 336 events, close to the prespecified 372 events, and confirmed the findings of the protocol defined analysis.
The analysis of predefined subgroups found that the type of index infarction (NSTEMI or STEMI) had a significant interaction with the study effect (Pinteraction = 0.013), with a large risk reduction in NSTEMI patients, but no effect in STEMI patients. A comparison of STEMI and NSTEMI patients showed that the incidence of MACE was by far higher in NSTEMI than in STEMI patients, an observation that has been described before (18, 19). Patients with NSTEMI did not display a systematic difference in baseline characteristics compared to STEMI patients. The added post-hoc multivariate risk model using all available baseline variables except whether the index MI was STEMI or NSTEMI showed that the number of risk factors interacted with the study effect with borderline statistical significance. A higher risk of meeting an endpoint was connected to a higher benefit of monitoring by the ICM. Hence, the negative findings of the BIO|GUARD-MI trial are possibly related to a too low clinical risk of the included population. Whether there may be a benefit in patients with higher risk, e.g., the NSTEMI population or other subgroups will need further analysis.
The most frequent treatments were oral anticoagulation after atrial fibrillation and reduction of beta blockade or pacemaker implantation after bradycardia or pauses. Despite this we observed the strongest trends (no differences were statistically significant) in reductions of acute coronary syndrome and worsening of heart failure whereas strokes were not reduced. However, since 37% of ICM patients vs. 25% of non-ICM patients were on anticoagulations at the end of the study, these event numbers may be due to chance. CARISMA found a very strong correlation between ICM detected pauses and cardiovascular death (HR 6.6, P < 0.001), many of which were due to terminal heart failure (9). This influence is also not obvious. It may be possible that arrhythmias detected by an ICM serve as risk indicators of a worsening status, after which immediate action is required, rather than a trigger of a major cardiac event. Higher-risk patients may simply require more attention, which is triggered by arrhythmia detection in the ICM group, and they may have more therapeutic options after arrhythmia diagnosis. We found a higher share of NSTEMI patients with ACEi/ARB at termination in the ICM group than in the control group, suggesting that the treatment of patients after arrhythmias may improve prognostically effective therapies which are not related to the arrhythmia. The recently concluded SMART-MI study had a design comparable to our trial but failed to show even a trend towards improvement in the secondary clinical outcome endpoint (10). This may be due to an insufficient sample size, but also due to a better-than-normal post-MI patient care with 6-monthly follow-ups in tertiary centers, possibly leaving less room for improvements after arrhythmias were detected.
Limitations
Our study must be interpreted considering several limitations. First, we have discontinued the study prematurely after a planned interim analysis raised doubt about the integrity of the adverse event and endpoint reporting. The concern about the validity of results from studies with premature termination is that termination may be intentional at a time when interim results are favorable. We can rule this out because the termination (after the last patient's final visit) was defined in an amended study protocol more than half a year before study closure. Second, while procedural changes allowed us to establish reporting of adverse events without evident bias, we did not meet the targeted number of primary endpoints. This increases the likelihood of a false-negative study result but does not put the results in doubt. Third, although the NSTEMI/STEMI subgroups were prespecified, the absence of a statistically significant study effect in the total population precludes a precise estimation of the alpha error in subsequent subgroup analyses. However, the interaction of risk factors derived from a multivariate analysis with the study benefit suggests that the increased risk in the NSTEMI subgroup may be the basis of the observed difference between NSTEMI and STEMI subgroups.
Conclusion
In conclusion, post-MI patients with mildly reduced or preserved ejection fraction have a large burden of asymptomatic arrhythmias. Arrhythmia monitoring with an ICM allows the implementation of guideline recommended therapies in consequence of these arrhythmias. Our study failed to show that this strategy improves the outcome in the total study population. Sub-analyses indicate that the strategy could be beneficial in patient populations at higher risk for cardiovascular events and should encourage further research in the field of arrhythmia monitoring, and more generally the monitoring of physiological parameters, in chronically diseased patients.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statement
The study involving humans was approved by ethics committees relevant to all involved hospitals. A list is available upon request from the first author. The study was conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
Author contributions
CJ: Conceptualization, Methodology, Writing – original draft. PEBT: Conceptualization, Investigation, Methodology, Writing – review & editing. SR: Investigation, Writing – review & editing. TS: Investigation, Writing – review & editing. UB: Investigation, Writing – review & editing. PJ: Investigation, Writing – review & editing. MT: Investigation, Writing – review & editing. JF: Investigation, Writing – review & editing. MW: Investigation, Writing – review & editing. PDC: Investigation, Writing – review & editing. AK: Investigation, Writing – review & editing. DS: Investigation, Writing – review & editing. AB: Investigation, Writing – review & editing. MG: Investigation, Writing – review & editing. BM: Investigation, Writing – review & editing. DN: Investigation, Writing – review & editing. RM: Investigation, Writing – review & editing. PN: Investigation, Writing – review & editing. RT: Investigation, Writing – review & editing. JM: Investigation, Writing – review & editing. CS: Investigation, Writing – review & editing. JB: Investigation, Writing – review & editing. HS: Investigation, Writing – review & editing. JS: Methodology, Writing – review & editing. SB: Conceptualization, Investigation, Methodology, Writing – review & editing. PS: Conceptualization, Investigation, Methodology, Writing – review & editing.
Funding
The author(s) declare financial support was received for the research, authorship, and/or publication of this article.
This work was supported by Biotronik SE & Co. KG (Berlin, Germany). The funder supported protocol development, created electronic case-report forms using the MedNet Solutions platform (Minnetonka, MN, USA), assured source data verification and served as the core statistical unit. The funder had no influence on the decision to submit the publication.
Acknowledgments
We are most grateful to the DSMB that informed us concerning an increase in adverse events in the ICM group that only they could recognize at that time. Their charter only obliged them to inform the sponsor if prespecified futility or superiority borders were crossed, which was not the case. However, that they acted otherwise is proof of their sense of responsibility and their concern for the integrity of the study results. The authors are thankful for project management to Sascha Mrosk (lead), Maria Jung, Dörte Vossmann, Maike Kohle, and Gamze Atas, for statistical analyses to Bernd Brüsehaber (lead), Katharina Ingel, and Irina Köhler, and to Dejan Danilovic for critical reading and editing of the manuscript.
Conflict of interest
UB has received lecture fees from Boehringer, Astra Zeneca and Bayer, and travel costs from Boehringer, Astra Zeneca, Bayer, and Bristol Myers Squibb. MG reports consulting and lecture fees from Abbott Medical, Biotronik, Boston Sc. and Medtronic. BM reports grant or contract payments from Medtronic and Boston Scientific and lecture fees from Biotronik and Abbott Medical. RM reports grant or contract payments from Abbott Medical, Medtronic, Bayer and lecture fees from Bayer. RT reports consulting fees from Abbott and Boston Sc. and honoraria for lectures from Abbott Medical, Biotronik and Boston Sc. JS is an employee of Biotronik. SB reports lecture fees and travel costs from Biotronik in the context of this study, and lecture fees from Astra Zeneca, Bayer, Berlin Chemie, Boehringer, Bristol Myers Squibb, and Novartis, and DSMB or advisory board membership fees from Astra Zeneca, Bayer, Berlin Chemie, Boehringer, Bristol Myers Squibb, and Novartis.
The authors declare that this study received funding from Biotronik SE & Co. KG. The funder supported study design, data collection, analysis, interpretation of data and the writing of this article.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fcvm.2024.1300074/full#supplementary-material
References
1. Khan MA, Hashim MJ, Mustafa H, Baniyas MY, Al Suwaidi SKBM, AlKatheeri R, et al. Global epidemiology of ischemic heart disease: results from the global burden of disease study. Cureus. (2020) 12(7):e9349. doi: 10.7759/cureus.9349
2. Knuuti J, Wijns W, Saraste A, Capodanno D, Barbato E, Funck-Brentano C, et al. 2019 ESC guidelines for the diagnosis and management of chronic coronary syndromes. Eur Heart J. (2020) 41:407–77. doi: 10.1093/eurheartj/ehz425
3. Hindricks G, Taborsky M, Glikson M, Heinrich U, Schumacher B, Katz A, et al. Implant-based multiparameter telemonitoring of patients with heart failure (IN-TIME): a randomised controlled trial. Lancet. (2014) 384:583–90. doi: 10.1016/S0140-6736(14)61176-4
4. Crossley GH, Boyle A, Vitense H, Chang Y, Mead RH. The CONNECT (clinical evaluation of remote notification to reduce time to clinical decision) trial: the value of wireless remote monitoring with automatic clinician alerts. J Am Coll Cardiol. (2011) 57:1181–9. doi: 10.1016/j.jacc.2010.12.012
5. Guédon-Moreau L, Lacroix D, Sadoul N, Clémenty J, Kouakam C, Hermida JS, et al. A randomized study of remote follow-up of implantable cardioverter defibrillators: safety and efficacy report of the ECOST trial. Eur Heart J. (2013) 34:605–14. doi: 10.1093/eurheartj/ehs425
6. Hindricks G, Varma N, Kacet S, Lewalter T, Søgaard P, Guédon-Moreau L, et al. Daily remote monitoring of implantable cardioverter-defibrillators: insights from the pooled patient-level data from three randomized controlled trials (IN-TIME, ECOST, TRUST). Eur Heart J. (2017) 38:1749–55. doi: 10.1093/eurheartj/ehx015
7. Geller JC, Lewalter T, Bruun NE, Taborsky M, Bode F, Nielsen JC, et al. Implant-based multi-parameter telemonitoring of patients with heart failure and a defibrillator with vs. Without cardiac resynchronization therapy option: a subanalysis of the IN-TIME trial. Clin Res Cardiol. (2019) 108:1117–27. doi: 10.1007/s00392-019-01447-5
8. Morgan JM, Kitt S, Gill J, McComb JM, Ng GA, Raftery J, et al. Remote management of heart failure using implantable electronic devices. Eur Heart J. (2017) 38:2352–60. doi: 10.1093/eurheartj/ehx227
9. Bloch Thomsen PE, Jons C, Raatikainen MJ, Moerch Joergensen R, Hartikainen J, Virtanen V, et al. Long-term recording of cardiac arrhythmias with an implantable cardiac monitor in patients with reduced ejection fraction after acute myocardial infarction: the cardiac arrhythmias and risk stratification after acute myocardial infarction (CARISMA) study. Circulation. (2010) 122:1258–64. doi: 10.1161/CIRCULATIONAHA.109.902148
10. Bauer A, Sappler N, von Stülpnagel L, Klemm M, Schreinlechner M, Wenner F, et al. Telemedical cardiac risk assessment by implantable cardiac monitors in patients after myocardial infarction with autonomic dysfunction (SMART-MI-DZHK9): a prospective investigator-initiated, randomised, multicentre, open-label, diagnostic trial. Lancet Digit Health. (2022) 4:e105–16. doi: 10.1016/S2589-7500(21)00253-3
11. Jons C, Jacobsen UG, Joergensen RM, Olsen NT, Dixen U, Johannessen A, et al. The incidence and prognostic significance of new-onset atrial fibrillation in patients with acute myocardial infarction and left ventricular systolic dysfunction: a CARISMA substudy. Heart Rhythm. (2011) 8:342–8. doi: 10.1016/j.hrthm.2010.09.090
12. Gang UJ, Jøns C, Jørgensen RM, Abildstrøm SZ, Messier MD, Haarbo J, et al. Risk markers of late high-degree atrioventricular block in patients with left ventricular dysfunction after an acute myocardial infarction: a CARISMA substudy. Europace. (2011) 13:1471–7. doi: 10.1093/europace/eur165
13. Jons C, Sogaard P, Behrens S, Schrader J, Mrosk S, Bloch Thomsen PE. The clinical effect of arrhythmia monitoring after myocardial infarction (BIO-GUARD|MI): study protocol for a randomized controlled trial. Trials. (2019) 20:563. doi: 10.1186/s13063-019-3644-5
14. Piorkowski C, Busch M, Nölker G, Schmitt J, Roithinger FX, Young G, et al. Clinical evaluation of a small implantable cardiac monitor with a long sensing vector. Pacing Clin Electrophysiol. (2019) 42:1038–46. doi: 10.1111/pace.13728
15. Deneke T, Cabanas P, Hofer D, Gaspar T, Pierre B, Bisignani G, et al. New-generation miniaturized insertable cardiac monitor with a long sensing vector: insertion procedure, sensing performance, and home monitoring transmission success in a real-world population. Heart Rhythm O2. (2022) 3:152–9. doi: 10.1016/j.hroo.2022.01.010
16. Søgaard P, Behrens S, Konyi A, Taborsky M, Christiansen PD, Jacobsen PK, et al. Transmission and loss of ECG snapshots: remote monitoring in implantable cardiac monitors. J Electrocardiol. (2019) 56:24–8. doi: 10.1016/j.jelectrocard.2019.06.005
17. Rogers JK, Pocock SJ, McMurray JJ, Granger CB, Michelson EL, Östergren J, et al. Analysing recurrent hospitalizations in heart failure: a review of statistical methodology, with application to CHARM-preserved. Eur J Heart Fail. (2014) 16:33–40. doi: 10.1002/ejhf.29
18. Polonski L, Gasior M, Gierlotka M, Osadnik T, Kalarus Z, Trusz-Gluza M, et al. A comparison of ST elevation versus non-ST elevation myocardial infarction outcomes in a large registry database: are non-ST myocardial infarctions associated with worse long-term prognoses? Int J Cardiol. (2011) 152:70–7. doi: 10.1016/j.ijcard.2010.07.008
19. Vora AN, Wang TY, Hellkamp AS, Thomas L, Henry TD, Goyal A, et al. Differences in short- and long-term outcomes among older patients with ST-elevation versus non-ST-elevation myocardial infarction with angiographically proven coronary artery disease. Circ Cardiovasc Qual Outcomes. (2016) 9:513–22. doi: 10.1161/CIRCOUTCOMES.115.002312
Keywords: cardiac arrhythmia, myocardial infarction, implantable cardiac monitor, telemedicine, randomized controlled trial
Citation: Jøns C, Bloch Thomsen PE, Riahi S, Smilde T, Bach U, Jacobsen PK, Táborský M, Faluközy J, Wiemer M, Christensen PD, Kónyi A, Schelfaut D, Bulava A, Grabowski M, Merkely B, Nuyens D, Mahajan R, Nagel P, Tilz R, Malczynski J, Steinwender C, Brachmann J, Serota H, Schrader J, Behrens S and Søgaard P (2024) Arrhythmia monitoring and outcome after myocardial infarction (BIO|GUARD-MI): a randomized trial. Front. Cardiovasc. Med. 11:1300074. doi: 10.3389/fcvm.2024.1300074
Received: 23 September 2023; Accepted: 16 April 2024;
Published: 13 May 2024.
Edited by:
Pietro Francia, University Sapienza, ItalyReviewed by:
Svetlana Apostolović, University Clinical center, SerbiaAttila Frigy, George Emil Palade University of Medicine, Pharmacy, Sciences and Technology of Târgu Mureş, Romania
Heikki Veli Huikuri, University of Oulu, Finland
© 2024 Jøns, Bloch Thomsen, Riahi, Smilde, Bach, Jacobsen, Táborský, Faluközy, Wiemer, Christensen, Kónyi, Schelfaut, Bulava, Grabowski, Merkely, Nuyens, Mahajan, Nagel, Tilz, Malczynski, Steinwender, Brachmann, Serota, Schrader, Behrens and Søgaard. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Christian Jøns Y2hyam9lbnNAZ21haWwuY29t
†These authors share senior authorship
‡ORCID Christian Jøns orcid.org/0000-0002-1876-2623
Poul Erik Bloch Thomsen orcid.org/0000-0002-0556-0379
Sam Riahi orcid.org/0000-0003-1849-9463
Tom Smilde orcid.org/0000-0002-9638-7654
Ulrich Bach orcid.org/0009-0009-7692-1301
Peter Karl Jacobsen orcid.org/0000-0002-1520-8774
Miloš Táborský orcid.org/0000-0002-5036-2347
Marcus Wiemer orcid.org/0000-0003-4781-8064
Per Dahl Christensen orcid.org/0000-0003-3396-9240
Attila Kónyi orcid.org/0000-0002-5911-2774
Dan Schelfaut orcid.org/0000-0001-8262-333X
Alan Bulava orcid.org/0000-0002-1742-207X
Marcin Grabowski orcid.org/0000-0003-3306-0301
Béla Merkely orcid.org/0000-0001-6514-0723
Dieter Nuyens orcid.org/0000-0001-9390-3273
Rajiv Mahajan orcid.org/0000-0003-3375-5568
Patrick Nagel orcid.org/0009-0009-0921-1190
Roland Tilz orcid.org/0000-0002-0122-7130
Clemens Steinwender orcid.org/0000-0002-4963-5563
Johannes Brachmann orcid.org/0000-0002-9221-9856
Jürgen Schrader orcid.org/0000-0002-3656-6327
Steffen Behrens orcid.org/0000-0002-7233-2296
Peter Søgaard orcid.org/0000-0002-7441-0630