
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Cardiovasc. Med., 06 April 2023
Sec. Cardiac Rhythmology
Volume 10 - 2023 | https://doi.org/10.3389/fcvm.2023.1140276
 Diana Mojón-Álvarez1,2
Diana Mojón-Álvarez1,2 Andrea Izquierdo1,2
Andrea Izquierdo1,2 Héctor Cubero-Gallego1,3
Héctor Cubero-Gallego1,3 Alicia Calvo-Fernández1,2,4
Alicia Calvo-Fernández1,2,4 Jaume Marrugat5,6Silvia Pérez-Fernández7Paula Cabero1Claudia Solà-Richarte1Cristina Soler1Núria Farré1,2,3,4
Jaume Marrugat5,6Silvia Pérez-Fernández7Paula Cabero1Claudia Solà-Richarte1Cristina Soler1Núria Farré1,2,3,4 Beatriz Vaquerizo1,2,3,4,5*
Beatriz Vaquerizo1,2,3,4,5*
Background and objective: Prolonged QTc interval on admission and a higher risk of death in SARS-CoV-2 patients have been reported. The long-term clinical impact of prolonged QTc interval is unknown. This study examined the relationship in COVID-19 survivors of a prolonged QTc on admission with long-term adverse events, changes in QTc duration and its impact on 1-year prognosis, and factors associated with a prolonged QTc at follow-up.
Methods: We conducted a single-center prospective cohort study of 523 SARS-CoV-2-positive patients who were alive on discharge. An electrocardiogram was taken on these patients within the first 48 h after diagnosis and before the administration of any medication with a known effect on QT interval and repeated in 421 patients 7 months after discharge. Mortality, hospital readmission, and new arrhythmia rates 1 year after discharge were reviewed.
Results: Thirty-one (6.3%) survivors had a baseline prolonged QTc. They were older, had more cardiovascular risk factors, cardiac disease, and comorbidities, and higher levels of terminal pro-brain natriuretic peptide. There was no relationship between prolonged QTc on admission and the 1-year endpoint (9.8% vs. 5.5%, p = 0.212). In 84% of survivors with prolonged baseline QTc, it normalized at 7.9 ± 2.2 months. Of the survivors, 2.4% had prolonged QTc at follow-up, and this was independently associated with obesity, ischemic cardiomyopathy, chronic obstructive pulmonary disease, and cancer. Prolonged baseline QTc was not independently associated with the composite adverse event at 1 year.
Conclusions: Prolonged QTc in the acute phase normalized in most COVID-19 survivors and had no clinical long-term impact. Prolonged QTc at follow-up was related to the presence of obesity and previously acquired chronic diseases and was not related to 1-year prognosis.
The world has been experiencing a pandemic since December 2019 from a novel coronavirus, responsible for the Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2), which has caused great morbidity and mortality throughout the world (1). Although the effects of coronavirus disease 2019 (COVID-19) are predominantly respiratory, some cardiovascular effects, like nonspecific myocardial damage, heart failure, QTc prolongation, and arrhythmias have been described (2–4). Some studies have reported an association between QTc prolongation on admission and higher mortality risk in hospitalized COVID-19 patients (5, 6). A significant relationship between systemic inflammation, QTc prolongation, and arrhythmias during the acute phase of infections has been demonstrated in both COVID and non-COVID-19 patients (7, 8). The characteristic systemic inflammation caused by COVID-19 disease (“cytokine storm”) is likely a crucial factor in QTc prolongation by several mechanisms (9–11).
There is little information on the long-term consequences of COVID-19 in patients after hospital discharge. Most studies have been limited to hospitalized individuals, and all had a short duration of follow-up and narrow selection of cardiovascular outcomes (12–14). Recently, a large study showed that, beyond the first 30 days of infection, people with COVID-19 exhibited increased risk for and 12-month burden of cardiovascular diseases (15).
Considering the prognostic role of a prolonged QTc at hospital admission and availability of electrocardiogram (ECG) in any healthcare setting, ECG could be a potential tool to identify high-risk patients. Thus, we aimed to describe the long-term impact of a prolonged QTc on admission in COVID-19 survivors and identify potential risk factors related to a prolonged QTc at follow-up.
A single-center (Hospital del Mar—Barcelona, Spain) prospective cohort study of consecutive patients hospitalized with COVID was conducted. The acute impact of prolonged QTc interval on admission in SARS-CoV-2 patients has been published, and trial design and results have previously been described in detail (5). In brief, our initial cohort included a total of 623 consecutive patients with polymerase chain reaction test (PCR) positive to SARS-CoV-2 recruited from 27 February to 7 April 2020. An ECG was taken on these patients within the first 48 h after diagnosis and before the administration of any medication with a known effect on QT interval. Baseline ECG was defined as the ECG taken within the first 48 h after laboratory-confirmed COVID-19 diagnosis and before the administration of any medication with a known effect on the QT interval. At the time of the pandemic, our institutional protocol recommended an ECG before starting any medication with a known effect on QT interval. Prolonged QTc was defined as a QTc≥480 ms (16, 17). From this initial cohort, patients who were alive upon discharge were included in this second study. Five hundred and forty-two patients with a baseline ECG were discharged alive during the study period. Nineteen patients were lost to follow-up. Therefore, the final sample was 523 patients with clinical follow-up. Of those, 80.5% consented to a repeat ECG at 7-month follow-up (Figure 1).
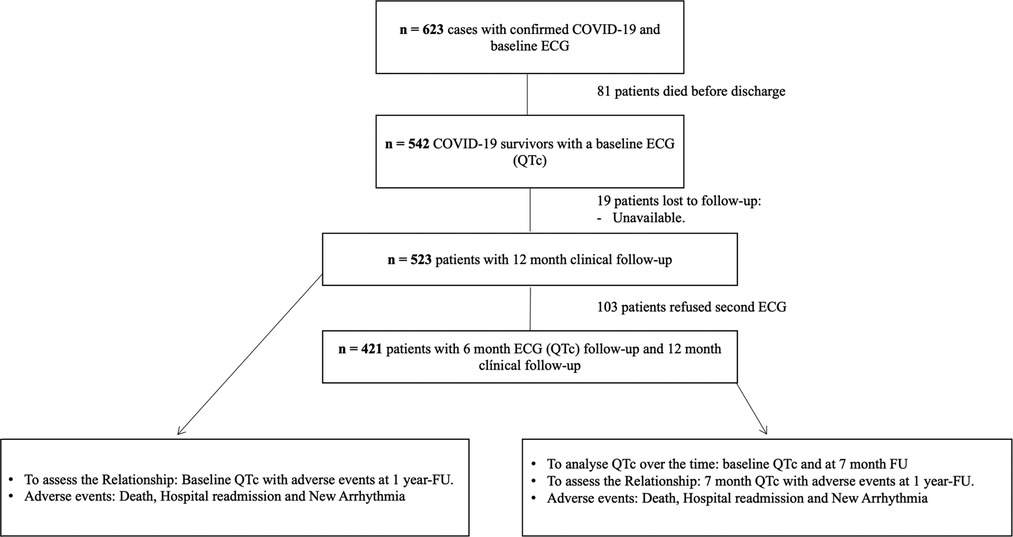
Figure 1. Flowchart of patient inclusion.
Demographic characteristics (age and sex), comorbidities, laboratory parameters, chest radiography, electrocardiographic findings, treatments, complications, and outcomes were collected prospectively using an electronic data capture system. Patients had an in-person follow-up for repeat ECG and blood test analysis at 7 months. One-year follow-up was performed by telephone contact and through electronic medical records.
This study was performed according to the principles of the Declaration of Helsinki, ISO14155, and clinical practice guidelines. The study protocol was approved by the Institutional Ethics Committee and the hospital research committee. Informed consent was obtained from all patients.
Standard resting 12-lead ECG was obtained in all patients using the Philips PageWriter TC30 Cardiograph (Koninklijke Philips, Eindhoven, Netherlands). Two ECGs were obtained. The first one was performed within the first 48 h after laboratory-confirmed COVID-19 diagnosis. We considered 6 months as the time enough to normalize the QTc interval if its prolongation was related with SARS-CoV-2 infection. The second ECG was performed on the COVID-19 survivors who agreed to come to the hospital after discharge. For organizational reasons, we started our follow-up at 5.7 months, with a mean follow-up of 7.9 months.
The following ECG parameters were calculated: QRS interval (ms), QT interval, and QTc that were automatically calculated as the time from the start of the Q wave to the end of the T wave and corrected for heart rate by the Bazett formula (QTc) in ECG I and ECG II. All the measures were manually revised and checked by trained researchers. In the setting of a broad QRS complex, we used the Bogossian formula to correct the QT. Prolonged QTc was defined as a QTc ≥480 ms (17). A baseline QTc <480 ms and QTc≥480 at 7 months was named new prolonged QTc at follow-up. A baseline QTc≥480 ms that continued to be prolonged (QTc ≥480 ms) at 7 months was named persistent prolonged QTc at follow-up. A baseline QTc ≥480 ms that progressed to normal (QTc < 480 ms) at 7 months was named normalized QTc at follow-up.
The primary endpoint was a composite of death, new episode of arrhythmia, or all-cause hospital readmission at 1 year from initial hospital admission for COVID-19. The secondary endpoints were to describe the temporal evolution of the QTc interval and its relationship with prognosis and factors associated with QTc changes over time.
A new arrhythmia episode was defined as any new ECG-confirmed diagnosis of supraventricular or ventricular arrhythmia that was not present on the baseline ECG. Obesity was defined as a body mass index (BMI) over 30 kg/m2.
Continuous variables were expressed as the mean and SD except when not following the normal distribution, in which case they were expressed as the median and 25–75th percentile. Normal distribution was assessed using the Shapiro–Wilk test and normal Q–Q plot. Categorical variables were expressed as number and percentage. Differences between groups were assessed using Student's t-test or Mann–Whitney U test, as appropriate, for continuous variables and the Chi-square test for categorical variables. Differences between baseline and 7-month QTc were assessed using paired Student's t-test for continuous variables and the McNemar test for categorical variables. Kaplan–Meier survival curves for the composite endpoints were plotted, and the log-rank test was used to assess differences between groups of QTc at follow-up. Cox proportional hazard models were used to explore the risk factors associated with the occurrence of the composite endpoint, and logistic regression models were applied for prolonged QTc. The covariates entered in the model were chosen according to their clinical significance and whether the variable was statistically significant at univariate analysis. All statistical analyses were performed with R version 3.6.1 (R Foundation for Statistical Computing, Vienna, Austria). Statistical significance was set at p ≤ 0.05.
A total of 523 patients were followed up over a mean of 12.90 ± 1.68 months after their initial hospital admission for COVID-19. Baseline characteristics are described in Table 1.

Table 1. Comparison of baseline characteristics between hospitalized COVID-19 survivors with and without prolonged QTc on admission.
Patients discharged alive with baseline prolonged QTc were older and had more cardiovascular risk factors, cardiac disease (arrhythmias, coronary artery disease, significant valve heart disease), and comorbidities [previous stroke, chronic obstruction pulmonary disease (COPD), and chronic kidney disease]. Moreover, they had higher C-reactive protein levels, lactate dehydrogenase, procalcitonin, and N-terminal pro-brain natriuretic peptide (NT-proBNP), and lower estimated glomerular filtration rate.
In COVID-19 survivors, the composite primary endpoint (mortality, hospital readmission, or new arrhythmia) at 1-year follow-up was 10%, primarily due to noncardiac readmission (9.74%). The mortality rate was 0.95%, and only two patients (0.48%) had new atrial fibrillation (AF).
There was no relationship between prolonged QTc (at admission or follow-up) and the composite endpoint at 1 year (Tables 2 and 3 and <Figures 2A, B).
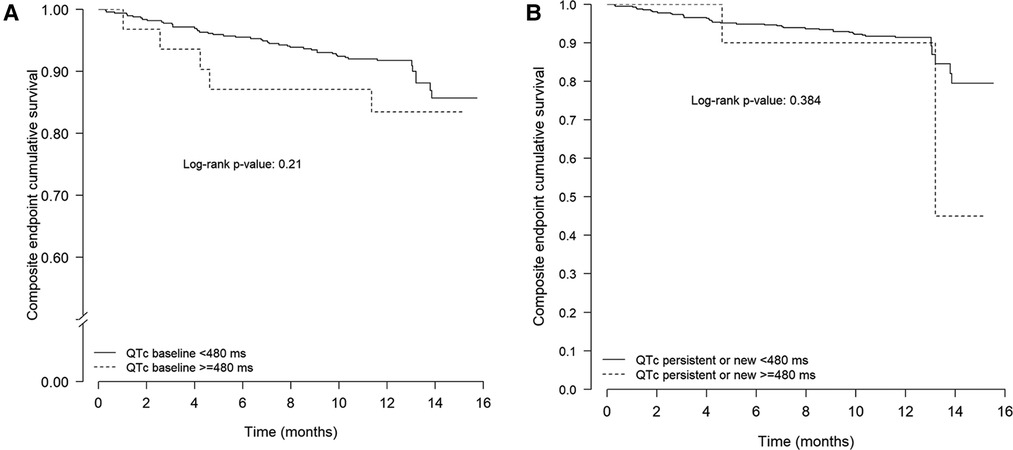
Figure 2. Kaplan–Meier curves for the composite endpoint (death or hospital readmission or new arrhythmia) in 421 COVID-19 survivors according to the presence or absence of persistent or new prolonged QTc (A) or persistent or new prolonged QTc at 7 months (B). COVID-19, coronavirus disease 2019.
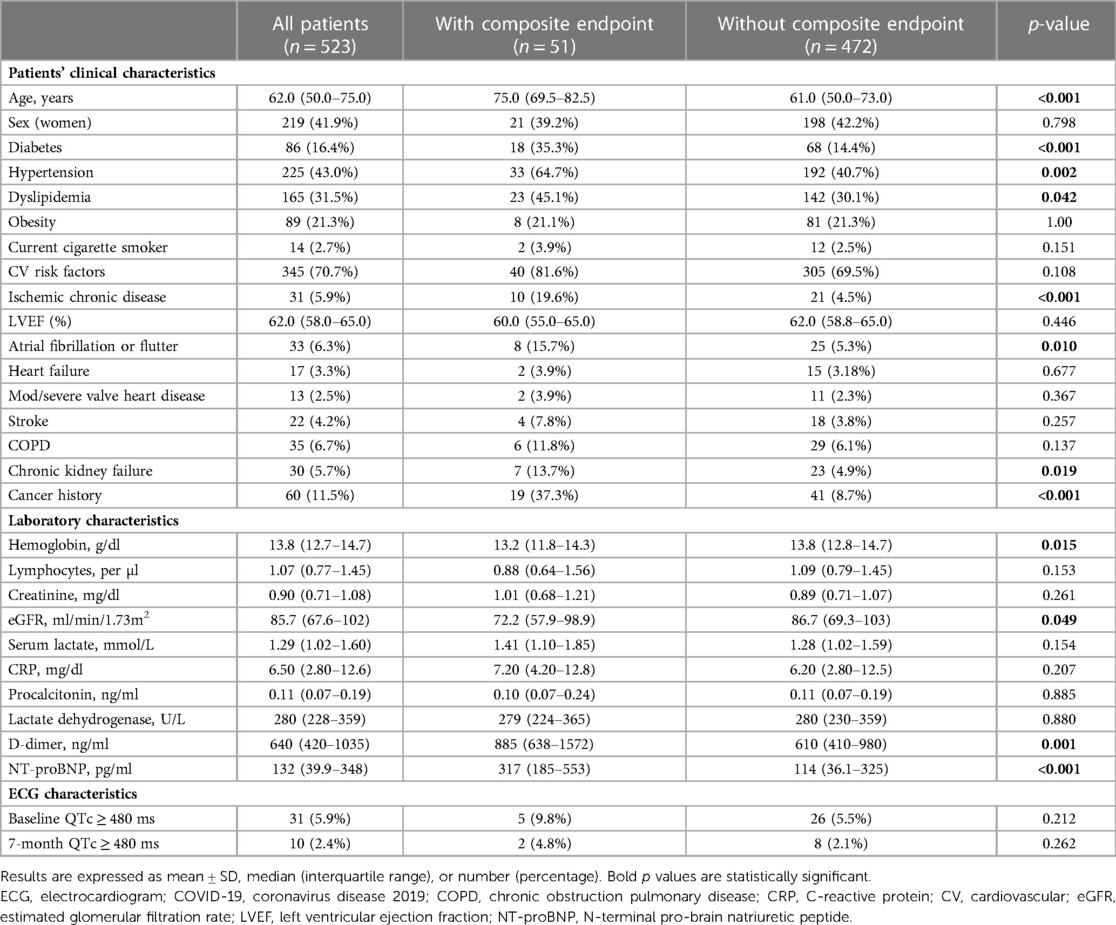
Table 2. Comparison of clinical, laboratory, and ECG characteristics between COVID-19 survivors with and without the composite endpoint at 1 year after hospital discharge.
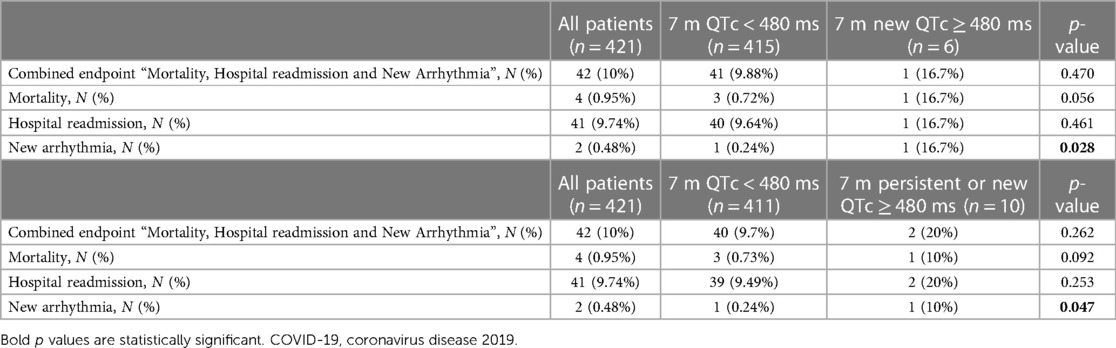
Table 3. Adverse events at 1 year after hospital discharge in COVID-19 survivors with and without prolonged QTc at 7 months follow-up.
Independent predictors of the composite endpoint are presented in Table 4. Age, diabetes mellitus, previous coronary artery disease, and cancer were independently related to the composite endpoint at 1 year, whereas prolonged QT was not {hazard ratio (HR) 0.86 [95% confidence interval (CI) 0.231–3.203], p = 0.822}.
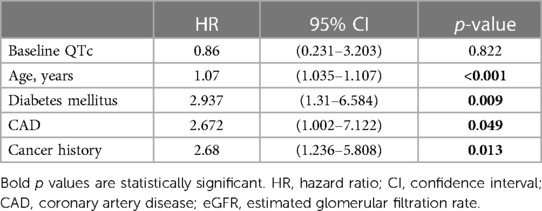
Table 4. Independent predictors of the composite endpoint (death, hospital readmission due to any cause, new arrhythmia) at 1 year after hospital discharge.
Although the initial protocol established that follow-up would be done at 6 months after the index hospitalization, several COVID waves and in-person visit limitations made that impossible for some patients. Thus, the mean follow-up was 7.9 ± 2.2 months. A subgroup of 421 patients who consented to a repeat ECG were included in this analysis. In this group, 25 (5.9%) patients had a prolonged QTc interval on admission; remarkably, it normalized in most of them (84%) at follow-up. Only 2.4% (10 patients) had a prolonged QTc at follow-up; 6 cases had a new prolonged QTc (from normal after initial admission to prolonged QTc at follow-up) and 4 had persistent QTs (already prolonged at baseline and continued to be prolonged at follow-up) (Table 5).
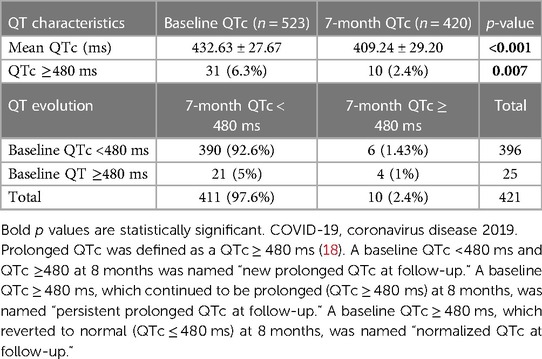
Table 5. QTc interval analysis at hospital admission and 7 months after COVID-19 survivors hospital discharge.
Supplementary Table S1 describes the baseline characteristics, blood tests, and treatment of patients with QTc prolongation at follow-up.
The independent predictors of QTc prolongation at follow-up were the presence of obesity, coronary artery disease, chronic obstructive pulmonary disease, and cancer (Table 6).
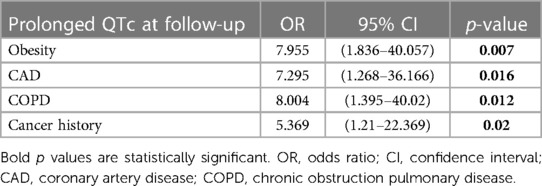
Table 6. Independent predictors of prolonged QT at follow-up.
At 1-year follow-up, only new atrial fibrillation occurred more often in patients with new prolonged QTc at follow-up (16.7% vs. 0.24%, p = 0.028) (Table 3).
Our study is a prospective registry of 523 patients with the aim of evaluating the natural history of QTc interval and its clinical impact on 1-year prognosis in COVID-19 survivors. Results showed that a prolonged QTc on admission had no clinical impact on the long-term follow-up of patients who survived hospitalization due to COVID-19. It normalized in most patients at 7 months after hospital discharge. Few patients demonstrated a new prolonged QTc at follow-up, and it was not associated with inflammatory markers or adverse events. Patients with prolonged QTc at follow-up had higher rates of atrial fibrillation at 1-year follow-up. The presence of obesity, COPD, coronary artery disease, and cancer were independently related to prolonged QTc at follow-up.
QTc interval prolongation occurs when a significant proportion of cells in the ventricular myocardium experience a reduction of outward repolarizing currents or an increase of inward currents, creating a prolongation of the action potential (18). This condition is characterized by both QTc prolongation and T wave abnormalities. The congenital form of long QTc syndrome is uncommon. However, acquired QTc prolongation is much more common and linked to different issues, especially in sick and hospitalized patients (19, 20).
The effect of acute SARS-CoV-2 or other acute infections on QTc prolongation and its relationship with a worse short-term prognosis is well established (5, 20, 21). However, little is known about the mid- and long-term QTc evolution after acute infection and its implications at follow-up. In a case series of four patients, Beer et al. reported transient marked QTc prolongation and ventricular arrhythmias in the setting of acute infection and inflammation. Prolonged QTc normalized after patients overcame the infection, but the medium- to long-term prognosis and complications were not explored (22). In our study, most of the COVID-19 survivors with a prolonged QTc interval on admission demonstrated normalization on the control ECG at follow-up. We did not observe a relationship between prolonged QTc at admission and the composite endpoint at 1 year. Assuming that QTc prolongation is a reflection of severity, the mechanisms that caused the QTc prolongation in patients who recovered from an acute infection would be at least partially resolved. The logical conclusion under this assumption would be that the basal QTc would not have a long-term influence on the prognosis of our patients, as we have reported in our study.
A significant relationship between systemic inflammation and QTc prolongation during the acute phase of infection has been demonstrated in COVID-19 and non-COVID-19 patients (6, 7, 22, 23). A recent study in patients with active severe COVID-19 showed that QTc was significantly prolonged if IL-6 levels were high, and it rapidly normalized in correlation with decrease in IL-6 (24).
In addition, some conditions have been associated with acquired prolonged QTc in outpatients. Previous reports have shown systemic inflammation and autoimmune diseases as factors that are crucially involved in ventricular repolarization (18). An independent association between C-reactive protein levels and QTc prolongation has been shown, even in apparently healthy subjects or in noninflammatory heart diseases like hypertension, coronary artery disease, or Takotsubo cardiomyopathy (25–27).
Given the evidence, if QTc alterations might be related to a pro-inflammatory state, it seems logical to think that overcoming acute coronavirus disease will lead to QTc normalization. Accordingly, in our study, most of the COVID-19 survivors with a prolonged QTc interval on admission demonstrated normalization in the control ECG at follow-up. It seems that abnormal acute ventricular repolarization observed in the setting of COVID-19 infection self-resolved as the viral illness course remitted. Banai et al. carried out a study in which prolonged QTc in hospitalized COVID-19 patients was associated with disease severity, myocardial injury, and 1-year mortality (28). However, they did not exclude patients who had died from COVID-19 in their analysis. In our study, we analyzed only patients who had survived SARS-CoV-2 infection and hospital admission, suggesting that our patients had completely overcome COVID-19.
In our study, the independent predictors of prolonged QTc at follow-up in COVID-19 survivors were the presence of obesity, previous coronary artery disease, COPD, and cancer. Patients affected by these diseases likely have some degree of endothelial dysfunction and chronic inflammation related to an increased level of circulating cytokines. The putative cytokine-mediated mechanisms are complex and include direct actions on cardiomyocyte ion channel function and indirect effects resulting from sympathetic activation (29).
As explained above, the presence of chronic diseases, such as obesity, COPD, coronary artery disease, and cancer, was related to prolonged QTc at follow-up. However, it is well known that these factors are also predictors of AF in the general population (30, 31). Interestingly, we observed a higher rate of new atrial fibrillation in patients with new prolonged QTc at follow-up (16.7% vs. 0.24%, p = 0.028). However, it was not significant in the multivariate regression model. Several studies have shown that individuals with a prolonged QTc interval have a high risk of developing atrial fibrillation (32, 33), although the pathophysiology of the ventricular action potential and its relationship with AF are not fully understood. Furthermore, a recent study has described a higher incidence of atrial fibrillation at 12-month follow-up in COVID-19 survivors (15).
It is possible that the QT interval was a marker of other AF risk factors, which might explain why prolonged QT was not found as an independent predictor in the multivariate regression model.
It is important to note that potential medication with a known effect on the QT interval was registered in the acute phase and at follow-up. In the acute phase, we only included patients in whom ECG was taken within the first 48 h after laboratory-confirmed COVID-19 diagnosis and before the administration of any medication with a known effect on the QT interval. We did not find any significant relation between patient’s treatment and prolonged QTc at follow-up (Supplementary Table S1).
Persistent COVID, i.e., persistent symptoms and late organ damage in patients who have suffered from COVID-19, is an entity that affects a substantial percentage of post-COVID-19 patients. Studies are being carried out to learn more about this syndrome, since it diminishes patients’ quality of life. Pulmonary sequelae have been established (34), but studies have also shown that cardiac sequelae could be a relevant topic. In a systematic review about cardiac sequelae after COVID-19, Ramadan et al. noted that survivors had a higher chance of developing heart failure, arrhythmias, and myocardial infarction (35). Considering the above arguments, ECG could be a widely available, safe, and cheap tool that could help detect patients at risk of developing arrhythmias or other cardiovascular diseases. However, we have not been able to prove the ability of QTc to predict long-term adverse events in COVID-19 survivors.
Our study has some limitations. The study was performed in a single center and thus may not have been representative of the overall population. The small number of patients with prolonged QTc at follow-up limited the statistical power and number of conclusions that could be extracted. A more extended follow-up to collect more data would be very helpful. Moreover, we did not collect data on electrolyte levels in our patients, and this could be a limitation in interpreting the results of our study. We were not able to monitor our patients with 24 h Holter monitoring or other kinds of cardiac-rhythm monitoring devices during follow-up. We only collected clinical episodes of arrhythmia, and we did not register subclinical arrhythmic events, which could have been a limitation of our study.
Acute prolonged QTc observed in the setting of COVID-19 infection self-resolved in most COVID-19 survivors at 6 months after hospital discharge. Prolonged QTc on admission had no clinical impact on the long-term follow-up. QTc prolongation in COVID-19 survivors was not related to adverse events at 1 year. Notably, few patients showed QTc prolongation at follow-up; QTc prolongation was independently related to obesity and chronic disease.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
The studies involving human participants were reviewed and approved by Institutional Ethics Committee and the hospital research committee (CEIm 2020/9178). The patients/participants provided their written informed consent to participate in this study.
DM-Á, BV, and NF conceived and designed the study. DM-Á, AI, PC, CS-R, and CS contributed to patient recruitment and data acquisition. DM-Á, BV, and SP-F contributed to data analysis. DM-Á, HC-G, AC-F, JM, NF, and BV made important intellectual contributions and actively participated in the interpretation of the data. DM-Á and BV wrote the paper. All authors contributed to the article and approved the submitted version.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fcvm.2023.1140276/full#supplementary-material.
ECG, electrocardiogram; COVID-19, coronavirus disease 2019; SARS-CoV-2, severe acute respiratory syndrome coronavirus 2.
1. Huang C, Wang Y, Li X, Ren L, Zhao J, Hu Y, et al. Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. Lancet. (2020) 395(10223):497–506. doi: 10.1016/S0140-6736(20)30183-5
2. Zheng YY, Ma YT, Zhang JY, Xie X. COVID-19 and the cardiovascular system. Nat Rev Cardiol. (2020) 17(5):259–60. doi: 10.1038/s41569-020-0360-5
3. Kochi AN, Tagliari AP, Forleo GB, Fassini GM, Tondo C. Cardiac and arrhythmic complications in patients with COVID-19. J Cardiovasc Electrophysiol. (2020) 31(5):1003–8. doi: 10.1111/jce.14479
4. Calvo-Fernández A, Izquierdo A, Subirana I, Farré N, Vila J, Durán X, et al. Marcadores de daño miocárdico en la predicción del pronóstico a corto plazo de los pacientes con COVID-19. Revista Española de Cardiología. (2021) 74(7):576–83. doi: 10.1016/j.recesp.2020.09.017
5. Farré N, Mojón D, Llagostera M, Belarte-Tornero LC, Calvo-Fernández A, Vallés E, et al. Prolonged QT interval in SARS-CoV-2 infection: prevalence and prognosis. JCM. (2020) 9(9):2712. doi: 10.3390/jcm9092712
6. Vicentini A, Masiello L, D’Amore S, Baldi E, Ghio S, Savastano S, et al. QTc interval and mortality in a population of SARS-2-CoV infected patients. Circ: Arrhythmia and Electrophysiol. (2020) 13(11):e008890. doi: 10.1161/CIRCEP.120.008890
7. Santoro F, Monitillo F, Raimondo P, Lopizzo A, Brindicci G, Gilio M, et al. QTc interval prolongation and life-threatening arrhythmias during hospitalization in patients with coronavirus disease 2019 (COVID-19): results from a multicenter prospective registry. Clin Infect Dis. (2021) 73(11):e4031–8. doi: 10.1093/cid/ciaa1578
8. Lazzerini PE, Acampa M, Laghi-Pasini F, Bertolozzi I, Finizola F, Vanni F, et al. Cardiac arrest risk during acute infections: systemic inflammation directly prolongs QTc interval via cytokine-mediated effects on potassium channel expression. Circ: Arrhythmia and Electrophysiol. (2020) 13(8):e008627. doi: 10.1161/CIRCEP.120.008627
9. Lazzerini PE, Laghi-Pasini F, Bertolozzi I, Morozzi G, Lorenzini S, Simpatico A, et al. Systemic inflammation as a novel QT-prolonging risk factor in patients with torsades de pointes. Heart. (2017) 103(22):1821–9. doi: 10.1136/heartjnl-2016-311079
10. Lazzerini PE, Capecchi PL, Laghi-Pasini F. Systemic inflammation and arrhythmic risk: lessons from rheumatoid arthritis. Eur Heart J. (2016) 38(22):1717–27. doi: 10.1093/eurheartj/ehw208
11. Wu KC, Zhang L, Haberlen SA, Ashikaga H, Brown TT, Budoff MJ, et al. Predictors of electrocardiographic QT interval prolongation in men with HIV. Heart. (2019) 105(7):559–65. doi: 10.1136/heartjnl-2018-313667
12. Izquierdo A, Mojón D, Bardají A, Carrasquer A, Calvo-Fernández A, Carreras-Mora J, et al. Myocardial injury as a prognostic factor in mid- and long-term follow-up of COVID-19 survivors. JCM. (2021) 10(24):5900. doi: 10.3390/jcm10245900
13. Huang C, Huang L, Wang Y, Li X, Ren L, Gu X, et al. 6-month consequences of COVID-19 in patients discharged from hospital: a cohort study. Lancet. (2021) 397(10270):220–32. doi: 10.1016/S0140-6736(20)32656-8
14. Carfì A, Bernabei R, Landi F, for the Gemelli Against COVID-19 Post-Acute Care Study Group. Persistent symptoms in patients after acute COVID-19. JAMA. (2020) 324(6):603. doi: 10.1001/jama.2020.12603
15. Xie Y, Xu E, Bowe B, Al-Aly Z. Long-term cardiovascular outcomes of COVID-19. Nat Med. (2022) 28(3):583–90. doi: 10.1038/s41591-022-01689-3
16. Zeppenfeld K, Tfelt-Hansen J, de Riva M, Winkel BG, Behr ER, Blom NA, et al. 2022 ESC guidelines for the management of patients with ventricular arrhythmias and the prevention of sudden cardiac death. Eur Heart J. (2022) 43(40):3997–4126. doi: 10.1093/eurheartj/ehac262
17. Priori SG, Blomström-Lundqvist C, Mazzanti A, Blom N, Borggrefe M, Camm J, et al. 2015 ESC guidelines for the management of patients with ventricular arrhythmias and the prevention of sudden cardiac death: the task force for the management of patients with ventricular arrhythmias and the prevention of sudden cardiac death of the European Society of Cardiology (ESC) endorsed by: Association for European Paediatric and Congenital Cardiology (AEPC). Eur Heart J. (2015) 36(41):2793–867. doi: 10.1093/eurheartj/ehv316
18. Antzelevitch C. Arrhythmogenic mechanisms of QT prolonging drugs: is QT prolongation really the problem? J Electrocardiol. (2004) 37:15–24. doi: 10.1016/j.jelectrocard.2004.08.004
19. Lazzerini PE, Capecchi PL, Laghi-Pasini F. Long QT syndrome: an emerging role for inflammation and immunity. Front Cardiovasc Med. (2015) 2:26. doi: 10.3389/fcvm.2015.00026
20. Yu H, Zhang L, Liu J, Liu Y, Kowey PR, Zhang Y, et al. Acquired long QT syndrome in hospitalized patients. Heart Rhythm. (2017) 14(7):974–8. doi: 10.1016/j.hrthm.2017.03.014
21. Bergamaschi L, D’Angelo EC, Paolisso P, Toniolo S, Fabrizio M, Angeli F, et al. The value of ECG changes in risk stratification of COVID-19 patients. Ann Noninvasive Electrocardiol. (2021) 26(3):e12815. doi: 10.1111/anec.12815
22. Beer D, Isakadze N, McClellan R, Calkins H, Barth AS. Acquired long QT and ventricular arrhythmias in the setting of acute inflammation. JACC Case Rep. (2021) 3(8):1103–7. doi: 10.1016/j.jaccas.2021.04.034
23. Isakadze N, Engels MC, Beer D, McClellan R, Yanek LR, Mondaloo B, et al. C-reactive protein elevation is associated with QTc interval prolongation in patients hospitalized with COVID-19. Front Cardiovasc Med. (2022) 9:866146. doi: 10.3389/fcvm.2022.866146
24. Lazzerini PE, Accioli R, Acampa M, Zhang WH, Verrengia D, Cartocci A, et al. Interleukin-6 elevation is a key pathogenic factor underlying COVID-19-associated heart rate-corrected QT interval prolongation. Front Cardiovasc Med. (2022) 9:893681. doi: 10.3389/fcvm.2022.893681
25. Panoulas VF, Toms TE, Douglas KMJ, Sandoo A, Metsios GS, Stavropoulos-Kalinoglou A, et al. Prolonged QTc interval predicts all-cause mortality in patients with rheumatoid arthritis: an association driven by high inflammatory burden. Rheumatology. (2014) 53(1):131–7. doi: 10.1093/rheumatology/ket338
26. Haensel A, Mills PJ, Nelesen RA, Ziegler MG, Dimsdale JE. The relationship between heart rate variability and inflammatory markers in cardiovascular diseases. Psychoneuroendocrinology. (2008) 33(10):1305–12. doi: 10.1016/j.psyneuen.2008.08.007
27. Song BG, Chung SM, Kim SH, Kim HJ, Kang GH, Park YH. The QT prolongation and clinical features in patients with Takotsubo cardiomyopathy: experiences of two tertiary cardiovascular centers. Anadolu Kardiyol Derg. (2014) 14(2):162–9. doi: 10.5152/akd.2013.4745
28. Banai A, Szekely Y, Lupu L, Borohovitz A, Levi E, Ghantous E, et al. QT Interval prolongation is a novel predictor of 1-year mortality in patients with COVID-19 infection. Front Cardiovasc Med. (2022) 9:869089. doi: 10.3389/fcvm.2022.869089
29. Kobayashi H, Kobayashi Y, Yokoe I, Kitamura N, Nishiwaki A, Takei M, et al. Heart rate–corrected QT interval duration in rheumatoid arthritis and its reduction with treatment with the interleukin 6 inhibitor tocilizumab. J Rheumatol. (2018) 45(12):1620–7. doi: 10.3899/jrheum.180065
30. Hindricks G, Potpara T, Dagres N, Arbelo E, Bax JJ, Blomström-Lundqvist C, et al. 2020 ESC guidelines for the diagnosis and management of atrial fibrillation developed in collaboration with the European Association for Cardio-Thoracic Surgery (EACTS). Eur Heart J. (2021) 42(5):373–498. doi: 10.1093/eurheartj/ehaa612
31. Menichelli D, Vicario T, Ameri P, Toma M, Violi F, Pignatelli P, et al. Cancer and atrial fibrillation: epidemiology, mechanisms, and anticoagulation treatment. Prog Cardiovasc Dis. (2021) 66:28–36. doi: 10.1016/j.pcad.2021.04.004
32. Nielsen JB, Graff C, Pietersen A, Lind B, Struijk JJ, Olesen MS, et al. J-Shaped association between QTc interval duration and the risk of atrial fibrillation. J Am Coll Cardiol. (2013) 61(25):2557–64. doi: 10.1016/j.jacc.2013.03.032
33. Zhang N, Gong M, Tse G, Zhang Z, Meng L, Yan BP, et al. Prolonged corrected QT interval in predicting atrial fibrillation: a systematic review and meta-analysis. Pacing Clin Electrophysiol. (2018) 41(3):321–7. doi: 10.1111/pace.13292
34. Fortini A, Torrigiani A, Sbaragli S, Lo Forte A, Crociani A, Cecchini P, et al. COVID-19: persistence of symptoms and lung alterations after 3–6 months from hospital discharge. Infection. (2021) 49(5):1007–15. doi: 10.1007/s15010-021-01638-1
Keywords: COVID-19, electrocardiogram (ECG), arrhythmia, QTc interval, mortality
Citation: Mojón-Álvarez D, Izquierdo A, Cubero-Gallego H, Calvo-Fernández A, Marrugat J, Pérez-Fernández S, Cabero P, Solà-Richarte C, Soler C, Farré N and Vaquerizo B (2023) The natural history of QTc interval and its clinical impact in coronavirus disease 2019 survivors after 1 year. Front. Cardiovasc. Med. 10:1140276. doi: 10.3389/fcvm.2023.1140276
Received: 8 January 2023; Accepted: 21 March 2023;
Published: 6 April 2023.
Edited by:
Konstantinos Athanasios Gatzoulis, National and Kapodistrian University of Athens, GreeceReviewed by:
Christos-Konstantinos Antoniou, Athens Heart Center, Greece© 2023 Mojón-Álvarez, Izquierdo, Cubero-Gallego, Calvo-Fernández, Marrugat, Pérez-Fernández, Cabero, Solà-Richarte, Soler, Farré and Vaquerizo. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Beatriz Vaquerizo YmVhdmFxdWVyaXpvQHlhaG9vLmVz
Specialty Section: This article was submitted to Cardiac Rhythmology, a section of the journal Frontiers in Cardiovascular Medicine
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.