 Susy Kotit
Susy Kotit Magdi H. Yacoub
Magdi H. Yacoub
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Cardiovasc. Med. , 18 September 2023
Sec. Heart Valve Disease
Volume 10 - 2023 | https://doi.org/10.3389/fcvm.2023.1230965
This article is part of the Research Topic Global Excellence in Cardiovascular Medicine: Africa View all 15 articles
Background: Rheumatic Heart Disease (RHD) remains a major cause of valvular heart disease related mortality and morbidity in low- and middle-income countries, with significant variation in characteristics and course of the disease across different regions. However, despite the high disease burden, there is sparse region-specific data on demographics, disease characteristics and course in treated and untreated patients to guide policy.
Methods: The ARGI database is a hospital-based registry in a tertiary referral national centre (Aswan Heart Centre, AHC) in which all patients with the diagnosis of RHD are being included. The mode of presentation, including baseline clinical and echocardiographic characteristics (as well as other imaging modalities), biomarkers and genetics are being documented. Treatment modalities and adherence to treatment is being recorded and patients are followed up regularly every 6 and/or 12 months, or more frequently if needed.
Discussion: This study shows for the first time an in-depth analysis of the severity and phenotype of disease in Egyptian patients presenting with RHD as well as the progression with time and provides a platform for further comparisons of regional differences in these details as well as their causes. The ARGI database will be of help in achieving the objectives of the Cairo Accord aiming at eradication of RF and RHD.
Rheumatic heart disease (RHD) is the most common cause of acquired heart disease in children and young adults globally (1, 2) and remains a major health care problem causing significant morbidity and mortality at all ages. On global scale, RHD caused 305,651 deaths in 2019 and led to nearly 10.7 million (9.2–12.1) DALYs lost (3). In 2019, there were 2.8 million new cases and 40.5 million prevalent cases of RHD, representing 49.7% and 70.5% increases since 1990, respectively.
The characteristics and course of the disease vary across different regions (4–9). However, there is sparse data on RHD demographics, disease characteristics, age distribution, course of the disease, adverse events, the need and timing of medical interventions, long term outcomes, and mortality (4, 10, 11). To date, there is no similar data from Egypt (12, 13).
Development of databases for accurate data on epidemiology and natural disease history is vital for the prevention and control of RHD, as recommended in the Cairo Accord aiming at disease eradication (15). Comparing the results of different regional registries and the main causative factors, including the influence of genetics and epigenetics should help the global efforts to eradicate RHD (16, 17).
The Aswan Heart Centre (AHC) is a high volume tertiary referral centre with over 45,000 patients seen in outpatient clinics yearly, in which around one-quarter of the workload is related to RHD. The number of patients requiring interventions for RHD is increasing at AHC, and while there are other centres dealing with the disease, there is a pressing need to increase access to surgery for a population of 105 million individuals.
Furthermore, in spite of current medical and surgical treatment, adverse events remain significant (4, 14). Of particular interest remains the thrombosis of prosthetic valves which has been highlighted in a previous publication from AHC (14) but requires continuous efforts.
Our objective is to establish a RHD registry (Aswan Rheumatic heart disease registry, ARGI) to provide disease and regional specific data which could enhance the understanding of the global and regional epidemiology of RHD.
The ARGI database is a hospital-based registry in which all patients from all over Egypt with the diagnosis of RHD are being included.
The ARGI database was designed to address the following aims:
(1) Mode of presentation
(2) Type of treatment (and adherence, including penicillin prophylaxis)
(3) The outcome over time
All consecutive patients with a primary diagnosis of RHD (clinical or echocardiographic) seen at the out-patient clinics (OPD) and inpatient facilities at AHC are eligible to participate (Algorithm 1).
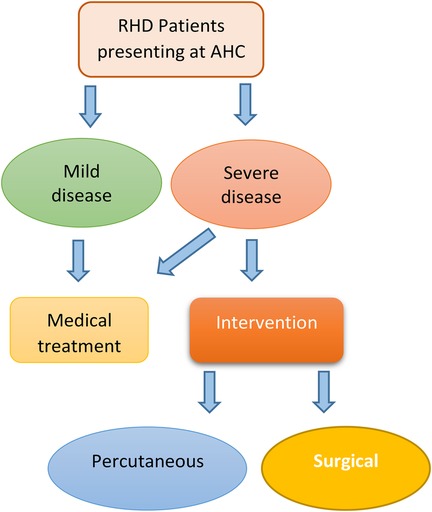
ALGORITHM 1. Patient flow chart.
(1) Mode of presentation
(a) Demographic characteristics (age and gender, etc), history of ARF
(b) Valves affected (the pattern and severity of valvular involvement)
(c) Previous interventions
(2) Type of treatment at the AHC and patient adherence
(a) Pharmacologic treatments, antibiotic prophylaxis, oral anticoagulation
(b) Intervention (percutaneous, surgical)
(3) Monitoring Rheumatic activity
(a) BioBank (blood samples taken at regular intervals from all patients (6-months))
(b) Collection of all surgically explanted tissues from repaired or replaced valves
(4) Monitoring outcome over time
(a) Adverse events
(b) Progression of cardiac disease (progression valvular disease, heart failure, etc)
Demographic information (age, gender, social class, geographic distribution, familial incidence, history of ARF) and clinical data (BP, heart rate, height, weight, medical history, co-morbidities, and previous interventions) are being collected at intervals of 6 months.
Echocardiography is performed for the analysis of the pattern and severity of valvular involvement at presentation and at each follow-up visit, classified using the current World Heart Federation (WHF) criteria (Supplementary Table S1) (18). Cardiac echocardiographic studies are stored online on a specialized platform. All images are reviewed by experienced cardiologists and the heart team.
MRI, CT and cardiac catheterization are performed when indicated.
Blood samples are being taken for biomarkers and DNA extraction. Following separation of the blood into serum and cell components as well as extraction of DNA, the samples are stored in the biobank for future analysis.
(A) Pharmacologic treatments and adherence are being documented, particularly secondary antibiotic prophylaxis, oral anticoagulation and anti-arrhythmic therapy
(B) Percutaneous (Balloon mitral valvuloplasty)
(C) Surgical interventions
Quality of life, adverse events (Supplementary Table S2), exercise capacity, LV and RV function, pulmonary hypertension and progression of valve disease are being assessed during 6 monthly follow-up visits. All-cause mortality is being monitored.
Management of the database is based at the AHC. The principal investigators (PI's) are responsible for the management of the registry, overseeing data collection and quality assurance. The PI's have been responsible for the development of the CRFs, consent forms, patient information sheets, and management algorithms, in addition to the development and maintenance of the web-based database.
The study has been approved by the Magdi Yacoub Foundation-AHC Research Ethics Committee (AHC-REC) in accordance with current practices, a consent form is obtained for specimen collection, storage and analysis. Detailed information sheets have been developed and are provided to each participant. All invasive investigations performed are according to prevailing standard of care guidelines.
A total of 2,510 consecutive patients with clinical and echocardiographic RHD have been enrolled in the ARGI database since March 2009. The age at the time of the first visit ranged from 3 to 86 years (40.11 ± 13.86) (Figure 1). The majority was female (n = 1,695, 67.5%). Only 123 patients (4.9%) had history of RF of which 23 (0.92%) were on secondary penicillin prophylaxis. Symptoms were present in 75.8% (n = 1,902) of the patients, with dyspnea present in 69.6% (n = 1,746) (Figure 2).
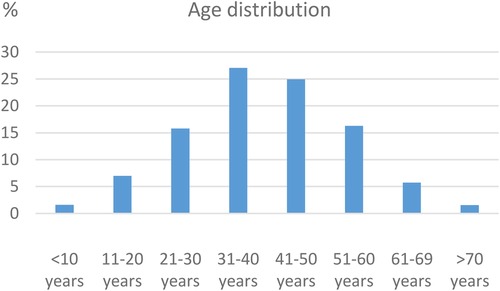
Figure 1. Age distribution at presentation (baseline).
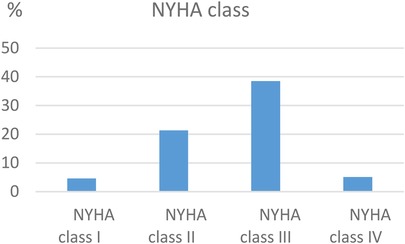
Figure 2. Distribution of NYHA class at presentation.
At enrolment, the majority (n = 2,287, 91.1%) of patients had moderate-to-severe valvular disease (Table 1 and Figure 3) complicated by atrial fibrillation (AF) (n = 723, 28.8%), cerebrovascular events (n = 146, 5.8%), infective endocarditis (n = 16, 0.63%) and thrombosis of valve prosthesis (n = 12, 0.47%). Previous cardiac intervention prior to the first visit to our centre was reported in 19.4% of the patients (n = 487). The age at the time of the first intervention ranged from 4 to 68 (28.21 ± 11.47). The most common first intervention reported was percutaneous balloon mitral valvoplasty (BMV) (n = 232, 47.6%).
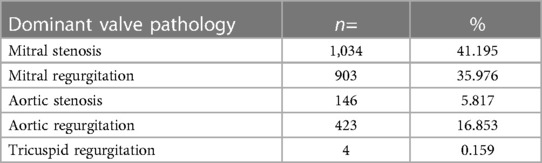
Table 1. Dominant valve pathology.
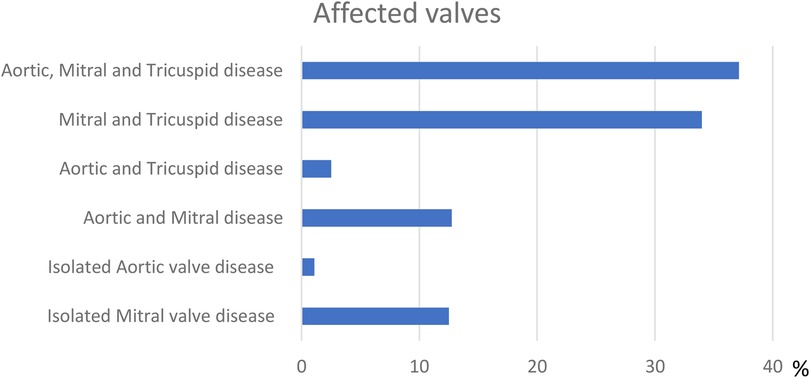
Figure 3. Valve affection.
During regular 6 monthly follow-up at our centre (n = 1,795) for periods ranging from 6 to 142 months (39.46 ± 34.18) (Table 2) a total of 1,303 (72.6%) patients underwent cardiac procedures (Table 3). The age at the time of the intervention ranged from 5 to 79 years (35.64 ± 12.63) at an average of 49.4 months since first presentation (range: 0–140 months, SD: 37.3 months).
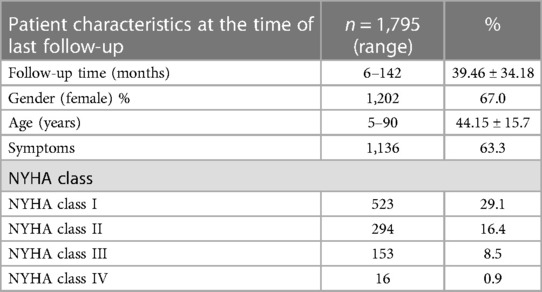
Table 2. Patient characteristics at the time of last follow-up.
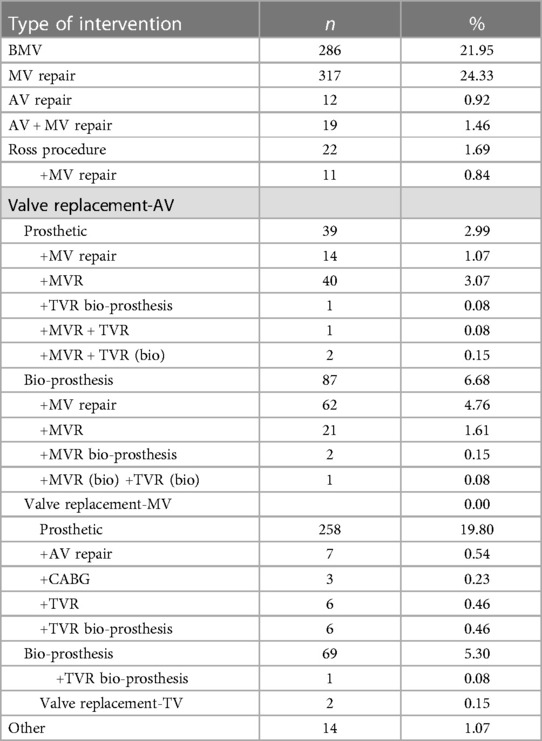
Table 3. Interventions.
Cerebrovascular events (n = 83, 4.6%), LA thrombus (n = 20, 1.1%), infective endocarditis (n = 13, 0.7%) and thrombosis of valve prosthesis (n = 18, 1%) occurred during follow-up. Patient mortality was 16% (n = 287) during the study period (39.46 ± 34.18 months), of which 162 (56.4%) patients had history of intervention.
Penicillin prophylaxis rate was 34.7% (n = 623), however, only 12.9% of these patients followed a correct penicillin prophylaxis schedule.
The ARGI database deals with late chronic disease and initiatives to diagnose earlier phases of disease including ARF (15, 19, 20) as well as population studies (21) are essential.
The preliminary results show for the first time an in-depth analysis of the severity and phenotype of disease in Egyptian patients presenting with RHD as well as the progression with time. The ARGI database provides a platform for further comparisons of regional differences in these details as well as their causes.
In addition, with the increasing numbers of patients recruited, the ARGI study will be combined and compared to similar studies from Egypt (13, 22, 23).
It is hoped that the ARGI study will be of help in achieving the objectives of the Cairo Accord aiming at eradication of RF and RHD.
The datasets presented in this study can be found in online repositories. The names of the repository/repositories and accession number(s) are: https://redcap.ahc-research.com/redcap/ with accession number: PID 117. Further enquiries can be directed to the corresponding author(s).
The authors confirm contribution to the paper as follows: study conception and design: MY, SK; data collection: SK; analysis and interpretation of results: MY, SK; draft manuscript preparation: MY, SK. All authors contributed to the article and approved the submitted version.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fcvm.2023.1230965/full#supplementary-material
1. Watkins DA, Johnson CO, Colquhoun SM, Karthikeyan G, Beaton A, Bukhman G, et al. Global, regional, and national burden of rheumatic heart disease, 1990–2015. N Engl J Med. (2017) 377(8):713–22. doi: 10.1056/NEJMoa1603693
2. “Rheumatic heart disease — Level 3 cause | Institute for Health Metrics and Evaluation.” Available at: http://www.healthdata.org/results/gbd_summaries/2019/rheumatic-heart-disease-level-3-cause (Accessed February 27, 2021).
3. Vos T, Lim SS, Abbafati C, Abbas KM, Abbasi M, Abbasifard M, et al. Global burden of 369 diseases and injuries in 204 countries and territories, 1990–2019: a systematic analysis for the global burden of disease study 2019. Lancet. (2020) 396:1204–22. doi: 10.1016/S0140-6736(20)30925-9
4. Karthikeyan G, Zühlke L, Engel M, Rangarajan S, Yusuf S, Teo K, Mayosi BM. Rationale and design of a global rheumatic heart disease registry: the REMEDY study. Am Heart J. (2012) 163(4):535–40.e1. doi: 10.1016/j.ahj.2012.01.003
5. Okello E, Beaton A, Mondo CK, Kruszka P, Kiwanuka N, Odoi-Adome R, Freers J. Rheumatic heart disease in Uganda: the association between MHC class II HLA DR alleles and disease: a case control study. BMC Cardiovasc Disord. (2014) 14(1):28. doi: 10.1186/1471-2261-14-28
6. Zühlke L, Karthikeyan G, Engel ME, Rangarajan S, Mackie P, Cupido-Katya Mauff B, et al. Clinical outcomes in 3343 children and adults with rheumatic heart disease from 14 low-and middle-income countries: two-year follow-up of the global rheumatic heart disease registry (the REMEDY study). Circulation. (2016) 134(19):1456–66. doi: 10.1161/CIRCULATIONAHA.116.024769
7. He VY, Condon JR, Ralph AP, Zhao Y, Roberts K, de Dassel JL, et al. Long-term outcomes from acute rheumatic fever and rheumatic heart disease: a data-linkage and survival analysis approach. Circ. (2016) 134:222–32. doi: 10.1161/Circ
8. Lawrence J, Carapetis JR, Griffiths K, Edwards K. Acute rheumatic fever and rheumatic heart disease: incidence and progression in the northern territory of Australia, 1997–2010. Circ. (2013) 128(5):492–501. doi: 10.1161/CIRCULATIONAHA.113.001477
9. Sliwa K, Carrington M, Mayosi BM, Zigiriadis E, Mvungi R, Stewart S. Incidence and characteristics of newly diagnosed rheumatic heart disease in urban African adults: insights from the heart of soweto study. Eur Heart J. (2010) 31(6):719–27. doi: 10.1093/eurheartj/ehp530
10. Zühlke L, Engel ME, Karthikeyan G, Rangarajan S, Mackie P, Cupido B, et al. Characteristics, complications, and gaps in evidence-based interventions in rheumatic heart disease: the global rheumatic heart disease registry (the REMEDY study). Eur Heart J. (2015) 36(18):1115–22. doi: 10.1093/eurheartj/ehu449
11. Negi PC, Mahajan K, Rana V, Sondhi S, Mahajan N, Rathour S, et al. Clinical characteristics, complications, and treatment practices in patients with RHD: 6-year results from HP-RHD registry. Glob Hear. (2018) 13(4):267–74, e2. doi: 10.1016/j.gheart.2018.06.001
12. Bassili A, Zaher SR, Zaki A, Abdel-Fattah M, Tognoni G. Profile of secondary prophylaxis among children with rheumatic heart disease in Alexandria, Egypt. East Mediterr Health J. (2000) 6(2–3):437–46. doi: 10.26719/2000.6.2-3.437
13. ElGhamrawy A, Abd El-Wahab F, Nabil N. P2745 trends in rheumatic heart disease in Egypt (200–2018): data from the national rheumatic heart prevention and control program. Eur Heart J. (2019) 40(Supplement):ehz748.1062. doi: 10.1093/eurheartj/ehz748.1062
14. Mahgoub A, Kotit S, Bakry K, Magdy A, Hosny H, Yacoub M. Thrombosis of mechanical mitral valve prosthesis during pregnancy: an ongoing “saga” in need of comprehensive solutions. Glob Cardiol Sci Pract. (2020) 2020(3):e202032. doi: 10.21542/gcsp.2020.32
15. Kotit S, Phillips DIW, Afifi A, Yacoub M. The “Cairo accord”- towards the eradication of RHD: an update. Front Cardiovasc Med. (2021) 8:690227. doi: 10.3389/fcvm.2021.690227
16. Gray LA, D’Antoine HA, Tong SYC, McKinnon M, Bessarab D, Brown N, et al. Genome-wide analysis of genetic risk factors for rheumatic heart disease in aboriginal Australians provides support for pathogenic molecular mimicry. J Infect Dis. (2017) 216:1460–70. doi: 10.1093/infdis/jix497
17. Parks T, Mirabel MM, Kado J, Auckland K, Nowak J, Rautanen A, et al. Association between a common immunoglobulin heavy chain allele and rheumatic heart disease risk in Oceania. Nat Commun. (2017) 8:1–10. doi: 10.1038/ncomms14946
18. Reményi B, Wilson N, Steer A, Ferreira B, Kado J, Kumar K, et al. World heart federation criteria for echocardiographic diagnosis of rheumatic heart disease–an evidence-based guideline. Nat Rev Cardiol. (2012) 9(5):297–309. doi: 10.1038/nrcardio.2012.7
19. Kotit S, Said K, ElFaramawy A, Mahmoud H, Phillips DIW, Yacoub MH. Prevalence and prognostic value of echocardiographic screening for rheumatic heart disease. Open Heart. (2017) 4(2):e000702. doi: 10.1136/openhrt-2017-000702
20. Gemechu T, Parry EHO, Yacoub MH, Phillips DIW, Kotit S. Community-based prevalence of rheumatic heart disease in rural Ethiopia: five-year follow-up. PLoS Negl Trop Dis. (2021) 15(10):e0009830. doi: 10.1371/journal.pntd.0009830
21. Sous M, Magdi E, Ebrahim N, Samuel I, Afify A, Ahmed M, et al. Abstract P632: the ballana heart study: preliminary results. Circulation. (2023) 147:AP632. doi: 10.1161/circ.147.suppl_1.P632
22. Sayed AK, Se'eda H, Eltewacy NK, El Sherif L, Ghalioub HS, Sayed A, et al. Awareness of rheumatic heart disease in Egypt: a national multicenter study. J Cardiovasc Dev Dis. (2021) 8(9):108. doi: 10.3390/jcdd8090108
Keywords: Rheumatic heart disease, Egypt, Aswan, database, registry
Citation: Kotit S and Yacoub MH (2023) The Aswan Rheumatic heart disease reGIstry: rationale and preliminary results of the ARGI database. Front. Cardiovasc. Med. 10:1230965. doi: 10.3389/fcvm.2023.1230965
Received: 29 May 2023; Accepted: 31 August 2023;
Published: 18 September 2023.
Edited by:
Masanori Aikawa, Harvard Medical School, United StatesReviewed by:
Peter Zilla, University of Cape Town, South Africa© 2023 Kotit and Yacoub. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Magdi H. Yacoub bS55YWNvdWJAaW1wZXJpYWwuYWMudWs=
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.