
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Cardiovasc. Med. , 23 May 2023
Sec. Cardiovascular Epidemiology and Prevention
Volume 10 - 2023 | https://doi.org/10.3389/fcvm.2023.1172828
 Alison N. Bonner1Shantal Jayawickreme1
Alison N. Bonner1Shantal Jayawickreme1 Angela M. Malek2Catherine J. Vladutiu3Clare Oliver-Williams4,5
Angela M. Malek2Catherine J. Vladutiu3Clare Oliver-Williams4,5 Yamnia I. Cortés6
Yamnia I. Cortés6 Hirofumi Tanaka7
Hirofumi Tanaka7 Michelle L. Meyer8*
Michelle L. Meyer8*
Introduction: Although studies have demonstrated a J-shaped association between parity and cardiovascular disease (CVD), the association with arterial stiffness is not fully understood.
Methods: We examined the association between parity and carotid-femoral pulse wave velocity (cfPWV), a measure of central arterial stiffness. We conducted a longitudinal analysis of 1220 women (mean age 73.7 years) who attended the Atherosclerosis Risk in Communities Study visit 5 (2011-2013). At visit 2 (1990-1992), women self-reported parity (number of prior live births), which we categorized as: 0 (never pregnant or pregnant with no live births); 1-2 (referent); 3-4; and 5+ live births. Technicians measured cfPWV at visit 5 (2011-2013) and visit 6 or 7 (2016-2019). Multivariable linear regression modeled the associations of parity with visit 5 cfPWV and cfPWV change between visit 5 and 6/7 adjusted for demographics and potential confounding factors.
Results: Participants reported 0 (7.7%), 1-2 (38.7%), 3-4 (40.0%), or 5+ (13.6%) prior live births. In adjusted analyses, women with 5+ live births had a higher visit 5 cfPWV (β=50.6 cm/s, 95% confidence interval: 3.6, 97.7 cm/s) than those with 1-2 live births. No statistically significant associations were observed for other parity groups with visit 5 cfPWV or with cfPWV change.
Discussion: In later life, women with 5+ live births had higher arterial stiffness than those with 1-2 live births, but cfPWV change did not differ by parity, suggesting women with 5+ live births should be targeted for early primary prevention of CVD given their higher arterial stiffness at later-life.
Cardiovascular disease (CVD) is the leading cause of death for women in the United States (U.S.), resulting in one third of all female deaths—approximately 400,000 deaths per year (1). While more than 26 million adults in the U.S. have diagnosed CVD (2), the level of undiagnosed CVD is significant, with 20% of myocardial infarctions going undetected at the time of occurrence (3). Notably, women are less likely than men to receive preventive guidance and treatments, such as statins, aspirin, and therapeutic lifestyle changes, which may lead to increased prevalence of subclinical CVD in women (1). In addition to traditional risk factors, certain CVD risk factors are unique to women, including pregnancy-related factors (4–8). Studies have shown that pregnancy-related factors, such as parity (defined as the number of prior live births) (6, 9), are associated with later-life CVD, as measured by the incidence of CVD and CVD events. Previous analyses have observed a J-shaped association between parity and incident CVD, with the lowest CVD risk among women who had 2 live births (6, 10). A recent analysis in the Atherosclerosis Risk in Communities (ARIC) Study, a population-based cohort examining the etiology of atherosclerosis, found that women with 5+ live births had a greater risk of CVD over a 30-year follow-up even after adjusting for socioeconomic factors and pregnancy complications (10). Since 2011, the American Heart Association's CVD prevention guidelines include an assessment of obstetric history when evaluating a woman's cardiovascular risk, emphasizing the role of pregnancy and pregnancy-related events in morbidity and mortality from CVD, and highlighting the importance of targeting younger women for primary prevention (5).
While associations between parity and later-life CVD events have been well established, data linking parity to subclinical vascular disease are limited. Arterial stiffness, a measure of structural and functional changes in the arterial walls can be used to assess preclinical stages of vascular disease and is a strong predictor of CVD events and mortality (11). Arterial stiffness is most commonly expressed by pulse wave velocity (PWV), which measures the transit time of the forward pulse wave between two arterial sites, such as carotid-femoral PWV (cfPWV) and brachial-ankle PWV (baPWV). Given its association with increased CVD risk, arterial stiffness is an active area of research for CVD risk stratification (6). Yet, the association between parity and arterial stiffness is not fully understood. Only one study to date has examined the relationship between parity and PWV, in which it was shown that higher parity was associated with higher baPWV, but not after adjusting for potential confounding factors (12). Thus, further studies are needed to characterize the association between parity and arterial stiffness. Understanding the mechanism by which childbearing increases CVD could help to direct preventive efforts in women earlier in life based on their obstetric history, with the goal of reducing CVD incidence in women.
Therefore, we aimed to evaluate the association between parity and central arterial stiffness in a population of older-aged women from diverse backgrounds across the U.S. We hypothesized that women who were never pregnant or pregnant with no live births and women with 5+ live births would have higher cfPWV and greater cfPWV change over time compared to women with 1–2 live births.
The ARIC study is a population-based, longitudinal study of 15,792 participants aged 45–64 years at the time of their enrollment in 1987–1989 from the following four U.S. communities: Forsyth County, North Carolina; Jackson, Mississippi; Minneapolis, Minnesota; and Washington County, Maryland. Details of the baseline visit have been previously described (13). This analysis includes 2,686 participants with cfPWV measured at visit 5 (2011–2013) and either visit 6 (2016–2017) or visit 7 (2018–2019). Due to PWV measurement quality concerns, we excluded participants with body mass index (BMI) >40 kg/m2 at either visit (n = 65) or missing BMI (n = 1), major arrhythmias (Minnesota code 8-1-3, 8-3-1, and 8-3-2; n = 47), Minnesota code 8-1-2 with low quality PWV waveforms (n = 12), self-reported aortic revascularization (n = 20), echocardiographic evidence of aortic stenosis or moderate or greater aortic regurgitation (n = 15), and missing covariates of interest (n = 11) (14). Due to small sample sizes, the following participants were excluded from all analyses: persons who self-identified as Asian or American Indian from any site (n = 9), African American from the Minnesota and Maryland sites (n = 8), and African American from the North Carolina site (n = 11). For this analysis, we further excluded men (n = 1,091), participants missing cfPWV values at both visit 5 and visit 6 or 7 (n = 165), and those missing parity information (n = 11). The final analytic sample included 1,220 women after exclusions. Participants provided written informed consent and ARIC was approved by the Institutional Review Boards at all field centers and other study agencies.
Before the study visit, participants were asked to not consume food or drinks, and to refrain from tobacco use and vigorous physical activity after midnight prior to the clinic visit or for 8 h prior to the visit. At visit 1, participants completed interviewer-administered questionnaires to assess demographic information, including age, race, and education level. Race and study center were defined as a combined variable for the analysis. At visit 5, participants completed another questionnaire to determine cigarette smoking status (current, former, never). Anthropometric and cardiometabolic measures, including BMI, waist circumference, blood pressure, mean arterial pressure, and heart rate were measured prior to PWV measurements. Blood samples were obtained following a standardized venipuncture protocol and shipped to ARIC central laboratories where assays for total cholesterol, high-density lipoprotein (HDL) cholesterol, triglycerides, and fasting glucose concentrations were performed. Low-density lipoprotein (LDL) cholesterol was calculated using the Friedewald equation (15). Glycated hemoglobin (HbA1c) was measured in EDTA whole blood on the Tosoh high-performance liquid chromatography Glycohemoglobin Analyzer (Tosoh Medics, Inc., San Francisco, CA) calibrated with standard values derived by the National Glycohemoglobin Standardization Program.
Body weight, measured to the nearest 0.1 kilogram, and height recorded to the nearest centimeter, were used to calculate BMI (weight/height2). Three seated blood pressure measurements were obtained after a five-minute rest using an oscillometric automated sphygmomanometer (Omron HEM-907 XL, Omron Co. Ltd., Kyoto, Japan) and the average of the last two measurements was used. Hypertension was defined as systolic blood pressure (SBP) ≥ 140 mmHg, diastolic blood pressure (DBP) ≥ 90 mmHg (16), or anti-hypertensive medication use. Diabetes mellitus was defined as fasting glucose ≥126 mg/dl, non-fasting glucose ≥200 mg/dl, anti-diabetic medication use, or self-reported physician diagnosis of diabetes mellitus.
At the baseline ARIC study visit, study staff administered a questionnaire asking women to report the total number of prior live births (parity). At visit 3, women were asked about age at menarche and whether they had ever been pregnant (gravidity). Using these data, we categorized women into four groups: 0 live births (never pregnant or pregnant with no live births), 1–2 live births, 3–4 live births, and 5+ live births.
At visits 5, 6, and 7, technicians measured cfPWV using the same standardized protocol. Details of the PWV methodology for the ARIC study have been reported (14). Briefly, technicians measured PWV using the automated waveform analyzer VP-1000 Plus (Omron Co., Ltd., Kyoto, Japan) (17) after participants were supine for 5–10 min. Carotid and femoral arterial pressure waveforms were acquired by applanation tonometry sensors on the left common carotid artery and left common femoral artery. PWV was calculated as distance divided by transit time. Distance for cfPWV was measured with a segmometer (Rosscraft, Surray, Canada) and calculated as the carotid to femoral distance minus the distance between the suprasternal notch to carotid. Technicians obtained at least two measurements and results were averaged (18). Repeat visits were conducted for a subset of participants at each field center approximately 4–8 weeks after visit 5 only (n = 79; mean age 75.7 years; 46 females). At visit 5, the intra-class correlation coefficient and 95% confidence interval (95% CI) for single cfPWV measurements were 0.70 (0.59, 0.81).
Participants missing information on PWV or any covariates were excluded from analysis.
Author MLM had full access to all the data in the study and takes responsibility for its integrity and the data analysis. Participant characteristics were compared by parity categories (0 live births, 1–2 live births, 3–4 live births, or 5+ live births). Categorical variables were presented as number and percentage, while continuous variables were presented as mean and standard deviation.
We winsorized cfPWV values that were beyond the 1% and 99% of the distribution for cfPWV at visit 5 (n = 23) and visit 6 or 7 (n = 21). Change in cfPWV was calculated as cfPWV at visit 6 or 7 minus cfPWV at visit 5, and these values were also winsorized (n = 20). We used analysis of covariance (ANCOVA) to estimate the adjusted means of cfPWV in each group. Multivariable linear regression modeled the associations of parity with cfPWV at visit 5 and change in cfPWV from visit 5 to 6/7. For the regression analyses, we adjusted for variables that were associated with both change in cfPWV and parity and variables known in the literature to be associated with both cfPWV and parity. Covariates included age, race-center (race by study center), education, and cardiometabolic factors measured at visit 5, including BMI, heart rate, mean arterial pressure (MAP), hypertension medication use, and diabetes mellitus. For cfPWV change, we additionally adjusted for years between visit 5 (2011–2013) and visit 6 (2016–2017) or visit 7 (2018–2019), with a mean time of 5.7 years. For the regression analyses, we estimated the association between parity and cfPWV and change in cfPWV in 3 models: model 1 adjusted for years between visit 5 and 6 or 7, model 2 additionally adjusted for age, race-center, and education, and model 3 additionally adjusted for BMI, heart rate, MAP, hypertension medication use, and diabetes mellitus.
Multivariable logistic regression was also used to evaluate associations of parity with higher cfPWV at visit 5 and elevated cfPWV change, both defined as >75th percentile of the distribution. Covariates and adjusted models were the same as those used in the regression analyses of continuous outcomes. P-values were two-sided with statistical significance of P < 0.05 (SAS, version 9.2, SAS Institute, Inc., Cary, NC).
Women were on average 73.7 years of age at visit 5, and 22% identified as African American. Participants reported having 0 live births (7.7%), 1–2 (38.7%), 3–4 (40.0%), or 5+ (13.6%) live births (Table 1). On average, women with 5+ live births were more likely than women in the other groups to be African American, have less than a high school education, a higher BMI, and a higher prevalence of diabetes and hypertension. They were also more likely to be younger at the birth of their first child.
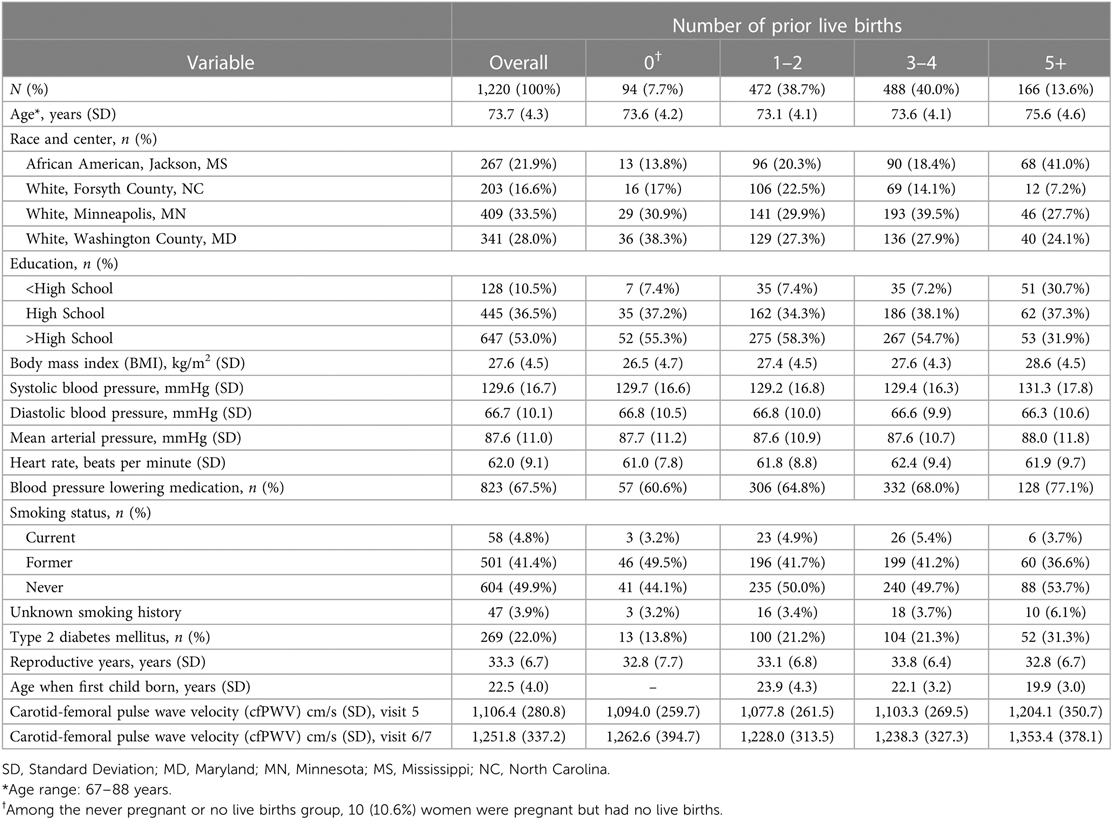
Table 1. Participant characteristics by parity categories at ARIC visit 5 (n = 1,220).
The age-adjusted mean of cfPWV at visit 5 compared by parity groups demonstrates a J-shaped curve with the lowest measurements in women with 1–2 live births (Figure 1), although the 95% CIs overlapped. Women with 5+ live births had higher cfPWV measurements when compared with women with 1–2 live births in the unadjusted model as well as the fully adjusted model (Model 3: β = 50.6, 95% CI: 3.6, 97.7) (Table 2). No other parity groups in any of the models demonstrated a statistically significant difference in cfPWV when compared to women with 1–2 live births.
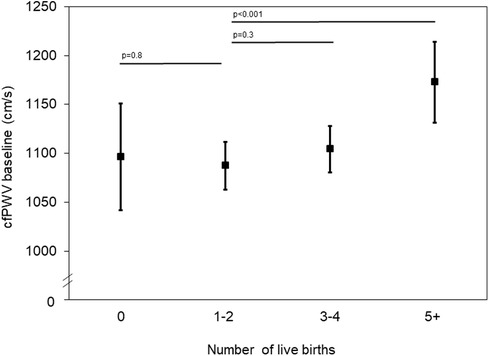
Figure 1. Carotid-femoral pulse wave velocity (cfPWV) measurements at visit 5 by parity group, adjusted for age.
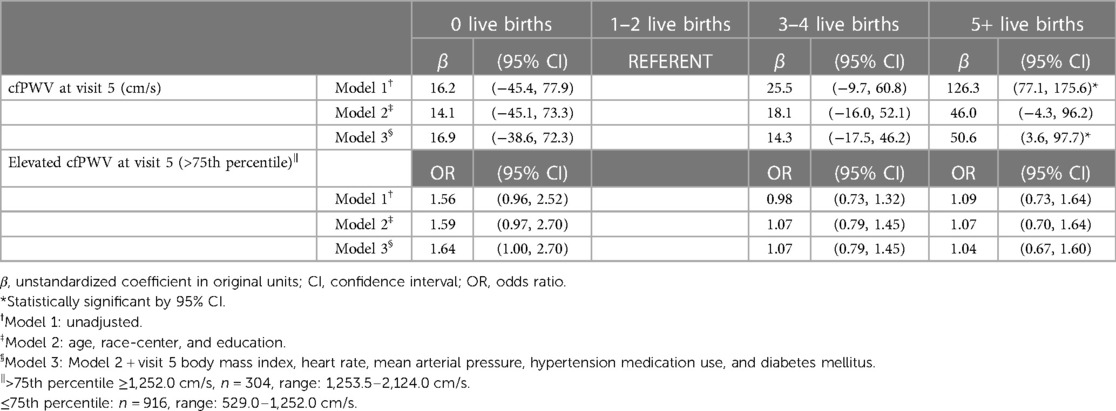
Table 2. Association of parity and carotid-femoral pulse wave velocity (cfPWV) at ARIC visit 5 (n = 1,220).
Compared to the referent group of women with 1–2 live births, the adjusted mean cfPWV change from visit 5 to 6/7 was lowest in women with 3–4 live births and higher in women with 0 live births and in women with 5+ live births, but these differences were not statistically significant as indicated by the 95% CI (means adjusted for age and years between visit 5 and 6 or 7; Figure 2). The average cfPWV change ranged from 135.5 cm/s in women with 3–4 live births to 163.9 cm/s in women with 0 live births. In multivariable regression analyses, cfPWV change from visit 5 to visit 6/7 (average follow-up time 5.7 years) compared to women with 1–2 live births was not significantly different in any of the other parity groups (Table 3).
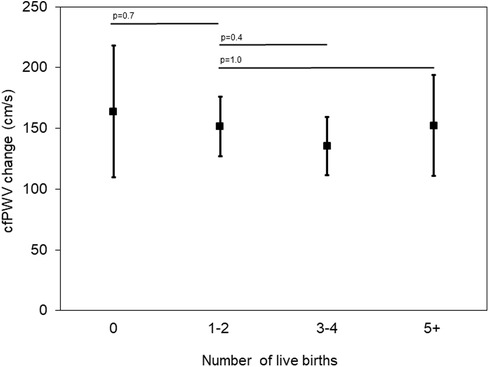
Figure 2. Carotid-femoral pulse wave velocity (cfPWV) change from visit 5 to visit 6/7 by parity group, adjusted for age and years between visit 5 and visits 6 or 7.
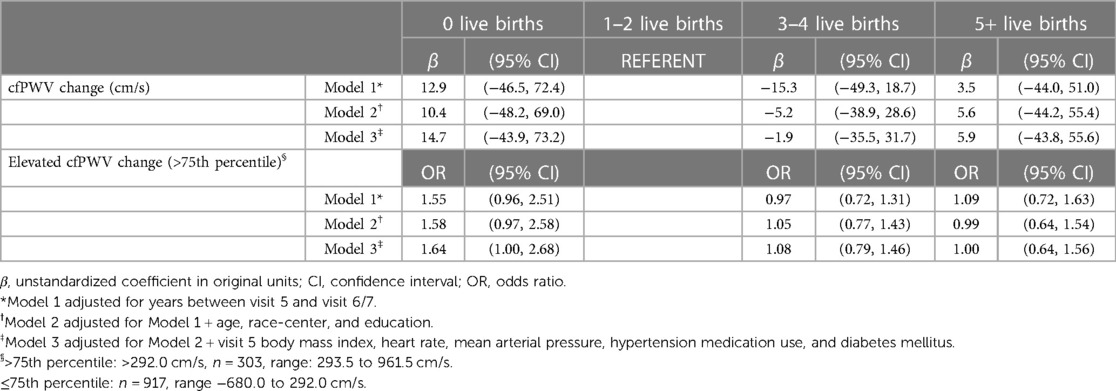
Table 3. Association of parity and carotid-femoral pulse wave velocity (cfPWV) change from ARIC visit 5 to visit 6/7 (n = 1,220).
Similar to the analysis of cfPWV as a continuous measurement, we did not observe a significant association between parity and higher categorical cfPWV (>75th percentile). However, those with 0 live births had higher odds of elevated cfPWV [odds ratio (OR) = 1.64, 95% CI: 1.00, 2.70], but this association was not statistically significant. Analysis of categorical change in cfPWV was also consistent with the continuous results, showing women with 0 live births were more likely to have elevated progression of cfPWV (>75th percentile) after adjusting for years between visit 5 and 6 or 7, age, race-center, education, heart rate, MAP, BMI, hypertension medication use, and diabetes mellitus (OR = 1.64, 95% CI: 1.00, 2.68), although this association was not statistically significant.
Using data from the ARIC study, which includes a population of older-aged women with diverse backgrounds from four communities in the U.S., we found that women with 5+ live births had higher measures of cfPWV at ARIC visit 5, with average cfPWV measures 50.6 cm/s higher than the referent group of women with 1–2 live births. The average cfPWV change ranged from 135.5 cm/s in women with 3–4 live births to 163.9 cm/s in women with no live births, though the difference between parity groups was not statistically significant.
Currently, only one other study has specifically examined the relationship between parity and PWV. Using data from the Study of Women's Health Across the Nation (SWAN), this prior study also found that higher parity (3+ live births) was associated with higher baPWV, though the association was not significant after adjusting for potential confounding factors, including demographic and cardiometabolic factors similar to those used in our study (12). However, baPWV measures both central and peripheral arterial stiffness, whereas our study uses cfPWV, a specific measure of central arterial stiffness (19). Additionally, the current study focused on older participants (73.7 years vs. 60.2 years), and has a larger sample size (1,220 vs. 964) than SWAN, which provided enough data to assess parity groups of 3–4 and 5+ live births (12).
Cross-sectional studies have shown that every 1 m/s elevation in cfPWV is associated with a 14% increased risk of a cardiovascular event (includes both cardiovascular deaths and nonfatal events) and a 15% increased risk of mortality by both cardiac and non-cardiac causes (11). Thus the increased cfPWV observed in the 5+ live births group in our study is consistent with previous studies showing an increased CVD risk in women with higher parity, including the Framingham Heart Study (6+ live births), the National Health and Nutrition Examination Survey I, Epidemiologic Follow-up Study (6+ live births), and the SWAN study (3+ live births) (6, 9, 10, 12, 20). Compared to the referent group, visit 5 cfPWV was statistically different only among women with 5+ live births. However; cfPWV was a slightly higher among women with no live births compared to the referent group, consistent with the association between parity and CVD demonstrated in prior studies, though there was a wide confidence interval in the current study (6, 9, 10).
Higher parity is also associated with a number of cardiometabolic factors that could cause increased arterial stiffness later in life, including increased body weight (21), increased waist circumference (21), elevated blood pressure (22), and insulin resistance (22). These associations are consistent with those observed in the ARIC study cohort, where we found women with 5+ live births had higher BMI, waist circumference, and prevalence of hypertension and diabetes mellitus, than women in the other parity groups. Thus, we included these factors as potential confounders in the analysis. Social factors, including race, socioeconomic status, and other unmeasured factors, are associated with differences in CVD risk and could also affect our results (23, 24). We adjusted for these social factors in the regression analyses (using education level as a representation of socioeconomic status 25), and despite the adjustments, women with 5+ live births had a higher cfPWV at visit 5.
In this study, parity was associated with cfPWV at visit 5, but not with cfPWV change. Previous studies have shown that arterial stiffening can be detected even in early childhood, with cfPWV progressing on average 0.2–0.7 m/s every 5 years (26). In older adults, this progression is more rapid, with cfPWV increasing on average by 0.8 m/s per year in those aged over 65 years, and by 0.99 m/s per year in those aged over 70 years (26). No other studies were found that looked at parity and progression of PWV over time. The lack of an association between parity and cfPWV change indicates that the vascular changes associated with pregnancy affect cfPWV earlier in life, but not how arterial stiffness progresses over time in later-life.
The progression of arterial stiffness during pregnancy has been evaluated and has shown that arterial stiffness changes to accommodate the presence and growth of the fetus, with PWV increasing in early pregnancy, decreasing in the second trimester, and returning to the woman's pre-pregnancy baseline in the postpartum period (27). This change is no longer significant when adjusted for MAP, indicating that the change in arterial stiffness is likely a response to the change in blood pressure observed during pregnancy. However, in women with more births, it may be less likely that these vascular alterations will completely return to their pre-pregnancy state, which could result in the differences we observed in later-life PWV. Since PWV in this study was measured much later than pregnancy-related vascular changes, it is possible that age-related progression of arterial stiffness and the prevalence of other vascular risk factors outweighs the effect of parity on cfPWV change. Additionally, because the cfPWV measurements were collected when the participants were 67–88 years of age, it is possible that parity has a more significant impact on arterial stiffness and progression of arterial stiffness earlier in the participants' lives than in later life. Obstetrician-Gynecologists could integrate CVD screening into postnatal care for primary prevention among women with higher parity. In mid-life, women with higher parity should be monitored for CVD risk, consistent with the American Heart Association's CVD prevention guidelines for including obstetric history when evaluating a woman's cardiovascular risk (5). Future work assessing the progression of arterial stiffness earlier in women's lives, particularly during the reproductive lifespan, could help to clarify if other factors in later life outweigh parity's effect on the progression of arterial stiffness or if there is no effect.
The categorical analysis of cfPWV change in this study, defined as cfPWV change >75th percentile, shows that women who were never pregnant or had no live births have a higher likelihood of elevated progression of cfPWV compared to women with 1–2 live births. This finding may be influenced by the effect of miscarriage, stillbirth, or therapeutic abortion on arterial stiffness or conditions that predispose women to pregnancy loss, such as with polycystic ovarian syndrome (PCOS), which is also associated with a higher risk of CVD (28). However, the small number of participants who were previously pregnant and had no live births limits the assessment of pregnancy loss in this analysis.
This study has a few limitations. Information on pregnancy outcomes and complications were not available, which can be more common in certain parity groups (29) and could affect arterial stiffness in these groups to varying degrees, as it is currently unclear what the causative relationship is between arterial stiffness and pregnancy outcomes and complications. Several demographic factors being assessed were self-reported many years after their occurrence and may be affected by recall bias, though recall of reproductive factors (age at menses and age at menopause) are moderately to highly accurate, even years later (30, 31). Additionally, arterial stiffness was only measured in older adulthood, thus we are unable to account for arterial stiffness levels before pregnancy. Lastly, there is the potential for survival bias due to attrition over the course of >25 years of follow-up. The surviving participants are likely healthier than those who did not attend the ARIC visit 5, which may attenuate the observed associations. Our internal validity of the results is supported by our multivariable statistical adjustment for participant characteristics related to attrition. However, it should be noted that this analysis was limited to White and African American participants with African American participants coming from a single study site, so these results may not be generalizable to other racial or ethnic groups or to African Americans in other geographic locations. We were unable to adjust for other social factors, such as lower socioeconomic status, neighborhood disadvantage, and healthcare access, though these factors are strongly related to higher parity and likely coincide with field center and education level, which were adjusted for in this study.
In conclusion, reproductive factors have an important role in evaluating women's cardiovascular risk, but the association of parity with subclinical CVD has not been fully determined. Demonstrating the association between parity and arterial stiffness helps to address this gap in knowledge. It highlights a potential target for primary prevention strategies in women with 5 or more prior live births who do not have clinical CVD. The mechanism by which pregnancy or parity increases arterial stiffness is unclear and requires more longitudinal research among women of younger ages.
The datasets presented in this study can be found in online repositories. The names of the repository/repositories and accession number(s) can be found below: The data underlying the results presented in the study are publicly available from NHLBI Biologic Specimen and Data Repository (https://biolincc.nhlbi.nih.gov/studies/aric/).
Ethical review and approval was not required for the study on human participants in accordance with the local legislation and institutional requirements. Participants provided written informed consent and ARIC was approved by the Institutional Review Boards at all field centers and other study agencies.
AB, SJ, MM, AM, CV, CO-W, YC, and HT contributed to the conception and design of the project. AB and MM contributed to the analysis of data. AB, SJ, MM, AM, CV, CO-W, YC, and HT contributed to the critical interpretation of the results. AB and MM contributed to the first draft of the manuscript. AB, SJ, MM, AM, CV, CO-W, YC, and HT contributed to the critical revision of the manuscript for its intellectual content and approved the final version of the manuscript. All authors contributed to the article and approved the submitted version.
The Atherosclerosis Risk in Communities study has been funded in whole or in part with Federal funds from the National Heart, Lung, and Blood Institute, National Institutes of Health, Department of Health and Human Services, under Contract nos. (HHSN268201700001I, HHSN268201700002I, HHSN268201700003I, HHSN268201700005I, HHSN268201700004I). Arterial stiffness was funded by R01AG053938. AB and SJ were supported by grant number T35-HL134624 from the National Heart, Lung, and Blood Institute. MM was supported by R01AG062488 and R01AG061088 from the National Institute on Aging. The funders had no role in study design, data collection and analysis, decision to publish, or preparation of the manuscript.
The authors thank the staff and participants of the ARIC study for their important contributions.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Garcia M, Mulvagh SL, Merz CNB, Buring JE, Manson JE. Cardiovascular disease in women: clinical perspectives. Circ Res. (2016) 118(8):1273–93. doi: 10.1161/CIRCRESAHA.116.307547
2. Virani SS, Alonso A, Aparicio HJ, Benjamin EJ, Bittencourt MS, Callaway CW, et al. Heart disease and stroke statistics-2021 update: a report from the American heart association. Circulation. (2021) 143(8):e254–743. doi: 10.1161/CIR.0000000000000950
3. Laslett LJ, Alagona P, Clark BA, Drozda JP, Saldivar F, Wilson SR, et al. The worldwide environment of cardiovascular disease: prevalence, diagnosis, therapy, and policy issues: a report from the American college of cardiology. J Am Coll Cardiol. (2012) 60(25 Suppl):S1–49. doi: 10.1016/j.jacc.2012.11.002
4. Grandi SM, Filion KB, Yoon S, Ayele HT, Doyle CM, Hutcheon JA, et al. Cardiovascular disease-related morbidity and mortality in women with a history of pregnancy complications. Circulation. (2019) 139(8):1069–79. doi: 10.1161/CIRCULATIONAHA.118.036748
5. Mosca L, Benjamin EJ, Berra K, Bezanson JL, Dolor RJ, Lloyd-Jones DM, et al. Effectiveness-based guidelines for the prevention of cardiovascular disease in women–2011 update: a guideline from the American heart association. J Am Coll Cardiol. (2011) 57(12):1404–23. doi: 10.1016/j.jacc.2011.02.005
6. Parikh NI, Cnattingius S, Dickman PW, Mittleman MA, Ludvigsson JF, Ingelsson E. Parity and risk of later-life maternal cardiovascular disease. Am Heart J. (2010) 159(2):215–21.e6. doi: 10.1016/j.ahj.2009.11.017
7. Bellamy L, Casas J-P, Hingorani AD, Williams D. Type 2 diabetes mellitus after gestational diabetes: a systematic review and meta-analysis. Lancet. (2009) 373(9677):1773–9. doi: 10.1016/S0140-6736(09)60731-5
8. Tooher J, Thornton C, Makris A, Ogle R, Korda A, Hennessy A. All hypertensive disorders of pregnancy increase the risk of future cardiovascular disease. Hypertension. (2017) 70(4):798–803. doi: 10.1161/HYPERTENSIONAHA.117.09246
9. Li W, Ruan W, Lu Z, Wang D. Parity and risk of maternal cardiovascular disease: a dose-response meta-analysis of cohort studies. Eur J Prev Cardiol. (2019) 26(6):592–602. doi: 10.1177/2047487318818265
10. Oliver-Williams C, Vladutiu CJ, Loehr LR, Rosamond WD, Stuebe AM. The association between parity and subsequent cardiovascular disease in women: the atherosclerosis risk in communities study. J Womens Health (Larchmt). (2019) 28(5):721–7. doi: 10.1089/jwh.2018.7161
11. Vlachopoulos C, Aznaouridis K, Stefanadis C. Prediction of cardiovascular events and all-cause mortality with arterial stiffness: a systematic review and meta-analysis. J Am Coll Cardiol. (2010) 55(13):1318–27. doi: 10.1016/j.jacc.2009.10.061
12. Cortés YI, Catov JM, Brooks M, El Khoudary SR, Thurston RC, Matthews KA, et al. Pregnancy-related events associated with subclinical cardiovascular disease burden in late midlife: SWAN. Atherosclerosis. (2019) 289:27–35. doi: 10.1016/j.atherosclerosis.2019.07.012
13. The ARIC Investigators. The atherosclerosis risk in communities (ARIC) study: design and objectives. Am J Epidemiol. (1989) 129(4):687–702. doi: 10.1093/oxfordjournals.aje.a115184
14. Meyer ML, Tanaka H, Palta P, Cheng S, Gouskova N, Aguilar D, et al. Correlates of segmental pulse wave velocity in older adults: the atherosclerosis risk in communities (ARIC) study. Am J Hypertens. (2016) 29(1):114–22. doi: 10.1093/ajh/hpv079
15. Friedewald WT, Levy RI, Fredrickson DS. Estimation of the concentration of low-density lipoprotein cholesterol in plasma, without use of the preparative ultracentrifuge. Clin Chem. (1972) 18(6):499–502. doi: 10.1093/clinchem/18.6.499
16. Unger T, Borghi C, Charchar F, Khan NA, Poulter NR, Prabhakaran D, et al. 2020 International society of hypertension global hypertension practice guidelines. Hypertension. (2020) 75(6):1334–57. doi: 10.1161/HYPERTENSIONAHA.120.15026
17. Cortez-Cooper MY, Supak JA, Tanaka H. A new device for automatic measurements of arterial stiffness and ankle-brachial index. Am J Cardiol. (2003) 91(12):1519–22; A9. doi: 10.1016/S0002-9149(03)00416-8
18. Meyer ML, Tanaka H, Palta P, Patel MD, Camplain R, Couper D, et al. Repeatability of central and peripheral pulse wave velocity measures: the atherosclerosis risk in communities (ARIC) study. Am J Hypertens. (2016) 29(4):470–5. doi: 10.1093/ajh/hpv127
19. Yu S, McEniery CM. Central versus peripheral artery stiffening and cardiovascular risk. Arterioscler Thromb Vasc Biol. (2020) 40(5):1028–33. doi: 10.1161/ATVBAHA.120.313128
20. Ness RB, Harris T, Cobb J, Flegal KM, Kelsey JL, Balanger A, et al. Number of pregnancies and the subsequent risk of cardiovascular disease. N Engl J Med. (1993) 328:1528–33. doi: 10.1056/NEJM199305273282104
21. Gunderson EP, Lewis CE, Wei GS, Whitmer RA, Quesenberry CP, Sidney S. Lactation and changes in maternal metabolic risk factors. Obstet Gynecol. (2007) 109(3):729–38. doi: 10.1097/01.AOG.0000252831.06695.03
22. Zoet GA, Paauw ND, Groenhof K, Franx A, Gansevoort RT, Groen H, et al. Association between parity and persistent weight gain at age 40–60 years: a longitudinal prospective cohort study. BMJ Open. (2019) 9(5):e024279. doi: 10.1136/bmjopen-2018-02427931061020
23. Brothers RM, Fadel PJ, Keller DM. Racial disparities in cardiovascular disease risk: mechanisms of vascular dysfunction. Am J Physiol Heart Circ Physiol. (2019) 317(4):H777–89. doi: 10.1152/ajpheart.00126.2019
24. Schultz WM, Kelli HM, Lisko JC, Varghese T, Shen J, Sandesara P, et al. Socioeconomic status and cardiovascular outcomes: challenges and interventions. Circulation. (2018) 137:2166–78. doi: 10.1161/CIRCULATIONAHA.117.029652
25. Winkleby MA, Jatulis DE, Frank E, Fortmann SP. Socioeconomic status and health: how education, income, and occupation ontribute to risk factors for cardiovascular disease. Am J Public Health. (1992) 82(6):816–20. doi: 10.2105/AJPH.82.6.816
26. Kucharska-Newton AM, Stoner L, Meyer ML. Determinants of vascular age: an epidemiological perspective. Clin Chem. (2019) 65(1):108–18. doi: 10.1373/clinchem.2018.287623
27. Mahendru AA, Everett TR, Wilkinson IB, Lees CC, McEniery CM. A longitudinal study of maternal cardiovascular function from preconception to the postpartum period. J Hypertens. (2014) 32(4):849–56. doi: 10.1097/HJH.0000000000000090
28. Zhao L, Zhu Z, Lou H, Zhu G, Huang W, Zhang S, et al. Polycystic ovary syndrome (PCOS) and the risk of coronary heart disease (CHD): a meta-analysis. Oncotarget. (2016) 7(23):33715–21. doi: 10.18632/oncotarget.9553
29. Bai J, Wong FWS, Bauman A, Mohsin M. Parity and pregnancy outcomes. Am J Obstet Gynecol. (2002) 186(2):274–8. doi: 10.1067/mob.2002.119639
30. den Tonkelaar I. Validity and reproducibility of self-reported age at menopause in women participating in the DOM-project. Maturitas. (1997) 27(2):117–23. doi: 10.1016/S0378-5122(97)01122-5
Keywords: arterial stiffness (AS), parity, womens health, ARIC atherosclerosis risk in communities study, longitudinal
Citation: Bonner AN, Jayawickreme S, Malek AM, Vladutiu CJ, Oliver-Williams C, Cortés YI, Tanaka H and Meyer ML (2023) Number of prior live births is associated with higher arterial stiffness but not its change in older women: the atherosclerosis risk in communities study. Front. Cardiovasc. Med. 10:1172828. doi: 10.3389/fcvm.2023.1172828
Received: 23 February 2023; Accepted: 27 April 2023;
Published: 23 May 2023.
Edited by:
Weihua Guan, University of Minnesota Twin Cities, United StatesReviewed by:
Abbi D. Lane-Cordova, University of South Carolina, United States© 2023 Bonner, Jayawickreme, Malek, Vladutiu, Oliver-Williams, Cortés, Tanaka and Meyer. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Michelle L. Meyer bWxtZXllckB1bmMuZWR1
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.