 Mingsong Zhang†
Mingsong Zhang† He Wang
He Wang Wei Sun
Wei Sun Bin Liu
Bin Liu- Department of Cardiology, The Second Hospital of Jilin University, Changchun, China
Heart failure is a serious threat to human health, with morbidity and mortality rates increasing despite the existence of multiple treatment options. Therefore, it is necessary to identify new therapeutic targets for this disease. Sacubitril/valsartan is a supramolecular sodium salt complex of the enkephalinase inhibitor prodrug sacubitril and the angiotensin receptor blocker valsartan. Its combined action increases endogenous natriuretic peptides while inhibiting the renin-angiotensin-aldosterone system and exerting cardioprotective effects. Clinical evidence suggests that sacubitril/valsartan is superior to conventional renin-angiotensin-aldosterone inhibitor therapy for patients with reduced ejection fraction heart failure who can tolerate angiotensin-converting enzyme inhibitors or angiotensin II receptor blockers. The therapy reduces the risk of heart failure hospitalization, cardiovascular mortality, and all-cause mortality and has a better safety and tolerability record. This review describes the potential pathophysiological mechanisms of cardiomyocyte injury amelioration by sacubitril/valsartan. We explore the protective effects of sacubitril/valsartan and outline the therapeutic value in patients with heart failure by summarizing the results of recent large clinical trials. Furthermore, a preliminary outlook shows that sacubitril/valsartan may be effective at treating other diseases, and provides some exploratory observations that lay the foundation for future studies on this drug.
1. Introduction
Heart failure (HF) is a common clinical condition characterized by typical clinical symptoms such as dyspnea, edema, and decreased exercise tolerance, together with signs resulting from structural or functional abnormalities of the heart. It can be divided into three categories based on the left ventricular ejection fraction (LVEF): preserved ejection fraction (LVEF ≥ 50%), mildly reduced ejection fraction (LVEF 40%–49%), and reduced ejection fraction (LVEF < 40%). The etiology, comorbidities, and treatment of different types of HF differ; however, their pathophysiological features have similarities (1). Activation of the sympathetic nervous system is the fastest adaptive response mechanism in HF leading to positive inotropic and chronotropic effects that maintain perfusion of vital organs through blood redistribution (2). The renin-angiotensin-aldosterone (RAAS) system is also activated to maintain hemodynamic stability. However, over-activated sympathetic nerves can have negative effects, such as direct toxicity of epinephrine to cardiomyocytes, and inducing cardiomyocyte hypertrophy and apoptosis. Activation of the RAAS system leads to sodium and water retention, myocardial hypertrophy, and fibrosis (3). In addition, the reduced effectiveness of the natriuretic peptide (NP) system in HF patients can further aggravate sodium retention, vasoconstriction, and volume overload which can seriously affect long-term prognosis (4). Clinical trials showed that neither exogenous NPs administration nor enkephalinase inhibition (NEPI) alone has a good therapeutic effect, which may be a detrimental for the over-activated RAAS system (5–7). Therefore, the development and the use of drugs that effectively inhibit the activation of the neuroendocrine system in patients with HF have shown to be effective in reducing mortality and hospitalizations in HF patients so much so that they are strongly recommended by international guidelines for the treatment of heart failure (8).
Sacubitril/valsartan (Entresto, development code LCZ696) was approved by the U.S. Food and Drug Administration (FDA) and the European Medicines Agency (EMA) in 2015 as the first successful angiotensin receptor- enkephalinase inhibitor (ARNI) on the market. Sacubitril/valsartan is a 1:1 combination of the NEPI prodrug sacubitril and the angiotensin II receptor blocker (ARB), valsartan (9, 10). The metabolized active form of sacubitril (LBQ657) inhibits enkephalinase. Enkephalinase is a naturally occurring zinc-dependent membrane metallopeptidase that metabolizes different vasoactive peptides including NPs, bradykinin, and angiotensin II (Ang II) (11). Enkephalinase inhibition leads to an increase in circulating NPs, especially atrial natriuretic peptide (ANP), brain natriuretic peptide (BNP), and other vasoactive peptides. It also has a therapeutic effect on many cardiovascular diseases (CVDs) through its antioxidant-, anti-inflammatory-, and antifibrotic effects. It should be noted that LBQ657 inhibits Ang II degradation by enkephalinase which results in increased Ang II levels and accelerated progression of HF; however, its combination with valsartan resolves this problem (Figure 1) (6, 12–14). Clinical evidence suggests that sacubitril/valsartan further reduces the risk of HF hospitalization, cardiovascular mortality, and all other causes of mortality in patients with HF who can tolerate angiotensin-converting enzyme inhibitors (ACEI) or ARBs, but also has a better safety and tolerability profile (15). This review provides a comprehensive and systematic overview of the pathophysiological mechanisms of sacubitril/valsartan in CVD, and an in-depth discussion of its role in several large clinical trials. This may be used as a guide to the widespread use of sacubitril/valsartan in clinical practice.
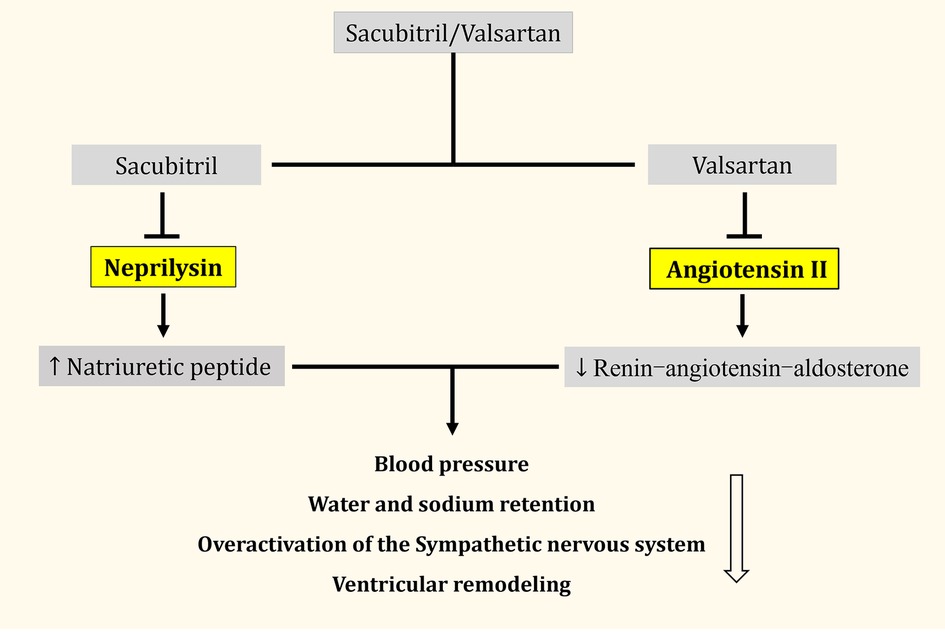
Figure 1. Simplified overview of the effects of sacubitril/valsartan.
2. Mechanisms of action of sacubitril valsartan: experimental evidences
2.1. Oxidative stress
Sacubitril/valsartan inhibits superoxide dismutase (SOD), catalase (CAT), glutathione peroxidase (GPx), glutathione S-transferase (GST), degradation of antioxidant enzymes, and oxidative stress in the isoprenaline (ISO)-induced myocardial infarction (MI) rat model (16). Furthermore, it reduces myogenic fiber damage and infarct size, and provides cardioprotective effects for the heart after MI.
Sacubitril/valsartan ameliorates cardiorenal syndrome (CRS)-mediated decreases in the expression levels of antioxidant enzymes, including NADPH oxidase 4 (NOX-4), xanthine oxidase, and CAT. It downregulates intracellular reactive oxygen species (ROS) levels, and ameliorates CRS-induced heart and kidney damage in rats (17). Furthermore, it significantly reduces the levels of nuclear transcription factor κB (NF-κB) p65, increases nuclear factor E2-related factor 2 (Nrf2) nuclear translocation levels, and improves chronic kidney disease (CKD)-mediated oxidative stress compared to valsartan alone (Table 1) (18).
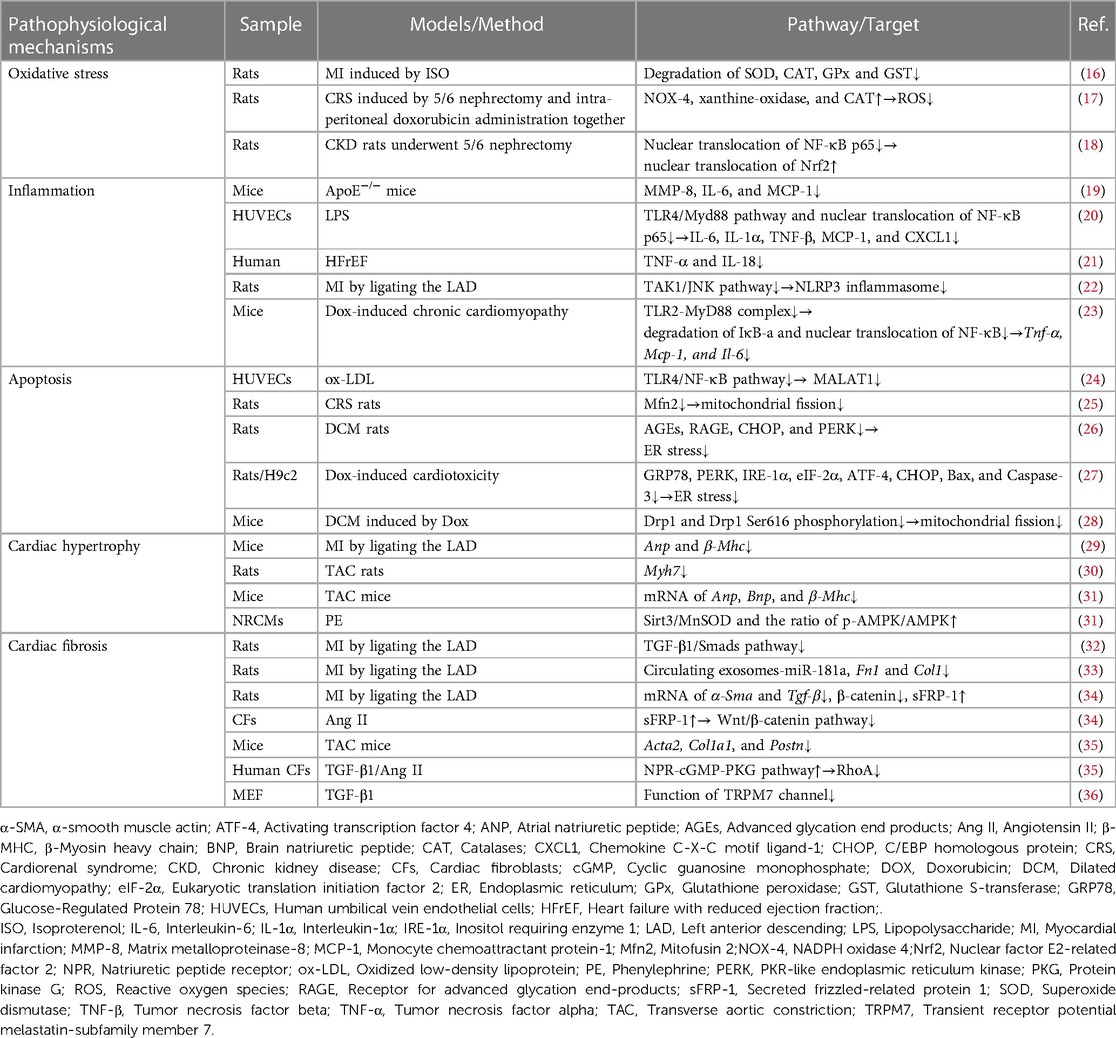
Table 1. Mechanisms of action of sacubitril valsartan: experimental evidences.
2.2. Inflammation
Atherosclerotic plaque formation is an inflammatory condition of the arterial wall. The expression of pro-inflammatory cytokines, including matrix metalloproteinase-8 (MMP-8), interleukin-6 (IL-6), and monocyte chemoattractant protein-1 (MCP-1) is downregulated in AS plaques of apolipoprotein E-deficient mice (apoE−/− mice) that were fed a high-fat diet after sacubitril/valsartan treatment. Furthermore, atherosclerotic plaque area and lipid content were reduced, collagen content and fibrous cap thickness were increased, and plaque stability was improved (19). Sacubitril/valsartan downregulates the expression of pro-inflammatory cytokines IL-6, IL-1α, tumor necrosis factor (TNF-β), chemokine (MCP-1), and chemokine CXC motif ligand-1 (CXCL1) by inhibiting the Toll-like receptor 4 (TLR4)/myeloid differentiation factor 88 (Myd88) pathway, NF-κB p65 nuclear translocation, and improving lipopolysaccharide (LPS)-induced endothelial cell inflammation (20). It significantly reduces circulating TNF-α and IL-18 levels in patients with HF with reduced ejection fraction (HFrEF) after 4 weeks of treatment, accompanied by improved peripheral vascular function and increased exercise tolerance (21).
Sacubitril/valsartan inhibits the inflammatory response and improves ventricular remodeling by blocking the TAK1/JNK signaling pathway and reducing the expression level of the NLRP3 inflammasome in rats with HF after MI (22). It inhibits formation of the TLR2-MyD88 complex, reverses DOX-induced degradation of IκB-α and increase of nuclear translocation of NF-κB, and downregulates the expression of pro-inflammatory genes, including TNF-α, MCP-1, and IL-6 in a mouse model of doxorubicin (DOX)-induced chronic cardiomyopathy; this causes a reduction in cardiac inflammation and amelioration of cardiac injury (23).
2.3. Apoptosis
Sacubitril/valsartan inhibits oxidized low-density lipoprotein-induced apoptosis in human umbilical vein endothelial cells and ameliorates endothelial injury by inhibiting the TLR4/NF-κB signaling pathway and downregulating metastasis-associated lung adenocarcinoma transcript 1 (MALAT1) expression (24). Administration of sacubitril/valsartan to rats fed a high-protein diet with CRS downregulates mitofusin 2 (Mfn2) expression, inhibits mitochondrial division, protects the functional integrity of mitochondria, inhibits apoptosis, and improves cardiac function (25).
Sacubitril/valsartan significantly downregulates advanced glycation end products formation and receptor for advanced glycation end-product (RAGE) expression while decreasing C/EBP homologous protein (CHOP) and phosphorylated PKR-like endoplasmic reticulum kinase (PERK) expression levels in rats with diabetic cardiomyopathy (DCM) (26). This leads to improved endoplasmic reticulum (ER) stress and DCM-induced apoptosis.
Sacubitril/valsartan downregulates the ER stress-related proteins glucose-regulated protein 78 (GRP78), PERK, inositol-requiring enzyme 1α (IRE-1α), eukaryotic translation initiation factor 2 (eIF-2α), activating transcription factor 4 (ATF4), and CHOP expression in the DOX-induced rat cardiotoxicity model and H9c2 cardiomyocyte model (27). Furthermore, it downregulates the expression of apoptotic proteins Bax and Caspase-3, reduces cardiomyocyte apoptosis and cardiac systolic dysfunction. It protects cardiac function by downregulating Drp1 protein expression and inhibiting Drp1 Ser616 phosphorylation in mouse cardiomyocytes, thereby reducing mitochondrial fission and apoptosis (28).
2.4. Cardiac hypertrophy
Sacubitril/valsartan downregulates the expression of cardiac hypertrophy marker genes, including ANP and β-myosin heavy chain (β-MHC), significantly reduced cardiomyocyte hypertrophy in the non-infarct and border zones, and attenuated adverse cardiac remodeling in a mouse model of MI constructed by ligation of the left anterior descending branch (29).
Sacubitril/valsartan treatment of an HF with preserved ejection fraction (HFpEF) rat model constructed by the transverse aortic constriction (TAC) procedure (30) significantly decreases left ventricular weight, downregulates Myh7 gene expression, and improves myocardial hypertrophy and diastolic dysfunction. Sacubitril/valsartan downregulates the mRNA levels of cardiac hypertrophy markers, including ANP, BNP, and β-MHC in a mouse model of TAC surgery-induced HF (31). This significantly reduces the cross-sectional area of cardiomyocytes. Sacubitril/valsartan upregulates sirtuin 3 (Sirt3)/manganese superoxide dismutase (MnSOD) expression and p-AMPK/AMPK ratio to inhibit phenylephrine-induced cardiomyocyte hypertrophy in vitro. Sirt3 knockdown abrogates the protective effect of sacubitril/valsartan on cardiomyocyte hypertrophy. This suggests that sacubitril/valsartan activates the Sirt3/MnSOD pathway to ameliorate pathological cardiac remodeling induced by pressure overload.
2.5. Cardiac fibrosis
In a post-MI rat model of HF, Wu et al. found that sacubitril/valsartan significantly inhibits the upregulation of transforming growth factor β1 (TGF-β1) and p-Smad3 protein expression in the rat infarcted myocardium (32). A similar model observed that sacubitril/valsartan downregulates circulating exosome miR-181a, decrease FN1 and COL1 gene expression levels, and decreases the fibrosis area (33). Sacubitril/valsartan reverses the increased transcript levels of α-smooth muscle actin (α-SMA) and TGF-β genes, suppresses β-catenin expression, and upregulates secreted frizzled-related protein 1 (sFRP-1) expression in rats with HF after MI. Further studies in primary mouse fibroblasts revealed that sacubitril/valsartan prevents the progression of myocardial fibrosis by inhibiting the Wnt/β-catenin pathway through SFRP1 upregulation (34).
Sacubitril/valsartan inhibits the expression of genes associated with myofibroblast transformation and activation (including Acta2, Col1a1, and Postn) in a mouse model of left ventricular pressure overload (35), blocks myofibroblast activation and reduces pathological accumulation of cardiac fibroblasts. Further experiments with TGF-β1/Ang II-stimulated human CF confirm that sacubitril/valsartan inhibits the function of RhoA and prevents the conversion of cardiac fibroblasts to myofibroblasts by activating the natriuretic peptide receptor (NPR)-cGMP-PKG signaling pathway. Meanwhile, LBQ657 inhibits TGF-β1-induced fibroblast activation by blocking the function of the TRPM7 channel in vitro (36).
3. Clinical trials of sacubitril/valsartan
3.1. PARAMOUNT
PARAMOUNT (NCT00887588) is a 36-week randomized, double-blind, multicenter, parallel-group, active-controlled phase II clinical trial (Table 2) evaluating the efficacy, safety, and tolerability of sacubitril/valsartan vs. valsartan in HF. Solomon et al. showed N-terminal pro-brain natriuretic peptide (NT-proBNP) rapidly declined from week 4 to week 12 and 36 of the primary trial endpoint in the sacubitril/valsartan-treated group compared to valsartan (37). Patients in the sacubitril/valsartan group have reduced left atrial size, reversed left atrial remodeling, significantly improved New York Heart Association (NYHA) classification, and good overall tolerability at week 36 (Table 3).
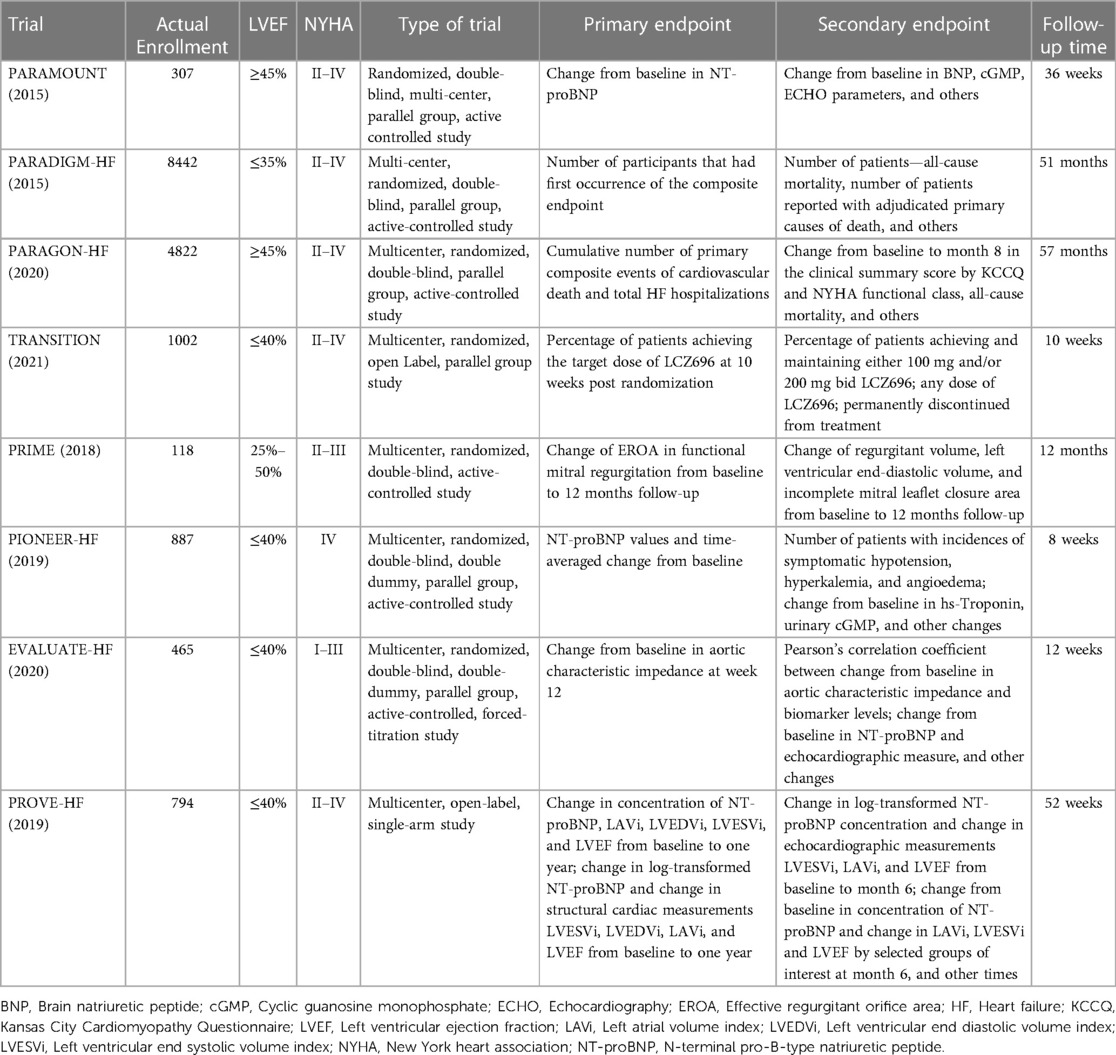
Table 2. Overview of sacubitril/valsartan clinical trials.
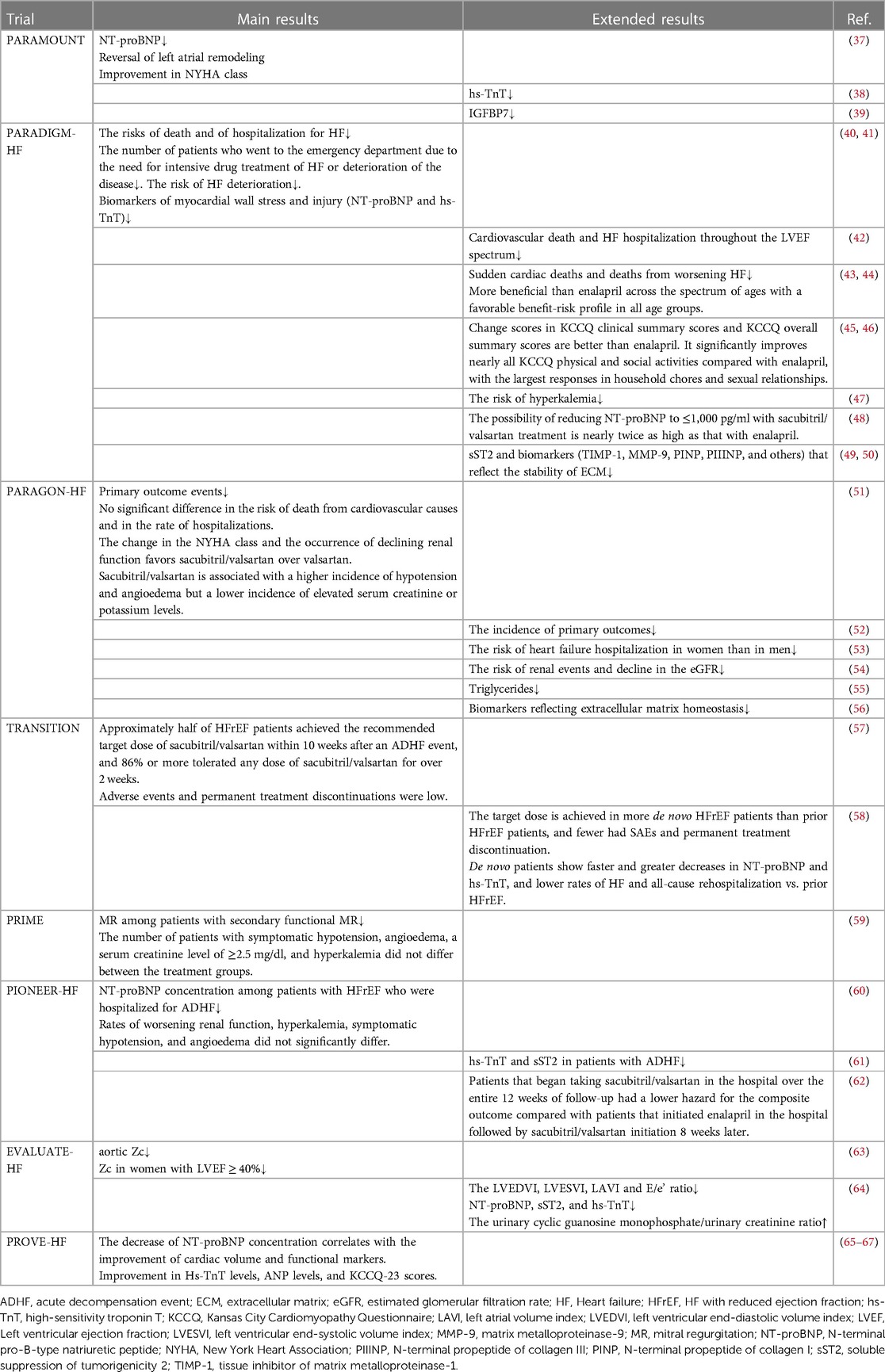
Table 3. Results of clinical trials with sacubitril/valsartan.
Jhund et al. found by testing high-sensitivity troponin T (hs-TnT) in patients from the PARAMOUNT trial that most had hs-TnT concentrations above the threshold for diagnosing myocardial injury (38). Higher hs-TnT concentrations were associated with increased age, elevated NT-proBNP levels, and lower estimated glomerular filtration rate (eGFR), suggesting a poorer prognosis for HFpEF. The reduction in hs-TnT was greater after 36 weeks of sacubitril/valsartan treatment than after valsartan treatment. Sacubitril/valsartan may attenuate myocardial injury in patients with HFpEF by enhancing the NPs system. Insulin-like growth factor-binding protein-7 (IGFBP7) is a senescence-associated protein that inhibits cell proliferation by arresting the cell cycle. Its elevated circulating concentrations is associated with cardiac hypertrophy, abnormal ventricular filling dynamics, and poor prognosis in patients with HFpEF (68). Januzzi et al. found that IGFBP7 concentrations in patients with HFpEF predicted the presence of left atrial dilation based in 228 participants from the PARAMOUNT trial (39). Interestingly, sacubitril/valsartan treatment leads to a decrease in IGFBP7 concentrations that is not observed in valsartan-treated patients. This decrease in IGFBP7 may be a direct effect of NEPI on age-related pathways or an effect of LBQ657 on the underlying pathophysiological processes of the disease; this needs further investigation (Table 3).
3.2. PARADIGM-HF
PARADIGM-HF (NCT01035255) is a multicenter, randomized, double-blind, parallel-group, active-controlled phase III clinical trial that compares the long-term efficacy and safety of enalapril and sacubitril/valsartan in patients with HFrEF (69). The trial was stopped early after a median follow-up of 27 months produced overwhelming benefits of sacubitril/valsartan. The 2014 results noted a significant advantage of sacubitril/valsartan over enalapril in reducing cardiovascular mortality, risk of HF hospitalization, HF symptoms, and physical limitations (40). Sacubitril/valsartan-treated patients require significantly fewer visits to the emergency department for intensive drug therapy for HF or for disease progression and have a reduced risk of worsening HF. The use of sacubitril/valsartan significantly reduces the rate of HF hospitalization while lowering NT-proBNP and hs-TnT levels during the first 30 days after randomization; this stabilizing effect on the course of HF may have an important impact on patient's quality of life (41).
Solomon et al. correlated the results of the PARADIGM-HF study with LVEF to assess the effectiveness of Sacubitril/Valsartan across the LVEF spectrum. The LVEF is a significant and independent predictor of all clinical outcomes in patients with HFrEF enrolled in the trial. Each 5% reduction in LVEF is associated with a 9% increase in the risk of cardiovascular death or hospitalization for HF. Sacubitril/valsartan effectively reduces cardiovascular death and hospitalization for HF across the LVEF spectrum (42). A study of the mode of death of deceased patients reveals that sacubitril/valsartan reduces cardiovascular mortality by 20% by decreasing the incidence of sudden death and progressive HF; however, it has no significant effect on the incidence of non-cardiovascular death (43). Sacubitril/valsartan reduces mortality in HFrEF, primarily by reducing cardiovascular death due to worsening HF. It has a significant benefit compared with enalapril across the age range of PARADIGM-HF, despite increasing mortality and HF hospitalization rates with patient age (44).
HF negatively affects health-related quality of life (HRQL) in the physical, psychological, and social domains. HRQL predicts the risk of future morbidity and mortality and is a key target for the treatment of patients with chronic HF (70). The Kansas City Cardiomyopathy Questionnaire (KCCQ) is an HF-specific HRQL test validated in patients with HFrEF (71). The KCCQ clinical summary score (KCCQ-CS) and KCCQ overall summary score (KCCQ-OS) are better in patients treated with sacubitril/valsartan than in those treated with enalapril and this trend persisted over the 8 month follow-up period (45). Furthermore, sacubitril/valsartan significantly improves physical and social activities in almost all HFrEF patients, especially in the areas of housework and sexual relationships (46).
The PARADIGM-HF trial also found that the risk of severe hyperkalemia is significantly reduced when mineralocorticoid receptor antagonists (MRA) are combined with sacubitril/valsartan, but not enalapril (47). Preferential use of sacubitril/valsartan in eligible patients with HFrEF improves the safety of MRA and allows patients to benefit with less risk.
Decreased NPs levels are associated with decreased morbidity and mortality, while increased NPs levels suggest a poor prognosis (48). Patients whose NT-proBNP level decreased to below 1,000 pg/ml have a 59% lower risk of the primary endpoint event than those who did not. The median NT-proBNP values are significantly lower in patients treated with sacubitril/valsartan than in those treated with enalapril after a month of randomization. Furthermore, the sacubitril/valsartan treatment is nearly twice as likely to reduce NT-proBNP levels to ≤1,000 pg/ml compared with enalapril. Elevated levels of soluble suppression of tumorigenicity 2 (sST2) correlate with the severity of adverse cardiac remodeling and fibrosis, and represent a potential prognostic biomarker for HFrEF. The sST2 levels decreased to a greater extent over time in patients from the sacubitril/valsartan treatment group than in those in the enalapril group in the PARADIGM-HF trial (49). In addition, sacubitril/valsartan treatment improves biomarkers reflecting extracellular matrix homeostasis (including TIMP-1, MMP-9, PINP, and PIIINP), reduces collagen synthesis and processing in vivo, and inhibits myocardial fibrosis (50).
3.3. PARAGON-HF
PARAGON-HF (NCT01920711) is a multicenter, randomized, double-blind, parallel-group, active-controlled, phase III clinical trial. The efficacy and safety of sacubitril/valsartan was compared to valsartan through assessing the reduction in cardiovascular mortality and overall HF hospitalization rates in patients with HFpEF. PARAGON-HF is the largest outcome trial conducted to date in patients with HFpEF (72), with more stringent inclusion criteria than those of previous trials.
The results of the study published in 2019 suggested that Sacubitril/valsartan has fewer primary outcome events than valsartan (51). The sacubitril/valsartan group has a lower (but not statistically significant) rate of HF hospitalization, along with no significant difference in the risk of cardiovascular mortality. Sacubitril/valsartan did not significantly reduce the overall hospitalization rate for HF and mortality from cardiovascular causes in patients with HFpEF. Sacubitril/valsartan is superior to valsartan in improving the NYHA classification and reducing the decline in renal function in four exploratory secondary outcomes. In terms of safety, Sacubitril/Valsartan is associated with a higher incidence of hypotension and vasogenic edema and a lower incidence of elevated creatinine or potassium ions. Pooled analysis of data from PARADIGM-HF (LVEF ≤ 40%; n = 8,399) and PARAGON-HF (LVEF ≥45%; n = 4,796) and grouped studies based on LVEF show a significantly lower incidence of primary outcome in patients treated with sacubitril/valsartan than in those treated with ACEI/ARB (52). Hospitalization for HF, cardiovascular death, and all-causes of mortality significantly decrease as LVEF increases, with the greatest decrease in cardiovascular mortality and a smaller decrease in hospitalization for HF. In particular the effect on outcomes continue across the spectrum of EF until 50% for men and 55% for women. Infact, the PARAGON-HF trial results suggest that sex alters the effect of sacubitril/valsartan vs. valsartan on the primary outcome event; the drug worked better for women than for men. Also, sacubitril/valsartan is more likely to reduce the risk of hospitalization for HF in female patients than valsartan (53).
The therapeutic benefit of sacubitril/valsartan in patients with HFpEF is amplified in the high-risk window following hospitalization compared with valsartan, and it potentially reduces the additional risk associated with the high-risk period; however, prospective trials are needed to validate this finding. Over time, sacubitril/valsartan does not significantly reduce the burden of HF signs and symptoms; however, it reduces the incidence of exertional dyspnea compared with valsartan and significantly reduces the incidence of renal composite outcomes and the overall rate of decline in eGFR (54).
Sacubitril/valsartan significantly reduces triglyceride levels by almost three-fold in patients with elevated triglyceride levels at baseline (55). In addition, sacubitril/valsartan reduces sST2, TIMP-1, and PIIINP levels, and increases CITP levels, inhibits profibrotic signaling, and this may be an important mechanism for the benefit observed on outcomes (56).
3.4. TRANSITION
Although the PARADIGM-HF trial shows that sacubitril/valsartan is superior to ACEI in reducing cardiovascular morbidity and mortality in HFrEF, only 2.3% of HFrEF in patients in the United States who were able to receive ARNI therapy (nearly 70% of HFrEF patients) were treated with sacubitril/valsartan at discharge (73). This may be owing to the lack of sufficient evidence on the benefit and safety of in-hospital sacubitril/valsartan initiation in the HFrEF patient population. The TRANSITION test is a good complement to the PARADIGM-HF test (57). TRANSITION (NCT02661217) is a multicenter, randomized, open-label, parallel-group phase IV clinical trial comparing sacubitril/valsartan treatment in patients with HFrEF admitted for an acute decompensation event (ADHF) administered at different times before and after hospital discharge (74).
Approximately half of the patients with HFrEF achieved the recommended target dose of sacubitril/valsartan within 10 weeks after ADHF; over 86% tolerated any dose of sacubitril/valsartan for over 2 weeks, and the percentage of patients who permanently discontinued sacubitril/valsartan owing to adverse events was low (57). A higher proportion of patients with new-onset HFrEF tolerated the target dose at week 10, and fewer experienced serious adverse events leading to permanent therapy discontinuation compared with patients with previously diagnosed HFrEF (58). Early intervention with sacubitril/valsartan may have greater benefits in delaying disease progression in patients with new-onset HFrEF. In addition, new-onset patients have a faster and greater decline in NT-proBNP and hs-TnT levels, and lower all-cause rehospitalization rates. In-hospital administration of sacubitril/valsartan results in a rapid and significant reduction in NT-proBNP levels: NT-proBNP is reduced by 28% at discharge among patients treated with sacubitril/valsartan in-hospital, and 46% of patients have a reduction in NT-proBNP from baseline levels to ≤1,000 pg/ml.
3.5. PRIME
PRIME (NCT02687932) is a prospective, multicenter, double-blind, randomized, active-controlled trial. This study investigated the effects of sacubitril/valsartan and valsartan in patients with functional mitral regurgitation (MR) secondary to left ventricular dysfunction by measuring the effective regurgitant orifice area (EROA), regurgitant flow, and cardiac function parameters. Sacubitril/valsartan reduces MR more than valsartan in patients with secondary functional MR. An intention-to-treat analysis of 117 patients shows that the sacubitril/valsartan and valsartan groups have significant differences in EROA (30% and 9% decrease, respectively), and in return flow at the study endpoint (33% and 12% decrease, respectively). The left ventricular end-systolic and end-diastolic volumes were significantly reduced in the sacubitril/valsartan group. In addition, there is no difference in the proportion of patients with adverse effects, such as symptomatic hypotension, angioedema, elevated serum creatinine levels, and hyperkalemia between the two treatment groups during the follow-up period (59). These findings support the positive effect on LV remodeling and mitral regurgitation in HFrEF patients.
3.6. PIONEER-HF
PIONEER-HF (NCT02554890) is a multicenter, randomized, double-blind, active-controlled trial in patients with ADHF with reduced ejection fraction compared with in-hospital initiation of sacubitril/valsartan therapy or enalapril therapy. PIONEER-HF is the first clinical trial to investigate the effectiveness and safety of sacubitril/valsartan treatment in patients with ADHF.
In-hospital initiation of sacubitril/valsartan treatment results in a greater reduction in NT-proBNP concentrations than enalapril treatment in patients with HFrEF hospitalized for ADHF. The decrease in NT-proBNP concentration is more pronounced in the sacubitril/valsartan group than in the enalapril group at weeks 4 and 8, and the variability in the magnitude of this decrease was particularly significant at week 1. Safety analysis shows no significant difference in the incidence of worsening renal function, hyperkalemia, and symptomatic hypotension between the sacubitril/valsartan and enalapril groups, and the rate of permanent discontinuation of the trial drug owing to adverse events is not significantly different between the two treatment groups (60). The efficacy and safety are not affected by previous history of HF, whether ACEI/ARB treatment is administered, or whether the target dose is achieved (75–77).
Post hoc analysis shows that sacubitril/valsartan significantly reduces hs-TnT and sST2 in patients with ADHF and parallels the decrease in NT-proBNP (61). This suggests that sacubitril/valsartan may reduce myocardial injury and improve hemodynamics at an early stage. In the continuing 4-week study, patients who started sacubitril/valsartan in the hospital have a lower incidence of HF rehospitalization or cardiovascular death than patients who started sacubitril/valsartan after 8 weeks of taking enalapril in the hospital. It is worth noting that change from enalapril to sacubitril/valsartan in the patient after 8 weeks results in a further 37% reduction in NT-proBNP levels (62). This indicates that delayed sacubitril/valsartan treatment still produces a large benefit to patients.
3.7. EVALUATE-HF
EVALUATE-HF (NCT02874794) is a randomized, double-blind, multicenter clinical trial investigating the effects of sacubitril/valsartan on aortic sclerosis and cardiac remodeling in patients with HFrEF compared with enalapril.
Sacubitril/valsartan did not significantly improve central aortic sclerosis in patients with HFrEF compared to enalapril. The primary endpoint of aortic characteristic impedance (Zc) decreases in the sacubitril/valsartan group and slightly increases in the enalapril group from baseline to 12 weeks, however the differences between the treatments are not statistically significant. Meanwhile, there was a significantly greater reduction in brachial artery systolic pressure in the sacubitril/valsartan group than in the enalapril group. Treatment with sacubitril/valsartan is associated with a more pronounced reduction in Zc in female patients from the subgroup of patients with baseline LVEF ≥40%. However, no sex difference is observed in the group of patients with LVEF <40% (63).
At the secondary endpoint, patients in the sacubitril/valsartan group showed greater decreases in left ventricular end-diastolic volume index (LVEDVI), left ventricular end-systolic volume index (LVESVI), left atrial volume index (LAVI), and the E/e, ratio from the baseline to week 12 compared with the enalapril group. However, LVEF did not significantly differ between groups during this period. The sacubitril/valsartan group showed greater reductions in NT-proBNP, sST2, and hs-cTnT levels at 12 weeks, while the urinary cyclic guanosine phosphate/creatinine ratio increases at 12 weeks. Post hoc analyses showed that changes in NT-proBNP significantly associate with changes in left ventricular volumes, and the improvement in the total KCCQ score is significantly higher in the sacubitril/valsartan group than in the enalapril group. A higher proportion of patients in the sacubitril/valsartan group show an improvement in the total KCCQ score of ≥5 points, and changes in the quality of life are associated with improvements in NT-proBNP. In terms of safety, incidence of hypotension, hyperkalemia, and deterioration of renal function is similar in both groups (64).
3.8. PROVE-HF
In previous studies, Sacubitril/valsartan treatment is strongly associated with a decrease in NT-proBNP levels in patients with HF. However, it is unclear whether the beneficial effect of sacubitril/valsartan in patients with HF is associated with the reversal of myocardial remodeling. PROVE-HF (NCT02887183) is a 12-month prospective, single-arm, open-label trial investigating the correlation between changes in NT-proBNP and long-term changes in cardiac remodeling measures after the initiation of sacubitril/valsartan in patients with HFrEF.
These results suggest that the reduction in NT-proBNP concentration correlates with improvements in cardiac volume and functional markers at 12 months. The change in NT-proBNP concentration significantly correlates with LVEF, LVEDVI, LVESVI, LAVI, and E/e, from baseline to month 12. In addition, blood hs-cTnT and ANP levels and KCCQ-23 scores significantly improve after 12 months of sacubitril/valsartan treatment, and these improvements are closely associated with the reversal of myocardial remodeling (65–67). The cardioprotective effect of sacubitril/valsartan in HFrEF patients may be associated with the reversal of cardiac remodeling (78). The improvement in NT-proBNP levels and myocardial remodeling by sacubitril/valsartan did not significantly differ between patients of different ethnicities, although greater mean gains are seen in black patients in the first half of the trial and in white patients in the second half (79, 80). However, the explanation of this phenomena requires further.
3.9. Other clinical trials
A prospective single-center study of 108 patients with symptoms of HF shows that patients with HFrEF and severe right ventricular dysfunction have a worse prognosis than patients with mild right ventricular dysfunction after treatment with sacubitril/valsartan, although both groups show significant improvements in left and right ventricular function (81).
A multicenter study of 727 patients with HFrEF suggests that sacubitril/valsartan improves the hemodynamic status of patients. The magnitude of hemodynamic improvement reduced composite risk of all-cause mortality and re-hospitalization for HF during follow-up is associated with the dose of sacubitril/valsartan. The relationship between the maximum dose of sacubitril/valsartan tolerated by patients and clinical efficacy warrants further exploration (82).
The LIFE trial evaluated the tolerability, safety, and efficacy of sacubitril/valsartan in patients with advanced HFrEF (patients with NYHA class IV and LVEF ≤35%) vs. valsartan alone. Sacubitril/valsartan did not improve the clinical composite endpoints of days to survival, days to discharge, and absence of HF events compared with valsartan (83).
The TAROT-HF study found that patients with non-ischemic cardiomyopathy (NICM) generally show a greater improvement in LVEF than patients with ischemic cardiomyopathy (ICM) after sacubitril/valsartan treatment (84).
4. Disease application of sacubitril/valsartan
Sacubitril/valsartan may be an effective treatment for HF and is a potential therapeutic agent for other diseases (Tables 4.1, 4.2).
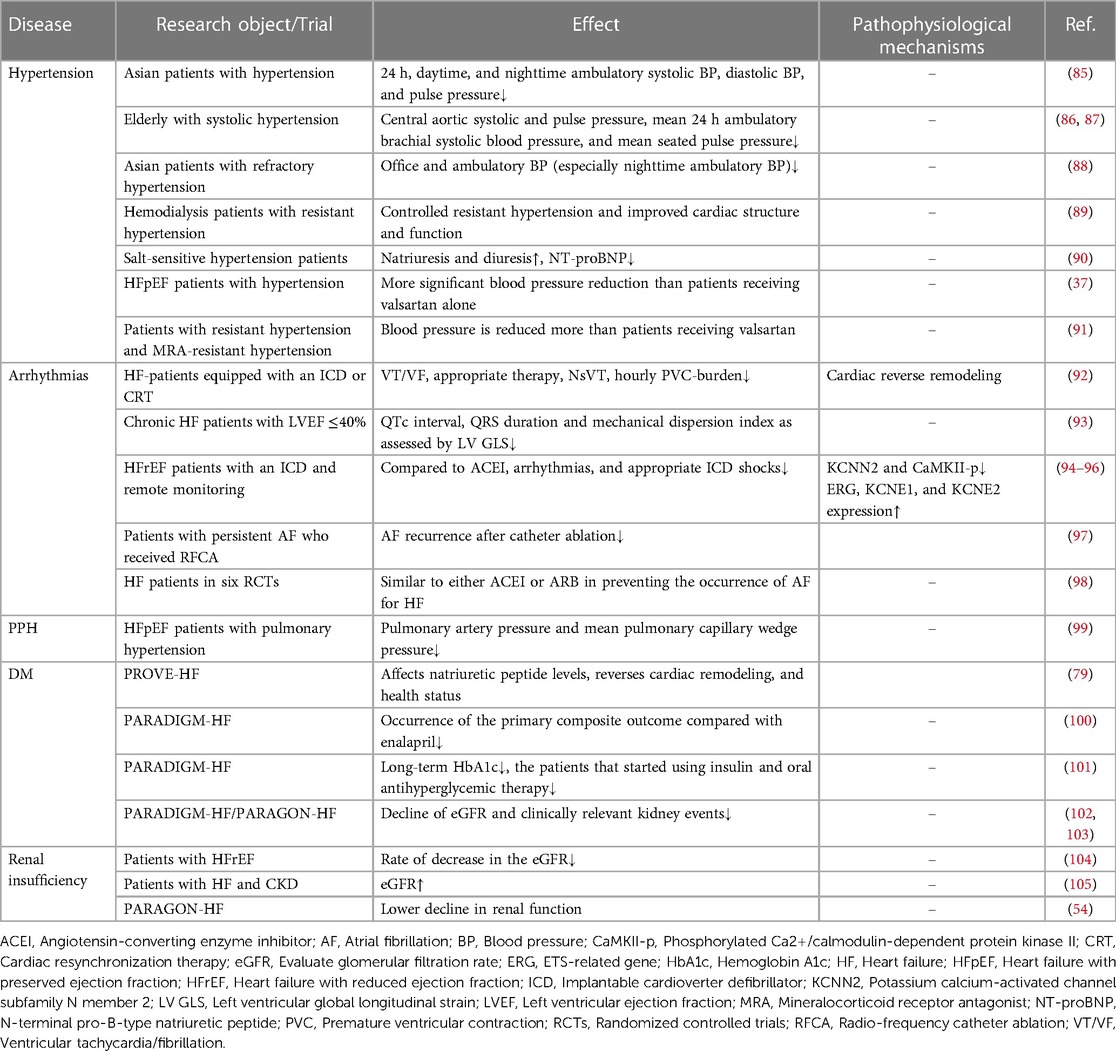
Table 4.1. Clinical trial of sacubitril/valsartan in other diseases.
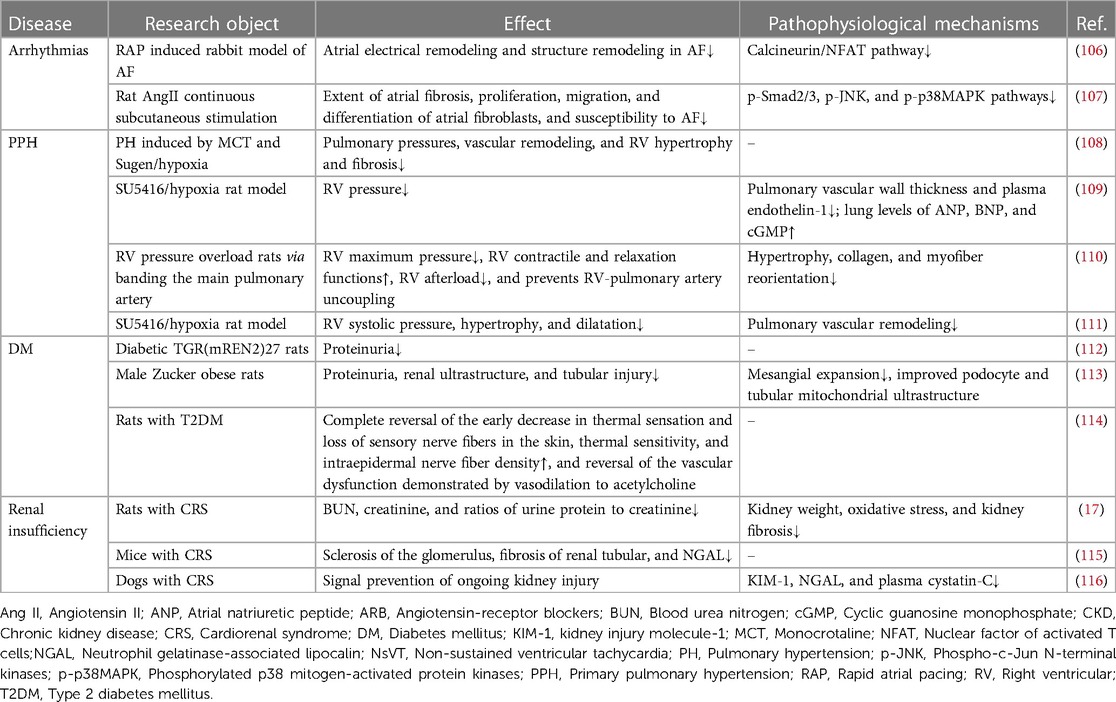
Table 4.2. Experimental studies of sacubitril/valsartan in other diseases.
4.1. Hypertension
Sacubitril/valsartan significantly reduces the 24-hour daytime and nighttime dynamic systolic-, diastolic-, and pulse pressures. It is well tolerated with no reported cases of angioedema (85). Patients treated with sacubitril/valsartan have more significant decreases in central arterial systolic pressure, central aortic pulse pressure, mean 24-hour ambulatory brachial artery systolic pressure, and mean sitting diastolic pressure than those treated with ACEI/ARB (86, 87). Sacubitril/valsartan significantly reduces office and ambulatory blood pressure and substantially reduces nocturnal ambulatory blood pressure in 66 Asian patients with refractory hypertension (88). And sacubitril/valsartan controls refractory hypertension, significantly reduces mean seated systolic and diastolic blood pressure, and partially improves cardiac structure in a single-center prospective study of 360 hemodialysis patients with refractory hypertension (89). This more pronounced antihypertensive effect may be partly attributed to the better urinary sodium excretion in hypertensive patients treated with sacubitril/valsartan compared with ACEI/ARB (90); however, the exact mechanism is unclear.
The application of sacubitril/valsartan also appears to be of greater benefit than traditional ACEI/ARB in HF patients with hypertension. The PARAMOUNT study shows that patients with HFpEF treated with sacubitril/valsartan for 12 weeks have a more significant reduction in blood pressure than patients treated with valsartan and are better tolerated (37). Meanwhile, there is no significant difference in the incidence of hypotension between the two groups. Refractory hypertension affects 10%–20% of HFpEF patients each year; some investigators have examined treatment of HFpEF patients with refractory hypertension using sacubitril/valsartan is significantly more effective than treatment with valsartan in the PARAGON-HF trial (91).
The 2017 ACC/AHA Heart Failure Guidelines were updated to include ARNI as the preferred treatment for HF patients with hypertension in addition to conventional therapy since sacubitril/valsartan lowers blood pressure and improves the prognosis of HF patients with combined hypertension (117). However, the mechanism facilitating sacubitril/valsartan efficacy over traditional ACEI/ARB analogs requires further investigation.
4.2. Cardiac arrhythmia
Clinical studies show that replacing ACEI/ARB treatment with sacubitril/valsartan in patients with HFrEF reduces the degree of burden of ventricular tachycardia or ventricular fibrillation, results in fewer ICD interventions, and significantly reduces the number and duration of non-sustained ventricular tachycardia (92). Sacubitril/valsartan treatment decreases the number of patients with sustained ventricular tachycardia, and the number of episodes of sustained ventricular arrhythmia significantly decreases in symptomatic patients (93). Sacubitril/valsartan reduces persistent ventricular tachycardia/ventricular fibrillation, non-persistent ventricular tachycardia, and paroxysmal atrial tachycardia/atrial fibrillation(AF) episodes in patients with HFrEF implanted with an ICD (94). These effects may be closely related to the downregulation of cardiac KCNN2 and phosphorylated calmodulin-dependent protein kinase II expression, and the upregulation of ERG, KCNE1, and KCNE2 expression (95, 96).
Sacubitril/valsartan also has therapeutic effects on AF. In patients with persistent AF who underwent radiofrequency ablation the probability of AF is significantly lower in patients treated with sacubitril/valsartan after 12 months of intervention than in patients treated with valsartan for the same duration (97). However, sacubitril/valsartan treatment did not significantly differ from enalapril or valsartan in preventing the development of AF in patients with HF in a meta-analysis of a randomized, double-blind, active controlled trial involving 15,512 patients. Notably, the authors did not deny the therapeutic effect of sacubitril/valsartan on AF (98). Sacubitril/valsartan reduces the incidence of AF in rabbits with rapid atrial pacing by attenuating atrial electrical and structural remodeling (106) and may reduce AF susceptibility by inhibiting p-Smad2/3, p-JNK, and p-p38MAPK pathways against Ang II-induced atrial fibrosis (107).
Although there is still a lack of convincing studies to prove the advantages of sacubitril/valsartan over conventional antiarrhythmic drugs, the current study suggests that sacubitril/valsartan has a protective effect against ventricular arrhythmias and AF, which may provide new ideas for the clinical treatment of arrhythmias.
4.3. Primary pulmonary hypertension (PPH)
The severity of PPH symptoms and survival are closely related to right ventricular function and right heart failure is the leading cause of death in patients with PPH. However, there are no treatments that directly target the right ventricle. Long-term application of sacubitril/valsartan reduces right ventricular remodeling and fibrosis, improves right ventricular systolic and diastolic function, reduces right ventricular afterload, and significantly reduces pulmonary artery pressure (108–110). These effects appear to be secondary to pulmonary vascular changes, including reduced pulmonary vascular remodeling (111). Sacubitril/valsartan inhibits the proliferation of pulmonary artery smooth muscle cells in patients with idiopathic PPH in vitro (108).
We also came across a study on the therapeutic effect of sacubitril/valsartan on PPH in patients. In a retrospective case study of 18 patients with PPH and HFpEF, conversion of ACEI/ARB to sacubitril/valsartan resulted in a significant reduction in pulmonary artery pressure and mean pulmonary capillary wedge pressure on right heart catheterization compared to ACEI/ARB use, with 12 of these patients having improved NYHA functional class. Invasive measurements further showed a significant reduction in right atrial pressure at follow-up (99). Emily et al. included five patients with HF who were temporarily unable to receive heart transplantation due to concomitant severe PPH, four of whom received heart transplantation within 5–36 days after starting sacubitril/valsartan therapy without complications such as postoperative PPH, right heart failure, or postoperative hypotension requiring vasopressor support (118). These cases seem to suggest that sacubitril/valsartan could be a potential treatment for advanced HF patients with severe PPH awaiting cardiac transplantation. Whether sacubitril/valsartan has effects independent of improved cardiac function in patients with PPH still requires more studies to explore and discover.
4.4. Diabetes mellitus
A post hoc analysis of the PROVE-HF trial shows that 361 of 794 patients have type 2 diabetes mellitus (T2DM). Cross-sectional studies show that T2DM patients and non-T2DM show similar levels of improvement in LVEF and KCCQ-OS after 12 months of treatment. Similar changes are observed in echocardiographic measurements. Longitudinal analysis shows that the mean NT-proBNP significantly decreases in both groups, while KCCQ-OS scores and the total benefit is slightly greater in the non-T2DM group than in the T2DM group. These results suggest that patients with T2DM starting sacubitril/valsartan treatment gain at least similar benefits to health status and reversal of cardiac remodeling compared with patients without T2DM (79). It is noteworthy that HF patients with T2DM tend to have worse cardiac function and prognosis than non-T2DM HF patients using conventional therapy (100).
A secondary study of the PARADIGM-HF trial shows that sacubitril/valsartan results in a more significant benefit in HF patients with T2DM than ACEI analogs. Patients with T2DM have a higher risk of major composite outcomes such as HF hospitalization or cardiovascular death compared to patients without a history of T2DM, while sacubitril/valsartan reduces the incidence of major composite outcomes compared to enalapril and has higher KCCQ scores than the enalapril group after 8 months treatment (101). Patients using sacubitril/valsartan have a greater reduction in HbA1c than those using enalapril after 1 and 3 years of follow-up. The proportion of patients starting treatment using insulin and oral hypoglycemic agent is significantly lower in the sacubitril/valsartan group than in the enalapril group (119).
Sacubitril/valsartan also has a significant protective effect on renal function in patients with T2DM. Post hoc analysis of the PARADIGM-HF trial (102) and the PARAGON-HF trial (103) shows that patients with HFpEF and DM have a greater decrease in the eGFR than patients without DM. Sacubitril/valsartan treatment attenuates eGFR decline, reduces clinically relevant renal events, and improves prognosis in patients with DM and non-DM HFpEF compared with valsartan treatment. And sacubitril/valsartan is more effective than ARB alone in reducing urinary protein excretion in diabetic rats in vivo (112). These renoprotective effects may be associated with reduced thylakoid expansion and improved podocyte and tubular mitochondrial ultrastructures (113). Notably, these protective effects are not dependent on improvements in blood pressure, blood glucose level, or oxidative stress.
Sacubitril/valsartan also shows a more pronounced advantage over ACEI/ARB analogs in terms of its protective effects against diabetic neuropathy. Early intervention with sacubitril/valsartan completely reverses the early decline in thermal sensation and loss of sensory nerve fibers in the skin compared with valsartan in a diabetic rat model. Furthermore, it significantly improves or even reverses the diabetes-induced reduction in corneal nerve fiber length and sensitivity. Late intervention with sacubitril/valsartan significantly improves thermal sensitivity and partial intraepidermal nerve fiber density. In addition, sacubitril/valsartan reverses the impaired vascular responsiveness to acetylcholine and improves diabetes-induced vasculopathy (114).
These studies suggest that sacubitril/valsartan helps HF patients with diabetes to better control their blood glucose, fight, or delay the progression of complications to some extent, and improve their cardiac function compared with ACEI/ARB drugs. This is expected to provide greater benefit to patients with diabetes. However, it is notable that the protective effect of sacubitril/valsartan on diabetes-related complications is only demonstrated in vivo, and there are no reliable clinical trials showing that the drug retains these significant effects in patients. The mechanism of its improvement in related complications needs to be further investigated.
4.5. Renal insufficiency
Kevin et al. showed that sacubitril/valsartan is more effective in slowing the rate of decline in eGFR than enalapril, and positively impacts cardiovascular and renal outcomes in patients with HFrEF with and without CKD. These renal and cardiovascular benefits are observed despite the increased urinary albumin/creatinine ratio of sacubitril/valsartan compared with enalapril (104). A meta-analysis noted that sacubitril/valsartan significantly increases eGFR; however, there is no difference in the urinary albumin/creatinine ratio between sacubitril/valsartan and controls, including the irbesartan, valsartan, and enalapril groups (105).
A secondary study of the PARAGON-HF trial suggests that patients with HFpEF administered sacubitril/valsartan have >50% lower incidence of eGFR decline relative to the baseline and a lower rate of overall eGFR decline compared to valsartan (54). However, a different conclusion was reached in a randomized double-blind trial that included 414 participants with an eGFR of 20–60 ml/min/1.73 m2 that were randomly assigned to sacubitril/valsartan treatment vs. irbesartan treatment for over 12 months [UK HARP-III trial]. Sacubitril/valsartan has similar effects to irbesartan on renal function and proteinuria, although it lowers blood pressure and cardiac biomarkers in patients with CKD (120). The difference in results between the two trials may be due to the fact that participants in HARP-III were younger, predominantly male, had higher blood pressure, more severe renal insufficiency, higher proteinuria levels, and a very low self-reported prevalence of HF and diuretic use compared to PARAGON-HF participants (54).
The renoprotective effects of sacubitril/valsartan are further corroborated by in vivo experiments. Sacubitril/valsartan significantly reduces plasma creatinine and urea nitrogen levels and the urine protein/creatinine ratio in rats. This protective effect on renal function in rats may be owing to the reduction in renal mass, reversal of oxidative stress damage in the kidney, and improvement in renal fibrosis (17). Another study showed that sacubitril/valsartan improves glomerulosclerosis, tubular atrophy, and fibrosis in CRS mice to a greater extent than valsartan and reduces plasma NT-proBNP and urinary neutrophil gelatinase-related apolipoprotein, but does not significantly improve blood creatinine (115). Similar results are observed in the CRS canine model. Sacubitril/valsartan significantly reduces the levels of kidney injury markers (KIM-1, NGAL, and plasma cystatin C), but has no significant effect on blood creatinine and urea nitrogen (116). These results suggest that sacubitril/valsartan protects against ongoing kidney injury, but does not improve or worsen overall kidney function.
Studies have reached different conclusions on whether sacubitril/valsartan improves renal function in patients with HF and animal models. However, it is undeniable that it has a protective effect on the kidney, which may be due to the inhibition of renal fibrosis and protection against ongoing renal injury. Further studies are required to determine whether sacubitril/valsartan is more effective at combating the decline in renal function than traditional ACEI/ARB drugs.
5. Prospect & outlook
The latest 2022 ACC/AHA/HFSA guidelines for the management of heart failure state that sacubitril/valsartan is recommended as a Class IA treatment to reduce morbidity and mortality in patients with NYHA Class II-III HFrEF (8). Sacubitril/valsartan is recommended as a Class IB alternative to ACEI or ARB to further reduce morbidity and mortality in patients with NYHA class II-III HFrEF with chronic HF symptoms. However, clinical studies investigating the effect of sacubitril/valsartan on ventricular remodeling, myocardial fibrosis, and hemodynamic improvement are currently limited to patients with HFrEF. Further clinical trials are required to determine the involvement of sacubitril/valsartan in other CVD treatments including HFpEF, acute myocardial infarction, AF, and hypertension since they were performed using small sample sizes, insufficient study lengths, and incomplete observations. However, we are reasonably confident that sacubitril/valsartan will become a transgenerational drug in the field of CVD treatment in the near future.
Author contributions
WS and BL contributed to conception, design and drafting of the manuscript. MZ, YZ, YL and HW contributed to data collection and manuscript drafting. All authors contributed to the article and approved the submitted version.
Funding
This study was supported by grants from the Major Science and Technology Project of Jilin Province (No. 20220303002SF), the Science and Technology Development Program of Jilin Province (No. 20190905002SF), the Health Science and Technology Capacity Improvement Project of Jilin Province (No. 2021LC016) and the National Clinical Key Specialty Project.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Abbreviations
αSMA, smooth muscle alpha actin; ACEI, angiotensin-converting enzyme inhibitor; ADHF, acute decompensation event; AF, atrial fibrillation; AGE, advanced glycation end product; Ang II, angiotensin II; ANP, atrial natriuretic peptide; ARB, angiotensin II receptor blocker; ARNI, angiotensin receptor- neprilysin inhibitor; AS atherosclerosis; ATF4, activating transcription factor 4; beta-MHC, β-myosin heavy chain; BNP, brain natriuretic peptide; CAT, catalase; CHOP, C/EBP homologous protein; CKD, chronic kidney disease; CRS, cardiorenal syndrome; CVD, cardiovascular diseases; CXCL1, chemokine CXC motif ligand-1; DCM, diabetic cardiomyopathy; DOX, doxorubicin; eIF-2α, eukaryotic translation initiation factor 2; ER, endoplasmic reticulum; EROA, effective regurgitant orifice area; GPx, glutathione peroxidase; GRP78, glucose-regulated protein 78; GST, glutathione S-transferase; HF, heart failure; HFpEF, HF with preserved ejection fraction; HFrEF, HF with reduced ejection fraction; HRQL, health-related quality of life; hs-TnT, high-sensitivity troponin T; ICD, implantable cardioverter defibrillator; ICM, ischemic cardiomyopathy; IGFBP7, insulin-like growth factor-binding protein-7; IL-6, interleukin-6; IRE-1α, inositol-requiring enzyme 1α; ISO, isoprenaline; KCCQ-CS, Kansas City Cardiomyopathy Questionnaire clinical summary score; KCCQ-OS, KKCCQ overall summary score; LAVI, left atrial volume index; LPS, lipopolysaccharide; LVEDVI, left ventricular end-diastolic volume index; LVEF, left ventricular ejection fraction; LVESVI, left ventricular end-systolic volume index; MALAT1, metastasis-associated lung adenocarcinoma transcript 1; MCP-1, monocyte chemoattractant protein-1; Mfn22, mitofusin 2; MI myocardial infarction; MMP-8, metalloproteinase-8; MnSOD, manganese superoxide dismutase; MR, mitral regurgitation; MRA, mineralocorticoid receptor antagonist; Myd88, myeloid differentiation factor 88; NEPI, enkephalinase inhibition; NF-κB, nuclear transcription factor κB; NICM, non-ischemic cardiomyopathy; NOX-4, NADPH oxidase 4; NP, natriuretic peptide; NPR, natriuretic peptide receptor; Nrf2, nuclear factor E2-related factor 2; NT-proBNP, N-terminal pro hormone B-type natriuretic peptide; NYHA, New York Heart Association; PERK, PKR-like endoplasmic reticulum kinase; PPH, primary pulmonary hypertension; RAAS, renin-angiotensin-aldosterone; RAGE, receptor for advanced glycation end-product; ROS, reactive oxygen species; SFRP1, secreted frizzled-related protein 1; Sirt, sirtuin; SOD, superoxide dismutase; sST2, soluble suppression of tumorigenicity 2; T2DM, type 2 diabetes mellitus; TAC, transverse aortic constriction; TGF-β1, transforming growth factor β1; TLR4, Toll-like receptor 4; TNF-β, tumor necrosis factor; Zc, aortic characteristic impedance.
References
1. Ponikowski P, Voors AA, Anker SD, Bueno H, Cleland JGF, Coats AJS, et al. 2016 ESC guidelines for the diagnosis and treatment of acute and chronic heart failure: the task force for the diagnosis and treatment of acute and chronic heart failure of the European society of cardiology (ESC) developed with the special contribution of the heart failure association (HFA) of the ESC. Eur Heart J. (2016) 37(27):2129–200. doi: 10.1093/eurheartj/ehw128
2. Riegger AJ. Hormones in heart failure–regulation and counterregulation. Eur Heart J. (1991) 12(Suppl D):190–2. doi: 10.1093/eurheartj/12.suppl_d.190
3. Tanai E, Frantz S. Pathophysiology of heart failure. Compr Physiol. (2015) 6(1):187–214. doi: 10.1002/cphy.c140055
4. Volpe M, Battistoni A, Rubattu S. Natriuretic peptides in heart failure: current achievements and future perspectives. Int J Cardiol. (2019) 281:186–9. doi: 10.1016/j.ijcard.2018.04.045
5. O'Connell JE, Jardine AG, Davidson G, Connell JM. Candoxatril, an orally active neutral endopeptidase inhibitor, raises plasma atrial natriuretic factor and is natriuretic in essential hypertension. J Hypertens. (1992) 10(3):271–7. doi: 10.1097/00004872-199203000-00011
6. Hubers SA, Brown NJ. Combined angiotensin receptor antagonism and neprilysin inhibition. Circulation. (2016) 133(11):1115–24. doi: 10.1161/circulationaha.115.018622
7. Gidlof O. Toward a new paradigm for targeted natriuretic peptide enhancement in heart failure. Front Physiol. (2021) 12:650124. doi: 10.3389/fphys.2021.650124
8. Heidenreich PA, Bozkurt B, Aguilar D, Allen LA, Byun JJ, Colvin MM, et al. 2022 AHA/ACC/HFSA guideline for the management of heart failure: a report of the American college of cardiology/American heart association joint committee on clinical practice guidelines. Circulation. (2022) 145(18):e895–1032. doi: 10.1161/CIR.0000000000001063
9. Gu J, Noe A, Chandra P, Al-Fayoumi S, Ligueros-Saylan M, Sarangapani R, et al. Pharmacokinetics and pharmacodynamics of LCZ696, a novel dual-acting angiotensin receptor-neprilysin inhibitor (ARNi). J Clin Pharmacol. (2010) 50(4):401–14. doi: 10.1177/0091270009343932
10. Ayalasomayajula S, Langenickel T, Pal P, Boggarapu S, Sunkara G. Clinical pharmacokinetics of sacubitril/valsartan (LCZ696): a novel angiotensin receptor-neprilysin inhibitor. Clin Pharmacokinet. (2017) 56(12):1461–78. doi: 10.1007/s40262-017-0543-3
11. Chen Y, Burnett JC Jr. Biochemistry, therapeutics, and biomarker implications of neprilysin in cardiorenal disease. Clin Chem. (2017) 63(1):108–15. doi: 10.1373/clinchem.2016.262907
12. McCormack PL. Sacubitril/valsartan: a review in chronic heart failure with reduced ejection fraction. Drugs. (2016) 76(3):387–96. doi: 10.1007/s40265-016-0544-9
13. Campbell DJ. Long-term neprilysin inhibition—implications for ARNIs. Nat Rev Cardiol. (2017) 14(3):171–86. doi: 10.1038/nrcardio.2016.200
14. Singh KD, Karnik SS. Angiotensin type 1 receptor blockers in heart failure. Curr Drug Targets. (2020) 21(2):125–31. doi: 10.2174/1389450120666190821152000
15. Ghionzoli N, Gentile F, Del Franco AM, Castiglione V, Aimo A, Giannoni A, et al. Current and emerging drug targets in heart failure treatment. Heart Fail Rev. (2021) 27(4):1119–36. doi: 10.1007/s10741-021-10137-2
16. Imran M, Hassan MQ, Akhtar MS, Rahman O, Akhtar M, Najmi AK. Sacubitril and valsartan protect from experimental myocardial infarction by ameliorating oxidative damage in wistar rats. Clin Exp Hypertens. (2019) 41(1):62–9. doi: 10.1080/10641963.2018.1441862
17. Yang CC, Chen YT, Chen CH, Li YC, Shao PL, Huang TH, et al. The therapeutic impact of entresto on protecting against cardiorenal syndrome-associated renal damage in rats on high protein diet. Biomed Pharmacother. (2019) 116:108954. doi: 10.1016/j.biopha.2019.108954
18. Suematsu Y, Jing W, Nunes A, Kashyap ML, Khazaeli M, Vaziri ND, et al. LCZ696 (sacubitril/valsartan), an angiotensin-receptor neprilysin inhibitor, attenuates cardiac hypertrophy, fibrosis, and vasculopathy in a rat model of chronic kidney disease. J Card Fail. (2018) 24(4):266–75. doi: 10.1016/j.cardfail.2017.12.010
19. Zhang H, Liu G, Zhou W, Zhang W, Wang K, Zhang J. Neprilysin inhibitor-angiotensin II receptor blocker combination therapy (sacubitril/valsartan) suppresses atherosclerotic plaque formation and inhibits inflammation in apolipoprotein E- deficient mice. Sci Rep. (2019) 9(1):6509. doi: 10.1038/s41598-019-42994-1
20. Gao A, Wang Y, Gao X, Tian W. LCZ696 Ameliorates lipopolysaccharide-induced endothelial injury. Aging (Albany NY). (2021) 13(7):9582–91. doi: 10.18632/aging.202692
21. Bunsawat K, Ratchford SM, Alpenglow JK, Park SH, Jarrett CL, Stehlik J, et al. Sacubitril-valsartan improves conduit vessel function and functional capacity and reduces inflammation in heart failure with reduced ejection fraction. J Appl Physiol. (2021) 130(1):256–68. doi: 10.1152/japplphysiol.00454.2020
22. Shen J, Fan Z, Sun G, Qi G. Sacubitril/valsartan (LCZ696) reduces myocardial injury following myocardial infarction by inhibiting NLRP3induced pyroptosis via the TAK1/JNK signaling pathway. Mol Med Rep. (2021) 24(3):676. doi: 10.3892/mmr.2021.12315
23. Ye S, Su L, Shan P, Ye B, Wu S, Liang G, et al. LCZ696 Attenuated doxorubicin-induced chronic cardiomyopathy through the TLR2-MyD88 Complex formation. Front Cell Dev Biol. (2021) 9:654051. doi: 10.3389/fcell.2021.654051
24. Bai W, Huo T, Chen X, Song X, Meng C, Dang Y, et al. Sacubitril/valsartan inhibits oxLDLinduced MALAT1 expression, inflammation and apoptosis by suppressing the TLR4/NFkappaB signaling pathway in HUVECs. Mol Med Rep. (2021) 23(6):402. doi: 10.3892/mmr.2021.12041
25. Yeh JN, Yue Y, Chu YC, Huang CR, Yang CC, Chiang JY, et al. Entresto protected the cardiomyocytes and preserved heart function in cardiorenal syndrome rat fed with high-protein diet through regulating the oxidative stress and Mfn2-mediated mitochondrial functional integrity. Biomed Pharmacother. (2021) 144:112244. doi: 10.1016/j.biopha.2021.112244
26. Belali OM, Ahmed MM, Mohany M, Belali TM, Alotaibi MM, Al-Hoshani A, et al. LCZ696 Protects against diabetic cardiomyopathy-induced myocardial inflammation, ER stress, and apoptosis through inhibiting AGEs/NF-kappaB and PERK/CHOP signaling pathways. Int J Mol Sci. (2022) 23(3):1288. doi: 10.3390/ijms23031288
27. Kim BS, Park IH, Lee AH, Kim HJ, Lim YH, Shin JH. Sacubitril/valsartan reduces endoplasmic reticulum stress in a rat model of doxorubicin-induced cardiotoxicity. Arch Toxicol. (2022) 96(4):1065–74. doi: 10.1007/s00204-022-03241-1
28. Xia Y, Chen Z, Chen A, Fu M, Dong Z, Hu K, et al. LCZ696 Improves cardiac function via alleviating Drp1-mediated mitochondrial dysfunction in mice with doxorubicin-induced dilated cardiomyopathy. J Mol Cell Cardiol. (2017) 108:138–48. doi: 10.1016/j.yjmcc.2017.06.003
29. Kompa AR, Lu J, Weller TJ, Kelly DJ, Krum H, von Lueder TG, et al. Angiotensin receptor neprilysin inhibition provides superior cardioprotection compared to angiotensin converting enzyme inhibition after experimental myocardial infarction. Int J Cardiol. (2018) 258:192–8. doi: 10.1016/j.ijcard.2018.01.077
30. Norden ES, Bendiksen BA, Andresen H, Bergo KK, Espe EK, Hasic A, et al. Sacubitril/valsartan ameliorates cardiac hypertrophy and preserves diastolic function in cardiac pressure overload. ESC Heart Fail. (2021) 8(2):918–27. doi: 10.1002/ehf2.13177
31. Peng S, Lu XF, Qi YD, Li J, Xu J, Yuan TY, et al. LCZ696 Ameliorates oxidative stress and pressure overload-induced pathological cardiac remodeling by regulating the Sirt3/MnSOD pathway. Oxid Med Cell Longev. (2020) 2020:9815039. doi: 10.1155/2020/9815039
32. Wu M, Guo Y, Wu Y, Xu K, Lin L. Protective effects of sacubitril/valsartan on cardiac fibrosis and function in rats with experimental myocardial infarction involves inhibition of collagen synthesis by myocardial fibroblasts through downregulating TGF-beta1/smads pathway. Front Pharmacol. (2021) 12:696472. doi: 10.3389/fphar.2021.696472
33. Vaskova E, Ikeda G, Tada Y, Wahlquist C, Mercola M, Yang PC. Sacubitril/valsartan improves cardiac function and decreases myocardial fibrosis via downregulation of exosomal miR-181a in a rodent chronic myocardial infarction model. J Am Heart Assoc. (2020) 9(13):e015640. doi: 10.1161/JAHA.119.015640
34. Liu J, Zheng X, Zhang C, Zhang C, Bu P. Lcz696 alleviates myocardial fibrosis after myocardial infarction through the sFRP-1/wnt/beta-catenin signaling pathway. Front Pharmacol. (2021) 12:724147. doi: 10.3389/fphar.2021.724147
35. Burke RM, Lighthouse JK, Mickelsen DM, Small EM. Sacubitril/valsartan decreases cardiac fibrosis in left ventricle pressure overload by restoring PKG signaling in cardiac fibroblasts. Circ Heart Fail. (2019) 12(4):e005565. doi: 10.1161/CIRCHEARTFAILURE.118.005565
36. Jia T, Wang X, Tang Y, Yu W, Li C, Cui S, et al. Sacubitril ameliorates cardiac fibrosis through inhibiting TRPM7 channel. Front Cell Dev Biol. (2021) 9:760035. doi: 10.3389/fcell.2021.760035
37. Solomon SD, Zile M, Pieske B, Voors A, Shah A, Kraigher-Krainer E, et al. Prospective comparison of AwARBoMOhfwpefI. The angiotensin receptor neprilysin inhibitor LCZ696 in heart failure with preserved ejection fraction: a phase 2 double-blind randomised controlled trial. Lancet. (2012) 380(9851):1387–95. doi: 10.1016/S0140-6736(12)61227-6
38. Jhund PS, Claggett BL, Voors AA, Zile MR, Packer M, Pieske BM, et al. Elevation in high-sensitivity troponin T in heart failure and preserved ejection fraction and influence of treatment with the angiotensin receptor neprilysin inhibitor LCZ696. Circ Heart Fail. (2014) 7(6):953–9. doi: 10.1161/CIRCHEARTFAILURE.114.001427
39. Januzzi JL Jr., Packer M, Claggett B, Liu J, Shah AM, Zile MR, et al. IGFBP7 (insulin-like growth factor-binding protein-7) and neprilysin inhibition in patients with heart failure. Circ Heart Fail. (2018) 11(10):e005133. doi: 10.1161/CIRCHEARTFAILURE.118.005133
40. McMurray JJ, Packer M, Desai AS, Gong J, Lefkowitz MP, Rizkala AR, et al. Angiotensin-neprilysin inhibition versus enalapril in heart failure. N Engl J Med. (2014) 371(11):993–1004. doi: 10.1056/NEJMoa1409077
41. Packer M, McMurray JJ, Desai AS, Gong J, Lefkowitz MP, Rizkala AR, et al. Angiotensin receptor neprilysin inhibition compared with enalapril on the risk of clinical progression in surviving patients with heart failure. Circulation. (2015) 131(1):54–61. doi: 10.1161/CIRCULATIONAHA.114.013748
42. Solomon SD, Claggett B, Desai AS, Packer M, Zile M, Swedberg K, et al. Influence of ejection fraction on outcomes and efficacy of sacubitril/valsartan (LCZ696) in heart failure with reduced ejection fraction: the prospective comparison of ARNI with ACEI to determine impact on global mortality and morbidity in heart failure (PARADIGM-HF) trial. Circ Heart Fail. (2016) 9(3):e002744. doi: 10.1161/CIRCHEARTFAILURE.115.002744
43. Desai AS, McMurray JJ, Packer M, Swedberg K, Rouleau JL, Chen F, et al. Effect of the angiotensin-receptor-neprilysin inhibitor LCZ696 compared with enalapril on mode of death in heart failure patients. Eur Heart J. (2015) 36(30):1990–7. doi: 10.1093/eurheartj/ehv186
44. Jhund PS, Fu M, Bayram E, Chen CH, Negrusz-Kawecka M, Rosenthal A, et al. Efficacy and safety of LCZ696 (sacubitril-valsartan) according to age: insights from PARADIGM-HF. Eur Heart J. (2015) 36(38):2576–84. doi: 10.1093/eurheartj/ehv330
45. Lewis EF, Claggett BL, McMurray JJV, Packer M, Lefkowitz MP, Rouleau JL, et al. Health-Related quality of life outcomes in PARADIGM-HF. Circ Heart Fail. (2017) 10(8):003430. doi: 10.1161/CIRCHEARTFAILURE.116.003430
46. Chandra A, Lewis EF, Claggett BL, Desai AS, Packer M, Zile MR, et al. Effects of sacubitril/valsartan on physical and social activity limitations in patients with heart failure: a secondary analysis of the PARADIGM-HF trial. JAMA Cardiol. (2018) 3(6):498–505. doi: 10.1001/jamacardio.2018.0398
47. Desai AS, Vardeny O, Claggett B, McMurray JJ, Packer M, Swedberg K, et al. Reduced risk of hyperkalemia during treatment of heart failure with mineralocorticoid receptor antagonists by use of sacubitril/valsartan compared with enalapril: a secondary analysis of the PARADIGM-HF trial. JAMA Cardiol. (2017) 2(1):79–85. doi: 10.1001/jamacardio.2016.4733
48. Ma M, Luo Q, Dong X, Cui S, Hocher B, Zeng S, et al. N-terminal prohormone B-type natriuretic peptide variability acts as a predictor of poor prognosis in patients with cardiorenal syndrome type 2. Bioengineered. (2021) 12(2):12407–19. doi: 10.1080/21655979.2021.2005219
49. O'Meara E, Prescott MF, Claggett B, Rouleau JL, Chiang LM, Solomon SD, et al. Independent prognostic value of Serum soluble ST2 measurements in patients with heart failure and a reduced ejection fraction in the PARADIGM-HF trial (prospective comparison of ARNI with ACEI to determine impact on global mortality and morbidity in heart failure). Circ Heart Fail. (2018) 11(5):e004446. doi: 10.1161/CIRCHEARTFAILURE.117.004446
50. Zile MR, O'Meara E, Claggett B, Prescott MF, Solomon SD, Swedberg K, et al. Effects of sacubitril/valsartan on biomarkers of extracellular matrix regulation in patients with HFrEF. J Am Coll Cardiol. (2019) 73(7):795–806. doi: 10.1016/j.jacc.2018.11.042
51. Solomon SD, McMurray JJV, Anand IS, Ge J, Lam CSP, Maggioni AP, et al. Angiotensin-Neprilysin inhibition in heart failure with preserved ejection fraction. N Engl J Med. (2019) 381(17):1609–20. doi: 10.1056/NEJMoa1908655
52. Solomon SD, Vaduganathan M BLC, Packer M, Zile M, Swedberg K, Rouleau J MAP, et al. Sacubitril/valsartan across the Spectrum of ejection fraction in heart failure. Circulation. (2020) 141(5):352–61. doi: 10.1161/CIRCULATIONAHA.119.044586
53. McMurray JJV, Jackson AM, Lam CSP, Redfield MM, Anand IS, Ge J, et al. Effects of sacubitril-valsartan versus valsartan in women compared with men with heart failure and preserved ejection fraction: insights from PARAGON-HF. Circulation. (2020) 141(5):338–51. doi: 10.1161/CIRCULATIONAHA.119.044491
54. Causland FR M, Lefkowitz MP, Claggett B, Anavekar NS, Senni M, Gori M, et al. Angiotensin-Neprilysin inhibition and renal outcomes in heart failure with preserved ejection fraction. Circulation. (2020) 142(13):1236–45. doi: 10.1161/circulationaha.120.047643
55. Selvaraj S, Claggett BL, Packer M, Zannad F, Anand IS, Pieske B, et al. Effects of sacubitril/valsartan on Serum lipids in heart failure with preserved ejection fraction. J Am Heart Assoc. (2021) 10(17):e022069. doi: 10.1161/JAHA.121.022069
56. Cunningham JW, Claggett BL, O'Meara E, Prescott MF, Pfeffer MA, Shah SJ, et al. Effect of sacubitril/valsartan on biomarkers of extracellular matrix regulation in patients with HFpEF. J Am Coll Cardiol. (2020) 76(5):503–14. doi: 10.1016/j.jacc.2020.05.072
57. Wachter R, Senni M, Belohlavek J, Straburzynska-Migaj E, Witte KK, Kobalava Z, et al. Initiation of sacubitril/valsartan in haemodynamically stabilised heart failure patients in hospital or early after discharge: primary results of the randomised TRANSITION study. Eur J Heart Fail. (2019) 21(8):998–1007. doi: 10.1002/ejhf.1498
58. Senni M, Wachter R, Witte KK, Straburzynska-Migaj E, Belohlavek J, Fonseca C, et al. Initiation of sacubitril/valsartan shortly after hospitalisation for acutely decompensated heart failure in patients with newly diagnosed (de novo) heart failure: a subgroup analysis of the TRANSITION study. Eur J Heart Fail. (2020) 22(2):303–12. doi: 10.1002/ejhf.1670
59. Kang DH, Park SJ, Shin SH, Hong GR, Lee S, Kim MS, et al. Angiotensin receptor neprilysin inhibitor for functional mitral regurgitation. Circulation. (2019) 139(11):1354–65. doi: 10.1161/circulationaha.118.037077
60. Velazquez EJ, Morrow DA, DeVore AD, Duffy CI, Ambrosy AP, McCague K, et al. Angiotensin-Neprilysin inhibition in acute decompensated heart failure. N Engl J Med. (2019) 380(6):539–48. doi: 10.1056/NEJMoa1812851
61. Morrow DA, Velazquez EJ, DeVore AD, Prescott MF, Duffy CI, Gurmu Y, et al. Cardiovascular biomarkers in patients with acute decompensated heart failure randomized to sacubitril-valsartan or enalapril in the PIONEER-HF trial. Eur Heart J. (2019) 40(40):3345–52. doi: 10.1093/eurheartj/ehz240
62. DeVore AD, Braunwald E, Morrow DA, Duffy CI, Ambrosy AP, Chakraborty H, et al. Initiation of angiotensin-neprilysin inhibition after acute decompensated heart failure: secondary analysis of the open-label extension of the PIONEER-HF trial. JAMA Cardiol. (2020) 5(2):202–7. doi: 10.1001/jamacardio.2019.4665
63. Mitchell GF, Solomon SD, Shah AM, Claggett BL, Fang JC, Izzo J, et al. Hemodynamic effects of sacubitril-valsartan versus enalapril in patients with heart failure in the EVALUATE-HF study: effect modification by left ventricular ejection fraction and sex. Circ Heart Fail. (2021) 14(3):e007891. doi: 10.1161/circheartfailure.120.007891
64. Desai AS, Solomon SD, Shah AM, Claggett BL, Fang JC, Izzo J, et al. Effect of sacubitril-valsartan vs enalapril on aortic stiffness in patients with heart failure and reduced ejection fraction: a randomized clinical trial. Jama. (2019) 322(11):1077–84. doi: 10.1001/jama.2019.12843
65. Murphy SP, Prescott MF, Maisel AS, Butler J, Piña IL, Felker GM, et al. Association between angiotensin receptor-neprilysin inhibition, cardiovascular biomarkers, and cardiac remodeling in heart failure with reduced ejection fraction. Circ Heart Fail. (2021) 14(6):e008410. doi: 10.1161/circheartfailure.120.008410
66. Murphy SP, Prescott MF, Camacho A, Iyer SR, Maisel AS, Felker GM, et al. Atrial natriuretic peptide and treatment with sacubitril/valsartan in heart failure with reduced ejection fraction. JACC Heart Fail. (2021) 9(2):127–36. doi: 10.1016/j.jchf.2020.09.013
67. Piña IL, Camacho A, Ibrahim NE, Felker GM, Butler J, Maisel AS, et al. Improvement of health Status following initiation of sacubitril/valsartan in heart failure and reduced ejection fraction. JACC Heart Fail. (2021) 9(1):42–51. doi: 10.1016/j.jchf.2020.09.012
68. Gandhi PU, Chow SL, Rector TS, Krum H, Gaggin HK, McMurray JJ, et al. Prognostic value of insulin-like growth factor-binding protein 7 in patients with heart failure and preserved ejection fraction. J Card Fail. (2017) 23(1):20–8. doi: 10.1016/j.cardfail.2016.06.006
69. McMurray JJ, Packer M, Desai AS, Gong J, Lefkowitz MP, Rizkala AR, et al. Dual angiotensin receptor and neprilysin inhibition as an alternative to angiotensin-converting enzyme inhibition in patients with chronic systolic heart failure: rationale for and design of the prospective comparison of ARNI with ACEI to determine impact on global mortality and morbidity in heart failure trial (PARADIGM-HF). Eur J Heart Fail. (2013) 15(9):1062–73. doi: 10.1093/eurjhf/hft052
70. Lewis EF. Assessing the impact of heart failure therapeutics on quality of life and functional capacity. Curr Treat Options Cardiovasc Med. (2013) 15(4):425–36. doi: 10.1007/s11936-013-0249-2
71. Butler J, Hamo CE, Udelson JE, Pitt B, Yancy C, Shah SJ, et al. Exploring new endpoints for patients with heart failure with preserved ejection fraction. Circ Heart Fail. (2016) 9(11):e003358. doi: 10.1161/CIRCHEARTFAILURE.116.003358
72. Solomon SD, Rizkala AR, Lefkowitz MP, Shi VC, Gong J, Anavekar N, et al. Baseline characteristics of patients with heart failure and preserved ejection fraction in the PARAGON-HF trial. Circ Heart Fail. (2018) 11(7):e004962. doi: 10.1161/CIRCHEARTFAILURE.118.004962
73. Ambrosy AP, Mentz RJ, Fiuzat M, Cleland JGF, Greene SJ, O'Connor CM, et al. The role of angiotensin receptor-neprilysin inhibitors in cardiovascular disease-existing evidence, knowledge gaps, and future directions. Eur J Heart Fail. (2018) 20(6):963–72. doi: 10.1002/ejhf.1159
74. Pascual-Figal D, Wachter R, Senni M, Belohlavek J, Noe A, Carr D, et al. Rationale and design of TRANSITION: a randomized trial of pre-discharge vs. Post-discharge initiation of sacubitril/valsartan. ESC Heart Fail. (2018) 5(2):327–36. doi: 10.1002/ehf2.12246
75. Ambrosy AP, Braunwald E, Morrow DA, DeVore AD, McCague K, Meng X, et al. Angiotensin receptor-neprilysin inhibition based on history of heart failure and use of renin-angiotensin system antagonists. J Am Coll Cardiol. (2020) 76(9):1034–48. doi: 10.1016/j.jacc.2020.06.073
76. Berg DD, Braunwald E, DeVore AD, Lala A, Pinney SP, Duffy CI, et al. Efficacy and safety of sacubitril/valsartan by dose level achieved in the PIONEER-HF trial. JACC Heart Fail. (2020) 8(10):834–43. doi: 10.1016/j.jchf.2020.06.008
77. Berardi C, Braunwald E, Morrow DA, Mulder HS, Duffy CI, O'Brien TX, et al. Angiotensin-Neprilysin inhibition in black Americans: data from the PIONEER-HF trial. JACC Heart Fail. (2020) 8(10):859–66. doi: 10.1016/j.jchf.2020.06.019
78. Januzzi JL J, Prescott MF, Butler J, Felker GM, Maisel AS, McCague K, et al. Association of change in N-terminal pro-B-type natriuretic peptide following initiation of sacubitril-valsartan treatment with cardiac structure and function in patients with heart failure with reduced ejection fraction. JAMA. (2019) 322(11):1085–95. doi: 10.1001/jama.2019.12821
79. Khan MS, Felker GM, Piña IL, Camacho A, Bapat D, Ibrahim NE, et al. Reverse cardiac remodeling following initiation of sacubitril/valsartan in patients with heart failure with and without diabetes. JACC Heart Fail. (2021) 9(2):137–45. doi: 10.1016/j.jchf.2020.09.014
80. Ibrahim NE, Piña IL, Camacho A, Bapat D, Felker GM, Maisel AS, et al. Racial and ethnic differences in biomarkers, health Status, and cardiac remodeling in patients with heart failure with reduced ejection fraction treated with sacubitril/valsartan. Circ Heart Fail. (2020) 13(11):e007829. doi: 10.1161/circheartfailure.120.007829
81. Bouali Y, Galli E, Paven E, Laurin C, Arnaud H, Oger E, et al. Impact of sacubitril/valsartan on systolic heart failure: right heart location and clustering analysis. Adv Clin Exp Med. (2022) 31(2):109–19. doi: 10.17219/acem/143433
82. Carluccio E, Dini FL, Bitto R, Ciccarelli M, Correale M, D'Agostino A, et al. Working group on heart failure of the Italian society of C. Benefit from sacubitril/valsartan is associated with hemodynamic improvement in heart failure with reduced ejection fraction: an echocardiographic study. Int J Cardiol. (2022) 350:62–8. doi: 10.1016/j.ijcard.2022.01.004
83. Mann DL, Givertz MM, Vader JM, Starling RC, Shah P, McNulty SE, et al. Effect of treatment with sacubitril/valsartan in patients with advanced heart failure and reduced ejection fraction: a randomized clinical trial. JAMA Cardiol. (2022) 7(1):17–25. doi: 10.1001/jamacardio.2021.4567
84. Lee YH, Chiou WR, Hsu CY, Lin PL, Liang HW, Chung FP, et al. Different left ventricular remodelling patterns and clinical outcomes between non-ischaemic and ischaemic aetiologies in heart failure patients receiving sacubitril/valsartan treatment. Eur Heart J Cardiovasc Pharmacother. (2022) 8(2):118–29. doi: 10.1093/ehjcvp/pvaa125
85. Kario K, Sun N, Chiang FT, Supasyndh O, Baek SH, Inubushi-Molessa A, et al. Efficacy and safety of LCZ696, a first-in-class angiotensin receptor neprilysin inhibitor, in Asian patients with hypertension: a randomized, double-blind, placebo-controlled study. Hypertension. (2014) 63(4):698–705. doi: 10.1161/hypertensionaha.113.02002
86. Williams B, Cockcroft JR, Kario K, Zappe DH, Brunel PC, Wang Q, et al. Effects of sacubitril/valsartan versus olmesartan on central hemodynamics in the elderly with systolic hypertension: the PARAMETER study. Hypertension. (2017) 69(3):411–20. doi: 10.1161/hypertensionaha.116.08556
87. Ruilope LM, Dukat A, Böhm M, Lacourcière Y, Gong J, Lefkowitz MP. Blood-pressure reduction with LCZ696, a novel dual-acting inhibitor of the angiotensin II receptor and neprilysin: a randomised, double-blind, placebo-controlled, active comparator study. Lancet. 2010;375(9722):1255–66. doi: 10.1016/s0140-6736(09)61966-8
88. Li W, Gong M, Yu Q, Liu R, Chen K, Lv W, et al. Efficacy of angiotensin receptor neprilysin inhibitor in Asian patients with refractory hypertension. J Clin Hypertens (Greenwich). (2022) 24(4):449–56. doi: 10.1111/jch.14454
89. Wang B, Wang GH, Ding XX, Tang HX, Zheng J, Liu BC, et al. Effects of sacubitril/valsartan on resistant hypertension and myocardial work in hemodialysis patients. J Clin Hypertens (Greenwich). (2022) 24(3):300–8. doi: 10.1111/jch.14422
90. Wang TD, Tan RS, Lee HY, Ihm SH, Rhee MY, Tomlinson B, et al. Effects of sacubitril/valsartan (LCZ696) on natriuresis, diuresis, blood pressures, and NT-proBNP in salt-sensitive hypertension. Hypertension. (2017) 69(1):32–41. doi: 10.1161/hypertensionaha.116.08484
91. Jackson AM, Jhund PS, Anand IS, Düngen HD, Lam CSP, Lefkowitz MP, et al. Sacubitril-valsartan as a treatment for apparent resistant hypertension in patients with heart failure and preserved ejection fraction. Eur Heart J. (2021) 42(36):3741–52. doi: 10.1093/eurheartj/ehab499
92. Martens P, Nuyens D, Rivero-Ayerza M, Van Herendael H, Vercammen J, Ceyssens W, et al. Sacubitril/valsartan reduces ventricular arrhythmias in parallel with left ventricular reverse remodeling in heart failure with reduced ejection fraction. Clin Res Cardiol. (2019) 108(10):1074–82. doi: 10.1007/s00392-019-01440-y
93. Valentim Gonçalves A, Pereira-da-Silva T, Galrinho A, Rio P, Moura Branco L, Soares R, et al. Antiarrhythmic effect of sacubitril-valsartan: cause or consequence of clinical improvement? J Clin Med. (2019) 8(6):869. doi: 10.3390/jcm8060869
94. de Diego C, González-Torres L, Núñez JM, Centurión Inda R, Martin-Langerwerf DA, Sangio AD, et al. Effects of angiotensin-neprilysin inhibition compared to angiotensin inhibition on ventricular arrhythmias in reduced ejection fraction patients under continuous remote monitoring of implantable defibrillator devices. Heart Rhythm. (2018) 15(3):395–402. doi: 10.1016/j.hrthm.2017.11.012
95. Chang PC, Wo HT, Lee HL, Lin SF, Chu Y, Wen MS, et al. Sacubitril/valsartan therapy ameliorates ventricular tachyarrhythmia inducibility in a rabbit myocardial infarction model. J Card Fail. (2020) 26(6):527–37. doi: 10.1016/j.cardfail.2020.03.007
96. Chang PC, Lin SF, Chu Y, Wo HT, Lee HL, Huang YC, et al. LCZ696 Therapy reduces ventricular tachyarrhythmia inducibility in a myocardial infarction-induced heart failure rat model. Cardiovasc Ther. (2019) 2019:6032631. doi: 10.1155/2019/6032631
97. Wang Q, Zhuo C, Xia Q, Jiang J, Wu B, Zhou D, et al. Sacubitril/valsartan can reduce atrial fibrillation recurrence after catheter ablation in patients with persistent atrial fibrillation. Cardiovasc Drugs Ther. (2022). doi: 10.1007/s10557-022-07315-1
98. Liu X, Liu H, Wang L, Zhang L, Xu Q. Role of sacubitril-valsartan in the prevention of atrial fibrillation occurrence in patients with heart failure: a systematic review and meta-analysis of randomized controlled trials. PLoS One. (2022) 17(1):e0263131. doi: 10.1371/journal.pone.0263131
99. Burgdorf C, Brockmöller J, Strampe H, Januszewski M, Remppis BA. Reduction of pulmonary hypertension after transition to sacubitril/valsartan in patients with heart failure with preserved ejection fraction. Front Cardiovasc Med. (2021) 8:734697. doi: 10.3389/fcvm.2021.734697
100. Walker AM, Patel PA, Rajwani A, Groves D, Denby C, Kearney L, et al. Diabetes mellitus is associated with adverse structural and functional cardiac remodelling in chronic heart failure with reduced ejection fraction. Diab Vasc Dis Res. (2016) 13(5):331–40. doi: 10.1177/1479164116653342
101. Kristensen SL, Preiss D, Jhund PS, Squire I, Cardoso JS, Merkely B, et al. Risk related to Pre-diabetes Mellitus and diabetes Mellitus in heart failure with reduced ejection fraction: insights from prospective comparison of ARNI with ACEI to determine impact on global mortality and morbidity in heart failure trial. Circ Heart Fail. (2016) 9(1):002560. doi: 10.1161/circheartfailure.115.002560
102. Packer M, Claggett B, Lefkowitz MP, McMurray JJV, Rouleau JL, Solomon SD, et al. Effect of neprilysin inhibition on renal function in patients with type 2 diabetes and chronic heart failure who are receiving target doses of inhibitors of the renin-angiotensin system: a secondary analysis of the PARADIGM-HF trial. Lancet Diabetes Endocrinol. (2018) 6(7):547–54. doi: 10.1016/s2213-8587(18)30100-1
103. Peikert A, Vaduganathan M, Mc Causland F, Claggett BL, Chatur S, Packer M, et al. Effects of sacubitril/valsartan versus valsartan on renal function in patients with and without diabetes and heart failure with preserved ejection fraction: insights from PARAGON-HF. Eur J Heart Fail. (2022) 24(5):794–803. doi: 10.1002/ejhf.2450
104. Damman K, Gori M, Claggett B, Jhund PS, Senni M, Lefkowitz MP, et al. Renal effects and associated outcomes during angiotensin-neprilysin inhibition in heart failure. JACC Heart Fail. (2018) 6(6):489–98. doi: 10.1016/j.jchf.2018.02.004
105. Kang H, Zhang J, Zhang X, Qin G, Wang K, Deng Z, et al. Effects of sacubitril/valsartan in patients with heart failure and chronic kidney disease: a meta-analysis. Eur J Pharmacol. (2020) 884:173444. doi: 10.1016/j.ejphar.2020.173444
106. Li LY, Lou Q, Liu GZ, Lv JC, Yun FX, Li TK, et al. Sacubitril/valsartan attenuates atrial electrical and structural remodelling in a rabbit model of atrial fibrillation. Eur J Pharmacol. (2020) 881:173120. doi: 10.1016/j.ejphar.2020.173120
107. Li SN, Zhang JR, Zhou L, Xi H, Li CY, Zhao L. Sacubitril/valsartan decreases atrial fibrillation susceptibility by inhibiting angiotensin II-induced atrial fibrosis through p-Smad2/3, p-JNK, and p-p38 signaling pathways. J Cardiovasc Transl Res. (2021) 15(1):131–42. doi: 10.1007/s12265-021-10137-5
108. Chaumais MC, Djessas MRA, Thuillet R, Cumont A, Tu L, Hebert G, et al. Additive protective effects of sacubitril/valsartan and bosentan on vascular remodelling in experimental pulmonary hypertension. Cardiovasc Res. (2021) 117(5):1391–401. doi: 10.1093/cvr/cvaa200
109. Clements RT, Vang A, Fernandez-Nicolas A, Kue NR, Mancini TJ, Morrison AR, et al. Treatment of pulmonary hypertension with angiotensin II receptor blocker and neprilysin inhibitor sacubitril/valsartan. Circ Heart Fail. (2019) 12(11):e005819. doi: 10.1161/circheartfailure.119.005819
110. Sharifi Kia D, Benza E, Bachman TN, Tushak C, Kim K, Simon MA. Angiotensin receptor-neprilysin inhibition attenuates right ventricular remodeling in pulmonary hypertension. J Am Heart Assoc. (2020) 9(13):e015708. doi: 10.1161/jaha.119.015708
111. Andersen S, Axelsen JB, Ringgaard S, Nyengaard JR, Hyldebrandt JA, Bogaard HJ, et al. Effects of combined angiotensin II receptor antagonism and neprilysin inhibition in experimental pulmonary hypertension and right ventricular failure. Int J Cardiol. (2019) 293:203–10. doi: 10.1016/j.ijcard.2019.06.065
112. Roksnoer LC, van Veghel R, Clahsen-van Groningen MC, de Vries R, Garrelds IM, Bhaggoe UM, et al. Blood pressure-independent renoprotection in diabetic rats treated with AT1 receptor-neprilysin inhibition compared with AT1 receptor blockade alone. Clin Sci (Lond). (2016) 130(14):1209–20. doi: 10.1042/cs20160197
113. Habibi J, Aroor AR, Das NA, Manrique-Acevedo CM, Johnson MS, Hayden MR, et al. The combination of a neprilysin inhibitor (sacubitril) and angiotensin-II receptor blocker (valsartan) attenuates glomerular and tubular injury in the zucker obese rat. Cardiovasc Diabetol. (2019) 18(1):40. doi: 10.1186/s12933-019-0847-8
114. Davidson EP, Coppey LJ, Shevalye H, Obrosov A, Yorek MA. Vascular and neural complications in type 2 diabetic rats: improvement by sacubitril/valsartan greater than valsartan alone. Diabetes. (2018) 67(8):1616–26. doi: 10.2337/db18-0062
115. Li Y, Kang L, Rong K, Zhang Y, Suo Y, Yuan M, et al. Renal protective effects and mechanisms of the angiotensin receptor-neprilysin inhibitor LCZ696 in mice with cardiorenal syndrome. Life Sci. (2021) 280:119692. doi: 10.1016/j.lfs.2021.119692
116. Sabbah HN, Zhang K, Gupta RC, Xu J, Singh-Gupta V. Effects of angiotensin-neprilysin inhibition in canines with experimentally induced cardiorenal syndrome. J Card Fail. (2020) 26(11):987–97. doi: 10.1016/j.cardfail.2020.08.009
117. Yancy CW, Jessup M, Bozkurt B, Butler J, Casey DE Jr., Colvin MM, et al. 2017 ACC/AHA/HFSA focused update of the 2013 ACCF/AHA guideline for the management of heart failure: a report of the American college of cardiology/American heart association task force on clinical practice guidelines and the heart failure society of America. Circulation. (2017) 136(6):e137–161. doi: 10.1161/cir.0000000000000509
118. Zern EK, Cheng S, Wolfson AM, Hamilton MA, Zile MR, Solomon SD, et al. Angiotensin receptor-neprilysin inhibitor therapy reverses pulmonary hypertension in End-stage heart failure patients awaiting transplantation. Circ Heart Fail. (2020) 13(2):e006696. doi: 10.1161/circheartfailure.119.006696
119. Seferovic JP, Claggett B, Seidelmann SB, Seely EW, Packer M, Zile MR, et al. Effect of sacubitril/valsartan versus enalapril on glycaemic control in patients with heart failure and diabetes: a post-hoc analysis from the PARADIGM-HF trial. Lancet Diabetes Endocrinol. (2017) 5(5):333–40. doi: 10.1016/s2213-8587(17)30087-6
Keywords: heart failure, sacubitril/valsartan, cardiovascular, clinical application, basic medical research
Citation: Zhang M, Zou Y, Li Y, Wang H, Sun W and Liu B (2023) The history and mystery of sacubitril/valsartan: From clinical trial to the real world. Front. Cardiovasc. Med. 10:1102521. doi: 10.3389/fcvm.2023.1102521
Received: 19 November 2022; Accepted: 13 March 2023;
Published: 28 March 2023.
Edited by:
Xiaofeng Yang, Temple University, United StatesReviewed by:
Savina Nodari, University of Brescia, ItalyGopal Chandra Ghosh, Rabindranath Thakur Diagnostic and Medical Care Center, India
© 2023 Sun, Zhang, Zou, Li, Wang and Liu. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Wei Sun c3Vud2VpOTExMTI2QGpsdS5lZHUuY24= Bin Liu bGl1YmluMzMzM0B2aXAuc2luYS5jb20=
†These authors have contributed equally to this work
Specialty Section: This article was submitted to Cardiovascular Pharmacology and Drug Discovery, a section of the journal Frontiers in Cardiovascular Medicine