
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Cardiovasc. Med., 12 June 2023
Sec. Heart Valve Disease
Volume 10 - 2023 | https://doi.org/10.3389/fcvm.2023.1197408
 Fernanda Castiglioni Tessari1,†
Fernanda Castiglioni Tessari1,† Maria Antonieta Albanez A. de M. Lopes1,2,†
Maria Antonieta Albanez A. de M. Lopes1,2,† Carlos M. Campos1,3
Carlos M. Campos1,3 Vitor Emer Egypto Rosa1*
Vitor Emer Egypto Rosa1* Roney Orismar Sampaio1
Roney Orismar Sampaio1 Frederico José Mendes Mendonça Soares1Rener Romulo Souza Lopes1Daniella Cian Nazzetta1Fábio Sândoli de Brito Jr1
Frederico José Mendes Mendonça Soares1Rener Romulo Souza Lopes1Daniella Cian Nazzetta1Fábio Sândoli de Brito Jr1 Henrique Barbosa Ribeiro1
Henrique Barbosa Ribeiro1 Marcelo L. C. Vieira1Wilson Mathias Jr1
Marcelo L. C. Vieira1Wilson Mathias Jr1 Joao Ricardo Cordeiro Fernandes1
Joao Ricardo Cordeiro Fernandes1 Mariana Pezzute Lopes1
Mariana Pezzute Lopes1 Carlos E. Rochitte1Pablo M. A. Pomerantzeff1
Carlos E. Rochitte1Pablo M. A. Pomerantzeff1 Alexandre Abizaid1
Alexandre Abizaid1 Flavio Tarasoutchi1
Flavio Tarasoutchi1
Introduction: Classical low-flow, low-gradient aortic stenosis (LFLG-AS) is an advanced stage of aortic stenosis, which has a poor prognosis with medical treatment and a high operative mortality after surgical aortic valve replacement (SAVR). There is currently a paucity of information regarding the current prognosis of classical LFLG-AS patients undergoing SAVR and the lack of a reliable risk assessment tool for this particular subset of AS patients. The present study aims to assess mortality predictors in a population of classical LFLG-AS patients undergoing SAVR.
Methods: This is a prospective study including 41 consecutive classical LFLG-AS patients (aortic valve area ≤1.0 cm2, mean transaortic gradient <40 mmHg, left ventricular ejection fraction <50%). All patients underwent dobutamine stress echocardiography (DSE), 3D echocardiography, and T1 mapping cardiac magnetic resonance (CMR). Patients with pseudo-severe aortic stenosis were excluded. Patients were divided into groups according to the median value of the mean transaortic gradient (≤25 and >25 mmHg). All-cause, intraprocedural, 30-day, and 1-year mortality rates were evaluated.
Results: All of the patients had degenerative aortic stenosis, with a median age of 66 (60–73) years; most of the patients were men (83%). The median EuroSCORE II was 2.19% (1.5%–4.78%), and the median STS was 2.19% (1.6%–3.99%). On DSE, 73.2% had flow reserve (FR), i.e., an increase in stroke volume ≥20% during DSE, with no significant differences between groups. On CMR, late gadolinium enhancement mass was lower in the group with mean transaortic gradient >25 mmHg [2.0 (0.0–8.9) g vs. 8.5 (2.3–15.0) g; p = 0.034), and myocardium extracellular volume (ECV) and indexed ECV were similar between groups. The 30-day and 1-year mortality rates were 14.6% and 43.8%, respectively. The median follow-up was 4.1 (0.3–5.1) years. By multivariate analysis adjusted for FR, only the mean transaortic gradient was an independent predictor of mortality (hazard ratio: 0.923, 95% confidence interval: 0.864–0.986, p = 0.019). A mean transaortic gradient ≤25 mmHg was associated with higher all-cause mortality rates (log-rank p = 0.038), while there was no difference in mortality regarding FR status (log-rank p = 0.114).
Conclusions: In patients with classical LFLG-AS undergoing SAVR, the mean transaortic gradient was the only independent mortality predictor in patients with LFLG-AS, especially if ≤25 mmHg. The absence of left ventricular FR had no prognostic impact on long-term outcomes.
Classical low-flow and low-gradient aortic stenosis (LFLG-AS) is a challenging clinical entity that has garnered increased recognition in recent years. It is characterized by a mismatch between a reduced aortic valve area (AVA) and a nonsevere transaortic mean gradient in patients with reduced left ventricular ejection fraction (LVEF). Recent studies report that classical LFLG-AS accounts for 5%–10% of patients with severe aortic stenosis (AS) (1, 2).
Although aortic valve replacement (AVR) is a well-established management strategy for classical LFLG-AS, studies on interventional risk prediction are largely noncontemporary and have primarily focused on transcatheter AVR (TAVR) (3–8). For instance, once considered a survival marker, left ventricular flow reserve (FR) has recently come under scrutiny for its prognostic relevance (2, 3, 7). Furthermore, earlier studies have examined a heterogeneous population of low-gradient AS, and their findings may not be entirely generalizable to classical LFLG-AS patients (5, 6, 9).
Therefore, there is currently a paucity of information regarding the current prognosis of classical LFLG-AS patients undergoing surgical AVR (SAVR) and the lack of a reliable risk assessment tool for this particular subset of AS patients. The present study aims to assess mortality predictors in a population of classical LFLG-AS patients undergoing SAVR.
This study included a prospective cohort comprising 41 consecutive patients with classical LFLG-AS (i.e., AVA ≤1.0 cm2, mean transaortic gradient <40 mmHg, and LVEF <50%) and SAVR indication. Exclusion criteria were (I) severe primary mitral or aortic regurgitation, (II) moderate-to-severe mitral stenosis, (III) cardiac magnetic resonance (CMR)-incompatible devices or contraindications to gadolinium-enhanced CMR, (IV) previous valve surgery, (V) nonischemic cardiomyopathies, and/or (VI) diagnosis of pseudo-severe AS on dobutamine stress echocardiography (DSE) (n = 4) (Figure 1). A dedicated electronic case report form was designed to collect baseline characteristics, procedure details, and clinical follow-up data. All patients underwent DSE, 2D and 3D transthoracic echocardiography, CMR with T1 mapping and late gadolinium enhancement (LGE) evaluation, and laboratory examination. Coronary angiography was performed in each patient, and coronary artery disease was considered in the presence of >50% luminal stenosis on the major epicardial coronary artery.

Figure 1. Study flowchart. Selection of the study population. All patients without flow reserve on dobutamine stress echocardiography underwent an aortic valve calcium score on computed tomography. AS, aortic stenosis; DSE, dobutamine stress echocardiography; FR, flow reserve; LFLG, low-flow, low-gradient.
Patients were divided into groups according to the mean transaortic gradient ≤25 or >25 mmHg. In order to obtain two groups with a balanced number of patients, this cutoff was determined from the median value of the mean transaortic gradient. All-cause mortality, intraprocedural mortality, 30-day mortality, 1-year mortality, stroke, myocardial infarction, pacemaker implantation, pericardial effusion, postprocedural atrial fibrillation, and reintervention were evaluated. Written informed consent was provided from all the patients, and the study protocol was reviewed and approved by the local institutional ethics committee.
All transthoracic echocardiographs were analyzed in a central echocardiography laboratory. DSE was performed as previously described (2, 10) using a commercially available ultrasound system (Vivid 9; GE Healthcare, Milwaukee, WI, United States), as rest 2D echocardiography. The presence of FR was defined as an increase in stroke volume ≥20% during DSE. True-severe AS was defined by the presence of a mean transaortic gradient ≥40 mmHg with an AVA ≤1.0 cm2 during DSE, and pseudo-severe AS was defined by a mean transaortic gradient <40 mmHg and an AVA >1.0 cm2. In the absence of FR, AS severity was confirmed by the computed tomography aortic valve calcium score and considered severe if ≥1,300 AU in women and ≥2,000 AU in men (11, 12). Echocardiographic parameters were measured using the methods recommended by the American Society of Echocardiography (13). Left ventricular global longitudinal strain was measured by speckle tracking with dedicated commercial software (EchoPAC V 110.0.x; GE Healthcare, Milwaukee, WI, United States), as previously reported (14). Three-dimensional echocardiography was performed using a commercially available ultrasound system (EPIQ Ultrasound, with a 5 MHz transducer; Philips, Andover, MA, United States), and the parameters were analyzed according to standard recommendations (15).
All CMR exams were performed using a clinical 1.5-T CMR scanner (Achieva; Philips, Best, the Netherlands), and the analyses were performed by two experienced investigators in a central CMR core laboratory at our institution. The analyses were performed using CVi42 (Circle CVi; Calgary, Canada) software, and images were acquired and coupled to the electrocardiograph during breath-hold. LGE imaging for myocardial fibrosis was performed 10 min after a bolus (0.2 mmol/kg body weight) of gadolinium-based contrast. Native T1 mapping and T1 postcontrast mapping were calculated before and 15–20 min after the intravenous injection of 0.2 mmol/kg gadolinium-based contrast, respectively, using the modified look-locker inversion-recovery sequence, performed in expiratory apnea, into three segments of the left ventricle short axis (base, mid, and apex). The T1 value was calculated as a global myocardial T1 (pre- and postgadolinium) value and excluded subendocardial and transmural fibrosis areas (segments with mid-wall LGE were included). Atrial fibrillation patients had controlled heart rates (60–90 bpm) during the exam, and T1 mapping image acquisition was repeated, taking into account the average of T1 values in both pre- and postgadolinium sequences. The extracellular volume (ECV) was calculated using the following formula: ECVmyo = (1 − hematocrit) × ΔR1myo/ΔR1blood, where ΔR1 = (1/T1 precontrast − 1/T1 postcontrast) (16). To calculate the indexed ECV (iECV), the following formula was used: ECV (excluding areas of focal fibrosis) × indexed left ventricular end-diastolic myocardial volume (17).
Continuous variables were presented as median (25th–75th percentile). Categorical variables were presented as percentages. The Mann–Whitney U-test was applied for continuous variables, and the Fisher exact test or χ2 test was applied for categorical variables, as appropriate. Cox regression analysis was used to evaluate the predictors of all-cause mortality. Variables with a p < 0.05 in univariate analyses were entered in the multivariable model and adjusted for FR. Survival curves were estimated using the Kaplan–Meier method and compared between patient groups with the log-rank test. All tests were two-tailed, and a p > 0.05 was used to indicate statistical significance. All analyses were conducted using statistical package SPSS, version 20 (IBM, Armonk, NY, United States).
Clinical characteristics and laboratory data are summarized in Table 1. A total of 41 patients with severe degenerative LFLG-AS were enrolled. The median age was 66 (60.0–73.5) years, with a male predominance (82.9%). Functional class III or IV by NYHA classification was present in 51.2%, 26.8% had angina, and only 3% had syncope. There was a high prevalence of comorbidities such as hypertension (68.3%), diabetes (39%), chronic kidney disease (39%), and atrial fibrillation (26.8%), and 36.6% had concomitant coronary artery disease. Almost one-third of the patients had left bundle branch block (29.3%) on the baseline electrocardiogram. The median EuroSCORE II was 2.19% (1.5%–4.78%), and the median STS was 2.19% (1.6%–3.99%). Patients were compared regarding the two-dimensional echocardiographic mean transaortic gradient. Twenty patients had a mean transaortic gradient ≤25 mmHg, and 21 patients had a mean transaortic gradient >25 mmHg. There were no differences in clinical and laboratory data regarding group definition (Table 1).
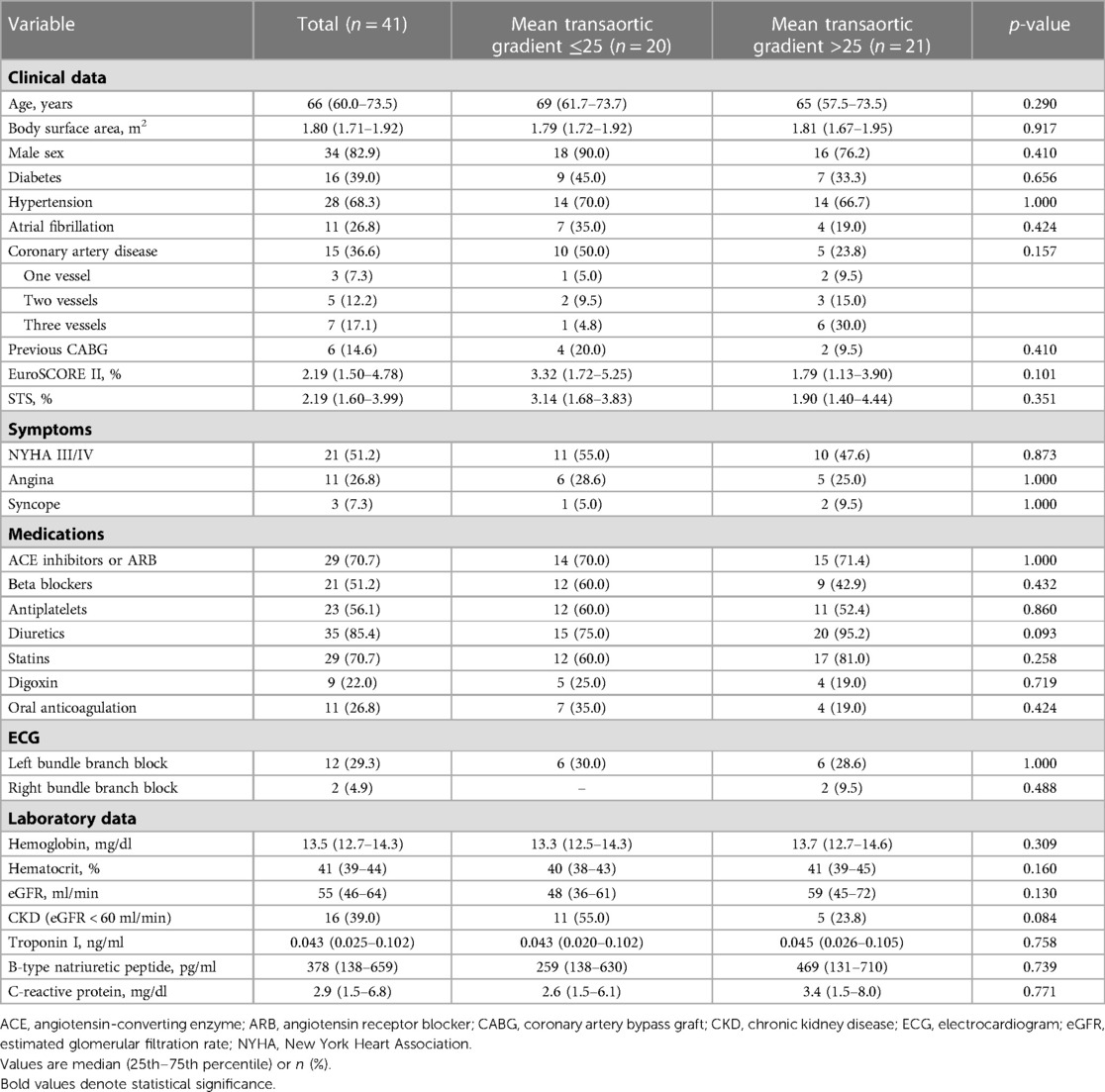
Table 1. Baseline clinical and laboratory data of the study population.
Baseline transthoracic and DSE data are summarized in Table 2. There were no differences between the groups regarding two- and three-dimensional echocardiography in terms of morphological and functional characteristics, except that patients in the mean transaortic gradient >25 mmHg group had, as expected, a higher mean transaortic gradient [33 (30–36) vs. 21 (19–23) mmHg; p < 0.001], peak transaortic gradient [53 (49–61) vs. 36 (30–39) mmHg; p < 0.001], and peak aortic valve velocity [3.64 (3.5–3.9) vs. 2.99 (2.70–3.11) m/s; p < 0.001]. The median stroke volume index was 34 (30–40) ml/m2, the global longitudinal strain was 10% (8.7%–12%) [–], and the valvuloarterial impedance was 5.2 (4.7–5.7) mmHg/ml/m2, with no difference between groups. Regarding three-dimensional echocardiography, data between groups were also similar, with a median LVEF of 31 (24–39)%, AVA of 0.83 (0.66–0.90) cm2, and AVA index of 0.43 (0.37–0.47) cm2/m2.

Table 2. Baseline two- and three-dimensional echocardiography and dobutamine stress echocardiography data.
On DSE, FR was present in most of the patients (73.2%), with no significant differences between the groups. Peak stress parameters did not differ significantly between the groups, except for the peak stress mean transaortic gradient, which was higher in the mean transaortic gradient ≤25 mmHg group [42 (33–49) vs. 32 (22–45) mmHg; p = 0.030]. In contrast to the 2D echocardiography evaluation, the median stroke volume index was higher in the mean transaortic gradient >25 mmHg group [32.2 (27.0–45.7) vs. 25.5 (20.2–31.2) ml/m2, p = 0.012]. However, this difference was no longer observed after dobutamine infusion [39 (35–45) vs. 30.6 (28.0–38.7) ml/m2, p = 0.063].
CMR data are shown in Table 3 and were similar between the groups, except for LGE mass, which was lower in the mean transaortic gradient >25 mmHg group [2.0 (0.0–8.9) vs. 8.5 (2.3–15.0) g; p = 0.034]. Delayed-enhancement images showed a transmural pattern in 29.3% and a mesocardial pattern in 26.8%. Interstitial fibrosis analyses were also similar between groups: overall ECVs including and excluding positive delayed-enhancement were 28.9% (26.8%–33.2%) and 28.7% (26.3%–31.9%), respectively, and iECV was 34.9 (24.9–40.8) ml/m2.
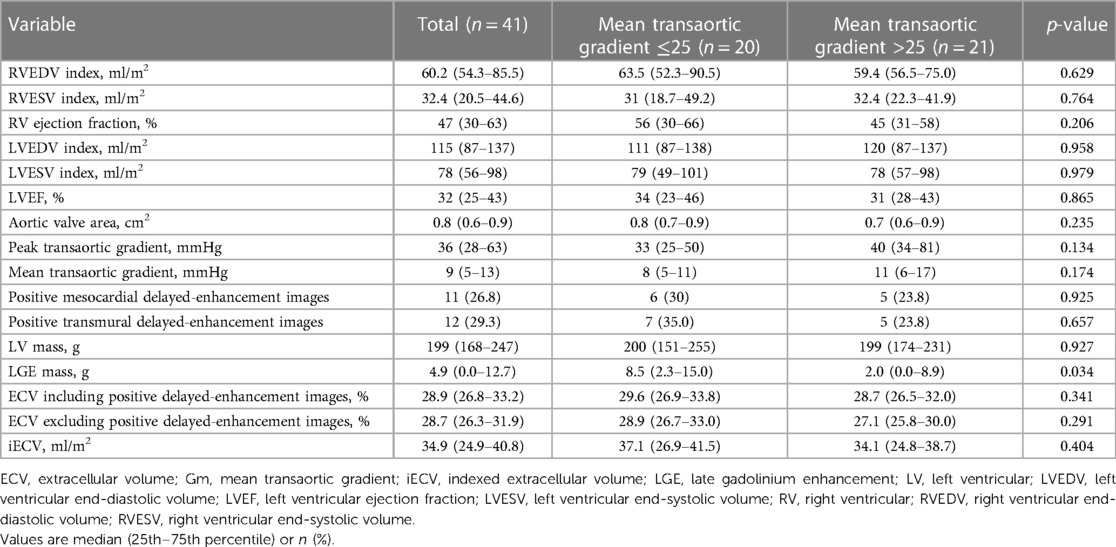
Table 3. Cardiac magnetic resonance data.
Procedural data and postprocedural outcomes are summarized in Table 4. The occurrence of postprocedural complications was evaluated and compared between the groups, with no statistical difference. Infection was the most frequent complication, followed by atrial fibrillation (43.9% and 19.5%, respectively). A definitive pacemaker was implanted in three (7.3%) patients; stroke and pericardial effusion both occurred in only one (2.4%) patient. Concomitant coronary artery bypass graft was performed in three patients from each group, with no statistical difference between groups. There was no ascending aortic procedure nor mitral valve intervention. Cardiopulmonary bypass time was the only variable with a difference between the groups and was lower in the patients with mean transaortic gradient >25 mmHg [60 (52–73) vs. 77 (60–100) min; p = 0.023]. Both 30-day and 1-year mortality rates were also similar, and there was no intraprocedural mortality.
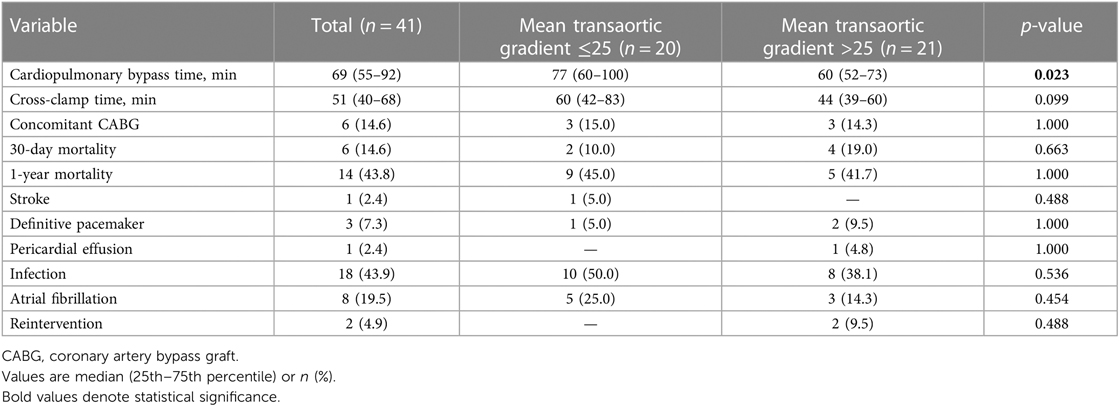
Table 4. Procedure data and post-procedure outcomes.
All-cause mortality was evaluated with a median follow-up of 4.1 (0.3–5.1) years. In the univariate analysis of predictors of all-cause mortality (Table 5 and Supplementary Table S1), three variables were associated with the outcome: STS [hazard ratio (HR): 1.253, 95% confidence interval (CI): 1.019–1.541, p = 0.032], 2D echocardiographic mean transaortic gradient (HR: 0.932, 95% CI: 0.882–0.984, p = 0.011), and C-reactive protein (HR: 1.033, 95% CI: 1.008–1.059, p = 0.011). However, in the multivariate analysis adjusted for FR, only 2D echocardiographic mean transaortic gradient was an independent predictor of mortality (HR: 0.908, 95% CI: 0.837–0.984, p = 0.019). As demonstrated in Figure 2, patients with transaortic mean gradient >25 mmHg had a lower rate of all-cause mortality during the follow-up (log-rank p = 0.038), while the presence of FR (Figure 3) had no impact on mortality (log-rank p = 0.239).

Figure 2. All-cause mortality according to the mean transaortic gradient. Survival curves according to the mean transaortic gradient ≤25 and >25 mmHg at rest echocardiography.
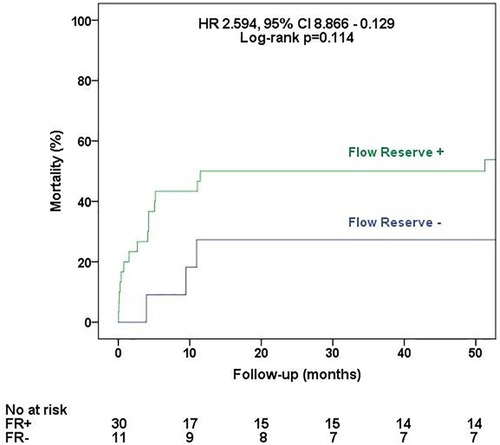
Figure 3. All-cause mortality according to the flow reserve status. Survival curves according to the presence or absence of flow reserve at dobutamine stress echocardiography.
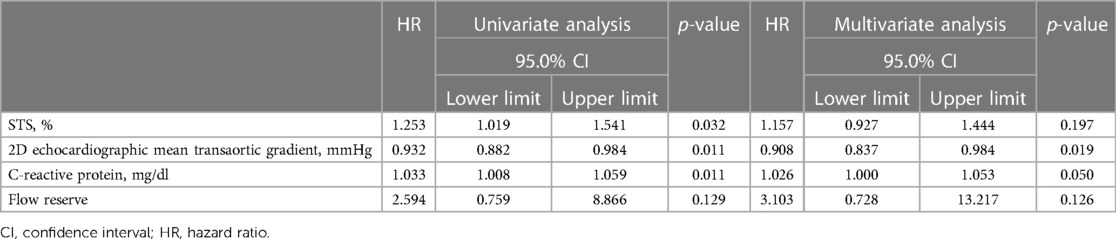
Table 5. Univariate and multivariate analyses of predictors of all-cause mortality adjusted for flow reserve.
The main findings of the present study, including patients with classical LFLG-AS undergoing SAVR, can be summarized as follows: (1) the rest transaortic mean gradient was the only independent predictor of mortality; and (2) the absence of left ventricular FR was not associated with worse outcomes in a median of 4-year follow-up.
Classical LFLG-AS affects only 5%–10% of the population with AS and represents an advanced stage of the disease, as the impaired left ventricle is unable to generate a rest high transaortic gradient. This entity is related to poor clinical outcomes, and conservative treatment has been associated with mortality rates as high as 60% in 2 years (8, 18). However, despite an increased risk for adverse outcomes even with surgical or transcatheter AVR, robust data show that aortic intervention is still beneficial compared to the traditional approach (9, 19–21). Thus, it is imperative to recognize the patients with classical LFLG-AS who will benefit from SAVR, and studies on this topic are scarce.
The absence of FR on DSE has been described for a long time as a predictor of higher mortality in patients undergoing SAVR, with an operative mortality rate of about 30% vs. 5%–7% in the presence of FR (8). However, several recent studies have tried to refute such a theory. First, a prospective study including patients with classical LFLG-AS evaluated by CMR demonstrated that the absence of FR is not related to the amount of diffuse interstitial fibrosis assessed by ECV and iECV, refuting the previous idea that patients without FR could have larger amounts of fibrosis and therefore an increased operative risk (2). Second, the TOPAS-TAVI registry demonstrated that the absence of FR was neither associated with higher mortality rates nor with lower LVEF recovery after TAVR (7). This is in line with Buchanan et al. (3), who showed that FR did not predict all-cause mortality at 30 days or 1 year after TAVR, and Sato et al. (20), who also demonstrated that FR was not a predictor of better survival (3, 20). However, Sato et al. (20) were the only ones who evaluated SAVR patients, but still, the analysis did not differentiate those who underwent TAVR procedures (20). Thus, the results of these studies may not necessarily extend to patients undergoing SAVR exclusively, as those included in the present study.
The multicentric TOPAS registry evaluated predictors of poor outcomes in patients with low-gradient AS undergoing SAVR, TAVR, or a medical approach (5, 7, 9). The TOPAS-TAVI registry demonstrated that lower hemoglobin levels, chronic obstructive pulmonary disease, and moderate-to-severe residual aortic regurgitation were predictors of poor outcomes in a 2-year follow-up after TAVR (7). Another substudy demonstrated a prognostic value of both brain natriuretic peptide (BNP) and high-sensitivity troponin T levels in patients with classical and paradoxical LFLG-AS. Moreover, when occurring simultaneously, values ≥550 pg/ml and ≥15 ng/L, respectively, were independent predictors of 2-year mortality, with higher mortality compared to the elevation of none or only one biomarker (5). A third study on patients undergoing CMR demonstrated that impaired ventricular global longitudinal strain (<−11%), higher ECV (>28%) and LGE presence were predictors of worse outcomes, with a cumulative effect on survival analysis curves (9). However, in these last two studies, the pooled data included not only classical LFLG-AS but also paradoxical AS and normal-flow low-gradient AS (5, 9). It is important to note that AS subtypes have different pathophysiologies since classical LFLG-AS is similar to heart failure with reduced ejection fraction, while the paradoxical AS has similar characteristics to heart failure with preserved ejection fraction. Thus, it is possible that mortality predictors may be different for such pathologies, and they should be studied separately.
Studies including only classical LFLG-AS patients undergoing SAVR are scarce and noncontemporary, revealing high surgical mortality but even worse outcomes with conservative medical treatment (4, 6, 8, 10, 18). Such data corroborate the indication of intervention in patients with classical LFLG-AS and the need for new risk prediction strategies. In line with previous studies, we demonstrated that a lower transaortic mean gradient was associated with worse outcomes, especially if ≤25 mmHg (6, 8). It is noteworthy that, despite there being no difference in LVEF between groups, these patients with lower gradients also presented lower cardiac output at rest and a trend to lower cardiac output at stress, as demonstrated by the basal and peak stroke volume index on DSE, which could indicate a more advanced stage of the disease and, hence, a poor prognosis.
The median value of the mean transaortic gradient (≤25 mmHg) was arbitrarily chosen as the cutoff to divide the population into two groups to obtain two groups with a comparable number of patients. Baseline characteristics were similar between them, except for LGE mass, which was higher among patients with a mean transaortic gradient ≤25 mmHg. Interestingly, different from the present study, LGE was also one of the mortality predictors described by Fukui et al. (9), and this discrepancy could be explained by the higher LGE prevalence demonstrated by that study (67% vs. 53.7% in the present study). In addition, the different populations included in their study (i.e., paradoxical LFLG and normal-flow low-gradient AS, besides classical LFLG-AS) may also impact the results (9). Patients with a mean transaortic gradient of ≤25 mmHg had longer cardiopulmonary bypass time. However, no surgical technical issues could account for this observation, as the rates of coronary artery bypass graft procedures were similar between the groups, and patients did not undergo any other concomitant interventions. Moreover, although longer cardiopulmonary bypass time may influence prognosis and introduce potential bias in the present study, it was not deemed significant as a predictor of mortality in the analysis.
Due to its less invasive nature, TAVR appears to have a higher survival benefit than SAVR (19). The present study demonstrated that classical LFLG-AS patients undergoing SAVR had a higher 30-day mortality rate (14.6%) than that predicted by EuroSCORE II [2.19% (1.50%–4.78%)] and the STS score [2.19% (1.60%–3.99%)]. Meanwhile, the TOPAS registry demonstrated a different scenario in those patients undergoing TAVR, with a 30-day mortality rate of 3.8%, which was lower than the mortality risk predicted by the STS score and EuroSCORE II [7.7% (5.3%–12.0%) and 10.5% (5.5%–17.3%), respectively] (7). However, currently available surgical risk scores may not adequately assess the operative risk, and further studies are needed to obtain better prediction tools for this specific high-risk population.
This is a single-center study with a heterogeneous population and a relatively small number of patients, although large for this entity. The small number of events may have impacted the mortality prediction, despite being enough to fit the developed model (22). In this cohort, different from the former studies, only patients with classical LFLG-AS undergoing SAVR were included. Moreover, further randomized studies are needed to compare treatment strategies in classical LGLF-AS patients (TAVR vs. SAVR).
In patients with classical LFLG-AS undergoing SAVR, the echocardiographic rest transaortic mean gradient was the only independent predictor of mortality. In addition, the absence of left ventricular FR was not associated with worse outcomes, confirming the diagnostic rather than the prognostic value of FR.
The original contributions presented in the study are included in the article/Supplementary Material, further inquiries can be directed to the corresponding author.
The studies involving human participants were reviewed and approved by Comite de Etica e Pesquisa do Hospital das Clinicas da Faculdade de Medicina da Universidade de Sao Paulo—HCFMUSP (55605922.9.0000.0068). Written informed consent for participation was not required for this study in accordance with national legislation and institutional requirements.
FCT, FT, MAAL, and VEER contributed to the conception and design of the study. FCT, VEER, MLCV, FSdBJ, RRSL, and DCN organized the database. VEER and CMC performed the statistical analysis. FCT and VEER wrote the first draft of the manuscript. FCT, VEER, and CMC wrote sections of the manuscript. FJMMS, HBR, WM, JRCF, CER, PMAP, AA, and RRSL contributed to the interpretation of data for the work. All authors contributed to the article and approved the submitted version.
This study was supported by a PhD grant (2013/06149-6) from Fundação de Amparo à Pesquisa do Estado de São Paulo.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fcvm.2023.1197408/full#supplementary-material
1. Pibarot P, Dumesnil JG. Low-flow, low-gradient aortic stenosis with normal and depressed left ventricular ejection fraction. J Am Coll Cardiol. (2012) 60(19):1845–53. doi: 10.1016/j.jacc.2012.06.051
2. Rosa VE, Ribeiro HB, Sampaio RO, Morais TC, Rosa ME, Pires LJ, et al. Myocardial fibrosis in classical low-flow, low-gradient aortic stenosis: insights from a cardiovascular magnetic resonance study. Circ Cardiovasc Imaging. (2019) 12(5):e008353. doi: 10.1161/CIRCIMAGING.118.008353
3. Buchanan KD, Rogers T, Steinvil A, Koifman E, Xu L, Torguson R, et al. Role of contractile reserve as a predictor of mortality in low-flow, low-gradient severe aortic stenosis following transcatheter aortic valve replacement. Catheter Cardiovasc Interv. (2019) 93(4):707–12. doi: 10.1002/ccd.27914
4. Clavel M-A, Fuchs C, Burwash IG, Mundigler G, Dumesnil JG, Baumgartner H, et al. Predictors of outcomes in low-flow, low-gradient aortic stenosis: results of the multicenter TOPAS study. Circulation. (2008) 118(14 Suppl 1):S234–42. doi: 10.1161/CIRCULATIONAHA.107.757427
5. Dahou A, Clavel M-A, Capoulade R, O’Connor K, Ribeiro HB, Côté N, et al. B-type natriuretic peptide and high-sensitivity cardiac troponin for risk stratification in low-flow, low-gradient aortic stenosis: a substudy of the TOPAS study. JACC Cardiovasc Imaging. (2018) 11(7):939–47. doi: 10.1016/j.jcmg.2017.06.018
6. Monin J-L, Quéré J-P, Monchi M, Petit H, Baleynaud S, Chauvel C, et al. Low-gradient aortic stenosis: operative risk stratification and predictors for long-term outcome: a multicenter study using dobutamine stress hemodynamics. Circulation. (2003) 108(3):319–24. doi: 10.1161/01.CIR.0000079171.43055.46
7. Ribeiro HB, Lerakis S, Gilard M, Cavalcante JL, Makkar R, Herrmann HC, et al. Transcatheter aortic valve replacement in patients with low-flow, low-gradient aortic stenosis: the TOPAS-TAVI registry. J Am Coll Cardiol. (2018) 71(12):1297–308. doi: 10.1016/j.jacc.2018.01.054
8. Tribouilloy C, Lévy F, Rusinaru D, Guéret P, Petit-Eisenmann H, Baleynaud S, et al. Outcome after aortic valve replacement for low-flow/low-gradient aortic stenosis without contractile reserve on dobutamine stress echocardiography. J Am Coll Cardiol. (2009) 53(20):1865–73. doi: 10.1016/j.jacc.2009.02.026
9. Fukui M, Annabi M-S, Rosa VE, Ribeiro HB, Stanberry LI, Clavel M-A, et al. Comprehensive myocardial characterization using cardiac magnetic resonance associates with outcomes in low gradient severe aortic stenosis. Eur Heart J Cardiovasc Imaging. (2023) 24(1):46–58. doi: 10.1093/ehjci/jeac089
10. de Filippi CR, Willett DL, Brickner ME, Appleton CP, Yancy CW, Eichhorn EJ, et al. Usefulness of dobutamine echocardiography in distinguishing severe from nonsevere valvular aortic stenosis in patients with depressed left ventricular function and low transvalvular gradients. Am J Cardiol. (1995) 75(2):191–4. doi: 10.1016/S0002-9149(00)80078-8
11. Otto CM, Nishimura RA, Bonow RO, Carabello BA, Erwin JP III, Gentile F, et al. 2020 ACC/AHA guideline for the management of patients with valvular heart disease: executive summary: a report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. J Am Coll Cardiol. (2021) 77(4):450–500. doi: 10.1016/j.jacc.2020.11.035
12. Vahanian A, Beyersdorf F, Praz F, Milojevic M, Baldus S, Bauersachs J, et al. 2021 ESC/EACTS guidelines for the management of valvular heart disease: developed by the task force for the management of valvular heart disease of the European Society of Cardiology (ESC) and the European Association for Cardio-Thoracic Surgery (EACTS). Eur Heart J. (2022) 43(7):561–632. doi: 10.1093/eurheartj/ehab395
13. Baumgartner H, Hung J, Bermejo J, Chambers JB, Edvardsen T, Goldstein S, et al. Recommendations on the echocardiographic assessment of aortic valve stenosis: a focused update from the European Association of Cardiovascular Imaging and the American Society of Echocardiography. Eur Heart J Cardiovasc Imaging. (2017) 18(3):254–75. doi: 10.1093/ehjci/jew335
14. Teske A, De Boeck BW, Melman PG, Sieswerda GT, Doevendans PA, Cramer MJ. Echocardiographic quantification of myocardial function using tissue deformation imaging, a guide to image acquisition and analysis using tissue Doppler and speckle tracking. Cardiovasc Ultrasound. (2007) 5:27. doi: 10.1186/1476-7120-5-27
15. Lang RM, Badano LP, Tsang W, Adams DH, Agricola E, Buck T, et al. EAE/ASE recommendations for image acquisition and display using three-dimensional echocardiography. Eur Heart J Cardiovasc Imaging. (2012) 13(1):1–46. doi: 10.1093/ehjci/jer316
16. Messroghli DR, Moon JC, Ferreira VM, Grosse-Wortmann L, He T, Kellman P, et al. Clinical recommendations for cardiovascular magnetic resonance mapping of T1, T2, T2* and extracellular volume: a consensus statement by the Society for Cardiovascular Magnetic Resonance (SCMR) endorsed by the European Association for Cardiovascular Imaging (EACVI). J Cardiovasc Magn Reson. (2017) 19(1):1–24. doi: 10.1186/s12968-017-0389-8
17. Chin CW, Everett RJ, Kwiecinski J, Vesey AT, Yeung E, Esson G, et al. Myocardial fibrosis and cardiac decompensation in aortic stenosis. JACC Cardiovasc Imaging. (2017) 10(11):1320–33. doi: 10.1016/j.jcmg.2016.10.007
18. Quere J-P, Monin J-L, Levy F, Petit H, Baleynaud S, Chauvel C, et al. Influence of preoperative left ventricular contractile reserve on postoperative ejection fraction in low-gradient aortic stenosis. Circulation. (2006) 113(14):1738–44. doi: 10.1161/CIRCULATIONAHA.105.568824
19. Annabi MS, Côté N, Dahou A, Bartko PE, Bergler-Klein J, Burwash IG, et al. Comparison of early surgical or transcatheter aortic valve replacement versus conservative management in low-flow, low-gradient aortic stenosis using inverse probability of treatment weighting: results from the TOPAS prospective observational cohort study. J Am Heart Assoc. (2020) 9(24):e017870. doi: 10.1161/JAHA.120.017870
20. Sato K, Sankaramangalam K, Kandregula K, Bullen JA, Kapadia SR, Krishnaswamy A, et al. Contemporary outcomes in low-gradient aortic stenosis patients who underwent dobutamine stress echocardiography. J Am Heart Assoc. (2019) 8(6):e011168. doi: 10.1161/JAHA.118.011168
21. Ueyama H, Kuno T, Harrington M, Takagi H, Krishnamoorthy P, Sharma SK, et al. Impact of surgical and transcatheter aortic valve replacement in low-gradient aortic stenosis: a meta-analysis. Cardiovasc Interv. (2021) 14(13):1481–92. doi: 10.1016/j.jcin.2021.04.038
22. Wynants L, Bouwmeester W, Moons K, Moerbeek M, Timmerman D, Van Huffel S, et al. A simulation study of sample size demonstrated the importance of the number of events per variable to develop prediction models in clustered data. J Clin Epidemiol. (2015) 68(12):1406–14. doi: 10.1016/j.jclinepi.2015.02.002
Keywords: aortic stenosis, risk prediction, valve surgery, echocardiography, cardiac magnetic resonance
Citation: Tessari FC, Lopes MAAL, Campos CM, Rosa VEE, Sampaio RO, Soares FJMM, Lopes RRS, Nazzetta DC, de Brito Jr FS, Ribeiro HB, Vieira MLC, Mathias Jr W, Fernandes JRC, Lopes MP, Rochitte CE, Pomerantzeff PMA, Abizaid A and Tarasoutchi F (2023) Risk prediction in patients with classical low-flow, low-gradient aortic stenosis undergoing surgical intervention. Front. Cardiovasc. Med. 10:1197408. doi: 10.3389/fcvm.2023.1197408
Received: 3 April 2023; Accepted: 22 May 2023;
Published: 12 June 2023.
Edited by:
Pompilio Faggiano, Fondazione Poliambulanza Istituto Ospedaliero, ItalyReviewed by:
Andrea Rossi, University of Verona, Italy© 2023 Tessari, Lopes, Campos, Rosa, Sampaio, Soares, Lopes, Nazzetta, Sândoli de Brito Júnior, Ribeiro, Vieira, Mathias, Fernandes, Lopes, Rochitte, Pomerantzeff, Abizaid and Tarasoutchi. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Vitor Emer Egypto Rosa dml0b3JlbWVyQHlhaG9vLmNvbS5icg==
†These authors share first authorship
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.