
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Cardiovasc. Med. , 03 August 2023
Sec. Heart Valve Disease
Volume 10 - 2023 | https://doi.org/10.3389/fcvm.2023.1196447
This article is part of the Research Topic Long-Term Durability of Biological Aortic Valves View all 6 articles
 Alizee Porto1*
Alizee Porto1* Gregoire Stolpe1Rita Badaoui1
Gregoire Stolpe1Rita Badaoui1 Vincent Boudouresques1Cornelia Deutsch2Cecile Amanatiou1Alberto Riberi1Vlad Gariboldi1
Vincent Boudouresques1Cornelia Deutsch2Cecile Amanatiou1Alberto Riberi1Vlad Gariboldi1 Frédéric Collart1
Frédéric Collart1 Alexis Theron1*
Alexis Theron1*
Introduction: The use of an aortic bioprosthesis is on the rise in younger patients with severe aortic stenosis despite the risk of accelerated structural valve degeneration (SVD). In the search for an optimal valve substitute that would not be prone to SVD, the INSPIRIS bioprosthesis represents a promising solution to lowering the risk of SVD. Here, we report the 1-year outcomes of the INSPIRIS RESILIA aortic bioprosthesis in a population of young patients who underwent aortic valve replacement.
Methods: In this prospective single-center study, we included all consecutive patients receiving INSPIRIS RESILIA bioprosthesis between June 2017 and July 2021. Patients with isolated severe aortic regurgitation were excluded. Clinical assessment and transthoracic echocardiography were performed preoperatively and at 1 year post-operatively. The primary outcome was overall mortality at one year.
Results: A total of 487 patients were included. The mean age was 58.2 ± 11.5 years, 75.2% were men. Most of the interventions were elective, with a mean EuroSCORE II of 4.8 ± 7.9. The valve annulus size in most cases was either 23 mm or 25 mm. Overall mortality at 1-year was 4.1%. At 1-year, 7 patients (1.4%) had a stroke, 4 patients (0.8%) had a myocardial infarction, and 20 patients (4.1%) were hospitalized for congestive heart failure. The Kaplan-Meier estimated survival rates and survival without major adverse cardiac events at 1-year were 96.4% and 96.7%, respectively. At 1-year follow-up, 10 patients (2.1%) had endocarditis and 1 patient (0.2%) had partial prosthetic thrombosis. Pacemaker implantation at 1-year post-operative was necessary in 27 patients (5.5%). Severe patient prosthesis mismatch and severe intra valvular regurgitation were 1.2% and 0.6%, respectively. The Kaplan-Meier estimated survival rates at 1-year of no infective endocarditis preoperative and infective endocarditis preoperative were 97.9 ± 0.7% and 89.5 ± 3.3%, respectively (P < 0.001). Excluding endocarditis-related complication, no structural valve deterioration and no valve failure requiring redo surgery were reported.
Conclusion: This is the largest single-center descriptive study of the 1-year outcomes after INSPIRIS RESILIA bioprosthesis implantation. The EDWARDS INSPIRIS RESILIA bioprosthesis provides encouraging clinical outcomes with an excellent 1- year survival rates and good hemodynamic performance. Long-term studies are mandatory to assess valve durability.
Aortic stenosis is the most common valvular heart disease in developed countries, with a prevalence of 3.4% and an incidence of 5 in 1.000 per year among the population at age 65 years (1). Since 1960, the gold standard treatment for this disease has been surgical valve replacement. The management of these patients has changed in recent decades due to the development of the Transcatheter Aortic Valve Implantation (TAVI) technique. According to the European guidelines concerning aortic stenosis, patients over 75 years of age can benefit from TAVI (2). Conventional surgery for aortic valve replacement (AVR) is therefore currently indicated for younger patients, since it allows left ventricle mass regression by reducing LV afterload, thereby improving survival and quality of life, and avoiding the risk of congestive heart failure. The choice between a biological and a mechanical valve remains a controversial issue in younger patients, as neither type of prosthesis has shown its superiority on prognosis in patients aged between 50 and 65 years (3, 4). Moreover, both types of prosthesis have disadvantages that can impact the quality of life: bleeding risk of anti-coagulant treatments for mechanical valves and risk of structural valve degeneration (SVD) for bioprosthesis (5).
This SVD involves the unavoidable risk of reintervention, especially in patients under 65 years (6) and this management has also been modified by endovascular approach with Valve-In-Valve (VIV) aortic implantation (7).
The durability of the bioprosthesis is therefore an important issue, especially in younger patients. That is why the INSPIRIS RESILIA aortic valve with a novel model was developed by Edwards Lifesciences (Irvine, USA). It is a bioprosthetic bovine pericardial tissue valve with a special integrity preserving technology. In addition to having a phospholipid removal process, this technology allows the blockage of residual aldehyde groups known to bind calcium. Moreover, VFit technology present in this bioprosthesis was designed to allow for potential VIV procedures in the future, by increasing the size of the annular stent at the time of a new valve implantation.
Early clinical experience with the INPIRIS RESILIA valve showed encouraging results in terms of early safety and effectiveness of AVR (8, 9). Intermediate-term outcomes have shown the absence of early thrombosis events or non-calcific valve deterioration (10, 11). Five-year results have also been described, concluding in encouraging findings on the safety and hemodynamic performance of this bioprosthesis (12, 13).
However, the use of a new biological valve implies that different short and medium term studies be performed, to confirm the previous results.
Our aim was to evaluate the 1-year outcome of the INSPIRIS RESILIA aortic valve (Edwards Lifesciences) in a population of young patients who underwent AVR for severe aortic stenosis.
In this prospective single-center study, we included all patients receiving the INSPIRIS RESILIA bioprosthesis between June 2017 and July 2021, at La Timone Hospital in Marseille, France. Patients with severe aortic stenosis were included. Patients under 18 years old, those with isolated severe aortic regurgitation, and those declining to participate in follow-up were excluded. Demographic characteristics preoperative and intraoperative variables were collected: age, sex, cardiovascular risk factors, past medical and surgical history, EuroSCORE II, and infective endocarditis (IE).
Consent was obtained from patients to participate in this anonymous publication. Our Clinical Trials registration number was RGPD2019-48.
Since 2017, a new generation biological valve, INSPIRIS RESILIA (Edwards Lifesciences), has been utilized in our center. All patients had a full sternotomy. After completion of cardiopulmonary bypass (CPB) and cross clampage (CC), an aortotomy was performed. The choice of the type of prosthesis was left to the surgeon's discretion after valve excision and annular decalcification. AVR could be associated with concomitant surgery, including coronary artery bypass graft CABG, mitral valve repair or replacement, aortic replacement, and tricuspid valve repair or replacement.
All outcomes were defined according to the Valve Academic Research Consortium-2 (VARC-2) consensus document (14).
At 30-days, early complications were overall and cardiovascular mortality, major bleeding (defined by re-exploration for bleeding or need for >4 blood unit replacement), renal failure, respiratory failure, sternal infection, stroke, cardiogenic shock, cardiac tamponade and pacemaker implantation.
One-year outcomes included overall and cardiovascular mortality, disabling stroke, myocardial infarction, rehospitalization for congestive heart failure (CHF), pacemaker implantation and IE.
Hemodynamic follow-up was assessed by echocardiography analyzed by a senior cardiologist.
Left ventricular ejection fraction (LVEF) was estimated using the Simpson Biplane method, and the Devereux formula was used to calculate LV mass index. The Continuous Doppler technique was used to estimate the transaortic gradient. The effective orifice area (EOA) was calculated using the continuity equation, and the indexed effective orifice area (iEOA) was calculated by dividing the EOA by body surface area. Moderate Patient Prosthesis Mismatch (PPM) was defined by an iEOA between 0.85 and 0.65 cm/m2 or between 0.75 and 0.55 cm/m2 if body mass index > 30 kg/m2, and severe PPM by an iEOA below 0.65 cm/m2 or 0.55 cm/m2 if body mass index > 30 kg/m2. Trans Valvular Regurgitation (TVR) and Para Valvular Leak (PVL) were described according to classification as mild, moderate or severe.
The primary endpoint was overall mortality at 1 year.
Secondary endpoints were cardiovascular mortality, major adverse cardiac events (defined by rehospitalization for congestive heart failure, stroke or myocardial infarction), early complications and at 1-year follow-up, evolution of functional status New York Heart Association (NYHA), hemodynamic follow-up, and mortality-morbidity of IE.
An analysis was carried out in three groups, according to the age of the patient: 50 years old or younger, between 50 and 65 years old, and 65 years or older. Preoperative data and follow-up were compared between these groups.
Another subgroup analysis was performed according to the IE preoperative status.
Statistical analyses were performed for the total study population on available data. Categorical variables are reported as absolute numbers and percentages (%). Continuous variables are presented as mean ± standard deviation (SD) or median [interquartile range (IQR)]. All continuous variables were checked for distribution using the Kolmogorov-Smirnov test. Comparisons were made using a Pearson's Chi-Square or Fisher's exact test for categorical variables. For continuous variables comparisons were performed according to their distribution, using a Student's t-test or Mann-Whitney_U test for 2-group comparison. Comparisons between more than 2 groups were made using the Kruskal-Wallis-H test, including a paired comparison if there was seen a significant difference between subgroups. Wilcoxon signed rank test for paired data was used for comparing echo data between baseline and follow-up. Kaplan-Meier estimates are provided for survival and safety outcomes. A P-value of <0.05 was considered statistically significant. All statistical analyses were performed using IBM SPSS Statistics version 29 (IBM, Armonk, New York).
Between June 2017 and July 2021, 506 patients were treated for AVR with an INSPIRIS RESILIA bioprosthesis. Fourteen patients were excluded for isolated aortic regurgitation and five patients declined to participate in this study. In total, 487 patients were included in the study (Figure 1).
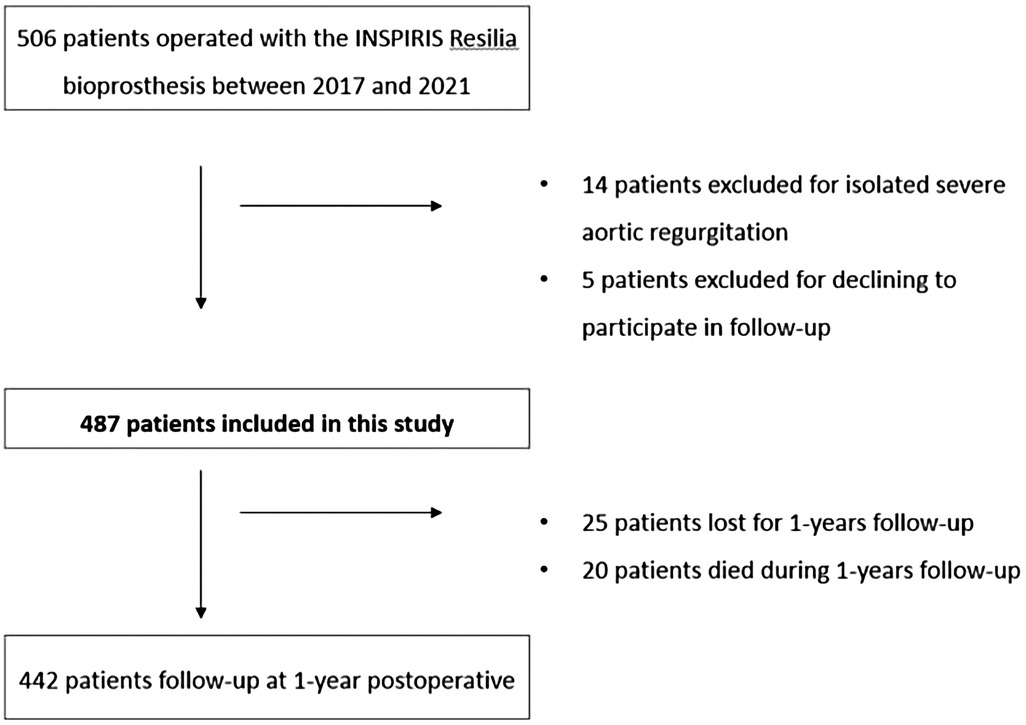
Figure 1. Patient disposition flowchart.
The mean patient age was 58.2 ± 11.5 years, 21.1% were under 50 years-old, with male predominance (75.2%). EuroScore II was 4.8 ± 7.9 and 227 patients (46.6%) were in NHYA Class III or IV. Most of the interventions were elective (363 patients, 74.5%). Ninety-one patients (18.7%) had endocarditis, 72 patients (14.8%) were redo surgery and 152 patients (31.2%) had aortic stenosis without aortic regurgitation. Baseline characteristics including cardiovascular risk factor are presented in Table 1.
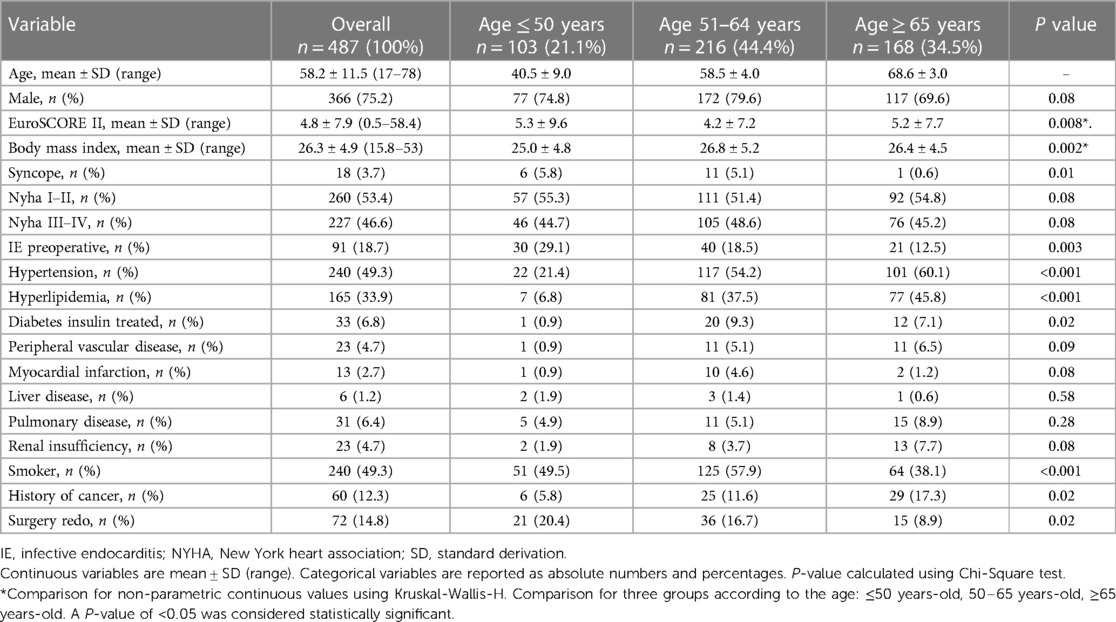
Table 1. Demographics characteristics among 489 patients treated with bioprosthetic INSPIRIS aortic valve for severe aortic stenosis. Comparison according to the age of patient.
Perioperatively, 210 (43.1%) patients had a concomitant procedure performed of which 114 (23.4%) had aortic replacement, 45 (9.2%) had mitral valve surgery replacement or repair and 36 (7.4%) had CABG. The mean CC and CPB times were 85.9 ± 33.9 min and 112.6 ± 49.5 min, respectively. INSPIRIS valves sizes 23 mm (170 patients, 34.9%) and 25 mm (125 patients, 25.7%) were the most implanted (Figure 2).
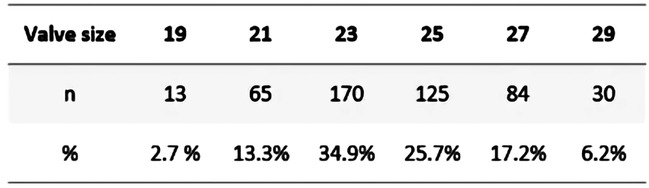
Figure 2. INSPIRIS RESILIA valve distribution according to size.
Mean duration of hospitalization was 16.6 ± 12.6 days.
At 30-days follow-up, 8 patients (1.6%) had died: 5 (1.0%) following cardiogenic shock, 2 (0.4%) following multiorgan failure, and 1 (0.2%) following mesenteric ischemia. Early complications occurred in 66 patients (13.6%) and included respiratory failure in 19 patients (3.9%), acute renal failure requiring dialysis in 12 patients (2.5%), cardiogenic shock necessitating extra-corporeal membrane oxygenation in 8 patients (1.6%), stroke in 4 patients (0.8%), cardiac tamponade in 12 patients (2.5%), major bleeding in 28 patients (5.7%), 16 (3.3%) of whom needed reintervention, and sternal infection in 4 (0.8%). Pacemaker implantation was required in 23 patients (4.7%) at discharge.
At 1-year post implant, 25 (5.1%) patients were lost to follow-up;
12 death occurred: 4 (0.8%) following congestive heart failure, 2 (0.4%) following COVID-19 infections, 1 (0.2%) following gastrointestinal bleeding, 2 (0.4%) following cerebral hemorrhages, and 1 (0.2%) from indeterminate causes. In total, the mortality rate at 1-year was 4.3% (20 patients). The Kaplan-Meier estimated survival rate at 1-year was 96.4 ± 0.9% (Figure 3). Regarding complications at 1-year, 7 patients (1.4%) had a stroke, 4 patients (0.8%) had myocardial infarction and 20 patients (4.1%) were hospitalized for congestive heart failure. The Kaplan-Meier estimated survival without major advance cardiac events at 1-year was 96.7 ± 0.8% (Figure 4).
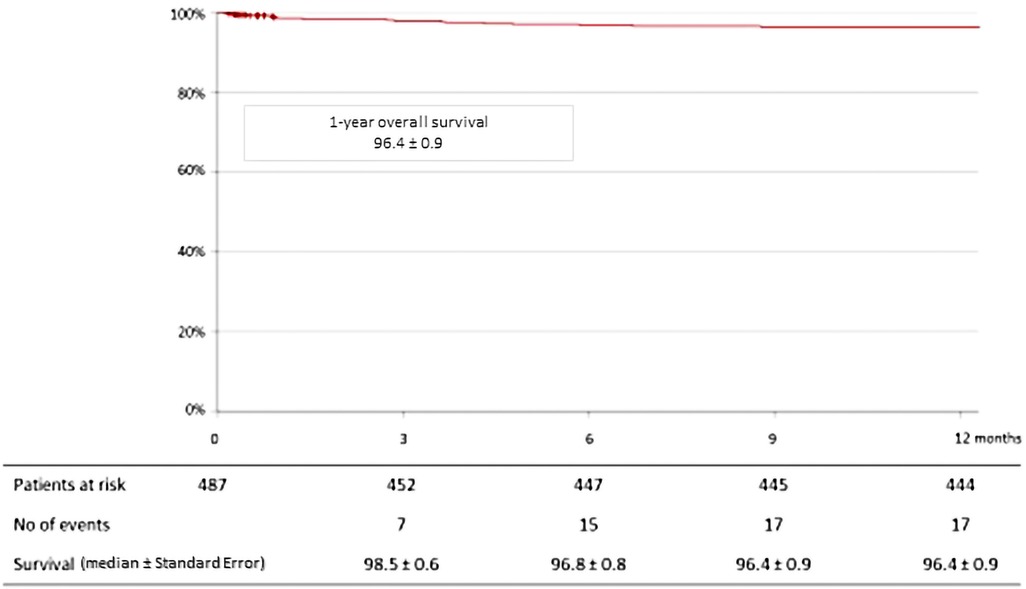
Figure 3. Kaplan-Meier curve for overall survival at 1-year among 489 patients treated with bioprosthetic INSPIRIS RESILIA aortic valve for severe aortic stenosis.
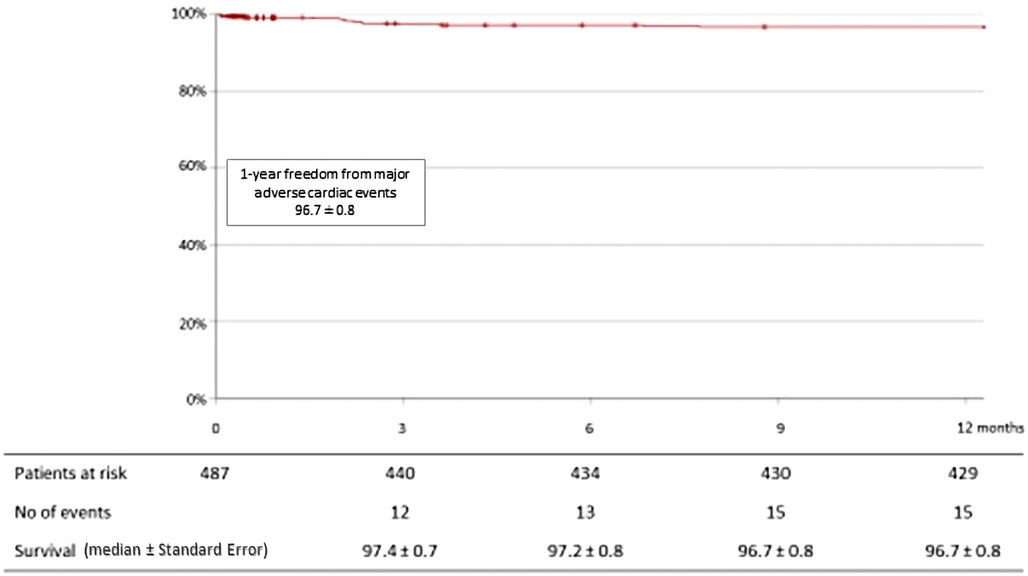
Figure 4. Kaplan-Meier curve for freedom from major adverse cardiac events (stroke, myocardial infarction and hospitalization for congestive heart failure) at 1-year among 489 patients treated with bioprosthetic INSPIRIS RESILIA aortic valve for severe aortic stenosis.
Pacemaker implantation for new-onset conduction disorders at 1-year was required in 27 patients (5.5%).
Ten patients (2.3%) developed IE at 1-year follow-up, 4 of which had recurrence IE.
Functional status was significantly improved (Figure 5): 227(46.7%) patients had NYHA III/IV preoperatively whereas 17 patients (3.9%) had NYHA III/IV postoperatively (P < 0.05).
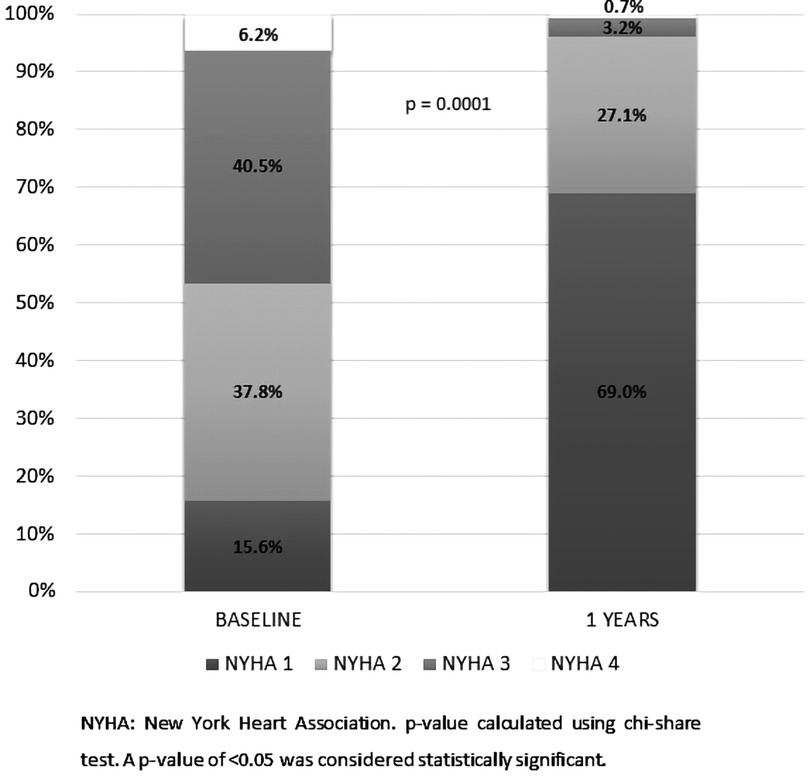
Figure 5. Change in New York heart association status from baseline to 1-year follow-up among 489 patients treated with bioprosthetic INSPIRIS RESILIA aortic valve for severe aortic stenosis. NYHA, New York heart association. P-value calculated using Chi-Square test. A P-value of <0.05 was considered statistically significant.
At 30-days, any implant malposition was reported, and 6.2% (30 patients) with moderate PPM and 1.4% (7 patients) with severe PPM were observed.
Concerning the evolution of the hemodynamic parameters at 1-year, the mean gradient decreased from 49 mmHg (43;55) preoperatively to 9 mmHg (7;12) at 1-year post-operative (P < 0.001), and the peak velocity decreased from 4.4 m/s (4.0;4.9) to 2.1 m/s (1.8;2.4) (P < 0.001) (Table 2).
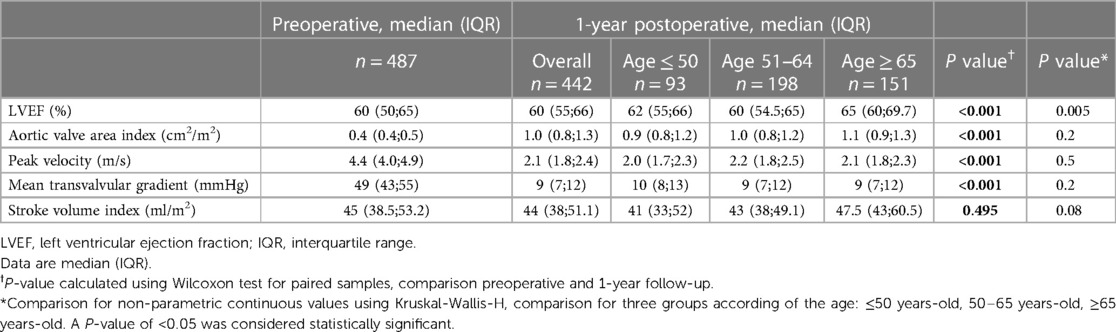
Table 2. Transthoracic echocardiography characteristics from preoperative to 1-year post-operatively among 489 patients treated with a bioprosthetic INSPIRIS RESILIA aortic valve for severe aortic stenosis. Comparison according to the age of patient.
Moderate and severe PPM were observed in 51 (10.5%) patients and 6 (1.2%) patients, respectively. Concerning prosthetic regurgitation, moderate and severe TVR were reported in 2 patients (0.4%) and in 1 patient (0.2%), respectively. Moderate or severe PVL was observed in 7 patients (1.4%) and 3 patients (0.6%), respectively.
One patient (0.2%) developed partial valvular thrombosis with favorable evolution under anticoagulant treatment.
Three subgroups were analyzed: 103 patients (21.1%) were 50 years old or younger, 216 (44.4%) were between 50 and 65 year old and 168 (34.5%) were65 years orolder. Patients under 50 years-old had a higher EuroSCORE II (5.3 ± 9.6) and presented more often with preoperative IE (29.1%); 20.4% of the cases were redo surgeries. Patients between 50 and 65 years old were predominantly male (79.6%), had hypertension (54.2%) and were smokers (57.9%) (Table 1).
During the follow-up, overall mortality was 6.6%, 3.4% and 4.4% for the three successive age groups (P = 0.53). Moreover, there was no significant difference in term of morbidity according to major adverse cardiac events (Table 3).
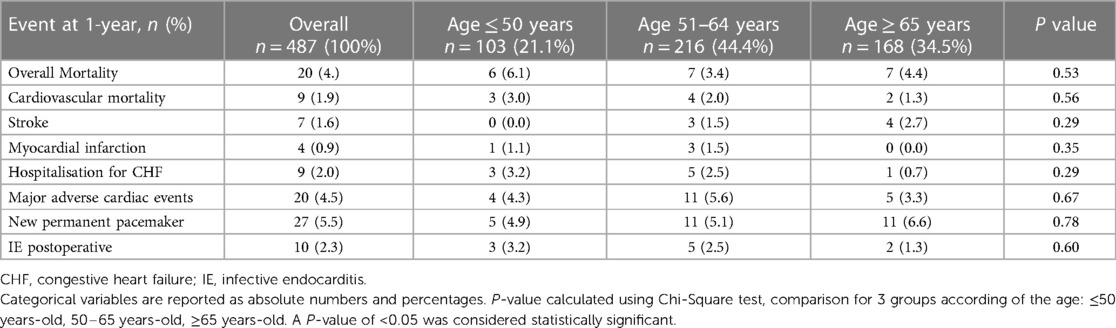
Table 3. At 1-year post-operatively, mortality and morbidity among 489 patients treated with bioprosthetic INSPIRIS aortic valve for severe aortic stenosis. Comparison according to the age of patient.
Concerning transthoracic echocardiography characteristics at 1-year, the group of patients 65 years or older had a greater increase in LVEF (65%, P = 0.005) and in stroke volume index (47.5 ml/m2, P = 0.08) compared with the other two groups. Evolution of the aortic valve area index, the peak velocity and the mean trans-valvular gradient showed no difference between these three groups (Table 2).
Patients with preoperative IE were younger (median age 54.7 ± 12.7 years, P = 0.002), with a higher EuroSCORE II (11.5 ± 12.4, P < 0.001) compared to the IE-free group (median age 59.0 ± 11.0 and EuroSCORE II 3.3 ± 5.5). Elective procedure was realized in 12.1% of the cases (11 patients) and redo surgery in 38.5% (35 patients), with a significant difference in the IE-free group, 88.9% (352 patients, P < 0.001) and 9.3% (37 patients, P < 0.001), respectively.
The Kaplan-Meier estimated survival rates at 1-year for IE-free group and IE group were 97.9 ± 0.7% and 89.5 ± 3.3%, respectively (P < 0.001) (Figure 6). Major adverse cardiac event accounted for 4.4% (16 patients) in IE-free group and 5.3% (4 patients) in the IE group.
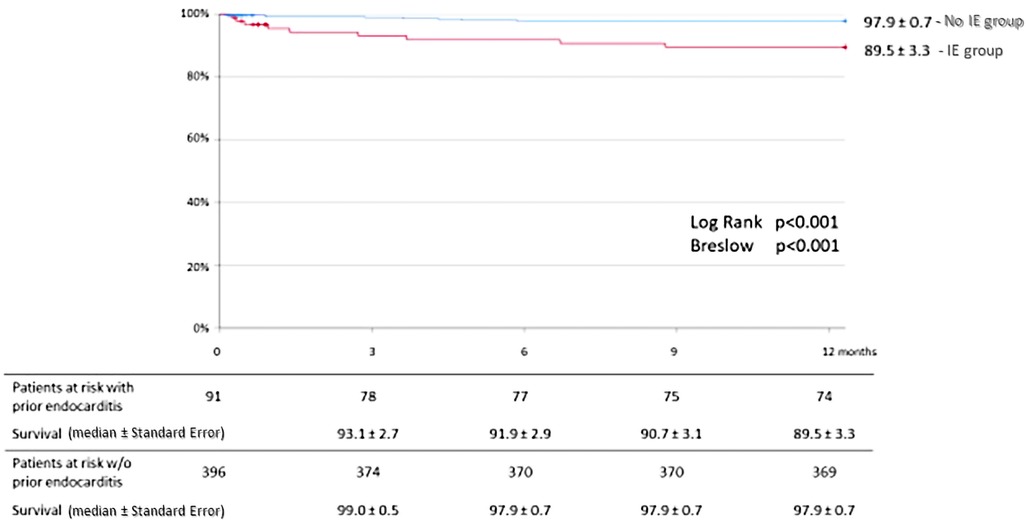
Figure 6. Kaplan-Meier curves for overall survival at 1-year in sub-group analysis of patients with and without prior infective endocarditis. IE, infective endocarditis.
Concerning prosthetic regurgitation, one severe TVL was reported in the IE group (Table 4).
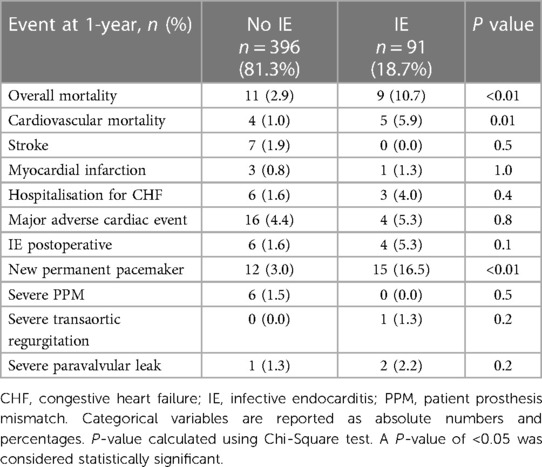
Table 4. Postoperative mortality and morbidity at 1-year follow-up according to endocarditis preoperative status among 489 patients treated with bioprosthetic INSPIRIS aortic valve for severe aortic stenosis.
Redo cardiac surgery at 1-year was required in 6 patients (1.2%): 3 patients had recurrence IE and 3 patients had IE post-operative.
Excluding IE related causes, no structural valve deterioration and valve failure requiring redo surgery were described.
This prospective study offers results on almost 500 patients undergoing AVR with the INSPIRIS RESILIA Edwards bioprosthesis. One-year overall mortality was 4.1% and cardiovascular mortality was 1.9%. A low rate of major cardiac events was observed, as well as satisfactory functional and hemodynamic outcomes. The rate of moderate or severe TVR (0.6%) and the rate of moderate or severe PVL (2.1%) were low. Excluding IE related causes, no structural valve deterioration and valve failure requiring redo surgery were described.
Short and medium term results for the INSPIRIS RESILIA Edwards bioprosthesis have been described in previous studies: low morbidity and mortality, along with a significant decrease in symptoms (10, 11, 15, 16).
In our study, there was no SVD described at 1-year and the risk of valvular reintervention was only related to infective IE. The causes of SVD are threefold, including chemical mechanisms, hemodynamic rheological stresses and an inappropriate immunological response by the host. Regarding the chemical mechanisms, residual phospholipid and aldehyde moieties in processed bioprosthetic valve leaflets are important contributors to the formation of calcium phosphate crystals (17, 18). Glutaraldehyde, an element used during the manufacturing of the bioprosthesis to fix and preserve the biological tissue, seems to preserve the valve's properties of resistance and elasticity and diminishes its antigenicity. However, it paradoxically promotes degeneration by increasing cellular permeability and the process of valvular calcification (19).
To address this problem, the RESILIA tissue of the Edwards INSPIRIS RESILIA bioprosthesis was developed. Due to the neutralization of the free aldehydes present on the prosthetic valve tissue by an industrial chemical process and the conservation of the prosthesis in a glutaraldehyde-free environment, it is likely that the structural degeneration of the prosthetic calcium is slowed down in vivo.
The COMMENCE Trial (20) included 689 patients and reported interesting findings at 5-year follow-up. Freedom from all-cause mortality, all-cause reoperation, and study valve explant were 89.2%, 98.7%, and 99.0%, respectively. Freedom from valve thrombosis, non-SVD, and SVD were all 100%.
Currently, there is no international consensus regarding the management of patients with aortic stenosis who are under 65 years old. In our study, 1 in 5 patients were under 50 years and almost half of the patients were between 50 and 65 years. The American guidelines recommend considering the replacement of the aortic valve by a bioprosthesis starting from the age of 50 (21), while the more conservative European guidelines advocate the use of bioprosthesis in patients over 60 years old (2). The American guidelines reasoning is based on the improved durability of the bioprosthesis which, and especially in the advent of aortic VIV procedure, avoids a surgical re-intervention. Therefore, it is important to consider the longterm cost and impact of this procedure on a young population. Improving the longevity of bioprosthetic valves will make it possible to optimize a patient's lifetime management.
On the other hand, VIV TAVI has emerged as a less invasive alternative to redo surgery for high and intermediate-risk patients. In a meta-analysis, Bruno et al. reported that 30-day all-cause and cardiovascular mortality were significantly lower with VIV compared with redo surgery, with risk of major bleeding significantly lower in patients undergoing VIV (22). However, Nalluri et al. (23) reported no significant difference in 30-day mortality and 1-year mortality between VIV TAVI and redo surgical AVR. Regarding hemodynamic efficiency, Gozdek et al. (7) considered that redo AVR offered superior echocardiographic outcomes with lower incidence of patient-prosthesis mismatch, fewer paravalvular leaks and lower mean postoperative aortic valve gradients. Surgical redo should remain the standard of care, particularly in the low-risk population. The VIV TAVI offers an effective, less invasive alternative for high- risk patients and those who are contraindicated for surgery. In our study, redo surgery was less frequent in patients over 65 years-old and conventional surgery was preferred in younger patients.
INSPIRIS RESILIA valve with VFit technology was developed by adding one sliding zoneto the metal frame of the stent to facilitate the expansion of the prosthetic ring during VIV procedures. The objective is to allow for the implantation of a larger diameter prosthesisthus reducing the risk of mismatch. Moreover, this avoids “cracking” the outcomes of which appear unfavorable with a higher risk of in-hospital mortality and major bleeding, as well as modest improvements in hemodynamic status (24).
We also analyzed IE which affected almost 1 in 5 preoperative patients in our study. At 1-year, the mortality rate of these patients was 10.7%. This rate seems low compared to literature data (25), and can be explained by the younger patient population benefiting from an INSPIRIS RESILIA bioprosthesis and the absence of data regarding annular involvement.
In our study, post-operative IE was responsible for valvular degeneration and for a higher risk of reintervention at 1-year follow-up. Prosthetic valve IE is the most severe form of IE, the incidence was 0.3%–1.2% per patient-years and the actual risk of recurrence of IE varies between 2 and 6% (25).
This study has limitations. First, this is a single arm study without comparative groups.
Moreover we only studied follow up for 1-year. Consequently, we cannot fully address the question of long term durability. The generalizability of the results may be limited by the absence of a predetermined sample size and post-hoc power analysis. Concerning patients under 50 years old, the data is difficult to interpret because of the preoperative overrepresentation of IE in this population. This explains the excess of adverse event in this population. Concerning IE, our data seem to favor INSPIRIS use in this population, however the low number of patients in the study is insufficient to fully address this question. The fact of not excluding patients treated for endocarditis is a bias of confusion, with more complicated consequences. However, this allows us to have a real-work practice.
The Management Of Aortic Stenosis In Young Subjects remains an important topic of discussion. The new generation INPIRIS RESILIA aortic valve bioprosthesis demonstrated excellent hemodynamic performance and safety outcomes at one-year follow-up. Long-term studies are needed to further assess valve durability.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
The studies involving human participants were reviewed and approved by RGPD2019-48. The patients/participants provided their written informed consent to participate in this study.
All authors contributed to the study conception, design, and writing. Conceptualization, AP, FC, VG, AR and AT; methodology, AP and AT; validation, AP, FC, VG and AT; investigation, CA; data curation, CD; writing—original draft preparation, AP, GS, RB, VB and AT; writing—review and editing, AP, GS, RB and AT; visualization, AP, GS, RB and AT; supervision, AP and AT. All authors contributed to the article and approved the submitted version.
The authors declare that this study was funded by Edwards Lifesciences. The funder was not involved in the study design, collection, analysis, interpretation of data, writing of this article or the decision to submit it for publication.
CD is employed by Edwards Lifesciences to perform the statistical analysis.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
AVR, aortic valve replacement; CABG, coronary artery bypass graft; CPB, cardiopulmonary by-pass; CC, cross clampage; CHF, congestive heart failure; EOA, effective orifice area; IE, infective endocarditis; IQR, inter quartile range; iEOA, indexed effective orifice area; LVEF, left ventricular ejection fraction; NYHA, New York heart association; PPM, patient prosthesis mismatch; PVL, para valvular leak; SD, standard deviation; SVD, structural valve degeneration; TAVI, transcatheter aortic valve implantation; TVR, trans valvular regurgitation; VIV, valve-in-valve.
1. Osnabrugge RLJ, Mylotte D, Head SJ, Van Mieghem NM, Nkomo VT, LeReun CM, et al. Aortic stenosis in the elderly. J Am Coll Cardiol. (2013) 62(11):1002–12. doi: 10.1016/j.jacc.2013.05.015
2. Vahanian A, Beyersdorf F, Praz F, Milojevic M, Baldus S, Bauersachs J, et al. 2021 ESC/EACTS guidelines for the management of valvular heart disease. Eur Heart J. (2022) 43(7):561–632. doi: 10.1093/eurheartj/ehab395
3. Kulik A, Bedard P, Lam B, Rubens F, Hendry P, Masters R, et al. Mechanical versus bioprosthetic valve replacement in middle-aged patients. Eur J Cardiothorac Surg. (2006) 30(3):485–91. doi: 10.1016/j.ejcts.2006.06.013
4. Schnittman SR, Adams DH, Itagaki S, Toyoda N, Egorova NN, Chikwe J. Bioprosthetic aortic valve replacement: revisiting prosthesis choice in patients younger than 50 years old. J Thorac Cardiovasc Surg. (2018) 155(2):539–547.e9. doi: 10.1016/j.jtcvs.2017.08.121
5. Zhao DF, Seco M, Wu JJ, Edelman JB, Wilson MK, Vallely MP, et al. Mechanical versus bioprosthetic aortic valve replacement in middle-aged adults: a systematic review and meta-analysis. Ann Thorac Surg. (2016) 102(1):315–27. doi: 10.1016/S0003-4975(16)30623-3
6. Minakata K, Tanaka S, Okawa Y, Shimamoto M, Kaneko T, Takahara Y, et al. Long-term outcome of the carpentier-edwards pericardial valve in the aortic position in Japanese patients. Circ J. (2014) 78(4):882–9. doi: 10.1253/circj.CJ-13-1068
7. Gozdek M, Raffa GM, Suwalski P, Kołodziejczak M, Anisimowicz L, Kubica J, et al. Comparative performance of transcatheter aortic valve-in-valve implantation versus conventional surgical redo aortic valve replacement in patients with degenerated aortic valve bioprostheses: systematic review and meta-analysis. Eur J Cardiothorac Surg. (2018) 53(3):495–504. doi: 10.1093/ejcts/ezx347
8. Bartuś K, Litwinowicz R, Kuśmierczyk M, Bilewska A, Bochenek M, Stąpór M, et al. Primary safety and effectiveness feasibility study after surgical aortic valve replacement with a new generation bioprosthesis: one-year outcomes. Kardiol Pol. (2018) 76(3):618–24. doi: 10.5603/KP.a2017.0262
9. Bartus K, Litwinowicz R, Bilewska A, Stapor M, Bochenek M, Rozanski J, et al. Intermediate-term outcomes after aortic valve replacement with a novel RESILIATM tissue bioprosthesis. J Thorac Dis. (2019) 11(7):3039–46. doi: 10.21037/jtd.2019.07.33
10. Fukunaga N, Yoshida S, Shimoji A, Maeda T, Mori O, Yoshizawa K, et al. Hemodynamic performance of INSPIRIS RESILIA aortic bioprosthesis for severe aortic stenosis: 2-year follow-up in Japanese cohort. J Artif Organs. (2022) 25(4):323–8. doi: 10.1007/s10047-022-01316-5
11. Johnston DR, Griffith BP, Puskas JD, Bavaria JE, Svensson LG, Blackstone EH, et al. Intermediate-term outcomes of aortic valve replacement using a bioprosthesis with a novel tissue. J Thorac Cardiovasc Surg. (2021) 162(5):1478–85. doi: 10.1016/j.jtcvs.2020.01.095
12. Bartus K, Litwinowicz R, Bilewska A, Stapor M, Bochenek M, Rozanski J, et al. Final 5-year outcomes following aortic valve replacement with a RESILIATM tissue bioprosthesis. Eur J Cardiothorac Surg. (2021) 59(2):434–41. doi: 10.1093/ejcts/ezaa311
13. Bavaria JE, Griffith B, Heimansohn DA, Rozanski J, Johnston DR, Bartus K, et al. Five-year outcomes of the COMMENCE trial investigating aortic valve replacement with RESILIA tissue. Ann Thorac Surg. (2023) 115(6):1429–36. doi: 10.1016/j.athoracsur.2021.12.058
14. Kappetein AP, Head SJ, Genereux P, Piazza N, van Mieghem NM, Blackstone EH, et al. Updated standardized endpoint definitions for transcatheter aortic valve implantation: the valve academic research consortium-2 consensus document (VARC-2). Eur J Cardiothorac Surg. (2012) 42(5):S45–60. doi: 10.1093/ejcts/ezs533
15. Puskas JD, Bavaria JE, Svensson LG, Blackstone EH, Griffith B, Gammie JS, et al. The COMMENCE trial: 2-year outcomes with an aortic bioprosthesis with RESILIA tissue†. Eur J Cardiothorac Surg. (2017) 52(3):432–9. doi: 10.1093/ejcts/ezx158
16. El-Sayed Ahmad A, Giammarino S, Salamate S, Fehske W, Sirat S, Amer M, et al. Clinical performance of a novel bioprosthetic surgical aortic valve in a German high-volume center. J Card Surg. (2022) 37(12):4833–40. doi: 10.1111/jocs.17198
17. Perrotta I, Davoli M. Collagen mineralization in human aortic valve stenosis: a field emission scanning electron microscopy and energy dispersive spectroscopy analysis. Ultrastruct Pathol. (2014) 38(4):281–4. doi: 10.3109/01913123.2014.901468
18. Schoen FJ, Levy RJ. Calcification of tissue heart valve substitutes: progress toward understanding and prevention. Ann Thorac Surg. (2005) 79(3):1072–80. doi: 10.1016/j.athoracsur.2004.06.033
19. Velho TR, Pereira RM, Fernandes F, Guerra NC, Ferreira R, Nobre Â. Bioprosthetic aortic valve degeneration: a review from a basic science perspective. Braz J Cardiovasc Surg. 2022;37(2). doi: 10.21470/1678-9741-2020-0635
20. Bavaria JE, Griffith B, Heimansohn DA, Rozanski J, Johnston DR, Bartus K, et al. Five-year outcomes of the COMMENCE trial investigating aortic valve replacement with RESILIA tissue. Ann Thorac Surg. (2023) 11(6):1429–36. doi: 10.1016/j.athoracsur.2021.12.058
21. Otto CM, Nishimura RA, Bonow RO, Carabello BA, Erwin JP, Gentile F, et al. 2020 ACC/AHA guideline for the management of patients with valvular heart disease: executive summary: a report of the American college of cardiology/American heart association joint committee on clinical practice guidelines. Circulation. (2021) 143(5):e72–e227. doi: 10.1161/CIR.0000000000000923
22. Bruno F, Elia E, D’Ascenzo F, Marengo G, Deharo P, Kaneko T, et al. Valve-in-valve transcatheter aortic valve replacement or re-surgical aortic valve replacement in degenerated bioprostheses: a systematic review and meta-analysis of short and midterm results. Catheter Cardiovasc Interv. (2022) 100(1):122–30. doi: 10.1002/ccd.30219
23. Nalluri N, Atti V, Munir AB, Karam B, Patel NJ, Kumar V, et al. Valve in valve transcatheter aortic valve implantation (ViV-TAVI) versus redo-surgical aortic valve replacement (redo-SAVR): a systematic review and meta-analysis. J Intervent Cardiol. (2018) 31(5):661–71. doi: 10.1111/joic.12520
24. Chhatriwalla AK, Allen KB, Depta JP, Rodriguez E, Thourani VH, Whisenant BK, et al. Outcomes of bioprosthetic valve fracture in patients undergoing valve-in-valve TAVR. JACC Cardiovasc Interv. (2023) 16(5):530–9. doi: 10.1016/j.jcin.2022.12.019
25. Habib G, Lancellotti P, Antunes MJ, Bongiorni MG, Casalta JP, Del Zotti F, et al. 2015 ESC guidelines for the management of infective endocarditis: the task force for the management of infective endocarditis of the European society of cardiology (ESC)Endorsed by: european association for cardio-thoracic surgery (EACTS), the European association of nuclear medicine (EANM). Eur Heart J. (2015) 36(44):3075–128. doi: 10.1093/eurheartj/ehv319
Keywords: aortic valve replacement, bioprosthetic valves, INPIRIS RESILIA valve, structural valve degeneration, mortality
Citation: Porto A, Stolpe G, Badaoui R, Boudouresques V, Deutsch C, Amanatiou C, Riberi A, Gariboldi V, Collart F and Theron A (2023) One-year clinical outcomes following Edwards INSPIRIS RESILIA aortic valve implantation in 487 young patients with severe aortic stenosis: a single-center experience. Front. Cardiovasc. Med. 10:1196447. doi: 10.3389/fcvm.2023.1196447
Received: 29 March 2023; Accepted: 26 June 2023;
Published: 3 August 2023.
Edited by:
Thierry Caus, University of Picardie Jules Verne, FranceReviewed by:
Mario Lusini, Campus Bio-Medico University Hospital, Italy© 2023 Porto, Stolpe, Badaoui, Boudouresques, Deutsch, Amanatiou, Riberi, Gariboldi, Collart and Theron. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Alizee Porto YWxpemVlLnBvcnRvQGFwLWhtLmZy Alexis Theron YWxleGlzLnRoZXJvbkBhcC1obS5mcg==
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.