
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
CLINICAL TRIAL article
Front. Cardiovasc. Med. , 22 November 2023
Sec. General Cardiovascular Medicine
Volume 10 - 2023 | https://doi.org/10.3389/fcvm.2023.1272897
This article is part of the Research Topic Implementation of Digital Health Intervention on Mobile Devices to Support Cardiovascular Disease Healthcare among Public Health View all 6 articles
 Ivone Silva1,2,3,†
Ivone Silva1,2,3,† Célia Sofia Moreira4
Célia Sofia Moreira4 Susana Pedras1*†
Susana Pedras1*† Rafaela Oliveira1
Rafaela Oliveira1 Carlos Veiga1
Carlos Veiga1 Luís Moreira5
Luís Moreira5 Daniel Santarém5Daniel Guedes5
Daniel Santarém5Daniel Guedes5 Hugo Paredes5,6
Hugo Paredes5,6
Aims: Investigate whether a Home-based Exercise Therapy (HBET) program for patients with Peripheral Arterial Disease (PAD) and Intermittent Claudication (IC) with a behavior change intervention, supported by a smartphone application, is effective in improving walking distances and performance, and quality of life (QoL) over 6 months.
Methods and results: This was a single-center, prospective, two-arm, single-blinded randomized controlled trial including 73 patients with PAD and IC, and three assessment moments: baseline, 3, and 6 months. Participants were randomized to receive a walking exercise prescription, with the support (n = 38) or without the support (n = 35) of the WalkingPad app, between January 2021 and July 2022. Both groups received two face-to-face behavior change sessions and 12 structured and targeted reinforcement phone calls over 6 months. Primary outcomes were between-group differences in pain-free walking distance (PFWD), functional walking distance (FWD), maximal walking distance (MWD), and 6-min walk distance (6 MWD) at 3 and 6 months. Secondary outcomes were QoL and walking impairment. Seventy-three patients (mean age 64 ± 7.2 years, 88% men) participated in this study, 60 of whom completed the three assessment moments. The whole sample significantly improved all primary outcomes in the first 3 months; that is, the average PFWD (151.1 m), FWD (175.2 m), MWD (171.1 m), and 6 MWD (30.8 m) increased from T1 to T2. Only MWD exhibited a significant average increase (35.0 m). Secondary outcomes also increased from baseline to 3 and 6 months. There were no between-group differences, except for MWD, which showed a greater increase at 6 months in the group that used the app, excluding patients with weak walking ability and extreme anxiety symptoms at baseline.
Conclusion: The intervention improved distances and walking skills as well as the physical, mental, and disease-related quality of life among adults with PAD and IC. The group that used the WalkingPad app improved their MWD in 6 months compared to the control group, except for patients with poor walking ability and extreme anxiety symptoms, which suggests the effectiveness of the WalkingPad app for patients with high walking ability and no severe anxiety symptoms. More research is needed to determine the durability of these findings and to explore what app functionality might promote the other outcomes.
Clinical Trial Registration: https://clinicaltrials.gov (NCT04749732).
Lower extremity peripheral arterial disease (PAD) is associated with reduced walking capacity and increased cardiovascular morbidity and mortality risk (1). Regular exercise significantly improves walking ability and performance in patients with PAD and is the first-line therapeutic measure recommended by clinical practice guidelines (2). Home-based exercise therapy (HBET) is a structured, unsupervised, self-directed walking program performed in the patient's residential area rather than in a clinical setting (3, 4). HBET programs are effective in improving walking performance and physical activity in the short term (3 months), but it is not entirely clear whether they are effective in the long term (6 months) (4, 5). However, adherence to exercise therapy is typically low because of the lack of supervision (5) (unlike supervised exercise therapy) and human nature (people tend to seek pleasure and avoid pain) (6).
Patients with PAD often have a low quality of life (QoL) associated with the inability to walk caused by pain (7). Moreover, there are high prevalence rates of anxiety and depressive disorders among patients with PAD, which in addition to being underdiagnosed (8), the emotional state plays a key role in decreasing disposition and adherence to physical exercise, increasing barriers and consequently restraining improvement of PAD (9).
Developing patients' intrinsic motivation through a theory-based behavior change intervention (10–12) is crucial to promote adherence to exercise therapy and desirable outcomes. In addition, patients with PAD are recommended to receive advice about lifestyle changes and medical therapies to reduce the risk of atherosclerotic complications (13).
Smartphone apps are innovative, low-cost, and proven effective tools for improving walking abilities and distances (14–17). However, current HBET programs use smartphone apps primarily through commercially available fitness apps that sync with wearable activity monitors (WAM) to record and access data. Specific applications for PAD are scarce, and their efficacy is still unclear (18).
We hypothesized that the WalkingPad study (a single-center randomized clinical trial), a home-based exercise program with a behavior change intervention and a smartphone app—WalkingPad—will improve walking ability, distances, and QoL in people with PAD and intermittent claudication (IC) compared to a control group.
The Research Ethics Committee approved this trial on October 22, 2019 (reference: 069-DEFI/068-CES), and the protocol was registered on the US National Library of Medicine (ClinicalTrials.gov) with the identifier NCT04749732 on February 10, 2021. This is a single-center, prospective, two-arm, single-blinded (to patients) randomized controlled trial (RCT) that enrolled participants between March 2021 and July 2022. Participants provided informed consent. The study protocol is published and available online.
Participants were recruited from the outpatient clinic of the Angiology and Vascular Surgery Department of Centro Hospitalar Universitário de Santo António (CHUSA), Porto, Portugal, between January 2021 and July 2022.
Inclusion criteria for the study were: (1) PAD with IC (Fontaine II or Rutherford 1–3) due to atherosclerotic disease and stable IC for more than 3 months; (2) Ankle Brachial Index (ABI) below 0.9 at rest or below 0.73 after exercise (20% decrease); (3) Age range between 50 and 80 years; (4) MWD in treadmill test between 50 and 600 m.
Exclusion criteria were: (1) asymptomatic PAD; (2) critical ischemia (Fontaine III/IV or Rutherford 4–6); (3) previous lower extremity vascular surgery, angioplasty, or lumbar sympathectomy; (4) any condition other than PAD that limits walking; (5) unstable angina or myocardial infarction diagnosed in the last 6 months; (6) inability to obtain ABI measure due to non-compressible vessels; (7) use of cilostazol and pentoxifylline initiated within 3 months before the investigation; (8) active cancer, renal disease, or liver disease; (9) severe chronic obstructive pulmonary disease (GOLD stage III/IV); (10) severe congestive heart failure (NYHA class III/IV); (11) diagnosis of a psychiatric disease that impairs daily life activities and/or with medical records of decompensation episodes in the last year and/or non-adherence to drug therapy; and (12) cognitive impairment (MMSE ≤ 15 for illiterate patients, 22 for those with 1–11 years of schooling; 27 for >11 years).
Participants were randomly assigned in a 1:1 ratio to receive an exercise prescription with a behavior change intervention supported or not by a smartphone app, using a computer-generated randomization system, with randomly selected block sizes of 5 stratified by age (50 to 65 years old; 66 to 80 years old), and maximal walking distance (50 to 325 m; 326 to 600 m) (flow diagram as Supplementary Material S1). It was impossible to mask participants, the outcome assessor, and the psychologist for group allocation after randomization due to the nature of the interventions. The statistician was masked for group allocation.
All participants received standard PAD treatment, a physical exercise prescription, and a behavior change intervention. Standard treatment for PAD and IC followed the guidelines of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines (AHA/ACC) (2, 3, 19, 20).
The physical exercise prescription consisted of walking sessions, performed for at least 30 min per session, three times a week in the area of residence of the participants. Near-maximal pain during training was the outcome of claudication pain (21). The behavior change intervention was based on Self-Determination Theory (SDT), which focuses on the type and quality of motivation, and the satisfaction of basic psychological needs, as pre-eminent behavioral determinants (22–24). According to this theory, individuals become more autonomous or self-determined on a continuum that ranges from external motivation to internalization of motivation. As this continuum progresses, individuals are more likely to engage in new, long-term behaviors. To achieve this, motives or extrinsic reasons for changing and adhering to a new behavior must be internalized and become as intrinsic as possible. Thus, the behavioral change intervention aimed to facilitate this internalization process to nurture a more autonomous motivation. Also, motivational interviewing principles are considered effective in promoting and encouraging change (11, 25, 26). Patients received two face-to-face behavior change sessions, at baseline (T1) and 3 months (T2), conducted by a health psychologist, for a total of 4 h (120 min per session). Complementary, booster phone calls over the 24-week intervention period were used to support participants and identify barriers to goal completion, based on a personalized and individualized self-management approach to promote long-term adherence to the exercise prescription (27, 28).
Participants assigned to this group received a self-fulfilling walking practice diary to monitor and record walking sessions: frequency (date) and duration of the walking session, the number of stops, and the level of well-being (ranging from 0 very bad to 10 very good) to be filled in each walking session.
Participants assigned to this group received a smartphone (Samsung Galaxy A41 SM-A415F/DSN, Vietnam) with the WalkingPad app installed. The application has several features that make it an asset to HBET programs: (1) allows adherence to be measured objectively and guides the intervention of health professionals; (2) encourages patient self-management and empowerment—promoting responsible and informed self-management of the disease, and (3) regularly and routinely accompanies the patient during exercise sessions as an “exercise buddy”—providing emotional support. Patients received appropriate coaching on how to use the app and record their data. A web platform (WalkingPad web platform) received data from the app, allowing collaboration between different actors (health professionals, researchers, and engineers) in monitoring patient adherence, promoting patient responsibility in their strategy of care, and adjusting the provision of personalized feedback during booster phone calls to overcome personal barriers to physical exercise. Furthermore, although patients left the hospital with the phone and the application installed, they took with them an Application Installation Guide (Supplementary Material S2) and an Instruction Manual for using the application with a technical support number (Supplementary Material S3).
Medical history and clinical data were collected from the participants' electronic clinical medical records, and sociodemographic data were collected through a clinical interview.
Depressive symptoms were assessed by the Geriatric Depression Scale-5 (GDS), which includes five dichotomous items (yes/no) with higher results corresponding to more depressive symptoms (29, 30).
Anxiety symptoms were assessed by the Geriatric Anxiety Inventory-Short Form (GAI-SF), which includes five dichotomous items (yes/no), with higher results corresponding to more anxiety symptoms (31, 32).
The modified Gardner-Skinner Treadmill Protocol was used, according to which participants began to walk on the treadmill at 1 km/h with a 0% grade (33). After 2 min, the speed increases to 1.6 km/h at 0% grade. Then the speed is increased by 0.8 km/h every 2 min until reaching 3.2 km/h. After reaching 3.2 km/h, the speed is kept constant, and the grade increases by 2% every 2 min.
The 6-Minute Walk Test (6 MWT) was performed to evaluate the functional capacity of the individual to walk over a total of 6 min on a 100 ft (≈30 m) hallway (34) according to the American Thoracic Society guidelines (35).
The primary outcomes were pain-free walking distance (PFWD), functional walking distance (FWD), maximal walking distance (MWD), and 6 MWD at 3 and 6 months, measured by two tests. The treadmill test (33) and the 6-Minute Walk Test (34, 35). The walking distance measured with a standardized treadmill test is a widely used tool for functional assessment and monitoring of exercise rehabilitation, where PFWD, FWD, and MWD are objective measures of improvement. In turn, the 6 MWT is an individualized test that assesses the submaximal level of functional capacity (35, 36). The patient chooses the intensity of the exercise and can rest during the test, which better reflects the functional level of exercise practiced in daily physical activities. The primary outcomes reflect the effectiveness (beneficial effect) and not the harm (adverse effect) of the intervention.
Secondary outcomes were: (1) health-related quality of life (QoL) assessed by the Vascular Disease-Specific Quality of Life Questionnaire (VascuQoL-6, scores ranging from 6 to 24, higher scores indicate better QoL) (36–38); and by the 12-Item Short Form Health Survey (SF-12, includes two summary component scores, higher scores indicate better physical and mental QoL) (39, 40); and (2) the Walking Impairment Questionnaire (WIQ) was used to assess the daily walking ability of patients in three domains: distance, speed, and climbing stairs (values range from 0 to 100%, and higher scores indicate less impairment in walking abilities/performance) (41).
In most RCTs, especially in clinical settings, it is possible to assess the effectiveness of an intervention using a single primary outcome. However, in many situations, a comprehensive understanding of the effects of an intervention requires analysing multiple outcomes. Indeed, patients' health status cannot be fully evaluated using a single outcome, and distinct outcomes may provide different but equally important information about the effectiveness of the intervention (42). Fortunately, developments in statistical methods have allowed researchers to account for multiple outcomes in RCTs (43), especially those that represent the same outcome at different time points, as well as to use suitable families of distributions. In this study, we expected the WalkingPad intervention to improve patients' MWD, PFWD, FWD, and 6 MWD (42, 43). For this reason, these four outcomes were used to define the effectiveness of the intervention and thus, this study comprises these four primary outcomes.
As an investigative outcome, the outcome assessor collected adverse events at the 3- and 6 months follow-ups.
When designing this study, we planned to enroll three arms (two intervention groups and one control group) and a total sample of 200 participants, accounting for 20% dropouts and adverse events. However, later, the power analysis carried out indicated that 57 participants were needed for each group and was published in the protocol. However, as it was not possible to recruit this number of participants, due to the Covid-19 pandemic, a new analysis was carried out (at T0) (a posteriori) to find out what effect size the sample would be able to “capture”, that is, whether this number was sufficient to detect between-group effects. Thus, power analysis was performed using the R package WebPower (44). As we were planning to analyze data through mixed-effect models, we selected a repeated-measures ANOVA, which accounts for both within and between-subject effects (45), two groups, three measurements, 5% of significance level, 80% of power, and a 10% attrition rate, grounded in other studies with this population. These conditions provided a minimum Cohen's f = 0.36 [or Cohen's d = 0.72, in this specific case] (46), which means that it would be possible to find large effect sizes. Therefore, we decided to proceed with the study.
Statistical analyses were conducted using R software, version 4.2.1, and the packages: lme4 (47), lmerTest (48), glmmTMB (49), and interactions (50). The level of significance was set at 0.05.
Analyses regarding the sociodemographic and clinical characterization of the sample and the evolution of the main variables of interest over time were conducted using mathematical models with appropriate families of distribution according to each outcome (dependent variable). Mixed-effects models have been chosen to perform all analyses due to their flexibility and efficiency in analyzing repeated measures, accounting for baseline differences in the outcomes (51). Remarkably, these models yield more efficient estimates, shifting estimates toward each other and making comparisons more conservative (52), ruling out the need to adjust for multiple comparisons or perform post-hoc tests (as with classical procedures such as ANOVA).
To assess differences in the outcomes, mathematical modeling was performed. Before running the models, a suitable family of distributions was selected for each outcome. More precisely, four different types of models were performed: normal linear models for data associated with normality (evaluated using histograms, boxplots, and QQ-plots), logistic models for dichotomous data, COM-Poisson models for count data, and beta models for limited data. Limited data included truncated data, such as MWD, and were previously transformed into percentages. In particular, we draw attention to the fact that, contrary to the majority of similar research works, we did not use the normal distribution to model the MWD since the respective data were subject to truncation and yielded some boundary observations (the normal distribution does not respect bounds). Models were only used to assess differences in outcomes, so the interpretation of model coefficients is not emphasized.
After screening the clinical medical records of patients attending the outpatient clinic of the Angiology and Vascular Surgery Department, 268 patients were identified. Of these, 119 were included and invited to attend a screening evaluation at the hospital to confirm inclusion criteria (at baseline), and 73 were included in the study, randomized, and allocated to one of the two groups (Figure 1). Of these, 60 participated in the three assessment moments. Patients were randomized into two groups: The Control Group (CG)—35 patients (31 men; mean age 64.0 ± 7.16 years) and the Experimental Group (EG)—38 patients (33 men; mean age 63.3 ± 6.73 years). Table 1 shows the sociodemographic and clinical characterization of the sample and between-group differences at the baseline.
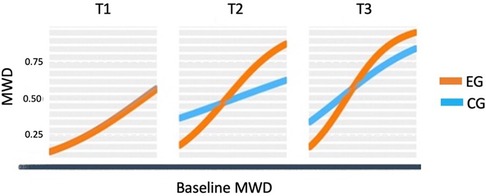
Figure 1. Graphic representation of the between-group differences in the average MWD over time (fitted data), at each time point.
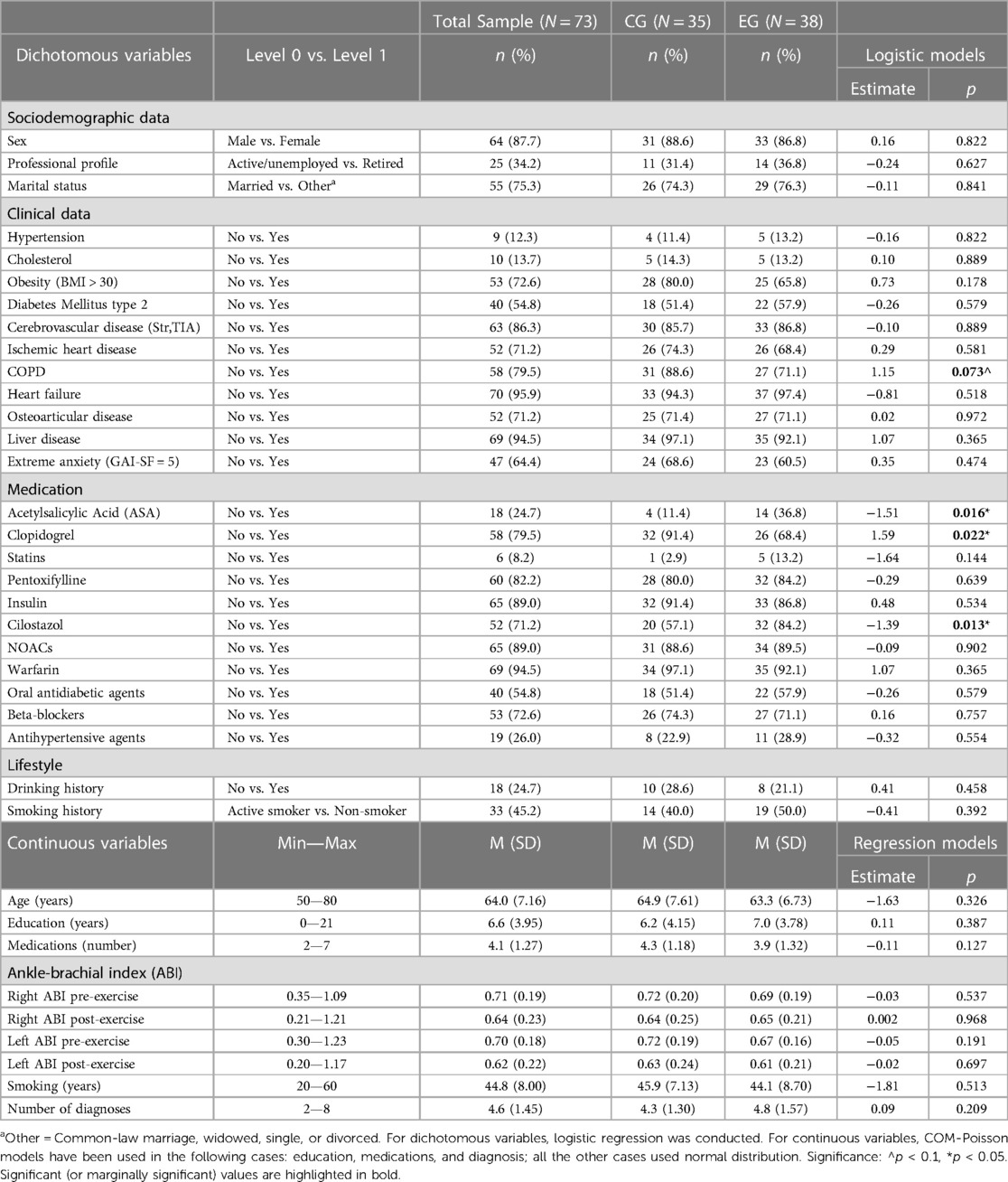
Table 1. Sociodemographic and clinical characterization of the sample and between-group differences at the baseline.
There was a significant main effect of time in primary and secondary outcomes. Results of the mixed-effects models show that the average MWD improved significantly over time for the whole sample (from T1 to T2 and from T2 to T3). The average PFWD and FWD increased over time, but from T2 to T3, the increase was insignificant. The same was true for 6 MWD.
Regarding secondary outcomes, the average QoL disease-related increased significantly over time, from T1 to T2 and from T2 to T3. The average physical and mental QoL increased over time, but from T2 to T3, the increase was not significant. The average WIQ distance increased over time, but from T2 to T3, the increase was only borderline significant. The average WIQ speed increased over time, but from T2 to T3, the increase was not significant. The average WIQ stairs increased from T1 to T2 and T2 to T3 over time. Results are shown in Table 2.
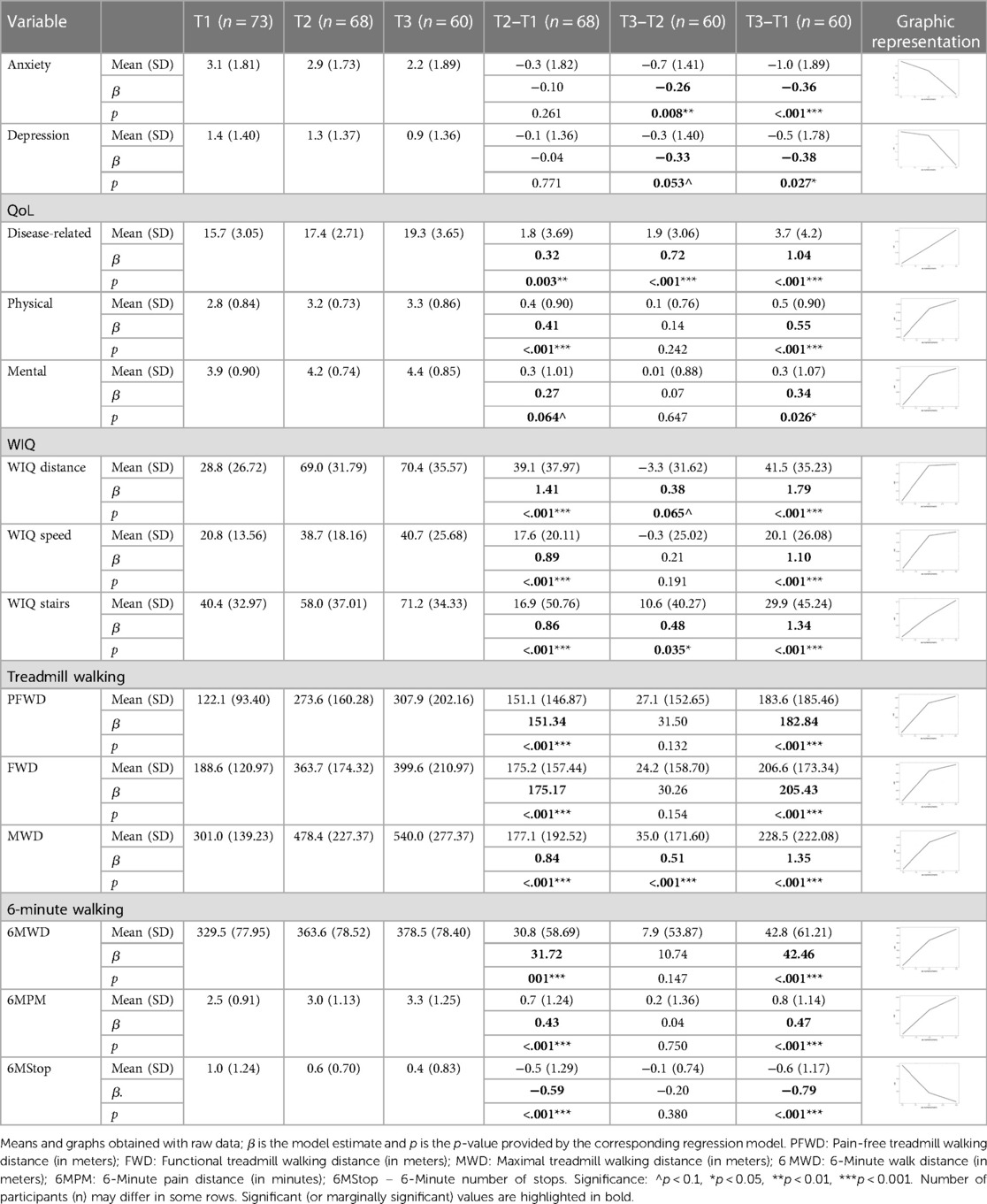
Table 2. Differences in the main variables of interest for the total sample, over time.
By the end of the study, no significant between-group differences regarding the average of the primary outcomes were found. Results are shown in Table 3. Notice, however, that the sample size of this study only allowed to detection of large effect sizes, which means that increasing the sample size would probably allow uncovering of some medium or small effects.
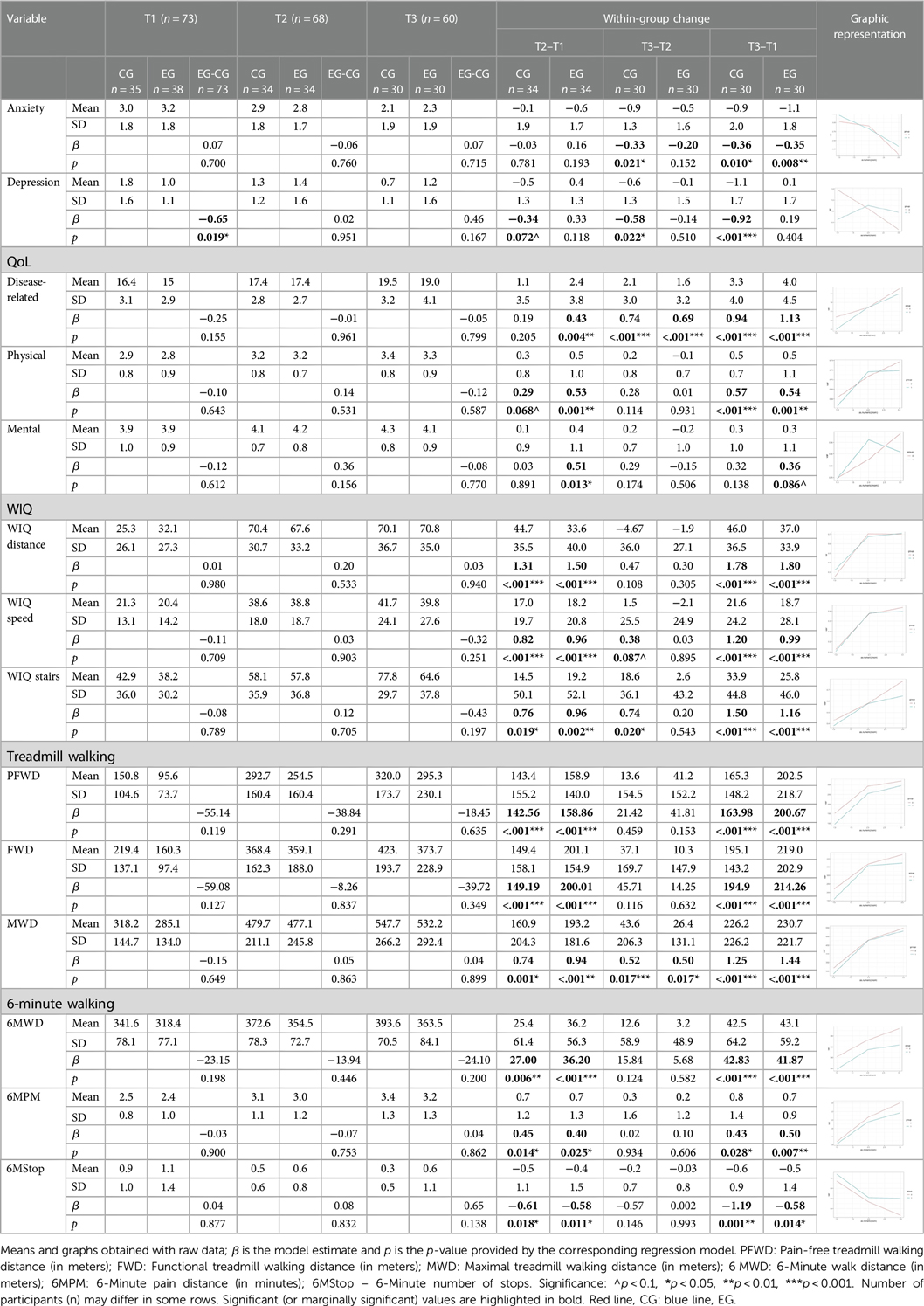
Table 3. Between-group differences in the main variables of interest, over time.
Therefore, we have proceeded with further modeling analysis in order to understand whether the relationships of the primary outcomes with other variables have evolved differently for the two groups over time. First, we performed an internal analysis of the outcome to investigate how baseline scores evolved over time. Second, we conducted an external analysis to understand how other baseline variables affected the outcome as time went by. To perform the group comparison, several multilevel models with three-way interactions of the form “Variable x Group x Moment” have been evaluated. Interestingly, this modeling analysis only detected between-group differences for the MWD outcome. More specifically, unlike the control group, in the EG the MWD has never lost its association with the baseline scores over time (more than that, time strengthened this relationship). Moreover, patients of the EG with no extreme anxiety showed a higher increase in the MWD by the 6-month follow-up, compared with the CG. We emphasize that the sample size of this study only allowed to detect large effect sizes and therefore, all significant effects found in this study are strong. Details of these two models are given below.
Although from the quantitative point of view, there is no significant between-group difference in the MWD improvement (score discounting the baseline MWD) over time, after controlling for participants' differences at the baseline, it is possible to uncover some important differences. Results are shown in Table 4. More specifically, the predictive power of participants' baseline MWD over time was significantly different for the two groups. In the CG, this predictive power did not vary significantly over time; however, in the EG, it increased and became significantly higher at T2 (estimate difference of 4.89, p = 0.013) and T3 (estimate difference of 4.67, p = 0.024, at T3), when compared to the CG. This means that in the EG, a part of the improvement is explained by participants' baseline MWD, in contrast to the CG, where this causal relationship was not observed. Thus, participants from the EG improved a proportion of their baseline MWD and, as a result, the higher the baseline MWD, the higher the improvement achieved afterward. This between-group difference is particularly prominent in the 6-month follow-up, with an improvement of 5.17 (p = 0.003) in the EG and 0.44 (p = 0.779) in the CG. Thus, the baseline MWD only predicts the MWD improvement at T3 in the EG. Notice that this is a qualitative between-groups difference in the MWD over time.

Table 4. Between-group differences in the MWD over time: (a) the predictive power of baseline MWD, and (b) the extreme anxiety diagnosis at the baseline.
The predictive power of MWD was intensified over time, meaning that participants from the EG benefited from the WalkingPad app, except those with a weak walking ability (Figure 1). It also indicates that the MWD in the EG, unlike in the CG, exhibited strong stability over time.
Furthermore, anxiety (fixed at baseline) had a significant between-group different effect on MWD (depression also showed a similar result, but it disappeared when controlling for anxiety). Except for patients with extreme anxiety symptoms at the baseline, the EG showed a higher increase in the MWD at T3 (increase difference = 0.91, p = 0.026). For patients with extreme anxiety symptoms at the baseline, the increase from T1 to T3 was not significantly different for the two groups (increase difference = 0.75, p = 0.137) (Figures 2, 3).
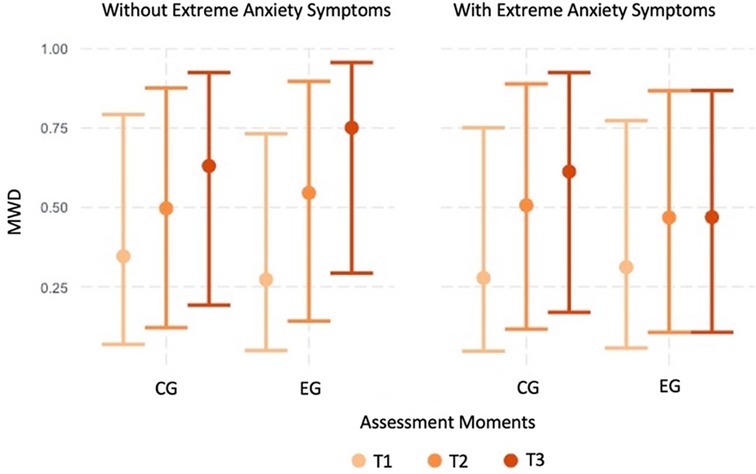
Figure 2. Graphic representation of the between-group differences in the average MWD over time (fitted data), for participants with and without extreme anxiety symptoms.
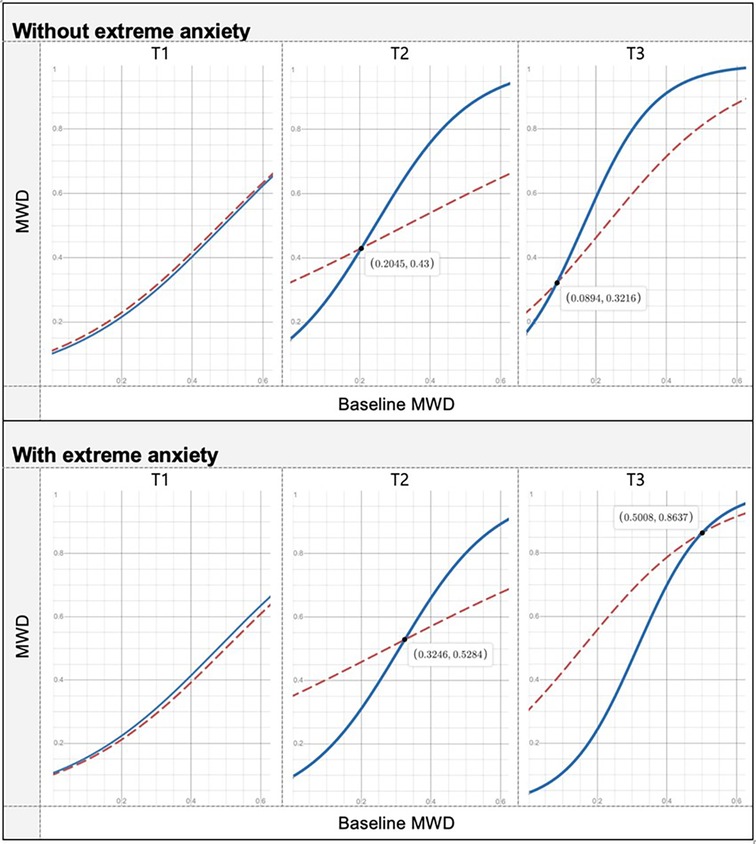
Figure 3. Graphic representation of the between-group differences in the average MWD over time (fitted data), at each time point, separating the cases with and without extreme anxiety. Red line, CG: blue line, EG.
The WalkingPad program significantly improved MWD over time (from T1 to T2 and from T2 to T3) and PFWD and FWD from T1 to T2. If, on the one hand, improvements in distances are achieved essentially in the first 3 months, on the other hand, the other three months are essential to improve the MWD. Therefore, these results support the 6-month duration of an HBET. Furthermore, the results found for walking distances on treadmill evaluation were much higher than those found in other studies that also focused on the effects of an HBET supported by a psychological intervention based on behavioral change or education (53–56). However, only one study had a 6-month follow-up and did not achieve these promising results (55). The increase in 6 MWD was also significant from T1 to T2 (32 m), similar to other studies (1, 53–56) but not from T2 to T3, as expected (57, 58). These results may reflect the effectiveness of the behavior change intervention, carried out face-to-face and by telephone in the 6 months, in promoting a more integrated type of motivation and, consequently, greater adherence to physical exercise (10, 12, 23–28). The WalkingPad app was innovative as it effectively improved MWD at 6 months.
Walking distance and speed increased in the first 3 months but not in the last three. In turn, climbing stairs increased over time: from T1 to T2 and T2 to T3.
Disease-related QoL increased significantly over time, but general mental and physical QoL only increased from T1 to T2, suggesting that the effect of the WalkingPad program on disease-specific QoL was significant and progressive, reinforcing the advantage of a 6-month program to achieve improvements in quality of life. QoL of PAD patients is significantly associated with claudication pain, walking distance, and stairs climbing (7); thus, as walking distances and skills increase, so does QoL over the 6 months. General physical and mental QoL is subject to the influence of other external factors and only increases in the first 3 months, although it proves the effectiveness of physical exercise for the subjective perception of QoL.
Regarding the experimental group, the WalkingPad app positively affects patients' MWD, with higher baseline scores being associated with a stronger positive effect over time. However, this positive effect was not observed for people with weak walking ability and extreme anxiety symptomatology at the baseline. Therefore, this app may be recommended to people who score mid-to-high at the baseline MWD unless they have extreme anxiety symptomatology. For people scoring low at the MWD or having extreme anxiety symptomatology at the baseline, the app did not have a significant effect contrary to the expectations and results found in other studies (14, 16, 59, 60).
The WalkingPad app may be recommended to PAD patients, except for those with weak walking ability and extreme anxiety symptoms. We hypothesized that the app can trigger more anxiety in people who are already anxious. Thus, in clinical practice, the health professional must assess the patient's anxiety to understand whether the physical exercise prescription should involve the app or not.
The 6-month duration is crucial to achieving results in maximal walking distance and QoL, as well as the behavioral change intervention that seems to have been the essential driver for promising results. Thus, this is the first study with a 6-month follow-up that achieved promising results in walking distances and quality of life. The behavior change intervention carried out in person and by telephone during the 6 months was decisive for the effectiveness of the physical exercise program, considering the importance of behavior change for the consistent adoption of a healthy habit. This study also shows that physical exercise programs should be at least 6 months in duration because disease-related QoL increased significantly over time, but overall mental and physical QoL only increased from T1 to T2, suggesting that the effect of WalkingPad program on QoL was progressive and not immediate. Furthermore, this study suggests that a smartphone app may not be useful for all patients. In fact, the app may be recommended for people with medium to high baseline MWD scores, unless they have extreme anxiety symptomatology, and for those who still have good walking skills (high MWD) at baseline, associated with a stronger positive effect over time.
This study has some limitations that must be recognized. The sample was collected in only one hospital, being a unicentric study, and the results cannot be generalized to structured and supervised interventions (SET). Furthermore, the lack of gender heterogeneity in the sample (larger number of male patients) and the single-blind nature of the study, when the ideal was to be a double-blind study, must be recognized as limitations.
The sample size was small. Data were analysed according to the most recent statistical recommendations for longitudinal data, namely, using multilevel (or mixed-effect) models with suitable families of distributions. Several models have been investigated and we only report those (two) that were able to detect significant effects. Models are like microscopes whose augmenting power is defined by the sample size, with larger size providing greater power. We emphasize that the sample size of this study only allowed the detection of large effect sizes (increasing the sample would probably detect more effects), and therefore, all significant effects found in this study are strong. For this reason, we believe that our results will be easily corroborated by future studies, as long as they use the same conditions and the same statistical methodology (R codes used in this project can be provided on formal request).
The study lasted only 6 months, and the durability of the program's effects was unknown. Thus, more research is needed to determine the durability of these findings. An exploratory and usability study must be carried out to understand which application functionalities should be improved to promote the other results, and the same protocol should be applied, including more intense and personalized psychological follow-up for more anxious people. Furthermore, future studies should test the differences between gender in the use of the app and how this use influences adherence to physical exercise and outcomes.
A 6-month home exercise program supported by a behavior change intervention improved distances and walking skills as well as the physical, mental, and disease-related quality of life among adults with PAD and IC. The group that used the WalkingPad app improved their MWD in 6 months compared to the control group, except for patients with poor walking ability and extreme anxiety symptoms, which suggest the effectiveness of the WalkingPad app for patients with high walking ability and no severe anxiety symptoms.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
The studies involving humans were approved by Centro Hospitalar Universitário Santo António Porto Research Ethics Committee. The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
IS: Investigation, Methodology, Conceptualization, Funding acquisition, Supervision, Writing – review & editing. CM: Writing – original draft, Formal analysis. SP: Writing – original draft, Data curation, Investigation, Methodology. RO: Data curation, Writing – original draft. CV: Data curation, Writing – original draft. LM: Data curation, Writing – review & editing. DS: Data curation, Writing – review & editing. DG: Data curation, Writing – review & editing. HP: Conceptualization, Investigation, Writing – review & editing.
The author(s) declare financial support was received for the research, authorship, and/or publication of this article.
This study is financed by the FEDER -European Regional Development Fund through NORTE 2020 – Northern Regional Operational Program, under PORTUGAL 2020 and by national funds, through the FCT – Foundation for Science and Technology, within the scope of the project with the reference NORTE-01-0145-FEDER-031161-PTDC/MEC-VAS/31161/2017. The research of CSM is supported by FCT (SFRH/BPD/84709/2012 under the QREN–POPH–Advanced Training, subsidized by the European Social Fund and by national MEC funds) and by CMUP, which is financed by national funds through FCT under the project with reference UIDB/00144/2020. IS was also supported by UIDB/00215/2020; UIDP/00215/2020; LA/P/0064/2020.
The authors would like to thank all the participants, as without them this study would not have been possible.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fcvm.2023.1272897/full#supplementary-material
1. Bearne LM, Volkmer B, Peacock J, Sekhon M, Fisher G, Galea Holmes MN, et al. Effect of a home-based, walking exercise behavior change intervention vs usual care on walking in adults with peripheral artery disease: the MOSAIC randomized clinical trial. JAMA. (2022) 327(14):1344–55. doi: 10.1001/jama.2022.3391
2. Gerhard-Herman MD, Gornik HL, Barrett C, Barshes NR, Corriere MA, Drachman DE, et al. 2016 AHA/ACC guideline on the management of patients with lower extremity peripheral artery disease: executive summary. Circulation. (2017) 135:686–725. doi: 10.1016/j.jacc.2016.11.008
3. Norgren L, Hiatt WR, Dormandy JA, Nehler MR, Harris KA, Fowkes FGR. Inter-society consensus for the management of peripheral arterial disease (TASC II). J Vasc Surg. (2007) 45:5–67. doi: 10.1016/j.jvs.2006.12.037
4. Bullard T, Ji M, An R, Trinh L, MacKenzie M, Mullen SP. A systematic review and meta-analysis of adherence to physical activity interventions among three chronic conditions: cancer, cardiovascular disease, and diabetes. BMC Public Health. (2019) 19(1):636–46. doi: 10.1186/s12889-019-6877-z
5. Golledge J, Singh TP, Alahakoon C, Pinchbeck J, Yip L, Moxon JV, et al. Meta-analysis of clinical trials examining the benefit of structured home exercise in patients with peripheral artery disease. Br J Surg. (2019) 106:319–31. doi: 10.1002/bjs.11101
6. Ekkekakis P, Dafermos M. Exercise is a many-splendored thing, but for some it does not feel so splendid: staging a resurgence of hedonistic ideas in the quest to understand exercise behavior. In: Acevedo EO, editor. The Oxford handbook of exercise psychology. New York, NY, US: Oxford University Press (2012). p. 295–333. (Oxford library of psychology).
7. Kim M, Kim Y, Ryu GW, Choi M. Functional status and health-related quality of life in patients with peripheral artery disease: a cross-sectional study. Int J Environ Res Public Health. (2021) 18:1–10. doi: 10.3390/ijerph182010941.
8. Aragão JA, De Andrade LGR, Neves OMG, Aragão ICS, Aragão FMS, Reis FP. Anxiety and depression in patients with peripheral arterial disease admitted to a tertiary hospital. J Vasc Bras. (2019) 18:1–11. doi: 10.1590/1677-5449.190002
9. Ragazzo L, Puech-Leao P, Wolosker N, de Luccia N, Saes G, Ritti-Dias RM, et al. Symptoms of anxiety and depression and their relationship with barriers to physical activity in patients with intermittent claudication. Clinics. (2021) 76:1–6. doi: 10.6061/clinics/2021/e1802
10. Davis R, Campbell R, Hildon Z, Hobbs L, Michie S. Theories of behaviour and behaviour change across the social and behavioural sciences: a scoping review. Health Psychol Rev. (2015) 9(3):323–44. doi: 10.1080/17437199.2014.941722
11. Galea MN, Weinman JA, White C, Bearne LM. Do behaviour-change techniques contribute to the effectiveness of exercise therapy in patients with intermittent claudication? A systematic review. Eur J Vasc Endovasc Surg. (2013) 46(1):132–41. doi: 10.1016/j.ejvs.2013.03.030
12. Michie S, Prestwich A. Are interventions theory-based? Development of a theory coding scheme. Health Psychol. (2010) 29(1):1–8. doi: 10.1037/a0016939
13. Wann-Hansson C, Wennick A. How do patients with peripheral arterial disease communicate their knowledge about their illness and treatments? A qualitative descriptive study. BMC Nurs. (2016) 15(1):1–9. doi: 10.1186/s12912-016-0151-9
14. Duscha BD, Piner LW, Patel MP, Crawford LE, Jones WS, Patel MR, et al. Effects of a 12-week mHealth program on functional capacity and physical activity in patients with peripheral artery disease. Am J Cardiol. (2018) 122:879–84. doi: 10.1016/j.amjcard.2018.05.018
15. Khambati H, Boles K, Jetty P. Google maps offers a new way to evaluate claudication. J Vasc Surg. (2017) 65:1467–72. doi: 10.1016/j.jvs.2016.11.047
16. Kim M, Kim C, Kim E, Choi M. Effectiveness of mobile health–based exercise interventions for patients with peripheral artery disease: systematic review and meta-analysis. JMIR Mhealth Uhealth. (2021) 9(2):1–15. doi: 10.2196/24080
17. Veiga C, Pedras S, Oliveira R, Paredes H, Silva I. A systematic review on smartphone use for activity monitoring during exercise therapy in intermittent claudication. J Vasc Surg. (2022) 76(6):1734–41. doi: 10.1016/j.jvs.2022.04.045
18. Paldán K, Steinmetz M, Simanovski J, Rammos C, Ullrich G, Jánosi RA, et al. Supervised exercise therapy using mobile health technology in patients with peripheral arterial disease: pilot randomized controlled trial. JMIR Mhealth Uhealth. (2021) 9(8):1–15. doi: 10.2196/24214
19. Aboyans V, Ricco JB, Bartelink MLEL, Björck M, Brodmann M, Cohnert T, et al. ESC guidelines on the diagnosis and treatment of peripheral arterial diseases, in collaboration with the European society for vascular surgery (ESVS). Eur Heart J. (2017) 2018(39):763–816. doi: 10.1093/eurheartj/ehx095
20. Treat-Jacobson D, McDermott MM, Bronas UG, Campia U, Collins TC, Criqui MH, et al. Optimal exercise programs for patients with peripheral artery disease. Circulation. (2019) 139:10–33. doi: 10.1161/CIR.0000000000000623
21. Makris GC, Lattimer CR, Lavida A, Geroulakos G. Availability of supervised exercise programs and the role of structured home-based exercise in peripheral arterial disease. Eur J Vasc Endovasc Surg. (2012) 44:569–75. doi: 10.1016/j.ejvs.2012.09.009
22. Deci E, Ryan R. Intrinsic motivation and self-determination in human behavior. 1st ed. New York: Springer (1985).
23. Deci E, Ryan R. Self-determination theory: a macrotheory of human motivation, development, and health. Can Psychol-Psychol Can. (2008) 49:182–5. doi: 10.1037/a0012801
24. Ryan RM, Deci EL. The darker and brighter sides of human existence: basic psychological needs as a unifying concept. Psychol Inq. (2000) 11(4):319–38. doi: 10.1207/S15327965PLI1104_03
25. Miller W, Rollnick S. Motivational interviewing: Helping people change. 3rd ed. New York: Guilford Press (2012).
26. Patrick H, Williams GC. Self-determination theory: its application to health behavior and complementarity with motivational interviewing. Int J Behav Nutr Phys Act. (2012) 9:1–12. doi: 10.1186/1479-5868-9-18
27. Goode AD, Reeves MM, Eakin EG. Telephone-delivered interventions for physical activity and dietary behavior change: an updated systematic review. Am J Prev Med. (2012) 42:81–8. doi: 10.1016/j.amepre.2011.08.025
28. Huffman JC, Harnedy LE, Massey CN, Carrillo A, Feig EH, Chung WJ, et al. A phone and text message intervention to improve physical activity in midlife: initial feasibility testing. Health Psychol Behav Med. (2022) 10(1):291–315. doi: 10.1080/21642850.2022.2049796
29. Yesavage J, Rose T, Lum O. Development and validation of a geriatric depression screening scale: a preliminary report. J Psychiatr Res. (1983) 17:37–49. doi: 10.1016/0022-3956(82)90033-4
30. Santos AJ, Nunes B, Kislaya I, Gil AP, Ribeiro O. Validation study of a reduced version of the geriatric depression scale in Portugal. Análise Psicológica. (2019) 37:405–15. doi: 10.14417/ap.1505
31. Byrne GJ, Pachana NA. Development and validation of a short form of the geriatric anxiety inventory - the GAI-SF. Int Psychogeriatr. (2011) 23:125–31. doi: 10.1017/S1041610210001237
32. Silva L dos SV e, de Oliveira GM, Yokomizo JE, Saran LF, Bottino CM de C, Yassuda MS. The geriatric anxiety inventory in primary care: applicability and psychometric characteristics of the original and short form. Arch Clin Psychiatry. (2016) 43:103–6. doi: 10.1590/0101-60830000000094
33. Kruidenier LM, Nicolaï SPA, Willigendael EM, de Bie RA, Prins MH, Teijink JAW. Functional claudication distance: a reliable and valid measurement to assess functional limitation in patients with intermittent claudication. BMC Cardiovasc Disord. (2009) 9:1–7. doi: 10.1186/1471-2261-9-9
34. Treat-Jacobson D, McDermott MM, Beckman JA, Burt MA, Creager MA, Ehrman JK, et al. Implementation of supervised exercise therapy for patients with symptomatic peripheral artery disease. Circulation. (2019) 140:700–10. doi: 10.1161/CIR.0000000000000727
35. ATS Committee on Proficiency Standards for Clinical Pulmonary Function Laboratories. ATS statement: guidelines for the six-minute walk test. Am J Respir Crit Care Med. (2002) 166(1):111–7. doi: 10.1164/ajrccm.166.1.at1102. Erratum in: Am J Respir Crit Care Med. (2016) 193(10):1185.12091180
36. Nordanstig J, Wann-Hansson C, Karlsson J, Lundström M, Pettersson M, Morgan MBF. Vascular quality of life questionnaire-6 facilitates health-related quality of life assessment in peripheral arterial disease. J Vasc Surg. (2014) 59:700–7. doi: 10.1016/j.jvs.2013.08.099
37. Larsen ASF, Reiersen AT, Jacobsen MB, Kløw NE, Nordanstig J, Morgan M, et al. Validation of the vascular quality of life questionnaire-6 for clinical use in patients with lower limb peripheral arterial disease. Health Qual Life Outcomes. (2017) 15:184. doi: 10.1186/s12955-017-0760-3
38. Correia M, Andrade-Lima A, Oliveira PL, Domiciano RM, Domingues WJ, Wolosker N, et al. Translation and validation of the Brazilian-Portuguese short version of vascular quality of life questionnaire in peripheral artery disease patients with intermittent claudication symptoms. Ann Vasc Surg. (2018) 51:48–54. doi: 10.1016/j.avsg.2018.02.026
39. Ware J, Kosinski M, Keller S. SF-12: how to score the SF-12 physical and mental health summary scales. 2nd ed. Boston, MA: The Health Institute (1995).
40. Ferreira PL, Noronha Ferreira L, Nobre Pereira L. Medidas sumário física e mental de estado de saúde para a população portuguesa. Revista Portuguesa de Saude Publica. (2012) 30(2):163–71. doi: 10.1016/j.rpsp.2012.12.007
41. Nicolaï SPA, Kruidenier LM, Rouwet EV, Graffius K, Prins MH, Teijink JAW. The walking impairment questionnaire: an effective tool to assess the effect of treatment in patients with intermittent claudication. J Vasc Surg. (2009) 50:89–94. doi: 10.1016/j.jvs.2008.12.073
42. Mayo NE, Scott S. Evaluating a complex intervention with a single outcome may not be a good idea: an example from a randomised trial of stroke case management. Age Ageing. (2011) 40(6):718–24. doi: 10.1093/ageing/afr061
43. Vickerstaff V, Ambler G, Omar RZ. A comparison of methods for analysing multiple outcome measures in randomised controlled trials using a simulation study. Biom J. (2021) 63(3):599–615. doi: 10.1002/bimj.201900040
44. Zhang Z, Mai Z, Yang M, Xu Z, McNamara C. WebPower: Basic and Advanced Statistical Power Analysis. (2018).
45. Perugini M, Gallucci M, Costantini G. A practical primer to power analysis for simple experimental designs. Int Rev Soc Psychol. (2018) 31(1):1–23. doi: 10.5334/irsp.181
46. Cohen J. Statistical power analysis for the behavioral sciences second edition. 2nd ed. New York: Lawrence Erlbaum Associates (1988).
47. Bates D, Mächler M, Bolker BM, Walker SC. Fitting linear mixed-effects models using lme4. J Stat Softw. (2015) 67(1):1–48. doi: 10.18637/jss.v067.i01
48. Kuznetsova A, Brockhoff PB, Christensen RHB. Lmertest package: tests in linear mixed effects models. J Stat Softw. (2017) 82(13):1–26. doi: 10.18637/jss.v082.i13
49. Brooks ME, Kristensen K, Van Benthem KJ, Magnusson A, Berg CW, Nielsen A, et al. glmmTMB balances speed and flexibility among packages for zero-inflated generalized linear mixed modeling. R J. (2017) 9(2):378–400. doi: 10.32614/RJ-2017-066
51. Winter B. Linear models and linear mixed effects models in R with linguistic applications. Arxiv (2013).
52. Gelman A, Hill J, Yajima M. Why we (usually) don’t have to worry about multiple comparisons. J Res Educ Eff. (2012) 5(2):189–211. doi: 10.1080/19345747.2011.618213
53. Collins TC, Lunos S, Carlson T, Henderson K, Lightbourne M, Nelson B, et al. Effects of a home-based walking intervention on mobility and quality of life in people with diabetes and peripheral arterial disease: a randomized controlled trial. Diabetes Care. (2011) 34(10):2174–9. doi: 10.2337/dc10-2399
54. Gardner AW, Parker DE, Montgomery PS, Scott KJ, Blevins SM. Efficacy of quantified home-based exercise and supervised exercise in patients with intermittent claudication: a randomized controlled trial. Circulation. (2011) 123(5):491–8. doi: 10.1161/CIRCULATIONAHA.110.963066
55. Collins T, Geana M, Overton K, Benton M, Lu L, Khan F, et al. Use of a smartphone app versus motivational interviewing to increase walking distance and weight loss in overweight/obese adults with peripheral artery disease: pilot randomized trial. JMIR Form Res. (2022) 6(2):1–10. doi: 10.2196/30295
56. Tew GA, Humphreys L, Crank H, Hewitt C, Nawaz S, Al-Jundi W, et al. The development and pilot randomised controlled trial of a group education programme for promoting walking in people with intermittent claudication. Vasc Med. (2015) 20(4):348–57. doi: 10.1177/1358863X15577857
57. Gardner AW, Parker DE, Montgomery PS, Blevins SM. Step-monitored home exercise improves ambulation, vascular function, and inflammation in symptomatic patients with peripheral artery disease: a randomized controlled trial. J Am Heart Assoc. (2014) 3(5):1–11. doi: 10.1161/JAHA.114.001107
58. McDermott MM, Liu K, Guralnik JM, Criqui MH, Spring B, Tian L, et al. Home-based walking exercise intervention in peripheral artery disease: a randomized clinical trial. JAMA. (2013) 310:57–65. doi: 10.1001/jama.2013.7231
59. Argent R, Daly A, Caulfield B. Patient involvement with home-based exercise programs: can connected health interventions influence adherence? JMIR Mhealth Uhealth. (2018) 6:47. doi: 10.2196/mhealth.8518
Keywords: home-based exercise therapy, peripheral arterial disease, intermittent claudication, quality of life, smartphone application
Citation: Silva I, Moreira CS, Pedras S, Oliveira R, Veiga C, Moreira L, Santarém D, Guedes D and Paredes H (2023) Effect of a monitored home-based exercise program combined with a behavior change intervention and a smartphone app on walking distances and quality of life in adults with peripheral arterial disease: the WalkingPad randomized clinical trial. Front. Cardiovasc. Med. 10:1272897. doi: 10.3389/fcvm.2023.1272897
Received: 4 August 2023; Accepted: 25 October 2023;
Published: 22 November 2023.
Edited by:
Han Feng, Tulane University, United StatesReviewed by:
Hadi Younes, Tulane University, United States© 2023 Silva, Moreira, Pedras, Oliveira, Veiga, Moreira, Santarém, Guedes and Paredes. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Susana Pedras c3VzYW5hcGVkcmFzQGdtYWlsLmNvbQ==
†These authors have contribute equally to this work and share first authorship
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.