
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Cardiovasc. Med. , 20 November 2023
Sec. General Cardiovascular Medicine
Volume 10 - 2023 | https://doi.org/10.3389/fcvm.2023.1282018
 Iván J. Núñez-Gil1,2*†
Iván J. Núñez-Gil1,2*† Francesco Santoro3,†
Francesco Santoro3,† Ravi Vazirani1
Ravi Vazirani1 Giuseppina Novo4
Giuseppina Novo4 Emilia Blanco-Ponce5
Emilia Blanco-Ponce5 Luca Arcari6
Luca Arcari6 Aitor Uribarri7,8,9Luca Cacciotti6
Aitor Uribarri7,8,9Luca Cacciotti6 Federico Guerra10Jorge Salamanca11
Federico Guerra10Jorge Salamanca11 Beatrice Musumeci12
Beatrice Musumeci12 Oscar Vedia1Enrica Mariano13Clara Fernández-Cordón14Pasquale Caldarola15
Oscar Vedia1Enrica Mariano13Clara Fernández-Cordón14Pasquale Caldarola15 Roberta Montisci16Natale Daniele Brunetti3Ibrahim El-Battrawy17,18
Roberta Montisci16Natale Daniele Brunetti3Ibrahim El-Battrawy17,18 Mohammad Abumayyaleh19Ibrahim Akin19Ingo Eitel20,21Thomas Stiermaier20,21
Mohammad Abumayyaleh19Ibrahim Akin19Ingo Eitel20,21Thomas Stiermaier20,21
Aims: To assess the influence of tobacco on acute and long-term outcomes in Takotsubo syndrome (TTS).
Methods: Patients with TTS from the international multicenter German Italian Spanish Takotsubo registry (GEIST) were analyzed. Comparisons between groups were performed within the overall cohort, and an adjusted analysis with 1:1 propensity score matching was conducted.
Results: Out of 3,152 patients with TTS, 534 (17%) were current smokers. Smoker TTS patients were younger (63 ± 11 vs. 72 ± 11 years, p < 0.001), less frequently women (78% vs. 90%, p < 0.001), and had a lower prevalence of hypertension (59% vs. 69%, p < 0.01) and diabetes mellitus (16% vs. 20%, p = 0.04), but had a higher prevalence of pulmonary (21% vs. 15%, p < 0.01) and/or psychiatric diseases (17% vs. 12%, p < 0.01). On multivariable analysis, age less than 65 years [OR 3.85, 95% CI (2.86–5)], male gender [OR 2.52, 95% CI (1.75–3.64)], history of pulmonary disease [OR 2.56, 95% CI (1.81–3.61)], coronary artery disease [OR 2.35, 95% CI (1.60–3.46)], and non-apical ballooning form [OR 1.47, 95% CI (1.02–2.13)] were associated with smoking status. Propensity score matching (PSM) 1:1 yielded 329 patients from each group. Smokers had a similar rate of in-hospital complications but longer in-hospital stays (10 vs. 9 days, p = 0.01). During long-term follow-up, there were no differences in mortality rates between smokers and non-smokers (5.6% vs. 6.9% yearly in the overall, p = 0.02, and 6.6%, vs. 7.2% yearly in the matched cohort, p = 0.97).
Conclusions: Our findings suggest that smoking may influence the clinical presentation and course of TTS with longer in-hospital stays, but does not independently impact mortality.
Takotsubo syndrome (TTS), also known as stress-induced cardiomyopathy or broken heart syndrome, is a rare but potentially life-threatening condition characterized by acute and reversible ventricular dysfunction (1–4). While it clinically can mimic an acute coronary syndrome (ACS), the etiology of TTS remains unknown and is frequently linked with stressful situations (mainly negative but also positive).
Similar to ACS, recent research has identified several differential potential risk factors including different metabolomics (5).
On the other hand, tobacco smoking habit has been associated with the development of several conditions and increased mortality, contributing to more than 7 million deaths every year and being a main cause of preventable diseases worldwide (6). Global statistics indicate that there are approximately 1.1 billion active smokers and that 80% of them live in low- and middle-income countries (6). However, the potential influence of smoking on TTS is not fully understood due to limited available data (7). Given the potential risks associated with smoking and cardiovascular diseases, and the fact that women with TTS have been deemed to report a higher prevalence of lifetime smoking than healthy women volunteers (8), the present study aimed to undertake an analysis of the impact of smoking on patients with TTS included in the large, multicentric and international German Italian Spanish Takotsubo (GEIST) registry, to provide a more comprehensive picture of disease characteristics and outcomes in this subset of patients.
This study included data from 3,152 consecutive patients enrolled in the GEIST registry [NCT04361994] as of November 2022. As previously reported, the inclusion of patients in the registry was performed by fulfilling the following TTS diagnostic criteria: (1) transient segmental wall motion abnormalities of the left or right ventricle, extending beyond a single epicardial vascular distribution; (2) absence of any potential culprit coronary artery disease; (3) new and reversible electrocardiography abnormalities; (4) elevated cardiac troponin levels; and (5) recovery of ventricular systolic function at follow-up unless previously deceased (9).
Coronary artery disease was defined as the presence of coronary calcifications, atherosclerosis, plaques, and/or stenosis, with stenosis >50% of the lumen diameter in arteries with a diameter amenable to percutaneous intervention in previous admissions (9). TTS secondary forms, as previously defined (10), were considered when a physical trigger or emotional plus physical triggers were present. Primary forms were those without triggers or with an isolated identifiable emotional trigger (10, 11). Right ventricular involvement was considered as such when any abnormality was demonstrated in the echocardiogram at that level and included in the clinical report. Left ventricular tract (LVOT) obstruction was considered when a ≥30 mmHg gradient was demonstrated in the echocardiogram or after an invasive direct measurement. Left ventricular thrombus was considered when a compatible image was discovered in any imaging technique. For the purposes of the present study, we provided a stepwise comparison between current smoker TTS patients (at the admission time) and non-smoker TTS patients within the study sample (Figure 1).
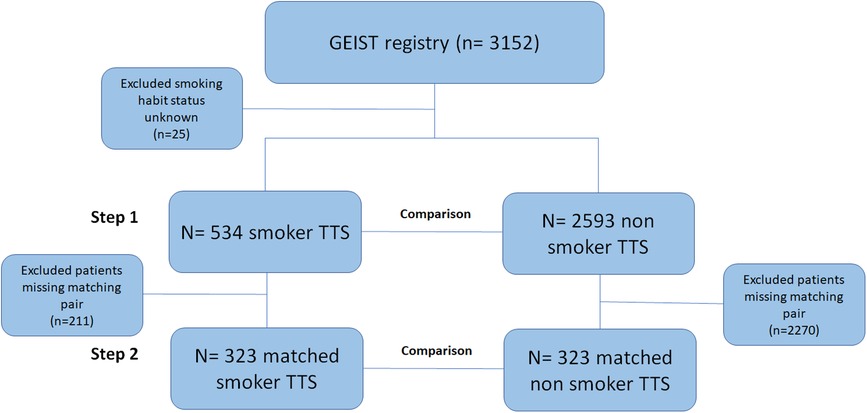
Figure 1. The study consisted of an analysis of the international multicenter GEIST registry. The diagram depicts the study design, for which comparisons were performed between smoker and non-smoker TTS patients both in the overall (step 1) and matched (step 2) cohorts. GEIST, German Italian Spanish Takotsubo; TTS, Takotsubo syndrome.
Initially (Step 1), the comparison was made for smoker and non-smoker patients within the overall population, after excluding those patients with current smoking habit status not disclosed or unknown (n = 25).
Afterward (Step 2), a propensity score matching (PSM) analysis was used to identify subgroups of smokers and non-smoker TTS patients with a 1:1 nearest neighbor matching. After univariate assessment, PSM variables included age, sex, hypertension, diabetes, malignancies, coronary artery disease, atrial fibrillation, and any pulmonary or psychiatric disease. Match tolerance was set at 0.02, without replacement. The matched cohort consisted of 329 pairs of TTS patients for which additional comparison was carried out.
Demographic and clinical characteristics as well as the presence and type of the preceding stressful trigger, ballooning patterns, in-hospital complications, and outcome were recorded at admission, as previously described (2, 9, 12). Recovery of left ventricular systolic function was documented 1–6 months after the acute event in all surviving patients. Long-term outcome was tested by outpatient visits, medical records, or phone interviews. All patients were managed in accordance with the Declaration of Helsinki and signed an informed consent for the processing of personal data for scientific research purposes. The primary outcome was all-cause fatality.
Categorical variables were compared using a Chi-square analysis or Fisher's exact test as appropriate. Continuous variables were presented as mean ± standard deviation. The Student's T-test for independent samples was used to compare continuous variables. Univariable and multivariable logistic regression analyses were used to calculate estimated ORs and 95% CIs for factors associated with smoking habits in patients with TTS. Collinearity was tested and dismissed considering variance inflation factors (VIF) as <5. Cox regression analysis models were carried out to assess factors independently associated with long-term mortality in the overall cohort. Standardized mean differences (SMD) were provided to depict effect size in the overall and the matched cohort after PSM. Kaplan–Meier curves and log-rank test were used to assess survival function at follow-up in both the overall and matched cohort. All data were analyzed with SPSS software version 24.0 (SPSS Inc., Chicago, Illinois, USA). A two-tailed p-value <0.05 was considered significant.
Baseline demographic, clinical characteristics, and outcomes within the overall and matched cohorts stratified by smoking habit are provided in Table 1 with events summarized in Figure 2. Of the 3,127 patients included in the present analysis from the GEIST registry, 534 (17%) were smokers.
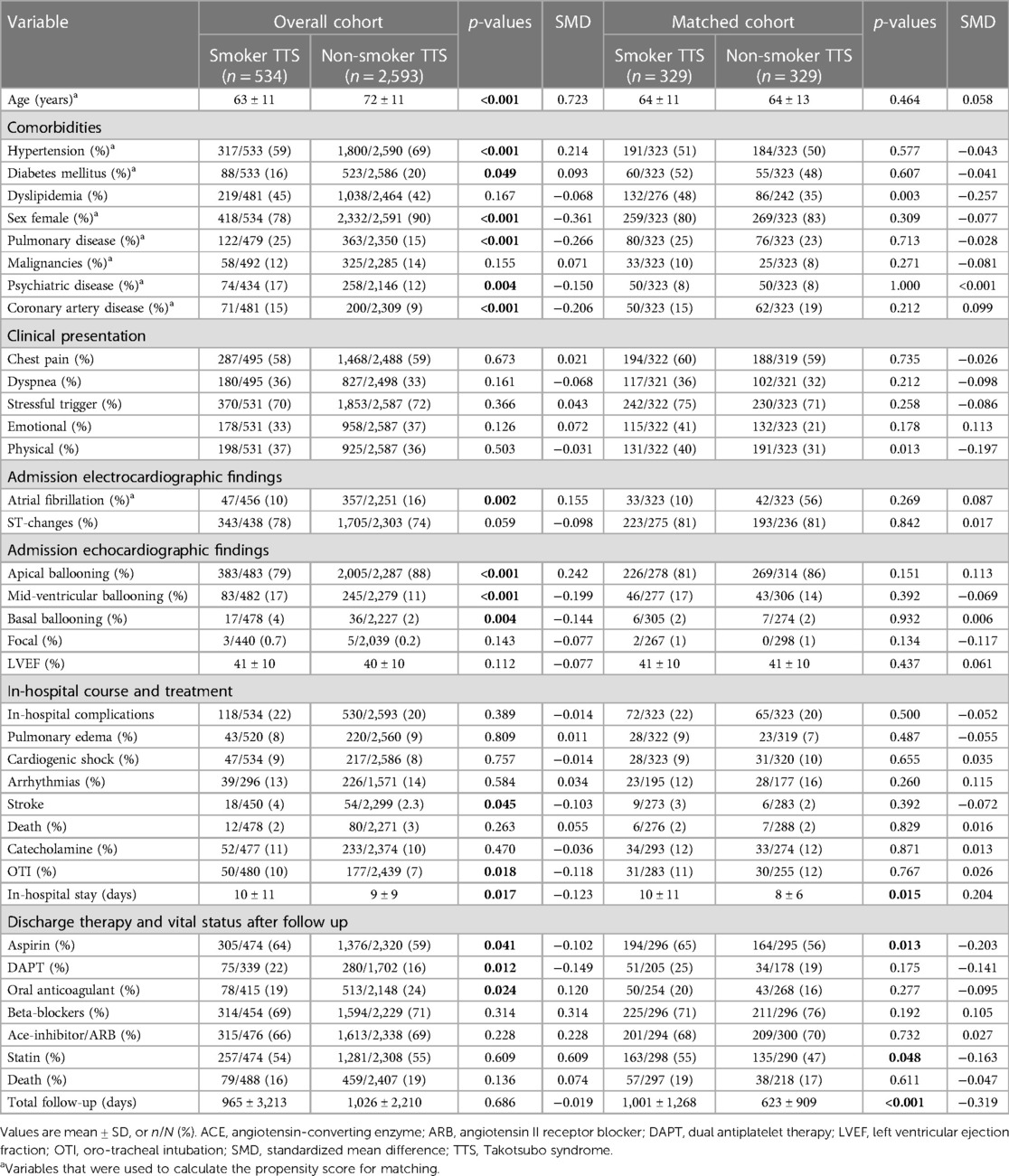
Table 1. Baseline characteristics of patients within the overall and matched cohorts.
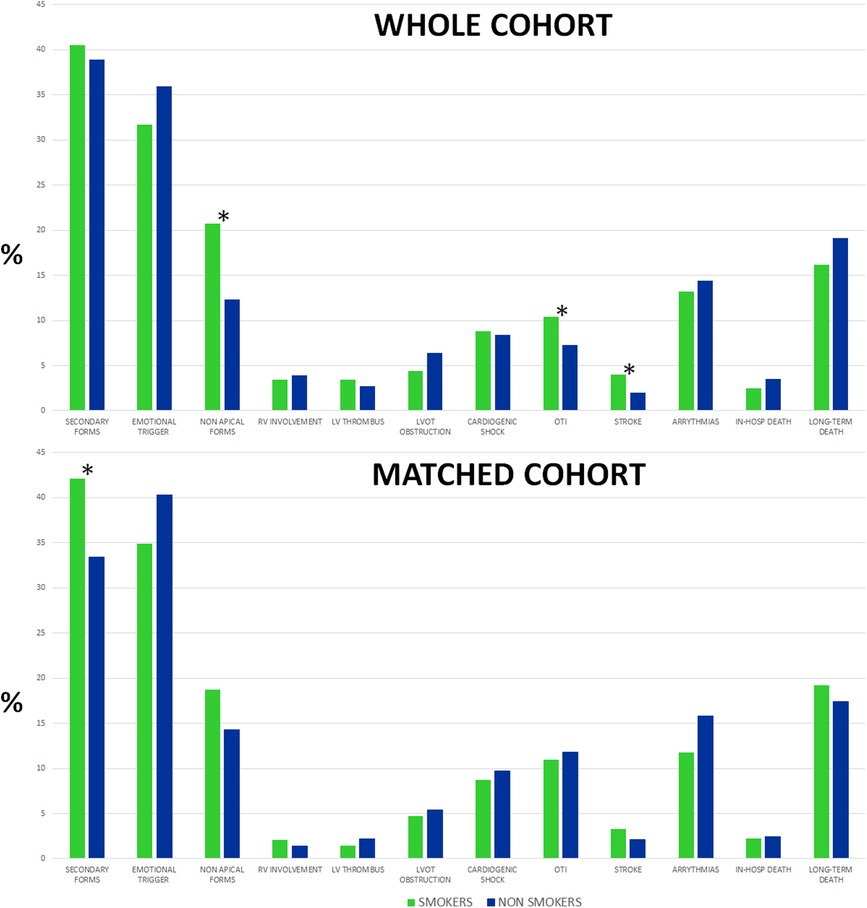
Figure 2. TTS presentation profile, in-hospital complications, and mortality were dichotomized by smoking habit in the overall population (top) and matched cohort (bottom). *Statistical differences of clinical features (p < 0.05). TTS, Takotsubo syndrome.
Smoker TTS patients were significantly younger (63 ± 11 vs. 72 ± 11 years, p < 0.001), less frequently women (78% vs. 90%, p < 0.001), and presented with significantly lower prevalence of some comorbid conditions (hypertension 59% vs. 69%, p < 0.001; diabetes mellitus 16% vs. 20%, p = 0.049 or admission atrial fibrillation 10% vs. 16%, p = 0.002) but had a higher prevalence of pulmonary diseases (21% vs. 15%, p < 0.001) or psychiatric diseases (17% vs. 12%, p = 0.004), as compared to non-smokers.
On clinical presentation, smoker TTS patients reported a similar dyspnea rate (36% vs. 33%, p = 0.16) and similar chest pain percentage compared to non-smokers (58% vs. 59%, p = 0.67), which was the main onset complaint. If any stressful trigger was frequent, it was present in a similar percentage between smokers and non-smokers (70% vs. 72%, p = 0.366) with a similar distribution of emotional and physical causes.
No significant differences were detected regarding ECG parameters but the ballooning pattern was dissimilar. Smoker TTS patients presented with a lower rate of apical ballooning (79% vs. 88%, p < 0.001) and a higher percentage of atypical forms, but overall onset left ventricular ejection fraction was similar (41 ± 10% vs. 40 ± 10%, p = 0.11).
On multivariable analysis (Table 2), older age [odds ratio (OR for ≥65 years) 0.26, 95% CI (0.20–0.35)], male sex [OR 2.52, 95% CI (1.75–3.64)], presence of pulmonary disease [OR 2.56, 95% CI (1.81–3.61)], coronary artery disease [OR 2.35, 95% CI (1.60–3.46)], and non-apical ballooning form [OR 1.47, 95% CI (1.02–2.13)] remained independently associated with the smoking status.
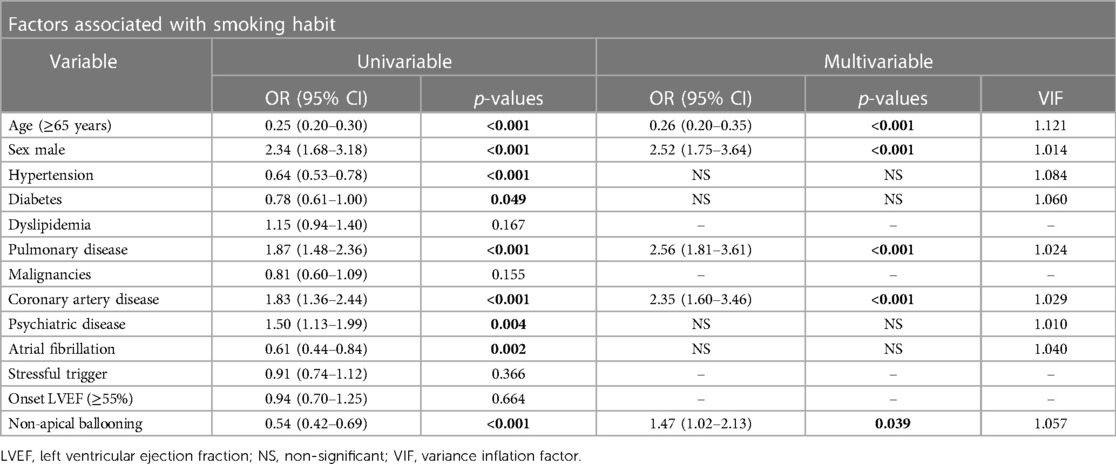
Table 2. Univariable and multivariable analysis for factors associated with smoking habit in the overall TTS cohort.
During the hospital course, in the overall cohort, smokers presented a comparable percentage of complications, except for a higher need for orotracheal intubation and stroke rate (Figure 2). Moreover, smoker TTS patients had longer lengths of hospital stays (10 vs. 9 days, p = 0.017) with similar in-hospital mortality (2% vs. 3%, p = 0.26). At discharge, smoker TTS patients received a more intense antiplatelet treatment.
After propensity score matching, smoker and non-smoker TTS patients presented no significant differences regarding in-hospital complications, as shown in Table 1 and Figure 2.
During long-term follow-up, mortality rates were 6.7% per patient-year (smokers 5.6% and non-smokers 6.9%, p = 0.02) in the overall cohort and 6.8% per patient-year (smokers 6.6%, non-smokers 7.2%, p = 0.97) in the matched cohort respectively.
Smoker TTS patients experienced similar in-hospital mortality rates both in the overall cohort and in the matched cohort (2% vs. 3% and 2% vs. 2%; p = 0.263 and p = 0.829, respectively). Assessing long-term mortality rate after the complete follow-up, smoker TTS presented numerically less mortality in the overall cohort but not in the matched cohort (16% vs. 19%, p = 0.14 and 19% vs. 17% p = 0.61, respectively). Kaplan-Meier actuarial survival curves with in-hospital and long-term mortality in the study cohorts are displayed in Figures 3, 4.
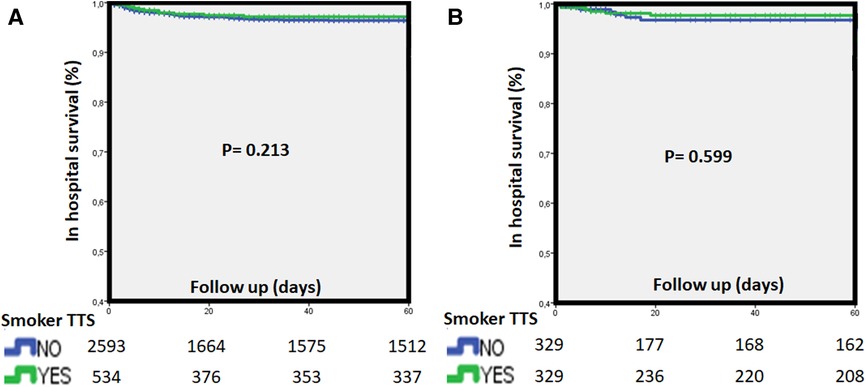
Figure 3. Kaplan-Meier survival curves for in-hospital death (A) dichotomized by smoking habit in the overall population (top) and matched cohort (B) TTS, Takotsubo syndrome.
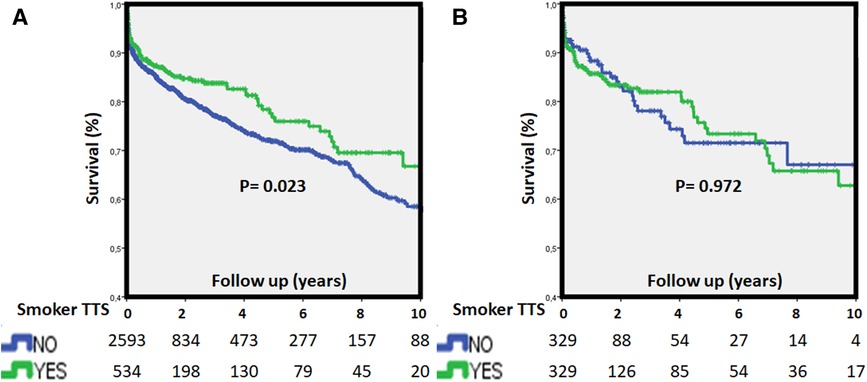
Figure 4. Kaplan-Meier survival curves for long-term (A) mortality stratified by smoking habit in the overall population (top) and matched cohort (B) long-term worse outcome in non-smokers was detected, albeit there was similar long-term mortality after adjustment. TTS, Takotsubo syndrome.
In the multivariable analysis (Table 3), smoker habit was not shown to be an independent predictor of in-hospital mortality or long-term mortality, in line with PSM analysis. In the present study, independent predictors of long-term mortality were age [hazard ratio (HR) 1.17 per 5 years increase; 95% CI (1.10–1.25); p < 0.001], male sex [HR 1.63; 95% CI (1.18–2.24); p = 0.003], diabetes [HR 1.60; 95% CI (1.24–2.05); p < 0.001], pulmonary disease [HR 1.36; 95% CI (1.02–1.82); p = 0.039], malignancies [HR 1.38; 95% CI (1.03–1.85); p = 0.029], absence of onset ST changes [HR 2.32; 95% CI (1.85–2.50); p < 0.001], secondary TTS forms [HR 2.40; 95% CI (1.89–3.05); p < 0.001], and LVEF at admission [HR 1.15 per 5 points decrease; 95% CI (1.09–1.22); p < 0.001].
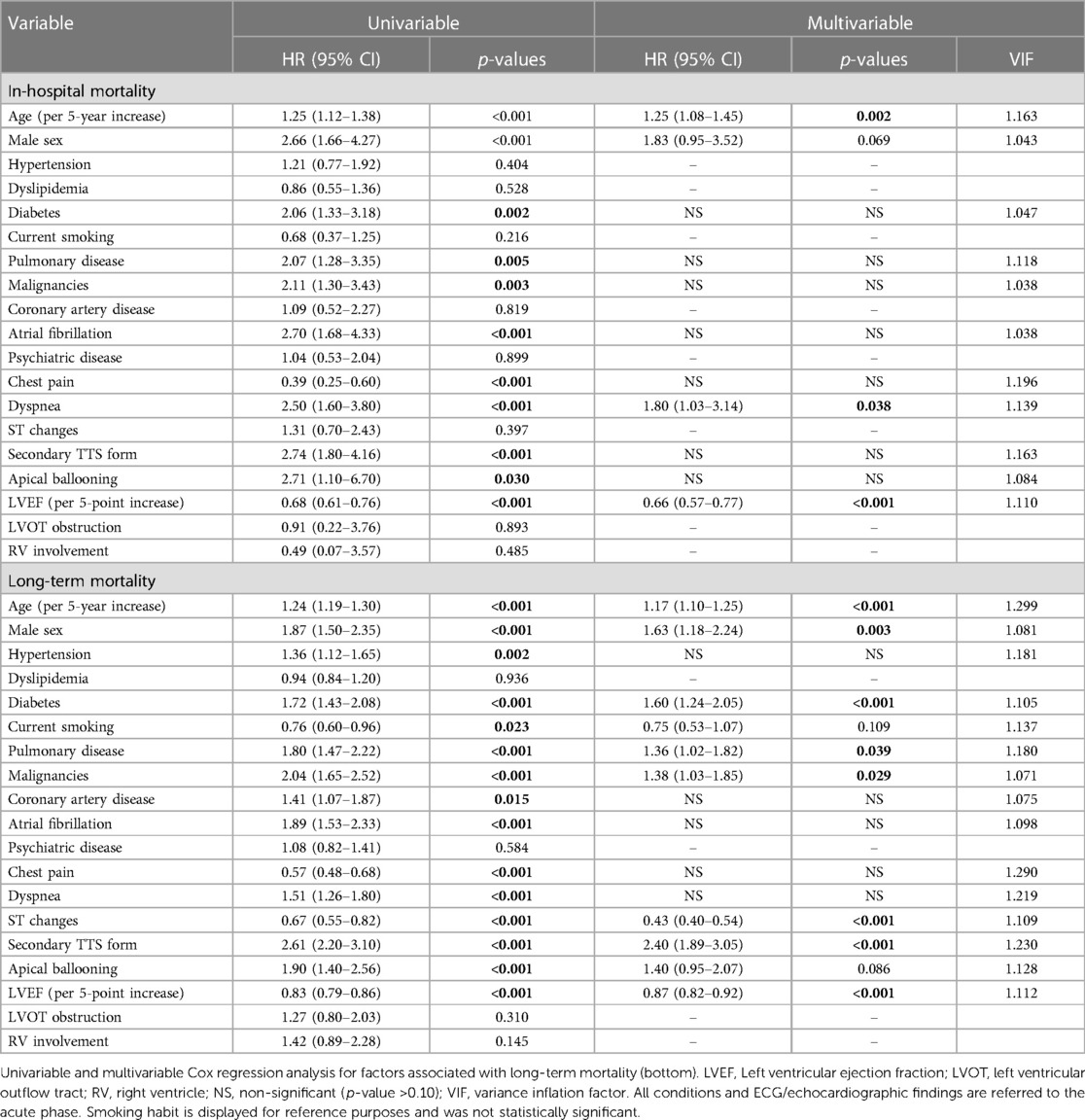
Table 3. Univariable and multivariable Cox regression analysis for factors associated with in-hospital mortality (top).
To the best of our knowledge, this research provides the largest study addressing the impact of tobacco on patients with TTS. The main findings from this international TTS registry are as follows: (1) Smoking habit has a prevalence of approximately 17% within the overall GEIST population and is independently associated with younger age, male sex, pulmonary and coronary disease, and a higher percentage of atypical TTS forms (non-apical); (2) In-hospital complications are pretty similar between smokers and non-smokers, although the length of hospital stay is higher in the smoking group in both the overall and matched cohorts; and (3) Long-term mortality after the acute phase is not significantly different between smokers and non-smokers in the matched cohort.
Tobacco use is a well-documented major risk factor for cardiovascular diseases (6) such as coronary artery disease, myocardial infarction, peripheral artery disease, and hypertension. It also increases the risk of other cardiovascular complications such as deep vein thrombosis, pulmonary embolism, and arrhythmias, including atrial fibrillation. Additionally, tobacco use significantly enhances the likelihood of ischemic stroke and malignancies among other diseases. Quitting smoking is crucial in reducing the risk of developing cardiovascular complications.
The pathophysiology of TTS is still unclear and likely depends on various factors, including different diseases with different causes and outcomes. It has been associated with several stressful triggers, interestingly even in positive situations (“happy heart syndrome”) (13). Recently, Li et al. identified four TTS patient clusters (14), with prognostic relevance, using latent class analysis in an administrative database. One of these clusters, where all patients had chronic obstructive pulmonary disease (COPD) and many were smokers (45.8%), had the highest in-hospital mortality (3.4%). In addition to the fact that COPD and smoking share pathophysiological mechanisms, tobacco use can also disrupt the balance of the autonomic nervous system and increase plasma catecholamine levels (15, 16). Some studies have suggested that sympathetic nervous system activation and higher plasma catecholamine levels are associated with poor prognosis in patients with TTS (17). In fact, TTS has been described to happen during severe dyspnea in COPD, a specific phenotype called “bronchogenic” TTS, with frequent atypical presentation (18). Moreover, patients with pulmonary disease are more prone to develop acute respiratory failure, which, together with TTS could worsen the prognosis (14). In our smoking cohort, despite being younger, we found a higher raw incidence of orotracheal intubation (OTI) and atypical forms reflecting this point.
Regarding the clinical presentation, Zaghol et al. described a single-center series of 264 patients with TTS showing that smokers had a different clinical profile, consistent with our study. Indeed, patients were younger (65.6 vs. 68.5 years), there were more men (16.2% vs. 6.8%), and they had a higher prevalence of pulmonary diseases-COPD (30.8% vs. 6.7%), as well as presented with dyspnea (50.0% vs. 38.1%), requiring more frequently mechanical ventilation, with more atypical forms, despite similar ejection fraction and wall motion abnormality distribution (7). Length of intensive unit and hospitalization stay were also higher in smokers (7), as in the present study.
Yet, in our series, once PSM was adjusted by comorbidities, including age, sex, or pulmonary disease, the differences in mechanical ventilation disappeared although a numerical trend of non-apical forms was maintained.
Redfors et al. reported a Swedish nationwide comparison among TTS, STEMI, and NSTEMI with SCAAR data. This study found smoking habit as an independent predictor of adverse clinical outcomes regarding acute heart failure (HR 2.11 95% CI 1.44–3.08), 30-day mortality (HR 2.29 95% CI 1.38–3.82), and 5-year mortality (HR 2.21 95% CI 1.64–2.98) (19). All models contained the following covariate set: age, sex, diabetes mellitus, insulin-treated diabetes mellitus, hypertension, hyperlipidemia, current smoker, previous smoker, prior myocardial infarction, prior percutaneous coronary intervention, concomitant coronary artery disease, and calendar year (19). Nonetheless, the main purpose of the study was a prognostic comparison among TTS, STEMI, and NSTEMI, and detailed information about other variables such as malignancies, pulmonary disease, TTS form, or triggers was not provided. Additionally, as recognized by the authors, their data did not allow them to assess the relative contribution of sex-related differences in the type of TTS stressor to the excess mortality observed in men (19). Our series, with a similar short-term mortality rate (3%) but a higher rate in the long term, included data from three countries, namely, Spain, Italy, and Germany. Thus, a country effect could not be discarded due to reporting differences, socioeconomic factors, rural–urban features, climate and other geographical factors, or regional healthcare policies.
Scarboro et al. performed a retrospective chart review of 210 TTS cases focusing on all-cause repeat hospital or emergency encounters. The authors remarked that standard medical therapy was not associated with protection and that tobacco smoking could lead to recurrent medical encounters with both cardiac and non-cardiac effects (20). In fact, in the same line, despite some prognostic TTS scores that have been previously published (GEIST, INTERTAK), a smoking habit is not included in any of them (2, 21).
However, while tobacco use increases oxidative stress, data in human cardiomyocytes modeling TTS also showed an increase in oxidative stress. It might be speculative that both TTS and concomitant smoking are relevant predictors of oxidative stress in cardiomyocytes and subsequently myocardial dysfunction (22).
Taken together, the data from the present study enforces the negative role of smoking in TTS, ruling out a “TTS smoking paradox” that suggests a positive influence on prognosis (23).
No cause-effect relationships can be established based on the present data due to the observational nature of the study, and further mechanistic investigations are needed. Smoking habit status during follow-up or the amount of tobacco consumed were not available and were not considered in the analysis. However, this study presents a large cohort with patient-level data on an infrequent disease managed in real-life settings, making it potentially the largest analysis on this topic to date.
Our findings suggest that while smoking may influence the clinical presentation and course of TTS, it does not independently contribute to worse outcomes in terms of mortality. Further research is needed to better understand the complex relationship between smoking and TTS, including potential underlying mechanisms and long-term effects.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
The studies involving humans were approved by Hospital Clínico San Carlos, Madrid, Spain (C.I. 11/349-E). The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
IN-G: Conceptualization, Data curation, Formal Analysis, Funding acquisition, Investigation, Methodology, Resources, Software, Supervision, Writing – original draft, Writing – review and editing. FS: Conceptualization, Supervision, Validation, Writing – original draft, Writing – review and editing. RV: Writing – review and editing. GN: Writing – review and editing. EB-P: Writing – review and editing. LA: Writing – review and editing. AU: Writing – review and editing. LC: Writing – review and editing. FG: Writing – review and editing. JS: Writing – review and editing. BM: Writing – review and editing. OV: Writing – review and editing. EM: Writing – review and editing. CF-C: Writing – review and editing. PC: Writing – review and editing. RM: Writing – review and editing. NB: Writing – review and editing. IB: Writing – review and editing. MA: Writing – review and editing. IA: Writing – review and editing. IE: Writing – review and editing. TS: Writing – review and editing.
The author(s) declare financial support was received for the research, authorship, and/or publication of this article.
FIC (Fundación Interhospitalaria para la Investigación en Cardiología) supported RETAKO.
All Takotsubo fighters and our patients.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The author(s) declared that they were an editorial board member of Frontiers, at the time of submission. This had no impact on the peer review process and the final decision.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Ghadri JR, Kato K, Cammann VL, Gili S, Jurisic S, Di Vece D, et al. Long-term prognosis of patients with Takotsubo syndrome. J Am Coll Cardiol. (2018) 72:874–82. doi: 10.1016/j.jacc.2018.06.016
2. Santoro F, Núñez Gil IJ, Stiermaier T, El-Battrawy I, Guerra F, Novo G, et al. Assessment of the German and Italian stress cardiomyopathy score for risk stratification for in-hospital complications in patients with Takotsubo syndrome. JAMA Cardiol. (2019) 4:892. doi: 10.1001/jamacardio.2019.2597
3. Lyon AR, Bossone E, Schneider B, Sechtem U, Citro R, Underwood SR, et al. Current state of knowledge on Takotsubo syndrome: a position statement from the taskforce on Takotsubo syndrome of the heart failure association of the European society of cardiology. Eur J Heart Fail. (2016) 18:8–27. doi: 10.1002/ejhf.424
4. Dias A, Núñez Gil IJ, Santoro F, Madias JE, Pelliccia F, Brunetti ND, et al. Takotsubo syndrome: state-of-the-art review by an expert panel – part 2. Cardiovasc Revascularization Med. (2019) 20:153–66. doi: 10.1016/j.carrev.2018.11.016
5. Nuñez-Gil IJ, Andrés M, Benito B, Bernardo E, Vedia O, Ferreira-Gonzalez I, et al. Serum metabolomic analysis suggests impairment of myocardial energy production in Takotsubo syndrome. Metabolites. (2021) 11(7):439. doi: 10.3390/metabo11070439
6. Okorare O, Evbayekha EO, Adabale OK, Daniel E, Ubokudum D, Olusiji SA, et al. Smoking cessation and benefits to cardiovascular health: a review of literature. Cureus. (2023) 15(3):e35966. doi: 10.7759/cureus.35966
7. Zaghlol R, Ali L, Barac A. Tobacco smoking predicts worse outcomes in hospitalized patients with Takotsubo cardiomyopathy. Circulation. (2019) 140:A12626. Available at: https://www.ahajournals.org/doi/abs/10.1161/circ.140.suppl_1.12626
8. Harris KM, Rosman L, Burg MM, Salmoirago-Blotcher E. Modifiable lifestyle factors in women with Takotsubo syndrome: a case-control study. Heart Lung. (2020) 49(5):524–9. doi: 10.1016/j.hrtlng.2020.03.001
9. Arcari L, Núñez Gil IJ, Stiermaier T, El-Battrawy I, Guerra F, Novo G, et al. Gender differences in Takotsubo syndrome. J Am Coll Cardiol. (2022) 79(21):2085–93. doi: 10.1016/j.jacc.2022.03.366
10. Núñez-Gil IJ, Almendro-Delia M, Andrés M, Sionis A, Martin A, Bastante T, et al. Secondary forms of Takotsubo cardiomyopathy: a whole different prognosis. Eur Hear J Acute Cardiovasc Care. (2016) 5:308–16. doi: 10.1177/2048872615589512
11. Pätz T, Santoro F, Cetera R, Ragnatela I, El-Battrawy I, Mezger M, et al. Trigger-associated clinical implications and outcomes in Takotsubo syndrome: results from the multicenter GEIST registry. J Am Heart Assoc. (2023) 12(14):e028511. doi: 10.1161/JAHA.122.028511
12. Almendro-Delia M, Núñez-Gil IJ, Lobo M, Andrés M, Vedia O, Sionis A, et al. Short- and long-term prognostic relevance of cardiogenic shock in Takotsubo syndrome. JACC Hear Fail. (2018) 6:928–36. doi: 10.1016/j.jchf.2018.05.015
13. Stiermaier T, Walliser A, El-Battrawy I, Pätz T, Mezger M, Rawish E, et al. Happy heart syndrome: frequency, characteristics, and outcome of Takotsubo syndrome triggered by positive life events. JACC Heart Fail. (2022) 10(7):459–66. doi: 10.1016/j.jchf.2022.02.015
14. Li P, Dai Q, Cai P, Teng C, Pan S, Dixon RAF, et al. Identifying different phenotypes in Takotsubo cardiomyopathy by latent class analysis. ESC Heart Fail. (2021) 8(1):555–65. doi: 10.1002/ehf2.13117
15. Morgan AD, Zakeri R, Quint JK. Defining the relationship between COPD and CVD: what are the implications for clinical practice? Ther Adv Respir Dis. (2018) 12:1753465817750524. doi: 10.1177/1753465817750524
16. Middlekauff HR, Park J, Moheimani RS. Adverse effects of cigarette an noncigarette smoke exposure on the autonomic nervous system: mechanisms and implications for cardiovascular risk. J Am Coll Cardiol. (2014) 64:1740–50. doi: 10.1016/j.jacc.2014.06.1201
17. Matsuura T, Ueno M, Iwanaga Y, Miyazaki S. Importance of sympathetic nervous system activity during left ventricular functional recovery and its association with in-hospital complications in Takotsubo syndrome. Heart Vessels. (2019) 34:1317–24. doi: 10.1007/s00380-019-01359-4
18. Rajwani A, Adam Z, Hall JA. Bronchogenic stress cardiomyopathy: a case series. Cardiology. (2015) 130:106–11. doi: 10.1159/000369296
19. Redfors B, Jha S, Thorleifsson S, Jernberg T, Angerås O, Frobert O, et al. Short- and long-term clinical outcomes for patients with Takotsubo syndrome and patients with myocardial infarction: a report from the Swedish coronary angiography and angioplasty registry. J Am Heart Assoc. (2021) 10(17):e017290. doi: 10.1161/JAHA.119.017290
20. Scarboro D, Patel H, Roby M, Sane D. Predictors of subsequent hospital encounters in patients with Takotsubo cardiomyopathy. J Am Coll Cardiol. (2020) 75(11_Supplement_1):872. doi: 10.1016/S0735-1097(20)31499-6
21. Ghadri JR, Cammann VL, Jurisic S, Seifert B, Napp LC, Diekmann J, et al. A novel clinical score (InterTAK diagnostic score) to differentiate Takotsubo syndrome from acute coronary syndrome: results from the international Takotsubo registry. Eur J Heart Fail. (2017) 19(8):1036–42. doi: 10.1002/ejhf.683
22. Fan X, Yang G, Kowitz J, Akin I, Zhou X, El-Battrawy I. Takotsubo syndrome: translational implications and pathomechanisms. Int J Mol Sci. (2022) 23(4):1951. doi: 10.3390/ijms23041951
Keywords: Takotsubo syndrome, prognosis, smoking habit, mortality, registry, apical ballooning
Citation: Núñez-Gil IJ, Santoro F, Vazirani R, Novo G, Blanco-Ponce E, Arcari L, Uribarri A, Cacciotti L, Guerra F, Salamanca J, Musumeci B, Vedia O, Mariano E, Fernández-Cordón C, Caldarola P, Montisci R, Brunetti ND, El-Battrawy I, Abumayyaleh M, Akin I, Eitel I and Stiermaier T (2023) Smoking influence in Takotsubo syndrome: insights from an international cohort. Front. Cardiovasc. Med. 10:1282018. doi: 10.3389/fcvm.2023.1282018
Received: 23 August 2023; Accepted: 23 October 2023;
Published: 20 November 2023.
Edited by:
Michiaki Nagai, University of Oklahoma Health Science Center, United StatesReviewed by:
Mohammed Faisaluddin, Rochester General Hospital, United States© 2023 Núñez-Gil, Santoro, Vazirani, Novo, Blanco-Ponce, Arcari, Uribarri, Cacciotti, Guerra, Salamanca, Musumeci, Vedia, Mariano, Fernández-Cordón, Caldarola, Montisci, Brunetti, El-Battrawy, Abumayyaleh, Akin, Eitel and Stiermaier. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Iván J. Núñez-Gil aWJuc2t5QHlhaG9vLmVz
†These authors have contributed equally to this work
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.