 Li-Da Wu
Li-Da Wu Peng Chu
Peng Chu Chao-Hua Kong†
Chao-Hua Kong† Jun-Xia Zhang
Jun-Xia Zhang Shao-Liang Chen
Shao-Liang Chen
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Cardiovasc. Med. , 17 April 2023
Sec. Cardiovascular Pharmacology and Drug Discovery
Volume 10 - 2023 | https://doi.org/10.3389/fcvm.2023.1157163
This article is part of the Research Topic Debates in Cardiovascular Pharmacology and Drug Discovery: 2022 View all 6 articles
Aims: We aim to examine the association of estimated pulse wave velocity (ePWV) with all-cause and cardiovascular mortality in patients with diabetes.
Methods: All of adult participants with diabetes from the National Health and Nutrition Examination Survey (NHANES) (1999–2018) were enrolled. ePWV was calculated according to the previously published equation based on age and mean blood pressure. The mortality information was obtained from the National Death Index database. Weighted Kaplan-Meier (KM) plot and weighted multivariable Cox regression was used to investigate the association of ePWV with all-cause and cardiovascular mortality risks. Restricted cubic spline was adopted to visualize the relationship between ePWV and mortality risks.
Results: 8,916 participants with diabetes were included in this study and the median follow-up duration was ten years. The mean age of study population was 59.0 ± 11.6 years, 51.3% of the participants were male, representing 27.4 million patients with diabetes in weighted analysis. The increment of ePWV was closely associated with increased risks of all-cause mortality (HR: 1.46, 95% CI: 1.42–1.51) and cardiovascular mortality (HR: 1.59, 95% CI: 1.50–1.68). After adjusting for cofounding factors, for every 1 m/s increase in ePWV, there was a 43% increased risk of all-cause mortality (HR: 1.43, 95% CI: 1.38–1.47) and 58% increased of cardiovascular mortality (HR: 1.58, 95% CI: 1.50–1.68). ePWV had positive linear associations with all-cause and cardiovascular mortality. KM plots also showed that the risks of all-cause and cardiovascular mortality were significantly elevated in patients with higher ePWV.
Conclusions: ePWV had a close association with all-cause and cardiovascular mortality risks in patients with diabetes.
Arterial stiffness is an important cardiovascular risk factor and strongly associated with increased mortality (1, 2). Arterial stiffness can be assessed by carotid-femoral pulse wave velocity (cf-PWV), which is now listed in the guidelines for detecting organ damage caused by hypertension (3). However, cf-PWV is not widely used in clinical practice due to its measurement needs experienced staff and specialized equipment. Estimated pulse wave velocity (ePWV) is a novel index calculated based on mean blood pressure (MBP) and age (4–6). Although ePWV cannot substitute cf-PWV, it has been validated that ePWV reliably reflects the degree of arterial stiffness (7–9). Moreover, studies already demonstrated that ePWV had predictive value for cardiovascular risks (10, 11). Nevertheless, whether ePWV is associated with all-cause mortality and cardiovascular mortality in patients with diabetes remains exclusive.
Vascular remodeling is thought to be an important feature of human aging, loss of arterial elasticity is common as people age (12, 13). But at the individual level, vascular remodeling is actually a dynamic process, influenced by life style, genetic/epigenetic factors, and biological cues (14–16). Diabetes is an important risk factor for vascular remodeling, which can cause extracellular matrix changes, eventually leading to arterial remodeling and arterial stiffness (17, 18). It has been reported that arterial stiffness is greater in patients with diabetes than in individuals without diabetes (19, 20). Zhang et al. observed that reactive oxygen species were significantly elevated in the arteries of STZ-induced diabetic rats, and oxidative stress can lead to deposition of collagen and arterial fibrosis (21). Besides, arterial stiffness was shown to predict Alzheimer's disease, atrial fibrillation, and stroke (22–24). Therefore, more attention should be paid to arterial stiffness in patients with diabetes.
Although several studies have already investigated the association of ePWV and mortality in general population, to the best of our knowledge, the association between ePWV and mortality in the high-risk population of patients with diabetes remains exclusive. In the present study, based on a large multiracial population from National Health and Nutrition Examination Survey (NHANES), we investigated the association of ePWV with all-cause mortality and cardiovascular mortality in patients with diabetes.
NHANES is a continuous cross-sectional survey, conducted once every 2 years by the National Center for Health Statistics in the Centers for Disease Control and Prevention (25, 26). The method of “stratified multistage probability sampling” was adopted to screen out representative participants in NHANES survey (26). Detailed methods are described in the NHANES website (http://www.cdc.gov/nchs/nhanes.htm). All participants enrolled in NHANES provided written informed consent, and the whole procedures were approved by the Institutional Review Board of the Centers for Disease Control and Prevention. An analysis of the ten consecutive NHANES circles (1999–2018) was performed in the present study. Participants meeting one or more of the following criteria were considered to have diabetes: (1) self-reported diabetes; (2) individuals with prescribed antidiabetic medications; (3) fasting glucose ≥7.0 mmol/L or plasma HbA1c ≥ 6.5% (27). Among a total of 101,316 participants from NHANES survey, 9,233 individuals were diagnosed as diabetes. After excluding 317 participants younger than 18 years old or pregnant, a total of 8,916 adults with diabetes were enrolled in the present study.
The blood pressure was recorded by a trained examiner after participants resting quietly in a seated position for 5 min according to the protocol of blood pressure measurement released by the American Heart Association (28). The average systolic blood pressure (SBP) and diastolic blood pressure (DBP) of three consecutive measurements was obtained and reported. Same as previous published studies (29, 30), MBP was calculated as algorithm (1):
ePWV was calculated based on the algorithm (2):
Participants enrolled in this study were linked to the National Death Index (NDI) database (https://www.cdc.gov/nchs/data-linkage/mortality-public.htm) to obtain death certificate data and determine mortality status. Publicly accessible death data were adopted from the start of follow-up to December 31, 2019 (the last update date of NDI database). Mortality outcomes were determined according the International Statistical Classification of Diseases, 10th Revision (ICD-10) (31). In ICD-10, cardiovascular death is defined as a death caused by a disease or condition related to the circulatory system. ICD-10 codes for cardiovascular death include a range of codes related to heart failure (I50), cerebrovascular accidents or strokes (CVA) (I60–I69), and poisoning or adverse effects of agents affecting the cardiovascular system (T46).
Age, sex, race/ethnicity, education levels and family income were obtained from the demographic questionnaires of NHANES survey. Alcohol consumption, smoking status and status of other chronic diseases were adopted from the health questionnaires. Moreover, Charlson comorbidity index (CCI) was also calculated based on the heathy status of participants (32). Age (years) was used as a continuous variable. Sex was classified as male or female. Race/ethnicity was classified as Mexican American, non-Hispanic White, non-Hispanic Black, Mexican, and others. Body mass index (BMI) was measured and categorized into: <25.0, 25.0–29.9, and >29.9 kg/m2 according to the definition of obesity and overweight. Smoking status were categorized as never smoker, ever smoker, and current smoker as suggested by NHANES (33). Drinking status were categorized as nondrinker, low to moderate drinker, and heavy drinker as suggested by NHANES (34). Education levels were divided into three levels, less than high school, high school or equivalent, and college or above. After at least 8 h of an overnight fast, 5 ml blood samples were collected and used to examine the levels of serum insulin, blood glucose, HbA1c, total triglyceride (TG), total cholesterol (TC), high-density lipoprotein cholesterol (HDL-C), low-density lipoprotein cholesterol (LDL-C), C-reactive protein (CRP), NHANES website provided the detailed procedures in collecting blood biochemical measurements.
We followed the NHANES analytic and reporting guidance in the present study. To reduce bias induced by post-stratification, non-response, and oversampling, stratified multistage probability sampling was adopted in NHANES. According to the primary sampling unit, a specific sampling weight was assigned to each participant to ultimately produce representative estimates in the nation-wide. All data was produced according to the finally 20-years survey weight in statistical analysis. Continuous variables were presented as the weighted mean [95% confidence interval (CI)], and categorical variables were represented as proportions (95% CI). Baseline characteristics and were compared using adjusted Wald test for continuous variables and Rao-Scott χ2 test for categorical variables. Restricted cubic spline was adopted to visualize the linear relationship between ePWV and all-cause mortality and cardiovascular mortality. The p-value of linearity in RCS analysis is determined by comparing the fit of a linear model to that of a more complex model that includes splines, using the likelihood ratio test to obtain a test statistic and its associated p-value. We adopted the currently most recommended method of selecting 3 knots for RCS analysis. Weighted multivariable Cox regression was used to further investigate the association of ePWV with mortality risks. Since ePWV is calculated based on age and blood pressure, we found significant multicollinearity between age, SBP, and ePWV in the first adjusted cox regression model (Supplementary Table S1). Therefore, model I was finally adjusted for sex, race/ethnicity, and study circle, and model II was finally adjusted for sex, race/ethnicity, study circle, education levels, smoking, drinking, hypertension, and CCI. Results of Cox regression were presented as Hazard ratios (HRs) and 95% CI. As the missing values were within an acceptable range of approximately 20%, we used multiple imputation to handle the missing data. A P value < 0.05 was considered significant. All statistical analyses were conducted using R software (version 4.1.6, R Foundation for Statistical Computing, Vienna, Austria).
A total of 8,916 participants with diabetes from NHANES survey were included in this study, representing 27.4 million patients with diabetes in the US. The mean age of study population was 59.0 years, 51.3% of the participants were male. The weighted mean level of ePWV was 9.50 m/s, and the median ePWV was 9.73 m/s. As shown in Table 1, patients with higher ePWV (ePWV ≥ 9.73 m/s) were older (71.1 vs. 50.2 years), more often quit smoking, and more likely to suffer from hypertension (85.8% vs. 60.4%) and other cardiovascular diseases. The proportion of participants with CCI ≥ 2 was significant higher in participants with higher ePWV. The comparison of cardiometabolic markers between two groups was shown in Table 2.
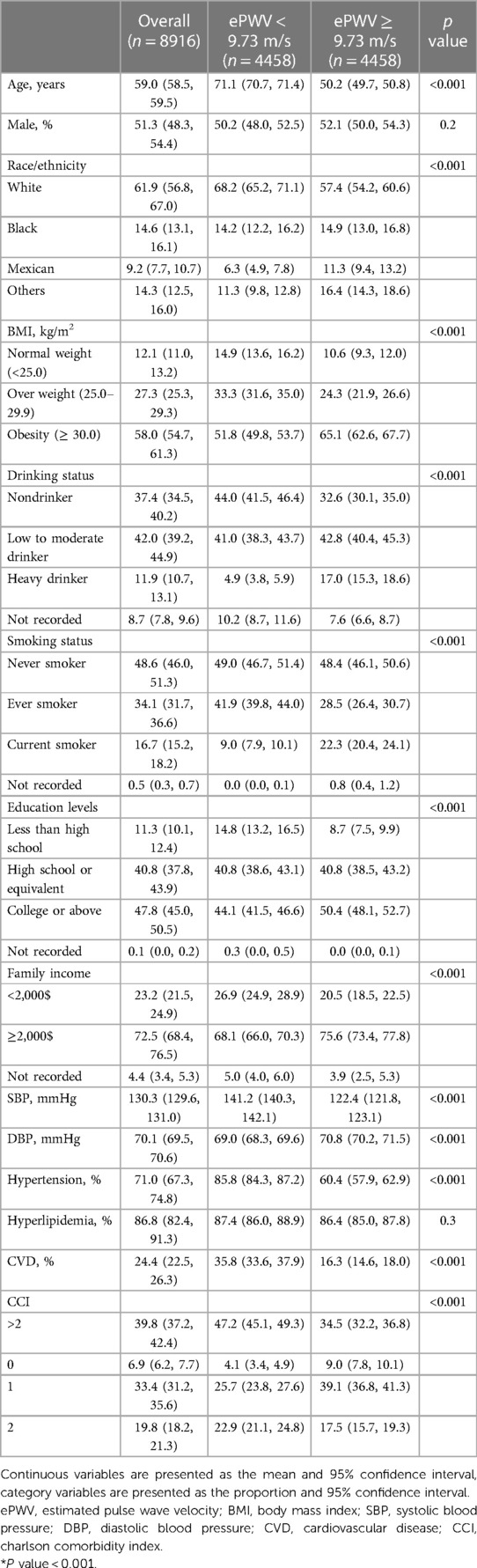
Table 1. Baseline characteristics of study population.
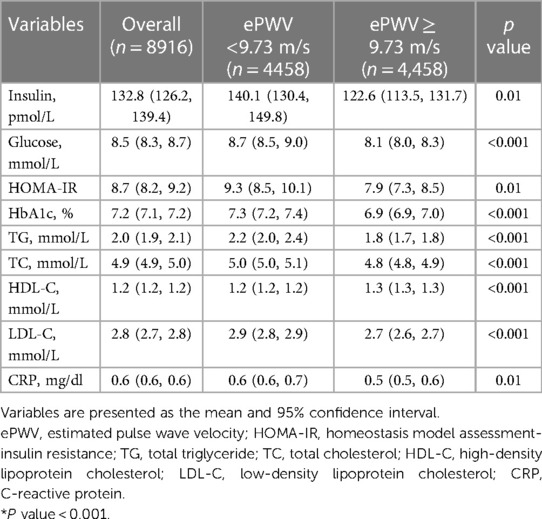
Table 2. Cardiometabolic markers of study population.
The median follow-up time was 10.0 (95% CI: 9.8–10.2) years. During that time, 2,407 (27.0%) of 8,916 patients with diabetes died, including 684 (7.7%) cardiovascular deaths. Weighted all-cause mortality (1,000 person-years) of the study population was 33.6 (95% CI: 32.8–33.9), and weighted cardiovascular mortality was 5.6 (95% CI: 5.2–5.8). Results of restricted cubic spline showed that ePWV positively correlated with all-cause mortality and cardiovascular mortality, the linear relationship was visualized in Figure 1. Weighted Kaplan-Meier (KM) plots also showed the risks of all-cause mortality (Figure 2A) and cardiovascular mortality (Figure 2B) were significantly elevated in patients with higher ePWV. We also adopted weighted multivariable Cox regression analyses to investigate the association between ePWV and mortality risk. In the non-adjusted model, we found that every 1 m/s increase in ePWV, there was a 46% increased risk of all-cause mortality (HR: 1.46, 95% CI: 1.42–1.51) and 59% increased risk of cardiovascular mortality (HR: 1.59, 95% CI: 1.50–1.68). After adjusting for confounding factors including sex, race/ethnicity, study circle, education levels, smoking, drinking, hypertension, and CCI, the relationship between ePWV and all-cause mortality (HR: 1.43, 95% CI: 1.38–1.47) and cardiovascular mortality (HR: 1.58, 95% CI: 1.50–1.68) were still significant (Table 3). Although covariates were adjusted, considering individuals with higher ePWV have a higher proportion of pre-existing cardiovascular disease due to the characteristics of ePWV that are highly associated with age. Subgroup analysis stratified by age, gender, presence of hypertension, and cardiovascular disease as you suggested. In patients with pre-existing cardiovascular disease and patients without pre-existing cardiovascular disease, ePWV both showed a favor prognostic value (Figure 3). Since ePWV is calculated based on age and blood pressure, we found significant multicollinearity between age, SBP, and ePWV. However, considering age and SBP are strongest risk factor for all-cause and cardiovascular mortality, we further included age and SBP in the model to determine whether ePWV is an independent risk factor for cardiovascular mortality. Of note, we found that ePWV is not an independent risk factor for all-cause mortality (HR: 1.08, 95% CI: 0.98–1.2, p = 0.12) and cardiovascular mortality (HR: 1.18, 95% CI: 0.98–1.42, p = 0.09) adjusting for age and SBP.
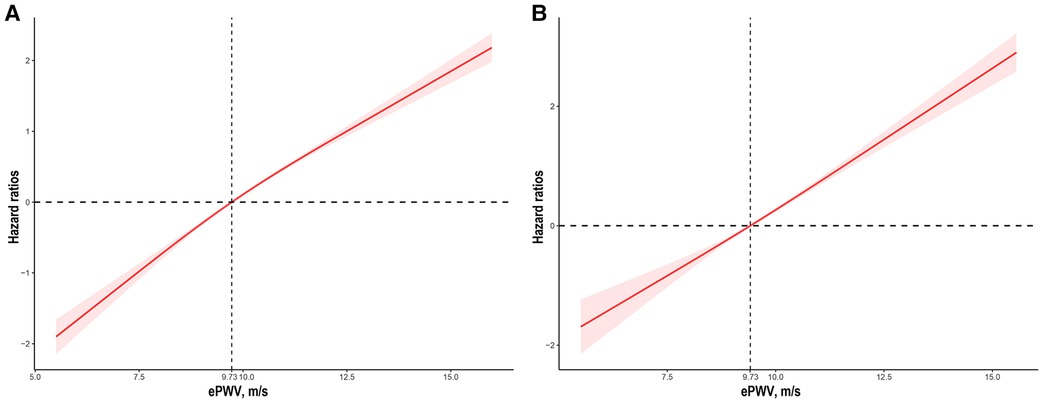
Figure 1. The association of ePWV with all-cause (A) and cardiovascular mortality (B) among participants with diabetes visualized by the restricted cubic spline. HRs were adjusted for sex, race/ethnicity, study circles, education levels, smoking, drinking, hypertension, and CCI. Both p for linearity <0.001. ePWV, estimated pulse wave velocity; CCI, Charlson comorbidity index.
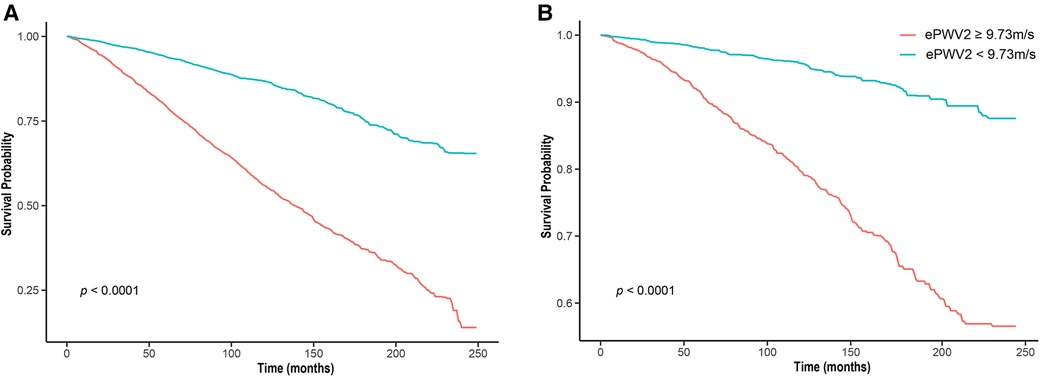
Figure 2. Kaplan–Meier survival curve of patients with lower (< 9.73m/s) ePWV and higher (≥ 9.73m/s) ePWV. ePWV, estimated pulse wave velocity (A) all cause survival; (B) cardiovascular cause survival.
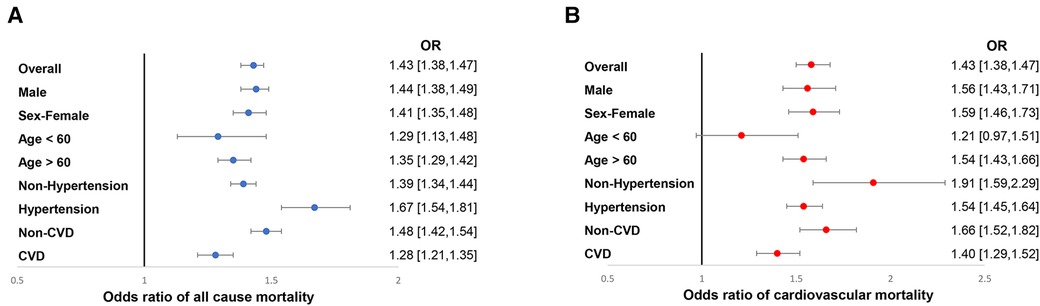
Figure 3. Subgroup analysis of the association between ePWV with all-cause (A) and cardiovascular mortality (B) among participants with diabetes. HRs were adjusted for sex, race/ethnicity, study circles, education levels, smoking, drinking, hypertension, and CCI. ePWV, estimated pulse wave velocity; CCI, Charlson comorbidity index.

Table 3. Cox regression analysis on the association between ePWV and All-cause mortality and cardiovascular mortality.
We also carried out time-dependent ROC curve analysis to evaluate the prognostic value of ePWV for all-cause mortality and cardiovascular mortality. The results showed that ePWV had a good predicting value of all-cause mortality (Figures 4A,B) and cardiovascular mortality (Figures 4C,D) in short-term, medium-term, and long-term. We found that best cut-off value of ePWV for 3 years, 5 years, and 10 years all-cause mortality were 14.23, 9.95, and 12.45, respectively. The best cut-off value of ePWV for 3 years, 5 years, and 10 years cardiovascular mortality were 7.53, 9.17, and 12.63, respectively.
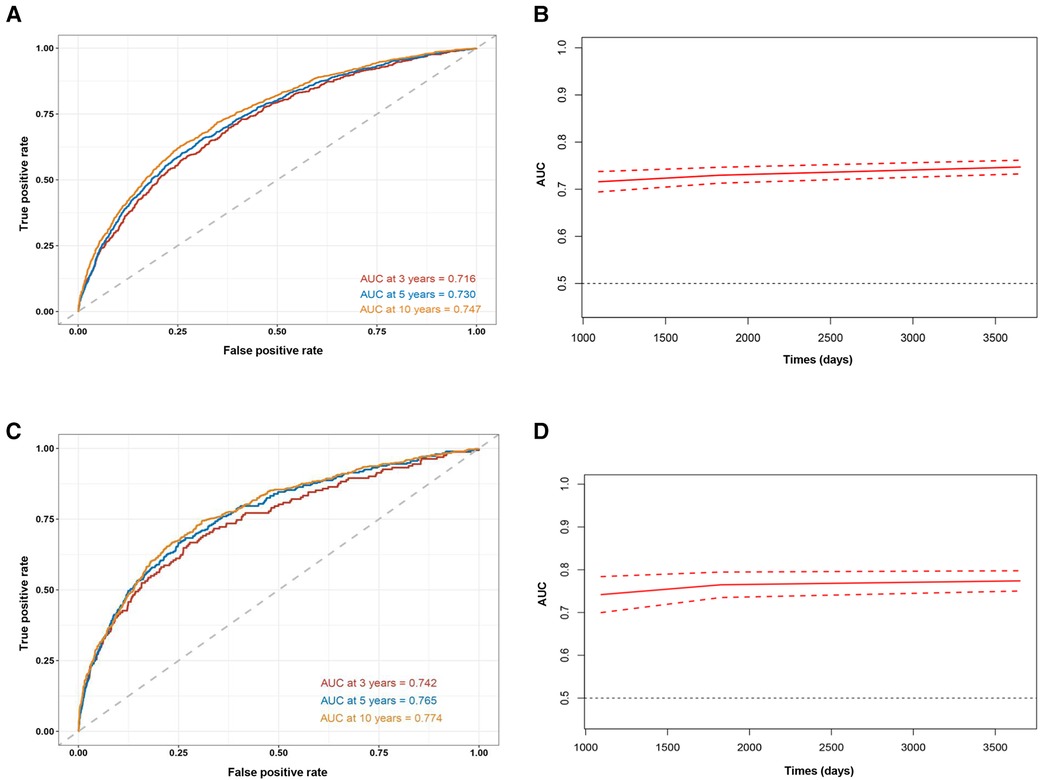
Figure 4. Time-dependent ROC curves (A) and time-dependent AUC values (B) of ePWV predicting all-cause mortality, and time-dependent ROC curves (C) and time-dependent AUC values (D) of ePWV predicting cardiovascular mortality.
Concurring with aging, arterial stiffness is a type of inflammatory lesion of the artery, which can make the arterial wall thick, and make the lumen narrow (35). The most important causes of arterial stiffness are high blood pressure, hyperlipidemia and smoking. Moreover, obesity, diabetes, physical inactivity, and stress can all contribute to arterial stiffness (36). The manifestations of arterial stiffness are mainly determined by the degree of ischemia in the affected organs. Most of the patients with early arterial stiffness nearly have no clinical symptoms. However, numerous studies have already demonstrated that arterial stiffness can lead to increased cardiovascular risk (8, 29, 37). There is a lack of sensitive and specific laboratory diagnostic methods for early arterial stiffness. cf-PWV is considered as the gold standard method for diagnosing arterial stiffness. It is advisable to measure cf-PWV to determine whether there is arterial stiffness, as well as the location according to Doppler ultrasound. According to the guidelines, cf-PWV greater than 10 m/s indicates the occurrence of arterial stiffness (1). Nevertheless, as previously mentioned, cf-PWV is not widely used in current clinical practice due to its measurement requires specialized equipment. It is important to understand the status of arterial stiffness, especially in high-risk individuals such as patients with cardiovascular and cerebrovascular diseases. ePWV is a novel index calculated based age and MBP, which was firstly proposed in 2010 to estimate the degree of arterial stiffness (38). The use of ePWV has increased awareness of the dangers of aortic stiffness and helped physicians take advantage of it in clinical practice (10, 39, 40). In the present study, we adopted the previously published equation to calculate ePWV and applied it in a high-risk population with diabetes.
The 2018 European Society of Hypertension/European Society of Cardiology (ESH/ESC) guideline for the management of hypertension recommend measuring PWV as a marker of target organ damage in order to improve cardiovascular risk prediction. In recent years, the clinical value of ePWV has been extensively investigated (3). Vishram et al. conducted a prospective study based on a large low-risk European cohort and demonstrated that ePWV can predict cardiovascular outcomes in the general population (11). In a NHANES analysis published in J Am Coll Cardiol, investigators also found increased ePWV has a strong association with cardiovascular mortality and all-cause mortality risks in general population (37). It is interesting to note that Heffernan et al. performed another study with NHANES data and showed ePWV even had a predictive value for the residual-specific mortality (41). However, the exploration of roles of ePWV in high-risk population is still needed. Arterial stiffness is an important contributor to hypertension and hypertension can further promote arterial stiffness, resulting in a vicious cycle. Vlachopoulos et al. investigated roles of ePWV in high-risk individuals from the SPRINT trial. After 3.26 years follow-up, the researchers found that ePWV was associated with all-cause mortality and cardiovascular events in patients with hypertension (29). Study of Hametner et al. showed that ePWV was not only associated with mortality, but also risks of unplanned revascularization, stroke, and myocardial infarction among patients with suspected coronary artery disease undergoing invasive angiography (42). Our study paid attention to another high-risk population with diabetes. Compared with the study based on SPRINT cohort focusing on roles of ePWV in patients with hypertension, our study (i) has substantially longer follow-up time (median 10 years vs. median 3.26 years), (ii) recruited a similar number of participants (8,916 vs. 9,361 individuals), (iii) adjusted for more extensive confounding factors, such as CCI.
Diabetes is an important cause of arterial stiffness, and it is very necessary to pay attention to ePWV of patients with diabetes. Clinical studies have shown that patients with diabetes are more likely to develop arterial stiffness and had a higher cf-PWV than people without diabetes (43–45). The molecular mechanism of arterial stiffness caused by diabetes has also been widely investigated. Zhang et al. found that diabetes can activate MMP2, MMP9, and TGFβ1/Smad2/3 pathways, leading to elevated blood pressure and arterial stiffness (46). Glucose fluctuations often occurs in patients with diabetes after meals. Another study focused on the impact of glucose fluctuations on arterial stiffness showed that glucose fluctuations aggravated aortic fibrosis by promoting oxidative stress and activating Runx2 (21). Arterial stiffness can be used as an important prognostic indicator for patients with diabetes. Therefore, we conduct this study to evaluate the prognostic value of ePWV in a large high-risk population with diabetes from NHANES survey. In the present study, the increment of ePWV is closely associated with increased all-cause and cardiovascular mortality. Our results in this high-risk population (patients with diabetes) add to the existed findings from previous studies in low- and high-risk populations (general population and patients with hypertension). Therefore, controlling arterial stiffness is very important especially for patients with diabetes.
There are several strengths of our study. First, it was adequate to provide reliable conclusion and statistical power considering the large-scale sample size included and long follow-up duration; second, the participants included in this study were from NHANES survey, reducing selection bias caused by selective inclusion of specific hospitals and health insurance system; third, follow-up and mortality information were directly obtained from NDI database, it was collected by high-quality nationwide registers, and patients were followed until death. However, several limitations of this study should be mentioned. First, cf-PWV is not available in NHANES database, therefore, the compassion of ePWV and cf-PWV on the prognostic potential needs to be further explored; second, there may exist experienced subjective bias due to the self-reported covariates from NHANES database; third, whether the conclusion in the present study based on US participants could be applicable to other populations need to be further explored in the future work.
We analyzed 8,916 adult patients with diabetes from NHANES survey and found that ePWV is associated with all-cause and cardiovascular mortality risks during a long-term follow-up. Therefore, earlier prevention against arterial stiffness is important for patients with diabetes.
The datasets presented in this study can be found in online repositories. The names of the repository/repositories and accession number(s) can be found in the article/supplementary material.
This study was approved by National Center for Health Statistics Research Ethics Review Board. The participants provided informed consent to participate in the NHANES survey. The NHANES protocol complies with the U.S. Department of Health and Human Services Policy for the Protection of Human Research Subjects. NCHS IRB/ERC Protocol number: 2011-17. Ethical review and approval were waived for this study as it solely used publicly available data for research and publication. The patients/participants provided their written informed consent to participate in this study.
SC and JZ were involved in the experiment design. LW and PC performed the data analysis. LW, YS, YX and CK wrote the manuscript. CK, YS, YX, MZ and ZL reviewed the manuscript and provided critical suggestions. All authors contributed to the article and approved the submitted version.
This research is funded by the National Natural Science Foundation of China (Grant No. 81700398, No. 81970309 and No. 81770441), the Natural Science Foundation of Jiangsu Province (Grant No. BK20191117).
We acknowledge NHANES database for providing their platforms and contributors for uploading their meaningful datasets. And we thank all participants included in our present study. LW sincerely acknowledges his fiancee Nan Zhou for her love and care in their daily life. Wish their love forever!
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fcvm.2023.1157163/full#supplementary-material.
1. Williams B. Evaluating interventions to reduce central aortic pressure, arterial stiffness and morbidity–mortality. J Hypertens. (2012) 30(Suppl):S13–8. doi: 10.1097/HJH.0b013e328353e523
2. Voicehovska JG, Bormane E, Grigane A, Moisejevs G, Moreino E, Trumpika D, et al. Association of arterial stiffness with chronic kidney disease progression and mortality. Heart Lung Circ. (2021) 30:1694–701. doi: 10.1016/j.hlc.2021.08.011
3. Williams B, Mancia G, Spiering W, Agabiti Rosei E, Azizi M, Burnier M, et al. 2018 ESC/ESH guidelines for the management of arterial hypertension. Eur Heart J. (2018) 39:3021–104. doi: 10.1093/eurheartj/ehy339
4. van Hout MJ, Dekkers IA, Lin L, Westenberg JJ, Schalij MJ, Jukema JW, et al. Estimated pulse wave velocity (ePWV) as a potential gatekeeper for MRI-assessed PWV: a linear and deep neural network based approach in 2254 participants of The Netherlands epidemiology of obesity study. Int J Cardiovasc Imaging. (2022) 38:183–93. doi: 10.1007/s10554-021-02359-0
5. Mukai Y, Nakanishi K, Daimon M, Sawada N, Hirose K, Iwama K, et al. Association of arterial properties with left ventricular morphology and function in the community. J Hypertens. (2022) 40:2423–9. doi: 10.1097/HJH.0000000000003272
6. Boutouyrie P. Estimating is not measuring: the lessons about estimated pulse wave velocity. J Am Heart Assoc. (2022) 11:e025830. doi: 10.1161/JAHA.122.025830
7. Greve SV, Laurent S, Olsen MH. Estimated pulse wave velocity calculated from age and mean arterial blood pressure. Pulse (Basel). (2017) 4:175–9. doi: 10.1159/000453073
8. Greve SV, Blicher MK, Kruger R, Sehestedt T, Gram-Kampmann E, Rasmussen S, et al. Estimated carotid-femoral pulse wave velocity has similar predictive value as measured carotid-femoral pulse wave velocity. J Hypertens. (2016) 34:1279–89. doi: 10.1097/HJH.0000000000000935
9. Turi V-R, Luca CT, Gaita D, Iurciuc S, Petre I, Iurciuc M, et al. Diagnosing arterial stiffness in pregnancy and its implications in the cardio-renal-metabolic chain. Diagnostics (Basel). (2022) 12(9):2221. doi: 10.3390/diagnostics12092221
10. Ji C, Gao J, Huang Z, Chen S, Wang G, Wu S, et al. Estimated pulse wave velocity and cardiovascular events in Chinese. Int J Cardiol Hypertens. (2020) 7:100063. doi: 10.1016/j.ijchy.2020.100063
11. Vishram-Nielsen JKK, Laurent S, Nilsson PM, Linneberg A, Sehested TSG, Greve SV, et al. Does estimated pulse wave velocity add prognostic information?: mORGAM prospective cohort project. Hypertension. (2020) 75:1420–8. doi: 10.1161/HYPERTENSIONAHA.119.14088
12. Tembely D, Henry A, Vanalderwiert L, Toussaint K, Bennasroune A, Blaise S, et al. The elastin receptor Complex: an emerging therapeutic target against age-related vascular diseases. Front Endocrinol (Lausanne). (2022) 13:815356. doi: 10.3389/fendo.2022.815356
13. Dieffenbach PB, Aravamudhan A, Fredenburgh LE, Tschumperlin DJ. The mechanobiology of vascular remodeling in the aging lung. Physiology (Bethesda). (2022) 37:28–38. doi: 10.1152/physiol.00019.2021
14. Zhang L, Li C, Wang S, Avtanski D, Hadzi-Petrushev N, Mitrokhin V, et al. Tetrahydrocurcumin-related vascular protection: an overview of the findings from animal disease models. Molecules. (2022) 27(16):5100. doi: 10.3390/molecules27165100
15. Ho L, Hossen N, Nguyen T, Vo A, Ahsan F. Epigenetic mechanisms as emerging therapeutic targets and microfluidic chips application in pulmonary arterial hypertension. Biomedicines. (2022) 10(1):170. doi: 10.3390/biomedicines10010170
16. Visentin S, Grumolato F, Nardelli GB, Di Camillo B, Grisan E, Cosmi E. Early origins of adult disease: low birth weight and vascular remodeling. Atherosclerosis. (2014) 237:391–9. doi: 10.1016/j.atherosclerosis.2014.09.027
17. García RD, Asensio JA, Perdicaro DJ, de Los Ángeles Peral M. The role of inflammation as a preponderant risk factor in cardiovascular diseases. Curr Vasc Pharmacol. (2022) 20:244–59. doi: 10.2174/1570161120666220201160038
18. Sachdeva MM. Retinal neurodegeneration in diabetes: an emerging concept in diabetic retinopathy. Curr Diab Rep. (2021) 21:65. doi: 10.1007/s11892-021-01428-x
19. Loffredo L, Violi F. Metabolic endotoxemia and arterial stiffness in diabetes. Circ Res. (2022) 131:555–7. doi: 10.1161/CIRCRESAHA.122.321702
20. Huang H, Jin J, Chen Y, Wang L, Zhong J, Chen Z, et al. Visceral fat might impact left ventricular remodeling through changes in arterial stiffness in type 2 diabetes: a cross-sectional study. Int J Cardiol. (2022) 368:78–84. doi: 10.1016/j.ijcard.2022.08.033
21. Zhang Z-Y, Wang N, Qian L-L, Miao L-F, Dang S-P, Wu Y, et al. Glucose fluctuations promote aortic fibrosis through the ROS/p38 MAPK/Runx2 signaling pathway. J Vasc Res. (2020) 57:24–33. doi: 10.1159/000503608
22. Heffernan KS, Stoner L, Meyer ML, Loprinzi PD. Association between estimated pulse wave velocity and cognitive performance in older black and white adults in NHANES. J Alzheimers Dis. (2022) 88:985–93. doi: 10.3233/JAD-220042
23. Jae SY, Heffernan KS, Kim HJ, Kunutsor SK, Fernhall B, Kurl S, et al. Impact of estimated pulse wave velocity and socioeconomic status on the risk of stroke in men: a prospective cohort study. J Hypertens. (2022) 40:1165–9. doi: 10.1097/HJH.0000000000003118
24. Chen H, Chen G, Zhang L, Wu W, Li W, Wang X, et al. Estimated pulse wave velocity can predict the incidence of new-onset atrial fibrillation: a 11-year prospective study in a Chinese population. Front Cardiovasc Med. (2022) 9:912573. doi: 10.3389/fcvm.2022.912573
25. Reider CA, Chung R-Y, Devarshi PP, Grant RW, Hazels Mitmesser S. Inadequacy of immune health nutrients: intakes in US adults, the 2005-2016 NHANES. Nutrients. (2020) 12.
26. Graubard BI, Korn EL. Modelling the sampling design in the analysis of health surveys. Stat Methods Med Res. (1996) 5:263–81. doi: 10.1177/096228029600500304
27. Li B, Chen L, Hu X, Tan T, Yang J, Bao W, et al. Association of Serum uric acid with all-cause and cardiovascular mortality in diabetes. Diabetes Care. (2022). 46(2):425–3. doi: 10.2337/dc22-1339
28. Wu L-D, Kong C-H, Shi Y, Zhang J-X, Chen S-L. Associations between novel anthropometric measures and the prevalence of hypertension among 45,853 adults: a cross-sectional study. Front Cardiovasc Med. (2022) 9:1050654. doi: 10.3389/fcvm.2022.1050654
29. Vlachopoulos C, Terentes-Printzios D, Laurent S, Nilsson PM, Protogerou AD, Aznaouridis K, et al. Association of estimated pulse wave velocity with survival: a secondary analysis of SPRINT. JAMA Netw Open. (2019) 2:e1912831. doi: 10.1001/jamanetworkopen.2019.12831
30. Laugesen E, Olesen KKW, Peters CD, Buus NH, Maeng M, Botker HE, et al. Estimated pulse wave velocity is associated with all-cause mortality during 8.5 years follow-up in patients undergoing elective coronary angiography. J Am Heart Assoc. (2022) 11:e025173. doi: 10.1161/JAHA.121.025173
31. Fulgoni VL, Drewnowski A. No association between low-calorie sweetener (LCS) use and overall cancer risk in the nationally representative database in the US: analyses of NHANES 1988-2018 data and 2019 public-use linked mortality files. Nutrients. (2022) 14(23):4957. doi: 10.3390/nu14234957
32. Zhao H, Pan Y, Wang C, Guo Y, Yao N, Wang H, et al. The effects of metal exposures on charlson comorbidity Index using zero-inflated negative binomial regression model: NHANES 2011-2016. Biol Trace Elem Res. (2021) 199:2104–11. doi: 10.1007/s12011-020-02331-4
33. AlQobaly L, Abed H, Alsahafi Y, Sabbah W, Hakeem FF. Does smoking explain the association between use of e-cigarettes and self-reported periodontal disease? J Dent. (2022) 122:104164. doi: 10.1016/j.jdent.2022.104164
34. Chevli PA, Ahmad MI, Jogu HR, Dutta A, Anees MA, Sunkara PR, et al. Electrocardiographic subclinical myocardial injury and alcohol consumption: a cross-sectional analysis of data from the third national health and nutrition examination survey. Am J Cardiovasc Dis. (2018) 8(5):58–65. PMID:PMC6334197
35. Ma J, Chen X. Advances in pathogenesis and treatment of essential hypertension. Front Cardiovasc Med. (2022) 9:1003852. doi: 10.3389/fcvm.2022.1003852
36. Agbaje AO. Arterial stiffness precedes hypertension and metabolic risks in youth: a review. J Hypertens. (2022) 40:1887–96. doi: 10.1097/HJH.0000000000003239
37. Heffernan KS, Jae SY, Loprinzi PD. Association between estimated pulse wave velocity and mortality in U.S. adults. J Am Coll Cardiol. (2020) 75:1862–4. doi: 10.1016/j.jacc.2020.02.035
38. Collaboration RVfAS. Determinants of pulse wave velocity in healthy people and in the presence of cardiovascular risk factors: “establishing normal and reference values”. Eur Heart J. (2010) 31:2338–50. doi: 10.1093/eurheartj/ehq165
39. Chen H, Wu W, Fang W, Chen Z, Yan X, Chen Y, et al. Does an increase in estimated pulse wave velocity increase the incidence of hypertension? J Hypertens. (2021) 39:2388–94. doi: 10.1097/HJH.0000000000002945
40. Stamatelopoulos K, Georgiopoulos G, Baker KF, Tiseo G, Delialis D, Lazaridis C, et al. Estimated pulse wave velocity improves risk stratification for all-cause mortality in patients with COVID-19. Sci Rep. (2021) 11:20239. doi: 10.1038/s41598-021-99050-0
41. Heffernan KS, Jae SY, Loprinzi PD. Estimated pulse wave velocity is associated with residual-specific mortality: findings from the national health and nutrition examination survey. J Hypertens. (2021) 39:698–702. doi: 10.1097/HJH.0000000000002691
42. Hametner B, Wassertheurer S, Mayer CC, Danninger K, Binder RK, Weber T. Aortic pulse wave velocity predicts cardiovascular events and mortality in patients undergoing coronary angiography: a comparison of invasive measurements and noninvasive estimates. Hypertension. (2021) 77:571–81. doi: 10.1161/HYPERTENSIONAHA.120.15336
43. Gentilin A, Moghetti P, Cevese A, Mattioli AV, Schena F, Tarperi C. Circadian and sex differences in carotid-femoral pulse wave velocity in young individuals and elderly with and without type 2 diabetes. Front Cardiovasc Med. (2022) 9:952621. doi: 10.3389/fcvm.2022.952621
44. Serra C, Sestu A, Murru V, Greco G, Vacca M, Scuteri A. Diabetes affects the relationship between heart rate variability and arterial stiffness in a gender-specific manner. J Clin Med. (2022) 11(17):4937. doi: 10.3390/jcm11174937
45. Cohen JB, Mitchell GF, Gill D, Burgess S, Rahman M, Hanff TC, et al. Arterial stiffness and diabetes risk in framingham heart study and UK biobank. Circ Res. (2022) 131:545–54. doi: 10.1161/CIRCRESAHA.122.320796
Keywords: estimated pulse wave velocity, diabetes, arterial stiffness, NHANES, allcause mortality, cardiovascular mortality
Citation: Wu L-D, Chu P, Kong C-H, Shi Y, Zhu M-H, Xia Y-Y, Li Z, Zhang J-X and Chen S-L (2023) Estimated pulse wave velocity is associated with all-cause mortality and cardiovascular mortality among adults with diabetes. Front. Cardiovasc. Med. 10:1157163. doi: 10.3389/fcvm.2023.1157163
Received: 2 February 2023; Accepted: 20 March 2023;
Published: 17 April 2023.
Edited by:
Xiaofeng Yang, Temple University, United StatesReviewed by:
Francesco Bianco, Azienda Ospedaliero Universitaria Ospedali Riuniti, Italy© 2023 Wu, Chu, Kong, Shi, Zhu, Xia, Li, Zhang and Chen. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Shao-Liang Chen MTU4NTA3NzA3MzlAMTI2LmNvbQ== Jun-Xia Zhang emhhbmdqdW5zaGlhQG5qbXUuZWR1LmNu
†These authors have contributed equally to this work and share first authorship
Specialty Section: This article was submitted to Cardiovascular Pharmacology and Drug Discovery, a section of the journal Frontiers in Cardiovascular Medicine
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.