
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Cardiovasc. Med., 20 December 2023
Sec. Hypertension
Volume 10 - 2023 | https://doi.org/10.3389/fcvm.2023.1295174
 Miguel A. Prieto-Díaz1,2,†
Miguel A. Prieto-Díaz1,2,† Vicente Pallares-Carratala3,4*†
Vicente Pallares-Carratala3,4*† Rafael Manuel Micó-Pérez5,†
Rafael Manuel Micó-Pérez5,† Carlos Escobar-Cervantes6,†
Carlos Escobar-Cervantes6,† Vicente Martín-Sanchez7,†
Vicente Martín-Sanchez7,† Antonio Coca8,†Alfonso Barquilla-García9,†Sonsoles M. Velilla-Zancada10,†José Polo-García11,†
Antonio Coca8,†Alfonso Barquilla-García9,†Sonsoles M. Velilla-Zancada10,†José Polo-García11,† Antonio Segura-Fragoso12,†
Antonio Segura-Fragoso12,† Leovigildo Ginel-Mendoza13,†Álvaro Hermida-Ameijerias14,†
Leovigildo Ginel-Mendoza13,†Álvaro Hermida-Ameijerias14,† Sergio Cinza-Sanjurjo15,16,†
Sergio Cinza-Sanjurjo15,16,†  the Investigators of the IBERICAN study and of the Spanish Society of Primary Care Physicians SEMERGEN Foundation
the Investigators of the IBERICAN study and of the Spanish Society of Primary Care Physicians SEMERGEN Foundation
Objectives: To determine the clinical profile, according to the history of hypertension, the risk of developing hypertension, current antihypertensive treatment and BP control rates in patients with hypertension from the IBERICAN cohort.
Methods: IBERICAN is an ongoing prospective cohort study, whose primary objective is to determine the frequency, incidence, and distribution of CVRF in the adult Spanish population seen in primary care settings. This analysis shows the baseline clinical characteristics of patients with hypertension. Adequate BP control was defined as BP <140/90 mmHg according to 2013 ESH/ESC guidelines.
Results: A total of 8,066 patients were consecutively included, of whom 3,860 (48.0%) had hypertension. These patients were older (65.8 ± 10.9 vs. 51.6 ± 14.7 years; p < 0.001), had more cardiovascular risk factors, target organ damage and cardiovascular disease (CVD) in comparison with those without hypertension. The risk of hypertension increased with the presence of associated CV risk factors and comorbidities, particularly diabetes, obesity and the metabolic syndrome, and decreased with the intensity of physical activity. Regarding antihypertensive treatments, 6.1% of patients did not take any medication, 38.8% were taking one antihypertensive drug, 35.5% two drugs, and 19.6% three or more antihypertensive drugs. Overall, 58.3% achieved BP goals <140/90 mmHg. A greater probability of BP control was observed with increasing age of patients and the greater number of antihypertensive drugs. Blood pressure control was lower in hypertensive patients with diabetes, obesity, the metabolic syndrome, increased urinary albumin excretion, higher pulse pressure, and lack of antihypertensive treatment.
Conclusions: About half of patients attended in primary care settings have hypertension in Spain. Patients with hypertension have a worse CV clinical profile than non-hypertensive patients, with greater association of CVRF and CVD. Around four out of ten patients do not achieve the recommended BP goals, and higher use of combination therapies is associated with a better BP control.
Hypertension is the first cause of death and disability worldwide and one of the main modifiable risk factors for the development of cardiovascular disease (CVD) (1). Unfortunately, despite the efforts performed in the last decades to reduce hypertension burden through the reduction of blood pressure (BP) with antihypertensive treatment (2, 3), the fact is that awareness, treatment, and BP control remains suboptimal worldwide (4, 5). Despite the improvement in the prevention and treatment of CVD in Spain, it still remains the first cause of death, accounting for one quarter of all deaths in the country (6, 7). In fact, compared to 2021, death from cardiovascular (CV) causes only descended by 0.6% in 2022 in Spain (8).
Population-based studies in Spain have shown that around one third of adults have hypertension (more than 60% in those >65 years) (9, 10), but in subjects attended in primary care, these numbers reach to 50%–60% of patients (6, 11). Previous studies have shown that only half of treated hypertensive patients are adequately controlled, which would translate into around 30,000 CV deaths annually attributable to hypertension (7). Therefore, an improvement of the awareness, treatment and BP control in our country is urgently needed. In this context, monitoring the evolution of the proportion of patients with hypertension, as well as the optimal therapeutic approach of the hypertensive population seems mandatory (7). Although previous studies have analyzed these critical points (11–14), it seems desirable an update of the current management and control of these patients. On the other hand, primary care is the best setting for promoting the management, follow-up and control of cardiovascular risk factors (CVRF), including hypertension (6, 15).
Although numerous previous studies have analyzed the clinical characteristics and management of patients with arterial hypertension, it is necessary to update these results in a contemporary cohort of patients, analyzing the impact of the latest arterial hypertension guidelines and modern therapies on the management and achievement of BP goals, as well as those factors associated with blood pressure control. Additionally, it is also important to determine whether predictors of developing hypertension have changed over time.
The IBERICAN study (Identification of Spanish Population in Cardiovascular and Renal Risk) is an ongoing prospective cohort study, whose primary aim is to determine the frequency, incidence, and geographical distribution of CVRF in adults attended in primary care in Spain (6, 16, 17). In this article we report the clinical profile according to the history of hypertension, the risk of developing hypertension, current antihypertensive treatment and BP control rates in patients with hypertension from the IBERICAN cohort.
The design and characteristics of the study have been previously published (6, 16, 17). The IBERICAN study is an epidemiological, multicenter, observational, cohort study with a planned follow-up of 10 years, in which 8,066 patients between 18 and 85 years old were recruited by 519 primary care physicians, of the Spanish National Health System, between April 2014 and October 2018, by consecutive non-probabilistic sampling.
To estimate the sample size (18, 19), we followed the next steps: (1) we developed a multivariate Cox regression analysis predictive model to explain the effect of 10 independent variables on the incidence of cardiovascular events are, as the primary strictest objective of the IBERICAN study; (2) a minimum of 10–15 events in each variable was considered to estimate the number of needed events; (3) based on reported Spanish population data, the incidence of events in our population was estimated as 4.75/1,000 habitants/year; and (4) on the basis of this consideration, we calculated a sample size of 4.200–6.300 patients to predict 10–15 events in each variable. A 10% possible loose of patients along the follow-up was added to this figure, so the final number increased to a size of 6,600 patients. When the recruitment period was finished 8,066 patients had completed valid data.
To answer the main objective of the study a double analysis was planned: a longitudinal design to answer questions about the incidence of CVRF and CVD; and a cross-sectional design planned to answer questions about prevalence. This manuscript include data of this later analysis planned to know the prevalence of hypertension and its association with the other associated variables.
All patients provided written informed consent before inclusion. The study was approved by the Clinical Research Ethics Committee of the Hospital Clínico San Carlos in Madrid on 21 February 2013 (C.P. IBERICAN-C.I. 13/047-E) and is registered at https://clinicaltrials.gov with the number NCT02261441.
Patients included in the study underwent a conventional examination of clinical parameters and were treated according to usual clinical practice. As a result, non-pharmacological and pharmacological recommendations were performed according to physicianś judgement. No specific recommendations were performed for being included in the study. At baseline, socio-demographic data, CVRF (age, hypertension, obesity, smoking, diabetes mellitus, hypercholesterolemia, and sedentary lifestyle), HMOD, [high pulse pressure, ankle-brachial index <0.9, electrocardiographic or echocardiographic left ventricular hypertrophy (LVH), and urinary albumin excretion] and established CVD (ischemic heart disease, stroke, peripheral artery disease, heart failure, retinopathy, chronic kidney disease and atrial fibrillation) were collected. The variables were defined in accordance with the 2013 guidelines of the European Societies of Hypertension and Cardiology (ESH/ESC) (20), the current guidelines at the moment of inclusion. Obesity was defined as a body mass index >30 kg/m2, and sedentarism as doing physical less than 30 min of physical activity or absence of activity. The serum biochemistry data were recorded from the lab tests performed in the local laboratories within the last six months previous to the inclusion. The CV risk stratification of patients was carried out following the SCORE tables for low-risk countries, as this stratification was recommended at the time of enrolling (20). Patients outside the age limits for the SCORE algorithm were considered as the age closest to the corresponding interval. Data were collected in an electronic case report forms (eCRF) specifically developed for the study.
Subjects were defined as having hypertension if they had been already diagnosed as such by their physicians, or those who were taking antihypertensive medication.
According to the 2013 ESH/ESC guidelines (20), blood pressure measurement was performed with the patient seated, after 5 min of rest, through 2 determinations and obtaining the average. Adequate BP control was defined as SBP <140 mmHg, in all patients, except in individuals older than 80 years, in which a SBP between 150 and 140 mmHg was considered. Regarding DBP, the target <90 mmHg was considered in all patients, except in patients with diabetes in whom the DBP target was <85 mmHg. The BP control criteria are also in accordance with the current guidelines ESH 2023 (21). Treatments prescribed by physicians at baseline were recorded. The number and type of antihypertensive drugs [including angiotensin-converting enzyme inhibitors (ACEi), angiotensin receptor blockers (ARB), diuretics, calcium channel blockers (CCB), beta blockers, alpha blockers, renin inhibitors, and central acting agents] were also recorded in the overall hypertensive population.
Qualitative variables were expressed as frequencies and percentages and quantitative variables as the mean and standard deviation (SD). For the comparison of subgroups of patients (hypertension vs. no hypertension and men vs. women), parametric tests (Student's t-test) or non-parametric tests (Mann–Whitney U-test) were used for quantitative variables, according to the specific characteristics of the variables examined. The Chi-square test was used for qualitative variables.
In order to evaluate which factors were associated with the presence of hypertension and also those variables that were independently associated with BP control, binary logistic regression models were built. The multivariate models begun to be constructed by introducing those factors with a significance of p < 0.150 in the bivariates by the automatic variable selection method by steps backward. Only the significant factors were finally considered to build the model. Adjusted odds ratios (OR) and their 95% confidence interval were presented in both cases. In all contrasts, the null hypothesis was rejected when the alpha error was lower than 0.05. The statistical package SPSS 23.0 (Statistical Package for Social Sciences) for Windows (Armonk, NY, USA: IBM Corp. Released 2013. IBM SPSS Statistics for Windows, version 23.0 Armonk, NY: IBM Corp.) was used for the data analysis.
A total of 519 primary care physicians recruited 8,066 patients, of whom 3,860 (48.0%) had hypertension. Compared with patients without hypertension, patients with hypertension were older (65.8 ± 10.9 vs. 51.5 ± 14.6 years; p < 0.001), more frequently men (50.5% vs. 49.5%; p < 0.001), had a lower level of education (13.8% vs. 4.7% without any formal study; p < 0.001) and a higher body mass index (BMI 30.06 ± 5.5 vs. 27.03 ± 4.9 kg/m2; p < 0.001). Fasting glucose, triglycerides, creatinine, albumin-to-creatinine ratio and uric acid levels were also higher among patients with hypertension, whereas HDL-cholesterol and estimated glomerular filtration rate (eGFR) were lower (Table 1).
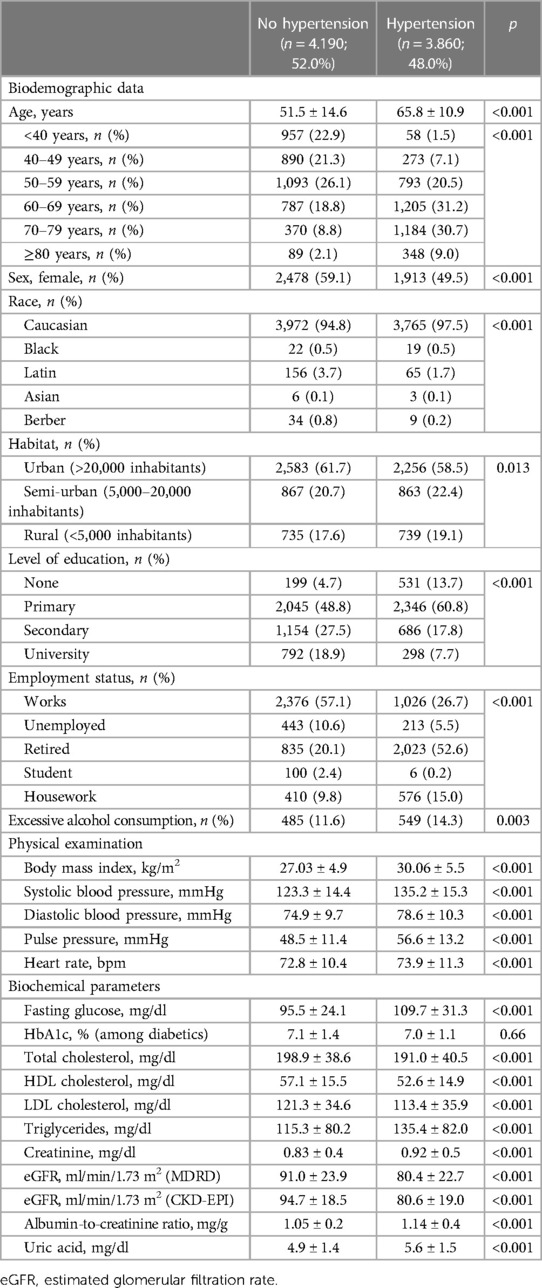
Table 1. Clinical characteristics of the study population according to the history of hypertension (n = 8,066).
Cardiovascular risk factors and comorbidities were more common in the hypertensive population, including hypercholesterolemia (65.9% vs. 36.0%; p < 0.001), diabetes (31.6% vs. 9.6%; P < 0.001), obesity (45.9% vs. 22.6%; p < 0.001), and sedentary lifestyle (34.9% vs. 24.3%; p < 0.001). However, patients without hypertension were more commonly current smokers (21.2% vs. 13.7%; p < 0.001). As expected, the presence of any HMOD was also more frequent in patients with hypertension (44.3% vs. 14.7%; p < 0.001), as well as the presence of clinical CVD (24.1% vs. 9.3%; p < 0.001) (Table 2).
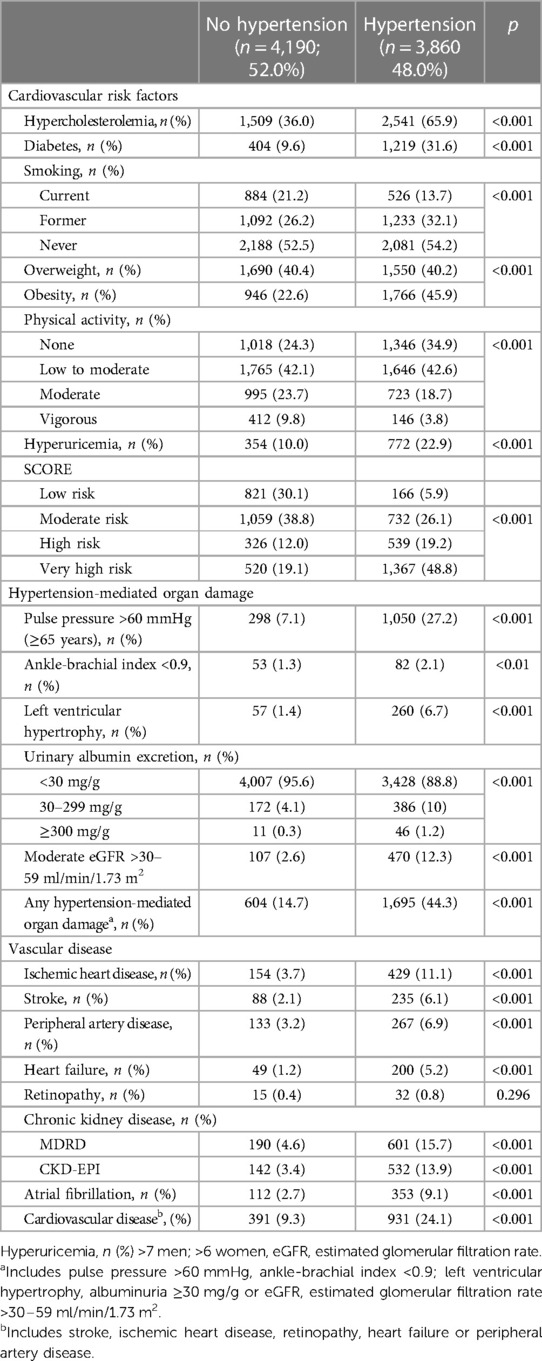
Table 2. Cardiovascular risk factors, hypertension-mediated organ damage and cardiovascular disease according to the history of hypertension (n = 8,066).
The risk of having hypertension increased with the presence of associated CVRF and comorbidities, particularly diabetes and obesity. By contrast, the risk of hypertension decreased with the intensity of physical activity. Similarly, the risk of hypertension increased with the presence of increased urinary albumin excretion, ischemic heart disease, stroke, peripheral artery disease, heart failure, chronic kidney disease and atrial fibrillation. This was particularly high in patients with chronic kidney disease, atrial fibrillation, urinary albumin excretion ≥300 mg/g, and stroke (Table 3).
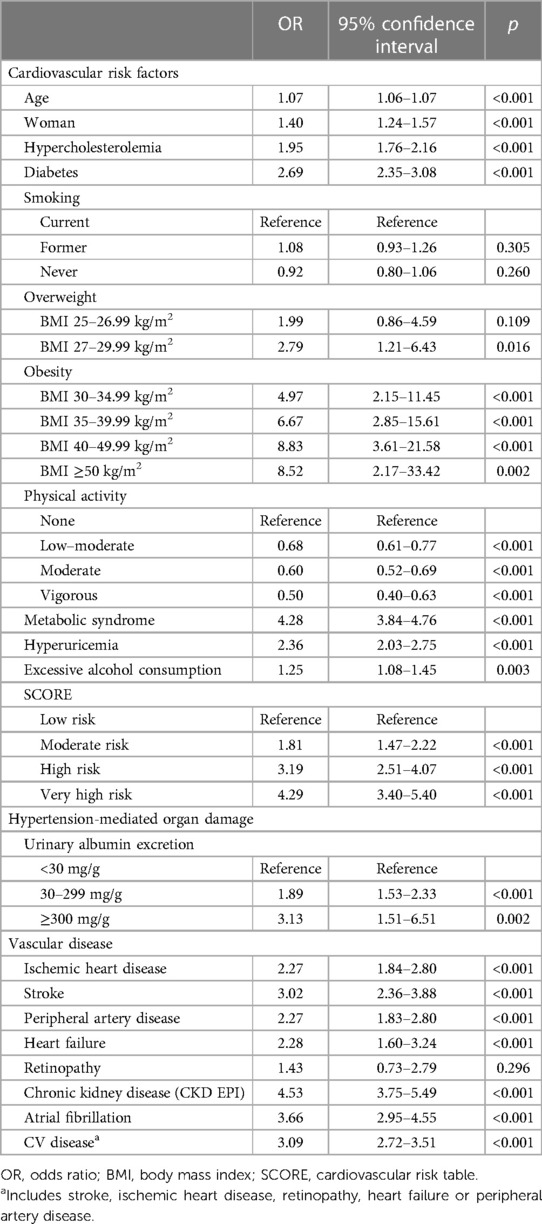
Table 3. Risk of hypertension according to the association of cardiovascular risk factors, hypertension-mediated organ damage and cardiovascular disease.
Antihypertensive treatment in the whole hypertensive population and according to gender is shown in Table 4. Overall, 58.8% of patients followed the recommendations about diet and physical activity. For different reasons 6.1% of patients did not take any drug, 38.8% were taking one prescribed antihypertensive drug, 35.5% two antihypertensive drugs and the remaining 19.6% three or more prescribed drugs. The most commonly prescribed antihypertensive agents were renin-angiotensin-system (RAS) blockers 81% (ACEi 38.5%, ARB 42.5%) followed by diuretics 45.3%, particularly thiazide or thiazide-like diuretics. Diuretics were taken more frequently by women (41.6% vs. 49.0%: p < 0.001), whereas ACEi (41.8% vs. 35.1%; p < 0.001) and alpha blockers (4.8% vs. 1.4%; p < 0.001) were more frequent in men. Treatment with statins was higher in patients with hypertension compared with those without hypertension (76.7% vs. 56.6%, p < 0.001).
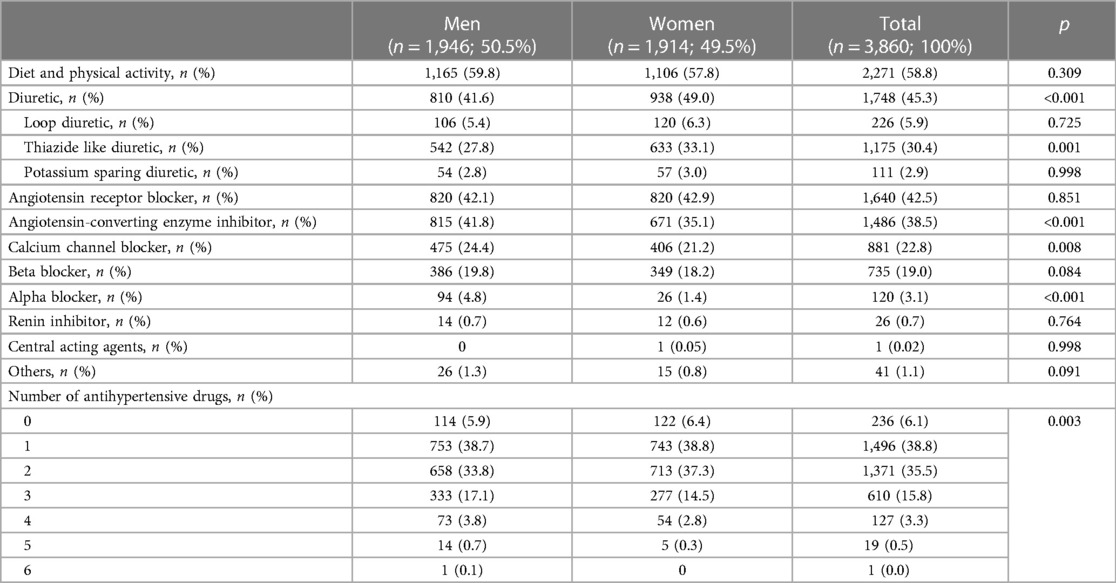
Table 4. Antihypertensive treatment in patients with hypertension.
Overall, 58.3% of hypertensive patients achieved recommended BP targets. There was a trend towards a higher BP control among women than men (61.6% vs. 57.8%; p = 0.036). According to the binary logistic regression model, the variables which were likely to associate independently with BP control were male/female gender, age, diabetes, obesity, the metabolic syndrome, current smoking, urinary albumin excretion (30–299 mg/g), pulse pressure >60 mmHg (≥65 years), any HMOD, retinopathy, antihypertensive treatment and number of antihypertensive drugs (Table 5). Figure 1 shows the variables resulting from the final model. The strongest independent positive association with BP control was observed in relation to the number of antihypertensive drugs (OR: 1.10; p < 0.041), where the higher the number of drugs the better BP control, and with older age (OR: 1.06; p < 0.001). A negative relationship with BP control was found with diabetes, obesity, the metabolic syndrome, urinary albumin excretion, high pulse pressure, and lack of antihypertensive treatment.
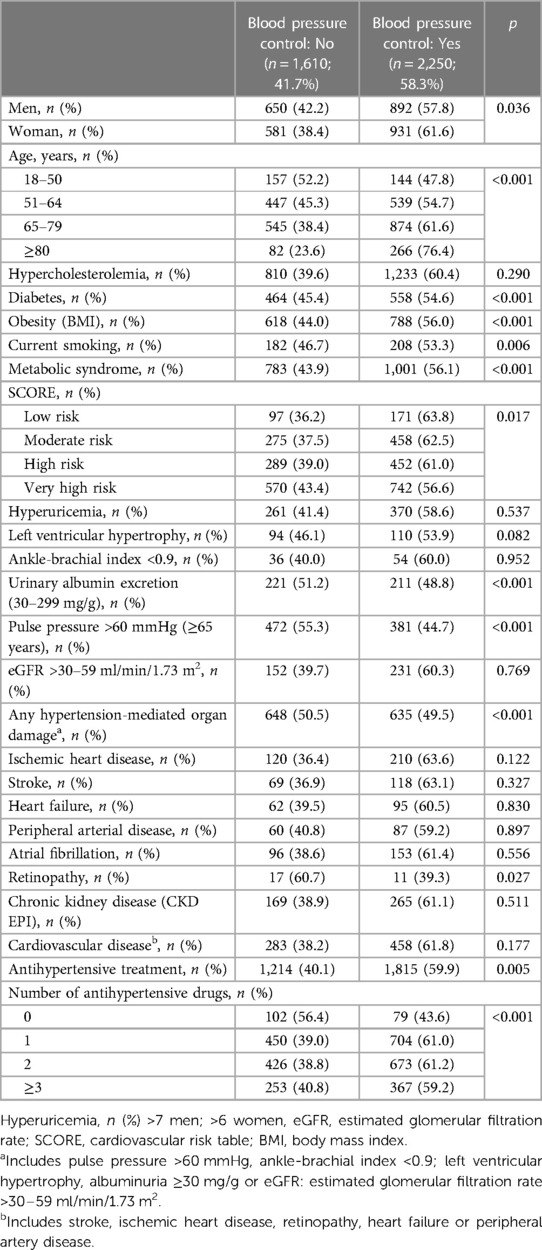
Table 5. Blood pressure control in relation to the association of cardiovascular risk factors, hypertension-mediated organ damage, clinical cardiovascular disease, and antihypertensive treatment.
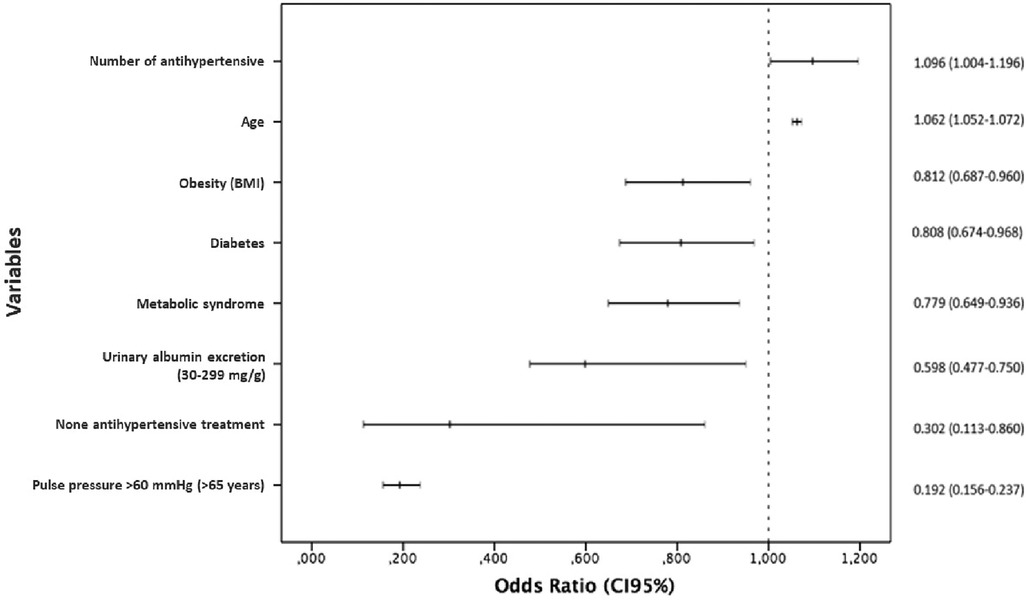
Figure 1. Variables associated to blood pressure control in hypertensive patients*. *Multivariate logistic regression, stepwise backward method (LR). CI, Confidence interval; Number of antihypertensive drugs; Age; Obesity; Diabetes; Metabolic syndrome; Urinary albumin excretion (30–299 mg/g); None antihypertensive treatment; Pulse pressure >60 mmHg (≥65 years).
This study performed in a wide sample of patients recruited by general practitioners in Spain showed that approximately half of patients attended in primary care setting had hypertension. Patients with hypertension had a worse clinical profile than non-hypertensive patients, with more associated CVRF, HMOD and clinical CVD. Although the majority of this patients were treated with combinations of antihypertensive drugs, approximately four out of ten patients did not achieve the recommended BP goals.
The IBERICAN study shows a real map of the burden of CVRF and CVD in daily clinical practice in primary care centers in Spain. In the IBERICAN cohort, 48% of patients had hypertension. This frequency was higher than that reported in population-based surveys (30%–35%) (4, 5, 9, 10, 22). However, it should be noted that IBERICAN was a clinical-based study of patients seen in primary care setting. IBERICAN is a very useful study that will help to increase knowledge about CV risk in primary care settings (23) and these data clearly indicate that hypertension is the major health care problem that should be ruled out in every patient without a previous history of hypertension attended by general practitioners (4).
As expected, patients with hypertension had more associated CVRF, HMOD and clinical CVD, confirming previous results by other authors (9–14). The risk of having hypertension is associated with other CVRF as diabetes, obesity, and the metabolic syndrome, that increased the risk, or intensity of physical activity, that reduced it. Our results confirm the impact of excess weight, salt intake and low physical activity that cause close of 50% of the hypertension cases (7). This relationship highlighted the importance to a correct management of all CVRF, including promotion of a healthy lifestyle, and not only hypertension, to reduce the global cardiovascular risk of the patients (24, 25). Our results also showed an important relationship of hypertension risk development with epidemiological data as male gender, age over 65 years, be pensioned, living in a rural area, lower educational level, and low income. These results completed the role described by other authors about the social determinants in the development of hypertension and BP control (12, 26).
Approximately 60% of hypertensive patients of the IBERICAN cohort achieved the BP targets recommended by the guidelines. With regard to treatment, 6.1% of patients did not take any drug, 38.8% were taking one prescribed antihypertensive drug, 35% two antihypertensive drugs and 20% three or more prescribed drugs. Our results show the trends in Spain, where we observed an increase in BP control from 36% in 2002 to 46% in 2010 among hypertensive patients treated by primary care physicians (27), mainly related with a progressive higher use of combination therapy (from 44% to 64%) (27), similarly to other studies describing a direct relationship between the use of combination treatment and improvement of BP control (60%–65%) (13, 28). Even considering a great variability among different countries (4), BP control rates have remained stable in the last decade in the world (30%–50%), despite the improvement in detection, awareness, treatment and control of BP in high-income countries along the 80s and 90s (5). The challenge of improving BP control worldwide may be overcome, and our results clearly indicate how other associated CVRF and the increase in the use of antihypertensive combination strategies could improve this control, addressing the main clinical problems of therapeutic inertia (29) and adherence to chronic cardiovascular treatments (30).
Interestingly, in contrast with previous reports (31) our results show that patients with better BP control had more frequently diabetes, obesity, hypercholesterolemia, current smoking, LOMH and CVD compared to uncontrolled patients, exhibiting a higher CV risk. A probable explanation is that the identification of these conditions by primary care physicians let them to a better stratification of the patient global CV risk and intensify pharmacological treatment. It would be very interesting what will be the effect of this situation in the prognosis of patients of our cohort when we can analyze the cardiovascular risk in the follow up along the next years.
This study has some limitations. The participation of primary care physicians was volunteer and not random, which does not allow to strictly generalize our results to the population daily attended in primary care. Besides, the number of included patients per physician and year was very low, what may be a potential major bias in the interpretation of the results. It may be speculated that only physicians most interested in CVD were those participating as researchers. This could explain the excellent reported data concerning antihypertensive drug prescription and BP control, what may not be extrapolated to real clinical practice.
Our aim was to analyze the relationship between the CVRF with the prevalence of hypertension and BP control with other variables, and the sample recruited let us to make these analyses with a high statistical power. In addition, when comparing frequencies, the lack of control group only permits to perform indirect comparisons with the results obtained in other studies. In fact, the results of this study probably represent the best and more actually scenario in hypertension control in the population cared by general practitioners of the Public Health System in Spain, and perhaps the situation, specially in the BP control, is worst in real world. In any case, this bias does not invalidate the observed association among hypertension and other CVRF, HMOD, and CVD in our study.
In conclusion, patients with hypertension are very common in the primary care setting, exhibiting a worse clinical profile that deserves a more aggressive and comprehensive approach to actually reduce CV burden. Despite that four out of ten patients do not achieve recommended BP goals many of them are still treated in monotherapy. It is necessary to develop strategies to implement a more appropriate and intense treatment in hypertensive patients through the use of combination therapy, preferably in a single pill fixed-dose combination to improve medication adherence, long-term persistence, and CV morbidity and mortality.
The original contributions presented in the study are included in the article/Supplementary Material, further inquiries can be directed to the corresponding author.
The studies involving humans were approved by the Clinical Research Ethics Committee of the Hospital Clínico San Carlos in Madrid on 21 February 2013 (C.P. IBERICAN-C.I. 13/047-E) and is registered at https://clinicaltrials.gov with the number NCT02261441. The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
MP-D: Conceptualization, Funding acquisition, Methodology, Supervision, Validation, Visualization, Writing – original draft, Writing – review & editing. VP-C: Conceptualization, Funding acquisition, Methodology, Supervision, Validation, Visualization, Writing – original draft, Writing – review & editing. RM-P: Funding acquisition, Supervision, Validation, Visualization, Writing – review & editing. CE-C: Conceptualization, Methodology, Supervision, Validation, Visualization, Writing – original draft, Writing – review & editing. VM-S: Supervision, Validation, Visualization, Writing – review & editing. AC: Supervision, Validation, Visualization, Writing – review & editing. AB-G: Supervision, Validation, Visualization, Writing – review & editing. SV-Z: Supervision, Validation, Visualization, Writing – review & editing. JP-G: Funding acquisition, Supervision, Validation, Visualization, Writing – review & editing. AS-F: Methodology, Supervision, Validation, Visualization, Writing – review & editing. LG-M: Funding acquisition, Supervision, Validation, Visualization, Writing – review & editing. ÁH-A: Supervision, Validation, Visualization, Writing – review & editing. SC-S: Conceptualization, Funding acquisition, Methodology, Project administration, Supervision, Validation, Visualization, Writing – original draft, Writing – review & editing.
The author(s) declare financial support was received for the research, authorship, and/or publication of this article.
The IBERICAN study is financed by the SEMERGEN Foundation with its own funds.
To the SEMERGEN Foundation for financing the study. To the researchers who have actively participated in the recruitment of patients. We also want to thank all patients for their participation in the study.
The SEMERGEN Foundation has received grants from Astra Zeneca and Menarini, but none of these grants were dedicated to financing any article of the IBERICAN study, including this article.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fcvm.2023.1295174/full#supplementary-material
1. Brouwers S, Sudano I, Kokubo Y, Sulaica EM. Arterial hypertension. Lancet. (2021) 398:249–61. doi: 10.1016/S0140-6736(21)00221-X
2. Blood Pressure Lowering Treatment Trialists’ Collaboration. Pharmacological blood pressure lowering for primary and secondary prevention of cardiovascular disease across different levels of blood pressure: an individual participant-level data meta-analysis. Lancet. (2021) 397:1625–36. doi: 10.1016/S0140-6736(21)00590-0
3. Blood Pressure Lowering Treatment Trialists’ Collaboration. Age-stratified and blood-pressure-stratified effects of blood-pressure-lowering pharmacotherapy for the prevention of cardiovascular disease and death: an individual participant-level data meta-analysis. Lancet. (2021) 398:1053–64. doi: 10.1016/S0140-6736(21)01921-8
4. NCD Risk Factor Collaboration (NCD-RisC). Worldwide trends in hypertension prevalence and progress in treatment and control from 1990 to 2019: a pooled analysis of 1201 population-representative studies with 104 million participants. Lancet. (2021) 398:957–80. doi: 10.1016/S0140-6736(21)01330-1
5. NCD Risk Factor Collaboration (NCD-RisC). Long-term and recent trends in hypertension awareness, treatment, and control in 12 high-income countries: an analysis of 123 nationally representative surveys. Lancet. (2019) 394(10199):639–51. doi: 10.1016/S0140-6736(19)31145-6
6. Cinza Sanjurjo S, Llisterri Caro JL, Barquilla García A, Polo García J, Velilla Zancada S, Rodríguez Roca GC, et al. Description of the sample, design and methods of the study for the identification of the spanish population at cardiovascular and renal risk (IBERICAN). Semergen. (2020) 46(1):4–15. doi: 10.1016/j.semerg.2019.10.006
7. Banegas JR, Gijón-Conde T. Hypertension: the most common chronic health problem in Spain. A call to action. Hipertens Riesgo Vasc. (2022) 39(3):121–7. doi: 10.1016/j.hipert.2022.03.004
8. Deaths according to the cause of death in Spain. Statistics National Institute (Instituto Nacional de Estadística INE) (2022). Available at: https://www.ine.es/dyngs/INEbase/es/operacion.htm?c=Estadistica_C&cid=1254736176780&menu=ultiDatos&idp=1254735573175.
9. Banegas JR, Graciani A, De la Cruz JJ, León L, Guallar P, Coca A, et al. Achievement of cardiometabolic goals in aware hypertensive patients in Spain: a nationwide population-based study. Hypertension. (2012) 60:898–905. doi: 10.1161/HYPERTENSIONAHA.112.193078
10. Gijón-Conde T, Sánchez-Martínez M, Graciani A, Cruz JJ, López-García E, Ortolá R, et al. Impact of the European and American guidelines on hypertension prevalence, treatment, and cardiometabolic goals. J Hypertens. (2019) 37:1393–400. doi: 10.1097/HJH.0000000000002065
11. Barrios V, Escobar C, Alonso-Moreno FJ, Prieto MA, Pallares V, Rodríguez-Roca G, et al. Evolution of clinical profile, treatment and blood pressure control in treated hypertensive patients according to the sex from 2002 to 2010 in Spain. J Hypertens. (2015) 33(5):1098–107. doi: 10.1097/HJH.0000000000000502
12. Corbatón-Anchuelo A, Martínez-Larrad MT, Del Prado-González N, Fernández-Pérez C, Gabriel R, Serrano-Ríos M. Prevalence, treatment, and associated factors of hypertension in Spain: a comparative study between populations. Int J Hypertens. (2018) 2018:4851512. doi: 10.1155/2018/4851512
13. Gijón-Conde T, Rodilla E, Molinero A, Alvargonzález M, Ruilope LM. Awareness, treatment and control of blood pressure according to place of recruitment and sex in the may measure month 2018 survey in Spain. Hipertens Riesgo Vasc. (2021) 38(1):4–12. doi: 10.1016/j.hipert.2020.07.003
14. Molinero A, Calvo E, Beaney T, Day E, Prats-Mas R, Fornos JA, et al. May measurement month 2019: an analysis of blood pressure screening results from Spain. Eur Heart J Suppl. (2021) 23(Suppl B):B138–40. doi: 10.1093/eurheartj/suab060
15. Egan BM, Sutherland SE, Rakotz M, Yang J, Hanlin RB, Davis RA, et al. Improving hypertension control in primary care with the measure accurately, act rapidly, and partner with patients’ protocol. Hypertension. (2018) 72(6):1320–7. doi: 10.1161/HYPERTENSIONAHA.118.11558
16. Llisterri-Caro JL, Cinza-Sanjurjo S, Martín-Sánchez V, Rodríguez-Roca GC, Micó-Pérez RM, Segura-Fragoso A, et al. Prevalence of chronic heart failure, associated factors, and therapeutic management in primary care patients in Spain, IBERICAN study. J Clin Med. (2021) 10(18):4036. doi: 10.3390/jcm10184036
17. Cinza-Sanjurjo S, Micó-Pérez RM, Velilla-Zancada S, Prieto-Díaz MA, Rodríguez-Roca GC, Barquilla García A, et al. Factors associated with cardiovascular risk and cardiovascular and renal disease in the IBERICAN study: final results. Semergen. (2020) 46(6):368–78. doi: 10.1016/j.semerg.2020.06.027
18. Perduzzi P, Concato J, Kemper E, Holford TR, Feinstein AR. A simulation study of the number of events per variable in logistic regression analysis. J Clin Epidemiol. (1996) 49:1373–9. doi: 10.1016/S0895-4356(96)00236-3
19. Núñez E, Steyerberg EW, Núñez J. Strategies for the elaboration of regression statistics models. Rev Esp Cardiol. (2011) 64(6):501–7. doi: 10.1016/j.recesp.2011.01.019
20. Mancia G, Fagard R, Narkiewicz K, Redon J, Zanchetti A, Böhm M, et al. 2013 ESH/ESC guidelines for the management of arterial hypertension the task force for the management of arterial hypertension of the European society of hypertension (ESH) and of the European society of cardiology (ESC). Eur Heart J. (2013) 34:2159–219. doi: 10.1093/eurheartj/eht151
21. Mancia G, Kreutz R, Brunström M, Burnier M, Grassi G, Januszewicz A, et al. 2023 ESH guidelines for the management of arterial hypertension the task force for the management of arterial hypertension of the European society of hypertension endorsed by the international society of hypertension (ISH) and the European renal association (ERA). J Hypertens. (2023) 41:51–4. doi: 10.1097/HJH.0000000000003480
22. Ruiz-García A, Arranz-Martínez E, García-Álvarez JC, Morales-Cobos LE, García-Fernández ME, de la Peña-Antón N, et al. Population and methodology of the SIMETAP study: prevalence of cardiovascular risk factors, cardiovascular diseases, and related metabolic diseases. Clin Invest Arterioscl. (2018) 30:197–208. doi: 10.1016/j.arteri.2018.04.006
23. Banegas JR. The IBERICAN project. Progressing in the knowledge of cardiovascular risk in primary care in Spain. Semergen. (2020) 46(1):1–3. doi: 10.1016/j.semerg.2019.12.001
24. Visseren FLJ, Mach F, Smulders YM, Carballo D, Koskinas KC, Bäck M, et al. 2021 ESC guidelines on cardiovascular disease prevention in clinical practice. Eur Heart J. (2021) 42(34):3227–337. doi: 10.1093/eurheartj/ehab484
25. Williams B, Mancia G, Spiering W, Rosei EA, Azizi M, Burnier M, et al. 2018 ESC/ESH guidelines for the management of arterial hypertension: the task force for the management of arterial hypertension of the European society of cardiology and the European society of hypertension. J Hypertens. (2018) 36:1953–2041. doi: 10.1097/HJH.0000000000001940
26. Nakagomi A, Yasufuku Y, Ueno T, Kondo K. Social determinants of hypertension in high-income countries: a narrative literature review and future directions. Hypertens Res. (2022) 45(10):1575–81. doi: 10.1038/s41440-022-00972-7
27. Llisterri JL, Rodriguez-Roca GC, Escobar C, Alonso-Moreno FJ, Prieto MA, Barrios V, et al. Treatment and blood pressure control in Spain during 2002–2010. J Hypertens. (2012) 30(12):2425–31. doi: 10.1097/HJH.0b013e3283592583
28. Rodilla E, Molinero A, Gijón-Conde T, Tous S, Fornós JA, Mera I, et al. May measurement month 2018: an analysis of blood pressure screening results from Spain. Eur Heart J Suppl. (2020) 22(Suppl H):H119–21. doi: 10.1093/eurheartj/suaa044
29. Escobar C, Barrios V, Alonso-Moreno FJ, Prieto MA, Valls F, Calderon A, et al. Evolution of therapy inertia in primary care setting in Spain during 2002–2010. J Hypertens. (2014) 32(5):1138–45. doi: 10.1097/HJH.0000000000000118
30. Vrijens B, Antoniou S, Burnier M, de la Sierra A, Volpe M. Current situation of medication adherence in hypertension. Front Pharmacol. (2017) 8:100. doi: 10.3389/fphar.2017.00100
Keywords: blood pressure, combined therapy, hypertension, primary care, cardiovascular risk
Citation: Prieto-Díaz MA, Pallares-Carratala V, Manuel Micó-Pérez R, Escobar-Cervantes C, Martín-Sanchez V, Coca A, Barquilla-García A, Velilla-Zancada SM, Polo-García J, Segura-Fragoso A, Ginel-Mendoza L, Hermida-Ameijerias Á, Cinza-Sanjurjo S and the Investigators of the IBERICAN study and of the Spanish Society of Primary Care Physicians SEMERGEN Foundation (2023) Clinical characteristics, treatment, and blood pressure control in patients with hypertension seen by primary care physicians in Spain: the IBERICAN study. Front. Cardiovasc. Med. 10:1295174. doi: 10.3389/fcvm.2023.1295174
Received: 15 September 2023; Accepted: 29 November 2023;
Published: 20 December 2023.
Edited by:
Thomas Kahan, Karolinska Institutet (KI), SwedenReviewed by:
Weimar Kunz Sebba Barroso, Universidade Federal de Goiás, Brazil© 2023 Prieto-Díaz, Pallares-Carratala, Manuel Micó-Pérez, Escobar-Cervantes, Martín-Sanchez, Coca, Barquilla-García, Velilla-Zancada, Polo-García, Segura-Fragoso, Ginel-Mendoza, Hermida-Ameijerias, Cinza-Sanjurjo and the Investigators of the IBERICAN study and of the Spanish Society of Primary Care Physicians SEMERGEN Foundation. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Vicente Pallares-Carratala cGFsbGFyZXMudmljQGdtYWlsLmNvbQ==
†ORCID Miguel A. Prieto-Díaz orcid.org/0000-0001-8079-6624 Vicente Pallares-Carratala orcid.org/0000-0002-2985-6078 Rafael Manuel Micó-Pérez orcid.org/0000-0002-2957-3182 Carlos Escobar-Cervantes orcid.org/0000-0001-5584-4735 Vicente Martín-Sanchez orcid.org/0000-0003-0552-2804 Antonio Coca orcid.org/0000-0001-6968-3266 Alfonso Barquilla-García orcid.org/0000-0001-7074-4951 Sonsoles M. Velilla-Zancada orcid.org/0000-0002-3695-5541 José Polo-García orcid.org/000-0002-3655-7180 Antonio Segura-Fragoso orcid.org/0000-0003-4884-2242 Leovigildo Ginel-Mendoza orcid.org/0000-0001-8350-3524 Álvaro Hermida-Ameijerias orcid.org/0000-0003-3757-262X Sergio Cinza-Sanjurjo orcid.org/0000-0002-4486-2820
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.