
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
REVIEW article
Front. Cardiovasc. Med. , 25 May 2023
Sec. Cardiac Rhythmology
Volume 10 - 2023 | https://doi.org/10.3389/fcvm.2023.1187754
This article is part of the Research Topic Electrical Management of Heart Failure: Shaping the future of cardiac pacing and electrophysiology View all 8 articles
 Nadeev Wijesuriya1,2*
Nadeev Wijesuriya1,2* Vishal Mehta1,2
Vishal Mehta1,2 Felicity De Vere1,2
Felicity De Vere1,2 Marina Strocchi1
Marina Strocchi1 Jonathan M. Behar1,2
Jonathan M. Behar1,2 Steven A. Niederer1,3
Steven A. Niederer1,3 Christopher A. Rinaldi1,2
Christopher A. Rinaldi1,2
Conduction system pacing (CSP) has emerged as a promising novel delivery method for Cardiac Resynchronisation Therapy (CRT), providing an alternative to conventional biventricular epicardial (BiV) pacing in indicated patients. Despite increasing popularity and widespread uptake, CSP has rarely been specifically examined in patients with atrial fibrillation (AF), a cohort which forms a significant proportion of the heart failure (HF) population. In this review, we first examine the mechanistic evidence for the importance of sinus rhythm (SR) in CSP by allowing adjustment of atrioventricular delays (AVD) to achieve the optimal electrical response, and thus, whether the efficacy of CSP may be significantly attenuated compared to conventional BiV pacing in the presence of AF. We next evaluate the largest clinical body of evidence in this field, related to patients receiving CSP following atrioventricular nodal ablation (AVNA) for AF. Finally, we discuss how future research may be designed to address the vital question of how effective CSP in AF patients is, and the potential hurdles we may face in delivering such studies.
Cardiac Resynchronisation Therapy (CRT) is a cornerstone in the electrical treatment of heart failure (1). Conventional CRT involves biventricular (BiV) pacing from transvenous leads in the right ventricle (RV) and a coronary sinus branch to provide epicardial left ventricular (LV) stimulation. The widespread uptake of CRT has been driven by evidence showing significant benefits in both hospitalisations and mortality for patients with symptomatic dyssynchronous heart failure, that is, those with a LV ejection fraction (EF) of below 35%, and a QRS duration (QRSd) of greater than 130 milliseconds (ms) on a 12 lead electrocardiograph (ECG) (2). In recent years, the indications for CRT have expanded, with studies showing benefits in patients with moderate LV dysfunction who have a high burden of RV pacing (3) and in those requiring an atrioventricular node ablation (AVNA) (4).
Despite its success, there is a significant proportion of patients who either do not derive clinical benefit from conventional CRT (5), or who cannot be treated due to failure of LV lead implantation or inadequate LV lead performance due to issues such as high thresholds and phrenic nerve stimulation (6). Conduction system pacing (CSP), that is, stimulation of His-Purkinje tissue using a transvenous lead-based system (7), is becoming increasingly popular, not only as a “bail-out” treatment in this population, but also potentially as a first-line option in selected patients (8). Initial studies on CSP focused on His-Bundle pacing (HBP), built on the attractive concept of restoring completely physiological ventricular activation. HBP achieves excellent cardiac resynchronisation, but implantation can be difficult, with success rates varying from 56%–95% (7, 9, 10). Challenges such as ventricular under-sensing, rising thresholds and requirement for lead revisions have also been observed during long-term follow up (11, 12). Left Bundle Branch Pacing (LBBP) is a relatively novel form of CSP which involves screwing a pacing lead deep into the interventricular septum from the RV in order to capture the left bundle system (13, 14). This technique has shown encouraging results from observational studies, with reported success rates of 80%–94% and significant improvements in LV function (13, 15). Robust data from randomized trials, however, is currently lacking, and despite widespread uptake and investigation of CSP, important questions on its use remain.
An area of significant clinical importance is the role of CSP both in the presence of, and in the treatment of atrial fibrillation (AF). AF is the most prevalent arrhythmia worldwide (16), and is very common in the heart failure population, affecting up to a third of patients receiving CRT (17). Several studies have reported an attenuation of clinical benefit achieved with CRT in the presence of AF (18–20). There are likely several mechanisms behind this, including the reduction in cardiac output associated with loss of atrial systole (21), low BiV pacing percentage due to uncontrolled ventricular rates (22), and increased risk of inappropriate shocks from implantable cardioverter defibrillators (ICDs) (23).
In view of the significant deleterious consequences that AF has on conventional CRT, and the increasing use of CSP in this patient population, it is crucial to examine whether the presence of AF affects outcomes of HBP and LBBP. This article focuses on two areas. First, we evaluate the possible impact of AF on CSP, specifically LBBP, due to the inability to improve ventricular dyssynchrony by adjusting AVDs to achieve fusion pacing with intrinsic RV conduction (13). Next we review the largest clinical body of evidence in the case of CSP use following AVNA for AF. Finally, we discuss how future studies may address the important issue of CSP efficacy in patients with AF.
The primary attraction of CSP is theoretically in more closely mimicking physiological ventricular electrical activation, thus minimising ventricular dyssynchrony. There is emerging evidence that the presence of sinus rhythm (SR) and intact AV node conduction may be crucial in this process. This raises the question of CSP efficacy, particularly LBBP efficacy, when patients are in AF or have complete heart block (CHB), which is highly pertinent in the AVNA population. The majority of evidence in this area is in the form of in-silico models, mechanistic and observational studies.
Curila et al. examined the activation patterns of patients receiving LBBP in a series of studies utilising ultra-high frequency ECG during temporary pacing protocols (24, 25). These studies demonstrated that LBB capture, whilst leading to accelerated LV lateral wall activation, led to increased interventricular dyssynchrony compared to LV septal myocardial pacing (LVSMP) due to late RV activation. Interestingly, this dyssynchrony was reduced in a proportion patients where bipolar anodal septal capture could be achieved, leading to simultaneous RBB, LV septal and LBB capture, compared to unipolar LBB capture in the same patients (26).
Strocchi et al. (27) simulated BiV activation on 24 four-chamber heart meshes in the presence of left bundle branch block (LBBB). The authors simulated conventional BiV epicardial pacing, BiV endocardial pacing with LV lead at the lateral wall, BiV endocardial pacing with LV lead at the LV septum, HBP, and LBBP. They found that both selective and non-selective HBP improved response metrics such as QRSd, LV activation time (LVAT), RV activation time (RVAT), BIV activation time (BiVAT) and BiV dyssynchrony index (BiV-DI) compared to BiV epicardial or endocardial pacing. With regards to LBBP, they reported that in the presence of simulated CHB, LBBP led to increased ventricular dyssynchrony compared to HBP due to increases in RVAT (141.3 ± 10.0 ms versus 111.8 ± 10.4 ms). RVAT, and therefore BiVAT, was improved in patients with intact native conduction when AV delay (AVD) optimisation was performed to allow intrinsic RV activation via the right bundle branch (RBB), with response metrics similar to those achieved with HBP (Figure 1). In the presence of CHB, RV apical pacing was required in addition to LV LBBP in order to maintain BiV synchrony by preventing late RV activation.
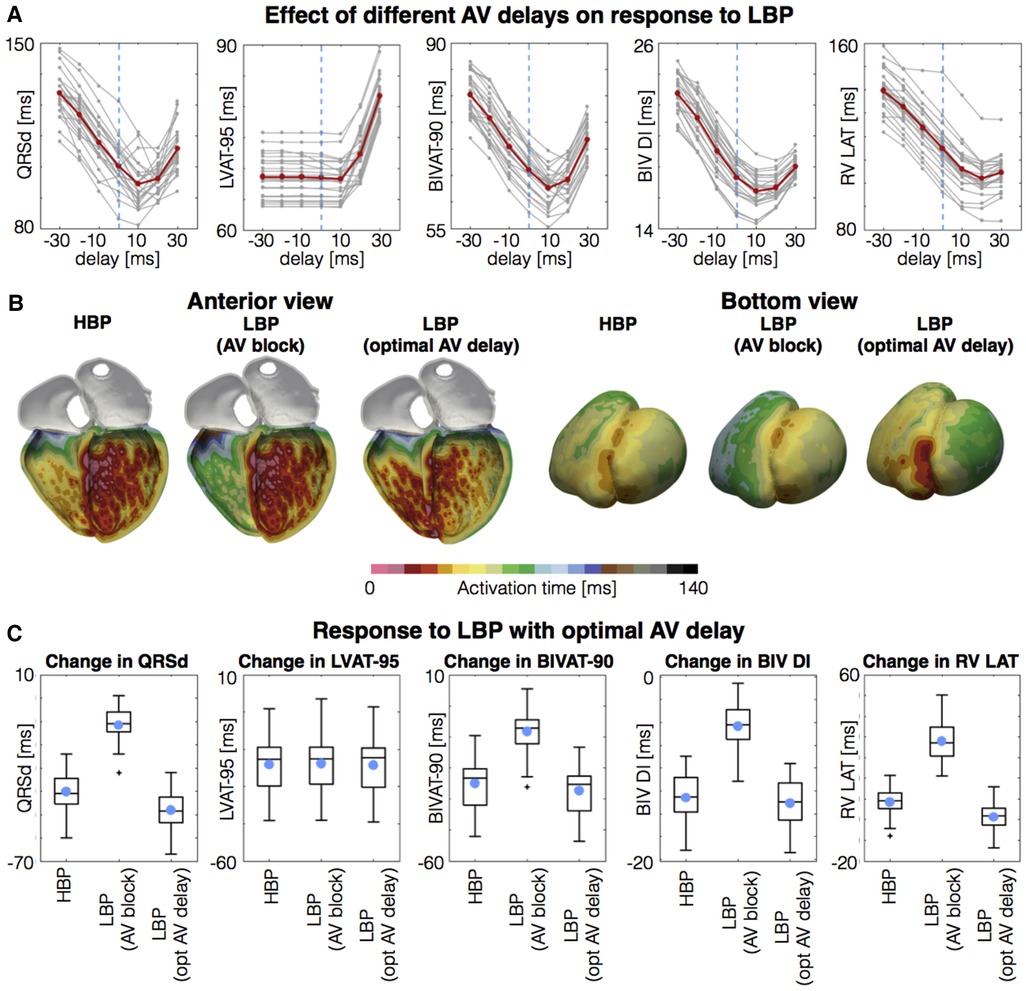
Figure 1. Response to LBP with optimized AV delay. (A) Response measures simulated with different AV delays. Negative and postive delays mean that the left bundle is paced before and after the atrial stimulus enters the His, respectively. Gray lines represent the patients. Red lines represent the mean. (B) Activation times with selective HBP, selective LBP with complete AV block and with optimal AV delay. (C) Boxplots of change in QRSd, LVAT-95, BIVAT-90, BIV DI, and RV Latest AT for selective HBP, selective LBP with complete AV block and with optimal AV delay. Light blue circles represent mean values. Plus symbols represent outliers. AV, atrioventricular; BIV DI, biventricular dyssynchronous index; BIVAT-90, 90% biventricular activation time; HBP, his-bundle pacing; LBP, left bundle pacing; LVAT-95, 95% left ventricular activation time; QRSd, QRS duration; RV LAT, right ventricular latest activation time. Reproduced from Strocchi et al (27) with permission.
This phenomenon has also been observed in-vivo. Padala et al. (15) report a case of LBBP as a bailout treatment for a patient with ischaemic cardiomyopathy and several failed coronary sinus lead implants. The baseline ECG showed sinus rhythm and LBBB with QRSd 156 ms. Pacing with AVD set at 40 ms resulted in LBBA capture with RBBB pattern in lead V1 with QRSd of 128 ms. Pacing with AVD set at 80 ms resulted in normalization of QRSd to 120 ms, due to fusion between anterograde RBBB conduction and LBBP (Figure 2).

Figure 2. Response to LBBP. (A) ECG showing SR and LBBB with QRSd 156 ms. (B) Pacing with AV delay set at 40 ms resulted in resulted in QRSd of 128 ms. (C) Pacing with AV delay set at 80 ms resulted in normalization of QRSd to 120 ms.
These results were supported by Huang et al. (28), who reported the outcomes of 63 patients with non-ischaemic cardiomyopathy and LBBB implanted with a LBBP device. They found that during unipolar tip LBBP, the QRSd narrowed significantly from 169 ± 16 ms at baseline to 118 ± 12 ms, and then further to 103 ± 9 ms (p < 0.05) during LBBP fused with native conduction by optimizing AVD.
A study performed by Wu et al. (29) again demonstrated the possible benefits of AVD optimisation. In a non-randomised comparison, 49 patients received HBP, 32 received LBBP and 54 received standard BiV pacing. In this study, HBP resulted in normalization of QRS morphology, with the mean paced QRSd of 100.7 ± 15.3 ms; LBBP resulted in a paced QRS morphology of RBBB pattern, with a mean paced QRSd was 110.8 ± 11.1 ms; the QRSd further reduced to 104.3 ± 8.1 ms with AVD optimization to promote fusion pacing. Maximum reduction in QRS duration was observed during HBP (Δ QRSd = 69 ms) and fused LBBP (Δ QRSd = 65 ms). A modest improvement was seen with LBBP in the absence of AVD optimisation (Δ QRS duration = 56 ms), and minor improvements were seen with BiV pacing (Δ QRS duration = 26 ms).
These studies suggest that, in order to achieve similar electrical outcomes to HBP, LBBP needs to be combined with AVD optimisation to obtain fusion with native RBBB conduction. However, the functional benefit gained from a relatively small improvement in QRSd remains unclear. In an acute electrocardiographic imaging (ECGi) and haemodynamic study using temporary pacing protocols, Ali et al. (30) found that the optimal AVD to achieve fusion pacing with LBBP resulted in the best acute systolic blood pressure increase in only 6 out of 19 patients in the study. This indicated that the relationship between the AVD and LBBP is more complex than simply achieving ventricular resynchronisation. Contributory factors such as the duration of passive ventricular filling, atrial mechanical systole and RV function mean that the optimal AVD for an individual patient is not a metric which can be determined purely electrically. Indeed, studies have shown that in conventional CRT, the optimal AVD for filling is different to the optimal AVD for fusion (31).
In addition, no in-vivo studies have thus far demonstrated that AVD optimisation to achieve fusion impacts the acute haemodynamic performance of LBBP when compared to conventional BiV epicardial pacing. For example, in an acute ECGi and haemodynamic study, Elliott et al. (32) reported that LBBP, HBP and BiV endocardial pacing all outperform conventional BiV epicardial pacing in the absence of AVD optimisation. As such, the presence or absence of AF may not have a significant enough bearing on the efficacy of LBBP to change treatment decisions surrounding CRT modality.
There is some comparative clinical evidence to support this. Huang et al. (28) reported an observational study of patients with non-ischaemic cardiomyopathy and LVEF < 50% who received LBBP. At 6-months follow up, there was no significant difference in improvement in LVEF or New York Heart Association (NYHA) functional class between the patients in SR (n = 48) and those in persistent AF (n = 14). This could suggest that improved ventricular synchrony due to less delayed RV activation during AVD optimisation (or indeed, anodal capture in applicable instances) may not necessarily translate to an improvement in clinical outcomes, and that examination of larger studies reporting longer term data will be needed to form more robust conclusions.
AVNA has been shown to improve CRT outcomes in patients with AF (18). Gasparini et al. reported results from the CERTIFY study (33), a multinational registry comprising 1,338 patients with AF and 6,046 patients in SR. They found that at median follow-up of 37 months, total mortality rates in patients with AF treated with AVNA (n = 443) were similar to patients in SR. In contrast, patients with AF treated with medications alone had a significantly higher mortality rate than patients in SR. The authors postulated that this was primarily due to an increase in BiV pacing percentage in the AVNA group compared to the non-AVNA group (96% vs. 87%).
With regards to the benefits of AVNA plus CRT over pharmacological therapy in patients with a narrow native QRS and symptomatic permanent AF, the APAF-CRT study (4) reported all-cause mortality in 133 patients randomised to pharmacological therapy or AVNA plus conventional BiV CRT. There was a significant reduction in all-cause mortality in the AVNA group (11% vs. 29%, p = 0.004), with similar results seen in both patients whose LVEF was <35% or >35%. Previous studies have demonstrated that CRT outperforms RV pacing alone in patients receiving AVNA (34). Evidence such as this has motivated the examination of CSP in patients requiring AVNA. This is currently where the bulk of clinical evidence is derived on the use of CSP in the context of AF.
Several small, retrospective studies have demonstrated the feasibility of HBP and AVNA. Vijayaraman et al. (35) reported the results of 42 consecutive patients who underwent HBP and AVNA, with an overall procedural success rate of 95%. They documented that the successful AVNA site was at or below the ring electrode in 22 patients (no acute change in HBP threshold); above the ring electrode in 13 patients, and from the left side in 2 patients (acute increase in HBP threshold in 7 of 15 patients). LVEF increased from 43% ± 13% to 50% ± 11% (p = 0.01), and NYHA functional status improved from 2.5 ± 0.5 to 1.9 ± 0.5 (p = 0.04). The overall increase in HBP threshold was 0.6 V at a mean follow up of 19 months. One patient required HBP lead revision. The authors concluded that HBP was a feasible technique for delivery of CRT post-AVNA. The study does, however, highlight the limitations of this intervention with regards to long-term lead performance, which may be ablation-site dependent. Similar success rates and echocardiographic improvements were reported in a retrospective study of 94 patients performed by Su et al. (36), as well as in several smaller studies (37, 38).
In terms of potential benefits of CSP and AVNA approach compared to pharmacological rate control therapy, Wang et al. (39) retrospectively analysed data from 86 non pacing-dependent patients with persistent AF undergoing ICD implantation. Fifty-two patients also underwent CSP to achieve CRT (HBP n = 44; LBBP n = 8), followed by an AVNA, while the remaining patients received pharmacological rate control. They reported that patients receiving CSP had lower incidence of inappropriate shock (15.6% vs. 0%, p < 0.01), and demonstrated an improvement in LVEF (15% vs. 3%, p < 0.001) compared to patients receiving ICD implantation and pharmacological rate control. Whilst this evidence is not as robust as the APAF-CRT prospective randomised trial (4), it does signal that CSP may perform similarly to conventional CRT post-AVNA with regards to added benefit over pharmacological rate control.
Data comparing CSP to conventional BiV pacing post-AVNA has also been published. In a small, retrospective analysis of 24 patients (HBP n = 12, BiV CRT n = 12), Zizek et al. (40) reported improved echo outcomes in the HBP group. These results have been subsequently supported in the ALTERNATIVE-AF trial (41). This was a randomized crossover trial which recruited patients with persistent AF and a LVEF ≤ 40%. All patients underwent AVNA and received both HBP and conventional BIV pacing. Fifty patients were randomized to either HBP or BiV pacing for 9 months (phase 1), then were switched to the alternative pacing modality for the next 9 months (phase 2), with 38 patients completing both phases, thus being included in the cross-over analysis. The primary endpoint was change in LVEF. A significant improvement in LVEF was observed with HBP compared to BiV pacing (phase 1: ΔLVEFHBP 21.3% and ΔLVEFBiV 16.7%; phase 2: ΔLVEFHBP 3.5% and ΔLVEFBiV −2.4%; pgeneralized additive model = 0.015). Significant improvements in LV end-diastolic diameter, NYHA functional class, and B-type natriuretic peptide level were observed with both pacing modalities compared with baseline, whereas no significant differences were observed between HBP and BiV pacing.
Vijayaraman et al. (42) published a non-randomised on-treatment comparison of 223 patients, with 110 having received CSP (84 HBP, 26 LBBP), and 113 receiving conventional pacing (CP, RVP or BiV pacing based on operator discretion). QRSd increased from 103 ± 30 ms to 124 ± 20 ms (p < .01) in CSP and 119 ± 32 ms to 162 ± 24 ms in CP (p < .001). During a mean follow-up of 27 ± 19 months, LVEF significantly increased from 46.5% ± 14.2% to 51.9% ± 11.2% (p = .02) in CSP and 36.4% ± 16.1% to 39.5% ± 16% (p = .04) in CP. The primary combined endpoint of time to death or heart failure hospitalisation was significantly reduced in CSP compared to CP (48% vs. 62%; hazard ratio 0.61, 95% CI: 0.42–0.89, p < .01). Of note, whilst this was a large study, 24% of patients with impaired LVEF received RVP, which likely negatively impacted outcomes in the CP cohort.
As yet, there are no randomised control trials examining the role of LBBP following AVNA, however, retrospective analyses have been performed. Cai et al. (43) prospectively enrolled 99 patients who received AVNA and LBBP for AF rate control. Implant success rate was 100%. LVEF improved from baseline 30.3% ± 4.9 to 47.3% ± 14.5 at 12 months follow-up in HF patients with reduced LVEF and from baseline 56.3% ± 12.1 to 62.3% ± 9.1 in HF patients with preserved LVEF (both p < 0.001). Outcomes of 86 of these patients were compared to a propensity-matched cohort who had received HBP. No significant differences in echocardiographic or clinical outcomes were observed between HBP and LBBP, however, lower thresholds, greater sensed R-wave amplitudes, and fewer complications were observed in the propensity-matched LBBP group (p < 0.05).
Pillai et al. (44) performed a retrospective analysis directly comparing 98 consecutive patients referred for CSP leads over a 7 year period, where 48 received HBP and 50 received LBBP prior to AVNA. The authors reported an acute success rate of the AVNA procedure of 94% vs. 100% (p = .11) in HBP vs. LBBP groups. Seven (14%) redo AVNA procedures were required in the HBP group. Mean procedural time (44 ± 24 min vs. 34 ± 16 min; p = .02) and mean fluoroscopy time (16 ± 18 min vs. 7 ± 6 min; p < .001) were significantly longer in the HBP vs. LBBP group. An acute rise in threshold was observed in 8 HBP cases (14.5%), and 4 (8%) developed exit block after AVNA. Chronic HBP threshold ≥2.5 V was seen in 23 patients (48%), and 4 (8%) of HBP leads were deactivated. Both forms of CSP preserved LVEF post-AVNA in patients with a baseline LVEF > 50%, and significantly improved function in those with a baseline LVEF <50%. The authors concluded that whilst CSP with either HBP or LBBP would preserve or restore LV systolic function post-AVNA, fewer acute procedural complications during AVNA and fewer long-term lead-related performance issues were observed in the LBBP group.
In terms of future directions, there have been both case reports (45) and series (46) demonstrating the feasibility of simultaneous CSP and AVNA. Vijayaraman et al. (46) reported procedural results of a cohort receiving HBP at the same time as AVNA. In 22 of 25 patients, AVNA was feasible via axillary access, with femoral access only required in 3 patients early in the centre's experience. The authors suggest that this combined procedure was not only safe and effective, but may reduce procedural duration and allow for early ambulation.
Taken together, the early evidence suggests that CSP may be a viable alternative to conventional BiV pacing post-AVNA for AF. The technical issues presented by the proximity of ablation site to HBP leads, and long-term issues with HBP lead performance mean that LBBP may be more beneficial moving forwards in this field. More robust data from randomised trials comparing LBBP with BiV pacing post-AVNA will be important in this regard.
Determining the efficacy of CSP in patients with AF is a crucial area to evaluate, given the increasingly widespread use of CSP, and the high burden of AF in the eligible populations.
A review of in-silico and mechanistic in-vivo evidence would suggest that HBP may provide improved electrical synchrony compared to conventional epicardial BiV pacing. However, with HBP potentially limited by technical difficulties at implantation and long-term lead performance issues, examining how LBBP improves dyssynchrony is perhaps more relevant. The current data does suggest that the presence of intact SR, and thus the ability to adjust paced AVDs to achieve fusion pacing with intrinsic RV conduction, does improve LBBP acute electrical outcomes. The concept of fusion pacing and AVD adjustment is not a novel concept, and has in fact been the subject of interest in conventional CRT (47). However, despite studies suggesting that the primary benefit in CRT and CSP may be related to AVD shortening (48), this theory has not been borne out in larger trials of AVD optimisation in CRT (49), perhaps due to the complex relationship between the AVD and cardiac output, with acute ventricular resynchronisation being only a part of the whole story. With regards to LBBP, it is yet to be determined whether AVD optimisation leads to improved long-term outcomes. Randomised trials comparing LBBP in SR and AF populations may address this, but given the modest improvements observed in acute electrical outcomes, prohibitively large sample sizes may be required to detect small differences in hard clinical endpoints. Of note, clinical effect sizes may be further diluted by a proportion of patients who exhibit anodal septal capture (26, 50). Such patients may not gain electrical benefit from AVD optimisation, as preservation of intrinsic RBB conduction would theoretically not be necessary in such instances. Another potential avenue of interest is whether therapies such as His-Optimised CRT (HOT-CRT) or Left Bundle Branch Optimised CRT (LOT-CRT) will be beneficial in AF to improve fusion in the absence of AVD optimisation (51, 52). These interventions have shown some promise at improving synchronisation in small observational studies, but their specific benefits in AF patients has as yet not been examined.
Our most substantial clinical body of evidence for CSP in AF comes from the post-AVNA population. These data so far suggest that CSP may be a viable alternative to BiV pacing in this group. However, larger prospective comparative studies are needed to determine whether CSP is equivalent in these cases. Real world data, such as registry, is also very valuable in this field, especially with regards to HBP, where trials performed in high-volume centres by experienced operators may under-estimate the complication rate and with this intervention, which is more technically challenging than LBBP.
Having said this, the most impactful path forward in furthering the field, of course, lies in randomised control trials, ideally studies recruiting exclusively patients with AF comparing CSP vs. BiV pacing in both traditional CRT populations and AVNA populations. There are inherent challenges, however, that come with designing such trials. Firstly, large sample sizes will be needed to adequately power these studies, and this may present problems, especially when the eligible recruitment pool is reduced. Slow recruitment leads to longer duration studies which in turn increases costs as well as drop-out rates. Perhaps equally relevant is that AF patients tend to be under-represented in large clinical CRT trials (53). With the driving force behind the largest studies primarily involving commercial funding and/or sponsorship, industry partners may be less motivated to support trials in AF patients, where the beneficial effects of these devices is likely to be attenuated, and regulatory approvals for broad indications have already been granted on the basis of previous evidence. It is vital, therefore, that well designed investigator-initiated studies are prioritised in the future. In an era where there are a plethora of available CRT treatments, a personalised approach may be needed for individual patients based on a variety of factors, including AF. Large, randomised trials are needed to provide the strong evidence base, crucial in informing the decisions.
NW: performed literature review and manuscript preparation. The remaining authors provided internal peer-review and expertise. All authors contributed to the article and approved the submitted version.
The authors are supported by the Wellcome/EPSRC Centre for Medical Engineering (WT203148/Z/16/Z). NW receives fellowship funding from the British Heart Foundation (FS/CRTF/22/24362). VM has received fellowship funding from Abbott. SAN acknowledges support from the UK Engineering and Physical Sciences Research Council (EP/M012492/1, NS/A000049/1, and EP/P01268X/1), the British Heart Foundation (PG/15/91/31812, PG/13/37/30280, SP/18/6/33805, RG/20/4/34803), US National Institutes of Health (NIH R01-HL152256), European Research Council (ERC PREDICT-HF 864055) and Kings Health Partners London National Institute for Health Research (NIHR) Biomedical Research Centre. JMB receives research funding and/or consultation fees from Abbott, Siemens Healthcare, EBR Systems, Biosense Webster outside of the submitted work. CAR receives research funding and/or consultation fees from Abbott, Medtronic, Boston Scientific, Spectranetics and MicroPort outside of the submitted work.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Glikson M, Nielsen JC, Kronborg MB, Michowitz Y, Auricchio A, Barbash IM, et al. 2021 ESC guidelines on cardiac pacing and cardiac resynchronization therapy. Eur Heart J. (2021) 42(35):3427–520. doi: 10.1093/eurheartj/ehab364 34455430
2. McAlister FA, Ezekowitz J, Hooton N, Vandermeer B, Spooner C, Dryden DM, et al. Cardiac resynchronization therapy for patients with left ventricular systolic dysfunction. JAMA. (2007) 297(22):2502. doi: 10.1001/jama.297.22.2502
3. Curtis AB, Worley SJ, Adamson PB, Chung ES, Niazi I, Sherfesee L, et al. Biventricular pacing for atrioventricular block and systolic dysfunction. N Engl J Med. (2013) 368(17):1585–93. doi: 10.1056/NEJMoa1210356
4. Brignole M, Pentimalli F, Palmisano P, Landolina M, Quartieri F, Occhetta E, et al. AV junction ablation and cardiac resynchronization for patients with permanent atrial fibrillation and narrow QRS: the APAF-CRT mortality trial. Eur Heart J. (2021) 42(46):4731–9. doi: 10.1093/EURHEARTJ/EHAB569
5. Young JB. Combined cardiac resynchronization and implantable cardioversion defibrillation in advanced chronic heart failure. JAMA. (2003) 289(20):2685. doi: 10.1001/jama.289.20.2685
6. Wouters PC, Vernooy K, Cramer MJ, Prinzen FW, Meine M. Optimizing lead placement for pacing in dyssynchronous heart failure: the patient in the lead. Heart Rhythm. (2021) 18(6):1024–32. doi: 10.1016/J.HRTHM.2021.02.011
7. Vijayaraman P, Chung MK, Dandamudi G, Upadhyay GA, Krishnan K, Crossley G, et al. His bundle pacing. J Am Coll Cardiol. (2018) 72(8):927–47. doi: 10.1016/J.JACC.2018.06.017
8. Upadhyay GA, Vijayaraman P. How to choose between his bundle pacing and biventricular pacing for cardiac resynchronization therapy. Curr Cardiovasc Risk Rep. (2019) 13(3):1–10. doi: 10.1007/S12170-019-0598-9/FIGURES/3
9. Bhatt AG, Musat DL, Milstein N, Pimienta J, Flynn L, Sichrovsky T, et al. The efficacy of his bundle pacing: lessons learned from implementation for the first time at an experienced electrophysiology center. JACC Clin Electrophysiol. (2018) 4(11):1397–406. doi: 10.1016/J.JACEP.2018.07.013
10. Sharma PS, Vijayaraman P, Ellenbogen KA. Permanent his bundle pacing: shaping the future of physiological ventricular pacing. Nat Rev Cardiol. (2019) 17(1):22–36. doi: 10.1038/s41569-019-0224-z
11. Lustgarten DL, Sharma PS, Vijayaraman P. Troubleshooting and programming considerations for his bundle pacing. Heart Rhythm. (2019) 16(5):654–62. doi: 10.1016/J.HRTHM.2019.02.031
12. Zanon F, Abdelrahman M, Marcantoni L, Naperkowski A, Subzposh FA, Pastore G, et al. Long term performance and safety of his bundle pacing: a multicenter experience. J Cardiovasc Electrophysiol. (2019) 30(9):1594–601. doi: 10.1111/JCE.14063
13. Zhang W, Huang J, Qi Y, Wang F, Guo L, Shi X, et al. Cardiac resynchronization therapy by left bundle branch area pacing in patients with heart failure and left bundle branch block. Heart Rhythm. (2019) 16(12):1783–90. doi: 10.1016/J.HRTHM.2019.09.006
14. Huang W, Chen X, Su L, Wu S, Xia X, Vijayaraman P. A beginner’s guide to permanent left bundle branch pacing. Heart Rhythm. (2019) 16(12):1791–6. doi: 10.1016/J.HRTHM.2019.06.016
15. Padala SK, Ellenbogen KA. Left bundle branch pacing is the best approach to physiological pacing. Heart Rhythm O2. (2020) 1(1):59–67. doi: 10.1016/J.HROO.2020.03.002/ATTACHMENT/2874B128-4D77-4217-B818-E7D7D6E38D33/MMC4.MP4
16. Lippi G, Sanchis-Gomar F, Cervellin G. Global epidemiology of atrial fibrillation: an increasing epidemic and public health challenge. Int J Stroke. (2020) 16(2):217–21. doi: 10.1177/1747493019897870 31955707
17. Lyons KJ, Ezekowitz JA, Liang L, Heidenreich PA, Yancy CW, DeVore AD, et al. Impact of current versus previous cardiac resynchronization therapy guidelines on the proportion of patients with heart failure eligible for therapy. JACC Heart Fail. (2017) 5(5):388–92. doi: 10.1016/J.JCHF.2017.02.018
18. Wilton SB, Leung AA, Ghali WA, Faris P, Exner DV. Outcomes of cardiac resynchronization therapy in patients with versus those without atrial fibrillation: a systematic review and meta-analysis. Heart Rhythm. (2011) 8(7):1088–94. doi: 10.1016/J.HRTHM.2011.02.014
19. Molhoek SG, Bax JJ, Bleeker GB, Boersma E, Van Erven L, Steendijk P, et al. Comparison of response to cardiac resynchronization therapy in patients with sinus rhythm versus chronic atrial fibrillation. Am J Cardiol. (2004) 94(12):1506–9. doi: 10.1016/J.AMJCARD.2004.08.028
20. Borleffs CJW, Ypenburg C, van Bommel RJ, Delgado V, van Erven L, Schalij MJ, et al. Clinical importance of new-onset atrial fibrillation after cardiac resynchronization therapy. Heart Rhythm. (2009) 6(3):305–10. doi: 10.1016/J.HRTHM.2008.12.017
21. Fang F, Lee A, cardiology CYC. cardiology CYC opinion in, 2014 undefined. Left atrial function in heart failure with impaired and preserved ejection fraction. journals.lww.com. Published online 2014. doi: 10.1097/HCO.0000000000000091.
22. Ruwald A, Kutyifa V. MRE heart, 2015 undefined. The association between biventricular pacing and cardiac resynchronization therapy-defibrillator efficacy when compared with implantable cardioverter defibrillator on. academic.oup.com. https://academic.oup.com/eurheartj/article-abstract/36/7/440/494367 (Accessed March 9, 2023)
23. Van Rees JB, Borleffs CJW, De Bie MK, Stijnen T, Van Erven L, Bax JJ, et al. Inappropriate implantable cardioverter-defibrillator shocks: incidence, predictors, and impact on mortality. J Am Coll Cardiol. (2011) 57(5):556–62. doi: 10.1016/J.JACC.2010.06.059
24. Curila K, Jurak P, Vernooy K, Jastrzebski M, Waldauf P, Prinzen F, et al. Left ventricular myocardial septal pacing in close proximity to LBB does not prolong the duration of the left ventricular lateral wall depolarization compared to LBB pacing. Front Cardiovasc Med. (2021) 8:1829. doi: 10.3389/FCVM.2021.787414
25. Curila K, Jurak P, Jastrzebski M, Prinzen F, Waldauf P, Halamek J, et al. Left bundle branch pacing compared to left ventricular septal myocardial pacing increases interventricular dyssynchrony but accelerates left ventricular lateral wall depolarization. Heart Rhythm. (2021) 18(8):1281–9. doi: 10.1016/J.HRTHM.2021.04.025
26. Curila K, Jurak P, Prinzen F, Jastrzebski M, Waldauf P, Halamek J, et al. Bipolar anodal septal pacing with direct LBB capture preserves physiological ventricular activation better than unipolar left bundle branch pacing. Published Online January. (2023) 10. doi: 10.1101/2023.01.09.23284263
27. Strocchi M, Lee AWC, Neic A, Bouyssier J, Gillette K, Plank G, et al. His-bundle and left bundle pacing with optimized atrioventricular delay achieve superior electrical synchrony over endocardial and epicardial pacing in left bundle branch block patients. Heart Rhythm. (2020) 17(11):1922–9. doi: 10.1016/J.HRTHM.2020.06.028
28. Huang W, Wu S, Vijayaraman P, Su L, Chen X, Cai B, et al. Cardiac resynchronization therapy in patients with nonischemic cardiomyopathy using left bundle branch pacing. JACC Clin Electrophysiol. (2020) 6(7):849–58. doi: 10.1016/J.JACEP.2020.04.011
29. Wu S, Su L, Vijayaraman P, Zheng R, Cai M, Xu L, et al. Left bundle branch pacing for cardiac resynchronization therapy: nonrandomized on-treatment comparison with his bundle pacing and biventricular pacing. Can J Cardiol. (2021) 37(2):319–28. doi: 10.1016/J.CJCA.2020.04.037
30. Ali N, Arnold AD, Miyazawa AA, Keene D, Chow JJ, Little I, et al. Comparison of methods for delivering cardiac resynchronization therapy: an acute electrical and haemodynamic within-patient comparison of left bundle branch area, his bundle, and biventricular pacing. EP Eur. (2023) 25(3):1060–7. doi: 10.1093/EUROPACE/EUAC245
31. Pereira H, Jackson TA, Claridge S, Behar JM, Yao C, Sieniewicz B, et al. Comparison of echocardiographic and electrocardiographic mapping for cardiac resynchronisation therapy optimisation. Cardiol Res Pract. (2019) 2019. doi: 10.1155/2019/4351693
32. Elliott MK, Strocchi M, Sieniewicz BJ, Sidhu B, Mehta V, Wijesuriya N, et al. Biventricular endocardial pacing and left bundle branch area pacing for cardiac resynchronization: mechanistic insights from electrocardiographic imaging, acute hemodynamic response, and magnetic resonance imaging. Heart Rhythm. (2023) 20(2):207–16. doi: 10.1016/J.HRTHM.2022.10.019
33. Gasparini M, Leclercq C, Lunati M, Landolina M, Auricchio A, Santini M, et al. Cardiac resynchronization therapy in patients with atrial fibrillation: the CERTIFY study (cardiac resynchronization therapy in atrial fibrillation patients multinational registry). JACC Heart Fail. (2013) 1(6):500–7. doi: 10.1016/J.JCHF.2013.06.003
34. Stavrakis S, Garabelli P, Reynolds DW. Cardiac resynchronization therapy after atrioventricular junction ablation for symptomatic atrial fibrillation: a meta-analysis. EP Europace. (2012) 14(10):1490–7. doi: 10.1093/EUROPACE/EUS193
35. Vijayaraman P, Subzposh FA, Naperkowski A. Atrioventricular node ablation and his bundle pacing. EP Europace. (2017) 19(suppl_4):iv10–6. doi: 10.1093/EUROPACE/EUX263
36. Su L, Cai M, Wu S, Wang S, Xu T, Vijayaraman P, et al. Long-term performance and risk factors analysis after permanent his-bundle pacing and atrioventricular node ablation in patients with atrial fibrillation and heart failure. EP Europace. (2020) 22(Supplement_2):ii19–26. doi: 10.1093/EUROPACE/EUAA306
37. Moriña-Vázquez P, Moraleda-Salas MT, Arce-León Á, Venegas-Gamero J, Fernández-Gómez JM, Díaz-Fernández JF. Effectiveness and safety of AV node ablation after his bundle pacing in patients with uncontrolled atrial arrhythmias. Pacing Clin Electrophysiol. (2021) 44(6):1004–9. doi: 10.1111/PACE.14252
38. Huang W, Su L, Wu S, Xu L, Xiao F, Zhou X, et al. Benefits of permanent his bundle pacing combined with atrioventricular node ablation in atrial fibrillation patients with heart failure with both preserved and reduced left ventricular ejection fraction. J Am Heart Assoc. (2017) 6(4). doi: 10.1161/JAHA.116.005309
39. Wang S, Wu S, Xu L, Xiao F, Whinnett ZI, Vijayaraman P, et al. Feasibility and efficacy of his bundle pacing or left bundle pacing combined with atrioventricular node ablation in patients with persistent atrial fibrillation and implantable cardioverter-defibrillator therapy. J Am Heart Assoc. (2019) 8(24). doi: 10.1161/JAHA.119.014253
40. Žižek D, Antolič B, Mežnar AZ, Zavrl-Džananović D, Jan M, Štublar J, et al. Biventricular versus his bundle pacing after atrioventricular node ablation in heart failure patients with narrow QRS. Acta Cardiologica. (2021) 77(3):222–30. doi: 10.1080/00015385.2021.1903196
41. Huang W, Wang S, Su L, Fu G, Su Y, Chen K, et al. His-bundle pacing vs biventricular pacing following atrioventricular nodal ablation in patients with atrial fibrillation and reduced ejection fraction: a multicenter, randomized, crossover study—the ALTERNATIVE-AF trial. Heart Rhythm. (2022) 19(12):1948–55. doi: 10.1016/J.HRTHM.2022.07.009
42. Vijayaraman P, Mathew AJ, Naperkowski A, Young W, Pokharel P, Batul SA, et al. Conduction system pacing versus conventional pacing in patients undergoing atrioventricular node ablation: nonrandomized, on-treatment comparison. Heart Rhythm O2. (2022) 3(4):368–76. doi: 10.1016/J.HROO.2022.04.005
43. Cai M, Wu S, Wang S, Zheng R, Jiang L, Lian L, et al. Left bundle branch pacing postatrioventricular junction ablation for atrial fibrillation: propensity score matching with his bundle pacing. Circ Arrhythm Electrophysiol. (2022) 15(10):656–67. doi: 10.1161/CIRCEP.122.010926
44. Pillai A, Kolominsky J, Koneru JN, Kron J, Shepard RK, Kalahasty G, et al. Atrioventricular junction ablation in patients with conduction system pacing leads: a comparison of his-bundle vs left bundle branch area pacing leads. Heart Rhythm. (2022) 19(7):1116–23. doi: 10.1016/J.HRTHM.2022.03.1222
45. Ringwala S, Knight BP, Verma N. Permanent his bundle pacing at the time of atrioventricular node ablation: a 3-dimensional mapping approach. HeartRhythm Case Rep. (2017) 3(6):323–5. doi: 10.1016/J.HRCR.2017.04.005
46. Vijayaraman P, Hashimova N, Mathew AJ, Subzposh FA, Naperkowski A. Simultaneous conduction system pacing and atrioventricular node ablation via axillary vs femoral access. Heart Rhythm. (2022) 19(6):1019–21. doi: 10.1016/J.HRTHM.2022.02.014
47. Waddingham PH, Lambiase P, Muthumala A, Rowland E, Chow AWC. Fusion pacing with biventricular, left ventricular-only and multipoint pacing in cardiac resynchronisation therapy: latest evidence and strategies for use. Arrhythm Electrophysiol Rev. (2021) 10(2):91. doi: 10.15420/AER.2020.49
48. Arnold AD, Shun-Shin MJ, Ali N, Keene D, Howard JP, Francis DP, et al. Contributions of atrioventricular delay shortening and ventricular resynchronization to hemodynamic benefits of biventricular pacing. Clin Electrophysiol. (2023) 9(1):117–9. doi: 10.1016/J.JACEP.2022.07.024
49. Ellenbogen KA, Gold MR, Meyer TE, Fernández Lozano I, Mittal S, Waggoner AD, et al. Primary results from the SmartDelay determined AV optimization: a comparison to other AV delay methods used in cardiac resynchronization therapy (SMART-AV) trial. Circulation. (2010) 122(25):2660–8. doi: 10.1161/CIRCULATIONAHA.110.992552
50. Vijayaraman P, Huang W. Atrioventricular block at the distal his bundle: electrophysiological insights from left bundle branch pacing. HeartRhythm Case Rep. (2019) 5(4):233–6. doi: 10.1016/J.HRCR.2019.01.006
51. Vijayaraman P, Herweg B, Ellenbogen KA, Gajek J. His-optimized cardiac resynchronization therapy to maximize electrical resynchronization: a feasibility study. Circ Arrhythm Electrophysiol. (2019) 12(2). doi: 10.1161/CIRCEP.118.006934
52. Jastrzębski M, Moskal P, Huybrechts W, Curila K, Sreekumar P, Rademakers LM, et al. Left bundle branch–optimized cardiac resynchronization therapy (LOT-CRT): results from an international LBBAP collaborative study group. Heart Rhythm. (2022) 19(1):13–21. doi: 10.1016/J.HRTHM.2021.07.057
Keywords: left bundle area pacing, his bundle pacing, atrial fibrillation, cardiac resynchonization therapy, heart failiure, AV nodal ablation
Citation: Wijesuriya N, Mehta V, De Vere F, Strocchi M, Behar JM, Niederer SA and Rinaldi CA (2023) The role of conduction system pacing in patients with atrial fibrillation. Front. Cardiovasc. Med. 10:1187754. doi: 10.3389/fcvm.2023.1187754
Received: 16 March 2023; Accepted: 24 April 2023;
Published: 25 May 2023.
Edited by:
Justin Luermans, Maastricht University Medical Centre, NetherlandsReviewed by:
Karol Curila, Charles University, Czechia© 2023 Wijesuriya, Mehta, De Vere, Strocchi, Behar, Niederer and Rinaldi. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Nadeev Wijesuriya bmFkZWV2LndpamVzdXJpeWFAa2NsLmFjLnVr
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.