 Jiale Shi1,2,†
Jiale Shi1,2,† Wei Li2,3,†Tangshan Zhang4Chengwen Han2,3
Wei Li2,3,†Tangshan Zhang4Chengwen Han2,3 Zhengjun Wang5Xinhao Pei3Xuetao Li2Zidong Zhao6Pengbo Wang6Jingying Han3Shiqiao Chen7*
Zhengjun Wang5Xinhao Pei3Xuetao Li2Zidong Zhao6Pengbo Wang6Jingying Han3Shiqiao Chen7*
- 1Shandong Provincial Hospital, Shandong University, Jinan, China
- 2Department of Second Clinical Medical School, Cheeloo College of Medicine, Shandong University, Jinan, China
- 3Department of Basic Medical School, Cheeloo College of Medicine, Shandong University, Jinan, China
- 4Department of Vascular Surgery, Jiyang District People's Hospital, Jinan, China
- 5Department of Cardiovascular Surgery, Shandong Provincial Hospital Affiliated to Shandong First Medical University, Jinan, China
- 6Department of Public Health School, Cheeloo College of Medicine, Shandong University, Jinan, China
- 7Department of Interventional Diagnosis and Treatment, Shandong Provincial Hospital Affiliated to Shandong First Medical University, Jinan, China
Introduction: Transcatheter aortic valve replacement (TAVR) is the first-line treatment for patients with moderate-to-high surgical risk of severe aortic stenosis. Paravalvular leakage (PVL) is a serious complication of TAVR, and aortic valve calcification contributes to the occurrence of PVL. This study aimed to investigate the effect of location and quantity of calcification in the aortic valve complex (AVC) and left ventricular outflow tract (LVOT) on PVL after TAVR.
Method: We performed a systematic review and meta-analysis to evaluate the effect of quantity and location of aortic valve calcification on PVL after TAVR using observational studies from PubMed and EMBASE databases from inception to February 16, 2022.
Results: Twenty-four observational studies with 6,846 patients were included in the analysis. A high quantity of calcium was observed in 29.6% of the patients; they showed a higher risk of significant PVL. There was heterogeneity between studies (I2 = 15%). In the subgroup analysis, PVL after TAVR was associated with the quantity of aortic valve calcification, especially those located in the LVOT, valve leaflets, and the device landing zone. A high quantity of calcium was associated with PVL, regardless of expandable types or MDCT thresholds used. However, for valves with sealing skirt, the amount of calcium has no significant effect on the incidence of PVL.
Conclusion: Our study elucidated the effect of aortic valve calcification on PVL and showed that the quantity and location of aortic valve calcification can help predict PVL. Furthermore, our results provide a reference for the selection of MDCT thresholds before TAVR. We also showed that balloon-expandable valves may not be effective in patients with high calcification, and valves with sealing skirts instead of those without sealing skirts should be applied more to prevent PVL from happening.
Systematic Review Registration: https://www.crd.york.ac.uk/PROSPERO/display_record.php?RecordID=354630, identifier: CRD42022354630.
1. Introduction
Transcatheter aortic valve replacement (TAVR) is the first-line treatment for patients with moderate-to-high surgical risk of severe aortic stenosis (1–3). Paravalvular leakage (PVL) is a serious complication of TAVR, which leads to an increased mortality rate (4–6). Aortic valve calcification is a factor contributing to the occurrence of PVL (7, 8); however, the location and pattern of calcification vary greatly between patients. Furthermore, the effects of calcification in various locations of the aortic valve complex (AVC) and left ventricular outflow tract (LVOT) are not fully understood. We performed a systematic review and meta-analysis to investigate the effect of location and quantity of calcification in the AVC and LVOT on PVL after TAVR. The present study was registered with PROSPERO (CRD42022354630). This manuscript is written in accordance with the Preferred Reported Items for Systematic Reviews and Meta-Analysis (PRISMA) checklist.
2. Systematic review
A systematic review of published data on the quantity and location of aortic valve calcification in patients who had undergone TAVR, and on the incidence of PVL after TAVR was conducted using PubMed and EMBASE databases. The guidance and reporting items specified in the PRISMA statement were adhered to (9). The following MeSH terms were used: transcatheter aortic valve replacement and calcium. The following keywords were used: paravalvular leakage and paravalvular regurgitation.
The databases were last accessed on February 16, 2022. The citations were screened at the title and abstract level, and the full text was retrieved if the relationship between calcification and PVL at either region of the aortic valve was reported. Studies that met the following criteria were included: (i) original design; (ii) reported data on the occurrence of PVL in patients after TAVR; (iii) quantity and specific location of calcification in the aortic valve of selected patients. When two similar studies were reported by the same institution or author, the most recent publication or one with additional information was included in the analysis. Case reports or studies published in languages other than English were excluded.
A standardized data summary form was used to extract data from patients and studies. Two investigators (LW and PXH) performed the data extraction twice. When necessary, consensus was reached with the help of a third investigator (SJL) to resolve any disagreements. When the precise data for the study were not available, the corresponding author was contacted, and additional information was requested.
Using the above criteria, we extracted the following data: (1) general characteristics (i.e., name of the authors, year of study, region, inclusion period, and sample size), (2) TAVR procedure (i.e., valve and expandable type), (3) characteristics of the calcification [i.e., multidetector computed tomography (MDCT) examination threshold, area scanned, and calcium volume or score], and (4) characteristics of PVL (i.e., extent and time definition).
We analyzed the data using Review Manager version 5.3 (RevMan; Copenhagen: The Nordic Cochrane Centre, The Cochrane Collaboration, 2014) and estimated the relative risk (RR), odds ratios (OR), as well as the standardized mean differences (SMD), with 95% confidence intervals (CI) for all available categorical and continuous variables. Given the possible heterogeneity in outcome ascertainment across trials, we analyzed our data based on SMD values as they provided a more comprehensive summary statistic on the size of the intervention effect in each study relative to the variability observed in that study. Continuous variables, which were reported as medians with the first and third quartile of the sample, were converted to mean and standard deviation values according to the method described by Luo et al. (10) and Wan et al. (11). The I2 index was used to assess the consistency across studies. The choice between a random- or fixed-effect model was not made based on the degree of heterogeneity but according to the recent recommendations outlined by the American Heart Association (12) (i.e., by determining the functional similarity between the included studies and estimating a common effect size that would apply to populations similar to those included in the meta-analysis).
To assess the potential effect of publication bias, we examined the funnel plots for asymmetry (Supplementary Figures S1–4). The risk of bias was evaluated through Revman. In addition, sub-analyses were performed to assess the effect of location, expandable type, and MDCT-detected threshold on the relationship between the quantity of calcium and PVL.
The systematic search using PubMed and EMBASE databases yielded 131 and 299 records, respectively, with 391 total records, which were reviewed at the title and abstract level after excluding duplicates. Of those, 159 were selected and assessed for eligibility at the full-text level, 132 were excluded from the quantitative analysis owing to missing detailed data on calcium quantity, and three were excluded due to duplicated datasets. This review included 24 studies in the final analysis (Figure 1), with an overall sample of 6,846 patients (Table 1). The risk of bias (13) for each included study was evaluated with Revman, and no significant bias was found. The calcium quantity was expressed as calcium volume or score, which was detected by MDCT using patient-specific detection or fixed threshold. The regions of interest, including the aortic valve leaflets, annulus, and LVOT, were detected similarly using MDCT. Two regions were defined as follows: AVC, containing the annulus and leaflets, and the device landing zone (DLZ), containing the AVC and LVOT (14, 15). The PVL was assessed using echocardiography after the procedure, at discharge, or after a month. PVL was classified into four grades: absent (0), trace or mild (1/4), mild-to-moderate (2/4), moderate-to-severe (3/4), and severe (4/4). We regarded paravalvular leakage ≥2/4 as significant (16). New generation valves referred to prosthetic valves with sealing skirts (17–19), which could fit to the wall of the blood vessel, such as outer skirt or downward skirt, while old generations had no sealing skirts.
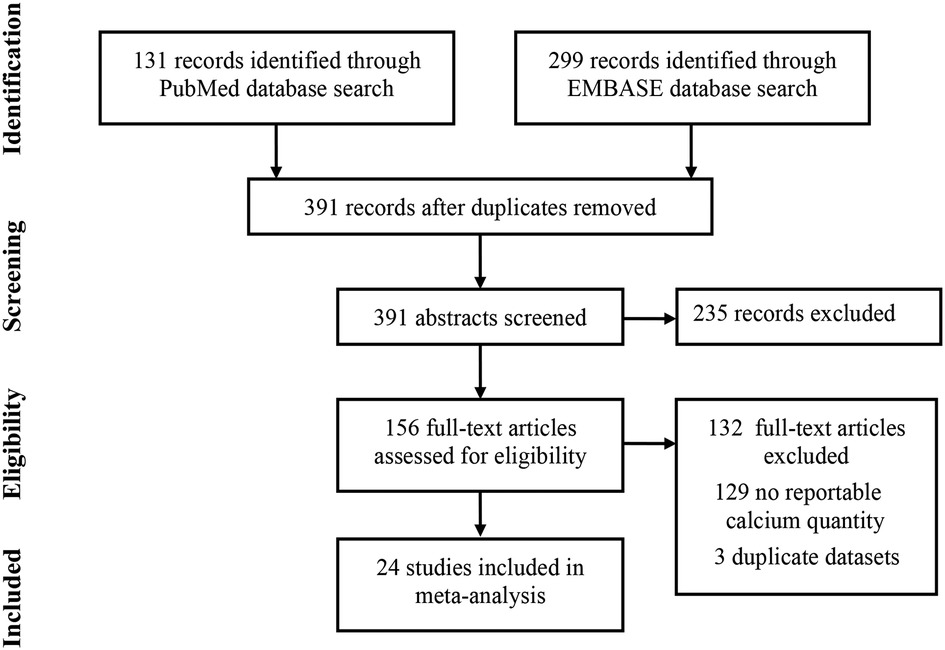
Figure 1. Flow chart of selected studies. Flow chart of studies evaluating the effect quantity and location of aortic valve calcification on paravalvular leakage (PVL) in transcatheter aortic valve replacement (TAVR) recipients. The studies were selected based on the Preferred Reported Items for Systematic Reviews and Meta-Analysis (PRISMA) statement.
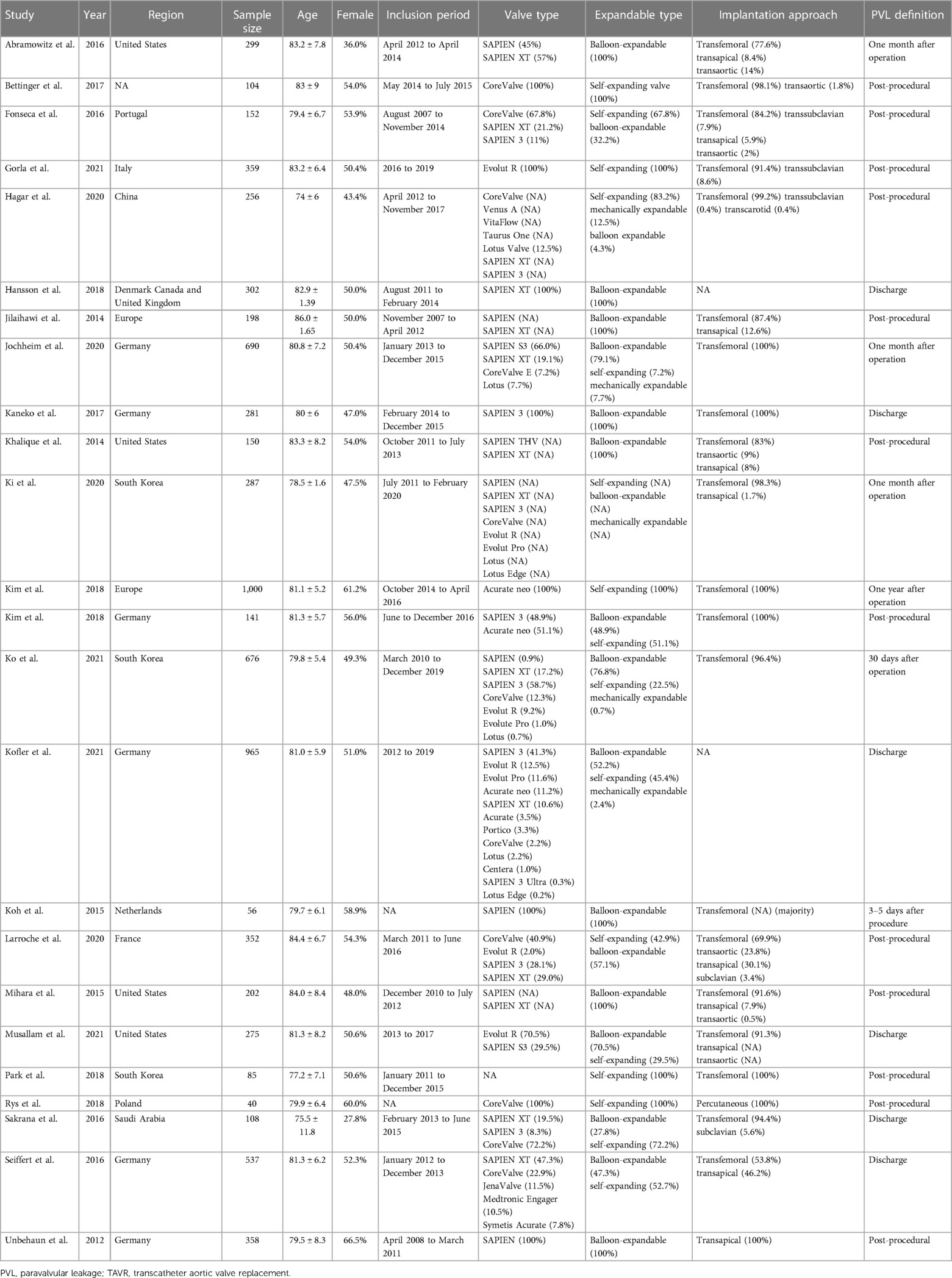
Table 1. Summary of studies evaluating the effect of aortic valve calcification on PVL after TAVR.
Six studies were included to evaluate the RR of significant PVL in patients with a high quantity of calcium. Kim et al. (20) defined the PVL in 1 year, while the duration was shorter in other studies. Overall, the percentage of high quantity of calcium in patients included in this analysis was 29.6%, and the risk of significant PVL ranged from 0% to 5.9% and 1.0% to 35.9% in patients without or with a high quantity of calcium, respectively. High quantity of calcification was observed to be significantly associated with PVL when valves without sealing skirt (RR 7.40, 95% CI 3.40–16.12; P < 0.001; Figure 2), while no such effect was observed for valves with sealing skirt (RR 2.24, 95% CI 0.28–17.68; P = 0.26; Figure 2). The total pooled results demonstrated a higher risk of significant PVL in patients with a high quantity of calcification compared to those with a low quantity (RR 3.79, 95% CI 2.29–6.28; P < 0.001; Figure 2). Heterogeneity across studies was observed (I2 = 15%). When the results from three studies were pooled, calcification in the DLZ or LVOT was found to have a significant effect on PVL (OR 3.72, 95% CI 2.80–4.95; P < 0.001; OR 2.08, 95% CI 1.07–4.03; P < 0.05; Figure 3, respectively), while no effect was observed for calcification in the annulus (OR 1.63, 95% CI 0.94–2.85; P = 0.08; Figure 3).
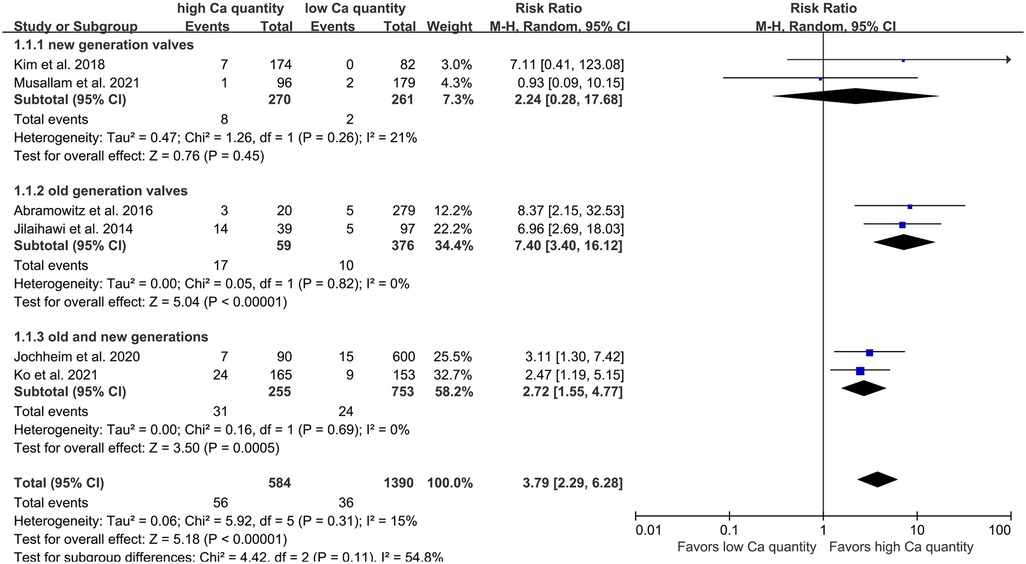
Figure 2. Risk of PVL in patients with aortic valve calcification after TAVR. RR, relative risk; PVL, paravalvular leakage; TAVR, transcatheter aortic valve replacement; M-H, Mantel-Haenszel.
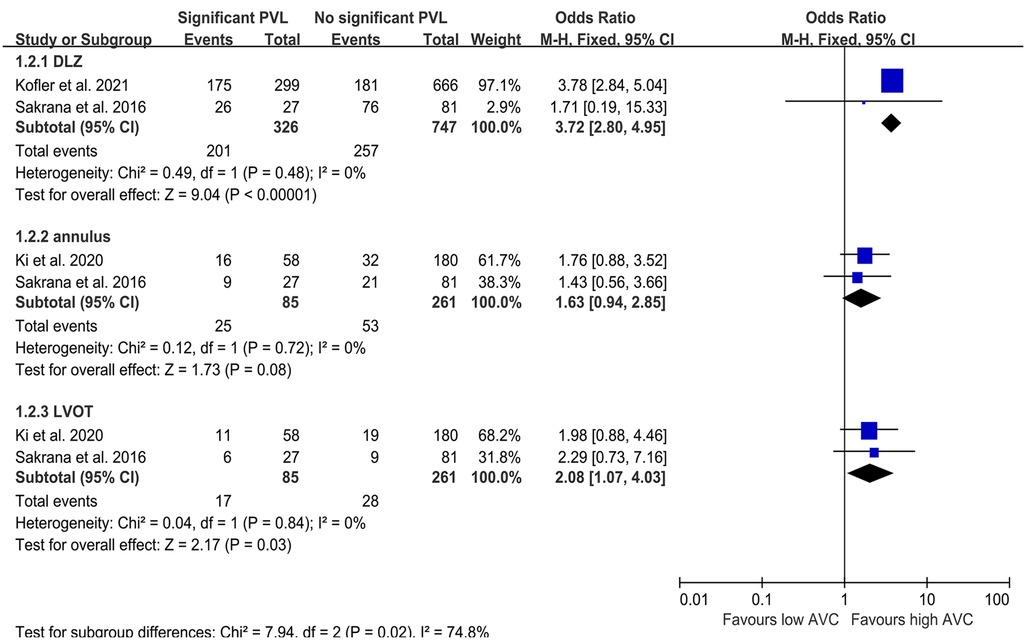
Figure 3. Odds ratio of PVL in patients with aortic valve calcification after TAVR. OR, odds ratio; PVL, paravalvular leakage; TAVR, transcatheter aortic valve replacement; M-H, Mantel-Haenszel; DLZ, device landing zone; LVOT, left ventricular outflow tract.
High quantities of calcification in the DLZ, LVOT, leaflets, and each cusp were associated with significant PVL (Figure 4), while no such effect was observed for calcification in the AVC (SMD 0.48, 95% CI −0.04–0.99; P = 0.07; Figure 4). On pooling the results of 13 studies, calcium quantity was found to be associated with PVL regardless of whether an individual-specific or fixed threshold was used for MDCT (Figure 5). Furthermore, the effect of aortic valve calcification on PVL after TAVR was similar for both self-expanding and balloon-expandable devices, both showing a significant effect on PVL (Figure 6).
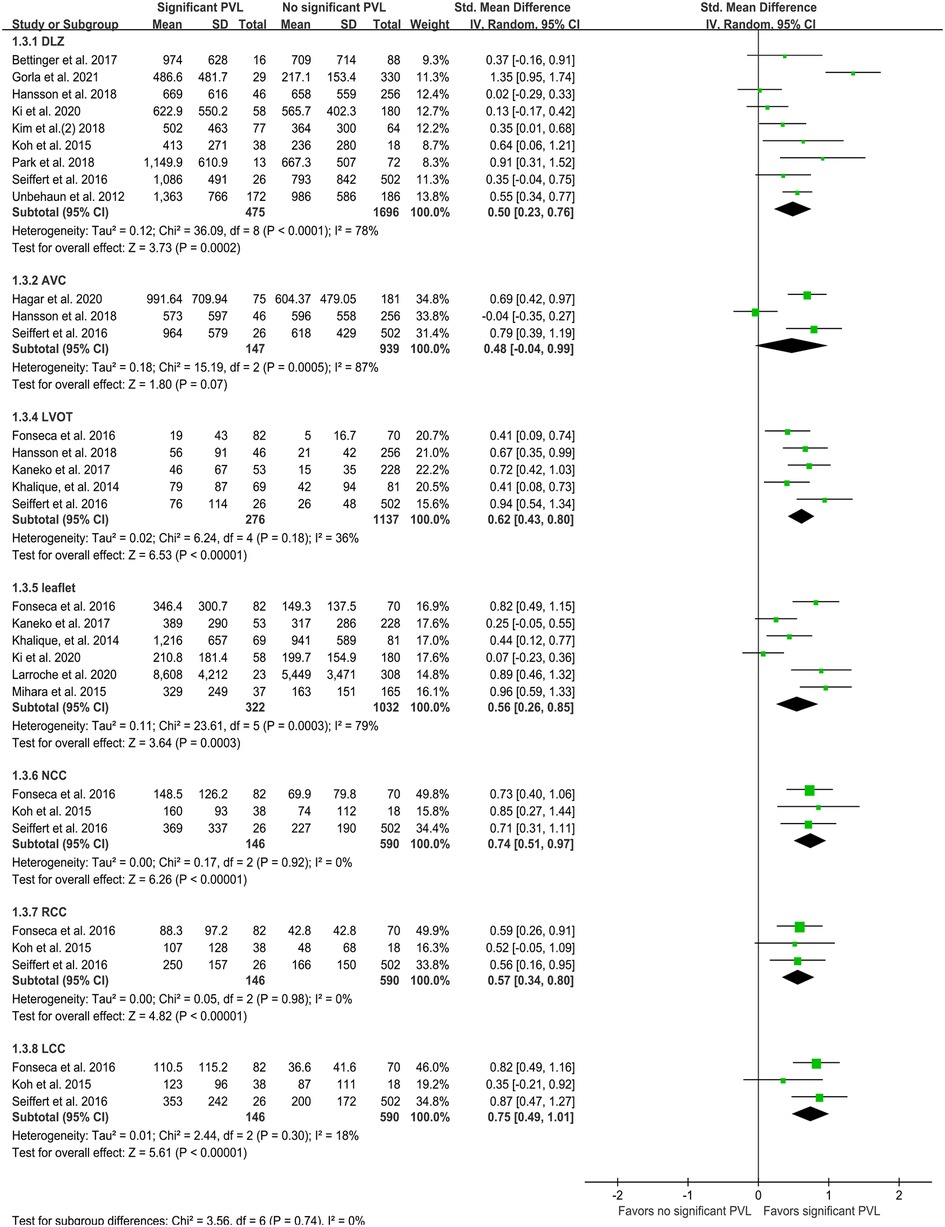
Figure 4. Quantity of calcification (mm3) per region. PVL, paravalvular leakage; IV, inverse variance; DLZ, device landing zone; AVC, aortic valve complex; LVOT, left ventricular outflow tract; NCC, non-coronary cusp; RCC, right coronary cusp; LCC, left coronary cusp.
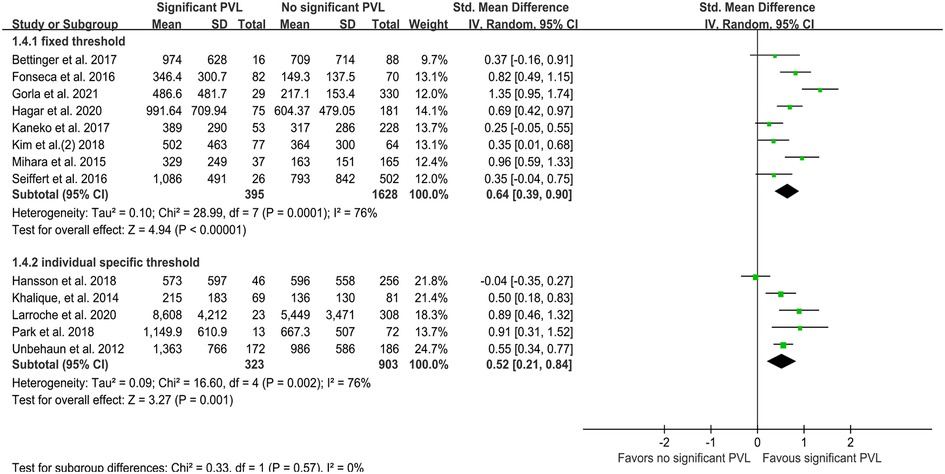
Figure 5. Quantity of calcification (mm3) per MDCT detected threshold type. MDCT, multidetector computed tomography; PVL, paravalvular leakage; IV, inverse variance.
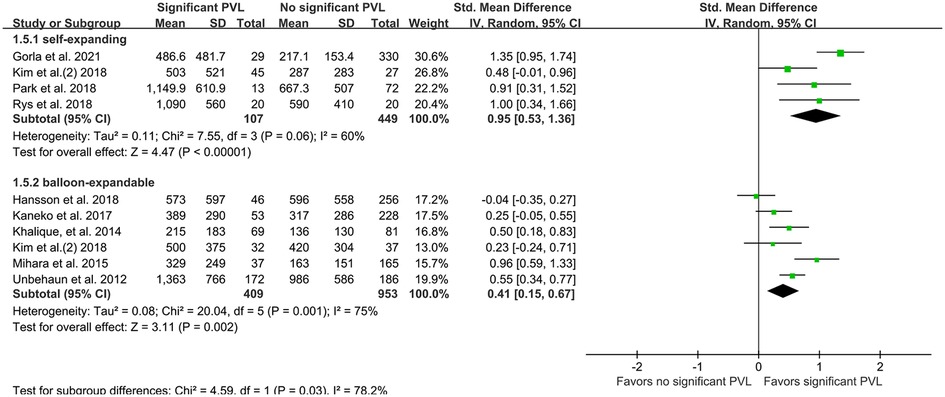
Figure 6. Quantity of calcification (mm3) per expandable type. PVL, paravalvular leakage; IV, inverse variance.
The present analysis suggested that PVL after TAVR was associated with the quantity of aortic valve calcification, especially in the LVOT, valve leaflets, and DLZ. Moreover, a high quantity of calcium was associated with PVL, regardless of whether a self-expanding/balloon-expandable valve was used or if a fixed/patient-specific detection threshold was used.
The clinical application of TAVR is currently being expanded to the treatment of younger and lower-risk patients with aortic stenosis (21, 22); however, PVL after TAVR is associated with adverse outcomes (23). Aortic valve calcification may result in PVL; thus, it was important to explore their relationship in detail. We pooled the results of recent studies and performed subgroup analyses by new or old generation valve, location, expandable type, and MDCT threshold type. To our knowledge, this is the first meta-analysis to analyze the effect of the quantity and location of aortic valve calcification on PVL after TAVR.
The effect of calcification on PVL after TAVR has remained controversial. It has been reported that the volume of aortic calcification influences PVL (7, 8, 24, 25); however, some studies suggest that the degree of calcification does not influence the likelihood of PVL occurrence after TAVR (26, 27). The present meta-analysis explored the effect of the quantity and location of calcification on PVL using the following three analyses: RR, OR, and SMD. We found that the quantity of calcification in the LVOT increases the risk of PVL after TAVR. The OR and SMD analyses suggested that calcification located in the annulus does not have a significant effect on PVL. It appeared that prosthesis implantation eliminates the obstructive characteristics of annulus calcification, while calcium in the LVOT remains unaffected (28). It is possible that the perfect anchoring of the prosthesis implantation could have prevented the calcification at the aortic valve annulus.
When assessing calcification using MDCT, Kofler et al. reported the use of individual-specific Hounsfield unit (HU) thresholds instead of the arbitrarily defined HU thresholds (29). The choice of an empirical, fixed threshold does not consider the variation in the canal attenuation between patients (30). However, we observed high levels of calcification significantly associated with PVL even after examining the patients with a fixed threshold. This may be because of the high quantity of calcification and minimal error caused by the examination threshold. In addition, Fonseca et al. found that the volume of calcium observed using a threshold of 850 HU is the best predictor of PVL (31). Therefore, we believe that for patients with high levels of calcification, it may be more appropriate to fix the threshold as this simplifies image processing.
Recent studies have reported that PVL after TAVR is more common in patients with self-expanding prostheses than in those with balloon-expandable prostheses (32). In contrast, other studies have reported no significant association between prosthesis expandable type and the incidence of PVL (33). We observed that a high quantity of calcium is associated with PVL regardless of the use of self-expanding or balloon-expandable prostheses. Therefore, the use of such devices may not improve PVL to a great extent in patients with high calcification. For these patients, next-generation devices may be more effective as newer methods, such as anchoring or sealing, repositioning, and inflatable cuffs, are used (7, 34) with added leakage-proof function (35).
Plus, subgroup analysis was conducted with the presence or absence of sealing skirts. Abramowitz et al. (36) and Jilaihawi et al. (37) conducted their studies only using old generation valves, while Kim et al. (20) and Musallam et al. (26) only used valves with sealing skirts, other two studies by Jochheim et al. (28) and Ko et al. (38) used both valves with and without sealing skirts. We observed that high quantity of calcification was associated with PVL significantly when only old generation valves were applied or both valves with and without sealing skirts were used, while no such effect was observed for valves with sealing skirt were used (RR 2.24, 95% CI 0.28–17.68; P = 0.26; Figure 2). Hence, we infer that sealing skirt has a marvelous effect on reducing the incidence of PVL, even for patients with high calcific quantity. However, the valve with skirt probably has extremely high requirements for the operator to release the valve at proper position (39).
With the increasing research evidence on calcification and PVL, we have found that the description of calcification is becoming more refined, and even computer-based calcification modeling is now being used. Moreover, valve replacement techniques are more diverse and patient-specific. As such, a quantitative account of these studies is challenging, and that we would be providing a qualitative overview of the related evidence and advances in the field. On one hand, research on computer models is rapidly progressing. Specifically, fluid-structure interaction (FSI) modeling can accurately simulate the effect of aortic valve calcification on PVL (40–42); in bicuspid aortic valve replacement due to calcification, a finite element model suggested that aligning the bioprosthetic commissures with the native commissures yielded the lowest PVL (41, 43). On the other hand, the description of calcified plaque features and PVL features is becoming increasingly accurate; however, interestingly, the related conclusions seem to be inconsistent. The aortic valve calcium scores for NCC, RCC, and NCC/RCC showed a significant relation with PVL located in the cusps of the aortic valve. Meanwhile, the scores for RCC and RCC/LCC showed a significant relation with PVL located in the commissures (44). Reportedly, with the use of SAPIEN 3 Ultra balloon-expandable valves, the amount of calcification on the leaflets is not related to PVL; only the Eccentricity Index affects the incidence of PVL (45). This index is calculated as the maximum absolute difference in calcium volume between the leakage sectors for AVC/LVOT; it describes asymmetrical calcium load (45). In addition, the use of progressively more advanced prosthetic valves may lower the incidence of PVL in patients with calcification, but it may involve higher costs. According to reports by Piayda et al., patients who received Evolut R and Pro treatment, even with severe calcification, did not experience PVL recurrence (46). Nevertheless, a computer simulation showed that Evolut Pro reduced PVL by half compared with Evolut R (43). Ong et al. discovered that Edwards SAPIEN 3 Ultra provides excellent performance in patients with significant valvular calcification (47). Theoretically, a meta-analysis on more refined calcification characteristics to single valve type is warranted. However, given the lack of consensus between relevant clinical studies to date, relevant data are scarce and limiting in this sense.
Our present meta-analysis has several limitations. All selected studies were retrospective, most being single-center observational studies. Moreover, subgroup analysis was performed for a small number of studies, which may induce bias. In addition, owing to the lack of available data, we did not perform a pooled analysis of the effect of the more specific location of calcification on PVL according to a more detailed classification of the valves.
This meta-analysis provided further evidence that aortic valve calcification—including its quantity and location—can negatively impact PVL. Our findings support the clinical relevance of developing preventive measures for PVL, particularly in patients with severe aortic valve calcification. Nevertheless, further studies are needed to develop more optimized and uniform treatment strategies to prevent PVL. The need for these studies is urgent as TAVR may soon become an important tool for the treatment of aortic stenosis.
3. Conclusions
Altogether, our present study elucidated the effect of aortic valve calcification on PVL and showed that the quantity and location of aortic valve calcification can help predict PVL. Furthermore, our results provide a reference for the selection of MDCT thresholds before TAVR. We also showed that balloon-expandable valves may not be effective in patients with high calcification, and valves with sealing skirts instead of those without sealing skirts should be applied more to prevent PVL from happening.
Data availability statement
The original contributions presented in the study are included in the article/Supplementary Material, further inquiries can be directed to the corresponding author/s.
Author contributions
JS and WL: contributed to the study design and conception. ZW and SC: provided administrative support. TZ and SC: helped procure the study materials. JS, WL, CH, XP, and XL: contributed to data collection and assembly. ZZ, PW, and JH: contributed to data analysis and interpretation. JS, WL, TZ, CH, ZW, XP, XL, ZZ, PW, JH, and SC: contributed to the first draft of the manuscript. All authors contributed to the article and approved the submitted version.
Funding
This work was supported by the Shandong Natural Science Foundation [grant number: ZR2021MH065].
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fcvm.2023.1170979/full#supplementary-material.
References
1. López-Tejero S, Núñez-García JC, Antúnez-Muiños P, González-Calle D, Martín-Moreiras J, Diego-Nieto A, et al. TAVR To solve perceval sutureless valve migration. JACC Cardiovasc Interv. (2022) 15(6):e65–e7. doi: 10.1016/j.jcin.2022.01.008
2. Schlotter F, Halu A, Goto S, Blaser MC, Body SC, Lee LH, et al. Spatiotemporal multi-omics mapping generates a molecular atlas of the aortic valve and reveals networks driving disease. Circulation. (2018) 138(4):377–93. doi: 10.1161/circulationaha.117.032291
3. Zhang X, Puehler T, Frank D, Sathananthan J, Sellers S, Meier D, et al. TAVR for all? The surgical perspective. J Cardiovasc Dev Dis. (2022) 9(7):223. doi: 10.3390/jcdd9070223
4. Guddeti RR, Gill GS, Garcia-Garcia HM, Alla VM. Transcatheter aortic valve replacement in mixed aortic valve disease: a systematic review and meta-analysis. Eur Heart J Qual Care Clin Outcomes. (2022) 8(2):169–76. doi: 10.1093/ehjqcco/qcab080
5. Laakso T, Laine M, Moriyama N, Dahlbacka S, Airaksinen J, Virtanen M, et al. Impact of paravalvular regurgitation on the mid-term outcome after transcatheter and surgical aortic valve replacement. Eur J Cardiothorac Surg. (2020) 58(6):1145–52. doi: 10.1093/ejcts/ezaa254
6. Pibarot P, Hahn RT, Weissman NJ, Arsenault M, Beaudoin J, Bernier M, et al. Association of paravalvular regurgitation with 1-year outcomes after transcatheter aortic valve replacement with the SAPIEN 3 valve. JAMA Cardiol. (2017) 2(11):1208–16. doi: 10.1001/jamacardio.2017.3425
7. Mauri V, Frohn T, Deuschl F, Mohemed K, Kuhr K, Reimann A, et al. Impact of device landing zone calcification patterns on paravalvular regurgitation after transcatheter aortic valve replacement with different next-generation devices. Open Heart. (2020) 7(1):e001164. doi: 10.1136/openhrt-2019-001164
8. Milhorini Pio S, Bax J, Delgado V. How valvular calcification can affect the outcomes of transcatheter aortic valve implantation. Expert Rev Med Devices. (2020) 17(8):773–84. doi: 10.1080/17434440.2020.1789456
9. Liberati A, Altman DG, Tetzlaff J, Mulrow C, Gøtzsche PC, Ioannidis JP, et al. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: explanation and elaboration. J Clin Epidemiol. (2009) 62(10):e1–34. doi: 10.1016/j.jclinepi.2009.06.006
10. Luo D, Wan X, Liu J, Tong T. Optimally estimating the sample mean from the sample size, median, mid-range, and/or mid-quartile range. Stat Methods Med Res. (2018) 27(6):1785–805. doi: 10.1177/0962280216669183
11. Wan X, Wang W, Liu J, Tong T. Estimating the sample mean and standard deviation from the sample size, median, range and/or interquartile range. BMC Med Res Methodol. (2014) 14:135. doi: 10.1186/1471-2288-14-135
12. Rao G, Lopez-Jimenez F, Boyd J, D'Amico F, Durant NH, Hlatky MA, et al. Methodological standards for meta-analyses and qualitative systematic reviews of cardiac prevention and treatment studies: a scientific statement from the American heart association. Circulation. (2017) 136(10):e172–e94. doi: 10.1161/cir.0000000000000523
13. Wang W, Zhang X, Shi Y, Xu S, Shi T, Han X, et al. Is valve-sparing aortic root replacement better than total aortic root replacement? An overview of reviews. Front Cardiovasc Med. (2023) 10:1115290. doi: 10.3389/fcvm.2023.1115290
14. Hansson NC, Leipsic J, Pugliese F, Andersen HR, Rossi A, Simonato M, et al. Aortic valve and left ventricular outflow tract calcium volume and distribution in transcatheter aortic valve replacement: influence on the risk of significant paravalvular regurgitation. J Cardiovasc Comput Tomogr. (2018) 12(4):290–7. doi: 10.1016/j.jcct.2018.02.002
15. Seiffert M, Fujita B, Avanesov M, Lunau C, Schoen G, Conradi L, et al. Device landing zone calcification and its impact on residual regurgitation after transcatheter aortic valve implantation with different devices. Eur Heart J Cardiovasc Imaging. (2016) 17(5):576–84. doi: 10.1093/ehjci/jev174
16. Détaint D, Lepage L, Himbert D, Brochet E, Messika-Zeitoun D, Iung B, et al. Determinants of significant paravalvular regurgitation after transcatheter aortic valve: implantation impact of device and annulus discongruence. JACC Cardiovasc Interv. (2009) 2(9):821–7. doi: 10.1016/j.jcin.2009.07.003
17. Choudhury T, Solomonica A, Bagur R. The ACURATE neo transcatheter aortic valve system. Expert Rev Med Devices. (2018) 15(10):693–9. doi: 10.1080/17434440.2018.1526675
18. Piazza N, Martucci G, Lachapelle K, de Varennes B, Bilodeau L, Buithieu J, et al. First-in-human experience with the medtronic CoreValve evolut R. EuroIntervention. (2014) 9(11):1260–3. doi: 10.4244/eijv9i11a215
19. Barbanti M, Costa G. SAPIEN 3 ultra transcatheter aortic valve device: two sides of the moon. JACC Cardiovasc Interv. (2020) 13(22):2639–41. doi: 10.1016/j.jcin.2020.08.011
20. Kim W-K, Hengstenberg C, Hilker M, Kerber S, Schaefer U, Rudolph T, et al. The SAVI-TF registry 1-year outcomes of the European post-market registry using the ACURATE neo transcatheter heart valve under real-world conditions in 1,000 patients. JACC Cardiovasc Interv. (2018) 11(14):1368–74. doi: 10.1016/j.jcin.2018.03.023
21. Mack MJ, Leon MB, Thourani VH, Makkar R, Kodali SK, Russo M, et al. Transcatheter aortic-valve replacement with a balloon-expandable valve in low-risk patients. N Engl J Med. (2019) 380(18):1695–705. doi: 10.1056/NEJMoa1814052
22. Popma JJ, Deeb GM, Yakubov SJ, Mumtaz M, Gada H, O'Hair D, et al. Transcatheter aortic-valve replacement with a self-expanding valve in low-risk patients. N Engl J Med. (2019) 380(18):1706–15. doi: 10.1056/NEJMoa1816885
23. Amrane H, Porta F, Van Boven AV, Kappetein AP, Head SJ. A meta-analysis on clinical outcomes after transaortic transcatheter aortic valve implantation by the heart team. EuroIntervention. (2017) 13(2):e168–e76. doi: 10.4244/eij-d-16-00103
24. Hamm CW, Arsalan M, Mack MJ. The future of transcatheter aortic valve implantation. Eur Heart J. (2016) 37(10):803–10. doi: 10.1093/eurheartj/ehv574
25. Pollari F, Dell'Aquila AM, Söhn C, Marianowicz J, Wiehofsky P, Schwab J, et al. Risk factors for paravalvular leak after transcatheter aortic valve replacement. J Thorac Cardiovasc Surg. (2019) 157(4):1406–15.e3. doi: 10.1016/j.jtcvs.2018.08.085
26. Musallam A, Buchanan KD, Yerasi C, Dheendsa A, Zhang C, Shea C, et al. Impact of left ventricular outflow tract calcification on outcomes following transcatheter aortic valve replacement. Cardiovasc Revasc Med. (2022) 35:1–7. doi: 10.1016/j.carrev.2021.07.010
27. Nakajima A, Naganuma T, Yuki H, Onishi H, Amano T, Yabushita H, et al. The impact of aortic valvular calcium on transcatheter heart valve distortion. J Interv Cardiol. (2021) 2021:8829906. doi: 10.1155/2021/8829906
28. Jochheim D, Deseive S, Gschwendtner S, Bischoff B, Jochheim S, Hausleiter S, et al. Impact of severe left ventricular outflow tract calcification on device failure and short-term mortality in patients undergoing TAVI. J Cardiovasc Comput Tomogr. (2020) 14(1):36–41. doi: 10.1016/j.jcct.2019.07.004
29. Kofler M, Meyer A, Schwartz J, Sundermann S, Penkalla A, Solowjowa N, et al. A new calcium score to predict paravalvular leak in transcatheter aortic valve implantation. Eur J Cardiothorac Surg. (2021) 59(4):894–900. doi: 10.1093/ejcts/ezaa424
30. Bettinger N, Khalique OK, Krepp JM, Hamid NB, Bae DJ, Pulerwitz TC, et al. Practical determination of aortic valve calcium volume score on contrast-enhanced computed tomography prior to transcatheter aortic valve replacement and impact on paravalvular regurgitation: elucidating optimal threshold cutoffs. J Cardiovasc Comput Tomogr. (2017) 11(4):302–8. doi: 10.1016/j.jcct.2017.04.009
31. Fonseca P, Figueiredo B, Almeida C, Almeida J, Bettencourt N, Sampaio F, et al. Aortic valve calcium volume predicts paravalvular regurgitation and the need for balloon post-dilatation after transcatheter aortic valve implantation. J Interv Cardiol. (2016) 29(1):117–23. doi: 10.1111/joic.12267
32. Abdel-Wahab M, Comberg T, Büttner HJ, El-Mawardy M, Chatani K, Gick M, et al. Aortic regurgitation after transcatheter aortic valve implantation with balloon- and self-expandable prostheses: a pooled analysis from a 2-center experience. JACC Cardiovasc Interv. (2014) 7(3):284–92. doi: 10.1016/j.jcin.2013.11.011
33. Sakrana AA, Nasr MM, Ashamallah GA, Abuelatta RA, Naeim HA, Tahlawi ME. Paravalvular leak after transcatheter aortic valve implantation: is it anatomically predictable or procedurally determined? MDCT study. Clin Radiol. (2016) 71(11):1095–103. doi: 10.1016/j.crad.2016.07.016
34. Généreux P, Head SJ, Hahn R, Daneault B, Kodali S, Williams MR, et al. Paravalvular leak after transcatheter aortic valve replacement: the new Achilles’ heel? A comprehensive review of the literature. J Am Coll Cardiol. (2013) 61(11):1125–36. doi: 10.1016/j.jacc.2012.08.1039
35. Meredith IT, Walters DL, Dumonteil N, Worthley SG, Tchétché D, Manoharan G, et al. 1-year outcomes with the fully repositionable and retrievable Lotus transcatheter aortic replacement valve in 120 high-risk surgical patients with severe aortic stenosis: results of the REPRISE II study. JACC Cardiovasc Inter. (2016) 9(4):376–84. doi: 10.1016/j.jcin.2015.10.024
36. Abramowitz Y, Jilaihawi H, Chakravarty T, Kashif M, Matar G, Hariri B, et al. Balloon-expandable transcatheter aortic valve replacement in patients with extreme aortic valve calcification. Catheter Cardiovasc Interv. (2016) 87(6):1173–9. doi: 10.1002/ccd.26311
37. Jilaihawi H, Makkar RR, Kashif M, Okuyama K, Chakravarty T, Shiota T, et al. A revised methodology for aortic-valvar complex calcium quantification for transcatheter aortic valve implantation. Eur Heart J Cardiovasc Imaging. (2014) 15(12):1324–32. doi: 10.1093/ehjci/jeu162
38. Ko E, Kang D-Y, Ahn J-M, Kim TO, Kim JH, Lee J, et al. Association of aortic valvular complex calcification burden with procedural and long-term clinical outcomes after transcatheter aortic valve replacement. Eur Heart J Cardiovasc Imaging. (2022) 23(11):1502–0. 10.1093/ehjci/jeab18034491331
39. Conte SM, Kearney K, Jain P, Watson A, Hayward C, Muller DW, et al. Plugging paravalvular leak in transcatheter aortic valves. JACC Case Rep. (2019) 1(5):696–702. doi: 10.1016/j.jaccas.2019.10.013
40. Luraghi G, Matas JFR, Beretta M, Chiozzi N, Iannetti L, Migliavacca F. The impact of calcification patterns in transcatheter aortic valve performance: a fluid-structure interaction analysis. Comput Methods Biomech Biomed Engin. (2021) 24(4):375–83. doi: 10.1080/10255842.2020.1817409
41. Ghosh RP, Marom G, Bianchi M, D'Souza K, Zietak W, Bluestein D. Numerical evaluation of transcatheter aortic valve performance during heart beating and its post-deployment fluid-structure interaction analysis. Biomech Model Mechanobiol. (2020) 19(5):1725–40. doi: 10.1007/s10237-020-01304-9
42. Luraghi G, Migliavacca F, García-González A, Chiastra C, Rossi A, Cao D, et al. On the modeling of patient-specific transcatheter aortic valve replacement: a fluid-structure interaction approach. Cardiovasc Eng Technol. (2019) 10(3):437–55. doi: 10.1007/s13239-019-00427-0
43. Lavon K, Marom G, Bianchi M, Halevi R, Hamdan A, Morany A, et al. Biomechanical modeling of transcatheter aortic valve replacement in a stenotic bicuspid aortic valve: deployments and paravalvular leakage. Med Biol Eng Comput. (2019) 57(10):2129–43. doi: 10.1007/s11517-019-02012-y
44. Pavicevic J, Nguyen TD, Caliskan E, Reser D, Frauenfelder T, Plass A, et al. Aortic valve calcium score is a significant predictor for the occurrence of post-interventional paravalvular leakage after transcatheter aortic valve implantation—results from a single center analysis of 260 consecutive patients. Int J Cardiol. (2015) 181:185–7. doi: 10.1016/j.ijcard.2014.12.032
45. Schaefer A, Plassmeier F, Schofer N, Vogel L, Ludwig S, Schneeberger Y, et al. Early commercial experience with a newly designed balloon-expandable transcatheter heart valve: 30-day outcomes and implications of preprocedural computed tomography. Interact Cardiovasc Thorac Surg. (2021) 32(3):426–32. doi: 10.1093/icvts/ivaa275
46. Piayda K, Hellhammer K, Veulemans V, Afzal S, Heidari H, Wimmer AC, et al. Performance of the CoreValve evolut R and PRO in severely calcified anatomy: a propensity score matched analysis. Heart Lung Circ. (2020) 29(12):1847–55. doi: 10.1016/j.hlc.2020.05.096
Keywords: paravalvular leakage (PVL), transcatheter aortic valve replacement (TAVI), aortic valve complex, calcification, left ventricular outflow tract (LVOT)
Citation: Shi J, Li W, Zhang T, Han C, Wang Z, Pei X, Li X, Zhao Z, Wang P, Han J and Chen S (2023) Quantity and location of aortic valve calcification predicts paravalvular leakage after transcatheter aortic valve replacement: a systematic review and meta-analysis. Front. Cardiovasc. Med. 10:1170979. doi: 10.3389/fcvm.2023.1170979
Received: 21 February 2023; Accepted: 9 May 2023;
Published: 24 May 2023.
Edited by:
Enyi Shi, China Medical University, ChinaReviewed by:
Liang Guo, The First Affiliated Hospital of China Medical University, ChinaMatteo Saccocci, San Raffaele Hospital (IRCCS), Italy
Dritan Useini, Herz-Kreislauf-Zentrum Klinikum Hersfeld-Rotenburg GmbH, Germany
© 2023 Shi, Li, Zhang, Han, Wang, Pei, Li, Zhao, Wang, Han and Chen. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Shiqiao Chen Y2hlbnNoaXFpYW9jY3VAMTYzLmNvbQ==
†These authors have contributed equally to this work and share first authorship