
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
STUDY PROTOCOL article
Front. Cardiovasc. Med. , 04 June 2024
Sec. Coronary Artery Disease
Volume 11 - 2024 | https://doi.org/10.3389/fcvm.2024.1293818
 Lanchun Liu1
Lanchun Liu1 Jie Wang1*
Jie Wang1* Jun Li1
Jun Li1 Xiao Li2
Xiao Li2 Rong Li3
Rong Li3 Yongmei Liu1
Yongmei Liu1 Guang Yang1
Guang Yang1 Qiyuan Mao1
Qiyuan Mao1 Lin Wang2
Lin Wang2 Zhengyang Yao3
Zhengyang Yao3 Yongcheng Wang2Shuli Zong2Chao Liu1
Yongcheng Wang2Shuli Zong2Chao Liu1
Background: Coronary heart disease (CHD) is representative of cardiovascular disease and the leading cause of death in humans. Previous studies have shown that kidney disease is associated with CHD, and current treatment options that can improve both cardiac and renal functions still have some limitations. The traditional Chinese medicine Bu-Shen-Huo-Xue granule (BSHXG) can promote blood rheology, inhibit platelet agglutination, and improve heart and kidney functions.
Methods: This is a multicenter, randomized, double-blind, placebo-controlled clinical trial. A total of 210 participants will be randomized to the intervention group and the placebo group. The Guang’anmen Hospital of China Academy of Chinese Medical Sciences is the leading center, and the Affiliated Hospital of Shandong University of Chinese Medicine and the First Affiliated Hospital of Guangzhou University of Chinese Medicine are the participating units. In addition to conventional pharmacotherapy for angina, the intervention group will receive BSHXG while the placebo group will receive BSHXG placebo. All participants will receive 2 months of treatment with 6 months of follow-up. The primary outcome is the efficacy of angina pectoris symptoms in CHD. Secondary outcomes are nitroglycerin arrest, ECG efficacy, Seattle Angina Questionnaire score, serology indicators, assessment of safety, and cardiovascular endpoint events. The transcriptome and metabolome will be used to screen biomarkers for diagnosis and efficacy evaluation.
Discussion: This study aimed to evaluate the efficacy and safety of Bu-Shen-Huo-Xue granule in the treatment of coronary heart disease, and to evaluate the benefits to patients with coronary heart disease from both cardiac and renal indicators.
Trial registration: This trial is approved by the Ethical Review Committee of the Guang’anmen Hospital China Academy of Chinese Medical Sciences with the number 2022-224-KY-01, and has been registered on the Chinese Clinical Trials Registry with the number ChiCTR2300070977 on 27 April 2023.
Cardiovascular-related diseases, as a major public health problem, were noted in the World Health Organization (WHO) Global Health Estimate Report 2022 (1), which states that about 33.2 million deaths occur worldwide from cancer, cardiovascular disease, diabetes, and chronic respiratory diseases due to increased population growth and increased life span. The “Summary of China Cardiovascular Health and Disease Report 2021” (2) also points out that the prevalence and mortality of cardiovascular diseases in China is still on the rise, with rural and urban cardiovascular diseases accounting for 46.74% and 44.26% of the causes of death, respectively, resulting in an increasing burden. Coronary heart disease (CHD) with unstable angina pectoris is a condition where the arteries very easily rupture and bleed because of plaques, and the prognosis is often dangerous. Although the existing secondary prevention concepts and treatments such as interventional therapy and coronary artery bypass grafting have achieved effective results, some patients still developed recurrent angina pectoris after revascularization, following a decline in quality of life, resistance against antiplatelet drugs, secondary formation of thrombosis, and concurrent anxiety and depression. These remain the clinical challenges that need to be addressed. A growing number of epidemiological studies have reported a link between chronic kidney disease (CKD) and CHD, perhaps providing another perspective on clinical treatment. Traditional Chinese Medicine (TCM) has been widely used in treating CHD for a long time and studies have confirmed the biological mechanism (3, 4). With the change of social lifestyle, the TCM syndrome for unstable angina pectoris with coronary heart disease presents a combination form of “kidney deficiency and blood stasis.” A clinical epidemiological survey on the distribution of TCM syndromes showed that qi deficiency was the main symptom of angina pectoris in coronary heart disease, accounting for up to 78.8%, second only to blood stasis, of which heart and kidney qi deficiency was the mainstay (5). Another study analyzed nine common symptom combinations of patients with angina pectoris through algorithms, of which the symptom group with qi deficiency and blood stasis as the main evidence accounted for as high as 21% (6). Studies have described the correlation between estrogen level and renal deficiency-type coronary heart disease and the intervention of kidney tonifying Chinese medicines (7). Bu-Shen-Huo-Xue Granule (BSHXG) is a common Chinese medicine for prevention and cure of CHD. It is based on the traditional Chinese medicine theory of “Tonifying the kidney and promoting blood circulation”. The existing research has some problems such as insufficient sample size, low quality, and insufficient evidence, therefore, we designed a multicenter, randomized, double-blind, placebo-controlled, clinical trial to evaluate the efficacy and safety of BSHXG in the treatment of CHD.
To evaluate the efficacy and safety of BSHXG in the treatment of kidney deficiency and blood stasis in unstable angina pectoris coronary heart disease. The mechanism of the drug will be explored from the transcriptomics and metabolomics levels, which provide a basis for the precise treatment of diseases.
This study is a multicenter, randomized, double-blind, placebo-controlled trial registered with the Chinese Clinical Trials Registry (registration number: ChiCTR2300070977). All documents, including study protocols, informed consent forms, and case report forms (CRFs) meet the requirements of the Declaration of Helsinki and have been reviewed by the Academic Committee and Ethics Committee of the Guang’anmen Hospital. The trial will be implemented based on the principles of Good Clinical Practice and reported according to the CONSORT statement (8). The trial flow diagram is illustrated in Figure 1.
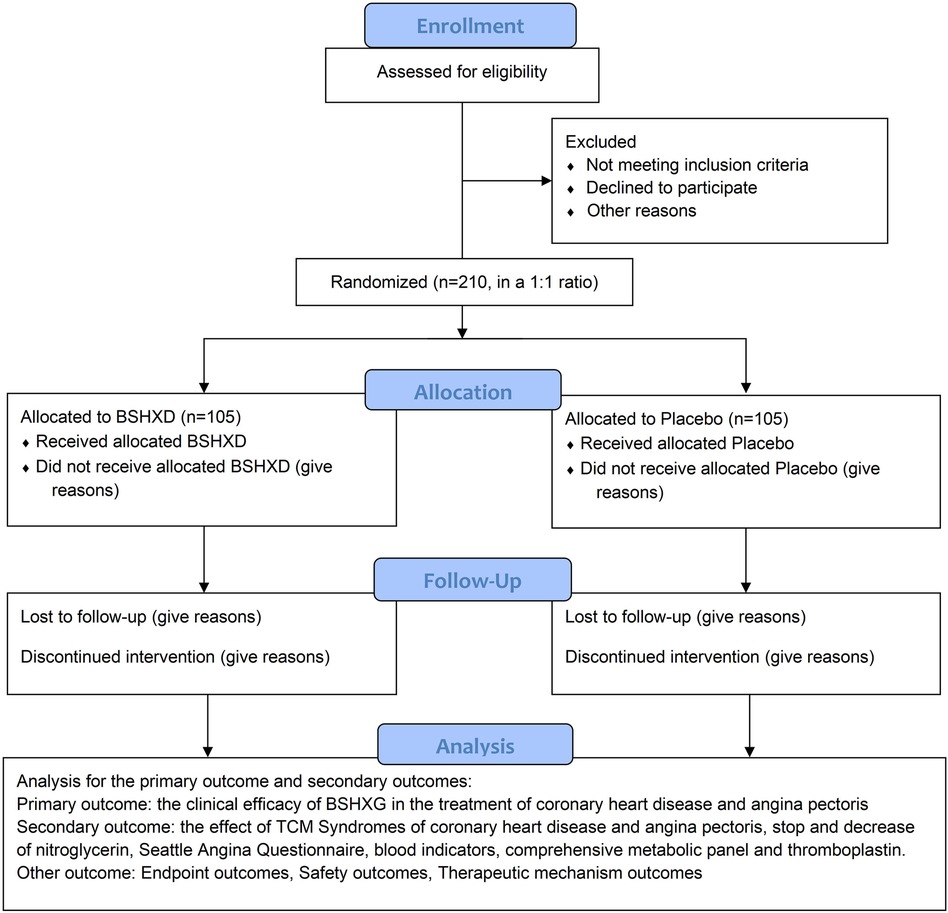
Figure 1. The flow chart of the trial.
This study was a randomized controlled trial, and the frequency of weekly angina attacks in participants was the primary outcome measure. One previous study suggested that the reduction of weekly angina attacks after interventional treatment is 4.2 with a standard deviation of 8.5 (9). Therefore, in the following formula, c is the ratio between two sample cases, n1 = n2, so c = 1. The variable σ is the standard deviation of 8.5, and δ is the expected effect of 4.2, so σ = 8.5 and δ = 4.2. Given a type I error rate of α = 0.05, and a power of 90% (type II error rate of β = 0.1), then uα = 1.96, uβ = 1.282. n1 = n2 = 88, the sample size for one group needs to be 88, resulting in n = 2 × 88 = 176 patients. Considering the maximum possible dropout rate is 15%, a total of 210 patients were needed to be allocated to reach the required number of patients for the efficacy analysis.
1. Aged 40–80 years old, male or female.
2. Typical chest pain behind the sternum, predictably accompanied by pressure, burning, and dying sensations.
3. Induced or aggravated by fatigue, emotional excitement, heavy meals, or cold.
4. Chest pain symptoms lasting for 3–5 min each time and lasting less than 30 min.
5. Can be relieved by rest and/or nitroglycerin within minutes.
6. Canadian Cardiovascular Society (CCS) Angina Grade II–III.
7. Must have experienced symptoms for a minimum specified period (at least 3 months) to confirm the instability of the angina. And there has been no worsening of the above symptoms in the past 3 months.
8. Patients who were diagnosed with kidney deficiency and blood stasis syndrome by TCM syndromes.
9. Provide previous medical records and examination reports that have a clear history of myocardial infarction, or coronary artery bypass grafting. Coronary angiography shows diameter stenosis of one or more main coronary arteries >70%, or diameter stenosis of the left main coronary artery >50%.
10. Patients who voluntarily sign the informed consent.
1. Severe valvular heart disease, severe neurosis, menopausal syndrome, hyperthyroidism, cervical spondylosis, biliary heart disease, stomach and esophageal reflux, and other non-coronary heart disease caused by chest pain.
2. Poor hypertension control (under drug control, blood pressure ≥160/100 mmHg at rest and occasionally within a week), severe cardiopulmonary insufficiency [ejection fraction (EF) <35%], severe arrhythmia (rapid atrial fibrillation, atrial flutter, paroxysmal ventricular tachycardia, atrioventricular block of type II and above, complete bundle branch block).
3. Complicated with serious primary diseases such as heart, brain, liver, kidney, hematopoietic system [hepatic function alanine aminotransferase (ALT) or aspartate transaminase (AST) value >1.5 times the upper limit of normal, patients with abnormal renal function], insulin-dependent type 2 diabetes.
4. Patients with depression or anxiety.
5. Pregnant or lactating women.
6. Patients with malignant tumors.
7. Patients with allergies and allergies to test drug components.
8. Patients with poor compliance and low possibility of follow-up.
9. Participants in other clinical trials within the past month.
10. Other major diseases or factors that interfere with the completion of the trial or affect the interpretation of the results.
The parallel randomization method was adopted, and the center was stratified and divided into experimental group and placebo group according to the ratio of 1:1. With the help of the SAS statistical software PROC PLAN process statement, the treatment allocations with serial numbers 001–210 were listed.
1. Drug packaging and distribution: according to the standardized operation steps of double-blind clinical trials, the experimental drug and placebo drug are packaged and distributed.
2. Blind code preservation regulations: adopt double-blind design in duplicate, separately sealed, and respectively stored.
3. Unblinding regulations: after all the research data are entered and locked, the staff of Guang’anmen Hospital are unblinded, and the statistical analyst writes a statistical analysis report.
4. Regulations on blinding individual cases in emergencies: when serious adverse events occur or emergency rescue is required, the main investigator decides whether it is necessary to open the emergency letter.
5. Provisions for the failure of double-blind test: blind leakage or emergency letter reading rate exceeds 20%.
1. Patients who do not meet the inclusion criteria.
2. Patients who have never used drugs after inclusion.
3. Patients with serious safety problems during the trial.
4. Patients whose drug treatment is ineffective and has no effect or clinical value.
5. Patients with non-fatal myocardial infarction, revascularization, and sudden cardiac death during the trial.
BSHXG consists of 10 kinds of Chinese Herbs (Table 1), including Salvia miltiorrhiza (Dan Shen), Ligusticum wallichii (Chuan Xiong), Peaoniae radix rubra (Chi Shao), Morinda officinalis (Ba Ji Tian), Fructus lycii (Gou Qi Zi), Cistanches herba (Rou Cong Rong), Fructus trichosanthes (Gua Lou), Ginseng radix et rhizoma (Ren Shen), Cassia twig (Gui Zhi), and Panax notoginseng (San Qi). It has a variety of pharmacological effects, including antioxidation, antiatherosclerosis, lipid-lowering, and antiplatelet aggregation.
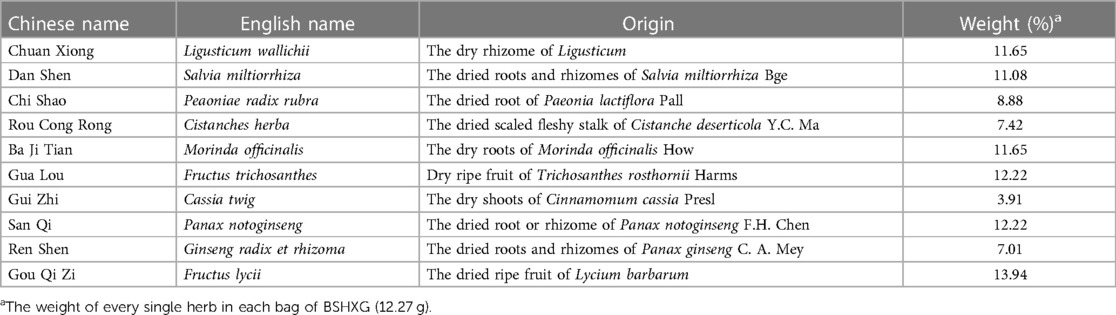
Table 1. The action of each traditional Chinese medicinal herb.
Western medicines for the treatment of coronary heart disease are allowed to be used in accordance with guidelines and clinically reasonable standards. Drugs that relieve symptoms and improve ischemia mainly include three categories, namely, β-blockers, nitrate drugs, and calcium channel blockers. In addition, trimetazidine can improve myocardial tolerance to ischemia and left ventricular function, as well as relieve angina pectoris, which can be used as a second-line drug by regulating myocardial energy substrates and increasing the aerobic oxidation ratio of glucose. When beta-blockers are contraindicated, ineffective, or have adverse reactions, nicorandil and ivabradine can be used to relieve symptoms. Drugs can be used to improve the prognosis and prevent adverse cardiovascular events such as myocardial infarction and death, mainly including antiplatelet drugs, lipid-lowering drugs, angiotensin-converting enzyme inhibitors (ACEI), or angiotensin II receptor antagonists agent (ARB). Detailed medication and dosage recommendations are provided in Table 2.
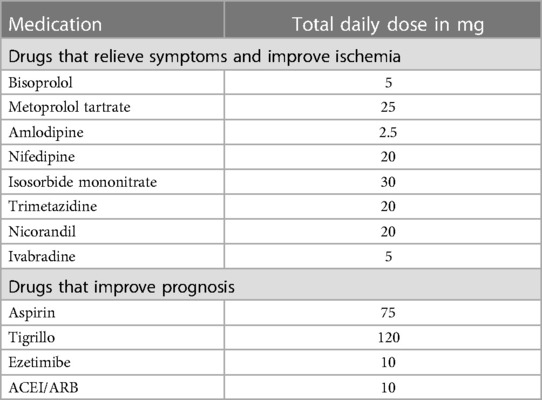
Table 2. Total daily dose of antianginal medication.
Drug name: Bu-Shen-Huo-Xue formula; Dosage form: granules; Specification: g/bag; Production unit: provided by Sichuan New Green Pharmaceutical Technology Development Co., Ltd.; Storage conditions: dry and ventilated place. Medication method of the experimental group: On the basis of conventional Western drug treatment, one bag of BSHXG is taken with warm boiled water at 0.5 h interval after intake of Western medicine. It is orally administered twice in the morning and evening, and the course of treatment is 8 weeks.
Placebo name: Bu-Shen-Huo-Xue placebo formula; Dosage form: granules; Specification: g/bag; Production unit: provided by Sichuan New Green Pharmaceutical Technology Development Co., Ltd.; Storage conditions: dry and ventilated place. Medication method of the control group is the same as for the experimental group.
Changes in the following outcomes from baseline (week 0) to intervention endpoints (week 8) will be assessed.
The primary outcome is to validate the clinical efficacy of BSHXG in the treatment of coronary heart disease and angina pectoris, including the values of change in the frequency and duration of angina before and after treatment.
(1) Effective: angina pectoris symptoms disappear or basically disappear.
(2) Improved: The frequency of angina pectoris attacks is reduced and the duration is shortened although it still exists.
(3) Ineffective: The frequency and duration of angina pectoris attacks are basically the same as before treatment.
(4) Aggravated: The frequency and duration of angina pectoris attacks increase.
1. The effect of TCM syndromes of coronary heart disease and angina pectoris
(1) Effective: TCM syndrome improvement >70%.
(2) Improved: TCM syndrome improvement >30%.
(3) Ineffective: TCM syndrome improvement <30%.
2. Stopping and decreasing of nitroglycerin
(1) Effective: Angina pectoris disappears or is basically relieved within 3 min (including 3 min) after taking the medicine.
(2) Improved: angina pectoris disappears or is basically relieved within 3–5 min after taking the medicine.
(3) Ineffective: Angina pectoris gradually relieves or does not improve more than 5 min after taking the medicine.
(4) Aggravated: Angina pectoris worsens after taking medication.
3. Seattle angina questionnaire
(1) Effective: standard points increase.
(2) Ineffective: the standard integral remains unchanged.
(3) Aggravated: reduction of standard points.
4. Blood indicators such as routine blood test, comprehensive metabolic panel, and thromboplastin
(1) Effective: The difference (mean ± standard deviation) between post-treatment and baseline is statistically significant (p < 0.01).
(2) Improved: The difference (mean ± standard deviation) between post-treatment and baseline is significant (p < 0.05).
(3) Ineffective: The difference (mean ± standard deviation) between post-treatment and baseline has no significance (p > 0.05).
(4) Aggravated: The difference between post-treatment and baseline (mean ± standard deviation) is opposite to the outcome of the treatment effect.
Cardiovascular endpoint events including all-cause mortality, non-fatal myocardial infarction, stroke, percutaneous coronary intervention (PCI) surgery, coronary bypass surgery, malignant arrhythmias, worsening angina pectoris, and re-hospitalization were followed 6 months after treatment. If the patient experiences any discomfort, new changes, or unexpected conditions during the trial research period, whether related to the intervention or not, he or she will be clinically evaluated and given coronary angiography examination or medical treatment.
1. Valid: no endpoint event occurred.
2. Invalid: an endpoint event occurs.
1. Vital signs: such as body temperature, blood pressure, breathing, and heart rate (recorded once at each observation point).
2. Routine laboratory tests for blood, urine, and stool (before and after medication).
3. Electrocardiogram (ECG), liver function (ALT, AST), kidney function [blood urea nitrogen (BUN), Creatinine (Cr)] (before and after medication).
4. Adverse events (detailed records at any time).
To explore the mechanism of BSHXG in transcriptomics in coronary heart disease renal deficiency blood stasis, the participants are made to give 4 ml of venous blood, which is placed in an anticoagulant separator vacuum collection tube [ethylenediaminetetraacetic acid (EDTA)], stored at 4°C, and peripheral blood nuclear cells (PBNCs) are isolated for no more than 6 h. RNA extraction of peripheral blood nucleated cells was performed in the cardiovascular laboratory to screen for differential molecules in transcriptomics before and after treatment.
1. In the process of this research, the main investigator will appoint a clinical supervisor to regularly conduct on-site supervision visits to the research unit to ensure that all the contents of the research plan are strictly observed, and the information filled in is correct.
2. Personnel participating in clinical trials must carefully study and discuss clinical trial protocols and manuals, and unify recording methods and judgment standards.
3. Researchers should truthfully, in detail, and carefully use pen or carbon pen to fill in the CRF item by item.
4. All observations and findings in the clinical trials should be verified to ensure the reliability of data and that the conclusions in the clinical trials are derived from original data.
5. Medical records and medical record forms are original records and generally cannot be changed. Any corrections may not alter the original records and may only be accompanied by a narrative of justification, signed and dated by the physician participating in the clinical trial.
6. Researchers should actively take measures (notification of follow-up and follow-up) to control the dropout rate of cases within 20%.
7. In order to ensure the compliance of the participants, the participants should fully understand the significance of taking drugs on time. Researchers should keep a record of their medication. Those who do not fully comply with the requirements should be persuaded in a timely manner, and the reasons should be recorded in detail.
8. Each research unit strictly grasps the quality control standards.
9. The accuracy, reliability, and abnormal judgment standards of laboratory tests should be unified among all centers.
10. Laboratory data should be recorded in the CRF and the original report should be glued to the medical record. Laboratory data within the normal range should also be recorded. All researchers involved in data entry and data management will sign a confidentiality agreement to prevent data leakage. The schedule of enrollment, interventions, and assessments can be checked in Table 3.
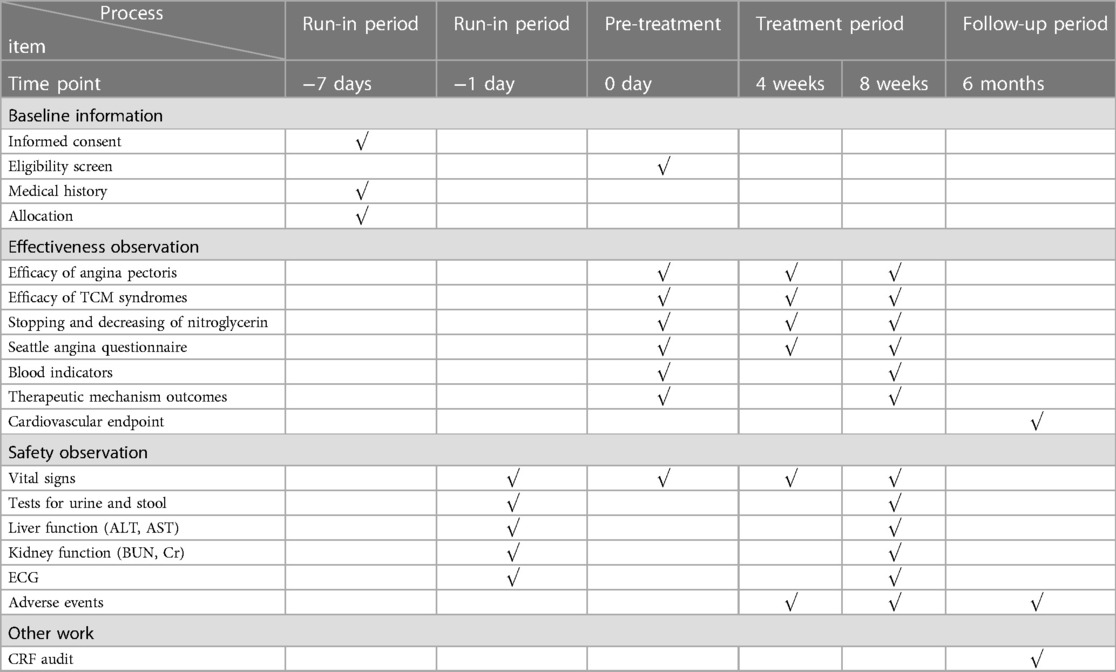
Table 3. Schedule of the data collection.
SPSS Statistics 20.0 was used for statistical analysis of the data. Measurement data were expressed as mean ± standard deviation (mean ± SD). When comparing the two sets of measurement data, if the normal distribution was in line, the t-test or paired t-test of two independent samples was used. If normal distribution was not present, the Mann–Whitney U test, also called the Wilcoxon non-parametric test, was used. The counting data were expressed as frequency or composition ratio and analyzed by Chi-square test. All trial data were double-sided, with a P < 0.05 indicating a statistically significant difference.
Coronary heart disease is a major global public health problem, with high morbidity and mortality. Although the use of Western medicine has significantly reduced the mortality rate of patients with coronary heart disease, there are still many patients with chest pain, chest tightness, shortness of breath, fatigue, and other symptoms, resulting in a decline in their quality of life and seriously affecting normal life. Traditional Chinese Medicine takes dialectical treatment as the core in improving symptoms and improving the quality of life, and believes that the pathogenesis of coronary heart disease has kidney deficiency at the foundation, and blood stasis as the target, therefore treatment should be legislated to replenish the kidney and activate blood (10, 11).
BSHXG used in this study is composed of 10 drugs. Modern research has found that Chuanxiong, the main active ingredient of tetramethylpyrazine, can dilate coronary arteries and improve blood oxygen supply to the myocardium (12, 13). The combination of Danshen and Chuanxiong can effectively improve blood rheological indexes including erythrocyte sedimentation rate, fibrinogen, hematocrit, whole blood viscosity, and plasma viscosity in patients with coronary heart disease (14). The total red peony glycosides in Chishao can exert its antithrombotic effect by reducing fibrinogen, red blood cell aggregation, and platelet aggregation (15). At the same time, modern studies have also found that the main component of Roucongrong, Cistanche Total Glycoside, can reduce the amplitude of ST segment elevation of ECG in rats with coronary ligation, reduce the area of myocardial infarction, regulate myocardial phosphocreatine kinase activity, and play a role in protecting ischemic myocardium (16). Bajitian can increase the activity of Ca2+-ATPase and Na+-k+-ATPase enzyme, reduce creatine kinase concentration, myocardial infarction area, and protect cardiomyocytes (17). Gualou has the effects of dilating coronary arteries, anti-platelet aggregation, protecting ischemic myocardium, improving oxygen tolerance, and inhibiting inflammatory reactions (18). Cinnamon in Guizhi has the effect of inhibiting the secretion of prostaglandin E2, and then exerts anti-inflammatory effects (19). Panax notoginseng in Sanqi can protect the vascular endothelium (20). Renshen has the effects of anti-atherosclerosis, anti-platelet aggregation, anti-thrombosis, improving myocardial ischemia and ventricular remodeling (21). Goqizi can reduce the content of cholesterol and triglycerides in human serum, reduce the degree of lipid peroxidation, improve superoxide dismutase (SOD) activity, maintain the balance of the body's antioxidant system, protect tissue cells from free radical damage, and reduce blood lipid content (22).
The studies involving humans were approved by the Ethical Review Committee of Guang’anmen Hospital China Academy of Chinese Medical Sciences. The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
LL: Writing – original draft, Investigation, Software, Validation, Writing – review & editing. JW: Funding acquisition, Project administration, Writing – original draft, Writing – review & editing. JL: Data curation, Supervision, Writing – original draft. XL: Data curation, Supervision, Writing – original draft. RL: Data curation, Supervision, Writing – original draft. YL: Data curation, Supervision, Writing – original draft. GY: Investigation, Software, Validation, Writing – original draft. QM: Investigation, Software, Validation, Writing – original draft. LW: Investigation, Software, Validation, Writing – original draft. ZY: Writing – original draft, Investigation, Software, Validation. YW: Investigation, Software, Validation, Writing – original draft. SZ: Investigation, Software, Validation, Writing – original draft. CL: Writing – review & editing.
The authors declare financial support was received for the research, authorship, and/or publication of this article.
This study was funded by the Traditional Chinese Medicine Inheritance and Innovation “Ten Million” talent project—Qhuang Project Chief Scientist Project (0201000401).
We thank Xin Wang for the data monitoring and concealment of the randomization sequence.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fcvm.2024.1293818/full#supplementary-material
1. World Health Statistics 2019: Monitoring Health for the SDGs, Sustainable Development Goals. Geneva: World Health Organization (2019).
2. Hu SS. Overview of Chinese cardiovascular health and disease report 2021. Chin J Circ. (2022) 37(6):26. doi: 10.3969/j.issn.1000-3614.2022.06.001
3. Liu LC, Mao QY, Liu C, Hu J, Duan L, Wang J. The effectiveness and safety of Bushen Huoxue decoction on treating coronary heart disease: a meta-analysis. Evid Based Complement Alternat Med. (2021) 2021:5541228. doi: 10.1155/2021/5541228
4. Liu C, Liu L, Gao J, Wang J, Liu Y. Identification of two long non-coding RNAs AC010082.1 and AC011443.1 as biomarkers of coronary heart disease based on logistic stepwise regression prediction model. Front Genet. (2021) 12:780431. doi: 10.3389/fgene.2021.780431
5. Wang J, Li J, Yao KW, Zhong JB. Study on the combination of angina syndrome and indications in coronary heart disease. J Trad Chin Med. (2007) 48(10):920–2. doi: 10.13288/j.11-2166/r.2007.10.029
6. Wang J, Xing YW, Chen JX, He QY, Chen J, Xi GC, et al. Study on the extraction and combination of angina syndrome elements in 1069 cases of coronary heart disease by entropy accumulation pile method in complex systems. Chin J Basic Med Trad Chin Med. (2008) 03:211–3. doi: 10.3969/j.issn.1006-3250.2008.03.024
7. Liu LC, Duan L, Liu C, Wang J. Correlation between estrogen levels and kidney deficiency syndrome in coronary heart disease and the intervention effect of kidney-tonifying traditional Chinese medicine. Chin J Trad Chin Med. (2021) 46(07):1738–42. doi: 10.19540/j.cnki.cjcmm.20201221.601
8. Moher D, Hopewell S, Schulz KF, Montori V, Gøtzsche PC, Devereaux PJ, et al. CONSORT 2010 explanation and elaboration: updated guidelines for reporting parallel group randomised trials. J Clin Epidemiol. (2010) 63(8):e1–37. doi: 10.1016/j.jclinepi.2010.03.004
9. Zhao L, Li DH, Zheng H, Chang XR, Cui J, Wang RH, et al. Acupuncture as adjunctive therapy for chronic stable angina: a randomized clinical trial. JAMA Intern Med. (2019) 179(10):1388–97. doi: 10.1001/jamainternmed.2019.2407
10. Liu C, Wang J. Its application and research in the treatment of coronary heart disease from the effect of kidney tonification on blood veins. Chin J Trad Chin Med. (2018) 33(3):841–3. CNKI:SUN:BXYY.0.2018-03-008
11. He HQ, Gao JL, Chen G, Liu C, Wang J. Application and research of kidney tonification and blood revitalization method in cardiovascular disease. J Cardiovasc Cerebrovasc Dis Integr Trad West Med. (2017) 15(14):1805–9. doi: 10.3969/j.issn.1672-1349.2017.14.041
12. Wu HM, Zhuo XH. Research progress on the pharmacological effects and clinical application of chuanxiongzine in cardiovascular and cerebrovascular diseases. Electron J Clin Med Lit. (2015) 2(9):1683–6. doi: 10.16281/j.cnki.jocml.2015.09.083
13. Zhang Z. Pharmacological effects and clinical application progress of chuanxiongzine on cardiovascular protection. China Pract Med. (2009) 4(7):129–30. doi: 10.3969/j.issn.1673-7555.2009.07.100
14. Cheng LY. Effect of Danshen Wuchuanxiong on blood rheology in patients with coronary heart disease. Electron J Integr Trad West Med Cardiovasc Dis. (2018) 6(35):157–8. doi: 10.3969/j.issn.2095-6681.2018.35.125
15. Zhang SK, Cao YB. Research progress on pharmacological effects of red peony. J Pharm Pract. (2021) 39(02):97–101. doi: 10.12206/j.issn.1006-0111.202006087
16. Mao XM, Wang XW, Li LL, Wang XF. Protective effect of cistanche total glycoside on myocardial ischemia in rats. Chin Trad Herb Drugs. (1999) 2:118–20. doi: 10.3321/j.issn:0253-2670.1999.02.019
17. Li K, Si ZY, Li YX, Huang K. Effect of halberdium on myocardial ischemia-reperfusion injury in rats. J Mil Med Coll. (2012) 33(3):277–9, 301.
18. Huang Y, Wang Q, Zhu XW, Gan C. Pharmacological effects and research progress of guarana in the treatment of coronary heart disease. Electron J Cardiovasc Dis Integr Trad West Med. (2019) 7(23):18. doi: 10.16282/j.cnki.cn11-9336/r.2019.23.011
19. Hu HX, Zhu XQ, Li ZF, Lin RH, Chen LD. Study on the anti-inflammatory effect of Guizhi decoction on the activation of microglia. Clin Pract Integr Trad Chin West Med. (2017) 17(1):152–5. doi: 10.13638/j.issn.1671-4040.2017.01.090
20. Chen YB, Dong YH. Clinical effect and pharmacological effect analysis of Panax notoginseng saponins in the treatment of hyperlipidemia. Chin Med Sci. (2016) 6(1):51–3, 139.
21. Liu L, Hu J, Mao Q, Liu C, He HQ, Hui XS. Functional compounds of ginseng and ginseng-containing medicine for treating cardiovascular diseases. Front Pharmacol. (2022) 13:1034870. doi: 10.3389/fphar.2022.1034870
Keywords: coronary heart disease, kidney deficiency, blood stasis, Bu-Shen-Huo-Xue, Chinese herbal medicine, traditional Chinese medicine, randomized controlled trial
Citation: Liu L, Wang J, Li J, Li X, Li R, Liu Y, Yang G, Mao Q, Wang L, Yao Z, Wang Y, Zong S and Liu C (2024) Efficacy and safety of the Chinese herbal medicine Bu-Shen-Huo-Xue granule for the treatment of coronary heart disease: study protocol for a multicenter, randomized, double-blinded, placebo-controlled clinical trial. Front. Cardiovasc. Med. 11:1293818. doi: 10.3389/fcvm.2024.1293818
Received: 13 September 2023; Accepted: 25 April 2024;
Published: 4 June 2024.
Edited by:
Fanyan Luo, Central South University, ChinaReviewed by:
Mohammed Faisaluddin, Rochester General Hospital, United States© 2024 Liu, Wang, Li, Li, Li, Liu, Yang, Mao, Wang, Yao, Wang, Zong and Liu. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Jie Wang, d2FuZ2ppZTAxMDNAMTI2LmNvbQ==
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.