 Marie-Hélène Grazide1,2
Marie-Hélène Grazide1,2 Wim Martinet
Wim Martinet Cécile Vindis
Cécile Vindis- 1Center for Clinical Investigation (CIC1436)/CARDIOMET, Rangueil University Hospital, Toulouse, France
- 2University of Toulouse III, Toulouse, France
- 3Department of Epidemiology, INSERM UMR 1027, Toulouse, France
- 4Laboratory of Physiopharmacology, University of Antwerp, Antwerp, Belgium
- 5Department of Cardiology, Rangueil University Hospital, Toulouse, France
Background: The discovery of novel biomarkers that improve current cardiovascular risk prediction models of acute coronary syndrome (ACS) is needed for the identification of very high-risk patients and therapeutic decision-making. Autophagy is a highly conserved catabolic mechanism for intracellular degradation of cellular components through lysosomes. The autophagy process helps maintain cardiac homeostasis and dysregulated autophagy has been described in cardiovascular conditions. Rubicon (Run domain Beclin-1-interacting and cysteine-rich domain-containing protein) is a key regulator of autophagy with a potential role in cardiac stress.
Objectives: The aims of the present study were to assess whether changes in circulating Rubicon levels are associated with ACS and to evaluate the added value of Rubicon to a clinical predictive risk model.
Methods and results: The study population included ACS patients (n = 100) and control subjects (n = 99) at high to very high cardiovascular risk but without known coronary event. Plasma Rubicon levels were measured in the whole study population by enzyme-linked immunosorbent assay. Multivariate logistic regression analyses established that Rubicon levels were inversely associated with ACS. A receiver operating characteristic curve analysis demonstrated that the addition of Rubicon improved the predictive performance of the model with an increased area under the curve from 0.868 to 0.896 (p = 0.038).
Conclusions: Plasma levels of the autophagy regulator Rubicon are associated with ACS and provide added value to classical risk markers for ACS.
1 Introduction
Cardiovascular disease (CVD) ranks as one of the most prevalent causes of morbidity and mortality worldwide. Despite considerable progresses in acute care and secondary prevention after acute coronary syndrome (ACS), the global burden is expected to rise because of the aging of the world population and increased obesity and diabetes (1). In this scenario, there is still a need to discover novel biomarkers for the prognostication and therapeutic decision-making. Autophagy is a highly conserved cellular catabolic process that is responsible for the destruction of long-lived proteins and organelles via a lysosome-dependent pathway. In the general form of autophagy, cytoplasmic cargo targeted for destruction is sequestered inside double-membrane vesicles called autophagosomes and is delivered to the lysosome by fusion for breakdown (2). This process is crucial for preserving cellular homeostasis and dysregulated autophagy has been associated to the pathogenesis of a wide array of diseases including cardiovascular conditions such as myocardial ischemia-reperfusion (I/R) (3–5). Of note, myocardial I/R is associated with type 1 myocardial infarction (MI) which is the consequence of atherosclerotic plaque rupture. The categories of patients with type 1 ST-elevation MI (STEMI) or type 1 non-ST-elevation MI (NSTEMI) are customarily included in the definition of ACS (6).
Once activated, autophagy proceeds through four sequential steps, each step requiring specific regulatory proteins and complexes that have been well described in several reviews and will not be detailed here (7). Ischemic injury activates autophagy in cardiomyocytes enabling them to cope with nutritional stress and improve cell survival (8–10). Nah and colleagues showed that autosis, a novel form of cell death caused by excessive autophagy, occurred during the late reperfusion phase in the mouse heart exposed to I/R. Notably, autosis is associated with reduced autophagic flux, blockade of autophagosome clearance and upregulation of Rubicon (RUN domain Beclin-1 interacting and cysteine-rich-containing protein) (11). Rubicon is one of the few endogenous inhibitors of autophagy during autophagosome maturation and autophagosome-lysosome fusion (12, 13). Rubicon has been also involved in autophagy-independent functions including LAP (LC3-associated phagocytosis), endosomal trafficking and inflammatory responses (14–16). The close relationship between Rubicon and myocardial I/R (11, 17) makes it as a potential biomarker for measuring autophagy level in clinical practice and a therapeutic target for modulating autophagy. At present, there is a lack of studies on the levels of circulating autophagy proteins as easily accessible diagnostic or prognostic tools for monitoring cardiac diseases even though autophagy is known to play a major role. Thanks to commercially available immunoassay kits, a panel of autophagy proteins were measured in human body fluids. Recent work has demonstrated that circulating levels of the autophagy/mitophagy proteins ATG5 and Parkin were found as diagnostic tools for early monitoring of patients with cognitive decline, for identifying the active phase of multiple sclerosis or related to the severity of hypoxic injury during perinatal hypoxic-ischemic encephalopathy (18–20). In addition, a correlation has been established between the level of serum circulating Beclin1 and the degree of airflow obstruction in COPD patients compared to healthy controls (21). Interestingly, Emmanuele and colleagues showed that healthy centenarians have increased circulating Beclin1 protein levels in comparison to a population of young healthy subjects or patients with MI (22). Thus, for our work we sought for the presence of Rubicon in the circulation and its possible association with myocardial infarction. At this end, using immunoassays we measured plasma Rubicon protein levels in a case-control study including patients who experienced ACS and very high-risk asymptomatic individuals according to a SCORE (Systematic Coronary Risk Evaluation) model (23).
2 Materials and methods
2.1 Study population
The population is a case-control study including ACS patients from a prospective cohort (NCT02405468) (24). Cases (n = 100, men and women) were patients who experienced an acute ischemic event and were enrolled 3 days after the acute ischemic phase (henceforward referred to as ACS patients). Demographic, clinical, and biological variables were recorded and a blood sample was collected. Coronary data and left ventricular ejection fraction were accessible for all patients. During the same period, subjects (n = 99, men and women) at very high cardiovascular risk (henceforward referred to as controls) but without any previous vascular or coronary event, were recruited in the Center for the Prevention of Cardiovascular Disease in the Cardiology Department (University Hospital Center, Toulouse, France). The exclusion criteria for the both populations included: infectious disease within 1 week before enrollment, immunocompromised patients, antibiotic treatment within 1 month before enrollment, chronic viral infection, chronic inflammatory intestinal bowel disease, renal failure (estimated glomerular filtration rate <50 ml/min per 1.73 m2) and pregnancy. The written informed consent was obtained from each individual. The study protocol conformed to the ethical guidelines of the 1975 Declaration of Helsinki and Toulouse Hospital guidelines. The study protocol was previously reviewed and approved by the regional board of health authorities (Agence Régionale de Santé Occitanie-Midi-Pyrénées, Toulouse, France) and the Institution's ethics committee on research on humans (Comité de protection des personnes du Sud-Ouest, Toulouse, France).
2.2 Blood sampling and plasma levels of Rubicon determination
EDTA plasma samples were prepared and stored at −80°C within a 3 h' delay. Rubicon were measured by using commercially available enzyme-linked immunosorbent assay kits [human Rubicon ELISA Kit (HUFI06681), Assay Genie, Dublin, Ireland]. Briefly, the ELISA Rubicon assay is a quantitative sandwich ELISA technique and was done on frozen (−80°C) EDTA plasma samples never thawed (haemolyzed samples were excluded). Once the samples (100 µl in each well), blanks and standards were plated, the plate is incubated with the specific biotin-conjugated primary antibody Rubicon and Avidin conjugated Horseradish Peroxidase. The signal intensity (yellow color) is measured on microplate reader at 450 nm.
2.3 Statistical analysis
Data are presented as means and standard deviations for quantitative variables and percentages for categorical variables. The distribution of qualitative variables between cases and controls was compared using the Chi2 test. Fisher's exact test was used when basic assumptions were not satisfied. The student's t-test was used to compare mean values of quantitative variables. The Shapiro–Wilk's and Levene's tests were applied to assess the normality of distribution of residuals and the homogeneity of variances. A logarithmic transformation of the variables or a Wilcoxon–Mann–Whitney test was achieved when basic assumptions of Student's t-test were not satisfied. The autophagy marker Rubicon was compared between cases and controls using the Mann and Whitney test. Relationships between the levels of Rubicon and metabolic parameters or cardiovascular risk factors were tested with a non-parametric measure of rank correlation (Spearman rank correlation). Autophagy factor was examined in a multivariate analysis by adjusting for variables of the basic model (gender, current smoker, hypertension, dyslipidemia, diabetes, obesity, age and heredity). Medical treatments were added in the basic model. Logistic regression analyses were performed with polynomial models (quadratic and cubic) to examine for possible non-linear relationships between continuous variables and case-control status. Because of a clearly non-linear relationship with Rubicon, logistic regression analyses were carried out using a categorization of the variable into quartiles. ROC curve analysis was performed to establish the capacity to discriminate cases and controls for Rubicon, the calculation of the standard error of the area under the curve (AUC) was done applying the Delong's method. All tests were two-tailed at the level of significance of 0.05. Analyses were achieved using SAS software, version 9.4 (SAS Institute, Cary, NC, USA) and STATA statistical software, release 14.1 (Stata Corporation, College Station, TX, USA).
3 Results
3.1 Population characteristics and analysis of Rubicon plasma concentrations
The case-control study was conducted on 199 individuals. The baseline variables of the ACS and control subjects are reported in Table 1. The high percentage of hypertension, dyslipidemia or obesity, as well as the significant differences in the medical treatments found in the control group, were explained by their enrollment in the Prevention of Cardiovascular Disease department (Toulouse University Hospital Center, Toulouse, France). Plasma levels of the autophagy regulator Rubicon were quantified in the studied subjects. The mean ± SD concentration of Rubicon at baseline was statistically (p < 0.001) lower in ACS patients (49.92 ± 9 pg/ml) compared with control subjects (57.45 ± 12.5 pg/ml) (Figure 1). After stratification by gender, dyslipidemia, diabetes, hypertension and smoking, plasma concentrations of Rubicon were found statistically lower in diabetes subjects (Supplementary Data 1).
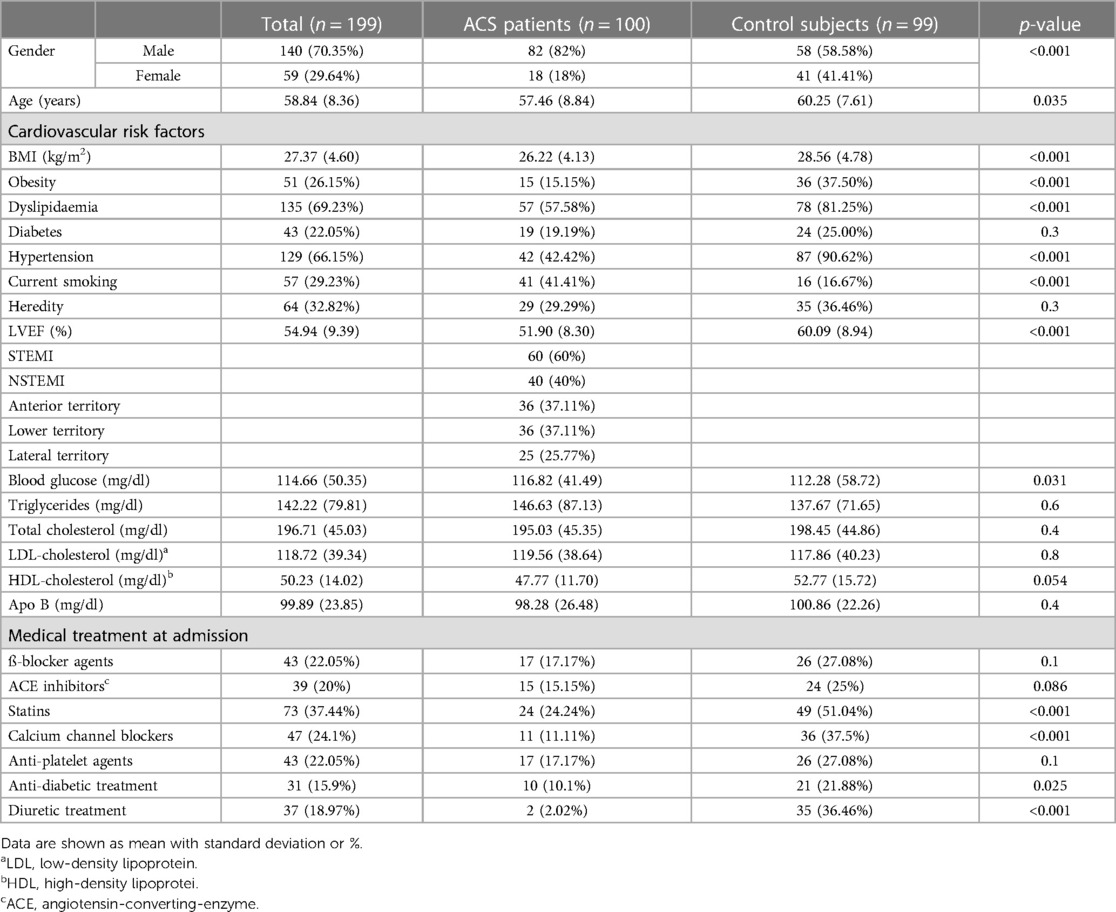
Table 1. Baseline characteristics of the study population.
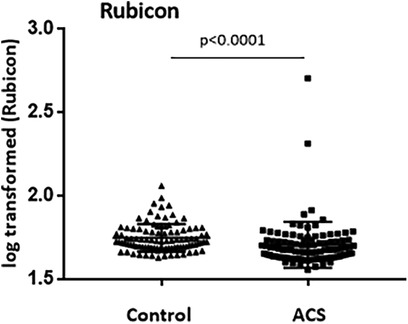
Figure 1. Plasma levels of Rubicon in the study population measured by enzyme-linked immunosorbent assay. The scatter plots represent the values (log transformed data) with standard deviation of control subjects (Control) and ACS patients (ACS).
3.2 Correlation between Rubicon with metabolic parameters and cardiovascular risk factors
Spearman rank correlation coefficients between Rubicon and metabolic parameters or cardiovascular risk markers were calculated. In the whole studied population, a significant positive correlation of Rubicon with lipid parameters such as total cholesterol (r = 0.141, p = 0.046), LDL (low-density lipoprotein)-cholesterol (r = 0.172, p = 0.015) and ApoB (r = 0.257, p = 0.007) was found.
3.3 Association of Rubicon with ACS
The results presented in Table 2 show the crude estimates and unadjusted/adjusted associations of the autophagy inhibitor Rubicon with the risk of ACS. The unadjusted logistic regression analysis revealed that Rubicon was significantly inversely associated with ACS. After adjustment for potential confounders including gender, age, obesity, dyslipidemia, hypertension, heredity, smoking and the medical treatments, the association with ACS remained statistically significant.
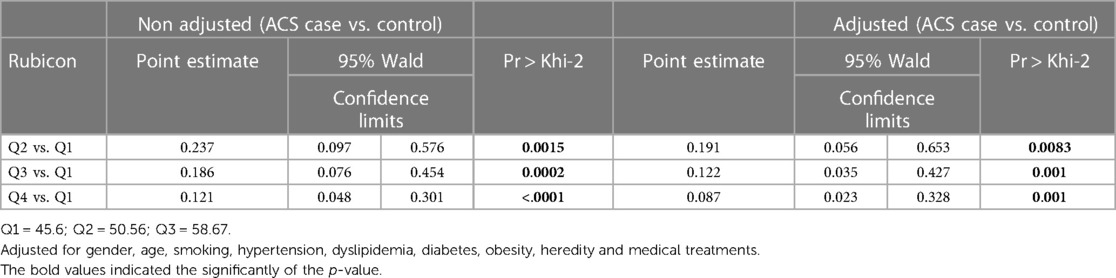
Table 2. Logistic regression analysis for Rubicon and the risk of ACS (cutoffs = quartiles).
3.4 Analysis of ROC curves and ACS risk prediction for Rubicon
We then assessed whether Rubicon could increase the predictive performance of a model comprising the classical cardiovascular risk factors (CVRF) and the medical treatments. A receiver operating characteristic (ROC) curve analysis was achieved and data in Table 3 show the performance (area under the curve, AUC) of clinical model, Rubicon alone or in combination with the model. The addition of Rubicon to the model led to a significant improvement of the predictive performance from 0.868 (95% CI 0.817–0.918) to 0.896 (95% CI 0.852–0.94, p = 0.038). Taken together, our results highlighted an incremental value of the autophagy biomarker Rubicon to traditional cardiovascular risk factors for ACS.
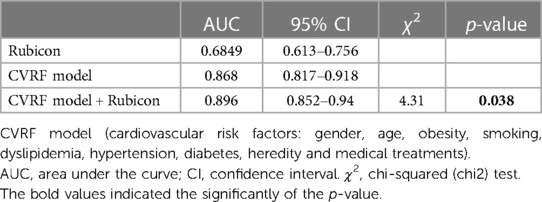
Table 3. Receiver operating characteristic (ROC) curve analysis comparing the predictive value of the autophagy regulator Rubicon.
4 Discussion
Novel reliable and sensitive biomarkers in coronary artery disease remains a major clinical need. In the present work, we explored for the first time the expression levels of plasma-circulating autophagy regulator Rubicon in a population of ACS patients compared to control subjects. Rubicon is one of the few negative regulators of autophagy. The protein inhibits autophagosome-lysosome fusion through binding to the PI3KC3 (phosphatidylinositol 3-kinase complex 3)-UVRAG (UV-irradiation-resistance-associated gene) complex (13). Levels of Rubicon increase in association with conditions of autophagy impairment such as aging (25). In our study, we could demonstrate that Rubicon levels are significantly decreased in ACS patients, which confirmed previous in vivo data describing autophagy activation during myocardial I/R (8). In a mouse model of myocardial I/R, ischemia stimulates autophagy through an AMPK (AMP kinase)-dependent mechanism due to the low energy and hypoxic conditions whereas reperfusion stimulates autophagy through a Beclin 1-dependent but AMPK-independent mechanism and reactive oxygen species production (8). Regarding the role of Rubicon in MI, we can only speculate based on in vivo studies of myocardial I/R. During the ischemic phase and the early phase of reperfusion, an increased autophagic flux and lysosomal activity is measured in the mouse myocardium, which correlates with decreased expression of the inhibitor Rubicon. However, 6 h after reperfusion the autophagic flux in the border zone decreases below basal levels coinciding with a gradually up-regulation of Rubicon (11). Therefore, on the basis of our results we hypothesized that the decreased level of circulating Rubicon in ACS patients compared to control subjects might reflect the activation of autophagy flux during ischemia and the early phase of reperfusion. Further studies are necessary to determine whether the differential expression of circulating Rubicon is a result of modulated intracellular production and/or different release mechanisms. Interestingly, a recent study showed that stressed cardiomyocytes can release large extracellular vesicles derived from autophagy which have been termed “exopheres” containing mitochondria and sarcomere proteins (26). Conceivably, we can hypothesize that autophagy mediated exocytosis can result in the release of proteins like Rubicon into the circulation. Interestingly, we also identified significant positive correlations between Rubicon and lipid parameters including total cholesterol, LDL-cholesterol and ApoB, which is in line with results showing downregulation of autophagy in heart tissues of hypercholesterolemic rats (27). Importantly, our study demonstrated for the first time that Rubicon is measured in body fluids and inversely associated with ACS independently of CVRF and medical treatments, corroborating the critical roles of Rubicon in CVD. Moreover, ROC curve analysis provided a powerful predictive model comprising Rubicon, cardiovascular risk factors and medical treatments. Indeed, the addition of Rubicon improved the predictive performance of the model alone thus bringing extra value for ACS risk prediction when included in a multi-biomarker approach. The strength and originality of the present work lies in the evaluation of two very-high-risk populations for primary and secondary prevention of cardiovascular risk. Indeed, the association of Rubicon with the risk of ACS is independent of CVRF and medical treatments, which supports the significance of circulating Rubicon as a relevant biomarker in ACS. Moreover, considering its active role in myocardial I/R, Rubicon may also represent a novel target for therapeutic interventions to reduce autosis during the reperfusion phase. Some limits in our work have to be taken into account. Though the population size had sufficient statistical power to distinguish significant differences, it would be useful to have a second independent cohort for validation. Furthermore, it would have been interesting to measure the baseline expression of Rubicon before the ACS event, nevertheless such information requires a longitudinal study of a population at high cardiovascular risk and 10-year follow-up. Moreover, our study examines circulating Rubicon levels in the acute phase, it will also be interesting to carry out a kinetics study of Rubicon expression comprising very early samples taken before 6 h, between 6 and 24 h and during a follow-up. From the perspective of our study, the discovery and the monitoring of circulating autophagy biomarkers for use in clinical practice represent a great opportunity to understand how levels of autophagy correlate with cardiac outcomes in individuals affected by CVD.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statement
The studies involving human participants were reviewed and approved by Agence Régionale de Santé Occitanie-Midi-Pyrénées (Toulouse, France) and the Institution's ethics committee on research on humans: Comité de protection des personnes du Sud-Ouest, (Toulouse, France). The patients/participants provided their written informed consent to participate in this study.
Author contributions
M-HG: Methodology, Writing – original draft. J-BR: Formal analysis, Methodology, Validation, Writing – review & editing. WM: Funding acquisition, Writing – review & editing. ME: Funding acquisition, Writing – review & editing, Resources. CV: Funding acquisition, Conceptualization, Data curation, Investigation, Supervision, Validation, Writing – original draft, Writing – review & editing.
Funding
The author(s) declare financial support was received for the research, authorship, and/or publication of this article.
This work was supported by an INSERM International Research Project (SUBSIDI) to CV and WM and by “La Fédération Française de la Cardiologie” to CV and ME.
Acknowledgments
The authors would like to acknowledge the nurses, K. Ioannides and C. Lagente, the patients and all investigators involved in this study, without whom the study would not have been possible.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The author(s) declared that they were an editorial board member of Frontiers, at the time of submission. This had no impact on the peer review process and the final decision.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fcvm.2023.1279899/full#supplementary-material
References
1. Timmis A, Townsend N, Gale C, Grobbee R, Maniadakis N, Flather M, et al. European Society of Cardiology: cardiovascular disease statistics 2017. Eur Heart J. (2018) 39(7):508–79. doi: 10.1093/eurheartj/ehx628
2. Klionsky DJ, Emr SD. Autophagy as a regulated pathway of cellular degradation. Science. (2000) 290(5497):1717–21. doi: 10.1126/science.290.5497.1717
3. De Meyer GR, Grootaert MO, Michiels CF, Kurdi A, Schrijvers DM, Martinet W. Autophagy in vascular disease. Circ Res. (2015) 116(3):468–79. doi: 10.1161/CIRCRESAHA.116.303804
4. Gustafsson AB, Gottlieb RA. Autophagy in ischemic heart disease. Circ Res. (2009) 104(2):150–8. doi: 10.1161/CIRCRESAHA.108.187427
5. Mialet-Perez J, Vindis C. Autophagy in health and disease: focus on the cardiovascular system. Essays Biochem. (2017) 61(6):721–32. doi: 10.1042/EBC20170022
6. Thygesen K, Alpert JS, Jaffe AS, Chaitman BR, Bax JJ, Morrow DA, et al. Fourth universal definition of myocardial infarction (2018). J Am Coll Cardiol. 2018;72(18):2231–64. doi: 10.1016/j.jacc.2018.08.1038
7. Yang Z, Klionsky DJ. Mammalian autophagy: core molecular machinery and signaling regulation. Curr Opin Cell Biol. (2010) 22(2):124–31. doi: 10.1016/j.ceb.2009.11.014
8. Matsui Y, Takagi H, Qu X, Abdellatif M, Sakoda H, Asano T, et al. Distinct roles of autophagy in the heart during ischemia and reperfusion: roles of AMP-activated protein kinase and Beclin 1 in mediating autophagy. Circ Res. (2007) 100(6):914–22. doi: 10.1161/01.RES.0000261924.76669.36
9. Ma X, Liu H, Foyil SR, Godar RJ, Weinheimer CJ, Hill JA, et al. Impaired autophagosome clearance contributes to cardiomyocyte death in ischemia/reperfusion injury. Circulation. (2012) 125(25):3170–81. doi: 10.1161/CIRCULATIONAHA.111.041814
10. Kanamori H, Takemura G, Goto K, Maruyama R, Ono K, Nagao K, et al. Autophagy limits acute myocardial infarction induced by permanent coronary artery occlusion. Am J Physiol Heart Circ Physiol. (2011) 300(6):H2261–71. doi: 10.1152/ajpheart.01056.2010
11. Nah J, Zhai P, Huang CY, Fernández Á F, Mareedu S, Levine B, et al. Upregulation of Rubicon promotes autosis during myocardial ischemia/reperfusion injury. J Clin Invest. (2020) 130(6):2978–91. doi: 10.1172/JCI132366
12. Minami S, Nakamura S, Yoshimori T. Rubicon in metabolic diseases and ageing. Front Cell Dev Biol. (2021) 9:816829. doi: 10.3389/fcell.2021.816829
13. Matsunaga K, Saitoh T, Tabata K, Omori H, Satoh T, Kurotori N, et al. Two Beclin 1-binding proteins, Atg14l and Rubicon, reciprocally regulate autophagy at different stages. Nat Cell Biol. (2009) 11(4):385–96. doi: 10.1038/ncb1846
14. Sun Q, Westphal W, Wong KN, Tan I, Zhong Q. Rubicon controls endosome maturation as a Rab7 effector. Proc Natl Acad Sci U S A. (2010) 107(45):19338–43. doi: 10.1073/pnas.1010554107
15. Martinez J, Malireddi RK, Lu Q, Cunha LD, Pelletier S, Gingras S, et al. Molecular characterization of LC3-associated phagocytosis reveals distinct roles for Rubicon, NOX2 and autophagy proteins. Nat Cell Biol. (2015) 17(7):893–906. doi: 10.1038/ncb3192
16. Yang CS, Rodgers M, Min CK, Lee JS, Kingeter L, Lee JY, et al. The autophagy regulator Rubicon is a feedback inhibitor of CARD9-mediated host innate immunity. Cell Host Microbe. (2012) 11(3):277–89. doi: 10.1016/j.chom.2012.01.019
17. Li Y, Liang P, Jiang B, Tang Y, Liu X, Liu M, et al. CARD9 Promotes autophagy in cardiomyocytes in myocardial ischemia/reperfusion injury via interacting with Rubicon directly. Basic Res Cardiol. (2020) 115(3):29. doi: 10.1007/s00395-020-0790-6
18. Castellazzi M, Patergnani S, Donadio M, Giorgi C, Bonora M, Bosi C, et al. Autophagy and mitophagy biomarkers are reduced in sera of patients with Alzheimer’s disease and mild cognitive impairment. Sci Rep. (2019) 9(1):20009. doi: 10.1038/s41598-019-56614-5
19. Tarocco A, Morciano G, Perrone M, Cafolla C, Ferrè C, Vacca T, et al. Increase of parkin and ATG5 plasmatic levels following perinatal hypoxic-ischemic encephalopathy. Sci Rep. (2022) 12(1):7795. doi: 10.1038/s41598-022-11870-w
20. Patergnani S, Castellazzi M, Bonora M, Marchi S, Casetta I, Pugliatti M, et al. Autophagy and mitophagy elements are increased in body fluids of multiple sclerosis-affected individuals. J Neurol Neurosurg Psychiatry. (2018) 89(4):439–41. doi: 10.1136/jnnp-2017-316234
21. Schlemmer F, Boyer L, Soumagne T, Ridoux A, Chouaid C, Maitre B, et al. Beclin1 circulating levels and accelerated aging markers in COPD. Cell Death Dis. (2018) 9(2):156. doi: 10.1038/s41419-017-0178-1
22. Emanuele E, Minoretti P, Sanchis-Gomar F, Pareja-Galeano H, Yilmaz Y, Garatachea N, et al. Can enhanced autophagy be associated with human longevity? Serum levels of the autophagy biomarker beclin-1 are increased in healthy centenarians. Rejuvenation Res. (2014) 17(6):518–24. doi: 10.1089/rej.2014.1607
23. Knuuti J, Wijns W, Saraste A, Capodanno D, Barbato E, Funck-Brentano C, et al. 2019 ESC guidelines for the diagnosis and management of chronic coronary syndromes. Eur Heart J. (2020) 41(3):407–77. doi: 10.1093/eurheartj/ehz425
24. Elbaz M, Faccini J, Laperche C, Grousset E, Roncalli J, Ruidavets JB, et al. Identification of a miRNA based-signature associated with acute coronary syndrome: evidence from the FLORINF study. J Clin Med. (2020) 9(6):1674–86. doi: 10.3390/jcm9061674
25. Nakamura S, Oba M, Suzuki M, Takahashi A, Yamamuro T, Fujiwara M, et al. Suppression of autophagic activity by Rubicon is a signature of aging. Nat Commun. (2019) 10(1):847. doi: 10.1038/s41467-019-08729-6
26. Nicolás-Ávila JA, Lechuga-Vieco AV, Esteban-Martínez L, Sánchez-Díaz M, Díaz-García E, Santiago DJ, et al. A network of macrophages supports mitochondrial homeostasis in the heart. Cell. (2020) 183(1):94–109.e23. doi: 10.1016/j.cell.2020.08.031
Keywords: Rubicon, autophagy regulator, biomarker, acute coronary syndrome, risk prediction
Citation: Grazide M-H, Ruidavets J-B, Martinet W, Elbaz M and Vindis C (2024) Plasma levels of autophagy regulator Rubicon are inversely associated with acute coronary syndrome. Front. Cardiovasc. Med. 10:1279899. doi: 10.3389/fcvm.2023.1279899
Received: 18 August 2023; Accepted: 18 December 2023;
Published: 5 January 2024.
Edited by:
Yuanhui Liu, Guangdong Provincial People’s Hospital, ChinaReviewed by:
Satvik Mareedu, The State University of New Jersey, United StatesAllen Sam Titus, Rutgers University, United States
© 2024 Grazide, Ruidavets, Martinet, Elbaz and Vindis. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Cécile Vindis Y2VjaWxlLnZpbmRpc0BpbnNlcm0uZnI=