 Théo Pezel1,2,3,4,5
Théo Pezel1,2,3,4,5 Solenn Toupin6
Solenn Toupin6 Thomas Hovasse4Stéphane Champagne4
Thomas Hovasse4Stéphane Champagne4 Thierry Unterseeh4Teodora Chitiboi7
Thierry Unterseeh4Teodora Chitiboi7 Puneet Sharma8Francesca Sanguineti4
Puneet Sharma8Francesca Sanguineti4 Philippe Garot4
Philippe Garot4 Jérôme Garot4*
Jérôme Garot4*
- 1Department of Cardiology, University Hospital of Lariboisiere, Université Paris-Cité, (Assistance Publique des Hôpitaux de Paris, AP-HP), Paris, France
- 2Inserm MASCOT-UMRS 942, Department of Data Science, University Hospital of Lariboisiere, Paris, France
- 3Department of Radiology, University Hospital of Lariboisiere, Université Paris-Cité, (Assistance Publique des Hôpitaux de Paris, AP-HP), Paris, France
- 4Cardiovascular Magnetic Resonance Laboratory, Institut Cardiovasculaire Paris Sud (ICPS), Hôpital Privé Jacques Cartier, Ramsay Santé, Massy, France
- 5MIRACL.ai laboratory, Multimodality Imaging for Research and Analysis Core Laboratory-Artificial Intelligence, Department of Data Science, Machine Learning and Artificial Intelligence in Health, University Hospital of Lariboisiere (AP-HP), Paris, France
- 6Siemens Healthcare France, Scientific Partnerships, Saint-Denis, France
- 7Siemens Healthcare GmbH, Department of CMR, Hamburg, Deutschland
- 8Digital Technologies and Innovation, Siemens Healthineers, Princeton, NJ, United States
Stress cardiovascular magnetic resonance (CMR) imaging has emerged as an accurate and cost-effective modality without ionizing radiation for risk stratification using ischemia and late gadolinium enhancement (LGE) as prognostic markers (1). Beyond these traditional stress CMR findings, recent studies have highlighted the incremental prognostic value of global longitudinal or circumferential strain using feature-tracking imaging measured during vasodilator stress (2), especially in patients with normal stress CMR, defined by the absence of ischemia and LGE, regardless of the LVEF value or the presence of wall motion abnormalities (3). Recent studies have shown that the regional circumferential myocardial strain (Ecc) could be a more accurate predictor of cardiovascular events than the LVEF value or global Ecc (4, 5). Also, it is suggested that an analysis of specific myocardial layers could further improve its prognostic value (4). The value of a stress CMR–derived layer-specific regional Ecc score compared with global Ecc has not yet been established. Therefore, in this short study, we aim to determine whether a fully automated regional circumferential strain score (RSS) measured during vasodilator stress CMR can provide incremental prognostic value in patients with normal CMR.
During the period between January and July 2017, we conducted a single-center study with a retrospective enrollment of all consecutive patients with normal stress CMR (Siemens Espree 1.5 T, absence of ischemia or LGE). A normal stress CMR examination was defined by the absence of both ischemia and LGE. Hyperemia was induced with dipyridamole (0.84 mg/kg over 3 min). A bolus of 0.1 mmol/kg gadolinium chelates was injected (5 ml/s) with acquisitions of four left ventricular short-axis and two long-axis views using first-pass perfusion imaging. Then, a stack of eight short-axis views covering the entire LV were obtained using the b-SSFP sequence. Cross-registered LGE images were acquired 10 min after contrast injection. An analysis of perfusion images was done visually by two blinded experienced operators. The definitions of ischemia and LGE were based on established criteria (1, 2). A fully automated machine learning algorithm was trained using a dense UNet on 3,000 CMR studies from the UK Biobank resource and validated on unseen CMR studies to assess the stress-GCS of each myocardial segment from short-axis cine images acquired at stress (3). All details of the AI software methodology have already been recorded (3). To calculate the RSS (4), each segment was rated from 0 to 2 points according to the Ecc value of each layer to grade the LV regional myocardial function for the 16-segment model as follows: (i) 0 points if Ecc was more than −10% for severe regional dysfunction; (ii) 1 point if Ecc was between −17 and −10% for moderate regional dysfunction; and (iii) 2 points if Ecc was <−17% for good regional function. Then, using endo-Ecc, mid-Ecc, and epi-Ecc for the 16-segment model, we defined Endo-, Mid-, and Epi-RSS, respectively, as three indices of segmental myocardial function ranging from 0 to 32 points. To summarize the overall regional myocardial function, we defined the RSS as a score ranging from 0 to 96 points, which corresponded to the sum of the Endo-, Mid-, and Epi-RSS. The follow-up consisted of yearly clinical visits and additional contacts in case of events. The primary outcome was the occurrence of MACE defined as cardiovascular mortality or nonfatal myocardial infarction. Cox regressions were used to evaluate the association of stress-RSS with the primary outcome after adjustment for the following traditional risk factors: age, male, body mass index, diabetes, hypertension, smoking, dyslipidemia, known coronary artery disease, and LVEF value.
Among the 1,823 consecutive patients referred for stress CMR, 1,491 (82%) patients underwent a normal CMR examination (65 ± 12 years, 67% men). Among these, 1,321 (88.9%) completed clinical follow-up [median follow-up 5.1 (4.8–5.4) years] with 52 MACEs. After adjustment for traditional risk factors, stress-RSS was inversely associated with the occurrence of MACE [adjusted hazard ratio (HR), 0.75; 95% CI: 0.70–0.80, Figure 1]. The annual mortality rate was higher in patients with stress-RSS < 50% (6.3%/year) than in patients with stress-RSS value ≥ 50% (0%/year, p < 0.001). The addition of stress-RSS showed the best improvement in model discrimination and reclassification to predict MACE above traditional risk factors, including the LVEF value, and over stress CMR findings (C-statistic improvement: 0.29; NRI = 0.569; IDI = 0.153, Chi-2 global = 125, all p < 0.001; LR-test p < 0.001), corresponding to slightly better results than the stress-GCS (C-statistic improvement: 0.27; NRI = 0.539; IDI = 0.108, Chi-2 global = 98.9, LR-test p < 0.001).
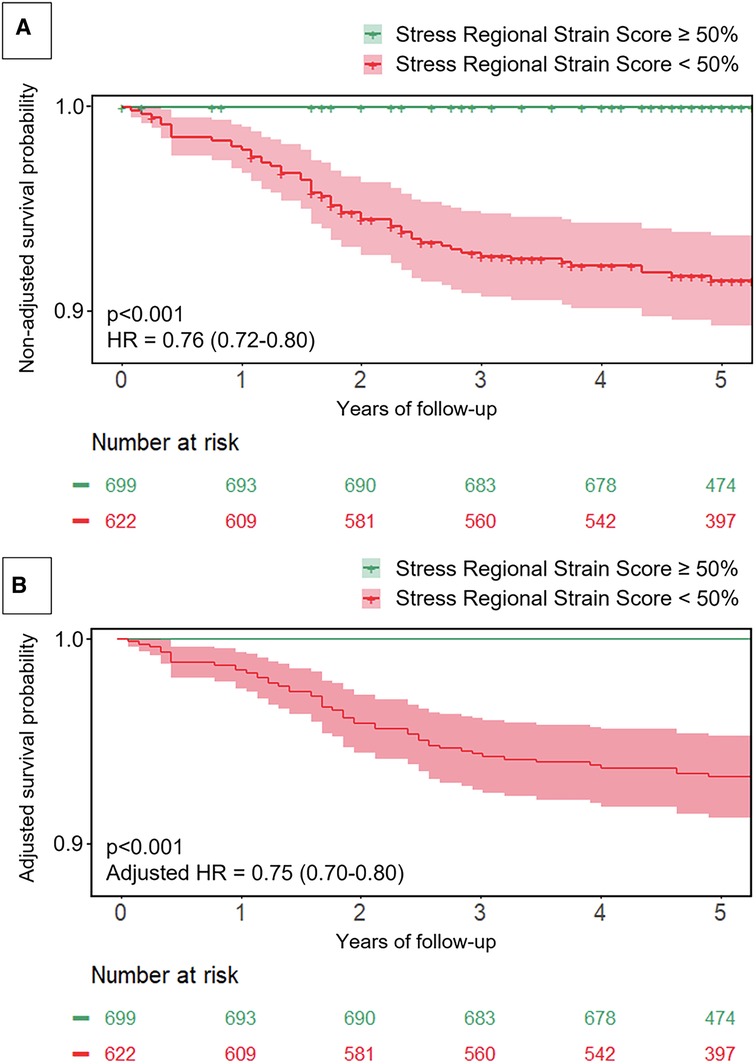
Figure 1. Survival curves for the occurrence of MACE according to RSS. The non-adjusted (A) and adjusted (B) event-free survival curves with confidence intervals for MACE were described. The adjustment used the final model including all traditional prognostic factors: age, male, body mass index, diabetes, hypertension, smoking, dyslipidemia, known coronary artery disease, LVEF value, and stress-RSS. HR indicates hazard ratio.
This was a single-center study with high-volume stress CMR studies (>3,700/year) with a relatively low adverse-event rate. Baseline data and follow-up information on medications were not collected. These limitations were related to patient care and reflected current clinical practice. This retrospective study could not capture all confounding factors potentially affecting decision-making and patient risk. Finally, dipyridamole was used as a vasodilator agent mainly because of medico-economic reasons and its similar efficacy/safety profile to that of adenosine. Further randomized clinical trials are required to assess the prognostic impact of stress-RSS in patients with normal CMR.
In conclusion, this study shows that layer-specific regional Ecc measured during stress CMR (stress-RSS) provides a robust, independent, and incremental predictive value for MACE over traditional risk factors and stress CMR findings in patients with normal CMR. These findings might reflect the subtle functional consequences of the impairment of microvasculature not depicted by conventional (non-quantitative) stress CMR data.
Author contributions
TP: Conceptualization, Data curation, Formal Analysis, Methodology, Validation, Visualization, Writing – original draft, Writing – review & editing, Investigation, Software, Supervision. ST: Investigation, Software, Writing – review & editing. TH: Investigation, Software, Writing – review & editing. SC: Investigation, Conceptualization, Software, Writing – review & editing. TU: Investigation, Software, Writing – review & editing. TC: Methodology, Software, Investigation, Writing – review & editing. PS: Methodology, Software, Investigation, Writing – review & editing. FS: Investigation, Writing – review & editing. PG: Investigation, Validation, Writing – review & editing. JG: Supervision, Validation, Visualization, Writing – review & editing.
Funding
The authors declare that no financial support was received for the research, authorship, and/or publication of this article.
Conflict of interest
ST, TC, AJ, and PS are employees of Siemens Healthcare.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The authors declared that they were an editorial board member of Frontiers, at the time of submission. This had no impact on the peer review process and the final decision.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Kwong RY, Ge Y, Steel K, Bingham S, Abdullah S, Fujikura K, et al. Cardiac magnetic resonance stress perfusion imaging for evaluation of patients with chest pain. J Am Coll Cardiol. (2019) 74:1741–55. doi: 10.1016/j.jacc.2019.07.074
2. Romano S, Romer B, Evans K, Trybula M, Shenoy C, Kwong RY, et al. Prognostic implications of blunted feature-tracking global longitudinal strain during vasodilator cardiovascular magnetic resonance stress imaging. JACC Cardiovasc Imaging. (2020) 13:58–65. doi: 10.1016/j.jcmg.2019.03.002
3. Pezel T, Garot P, Toupin S, Hovasse T, Sanguineti F, Champagne S, et al. Prognostic impact of artificial intelligence-based fully automated global circumferential strain in patients undergoing stress CMR. Eur Heart J—Cardiovasc Imaging. (2023) 24(9):1269–1279. doi: 10.1093/ehjci/jead100
4. Pezel T, Bluemke DA, Wu CO, Lima JAC, Ambale Venkatesh B. Regional strain score as prognostic marker of cardiovascular events from the multi-ethnic study of atherosclerosis (MESA). Front Cardiovasc Med. (2022) 9:870942. doi: 10.3389/fcvm.2022.870942
Keywords: cardiac MRI (CMRI), strain, stress CMR, artificial intelligence, strain score, major adverse cardiac event (MACE)
Citation: Pezel T, Toupin S, Hovasse T, Champagne S, Unterseeh T, Chitiboi T, Sharma P, Sanguineti F, Garot P and Garot J (2024) A fully automated stress regional strain score as a prognostic marker of cardiovascular events in patients with normal CMR. Front. Cardiovasc. Med. 10:1334553. doi: 10.3389/fcvm.2023.1334553
Received: 7 November 2023; Accepted: 21 December 2023;
Published: 8 January 2024.
Edited by:
Niek H. J. Prakken, University Medical Center Groningen, NetherlandsReviewed by:
Luca Arcari, M.G. Ospedale Vannini, Italy© 2024 Pezel, Toupin, Hovasse, Champagne, Unterseeh, Chitiboi, Sharma, Sanguineti, Garot and Garot. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Jérôme Garot amdhcm90QGFuZ2lvLWljcHMuY29t
Abbreviations BMI, body mass index; CAD, coronary artery disease; CI, confidence interval; CMR, cardiovascular magnetic resonance; HR, hazard ratio; IDI, integrative discrimination index; LGE, late gadolinium enhancement; LR, likelihood ratio; LV, left ventricular; LVEF, left ventricular ejection fraction; MI, myocardial infarction; NRI, net reclassification improvement.