
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
EDITORIAL article
Front. Cardiovasc. Med., 28 April 2023
Sec. Heart Valve Disease
Volume 10 - 2023 | https://doi.org/10.3389/fcvm.2023.1193544
This article is part of the Research TopicBicuspid Aortic Valve: From pathophysiological mechanisms, imaging diagnosis to clinical treatment methodsView all 14 articles
 Yi Zhang1,†
Yi Zhang1,† Tian-Yuan Xiong1,†
Tian-Yuan Xiong1,† Lars Sondergard2
Lars Sondergard2 Darren Mylotte3
Darren Mylotte3 Nicolo Piazza4
Nicolo Piazza4 Bernard Prendergast5,6
Bernard Prendergast5,6 Mao Chen1*
Mao Chen1*
Editorial on the Research Topic
Bicuspid aortic valve: from pathophysiological mechanisms, imaging diagnosis to clinical treatment methods
This Research Topic, entitled “Bicuspid Aortic Valve: From pathophysiological mechanisms, imaging diagnosis to clinical treatment methods”, is created to set a forum for researches that tackle the difference or uniqueness of the BAV entity, from genetic, cellular and pathophysiological mechanisms of BAV and the subsequent bicuspid aortic stenosis, clinical imaging for bicuspid aortic stenosis to unveil its function and anatomy, treatment innovations and strategies tailored for bicuspid aortic stenosis, to clinical outcomes. Herein, we introduce the 13 articles collected in this Research Topic (Table 1).
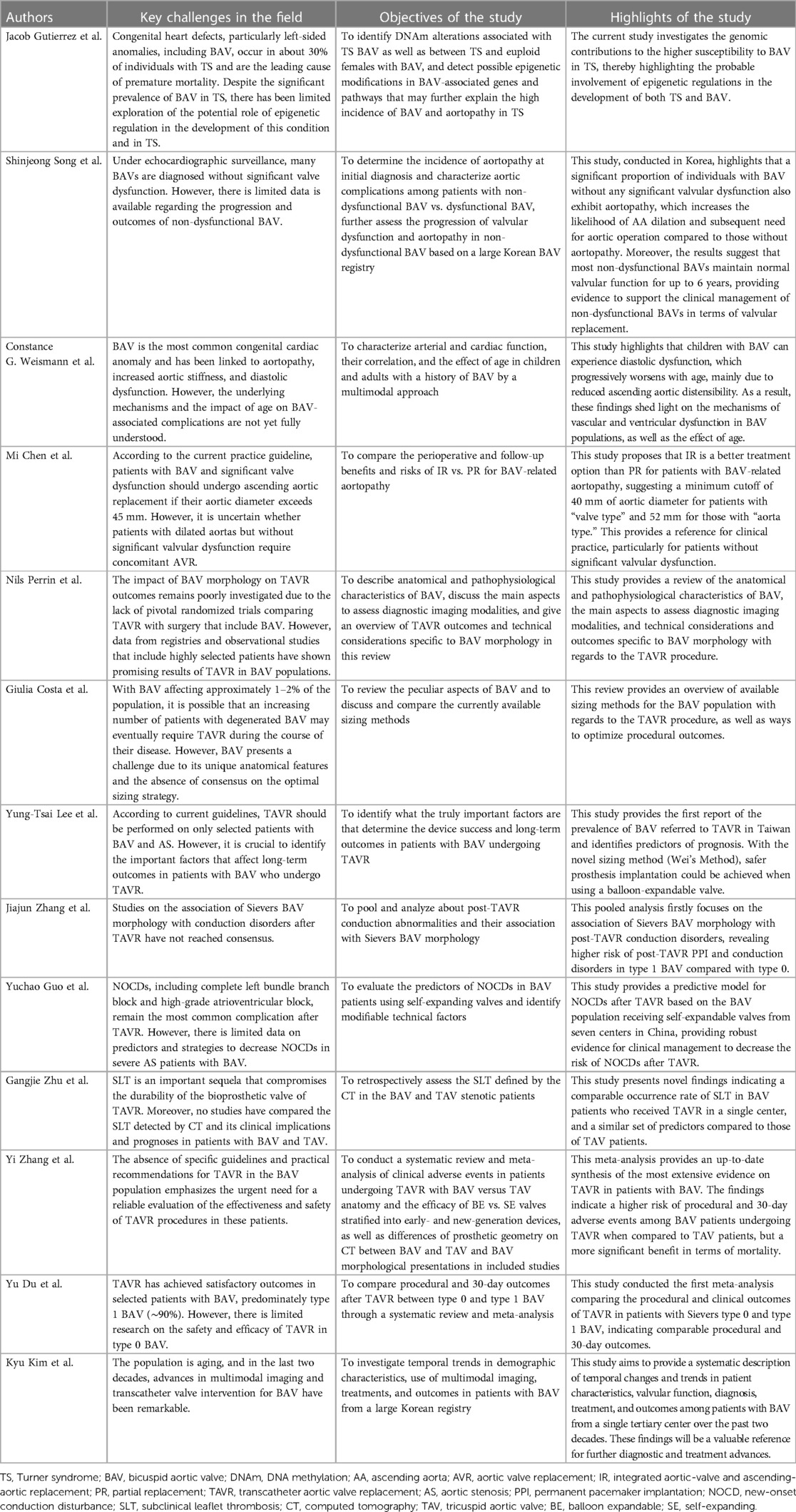
Table 1. Information and highlights of the 13 articles in the research topic.
The genetics behind BAV are acknowledged to be different from a normal tricuspid aortic valve (TAV), as patients with BAV may develop aortic malformations, valvular dysfunctions, or symptoms at a younger age. Several genomic mutations have been found to be associated with BAV, such as mutations in NOTCH1, ROBO4, etc. (1). In this research topic, Jacob Gutierrez et al. identified that patients with Turner syndrome (TS), a rare cytogenetic disorder presenting a 60-fold increased risk of BAV compared to the general population, have differentially methylated regions (DMRs) encompassing MYRF and enrichment for genomic targets, including genes in NOTCH1 and the downstream gene MYH11 in those with concomitant BAV. These DMRs in TS appeared to contribute to both BAV development and BAV-associated aortopathy, adding evidence in the genomic etiology of congenital BAV.
With the generalization of echocardiographic surveillance, the diagnosis of non-dysfunctional BAV (BAV without significant aortic stenosis or aortic regurgitation) is increasing. Based on a BAV registry enrolling patients from a single hospital in Seoul, Shinjeong Song et al. found that patients with non-dysfunctional BAV, especially the true BAV, were more likely to be considered as candidates for aortic surgery due to the progression of ascending aortic dilatation. In addition, most non-dysfunctional BAVs could still maintain normal valve function 6 years after their initial diagnosis. In patients with non-dysfunctional BAV, initial BAV function and degree of aorta dilatation might be important factors for disease progression and prognosis.
Aortopathy is common in the BAV population and may predispose to aortic stiffening, dilation and dissection. Despite controversies, aortic stiffening may lead to heart failure through arterio-ventricular interaction (2, 3). In this research topic, Constance G. Weismann et al. used a multimodal method to reveal that ascending aortic distensibility appears to be the most important predictor of diastolic dysfunction in the BAV population, with increased proximal aortic stiffness and wave reflection in both children and adults. Therefore, timely management of proximal arterial stiffness may be a target to prevent further diastolic dysfunction in the BAV population.
Concomitant aortic dilatation is present in about 20%–40% of BAV patients, which may be secondary to abnormalities of the aortic media (4, 5). Currently, guideline recommends ascending aortic replacement in dysfunctional BAV with concomitant dilated aorta if the cutoff of 45 mm is reached (6). Mi Chen et al. proposed a classification to describe the BAV-related dilated aortopathy into valve type and aorta type which represents the most dysfunctional part. Integrated aortic-valve and ascending-aortic replacement (IR) was associated with long-term mortality and reoperation benefits compared to partial replacement, with an IR cutoff of 40 mm in the “valve type” and 52 mm in the “aorta type”. This finding provides a preliminary exploration of the surgical therapy in BAV with different types of dilated aortopathy, providing a reference for clinical management.
Bicuspid aortic stenosis is one of the most encountered complications in patients with BAV, occurring in >20% of high-risk elderly patients undergoing surgery (7). With the advent of transcatheter aortic valve replacement (TAVR), patients with severe aortic stenosis of any surgical risk have an alternative beneficial therapy. However, bicuspid aortic stenosis has long been regarded as a challenging anatomy. Nils Perrin et al. reviewed the BAV population in the setting of TAVR Apart from the most widely known BAV classification proposed by Sievers, several novel classifications have been updated in aim to achieve better description of the anatomy and prediction of interventional outcomes (8–10). Despite the technical improvements in imaging modalities, difficulties remain in TAVR planning and execution for BAV due to its distinctive anatomy and hemodynamics. The eccentricity of the opening orifice, the asymmetric heavy burden of calcium deposition in BAV would increase the risk of device malposition and mal-expansion, annular rupture, etc. These suboptimal interactions could further lead to new-onset conduction disturbances (NOCDs) and subclinical leaflet thrombosis (SLT), impeding the durability of the bio-prosthesis and patient prognosis.
In order to achieve better results, several sizing strategies have been proposed. Giulia Costa et al. have discussed and compared the currently available sizing methods for TAVR in terms of BAV population, such as “annular” sizing, “supra-annular” sizing, “balloon-technique” BAV sizing, “raphe-based” sizing, Casper algorithm and LIRA method. A specific prosthesis sizing method, i.e., the Wei's method was proposed by Yung-Tsai Lee et al. which achieved safe implantation and efficacious performance of Sapien 3 in the BAV population. The different sizing techniques that have emerged have not yet been tested in large trials, and therefore a better understanding of BAV sizing is needed, especially with regard to different types of devices. Despite prosthesis iteration, new-onset conduction disturbances (NOCDs) are one of the most common complications of TAVR with an increased risk of mortality and rehospitalization (11). Sievers type 1 BAV morphology seems to have a higher risk of permanent pacemaker implantation (PPI) and NOCDs after TAVR than type 0, as reported by Jiajun Zhang et al. To best predict NOCDs in BAV after TAVR who received self-expanding valves, Yuchao Guo et al. have built a model including age, oversizing ratio on left ventricular outflow tract and Δcoronal membranous septum minus implantation depth. Moderate reduction of the oversizing ratio may be a feasible strategy to reduce conduction disturbances while maintaining good peri-procedural outcomes in heavily calcified bicuspid anatomy with short membranous septum length. Regarding the incidence of SLT in patients undergoing TAVR, comparable data were observed between BAV and TAV at 30 days or 1 year after TAVR, as reported by Gangjie Zhu et al. providing more specific evidence of SLT in the BAV population.
Studies are encouraging in the light of similar outcomes to TAVR for the BAV versus TAV population (12, 13). Yi Zhang et al. and Yu Du et al. have done meta-analyses focused on the prognosis of TAVR in BAV patients, both of which demonstrated similar in-hospital and 30-day post-TAVR mortality not only between BAV and TAV, but also between Sievers type 0 BAV and Sievers type 1 BAV, despite a higher risk of other procedural complications such as conversion to surgery, valve-in-valve, paravalvular leak, device failure, acute kidney injury, PPI, and stroke. BAV patients showed a lower 1-year mortality after TAVR than TAV in the report. As the application of TAVR in patients with BAV becomes more frequently on a day-to-day basis in clinical practice, consensus and studies aim for a standardized protocol on TAVR in BAV are being updated (14, 15). Further randomized trials are needed for guidance and standardization of specific peri-operative techniques of TAVR for heterogeneous BAV anatomies, as well as the prognosis in this population.
The demographic characteristics, multimodal imaging, and interventional therapy of BAV have changed over the past two decades. To explore the temporal trends of the aforementioned aspects of the BAV population, Kyu Kim et al. analyzed data from a large Korean registry, and revealed a significant temporal increase in both the age of initial diagnosis and indexed intervention or surgery in the BAV population. Over time, the proportions of non-dysfunctional BAV and significant aortic stenosis increased, while those of significant aortic regurgitation and infective endocarditis decreased. An increase in the use of bioprosthetic valves and TAVR, and survival improvements in BAV were observed.
In summary, the 13 articles in this Research Topic presented the latest advances in the aforementioned aspects of BAV. These discoveries help to better understand and guide clinical practice in this population. However, the conclusions need to be further validated by larger studies and randomized trials in view of the limitations caused by their small size and non-randomized natures.
YZ and T-YX drafted the editorial with guidance and comments from LS, DM, NP, BP, and MC. All authors contributed to the article and approved the submitted version.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Gould RA, Aziz H, Woods CE, Seman-Senderos MA, Sparks E, Preuss C, et al. ROBO4 variants predispose individuals to bicuspid aortic valve and thoracic aortic aneurysm. Nat Genet. (2019) 51:42–50. doi: 10.1038/s41588-018-0265-y
2. Weismann CG, Lombardi KC, Grell BS, Northrup V, Sugeng L. Aortic stiffness and left ventricular diastolic function in children with well-functioning bicuspid aortic valves. Eur Heart J Cardiovasc Imaging. (2016) 17:225–30. doi: 10.1093/ehjci/jev151
3. Lee SY, Shim CY, Hong GR, Seo J, Cho I, Cho IJ, et al. Association of aortic phenotypes and mechanical function with left ventricular diastolic function in subjects with normally functioning bicuspid aortic valves and comparison to subjects with tricuspid aortic valves. Am J Cardiol. (2015) 116:1547–54. doi: 10.1016/j.amjcard.2015.08.017
4. Masri A, Svensson LG, Griffin BP, Desai MY. Contemporary natural history of bicuspid aortic valve disease: a systematic review. Heart. (2017) 103:1323–30. doi: 10.1136/heartjnl-2016-309916
5. Siu SC, Silversides CK. Bicuspid aortic valve disease. J Am Coll Cardiol. (2010) 55:2789–800. doi: 10.1016/j.jacc.2009.12.068
6. Erbel R, Aboyans V, Boileau C, Bossone E, Bartolomeo RD, Eggebrecht H, et al. 2014 ESC guidelines on the diagnosis and treatment of aortic diseases: document covering acute and chronic aortic diseases of the thoracic and abdominal aorta of the adult. The task force for the diagnosis and treatment of aortic diseases of the European society of cardiology (ESC). Eur Heart J. (2014) 35:2873–926. doi: 10.1093/eurheartj/ehu281.25173340
7. Roberts WC, Janning KG, Ko JM, Filardo G, Matter GJ. Frequency of congenitally bicuspid aortic valves in patients ≥80 years of age undergoing aortic valve replacement for aortic stenosis (with or without aortic regurgitation) and implications for transcatheter aortic valve implantation. Am J Cardiol. (2012) 109:1632–6. doi: 10.1016/j.amjcard.2012.01.390
8. Sievers HH, Schmidtke C. A classification system for the bicuspid aortic valve from 304 surgical specimens. J Thorac Cardiovasc Surg. (2007) 133:1226–33. doi: 10.1016/j.jtcvs.2007.01.039
9. Michelena HI, Della Corte A, Evangelista A, Maleszewski JJ, Edwards WD, Roman MJ, et al. International consensus statement on nomenclature and classification of the congenital bicuspid aortic valve and its aortopathy, for clinical, surgical, interventional and research purposes. J Thorac Cardiovasc Surg. (2021) 162:e383–414. doi: 10.1016/j.jtcvs.2021.06.019
10. Jilaihawi H, Chen M, Webb J, Himbert D, Ruiz CE, Rodés-Cabau J, et al. A bicuspid aortic valve imaging classification for the TAVR era. JACC Cardiovasc Imaging. (2016) 9:1145–58. doi: 10.1016/j.jcmg.2015.12.022
11. Faroux L, Chen S, Muntané-Carol G, Regueiro A, Philippon F, Sondergaard L, et al. Clinical impact of conduction disturbances in transcatheter aortic valve replacement recipients: a systematic review and meta-analysis. Eur Heart J. (2020) 41:2771–81. doi: 10.1093/eurheartj/ehz924
12. Makkar RR, Yoon SH, Chakravarty T, Kapadia SR, Krishnaswamy A, Shah PB, et al. Association between transcatheter aortic valve replacement for bicuspid vs tricuspid aortic stenosis and mortality or stroke among patients at low surgical risk. J Am Med Assoc. (2021) 326:1034–44. doi: 10.1001/jama.2021.13346
13. Yoon SH, Bleiziffer S, De Backer O, Delgado V, Arai T, Ziegelmueller J, et al. Outcomes in transcatheter aortic valve replacement for bicuspid versus tricuspid aortic valve stenosis. J Am Coll Cardiol. (2017) 69:2579–89. doi: 10.1016/j.jacc.2017.03.017
14. Xiong TY, Ali WB, Feng Y, Hayashida K, Jilaihawi H, Latib A, et al. Transcatheter aortic valve implantation in patients with bicuspid valve morphology: a roadmap towards standardization. Nat Rev Cardiol. (2023) 20:52–67. doi: 10.1038/s41569-022-00734-5
Keywords: bicuspid aortic valve, valvular heart disease, aortopathy, aortic dilatation, transcatheter aortic valve replacement
Citation: Zhang Y, Xiong T-Y, Sondergard L, Mylotte D, Piazza N, Prendergast B and Chen M (2023) Editorial: Bicuspid aortic valve: from pathophysiological mechanisms, imaging diagnosis to clinical treatment methods. Front. Cardiovasc. Med. 10:1193544. doi: 10.3389/fcvm.2023.1193544
Received: 25 March 2023; Accepted: 18 April 2023;
Published: 28 April 2023.
Edited and Reviewed by: Elena Aikawa, Brigham and Women's Hospital and Harvard Medical School, United States
© 2023 Zhang, Xiong, Sondergard, Mylotte, Piazza, Prendergast and Chen. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Mao Chen aG1hb2NoZW5AdmlwLnNpbmEuY29t
†These authors have contributed equally to this work
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.