 Luise Adam1,2,3
Luise Adam1,2,3 Oliver Baretella1,2Martin Feller1,2Manuel Raphael Blum1,2Dimitrios David Papazoglou2Benoit Boland4,5Drahomir Aujesky2
Oliver Baretella1,2Martin Feller1,2Manuel Raphael Blum1,2Dimitrios David Papazoglou2Benoit Boland4,5Drahomir Aujesky2 Stéphanie Baggio1,6
Stéphanie Baggio1,6 Nicolas Rodondi1,2*
Nicolas Rodondi1,2*
- 1Institute of Primary Health Care (BIHAM), University of Bern, Bern, Switzerland
- 2Department of General Internal Medicine, Inselspital, Bern University Hospital, University of Bern, Bern, Switzerland
- 3Division of Angiology, Gefässzentrum, Kantonsspital Baden, Baden, Switzerland
- 4Geriatric Medicine, Cliniques Universitaires Saint-Luc, Brussels, Belgium
- 5Health Science Research Institute, UCLouvain, Louvain, Belgium
- 6Population Health Laboratory (#PopHealthLab), University of Fribourg, Fribourg, Switzerland
Background: Statin therapy in multimorbid older individuals with polypharmacy is controversial, particularly in primary prevention of cardiovascular disease. Thereby, physicians must weigh potential benefits against potential side effects, drug-drug interactions, and limited life expectancy.
Aim: To assess the prevalence and determinants of potentially inappropriate statin therapy in multimorbid older patients.
Methods: We conducted a cross-sectional analysis of patients aged ≥70 years with multimorbidity and polypharmacy in the Swiss study center of OPERAM, a cluster-randomized trial on pharmacotherapy optimization to reduce drug-related hospital admissions. We assessed potential underuse (no statin but formal indication) and potential overuse (statin but no formal indication, including predicted >60% one-year mortality based on the Walter Score) based on current guidelines for patients in secondary and primary cardiovascular prevention. We assessed the association of potential statin overuse and underuse with six patient characteristics (age, gender, number of diagnoses, number of medications, mental impairment, being housebound) in LASSO-selection analyses.
Results: Of 715 multimorbid older adults (79.7 ± 6.5 years, 39.9% women), 337 (47%) were on statin. Statin therapy was appropriate in 474 (66.3%), underused in 130 (18.2%), and overused in 111 (15.5%) patients. In participants in secondary cardiovascular prevention (n = 437), being female (odds ratio [OR] 2.65, 95% confidence interval [CI] 1.67–4.22) was significantly associated with potential underuse while being housebound (OR 3.53, 95%CI 1.32–9.46) and taking ≥10 medications (OR 1.95,95%CI 1.05–3.67) were associated with potential overuse. In participants in primary cardiovascular prevention (n = 278), 28.1% were potentially under- (9%) or overusing (19%) a statin, with no identified risk factor.
Conclusion: A third of hospitalized multimorbid older patients with polypharmacy potentially (either) overused or underused statin therapy. Among patients in secondary cardiovascular prevention, women were at risk for potential statin underuse. Housebound patients and those taking ≥10 medications were at risk for potential overuse of a statin. Physicians should carefully evaluate the indication for statin prescription in multimorbid older patients with polypharmacy.
Introduction
As people age, they are increasingly likely to suffer from more than one disease (multimorbidity): 60% of adults >65 suffer from more than three chronic diseases (1). These multimorbid patients may take different drugs to treat each disease (polypharmacy) (2), some of which may be inappropriate (3). Multimorbid patients are also at risk of underusing drugs (4). Both under- and overuse (inappropriate prescribing) may lead to avoidable hospital admissions and reduce the patient's quality of life (5–7). Therefore, polypharmacy among the multimorbid older patients must be managed carefully to meet the needs of the aging population. Multimorbidity, older age, and polypharmacy are associated with cardiovascular risk factors and disease (8): more than 50% of multimorbid patients have cardiovascular disease (CVD) (9) and are often prescribed statins to reduce cardiovascular events (CVE) and mortality in primary and secondary prevention (10, 11).
Statins are effective for secondary prevention of CVD even in old patients, with data until 82 years (12), but guidelines still suggest physicians consider individual factors that could influence their decision to start, change, or end statin therapy in older patients (13, 14). A small randomized controlled trial even showed that stopping statins in patients with life-limiting disease was safe, had no significant effect on mortality, and slightly increased quality of life (15, 16).
For primary prevention of atherosclerotic CVD, the current European Society of Cardiology and American Heart Association (AHA) guidelines recommend statins to match individual cardiovascular risk, setting the minimum bar at ≥5 to <10% 10-year risk of fatal and non-fatal atherosclerotic CVD (ASCVD) (17–19). Cardiovascular risk can be calculated with tools like the PROCAM-SCORE or SCORE2 (20, 21), which include age, gender, and known modifiable cardiovascular risk factors. Among older adults, the evidence of benefits of statins for primary prevention is less clear. The recent ESC guidelines for elderly recommend risk-factor treatment in older patients (≥70 years) with very high-risk for CVD (≥15% 10-year risk of CVD according to SCORE-OP2,) and apparently healthy older high-risk patients (7.5%–15% 10-year CVD risk, Class IIa recommendation) but there is insufficient evidence for low-density lipoprotein cholesterol (LDL-C) targets (22). The AHA guidelines neither suggest nor discourage statin prescription as primary prevention for this group of patients and they encourage physicians to individualize their recommendations, taking into account life expectancy, patient preferences, co-morbidities, and other factors (evidence level E) (13, 18, 19).
Based on current evidence, physicians should carefully consider whether to prescribe drug treatment in multimorbid older patients with polypharmacy since data have shown that such patients are at risk for inappropriate prescription (underuse and overuse) (3). To date, there is little data on whether statins are appropriately prescribed to multimorbid older patients with polypharmacy, and risk factors associated with statin under- and over prescription.
To overcome this research gap, we conducted a cross-sectional analysis of the OPERAM trial (OPtimising thERapy to prevent Avoidable hospital admissions in Multimorbid older people) to assess the prevalence and determinants of potentially inappropriate statin therapy in multimorbid older hospitalized patients.
Methods
We included participants from the Swiss study center (Bern University Hospital) of the cluster-randomized controlled OPERAM trial with detailed information on statin use, related factors and lipid values. A detailed protocol of OPERAM and its main results were published elsewhere (3, 23). We included only Swiss participants as the adjudication algorithm was based on local guidelines. Since the OPERAM trial studied a systematic drug review vs. usual care, we chose a cross-sectional study design at hospital admission, prior to the drug review, in order to receive the most accurate real life reflection.
Study population
The OPERAM trial included multimorbid (more than three diagnosed chronic diseases) patients ≥70 years old with polypharmacy (five or more chronic medications). Patients were excluded from this analysis if they were missing information essential for assessing appropriateness of the statin therapy (e.g., missing lipid values for primary prevention).
Outcomes: statin therapy appropriateness
Patients were classed according to ICD-10 coded diagnoses at baseline (Table 1) into patients with and without ASCVD. We classed patients with an ICD-10 code for ASCVD into secondary prevention and patients without ASCVD into primary prevention.
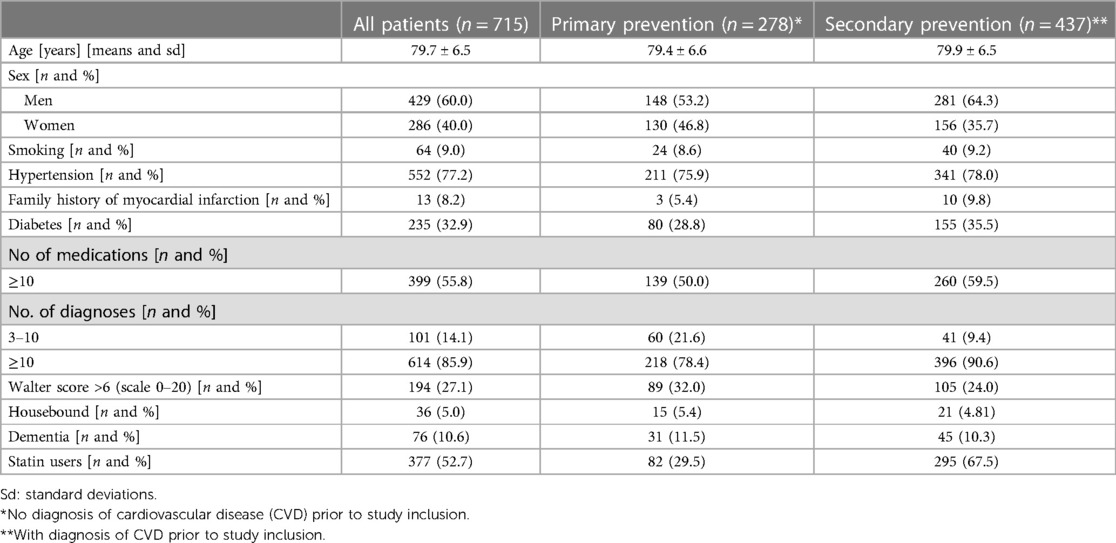
Table 1. Baseline characteristics.
Clinical ASCVD were defined as acute coronary syndromes, history of myocardial infarction, stable or unstable angina, coronary or other arterial revascularization, stroke, TIA, or peripheral arterial disease presumed to be of atherosclerotic origin, which occurred before study inclusion (24), and visceral atherosclerotic manifestations (Supplementary Table S2).
Patients who took a statin in accordance to current guidelines were classed as receiving appropriate statin therapy. Patients who took a statin without formal indication (overuse) or who did not receive statin therapy when statins were formally indicated (underuse) were classed as receiving “inappropriate statin therapy”.
To assess appropriateness for patients in primary prevention, we calculated the PROCAM-Score, adapted for Switzerland (25), as it is the most used risk score in Switzerland (26). We collected lipid profiles either during index hospitalization (hospitalization at the time of inclusion in the OPERAM trial) or from the patient's general practitioner (GP) whenever possible, preferably collected before lipid-lowering therapy initiation. If those values were unavailable, we used the last available lipid profile, either from their GP or from the OPERAM baseline visit. For patients with available lipid-values that were taken during statin therapy for primary prevention, we estimated the possible LDL-C value prior to statin initiation using the mean reduction values by the statin taken (27) in order to be able to better estimate the cardiovascular risk.
Predictors
We considered all patients with a diagnosis of cardiovascular ischemic disease to be patients who needed secondary prevention for cardiovascular events. Thus, all patients with cardiovascular disease were considered to be underusing a statin if they were not taking a statin. For all patients, we calculated the Walter Score to determine individual 1-year mortality risk (28); we considered a score >6 (>60% 1-year mortality) to be potentially life limiting. Since current evidence suggests that statin therapy offers no benefit when prescribed for primary prevention to patients with a life-limiting disease, we classed all patients whose Walter Score was >6 as potentially being overusing statins if they were using statins at baseline (Figure 1) (15, 29).
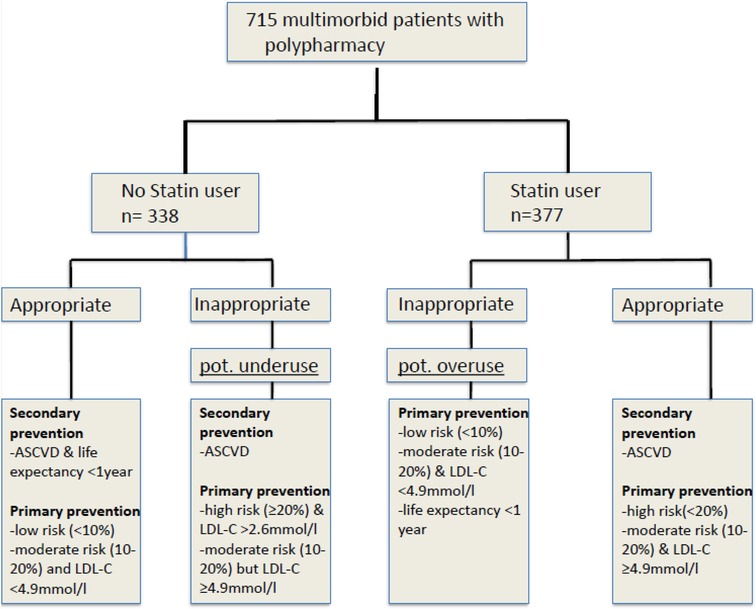
Figure 1. Adjudication algorithm according to AGLA score (25). Legend: abbreviations: ASCVD, LDL-C.
We calculated individual risk for cardiovascular events within the next 10 years based on the patient's AGLA Score (PROCAM Score adapted for Switzerland) (25). Because several guidelines make no clear recommendation for primary prevention in patients aged >75 years (18, 19, 22, 30), we calculated cardiovascular risk scores for those patients as if they were 75 years old. Additionally, the Walter Score was used to estimate individual life expectancy (above) and two medical doctors (LA, OB) independently reviewed the patients' chart to determine if they were on appropriate statin therapy. If the two reviewers disagreed, they consulted a third reviewer (MF). Figure 1 shows the study flow chart for adjudication, which we developed based on current guidelines.
The following predictors were included into our analysis: age (classed into three categories: 70–75, 76–85 and >85 years), sex, being housebound [defined as inability to leave the house unassisted e.g., for (primary) care visits], ≥5–9 chronic medications vs. ≥10 chronic medicationsco-morbidities (into ≥10 and <10 chronic diagnoses), and whether they suffered from dementia/cognitive impairment according to ICD-10 code. All these factors potentially influence the likelihood medication will be prescribed inappropriately (31).
Statistical analyses
We stratified patients according to their indication for statin use, i.e., primary and secondary cardiovascular prevention.
We first calculated descriptive statistics for all variables (percentages and n for categorical variables; means and standard deviations for continuous variables). We also calculated descriptive statistics for participants we included and excluded. Comparisons between included and excluded participants were performed using χ2 tests for categorical variables and t-tests for continuous variables.
Second, we assessed the bivariate associations between potential over- and underuse of a statin with risk factors (i.e., age sex, houseboundedness, co-morbidities and cognitive impairment) using logistic regression models, with potential underuse and overuse as two separate outcomes. We reported odd ratios (OR) with 95% confidence intervals (CI).
Third, we selected the variables with the strongest association with potential statin underuse and overuse using least absolute shrinkage and selection operator (LASSO) regression analyses. We chose this method because of the small numbers of patients in some subgroups. We used multiple logistic regression models with LASSO selection, with underuse and overuse as two separate outcomes. We also reported ORs with 95% CIs.
We used Stata Version 16.0 (StataCorp. 2019. Stata Statistical Software: Release 16. College Station, TX: StataCorp LLC.).
Results
The Swiss OPERAM study center included 822 hospitalized multimorbid patients ≥70 years with polypharmacy (≥5 medications); 17 patients (2.1%) withdrew their consent; and 90 patients (10.9%) were excluded because their available information did not allow us to adjudicate the appropriateness of statin therapy. We thus included 715 patients in our analysis (see the study flow chart in the Supplementary Figure S1). Included patients had a mean age of 79.7 years [±6.5 years standard deviation (SD)]; 60% were male (Table 1). In the secondary prevention group (n = 437), 295 patients (67.5%) used a statin and 105 (24%) patients had a Walter score >6, 68 (23%) of those using a statin (Supplementary Table S3). In the primary prevention group (n = 278), 82 patients (29.5%) used statins and 89 (32%) patients had a Walter Score >6.
Additional baseline characteristics of included patients are presented in Table 1 and comparisons of the baseline characteristics of patients we included and patients we excluded because we could not properly adjudicate them in Supplementary Table S1.
In the 278 patients in primary prevention, we determined estimated risk for CVE at 10-years was low (<10%) in 95 patients, intermediate (10%–20%) in 53 patients, and high (>20%) in 40 patients (Supplementary Table S3). Patients with a Walter Score >6 (n = 89) were classified as potential Statin-overusers without further risk calculation.
Appropriateness of statin therapy in secondary cardiovascular prevention:
Of the 437 patients in secondary prevention, 274 (62.7%) were using a statin appropriately, 105 (24%) patients were underusing a statin, while 58 (13.3%) patients were considered to be potentially overusing a statin as their predicted mortality risk was >60% based on their Walter Score (≥6 points) (Table 2).
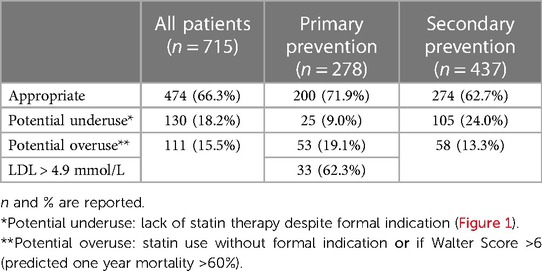
Table 2. Appropriateness of statin prescribing.
In secondary prevention, statin underuse was significantly associated with being very old (>85 years; OR 2.40; 95% CI 1.26–4.57) and female (OR 2.79; 95% CI1.78–4.38) in bivariate models (Table 3). We confirmed the association between underuse and being female with LASSO regression (OR 2.65; 95%CI 1.67–4.22).

Table 3. Associations between potential statin underuse and study variables.
Potential overuse was associated with being housebound (OR 3.58; 95% CI 1.38–9.28) and taking ≥10 medications (1.94; 95%CI 1.05–3.57) in bivariate analyses, which was confirmed after LASSO regression (OR 3.53 (1.32–9.46) and 1.95 (1.05–3.67)) (Table 4).
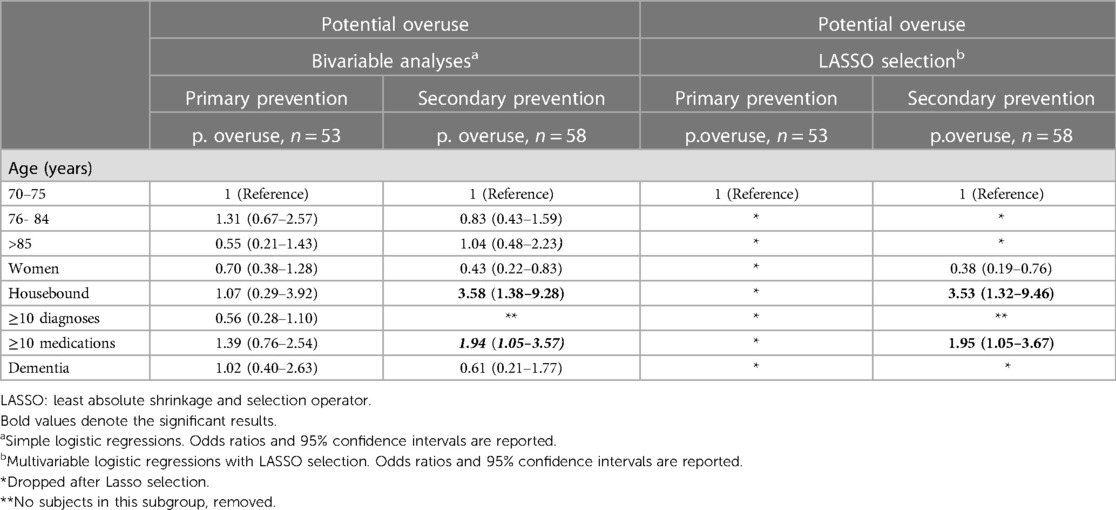
Table 4. Associations between potential statin overuse and study variables.
Appropriateness of statin therapy in primary cardiovascular prevention
Of the 278 patients in primary prevention, 200 (71.9%) were on appropriate statin therapy when they were included in the OPERAM trial, based on our prespecified criteria (Figure 1); 25 (9%) had intermediate to high cardiovascular risk but did not take a statin so we considered them as potentially underusing a statin, while 53 patients (19.1%) were potentially overusing statin (Table 2); 23 of these potential overusers (43.4%) had a Walter Score >6.
No factor among patients in primary prevention predicted a significantly higher risk for potential under—or overuse (Tables 3, 4) in bivariate analyses. We confirmed this finding with LASSO regressions. (Tables 3, 4).
Discussion
Among 715 multimorbid older (≥70 years) hospitalized patients, potentially inappropriate statin therapy was common (33.7%) due to potential underuse with (15.5%) and potential overuse (18.2%). Female gender was significantly associated with potential underuse in secondary prevention (OR 2.65). Being housebound (OR 3.53) and taking ≥10 medications (OR 1.95) were associated with potential overuse in secondary prevention. No specific risk factors were identified for potential over- or underuse in primary prevention.
Though the benefits of statins for primary prevention in the older patients remain controversial, statin therapy in secondary prevention in older patients is supported by evidence (22). Despite the evidence, this cross-sectional study found that 24% of patients in secondary prevention were potentially underusing statins. In secondary prevention, women, particularly, were at risk of underuse (OR 2.65), a finding that aligns with previous studies (32–34).
Statin use is clearly established for prevention of further cardiovascular events in secondary prevention, in both men and women (35). On average, women live longer than men and are therefore more likely to suffer from CVE (36). CVD is the main cause of death for women in developed countries (37, 38), but health care systems may not adequately consider women's cardiovascular risk (38). Though men and women have the same main cardiovascular risk factors, women may present differently in clinical exams, have different symptoms, and tests may not work as well for women as men (39, 40). Our findings align well with a population-based Italian study of older patients with polypharmacy, in which women were more likely to discontinue statin therapy (41).
Housebound patients in secondary prevention were at risk for overuse (defined as having a Walter Score >6) of a statin (OR 3.53), a finding that aligns with a Japanese study of eldery, housebound patient amongst whom potentially inappropriate prescribing was highly prevalent (42). This might be due to the fact that preventive medical visits are associated with a high effort by these patients and his/her proxies (42). A further factor could be that stopping an established statin therapy is currently a matter of discussion and doctors might be especially hesitant to stop a statin in a patient with established ASCVD despite advanced chronic illness and a high 1-year mortality risk (Walter Score > 6) (16). However, Kutner et al. found that stopping statins in patients with limited life expectancy was safe and slightly improved quality of life (15). In primary prevention, we found no pre-defined risk factor associated with higher risk of inappropriate statin therapy (neither potential underuse nor potential overuse), perhaps because it was more difficult to assess cardiovascular risk and define the necessity for statin therapy in the primary prevention group. Though older people are at higher cardiovascular risk, few RCTs have studied the potential benefits of statin therapy for primary prevention in the elderly. A recent meta-analysis of 28 RCTs that analyzed the benefits of statin therapy in 186,854 individuals (but only 8% aged >70 years) found that statin therapy benefited to patients over 70, but provided little evidence on patients in primary prevention (43). An age-stratified analysis of the JUPITER-trial and HOPE III study showed that taking Rosuvastatin would benefit patients >70 years regarding a composite outcome (pooled estimate HR 0.74) of nonfatal MI, stroke or cardiovascular death (44) but included only few patients >80 years. On the other hand, deprescribing statins in older patients is common in primary prevention in the very older people because clinicians might weigh the potential of side effects in frail patients higher than the potential long-term benefit (45). In an international survey using case vignettes, GPs recommended to stop statins for primary prevention especially in frail patients, those with evident side effects and patients with limited life expectancy (16). In general, evidence towards statin therapy in older people in primary prevention is limited, as shown by the discrepancies in different guidelines concerning statin therapy in the elderly (46). Especially for multimorbid older patients guidelines or recommendations concerning (deprescribing) statins are lacking (47).
Our finding of ASCVD prevalence (61%) aligns with previous studies of this older multimorbid population (8). We found statin therapy was prescribed to 52.5% in the entire patient cohort, (29.5% of patients in primary prevention and 67.5% of patients in secondary prevention). A 2011–2015 UK cohort study of statin prescription in old patients (>80 years) in primary prevention yielded similar results (30%) (45). Other studies from the UK and the US found that between 63% and 80% of the older population are taking statins (45, 32).
Limitations
We were limited in our ability to estimate cardiovascular risk in primary prevention, so we used the PROCAM Score adapted for Switzerland, approved for maximally 75-year-old, to determine cardiovascular risk at 10 years and had two medical doctors independently judge the patient's clinical situation on a case-by-case basis (including knowledge of patient's preferences; this data was collected during the OPERAM trial) as current guidelines suggest (18). Our study was also limited because it was conducted at only one center. Though we tried to assess the statin indication for each individual patient, we did not know why treating physicians decided to prescribe or withhold a statin.
Strengths
This is a cross-sectional analysis from the understudied, but especially in Western countries growing population of multimorbid older patients with polypharmacy. Assessing risk-factors for statin under- or overuse in this specific population of multimorbid eldery has not yet been done to our knowledge (48). We accounted for patient's specific risk factors as well as patients' individual life expectancy in a standardized way. Statins are among the most prescribed drugs for the prevention of first or recurrent cardiovascular events (49), which are highly prevalent in multimorbid older patients. This study provides evidence for risk factors that are associated with under- or overuse of a statin, alerting the clinician to frequently adapt and reassess statin therapy according to her/his patient's current situation and need.
Conclusion
A third of multimorbid older patients with polypharmacy either potentially overused or underused statins. Among participants in secondary cardiovascular prevention, women were at highest risk for potential underuse while housebound patients were at risk for potential overuse of a statin. Physicians should carefully evaluate their need for statin prescriptions in this understudied population and adapt prescriptions as needed.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statement
The studies involving humans were approved by Kantonale Ethikkomission Bern (KEK Nr. 2016-01200). The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their informed consent to participate in the OPERAM-trial.
Author contributions
LA, MF, MB, BB, DA; NR contributed to conception and design of the study. LA, OB, DP organized the database. LA, MF, MB, DP, SB performed the statistical analysis. LA wrote the first draft of the manuscript. All authors contributed to the article and approved the submitted version.
Funding
This work is part of the project “OPERAM: OPtimising thERapy to prevent Avoidable hospital admissions in the Multimorbid elderly” supported by the European Union's Horizon 2020 research and innovation program under the grant agreement No 634238, and by the Swiss State Secretariat for Education, Research and Innovation (SERI) under contract number 15.0137. The opinions expressed and arguments employed herein are those of the authors and do not necessarily reflect the official views of the European Commission and the Swiss government. This project was also partially funded by the Swiss National Scientific Foundation (SNSF 320030_188549) and by a grant from the Swiss National Science Foundation to study the usefulness of statins among older adults in primary prevention (IICT 33IC30-193052 to Nicolas Rodondi). The funder of the study had no role in study design, data collection, data analysis, data interpretation or writing of the report. LA work was supported through a “Young Talents in Clinical Research” Grant from the Gottfried and Julia Bangerter-Rhyner Foundation (YTCR_22/17). OB obtained a Protected Research Time (PRT) Grant from the University of Bern.
Acknowledgment
We thank Kali Tal for her editorial assistance.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fcvm.2023.1236547/full#supplementary-material
References
1. Barnett K, Mercer SW, Norbury M, Watt G, Wyke S, Guthrie B. Epidemiology of multimorbidity and implications for health care, research, and medical education: a cross-sectional study. Lancet. (2012) 380(9836):37–43. doi: 10.1016/S0140-6736(12)60240-2
2. Dalleur O, Boland B, De Groot A, Vaes B, Boeckxstaens P, Azermai M, et al. Detection of potentially inappropriate prescribing in the very old: cross-sectional analysis of the data from the BELFRAIL observational cohort study. BMC Geriatr. (2015) 15:156. doi: 10.1186/s12877-015-0149-2
3. Blum MR, Sallevelt B, Spinewine A, O'Mahony D, Moutzouri E, Feller M, et al. Optimizing therapy to prevent avoidable hospital admissions in multimorbid older adults (OPERAM): cluster randomised controlled trial. Br Med J. (2021) 374:n1585. doi: 10.1136/bmj.n1585
4. Kuijpers MA, van Marum RJ, Egberts AC, Jansen PA, Group OS. Relationship between polypharmacy and underprescribing. Br J Clin Pharmacol. (2008) 65(1):130–3. doi: 10.1111/j.1365-2125.2007.02961.x
5. Jin H, Tang C, Wei Q, Chen L, Sun Q, Ma G, et al. Age-related differences in factors associated with the underuse of recommended medications in acute coronary syndrome patients at least one year after hospital discharge. BMC Cardiovasc Disord. (2014) 14:127. doi: 10.1186/1471-2261-14-127
6. Jensen LD, Andersen O, Hallin M, Petersen J. Potentially inappropriate medication related to weakness in older acute medical patients. Int J Clin Pharm. (2014) 36(3):570–80. doi: 10.1007/s11096-014-9940-y
7. Klarin I, Wimo A, Fastbom J. The association of inappropriate drug use with hospitalisation and mortality: a population-based study of the very old. Drugs Aging. (2005) 22(1):69–82. doi: 10.2165/00002512-200522010-00005
8. Aubert CE, Streit S, Da Costa BR, Collet TH, Cornuz J, Gaspoz JM, et al. Polypharmacy and specific comorbidities in university primary care settings. Eur J Intern Med. (2016) 35:35–42. doi: 10.1016/j.ejim.2016.05.022
9. Violan C, Bejarano-Rivera N, Foguet-Boreu Q, Roso Llorach A, Pons-Vigues M, Martin Mateo M, et al. The burden of cardiovascular morbidity in a European mediterranean population with multimorbidity: a cross-sectional study. BMC Fam Pract. (2016) 17(1):150. doi: 10.1186/s12875-016-0546-4
10. Ebrahim S, Taylor FC, Brindle P. Statins for the primary prevention of cardiovascular disease. Br Med J. (2014) 348:g280. doi: 10.1136/bmj.g280
11. Koskinas KC, Siontis GCM, Piccolo R, Mavridis D, Raber L, Mach F, et al. Effect of statins and non-statin LDL-lowering medications on cardiovascular outcomes in secondary prevention: a meta-analysis of randomized trials. Eur Heart J. (2018) 39(14):1172–80. doi: 10.1093/eurheartj/ehx566
12. Shepherd J, Blauw GJ, Murphy MB, Bollen EL, Buckley BM, Cobbe SM, et al. Pravastatin in elderly individuals at risk of vascular disease (PROSPER): a randomised controlled trial. Lancet. (2002) 360(9346):1623–30. doi: 10.1016/S0140-6736(02)11600-X
13. Stone NJ, Intwala S, Katz D. Statins in very elderly adults (debate). J Am Geriatr Soc. (2014) 62(5):943–5. doi: 10.1111/jgs.12788_1
14. Rabar S, Harker M, O'Flynn N, Wierzbicki AS, Guideline Development G. Lipid modification and cardiovascular risk assessment for the primary and secondary prevention of cardiovascular disease: summary of updated NICE guidance. Br Med J. (2014) 349:g4356. doi: 10.1136/bmj.g4356
15. Kutner JS, Blatchford PJ, Taylor DH Jr., Ritchie CS, Bull JH, Fairclough DL, et al. Safety and benefit of discontinuing statin therapy in the setting of advanced, life-limiting illness: a randomized clinical trial. JAMA Intern Med. (2015) 175(5):691–700. doi: 10.1001/jamainternmed.2015.0289
16. van der Ploeg MA, Streit S, Achterberg WP, Beers E, Bohnen AM, Burman RA, et al. Patient characteristics and general practitioners’ advice to stop statins in oldest-old patients: a survey study across 30 countries. J Gen Intern Med. (2019) 34(9):1751–7. doi: 10.1007/s11606-018-4795-x
17. Aubert CE, Gencer B, Rodondi N. Recommendations for management of dyslipidemia in 2016 in Switzerland. Rev Med Suisse. (2016) 12(508):430–4.27089598
18. Mach F, Baigent C, Catapano AL, Koskinas KC, Casula M, Badimon L, et al. 2019 ESC/EAS guidelines for the management of dyslipidaemias: lipid modification to reduce cardiovascular risk. Eur Heart J. (2020) 41(1):111–88. doi: 10.1093/eurheartj/ehz455
19. Stone NJ, Robinson JG, Lichtenstein AH, Bairey Merz CN, Blum CB, Eckel RH, et al. 2013 ACC/AHA guideline on the treatment of blood cholesterol to reduce atherosclerotic cardiovascular risk in adults: a report of the American college of cardiology/American heart association task force on practice guidelines. Circulation. (2014) 129(25 Suppl 2):S1–45. doi: 10.1093/eurheartj/ehz455
20. Assmann G, Cullen P, Schulte H. Simple scoring scheme for calculating the risk of acute coronary events based on the 10-year follow-up of the prospective cardiovascular munster (PROCAM) study. Circulation. (2002) 105(3):310–5. doi: 10.1161/hc0302.102575
21. group Sw, collaboration ESCCr. SCORE2 risk prediction algorithms: new models to estimate 10-year risk of cardiovascular disease in Europe. Eur Heart J. (2021) 42(25):2439–54. doi: 10.1093/eurheartj/ehab309
22. Visseren FLJ, Mach F, Smulders YM, Carballo D, Koskinas KC, Back M, et al. 2021 ESC guidelines on cardiovascular disease prevention in clinical practice. Eur Heart J. (2021) 42(34):3227–337. doi: 10.1093/eurheartj/ehab484
23. Adam L, Moutzouri E, Baumgartner C, Loewe AL, Feller M, M'Rabet-Bensalah K, et al. Rationale and design of optimising therapy to prevent avoidable hospital admissions in multimorbid older people (OPERAM): a cluster randomised controlled trial. BMJ open. (2019) 9(6):e026769. doi: 10.1136/bmjopen-2018-026769
24. Powers WJ, Rabinstein AA, Ackerson T, Adeoye OM, Bambakidis NC, Becker K, et al. 2018 guidelines for the early management of patients with acute ischemic stroke: a guideline for healthcare professionals from the American heart association/American stroke association. Stroke. (2018) 49(3):e46–e110. doi: 10.1161/STR.0000000000000158
25. AGLA Risikorechner. https://www.agla.ch/de/rechner-und-tools/agla-risikorechner
26. Dallongeville J, Banegas JR, Tubach F, Guallar E, Borghi C, De Backer G, et al. Survey of physicians’ practices in the control of cardiovascular risk factors: the EURIKA study. Eur J Prev Cardiol. (2012) 19(3):541–50. doi: 10.1177/1741826711407705
27. Law MR, Wald NJ, Rudnicka AR. Quantifying effect of statins on low density lipoprotein cholesterol, ischaemic heart disease, and stroke: systematic review and meta-analysis. Br Med J. (2003) 326(7404):1423. doi: 10.1136/bmj.326.7404.1423
28. Walter LC, Brand RJ, Counsell SR, Palmer RM, Landefeld CS, Fortinsky RH, et al. Development and validation of a prognostic index for 1-year mortality in older adults after hospitalization. JAMA. (2001) 285(23):2987–94. doi: 10.1001/jama.285.23.2987
29. Grundy SM, Stone NJ, Bailey AL, Beam C, Birtcher KK, Blumenthal RS, et al. 2018 AHA/ACC/AACVPR/AAPA/ABC/ACPM/ADA/AGS/APhA/ASPC/NLA/PCNA guideline on the management of blood cholesterol: executive summary: a report of the American college of cardiology/American heart association task force on clinical practice guidelines. Circulation. (2019) 139(25):e1046–e81. doi: 10.1161/CIR.0000000000000624
30. US Preventive Services Task Force; Mangione CM, Barry MJ, Nicholson WK, Cabana M, Chelmow D, et al. Statin use for the primary prevention of cardiovascular disease in adults: US preventive services task force recommendation statement. JAMA. (2022) 328(8):746–53. doi: 10.1001/jama.2022.13044
31. Bare M, Lleal M, Ortonobes S, Gorgas MQ, Sevilla-Sanchez D, Carballo N, et al. Factors associated to potentially inappropriate prescribing in older patients according to STOPP/START criteria: MoPIM multicentre cohort study. BMC Geriatr. (2022) 22(1):44. doi: 10.1186/s12877-021-02715-8
32. Ngo-Metzger Q, Zuvekas S, Shafer P, Tracer H, Borsky AE, Bierman AS. Statin use in the U.S. for secondary prevention of cardiovascular disease remains suboptimal. J Am Board Fam Med. (2019) 32(6):807–17. doi: 10.3122/jabfm.2019.06.180313
33. Sarraju A, Spencer-Bonilla G, Chung S, Gomez S, Li J, Heidenreich P, et al. Statin use in older adults for primary cardiovascular disease prevention across a spectrum of cardiovascular risk. J Gen Intern Med. (2021) 37(11):2642–9. doi: 10.1007/s11606-021-07107-7
34. Rachamin Y, Grischott T, Rosemann T, Meyer MR. Inferior control of low-density lipoprotein cholesterol in women is the primary sex difference in modifiable cardiovascular risk: a large-scale, cross-sectional study in primary care. Atherosclerosis. (2021) 324:141–7. doi: 10.1016/j.atherosclerosis.2021.02.024
35. Saeed A, Kampangkaew J, Nambi V. Prevention of cardiovascular disease in women. Methodist Debakey Cardiovasc J. (2017) 13(4):185–92. doi: 10.14797/mdcj-13-4-185
36. Leening MJ, Ferket BS, Steyerberg EW, Kavousi M, Deckers JW, Nieboer D, et al. Sex differences in lifetime risk and first manifestation of cardiovascular disease: prospective population based cohort study. Br Med J. (2014) 349:g5992. doi: 10.1136/bmj.g5992
37. Gholizadeh L, Davidson P. More similarities than differences: an international comparison of CVD mortality and risk factors in women. Health Care Women Int. (2008) 29(1):3–22. doi: 10.1080/07399330701723756
38. Woodward M. Cardiovascular disease and the female disadvantage. Int J Environ Res Public Health. (2019) 16(7):1165. doi: 10.3390/ijerph16071165
39. Reynolds HR, Srichai MB, Iqbal SN, Slater JN, Mancini GB, Feit F, et al. Mechanisms of myocardial infarction in women without angiographically obstructive coronary artery disease. Circulation. (2011) 124(13):1414–25. doi: 10.1161/CIRCULATIONAHA.111.026542
40. Hochman JS, Tamis JE, Thompson TD, Weaver WD, White HD, Van de Werf F, et al. Sex, clinical presentation, and outcome in patients with acute coronary syndromes. Global use of strategies to open occluded coronary arteries in acute coronary syndromes IIb investigators. N Engl J Med. (1999) 341(4):226–32. doi: 10.1056/NEJM199907223410402
41. Rea F, Biffi A, Ronco R, Franchi M, Cammarota S, Citarella A, et al. Cardiovascular outcomes and mortality associated with discontinuing statins in older patients receiving polypharmacy. JAMA Netw Open. (2021) 4(6):e2113186. doi: 10.1001/jamanetworkopen.2021.13186
42. Onda M, Imai H, Takada Y, Fujii S, Shono T, Nanaumi Y. Identification and prevalence of adverse drug events caused by potentially inappropriate medication in homebound elderly patients: a retrospective study using a nationwide survey in Japan. BMJ Open. (2015) 5(8):e007581. doi: 10.1136/bmjopen-2015-007581
43. Cholesterol Treatment Trialists C. Efficacy and safety of statin therapy in older people: a meta-analysis of individual participant data from 28 randomised controlled trials. Lancet. (2019) 393(10170):407–15. doi: 10.1016/S0140-6736(18)31942-1
44. Ridker PM, Lonn E, Paynter NP, Glynn R, Yusuf S. Primary prevention with statin therapy in the elderly: new meta-analyses from the contemporary JUPITER and HOPE-3 randomized trials. Circulation. (2017) 135(20):1979–81. doi: 10.1161/CIRCULATIONAHA.117.028271
45. Gulliford M, Ravindrarajah R, Hamada S, Jackson S, Charlton J. Inception and deprescribing of statins in people aged over 80 years: cohort study. Age Ageing. (2017) 46(6):1001–5. doi: 10.1093/ageing/afx100
46. Hawley CE, Roefaro J, Forman DE, Orkaby AR. Statins for primary prevention in those aged 70 years and older: a critical review of recent cholesterol guidelines. Drugs Aging. (2019) 36(8):687–99. doi: 10.1007/s40266-019-00673-w
47. van der Ploeg MA, Floriani C, Achterberg WP, Bogaerts JMK, Gussekloo J, Mooijaart SP, et al. Recommendations for (discontinuation of) statin treatment in older adults: review of guidelines. J Am Geriatr Soc. (2020) 68(2):417–25. doi: 10.1111/jgs.16219
48. Aeschbacher-Germann M, Kaiser N, Speierer A, Blum MR, Bauer DC, Del Giovane C, et al. Lipid-lowering trials are not representative of patients managed in clinical practice: a systematic review and meta-analysis of exclusion criteria. J Am Heart Assoc. (2023) 12(1):e026551. doi: 10.1161/JAHA.122.026551
Keywords: polypharmacy, multimorbidity, cardiovascular prevention, statin, -guideline adherence
Citation: Adam L, Baretella O, Feller M, Blum MR, Papazoglou DD, Boland B, Aujesky D, Baggio S and Rodondi N (2023) Statin therapy in multimorbid older patients with polypharmacy- a cross-sectional analysis of the Swiss OPERAM trial population. Front. Cardiovasc. Med. 10:1236547. doi: 10.3389/fcvm.2023.1236547
Received: 7 June 2023; Accepted: 4 September 2023;
Published: 21 September 2023.
Edited by:
Lars Norgren, Örebro University, SwedenReviewed by:
Sree Kondapally, St George's University Hospitals NHS Foundation Trust, United KingdomValeria Conti, University of Salerno, Italy
© 2023 Adam, Baretella, Feller, Blum, Papazoglou, Boland, Aujesky, Baggio and Rodondi. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Nicolas Rodondi bmljb2xhcy5yb2RvbmRpQGluc2VsLmNo