 Muhammad Sabbah
Muhammad Sabbah Thomas Engstrøm
Thomas Engstrøm Niels Thue Olsen
Niels Thue Olsen Jacob Lønborg
Jacob Lønborg
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
BRIEF RESEARCH REPORT article
Front. Cardiovasc. Med. , 03 August 2023
Sec. Coronary Artery Disease
Volume 10 - 2023 | https://doi.org/10.3389/fcvm.2023.1227532
It is widely accepted that severe aortic valve stenosis (AS) can cause exhaustion of coronary flow reserve (CFR), leading to angina pectoris despite the absence of obstructive coronary artery disease. However, it is not established whether CFR is uniformly affected in the left and right coronary arteries. We addressed the differences in coronary physiology between the left anterior descending artery (LAD) and right coronary artery (RCA) in patients with severe AS before aortic valve replacement, by performing pair-wise comparisons of coronary flow reserve (CFR), fractional flow reserve (FFR), absolute hyperemic flow (Q), and minimal microvascular resistance (Rμ) in the LAD and RCA using intracoronary bolus and continuous saline thermodilution techniques (1). The patients in this analysis represent a subset from a previously published cohort in which the physiology of both the LAD and RCA was evaluated (1). Wilcoxon's signed rank test and paired t-test were used to test the differences in medians and means, respectively. Pearson's correlation coefficient was used to test the relationship between the difference in RCA–LAD CFR and left ventricular mass. Two-tailed p-values <0.05 were considered significant. IBM SPSS Statistics for Windows, version 28 (IBM Corp., Armonk, NY, USA), was used for statistical analyses.
A total of 27 patients were included in this analysis, of which 25 had a right-dominant system and two had a co-dominant system. The mean age was 74 ± 8 years, 11 (41%) were women, and the left ventricular ejection fraction was 67 ± 9%. The aortic valve area was 0.72 ± 0.19 cm2 with mean and peak gradients of 56 ± 15 mmHg and 87 ± 24 mmHg, respectively. Left ventricular hypertrophy (LVH) was present in 61% of patients (2). CFR in the LAD was significantly lower than in the RCA (Table 1). Although FFR was lower in the LAD than that in the RCA, the difference in CFR between the LAD and RCA remained statistically significant when using CFR adjusted for epicardial pressure loss (i.e., CFR divided by FFR, Table 1). There was no correlation between the absolute RCA–LAD CFR difference and the left ventricular mass indexed to body surface area, r = −0.011, p = 0.97. The resting transit time was significantly shorter in the LAD compared with that in the RCA, whereas hyperemic transit times were not significantly different (Table 1). Interestingly, absolute hyperemic flow and minimal microvascular resistance in the LAD and RCA were not significantly different (Table 1).
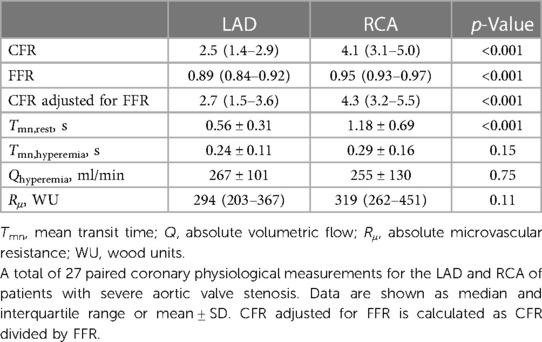
Table 1. Paired measurements of coronary physiological indices in the left anterior descending and right coronary artery in patients with severe aortic stenosis.
In healthy subjects, the coronary vascular bed is organized such that CFR is similar in the overall territory of all coronary arteries (3). The main finding of this study is that in severe AS, CFR is lower in the LAD compared with that in the RCA. This difference was not due to a difference in epicardial disease burden. Instead, our results indicate a higher resting flow in the LAD compared with that in the RCA, as shown once before with a Doppler-based approach (4). A possible explanation for this is that a proportion of RCA flow supplies the right ventricle which escapes the impact of AS, whereas the LAD exclusively supplies the pressure-loaded left ventricle and is thus taxed with a higher resting flow. In our previous work, we have shown that CFR in the LAD significantly increases 6 months after aortic valve replacement (5). Although changes in the RCA were not assessed in that study, it is conceivable that aortic valve replacement ultimately evens out the differences in CFR between the LAD and RCA found in this study.
In summary, CFR in the LAD is significantly lower than that in the RCA in patients with severe AS and right-dominant coronary systems. The difference is driven by a higher resting flow in the LAD compared with that in the RCA.
The raw data supporting the conclusions of this article will be made available by the authors upon reasonable request.
The studies involving human participants were reviewed and approved by Videnskabsetisk Komité, Region Hovedstaden, Denmark. The patients/participants provided their written informed consent to participate in this study.
MS contributed to the idea and drafted the manuscript. TE, JL, and NO contributed to the text and statistical analysis and revised the manuscript critically. All authors contributed to the article and approved the submitted version.
This work was supported by the BRIDGE—Translational Excellence Programme (bridge.ku.dk) at the Faculty of Health and Medical Sciences, University of Copenhagen, funded by the Novo Nordisk Foundation (grant agreement no. NNF20SA0064340).
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Sabbah M, Olsen NT, Minkkinen M, Holmvang L, Tilsted H, Pedersen F, et al. Microcirculatory function in nonhypertrophic and hypertrophic myocardium in patients with aortic valve stenosis. J Am Heart Assoc. (2022) 11:e025381. doi: 10.1161/JAHA.122.025381
2. Kawel-Boehm N, Hetzel SJ, Ambale-Venkatesh B, Captur G, Francois CJ, Jerosch-Herold M, et al. Reference ranges (“normal values”) for cardiovascular magnetic resonance (CMR) in adults and children: 2020 update. J Cardiovasc Magn Reson. (2020) 22:87. doi: 10.1186/S12968-020-00683-3
3. Kern MJ, Bach RG, Mechem CJ, Caracciolo EA, Aguirre FV, Miller LW, et al. Variations in normal coronary vasodilatory reserve stratified by artery, gender, heart transplantation and coronary artery disease. J Am Coll Cardiol. (1996) 28:1154–60. doi: 10.1016/S0735-1097(96)00327-0
4. Marcus ML, Doty DB, Hiratzka LF, Wright CB, Eastham CL. Decreased coronary reserve. N Engl J Med. (1982) 307:1362–6. doi: 10.1056/nejm198211253072202
Keywords: coronary flow reserve/methods, coronary physiology, aortic stenosis, thermodilution, microvascular
Citation: Sabbah M, Engstrøm T, Olsen NT and Lønborg J (2023) Variation in left and right coronary artery physiology in patients with severe aortic stenosis. Front. Cardiovasc. Med. 10:1227532. doi: 10.3389/fcvm.2023.1227532
Received: 23 May 2023; Accepted: 17 July 2023;
Published: 3 August 2023.
Edited by:
Branko Dusan Beleslin, Clinical Center of Serbia, SerbiaReviewed by:
William Kongto Hau, The Chinese University of Hong Kong, Hong Kong SAR, China© 2023 Sabbah, Engstrøm, Olsen and Lønborg. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Muhammad Sabbah bXVoYW1tYWRzYWJiYWgubXNAZ21haWwuY29t
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.