 Fabiana Lucà1*
Fabiana Lucà1* Furio Colivicchi2
Furio Colivicchi2 Fabrizio Oliva3Maurizio Abrignani4Giorgio Caretta5
Fabrizio Oliva3Maurizio Abrignani4Giorgio Caretta5 Stefania Angela Di Fusco2Simona Giubilato6
Stefania Angela Di Fusco2Simona Giubilato6 Stefano Cornara7
Stefano Cornara7 Concetta Di Nora8Andrea Pozzi8Irene Di Matteo3Anna Pilleri10Carmelo Massimiliano Rao1
Concetta Di Nora8Andrea Pozzi8Irene Di Matteo3Anna Pilleri10Carmelo Massimiliano Rao1 Antonio Parlavecchio1
Antonio Parlavecchio1 Roberto Ceravolo11Francesco Antonio Benedetto1Roberta Rossini12
Roberto Ceravolo11Francesco Antonio Benedetto1Roberta Rossini12 Raimondo Calvanese13
Raimondo Calvanese13 Sandro Gelsomino14Carmine Riccio15
Sandro Gelsomino14Carmine Riccio15 Michele Massimo Gulizia15On Behalf of Management and Quality Working Group ANMCO Cardiac Chronic Diseases ANMCO and Arrhythmias Working Group ANMCO
Michele Massimo Gulizia15On Behalf of Management and Quality Working Group ANMCO Cardiac Chronic Diseases ANMCO and Arrhythmias Working Group ANMCO
- 1Cardiology Department, Grande Ospedale Metropolitano di Reggio Calabria, GOM, Azienda Ospedaliera Bianchi Melacrino Morelli, Italy
- 2Cardiology Division, San Filippo Neri Hospital, ASL Roma 1, Roma, Italy
- 3De Gasperis Cardio Center, ASST Niguarda Hospital, Milano, Italy
- 4Cardiology Unit, Paolo Borsellino Hospital, ASP Trapani, Marsala, Italy
- 5Cardiology Unit, Sant'Andrea Hospital, ASL 5 Liguria, La Spezia, Italy
- 6Cardiology Division Cannizzaro Hospital, Catania, Italy
- 7Cardiology Division San Paolo Hospital, ASL 2, Savona, Italy
- 8Cardiology Division, Maria della Misericordia di Udine, Italy
- 9Cardiology Division, Valduce Hospital, Como, Italy
- 10Cardiology Division, Brotzu Hospital, Cagliari, Italy
- 11Cardiology Division, Giovanni Paolo II Hospital, Lamezia Terme, Italy
- 12Cardiology Division S. Croce e Carle Hospital, Cuneo, Italy
- 13Cardiology Division, Ospedale del Mare, Napoli, Italy
- 14Cardiothoracic Department, Maastricht University, Maastricht, The Netherlands
- 15Cardiovascular Department, A.O.R.N. Sant'Anna e San Sebastiano, Caserta, Italy
- 16Cardiology Department, Garibaldi Nesima Hospital, Catania, Italy
Intracranial hemorrhage (ICH) is considered a potentially severe complication of oral anticoagulants (OACs) and antiplatelet therapy (APT). Patients with atrial fibrillation (AF) who survived ICH present both an increased ischemic and bleeding risk. Due to its lethality, initiating or reinitiating OACs in ICH survivors with AF is challenging. Since ICH recurrence may be life-threatening, patients who experience an ICH are often not treated with OACs, and thus remain at a higher risk of thromboembolic events. It is worthy of mention that subjects with a recent ICH and AF have been scarcely enrolled in randomized controlled trials (RCTs) on ischemic stroke risk management in AF. Nevertheless, in observational studies, stroke incidence and mortality of patients with AF who survived ICH had been shown to be significantly reduced among those treated with OACs. However, the risk of hemorrhagic events, including recurrent ICH, was not necessarily increased, especially in patients with post-traumatic ICH. The optimal timing of anticoagulation initiation or restarting after an ICH in AF patients is also largely debated. Finally, the left atrial appendage occlusion option should be evaluated in AF patients with a very high risk of recurrent ICH. Overall, an interdisciplinary unit consisting of cardiologists, neurologists, neuroradiologists, neurosurgeons, patients, and their families should be involved in management decisions. According to available evidence, this review outlines the most appropriate anticoagulation strategies after an ICH that should be adopted to treat this neglected subset of patients.
1. Introduction
Intracranial Hemorrhage (ICH) is a well-recognized complication of oral anticoagulants (OACs) and antiplatelet therapy (APT) (1, 2). In patients with atrial fibrillation (AF) treated with OACs who survived a previous ICH, the risk of recurrent bleeding ranges from 1.3% to 7.4% (3, 4). It has been estimated that an annual rate of ICH of 0.3%–0.6% and 0.1%–0.2% in patients receiving vitamin K antagonists (VKA) and Direct oral anticoagulants (DOACs), respectively (5–7).
Therefore, OACs therapy in ICH survivors with AF is a clinical challenge. The risk of recurrent ICH might be balanced against the thromboembolic risk related to AF if patients are not adequately treated (8).
Although clinicians often encounter this issue in clinical practice, patients with a recent ICH and AF are poorly or not represented in randomized controlled trials (RCTs) on ischemic stroke risk management in AF (9).
Furthermore, the limited data available on whether AF patients surviving an ICH may benefit from OACs are conflicting (10).
It would be advisable to carefully consider the presence of specific risk factors, as well as the causes of ICH and neuroimaging findings in deciding whether to restart or initiate an OACs regimen after an ICH.
Finally, left atrial appendage (LAA) occlusion should be evaluated in AF patients with a high risk of recurrent ICH (11). This systematic review aims to summarize ICH's nosology and epidemiology and report available evidence on anticoagulation management after ICH in patients with AF. We also outline and discuss the most appropriate therapeutic strategies in patients with AF who have survived ICH, as national and international experts suggested.
2. Materials and methods
2.1. Search strategy
Literature sources have been investigated according to the rules of Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) (12).
Three authors (CD, IDM, AP) established the search strategy, which was then approved by another author (FL). PubMed, Medline, and SCOPUS databases have been used. The search was performed including the following terms (novel oral anticoagulants OR “NOACs” OR direct-acting oral anticoagulants OR DOACs OR anticoagulant drugs OR Vitamin K antagonists OR VKA) AND “atrial fibrillation” AND (Hemorrhagic stroke OR intracerebral hemorrhages) AND percutaneous left atrial appendage closure. Titles and abstracts of all articles published between January 2005 and March 2022 were initially analyzed. The literature was restricted to articles published in English. Three expert investigators (FC, SG, MG) performed queries and identified articles. The PRISMA checklist is reported in the Supplemental Material. The protocol has been registered on Prospero (n° 350413).
Additional articles found as references in original papers were crosschecked for inclusion.
2.2. Selection criteria and quality assessment
RCTs have not been included in the analysis. The inclusion criteria of the studies are listed below:
(1) human studies; (2) full articles about AF and ICH; (3) adequate information reported about the patient's assessment. Exclusion criteria were: (1) experimental animal (2) case reports, reviews, and (5) partial information for meta-analysis.
Two authors (FL and SADF) were responsible for selecting and extracting the studies and information, and outcomes of patients. Two reviewers (S.G. and MMG) independently evaluated the eligibility.
2.3. Results
The PRISMA flow diagram reporting the study selection process and exclusion reasons are represented in Figure 1. The number of studies screened was 15,234.
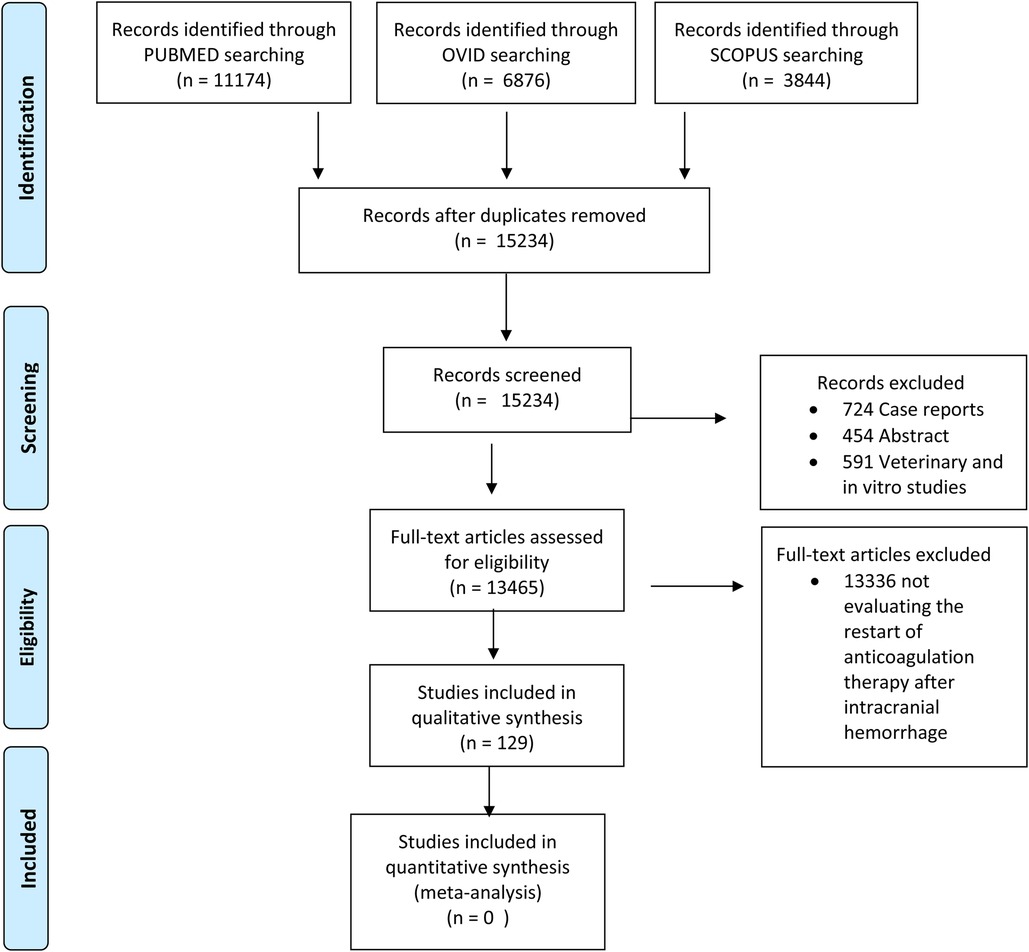
Figure 1. Prisma flow diagram.
Of these articles, 724 have been excluded as case reports, 454 as abstracts, and 591 as animal and experimental studies. Therefore, 13,465 full-text articles underwent further screening after the exclusion of 13,336 results which were not considered to be on-topic and suitable for other evaluation. Subsequently, 129 articles were further assessed.
3. Discussion
3.1. ICH nosology and etiology
ICH accounts for 10%–20% of all strokes and is correlated to higher mortality and a worse functional outcome (13). Three types of ICH have been described: (1) epidural hemorrhage (EDH)/subdural hemorrhage (SDH), (2) subarachnoid hemorrhage (SAH), (3) and intraparenchymal hemorrhage (IPH)/intraventricular hemorrhage (IVH) (14).
ICH is classified conventionally as primary or secondary based on the leading causes. A primary ICH due to hypertensive injury or cerebral amyloid angiopathy (CAA) damage, resulting in the spontaneous rupture of small vessels, has been reported in 80% of cases (15).
In this regard, cerebral vasculopathy due to chronic hypertension has been described to be the leading cause of ICH (16).
The small, penetrating arteries arising from the anterior, middle, or posterior cerebral arteries and from basilar branches have been reported as the most common site of hypertensive ICH (15). Conversely, it has been well-assessed that CAA is the leading cause of ICH in elderly people (17).
What in the classification of ICH should be considered most is its location in order to distinguish lobar or non-lobar and supratentorial or infratentorial (18). It has been shown that CAA is a common cause of lobar ICH (19). The rupture of cortical medium and small arterioles is frequently due to beta-amyloid deposition, causing both asymptomatic microhemorrhages and symptomatic lobar hemorrhages (20).
Basal ganglia, thalamus, pons, cerebellum, and the subcortical white matter have been described as the most common sites involved with hypertensive ICH characterized by the lipohyalinosis of small perforating arteries occurrence (21).
On the contrary arteriovenous malformations, cavernous angiomas, cerebral aneurysms, and aortic-venous fistulae, neoplasms, hemorrhagic conversion of an ischemic stroke, vasculitis, drug abuse, and bleeding diathesis have been reported as congenital and acquired causes of secondary ICH (22).
SAH, which is less common, occurs when bleeding takes place between the inner and outer layers of the tissue surrounding the brain.
A spontaneous occurrence has been described. However, head trauma could also result in SAH (23). Spontaneous (primary) SAH usually results from ruptured intracranial aneurysms. A congenital saccular or berry aneurysm is the cause of SAH in about 85% of patients (24). Aneurysmal hemorrhage may occur at any age ranging mainly from ages 40 to 65 (23). Brain aneurysms have been associated with smoking, female sex, and high blood pressure. Less common causes are arteriovenous malformations, mycotic aneurysms, bleeding disorders, and the use of blood thinners (23, 24).
3.2. Epidemiological aspects and risk factors of hemorrhagic stroke
3.2.1. Incidence
ICH has a very variable incidence in relation to geographical areas (it accounts for about 8%–15% of strokes in Western countries and more in developing ones) and ethnic groups (with the greatest incidence among Asians) (25). Its incidence increases with advancing age and is higher in men (25–27). It has also been associated with overweight, tobacco use, and alcohol assumption. Besides, male patients with ICH are younger than female patients (28).
3.2.2. Time trends
Worldwide, the absolute number of ICH cases is increasing, with an increase in incidence in the poorest countries and a reduction in China (29) and Western countries, likely due to better blood pressure control at the population level (25). In the Tromsø Study in Norway, ICH occurrence dropped in women between 1994 and 2013, with a reduction in non-lobar ICH, while incidence rates in men remained stable (IRR: 1.27, 95% CI: 0.69–2.31) (30). In a Danish study, age- and sex-related rates of ICH were inferior in the population cohort ranging between 33% to 28 in the years 2004–2005 and 2016–2017 respectively (31). Among patients aged ≥70 years, a statistically non-significant time trend in hemorrhagic stroke incidence reduction has been observed. However, evidence in incidence trends is conflicting. The Dijon register (27) shows that the incidence of ICH has remained relatively stable from 1985 to 2008 (12.4/100,000/year). In recent data from this study, stroke rates increased over time from 1987 to 2012 independently from the subtype of stroke (32), and the sex gap in incidence remained unchanged (27). In the French national hospital discharge database, from 2008 to 2014, the incidence of subjects referred to the hospital for hemorrhagic stroke was not dependent on age and sex, and it was stable (33). These data can be explained by the aging of the population, in conjunction with increased use of antithrombotic therapy and the increased presence of CAA, whose estimated prevalence in patients with ICH is 14.7% (34).
3.2.3. Risk factors
It has been shown that old age, male sex, Asian ethnicity, and the presence of CAA are non-modifiable risk factors for ICH. Chronic kidney failure (CKD), which is a marker of small cerebral vessel disease (25), is a further condition associated with increased ICH risk. Hypertension (30), smoking, and excessive alcohol consumption have been reported as modifiable factors associated with about 9 out of 10 cases of ICH. A possible role of low-density lipoprotein (LDL) cholesterol and triglycerides levels have been hypothesized, although it has not been demonstrated (25). Arterial hypertension boosts the odds of ICH, with very high blood pressure values (systolic blood pressure > 180 mmHg) at a presentation being an independent predictor of deep localization (34). Moreover, it is more strictly correlated with non-lobar than lobar hemorrhage (35). In Denmark, the prevalence of hypertension in the ICH population rose to 66% in the period between 2004 and 2017, probably because of the absence of an appropriate therapy or a suboptimal strategy in most patients (35). In northeast China, the high number of patients with inadequate pressure control has been correlated with significant stroke incidence (36). Regarding the relationship between alcohol exposure and stroke, an alcohol dehydrogenase genotype 1B (ADH1B, rs1229984), heterozygous or homozygous in drinks consumers, has been associated with an increased ICH risk (37).
Notably, recreational drugs with sympathomimetic action (including cocaine, heroin, and amphetamines) have been associated with increased ICH risk (38). The use of antiplatelet agents, mainly if associated with OACs, also increases ICH risk.
3.3. ICH natural history (risk of death or a new stroke, stratification of thrombotic/hemorrhagic risk)
ICH has high morbidity and mortality rates, which at one month is approximately 45% (39).
Although the significant morbidity and mortality have led the scientific community to focus on hemorrhagic stroke management, its prognosis has not improved significantly during the last several decades.
The most important predictors of death are older age, a low score on the Glasgow Coma Scale (40), greater ICH volume, the presence of intraventricular hemorrhage, and deep/infratentorial ICH area (15). Most of these factors are also included in the ICH score, which allows risk estimation at the ICH presentation (40).
A correlation between ICH and the recurrence of bleeding, ischemic events, and other vascular complications has been reported (15).
The rate of recurrent ICH is between 4% and 7% per patient-year, very similar to that of ischemic stroke, and depends on the cause, the presence of comorbid AF, and blood pressure (41).
The site of the first hemorrhage, which is often related to the cause of the hemorrhagic stroke, is also essential (15).
ICH recurrence risk is higher in patients with lobar hemorrhage, which is usually due to CAA.
Overall, patients with bleeding diathesis and those with vascular malformations are likely to have a higher risk of ICH recurrence.
This evidence could have important implications for the approach to secondary prevention of stroke and other thromboembolic events regarding whether or not to reintroduce antithrombotic therapy (42).
Moreover, blood pressure during follow-up has a crucial role in determining the risk of recurrence. The results of the PROGRESS trial demonstrated that reducing blood pressure, even within the “normal” range, caused a lower risk of recurrent stroke, particularly in those who entered the study for hemorrhagic stroke (43).
3.4. ICH and AF
ICH risk in patients with AF is related to OACs treatment. In the Dijon Stroke Registry (2006–2017), AF has been reported in 97 of 444 ICH patients (21.9%).
Among them, AF was known and treated with OACs in 65 patients (14.6%) while 13 subjects (2.9%) had unrecognized AF (44). An increase in the incidence of FA was observed between 2006 and 2017, rising from 17.2 to 25.8%. Furthermore, the percentage of patients treated with OACs and the percentage of new AF significantly increased over this decade (44). In contrast, patients without AF were younger (mean age: 70 vs. 78 years) and had a lower CHA2DS2-VASc score (2.5 vs. 3.6) (45).
The CHA2DS2-VASc score is a helpful tool for risk ischemic stratification (42, 46) in patients with ICH and AF. Conversely, the HAS-BLED score has been developed to assess the bleeding risk in AF patients needing OACs (47, 48). Moreover, HAS-BLED has been taught to better predict major bleeding risk compared to other score systems such as HEMORR(2)HAGES and ATRIA (49, 50).
Nevertheless, some factors that increase ICH risk, such as old age (51, 52), a lobar location of previous ICH (53), as well as CAA (54–57), cortical superficial siderosis (58), and lobar cerebral microbleeds (59) are not contemplated in the HAS-BLED (56, 57). Notably, it has been hypothesized that the HAS-BLED score largely underestimates ICH risk in CAA patients. Indeed recurrent ICH in CAA patients has been shown to be higher than it has been expected according to the HAS-BLED score, suggesting the need for further tools for a better risk stratification (60).
3.5. Oral anticoagulation as a risk factor: current evidence
In patients receiving OACs, up to the 10-fold increased risk of ICH has been reported ranging from 0.25% to 1.1% (61) with a 30-to 90-day mortality rate of 40%–65% (62–65). In Denmark, from 2004 to 2017, the use of OACs among ICH patients intensified to 18% (31).
In recent decades, however, the prevalence of previous use of OAT in patients with ICH has increased by approximately 50% (66, 67). The prevalence of patients who develop ICH during OACs is slightly but significantly higher in women (67).
Remarkably, in South Limburg, in the Netherlands (68), in the period between 2007 and 2009, 25.8% of total ICH (168 of 652) have been associated with OACs use in patients on VKA. An annual incidence of 40.9 total ICH and 10.5 OAC-related ICH per 100,000 people has been reported. Conversely, 23.2% of ICH have been correlated to OACs (121 of 522): however, in this case, 70 were on VKA while 51 were on DOACs). Accordingly, in the following decade, also the annual incidence significatively decreased (reaching 7.5 per 1,000,000 person-year), despite the aging population and the augmented number of OACs users.
Data from 2,452 subjects with a previous ICH (mean age 76 years, 41% female, who were mostly on VKA) highlighted the fact that taking no antithrombotic drug increased ischemic complications without influencing the ICH rate (69).
The introduction of DOACs and changes in OACs behavior have been associated with an inferior risk of ICH compared to VKA (70).
In RCTs assessing the effect of DOACs in patients with AF, the treatment was associated with a 40%–65% risk reduction of ICH compared to warfarin (Table 1) (71–74). Although these data are robust and encouraging, new questions have arisen concerning the hematoma expansion or bleeding volumes and their prognostic impact in patients treated with DOACs or VKA.
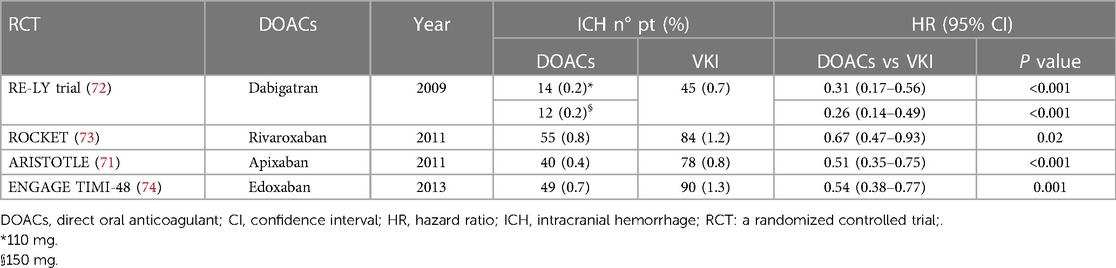
Table 1. Risk of ICH in patients treated with DOACs or VKI in RCT.
In this regard, few heterogeneous data with controversial results are available. In a multicenter study, Wilson et al. did not observe any difference between DOACs or VKA-ICH volume, with a similar 90-day rate of expansion of the initial hematoma, worse prognosis, and mortality (75). Similarly, some studies reported a comparable hematoma expansion between patients treated with DOACs or VKA (76, 77). Conversely, in an observational study that enrolled 2,245 patients with DOACs or VKA-associated ICH, Kurogi et al. reported that patients treated with DOACs were less likely to have moderate or severe impaired consciousness or need surgical hematoma removal (78). Different studies and meta-analyses of RCTs also demonstrated a reduction in in-hospital mortality in patients with ICH treated with DOACs compared to VKA (79, 80).
3.6. Time and modalities of OACs resumption
The resumption of OACs after intracranial bleeding represents a crucial clinical conundrum (Figure 2). Although a great risk of ischemic stroke in patients with AF and a history of ICH has been confirmed, this population has been substantially excluded from phase 3 RCTs of OACs for stroke prevention in spite of the higher ischemic risk (81). Thus, most available data derive from observational studies (3, 8, 9). According to the latest guidelines (82), the clinical choice of restarting anticoagulation should be made after a multiparametric evaluation taking into account not only the cardiologic point of view but also neurological, neuroimaging, and neurosurgery aspects (82). Furthermore, a personalized risk estimation balancing the recurrence of ICH and ischemic stroke risk should mostly influence what strategy to adopt (82). Though the ischemic risk profile could certainly be evaluated with a CHA2DS2-VASc score, the risk of recurrent ICH is multifactorial and more complex to be estimated because of the high variability in its incidence has been reported ranging from 1.3% to 7.4% (3). Etiology, location (lobar ICH at higher risk than non-lobar), and imaging features of ICH can help predict the risk of recurrence (Table 2).
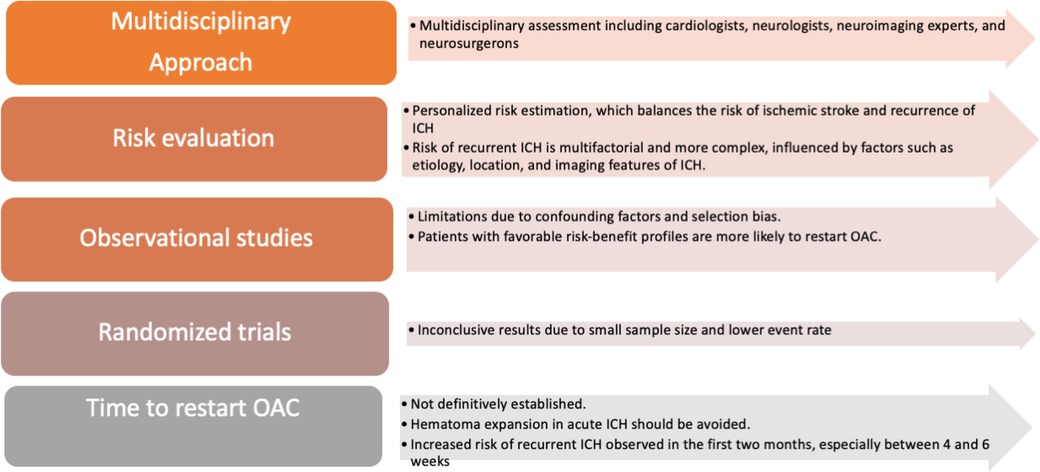
Figure 2. OACs resumption decision making. ICH: Intracranial Hemorrhage, OAC: Oral anticoagulant.
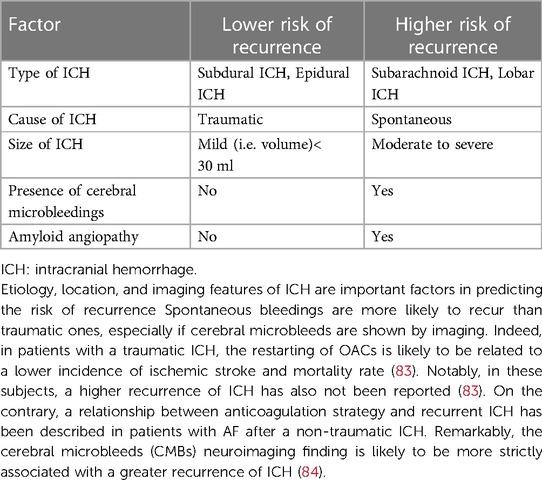
Table 2. Principal factors associated with the risk of recurrence of intracranial hemorrhage (ICH).
In the absence of antithrombotic therapies, an increased incidence of ischemic stroke compared to the recurrence of ICH has been shown in 2,452 AF patients with a previous ICH (mean age 76 years, 41% female, VKA was the most used OACs) (69). Notably, a significant reduction of thromboembolic risk in patients who have restarted OACs without raising the recurrence of ICH has been demonstrated (85).
However, these observational studies are burdened by limitations due to confounding factors and selection bias, as patients with favorable risk-benefit profiles were more likely to restart OACs (86). Data from RCTs are therefore warranted, and several studies are ongoing. Recently, data from the first two RCTs on this topic were published. Neither trial observed significant differences between OACs and no therapy for ischemic stroke or ICH. Although results were inconclusive due to the small size of the enrolled population and the lower event rate than expected, a trend favoring OACs resumption was found (87, 88).
It has not been definitively well established how much time from an ICH is needed to restart OACs (15). Hematoma expansion, expected in acute ICH, is aggravated by anticoagulation. Therefore, in the acute phase of ICH (<24–48 h), anticoagulant treatment should be avoided, and strategies to reverse anticoagulation should be considered (89, 90). An increased risk of recurrent ICH has been observed in the first two months, especially between 4 and six weeks after the index event (91). A wide range of optimal time range from 72 h (92) to 10–30 weeks (91) has been reported. A recent retrospective study performed in Korea showed that waiting 6–8 weeks after ICH for restarting anticoagulants was the safest choice in terms of lower risk of all-cause mortality while resuming anticoagulants after 4–6 weeks after ICH was riskier for bleedings (93).
Conversely, a 70-day waiting period to resume the anticoagulant has been shown to be likely to reduce the recurrence of events; therefore restarting at least after 28 days has been suggested (94).
Accordingly, on the basis of the Swedish registry data involving 2,619 adults, a waiting period of 7–8 weeks for restarting OACs in order to balance the observed risk of ischemic and hemorrhagic complications has been recommended (42). Moreover, restarting OACs six weeks after ICH would not have been correlated to an increased risk of intracranial bleeding over one year of follow-up (69). The majority of available data derived from patients treated with VKA and shorter times could be hypothesized with DOACs. Indeed, current guidelines recommend DOACs over VKA in DOACs-eligible patients (82). Overall, available data support a resumption of OACs at 7–8 weeks after ICH (42).
3.7. Resumption in specific cases: patients with lobar ICH
ICH location is essential in deciding whether and when to resume OACs (Table 3).
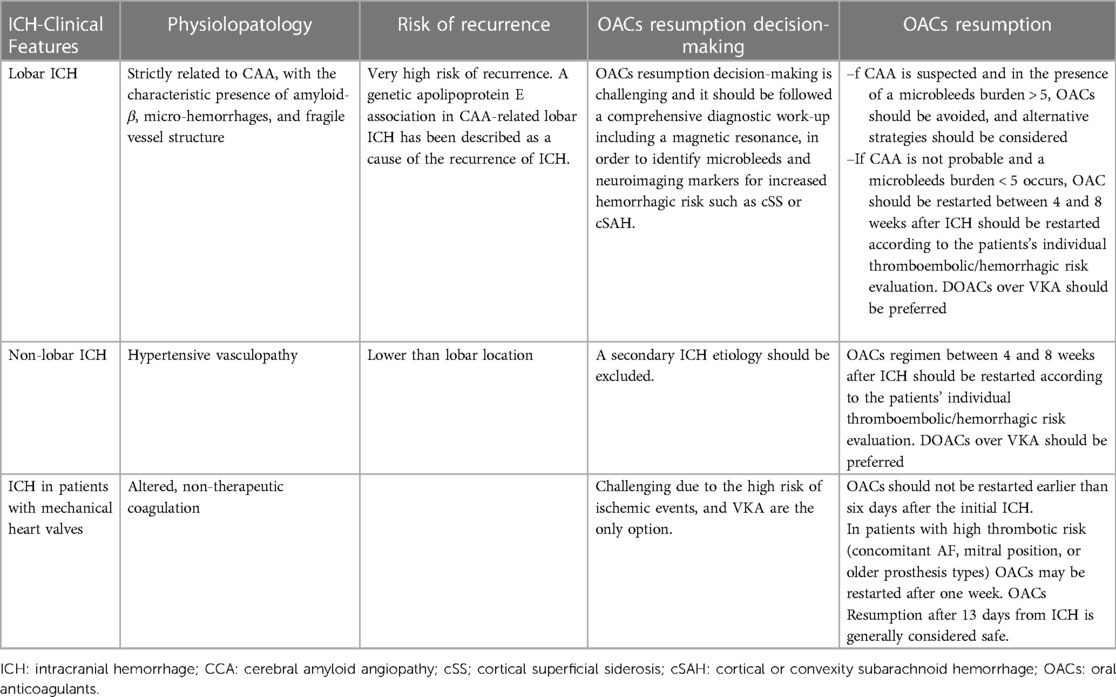
Table 3. OACs resumption modalities according to ICH subtype.
It has been well assessed that lobar ICH is associated with CAA; moreover, it is likely to recur more than other ICH subtypes (3, 95). On this account, according to the latest American guidelines (96), OAT after a lobar ICH should be avoided (97). Therefore, in patients with lobar ICH, it is essential to assess the possible presence of CAA using the modified Boston Criteria (98). MRI should also be integrated into the diagnostic workup before considering OACs resumption, as it could help in estimating the risk of ICH recurrence. Remarkably, the cerebral microbleeds (CMB) burden detected by iron-sensitive imaging is likely to be related not only to the occurrence of ICH but also to the recurrence after ICH in patients treated with OACs (99). Moreover, neuroimaging should be a helpful tool in recognizing particular conditions at higher hemorrhagic risk as acute convexity subarachnoid hemorrhage (cSAH) and cortical superficial siderosis (cSS) (99). The association of CAA and cSAH has been shown to be related to an ICH rate of 19% per patient-year (100). On the contrary, very few data are available about the risk of recurrent ICH in patients with CAA on OACs (101).
A sub-group analysis among 190 patients with probable or possible CAA from a more extensive meta-analysis showed a lower mortality rate and better functional parameters in patients who had restarted OACs, although this data was not sufficient to confirm a role of OACs in the outcomes (102). In conclusion, in subjects with lobar-ICH, an MRI evaluation of the presence of microbleeds, cSS or cSAH might lead to the decision to restart OACs or to adopt other strategies (i.e., LAA closure) (86).
3.8. Resumption in specific cases: patients with mechanical valves
In the presence of mechanical heart valves (MHV), OACs resumption is particularly challenging (Table 3). Firstly, the risk of ischemic events is particularly high in this population reaching 4% patient-years in the absence of OACs and reducing to 1% patient-years with anticoagulant treatment (103). According to the type and seat of the prosthesis, especially if AF coexists, the thromboembolic risk might boost (104). Secondly, in light of the fact that DOACs are not indicated in these patients, VKA is considered the only pharmacological opportunity.
For patients with MHV and a concomitant ICH, introducing the heparin anticoagulation strategy three days after the event and switching to VKA seven days later has been considered safe (105). Recently German multicentric RETRACE study involving 2,504 patients on OACs who survived ICH patients (166 with MHV) showed that restarting anticoagulation (heparins or VKA) within 14 days after an ICH has been associated with a significantly higher occurrence of major and intracranial bleedings (106). Conversely, OACs resumption seems to be safe after two weeks (106). In contrast, it could be reasonable to wait at least one week in patients in which thromboembolic risk is particularly high due to a concomitant AF, mitral prosthesis, or history of embolism) only to restart OACs (106).
3.9. Further caution measures for restarting DOACs in patients with previous ICH
When the decision to restart DOACs has been made, further preventive measures should be adopted in order to improve the safety of patients considered eligible.
On this matter, it has been claimed that the use of P-glycoprotein (P-gp) and cytochrome P450 (CYP) 3A4 inducers or inhibitors in patients concomitantly on DOACs, must be carefully taken into account considering that they could have an impact on anticoagulation. Notably, the assessment of potential interactions in ICH survivors on DOACs is nowhere as easy as it is in other patients and a more accurate examination ought to be done in order to avoid potential unexpected events.
Sánchez-Fuentes et al. (107) recently described the potential effects of herbal medicines, dietary supplements, and foods highlighting their potential interactions with DOACs. The findings of their interesting research (107) can be applied in clinical practice even in these patients who are certainly more complex in consideration of their clinical history. In addition, due to the growing interest in herbal products, probiotics, and prebiotics, and their widespread use, concomitant use with DOACs is likely to occur. The potential interactions are shown in the Figure 3.
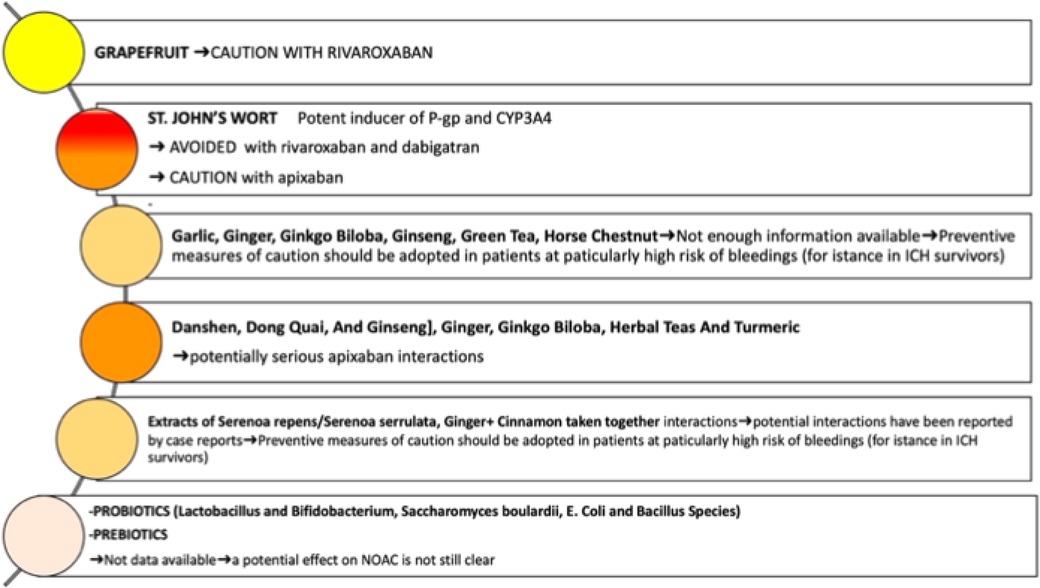
Figure 3. Potential effects of herbal medicines, probiotics and prebiotics on DOACs. Further preventive measures in patients with previous ICH should be adopted in order to improve the safety of patients considered DOACs eligible. Caution is needed in assessing potential interactions DOACs with other substances in ICH survivors to prevent them from potential adverse effects. The use of herbal products, food supplements, probiotics, and prebiotics, should be accurately evaluated.
Moreover, the potential effects of probiotics and prebiotics on anticoagulation strategy have also been examined (107). Although several beneficial effects have been confirmed (108, 109), their influence on gut microbiota composition is expected to interact with VKA. Consequently, an increase in the anticoagulant effect has been supposed. However, their potential interaction with DOACs is still not well investigated.
Overall, these results (107) suggest that it is worth improving the awareness of the potential impact of herbal medicines, dietary supplements, probiotics, and prebiotics in patients on DOACs and ICH survivors should be carefully evaluated.
3.10. Non-pharmacologic options (percutaneous left atrial appendage closure)
It has been assessed that approximately ninety percent of thrombi occur within the LAA in patients with AF (110). The discovery of LAA as the anatomical site with a higher probability of thrombus formation in AF patients led to non-pharmacological approaches. The mechanical occlusion of LAA aims to prevent embolization of any possible thrombus formed inside. Therefore, a percutaneous technique to obliterate LAA was developed. LAA closure (LAAC) is routinely performed via a venous transcatheter femoral access. A self-expanding device with a polymer membrane is delivered in the LAA throughout a trans-septal puncture in order to exclude the LAA cavity from the rest of the atrium, thereby obliterating the site that is the nidus for thrombus formation (111).
A meta-analysis of RCT on LAAC vs. DOACs (112) (1,516 patients from PROTECT AF (113, 114), PREVAIL (10, 115), and PRAGUE-17 (116); LAAC 933, OAC 583, in OAC group 65% warfarin, 35% DOACs), after a mean follow-up of 38.7 ± 17.2 months, showed that ischemic stroke incidence was similar in the two population.
However, OACs was associated with significantly more hemorrhagic strokes, cardiovascular death, and all-cause mortality.
A significant difference in major bleeding has not been reported, though non-procedure-related major bleeding favored LAAC.
Patients with a prior history of ICH have not been excluded from PROTECT (114) and PREVAIL (115) trials whose results allowed the introduction of LAAC in clinical practice.
Currently, recommendations for LAAC are not yet defined (Table 4).
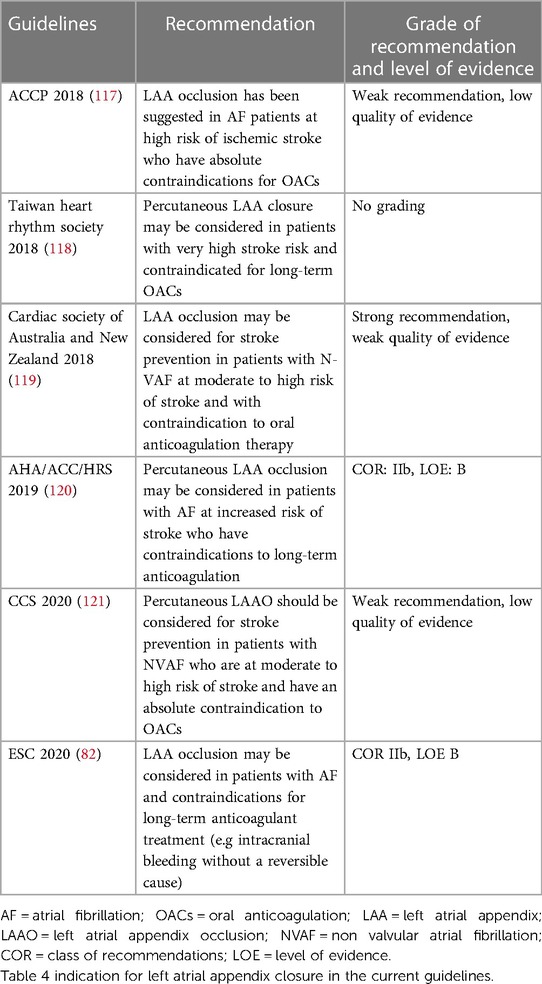
Table 4. Recommendation for left atrial appendage occlusion according to international guidelines.
Despite the lack of RCTs on LAAC in patients with previous ICH, there is every likelihood that LAA occlusion could be a beneficial option in these patients (122–127). LAAC could represent the only alternative in patients with an absolute contraindication to OACs.
A recent meta-analysis (11) of 7 retrospective studies enrolling 407 high-risk patients with a history of ICH who underwent LAAC (mean CHA2DS2VASC and HAS-BLED scores were respectively 4.8 ± 1.5 and 4 ± 1) showed promising results: an acute procedure success rate in 98.5% of the patients and a low rate of periprocedural complications (pericardial effusion 0.17%, device embolization 0.1%, device-related thrombosis 0.03%, major bleeding 0.02%, recurrent ICH 0% (95% CI: 0–0.56). At long-term follow-up, major bleeding and recurrent ICH (0.25% and 0.05%, respectively) occurred, resulting inferior to what would be expected on account of the high HAS-BLED score. Accordingly, also ischemic stroke incidence (0.54%) turned out to be lower than what would have been expected in the absence of OACs for a CHA2DS2VASC >4 (11). The anti-thrombotic regimen following LAAC was variable across countries. Combination therapy with warfarin and acetylsalicylic acid (ASA) (81–325 daily) has been used in the main RCTs (10, 113–115, 128, 129) for one and half months after the procedure until the 45 days transoesophageal echocardiography (TOE) follow-up. Provided that a residual shunt >5 mm and device surface thrombi (DST) did not occur, OACs was interrupted, and dual antiplatelet therapy (DAPT) regimen (ASA and Clopidogrel 75 mg daily) was prolonged for six months, followed by a lifelong single antiplatelet therapy (SAPT) approach (ASA 325 mg/day). An annual bleeding rate of 1.2%, 0.6%, and 3.1% at 45 days, six months, and five years FU has been reported, respectively (130, 131).
In 1,000 recipients who had undergone patent foramen ovale (PFO) or atrial septal defect (ASD) closure, DST occurred in 15%, 30%, and 55% of patients receiving warfarin, SAPT (ASA alone), and DAPT (ASA and clopidogrel), respectively (132).
Furthermore, in another analysis, the 99% of 143 subjects who successfully had LAA occlusion, received DAPT (clopidogrel and ASA) for 30–90 days, followed by SAPT (ASA only) for five months, showing a low thrombogenicity of AMPLAZER devices (133). In the Amplatzer Amulet device registry (134), 1,088 subjects, 71.7% with a history of major bleeding and 82.8% with contraindications to OACs, underwent LAAO closure. TOE was performed 30–90 days after closure, showing a complete procedure in 98.4% of cases and 1.6% of device-related thrombus (DRT). At discharge, 57.7%, 22.4%, and 11.2% received DAPT, SAPT, and OACs, respectively. Notably, the ischemic stroke was reduced by 67% compared to what would have been expected based on the CHA2DS2-VASc score, reporting an annual event rate of 2.2%, showing safe results in more than 80% of patients received exclusively APT (134). A DRT incidence rate of 2.3% has been reported in a metanalysis of 2,855 patients successfully treated with low-molecular-weight heparin for two weeks (135).
However, what makes the antithrombotic strategy challenge most, is that, in the real world, the majority of patients who were referred to LAAO closure have a history of bleeding and are considered unsuitable for VKA or DOACs (117, 136–138). Moreover, patients with contraindications to OAC sor DOACs have been excluded from RCTs. Therefore, due to the lack of RCTs, thromboembolic prevention is particularly complex in this subset of patients so that physicians, for fear of bleeding, usually consider minimal regimens as a 2-week DAPT, followed by SAPT, avoid prescribing OAC (139). A few preliminary data suggested that a regimen based on a low dose DOACs could be used instead of a full dose in very high-risk patients, showing the same thromboembolic protection after LAAC; however, randomized data are missing (140–144). In some extreme cases of high-bleeding risk patients, a single antiplatelet therapy or even no antithrombotic treatment was used after LAAC. A few small studies have evaluated the safety of SAPT following LAAC, and the result is not always concordant (142, 145–148).
Another approach consists of continuing DAPT until a six-month TOE follow-up and then deciding accordingly (139). Generally, if TOE excludes residual shunt >5 mm jet and device surface thrombi (DST), SAPT is continued (139). However, ASA 75–325 mg/day should be continued long-term (149), although it is frequent that antithrombotic agents are stopped within the first 12 months in patients without particular indications (139).
DAPT strategy after PFO closure seems to be effective in avoiding thrombus development despite bleeding complications (131, 150–153). However, the optimal DAPT duration remains largely debated.
After Watchman implantation, two main antithrombotic strategies have been proposed.
On one hand, according to bleeding risk, OACs should be prescribed for 45 days, followed by clopidogrel for six months, in low-bleeding-risk patients, whereas it should be avoided in those at high-risk (149). On the other hand, in patients with contraindications for OACs, DAPT (clopidogrel and ASA) may be continued for 1 to 6 months after the procedure (149). Furthermore, after AMPLATZER or Amulet implantation, DAPT (clopidogrel and aspirin) may be prescribed for 1 to 6 months after the procedure (149). A tailored approach may be adopted, including SAPT (ASA or clopidogrel) for a limited period, considering a team-based evaluation (149).
Another methodology that could be useful in particular cases is the epicardial ligation of the LAA for reducing the anticoagulant treatment both during and after the procedure, although a non-negligible incidence of residual leaks has been reported (154–157). The best approach to address this problem could be to discuss the issue in a multidisciplinary “stroke team” and tailor the post-procedural therapy based on patient characteristics.
Recent guidelines have highlighted the importance of a multidisciplinary “stroke team” formed ideally by neurologists, cardiologists, neuroradiologists, neurosurgeons, patients, and their families, which should be in charge of the therapeutic decision for each patient, tailoring the most appropriate therapy to patient characteristic. We think that nowadays, due to the lack of RCTs data, the routine reference to this team could represent the best approach to cope with complex cases.
One of the main issues of LAAC implementation is that there is no high-quality data on the duration and the type of therapy OAT after LAAC implantation, and there is a wide variety of treatments across different centers (150). Usually, OACs are used for a short period after LAAC. However, which OACs should be used and the optimal duration of this treatment is not established, and there is a high variation among registries (150). In the subset of patients with an absolute contraindication to OACs, dual antiplatelets with aspirin and clopidogrel could be used (150). The safety of this approach is currently unclear. In a meta-analysis of 83 observational studies (150), enrolling 12,326 patients compared short-term oral anticoagulation vs. dual antiplatelet, reported no difference in bleeding, stroke, device-related thrombus, and all-cause mortality. Of note, this meta-analysis does not report the percentage of patients with a history of ICH in the studies. The best approach to address this problem could be to discuss the issue in a multidisciplinary “stroke team” and tailor the post-procedural therapy based on patient characteristics.
In conclusion, LAAC is a safe alternative to reduce ischemic stroke in OAC-ineligible patients, in which this procedure is the only feasible therapeutic option.
Future clinical trials focused on choosing optimal anticoagulation strategies after ICH would be helpful for improving the therapeutic strategy in these patients.
3.11. Guidelines indications
Recommendations for restarting OACs have been summarized in Table 5.
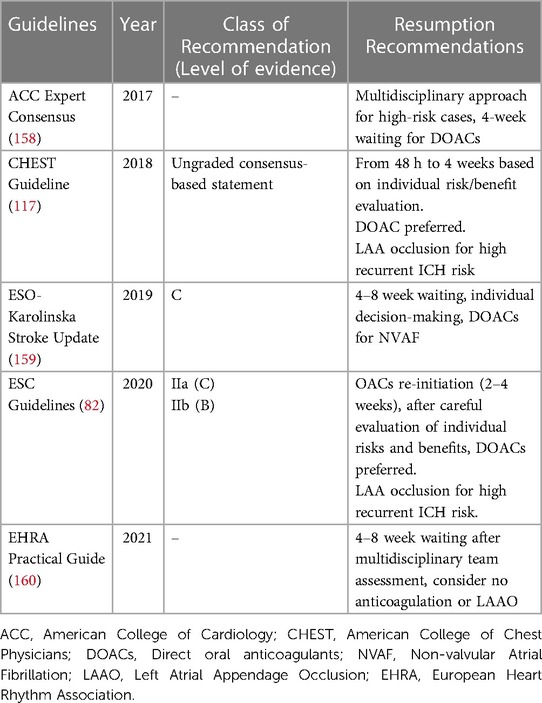
Table 5. When to restart OAC according to international guidelines.
According to 2018 consensus statements and recommendations from the European Stroke Organisation (ESO) 2018 (159).
It would be advisable to restart OACs in selected ICH patients rather than not using OACs in view of better outcomes not accompanied by an increased ICH recurrence rate for subjects with AF who survived an ICH (Grade C). Therefore DOACs could be considered safer compared to VKA in these patients (Grade C).
The re-introduction of OACs between the first four to eight weeks from index ICH is considered quite reasonable (Grade C) (159). A tailored decision-making on OACs after ICH should also take into account factors such as BP control, age, where ICH is located, and its dimension; in addition neuroimaging findings such as leukoaraiosis, cortical superficial siderosis, CAA should be considered (Grade C) OACs between the first four to eight weeks from index ICH seems to be safe (Grade C) (159).
According to the 2018 CHEST guidelines (117), anticoagulation with a DOACs after acute spontaneous ICH must be carefully evaluated, considering the risks and benefits. Moreover, for those selected patients at high risk of recurrent ICH, as in the case of a concomitant diagnosed or suspected CAA, LAA occlusion is suggested (117).
According to the 2019 American Heart Association and American Stroke Association (AHA/ASA) guidelines (161), it is reasonable to initiate OACs between 4 and 14 days after the onset of neurological symptoms for most patients with an acute ischemic stroke in the setting of AF.
According to the 2020 European Society of Cardiology (ESC) guidelines (161), the choice of restarting OAC in AF patients at high thromboembolic risk should be based on a multidisciplinary approach balancing potential advantages and disadvantages. DOACs should also be preferred compared to VKA (Class II a).
Conversely, a recent high-risk bleeding event such as ICH (within two weeks) is considered an absolute contraindication to OACs (161). Moreover, in AF patients at very high risk of recurrent ICH, LAA occlusion may be considered (161). In more detail, LAA occlusion may be a therapeutic option in patients with AF and intracranial bleeding without a reversible cause (Class recommendation IIb, level of evidence B) (161).
According to the 2021 European Heart Rhythm Association (EHRA) guidelines, the best timing to restart anticoagulation is after 4–8 weeks after a multidisciplinary assessment, and if considered not suitable, LAA occlusion is strongly recommended (160).
4. Conclusion
Robust data available on the timing and modalities of OACs resumption after a major bleeding event, such as an ICH, are lacking. Patients with a history of recent ICH were excluded from RCTs on stroke prevention in AF, so the recommendations of current guidelines are weak.
For fear of ICH, a potentially lethal adverse effect of anticoagulation regimen, physicians are commonly reluctant to reinitiate OACs in AF patients who survived an ICH, even in patients with a high estimated risk of AF-related ischemic stroke. The decision-making should be based on a multi-specialist approach. A careful balance of the advantages and disadvantages of restarting OAC must be considered.
Data availability statement
The original contributions presented in the study are included in the article/Supplementary Material, further inquiries can be directed to the corresponding author/s.
Group Members of Quality Working Group ANMCO, Cardiac Chronic Diseases ANMCO, and Arrhythmia Working Group ANMCO
Members of Management and Quality Group Working Group, ANMCO Fabiana Lucà, GOM Hospital, Bianchi Melacrino Morelli, Reggio Calabria, Italy (Chairperson); Simona Giubilato, Cannizzaro Hospital, Catania, Italy; Giorgio Caretta, S. Andrea Hospital, La Spezia, Italy; Stefano Cornara, Levante, San Paolo, Hospital, Savona, Italy; Irene Di Matteo, ASST, Niguarda Hospital, Milano, Italy.
Anna Members of Arrhythmias Workin Group ANMCO, Raimondo Calvanese, Ospedale del Mare, Napoli, Italy (Chairperson); Carlo Pignalberi San Filippo Neri Hospital; Roma, Italy; Francesco Borrello, Civile Pugliese Ciaccio Hospital, Catanzaro, Italy; Amir Kol, S.Camillo de Lellis Hospital, Rieti, Italy; Martina Nesti, San Donato Hospital, Pasquale Vergara, IRCCS San Raffaele Hospital, Milano, Italy; Manuel Antonio Conti, Civile G. Mazzini Hospital, Teramo, Italy; Federico Migliore, Università degli Studi di Padova, Italy; Pietro Rossi, Fatebenefratelli Hospital, Roma, Italy.
Members of Cardiac Chronic Diseases Working Group, ANMCO, Maurizio Giuseppe Abrignani, Paolo Borsellino Hospital, ASP Trapani, Marsala, Italy (Chairperson); Pier Luigi Temporelli, Istituti Clinici Scientifici Maugeri IRCCS, Gattico-Veruno, Novara, Italy; Giulio Binaghi, ARNAS G. Brotzu Hospital, Cagliari, Italy; Arturo Cesaro.
Author contributions
This statement is to certify that all authors have seen and approved the manuscript being submitted contributing significantly to the work, attest to the validity and legitimacy of the data and its interpretation, and agree to its submission. All authors agree with the content, and all give explicit consent to submit. All authors whose names appear on the submission: (1) made substantial contributions to the conception or design of the work (FL, FC, MMG, FO, SGe, MA); (2) made substantial contributions to the acquisition, analysis, or interpretation of data (APo, APi, CR, SF, GC, APa, SGi, IM, CN, SC); (3) drafted the work or revised it critically for important intellectual content (FB, RCe, MA, RR, RCa, CR, SF); (4) approved the version to be published (FL, SGe, MG, FO, FC, CR); (5) agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved (RR, APo, FL, SF, R, APi, SC, GC, CN). We attest that the article is the Authors’ original work, has not received prior publication, and is not under consideration for publication elsewhere. All authors contributed to the article and approved the submitted version.
Acknowledgments
We gratefully acknowledge Carol Winteringham for the English Editing of the Manuscript.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Anzai T, Grandinetti A, Katz AR, Hurwitz EL, Wu YY, Masaki K. Association between central sleep apnea and atrial fibrillation/flutter in Japanese-American men: the kuakini honolulu heart program (HHP) and honolulu-Asia aging study (HAAS). J Electrocardiol. (2020) 61:10–7. doi: 10.1016/j.jelectrocard.2020.05.005
2. Lin SY, Chang YC, Lin FJ, Tang SC, Dong YH, Wang CC. Post-Intracranial hemorrhage antithrombotic therapy in patients with atrial fibrillation. J Am Heart Assoc. (2022) 11:e022849. doi: 10.1161/jaha.121.022849
3. Poon MT, Fonville AF, Al-Shahi Salman R. Long-term prognosis after intracerebral haemorrhage: systematic review and meta-analysis. J Neurol Neurosurg Psychiatry. (2014) 85:660–7. doi: 10.1136/jnnp-2013-306476
4. Hanger HC, Wilkinson TJ, Fayez-Iskander N, Sainsbury R. The risk of recurrent stroke after intracerebral haemorrhage. J Neurol Neurosurg Psychiatry. (2007) 78:836–40. doi: 10.1136/jnnp.2006.106500
5. Hart RG, Diener HC, Yang S, Connolly SJ, Wallentin L, Reilly PA, et al. Intracranial hemorrhage in atrial fibrillation patients during anticoagulation with warfarin or dabigatran: the RE-LY trial. Stroke. (2012) 43:1511–7. doi: 10.1161/strokeaha.112.650614
6. Hankey GJ, Stevens SR, Piccini JP, Lokhnygina Y, Mahaffey KW, Halperin JL, et al. Intracranial hemorrhage among patients with atrial fibrillation anticoagulated with warfarin or rivaroxaban: the rivaroxaban once daily, oral, direct factor Xa inhibition compared with vitamin K antagonism for prevention of stroke and embolism trial in atrial fibrillation. Stroke. (2014) 45:1304–12. doi: 10.1161/strokeaha.113.004506
7. Steiner T, Weitz JI, Veltkamp R. Anticoagulant-Associated intracranial hemorrhage in the era of reversal agents. Stroke. (2017) 48:1432–7. doi: 10.1161/strokeaha.116.013343
8. Nielsen PB, Larsen TB, Skjøth F, Gorst-Rasmussen A, Rasmussen LH, Lip GY. Restarting anticoagulant treatment after intracranial hemorrhage in patients with atrial fibrillation and the impact on recurrent stroke, mortality, and bleeding: a nationwide cohort study. Circulation. (2015) 132:517–25. doi: 10.1161/circulationaha.115.015735
9. Brønnum Nielsen P, Larsen TB, Gorst-Rasmussen A, Skjøth F, Rasmussen LH, Lip GYH. Intracranial hemorrhage and subsequent ischemic stroke in patients with atrial fibrillation: a nationwide cohort study. Chest. (2015) 147:1651–8. doi: 10.1378/chest.14-2099
10. Reddy VY, Doshi SK, Kar S, Gibson DN, Price MJ, Huber K, et al. 5-Year Outcomes after left atrial appendage closure: from the PREVAIL and PROTECT AF trials. J Am Coll Cardiol. (2017) 70:2964–75. doi: 10.1016/j.jacc.2017.10.021
11. Garg J, Shah S, Shah K, Bhardwaj R, Contractor T, Mandapati R, et al. Left atrial appendage closure in patients with intracranial hemorrhage. J Interv Card Electrophysiol. (2022) 64(3):551–6. doi: 10.1007/s10840-022-01141-z
12. Liberati A, Altman DG, Tetzlaff J, Mulrow C, Gøtzsche PC, Ioannidis JP, et al. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: explanation and elaboration. J Clin Epidemiol. (2009) 62:e1–34. doi: 10.1016/j.jclinepi.2009.06.006
13. Feigin VL, Lawes CM, Bennett DA, Barker-Collo SL, Parag V. Worldwide stroke incidence and early case fatality reported in 56 population-based studies: a systematic review. Lancet Neurol. (2009) 8:355–69. doi: 10.1016/s1474-4422(09)70025-0
14. Lee JY, Kim JS, Kim TY, Kim YS. Detection and classification of intracranial haemorrhage on CT images using a novel deep-learning algorithm. Sci Rep. (2020) 10:20546. doi: 10.1038/s41598-020-77441-z
15. Schrag M, Kirshner H. Management of intracerebral hemorrhage: jACC focus seminar. J Am Coll Cardiol. (2020) 75:1819–31. doi: 10.1016/j.jacc.2019.10.066
16. O'Donnell MJ, Chin SL, Rangarajan S, Xavier D, Liu L, Zhang H, et al. Global and regional effects of potentially modifiable risk factors associated with acute stroke in 32 countries (INTERSTROKE): a case-control study. Lancet. (2016) 388:761–75. doi: 10.1016/s0140-6736(16)30506-2
17. Vinters HV. Cerebral amyloid angiopathy. A critical review. Stroke. (1987) 18:311–24. doi: 10.1161/01.str.18.2.311
18. Samarasekera N, Fonville A, Lerpiniere C, Farrall AJ, Wardlaw JM, White PM, et al. Influence of intracerebral hemorrhage location on incidence, characteristics, and outcome: population-based study. Stroke. (2015) 46:361–8. doi: 10.1161/strokeaha.114.007953
19. Baron JC, Boulouis G, Benzakoun J, Schwall C, Oppenheim C, Turc G, et al. Cerebral amyloid angiopathy-related acute lobar intra-cerebral hemorrhage: diagnostic value of plain CT. J Neurol. (2022) 269:2126–32. doi: 10.1007/s00415-021-10796-z
20. Viswanathan A, Greenberg SM. Cerebral amyloid angiopathy in the elderly. Ann Neurol. (2011) 70:871–80. doi: 10.1002/ana.22516
21. Dastur CK, Yu W. Current management of spontaneous intracerebral haemorrhage. Stroke Vasc Neurol. (2017) 2:21–9. doi: 10.1136/svn-2016-000047
22. Kahan J, Ong H, Ch'ang J, Merkler AE, Fink ME, Gupta A, et al. Comparing hematoma characteristics in primary intracerebral hemorrhage versus intracerebral hemorrhage caused by structural vascular lesions. J Clin Neurosci. (2022) 99:5–9. doi: 10.1016/j.jocn.2022.02.031
23. Lawton MT, Vates GE. Subarachnoid hemorrhage. N Engl J Med. (2017) 377:257–66. doi: 10.1056/NEJMcp1605827
24. Macdonald RL, Schweizer TA. Spontaneous subarachnoid haemorrhage. Lancet. (2017) 389:655–66. doi: 10.1016/s0140-6736(16)30668-7
25. An SJ, Kim TJ, Yoon BW. Epidemiology, risk factors, and clinical features of intracerebral hemorrhage: an update. J Stroke. (2017) 19:3–10. doi: 10.5853/jos.2016.00864
26. On S, Poh R, Salor RS, Philip RG, Chekkattu RH, Lim MA, et al. The burden and risks factors for intracerebral hemorrhage in a southeast Asian population. Clin Neurol Neurosurg. (2022) 214:107145. doi: 10.1016/j.clineuro.2022.107145
27. Giroud M, Delpont B, Daubail B, Blanc C, Durier J, Giroud M, et al. Temporal trends in sex differences with regard to stroke incidence: the dijon stroke registry (1987-2012). Stroke. (2017) 48:846–9. doi: 10.1161/strokeaha.116.015913
28. Yu K, Zhu S, He M, Li Z, Zhang L, Sui Z, et al. Epidemiological characteristics of 561 cases of intracerebral hemorrhage in Chengdu. China. Medicine (Baltimore). (2021) 100:e24952. doi: 10.1097/md.0000000000024952
29. Wang DZ, Xue XD, Zhang H, Xu ZL, Zhang Y, Song GD, et al. The trend of intracerebral hemorrhage mortality of the residents with different characteristics in Tianjin, China, 1999-2015. Zhonghua Yu Fang Yi Xue Za Zhi. (2018) 52:389–95. doi: 10.3760/cma.j.issn.0253-9624.2018.04.011
30. Carlsson M, Wilsgaard T, Johnsen SH, Johnsen LH, Løchen ML, Njølstad I, et al. Long-Term survival, causes of death, and trends in 5-year mortality after intracerebral hemorrhage: the tromsø study. Stroke. (2021) 52:3883–90. doi: 10.1161/strokeaha.120.032750
31. Pedersen TGB, Vinter N, Schmidt M, Frost L, Cordsen P, Andersen G, et al. Trends in the incidence and mortality of intracerebral hemorrhage, and the associated risk factors, in Denmark from 2004 to 2017. Eur J Neurol. (2022) 29:168–77. doi: 10.1111/ene.15110
32. Guéniat J, Brenière C, Graber M, Garnier L, Mohr S, Giroud M, et al. Increasing burden of stroke: the dijon stroke registry (1987-2012). Neuroepidemiology. (2018) 50:47–56. doi: 10.1159/000486397
33. Lecoffre C, de Peretti C, Gabet A, Grimaud O, Woimant F, Giroud M, et al. National trends in patients hospitalized for stroke and stroke mortality in France, 2008 to 2014. Stroke. (2017) 48:2939–45. doi: 10.1161/strokeaha.117.017640
34. Fakan B, Reisz Z, Zadori D, Vecsei L, Klivenyi P, Szalardy L. Predictors of localization, outcome, and etiology of spontaneous intracerebral hemorrhages: focus on cerebral amyloid angiopathy. J Neural Transm (Vienna). (2020) 127:963–72. doi: 10.1007/s00702-020-02174-2
35. Shen J, Guo F, Yang P, Xu F. Influence of hypertension classification on hypertensive intracerebral hemorrhage location. J Clin Hypertens (Greenwich). (2021) 23:1992–9. doi: 10.1111/jch.14367
36. Dong H, Liu S, Jing L, Tian M, Sun J, Pang Y, et al. Hypertension among hemorrhagic stroke patients in northeast China: a population-based study 2017-2019. Med Sci Monit. (2020) 26:e926581. doi: 10.12659/msm.926581
37. Lin CH, Nfor ON, Ho CC, Hsu SY, Tantoh DM, Liaw YC, et al. Association of ADH1B polymorphism and alcohol consumption with increased risk of intracerebral hemorrhagic stroke. J Transl Med. (2021) 19:227. doi: 10.1186/s12967-021-02904-4
38. Tsatsakis A, Docea AO, Calina D, Tsarouhas K, Zamfira LM, Mitrut R, et al. A mechanistic and pathophysiological approach for stroke associated with drugs of abuse. J Clin Med. (2019) 8:1295. doi: 10.3390/jcm8091295
39. van Asch CJ, Luitse MJ, Rinkel GJ, van der Tweel I, Algra A, Klijn CJ. Incidence, case fatality, and functional outcome of intracerebral haemorrhage over time, according to age, sex, and ethnic origin: a systematic review and meta-analysis. Lancet Neurol. (2010) 9:167–76. doi: 10.1016/s1474-4422(09)70340-0
40. Hemphill JC 3rd, Bonovich DC, Besmertis L, Manley GT, Johnston SC. The ICH score: a simple, reliable grading scale for intracerebral hemorrhage. Stroke. (2001) 32:891–7. doi: 10.1161/01.str.32.4.891
41. Bailey RD, Hart RG, Benavente O, Pearce LA. Recurrent brain hemorrhage is more frequent than ischemic stroke after intracranial hemorrhage. Neurology. (2001) 56:773–7. doi: 10.1212/wnl.56.6.773
42. Pennlert J, Overholser R, Asplund K, Carlberg B, Van Rompaye B, Wiklund PG, et al. Optimal timing of anticoagulant treatment after intracerebral hemorrhage in patients with atrial fibrillation. Stroke. (2017) 48:314–20. doi: 10.1161/STROKEAHA.116.014643
43. PROGRESS Collaborative Group. Randomised trial of a perindopril-based blood-pressure-lowering regimen among 6,105 individuals with previous stroke or transient ischaemic attack. Lancet. (2001) 358:1033–41. doi: 10.1016/s0140-6736(01)06178-5
44. Gabet A, Olié V, Béjot Y. Atrial fibrillation in spontaneous intracerebral hemorrhage, dijon stroke registry (2006-2017). J Am Heart Assoc. (2021) 10:e020040. doi: 10.1161/jaha.120.020040
45. Nielsen PB, Overvad TF, Andersen SD, Larsen TB, Skjøth F, Søgaard M, et al. Risk stratification for ischemic cerebrovascular events and mortality among intracerebral hemorrhage patients with and without atrial fibrillation: a nationwide cohort study. Cerebrovasc Dis. (2019) 48:236–43. doi: 10.1159/000504926
46. Maeda T, Nishi T, Funakoshi S, Tada K, Tsuji M, Satoh A, et al. Risks of bleeding and stroke based on CHA2DS2-VASc scores in Japanese patients with atrial fibrillation: a large-scale observational study using real-world data. J Am Heart Assoc. (2020) 9:e014574. doi: 10.1161/jaha.119.014574
47. Pisters R, Lane DA, Nieuwlaat R, de Vos CB, Crijns HJ, Lip GY. A novel user-friendly score (HAS-BLED) to assess 1-year risk of major bleeding in patients with atrial fibrillation: the euro heart survey. Chest. (2010) 138:1093–100. doi: 10.1378/chest.10-0134
48. Lip GY, Frison L, Halperin JL, Lane DA. Comparative validation of a novel risk score for predicting bleeding risk in anticoagulated patients with atrial fibrillation: the HAS-BLED (hypertension, abnormal renal/liver function, stroke, bleeding history or predisposition, labile INR, elderly, drugs/alcohol concomitantly) score. J Am Coll Cardiol. (2011) 57:173–80. doi: 10.1016/j.jacc.2010.09.024
49. Apostolakis S, Lane DA, Guo Y, Buller H, Lip GY. Performance of the HEMORR(2)HAGES, ATRIA, and HAS-BLED bleeding risk-prediction scores in patients with atrial fibrillation undergoing anticoagulation: the AMADEUS (evaluating the use of SR34006 compared to warfarin or acenocoumarol in patients with atrial fibrillation) study. J Am Coll Cardiol. (2012) 60:861–7. doi: 10.1016/j.jacc.2012.06.019
50. Roldán V, Marín F, Fernández H, Manzano-Fernandez S, Gallego P, Valdés M, et al. Predictive value of the HAS-BLED and ATRIA bleeding scores for the risk of serious bleeding in a “real-world” population with atrial fibrillation receiving anticoagulant therapy. Chest. (2013) 143:179–84. doi: 10.1378/chest.12-0608
51. Forman R, Slota K, Ahmad F, Garg R, John S, Da Silva I, et al. Intracerebral hemorrhage outcomes in the very elderly. J Stroke Cerebrovasc Dis. (2020) 29:104695. doi: 10.1016/j.jstrokecerebrovasdis.2020.104695
52. Bagg S, Pombo AP, Hopman W. Effect of age on functional outcomes after stroke rehabilitation. Stroke. (2002) 33:179–85. doi: 10.1161/hs0102.101224
53. Passero S, Burgalassi L, D'Andrea P, Battistini N. Recurrence of bleeding in patients with primary intracerebral hemorrhage. Stroke. (1995) 26:1189–92. doi: 10.1161/01.str.26.7.1189
54. Lin CM, Arishima H, Kikuta KI, Naiki H, Kitai R, Kodera T, et al. Pathological examination of cerebral amyloid angiopathy in patients who underwent removal of lobar hemorrhages. J Neurol. (2018) 265:567–77. doi: 10.1007/s00415-018-8740-z
55. Guidoux C, Hauw JJ, Klein IF, Labreuche J, Berr C, Duyckaerts C, et al. Amyloid angiopathy in brain hemorrhage: a postmortem neuropathological-magnetic resonance imaging study. Cerebrovasc Dis. (2018) 45:124–31. doi: 10.1159/000486554
56. Mehndiratta P, Manjila S, Ostergard T, Eisele S, Cohen ML, Sila C, et al. Cerebral amyloid angiopathy-associated intracerebral hemorrhage: pathology and management. Neurosurg Focus. (2012) 32:E7. doi: 10.3171/2012.1.Focus11370
57. Grysiewicz R, Gorelick PB. Incidence, mortality, and risk factors for oral anticoagulant-associated intracranial hemorrhage in patients with atrial fibrillation. J Stroke Cerebrovasc Dis. (2014) 23:2479–88. doi: 10.1016/j.jstrokecerebrovasdis.2014.06.031
58. Charidimou A, Boulouis G, Roongpiboonsopit D, Xiong L, Pasi M, Schwab KM, et al. Cortical superficial siderosis and recurrent intracerebral hemorrhage risk in cerebral amyloid angiopathy: large prospective cohort and preliminary meta-analysis. Int J Stroke. (2019) 14:723–33. doi: 10.1177/1747493019830065
59. Greenberg SM, Vernooij MW, Cordonnier C, Viswanathan A, Al-Shahi Salman R, Warach S, et al. Cerebral microbleeds: a guide to detection and interpretation. Lancet Neurol. (2009) 8:165–74. doi: 10.1016/s1474-4422(09)70013-4
60. Ward R, Ponamgi S, DeSimone CV, English S, Hodge DO, Slusser JP, et al. Utility of HAS-BLED and CHA(2)DS(2)-VASc scores among patients with atrial fibrillation and imaging evidence of cerebral amyloid angiopathy. Mayo Clin Proc. (2020) 95:2090–8. doi: 10.1016/j.mayocp.2020.03.034
61. da Silva IRF, Frontera JA. Resumption of anticoagulation after intracranial hemorrhage. Curr Treat Options Neurol. (2017) 19:39. doi: 10.1007/s11940-017-0477-y
62. Flaherty ML, Kissela B, Woo D, Kleindorfer D, Alwell K, Sekar P, et al. The increasing incidence of anticoagulant-associated intracerebral hemorrhage. Neurology. (2007) 68:116–21. doi: 10.1212/01.wnl.0000250340.05202.8b
63. Ikram MA, Wieberdink RG, Koudstaal PJ. International epidemiology of intracerebral hemorrhage. Curr Atheroscler Rep. (2012) 14:300–6. doi: 10.1007/s11883-012-0252-1
64. Schols AM, Schreuder FH, van Raak EP, Schreuder TH, Rooyer FA, van Oostenbrugge RJ, et al. Incidence of oral anticoagulant-associated intracerebral hemorrhage in The Netherlands. Stroke. (2014) 45:268–70. doi: 10.1161/strokeaha.113.003003
65. Karelis G, Micule M, Klavina E, Haritoncenko I, Kikule I, Tilgale B, et al. The Riga east university hospital stroke registry-an analysis of 4915 consecutive patients with acute stroke. Medicina (Kaunas). (2021) 57:632. doi: 10.3390/medicina57060632
66. Lovelock CE, Molyneux AJ, Rothwell PM. Change in incidence and aetiology of intracerebral haemorrhage in oxfordshire, UK, between 1981 and 2006: a population-based study. Lancet Neurol. (2007) 6:487–93. doi: 10.1016/s1474-4422(07)70107-2
67. Lauer A, Pfeilschifter W, Schaffer CB, Lo EH, Foerch C. Intracerebral haemorrhage associated with antithrombotic treatment: translational insights from experimental studies. Lancet Neurol. (2013) 12:394–405. doi: 10.1016/s1474-4422(13)70049-8
68. Peeters MT, Vroman F, Schreuder TA, van Oostenbrugge RJ, Staals J. Decrease in incidence of oral anticoagulant-related intracerebral hemorrhage over the past decade in The Netherlands. Eur Stroke J. (2022) 7:20–7. doi: 10.1177/23969873211062011
69. Korompoki E, Filippidis FT, Nielsen PB, Del Giudice A, Lip GYH, Kuramatsu JB, et al. Long-term antithrombotic treatment in intracranial hemorrhage survivors with atrial fibrillation. Neurology. (2017) 89:687–96. doi: 10.1212/wnl.0000000000004235
70. Wu T, Lv C, Wu L, Chen W, Lv M, Jiang S, et al. Risk of intracranial hemorrhage with direct oral anticoagulants: a systematic review and meta-analysis of randomized controlled trials. J Neurol. (2022) 269:664–75. doi: 10.1007/s00415-021-10448-2
71. Granger CB, Alexander JH, McMurray JJ, Lopes RD, Hylek EM, Hanna M, et al. Apixaban versus warfarin in patients with atrial fibrillation. N Engl J Med. (2011) 365:981–92. doi: 10.1056/NEJMoa1107039
72. Connolly SJ, Ezekowitz MD, Yusuf S, Eikelboom J, Oldgren J, Parekh A, et al. Dabigatran versus warfarin in patients with atrial fibrillation. N Engl J Med. (2009) 361:1139–51. doi: 10.1056/NEJMoa0905561
73. Patel MR, Mahaffey KW, Garg J, Pan G, Singer DE, Hacke W, et al. Rivaroxaban versus warfarin in nonvalvular atrial fibrillation. N Engl J Med. (2011) 365:883–91. doi: 10.1056/NEJMoa1009638
74. Giugliano RP, Ruff CT, Braunwald E, Murphy SA, Wiviott SD, Halperin JL, et al. Edoxaban versus warfarin in patients with atrial fibrillation. N Engl J Med. (2013) 369:2093–104. doi: 10.1056/NEJMoa1310907
75. Wilson D, Seiffge DJ, Traenka C, Basir G, Purrucker JC, Rizos T, et al. Outcome of intracerebral hemorrhage associated with different oral anticoagulants. Neurology. (2017) 88:1693–700. doi: 10.1212/wnl.0000000000003886
76. Melmed KR, Lyden P, Gellada N, Moheet A. Intracerebral hemorrhagic expansion occurs in patients using non-vitamin K antagonist oral anticoagulants comparable with patients using warfarin. J Stroke Cerebrovasc Dis. (2017) 26:1874–82. doi: 10.1016/j.jstrokecerebrovasdis.2017.04.025
77. von der Brelie C, Doukas A, Naumann R, Dempfle A, Larsen N, Synowitz M, et al. Clinical and radiological course of intracerebral haemorrhage associated with the new non-vitamin K anticoagulants. Acta Neurochir (Wien). (2017) 159:101–9. doi: 10.1007/s00701-016-3026-7
78. Kurogi R, Nishimura K, Nakai M, Kada A, Kamitani S, Nakagawara J, et al. Comparing intracerebral hemorrhages associated with direct oral anticoagulants or warfarin. Neurology. (2018) 90:e1143–1149. doi: 10.1212/wnl.0000000000005207
79. Inohara T, Xian Y, Liang L, Matsouaka RA, Saver JL, Smith EE, et al. Association of intracerebral hemorrhage among patients taking non–vitamin K antagonist vs vitamin K antagonist oral anticoagulants with in-hospital mortality. JAMA. (2018) 319:463–73. doi: 10.1001/jama.2017.21917
80. Wolfe Z, Khan SU, Nasir F, Raghu Subramanian C, Lash B. A systematic review and Bayesian network meta-analysis of risk of intracranial hemorrhage with direct oral anticoagulants. J Thromb Haemost. (2018) 16:1296–306. doi: 10.1111/jth.14131
81. Liu X, Guo S, Xu Z. Meta-Analysis of oral anticoagulants and adverse outcomes in atrial fibrillation patients after intracranial hemorrhage. Front Cardiovasc Med. (2022) 9:961000. doi: 10.3389/fcvm.2022.961000
82. Hindricks G, Potpara T, Dagres N, Arbelo E, Bax JJ, Blomström-Lundqvist C, et al. 2020 ESC guidelines for the diagnosis and management of atrial fibrillation developed in collaboration with the European association for cardio-thoracic surgery (EACTS): the task force for the diagnosis and management of atrial fibrillation of the European society of cardiology (ESC) developed with the special contribution of the European heart rhythm association (EHRA) of the ESC. Eur Heart J. (2021) 42:373–498. doi: 10.1093/eurheartj/ehaa612
83. Nielsen PB, Larsen TB, Skjøth F, Lip GY. Outcomes associated with resuming warfarin treatment after hemorrhagic stroke or traumatic intracranial hemorrhage in patients with atrial fibrillation. JAMA Intern Med. (2017) 177:563–70. doi: 10.1001/jamainternmed.2016.9369
84. Wilson D, Ambler G, Shakeshaft C, Brown MM, Charidimou A, Al-Shahi Salman R, et al. Cerebral microbleeds and intracranial haemorrhage risk in patients anticoagulated for atrial fibrillation after acute ischaemic stroke or transient ischaemic attack (CROMIS-2): a multicentre observational cohort study. Lancet Neurol. (2018) 17:539–47. doi: 10.1016/s1474-4422(18)30145-5
85. Charidimou A, Imaizumi T, Moulin S, Biffi A, Samarasekera N, Yakushiji Y, et al. Brain hemorrhage recurrence, small vessel disease type, and cerebral microbleeds: a meta-analysis. Neurology. (2017) 89:820–9. doi: 10.1212/WNL.0000000000004259
86. Sembill JA, Kuramatsu JB, Schwab S, Huttner HB. Resumption of oral anticoagulation after spontaneous intracerebral hemorrhage. Neurol Res Pract. (2019) 1:12. doi: 10.1186/s42466-019-0018-0
87. So SC. Effects of oral anticoagulation for atrial fibrillation after spontaneous intracranial haemorrhage in the UK: a randomised, open-label, assessor-masked, pilot-phase, non-inferiority trial. Lancet Neurol. (2021) 20:842–53. doi: 10.1016/S1474-4422(21)00264-7
88. Schreuder F, van Nieuwenhuizen KM, Hofmeijer J, Vermeer SE, Kerkhoff H, Zock E, et al. Apixaban versus no anticoagulation after anticoagulation-associated intracerebral haemorrhage in patients with atrial fibrillation in The Netherlands (APACHE-AF): a randomised, open-label, phase 2 trial. Lancet Neurol. (2021) 20:907–16. doi: 10.1016/S1474-4422(21)00298-2
89. Di Fusco SA, Lucà F, Benvenuto M, Iorio A, Fiscella D, D'Ascenzo F, et al. Major bleeding with old and novel oral anticoagulants: how to manage it. Focus on reversal agents. Int J Cardiol. (2018) 268:75–9. doi: 10.1016/j.ijcard.2018.05.060
90. Di Fusco SA, Lucà F, Benvenuto M, Iorio A, Fiscella D, D'Ascenzo F, et al. Major bleeding with old and novel oral anticoagulants: how to manage it. Focus on general measures. Int J Cardiol. (2018) 268:80–4. doi: 10.1016/j.ijcard.2018.05.061
91. Majeed A, Kim YK, Roberts RS, Holmström M, Schulman S. Optimal timing of resumption of warfarin after intracranial hemorrhage. Stroke. (2010) 41:2860–6. doi: 10.1161/strokeaha.110.593087
92. Hawryluk GW, Austin JW, Furlan JC, Lee JB, O'Kelly C, Fehlings MG. Management of anticoagulation following central nervous system hemorrhage in patients with high thromboembolic risk. J Thromb Haemost. (2010) 8:1500–8. doi: 10.1111/j.1538-7836.2010.03882.x
93. Moon JY, Bae GH, Jung J, Shin DH. Restarting anticoagulant therapy after intracranial hemorrhage in patients with atrial fibrillation: a nationwide retrospective cohort study. Int J Cardiol Heart Vasc. (2022) 40:101037. doi: 10.1016/j.ijcha.2022.101037
94. Eckman MH, Rosand J, Knudsen KA, Singer DE, Greenberg SM. Can patients be anticoagulated after intracerebral hemorrhage? A decision analysis. Stroke. (2003) 34:1710–6. doi: 10.1161/01.STR.0000078311.18928.16
95. Qureshi AI, Mendelow AD, Hanley DF. Intracerebral haemorrhage. Lancet. (2009) 373:1632–44. doi: 10.1016/S0140-6736(09)60371-8
96. Greenberg SM, Ziai WC, Cordonnier C, Dowlatshahi D, Francis B, Goldstein JN, et al. 2022 Guideline for the management of patients with spontaneous intracerebral hemorrhage: a guideline from the American heart association/American stroke association. Stroke. (2022) 53:e282–361. doi: 10.1161/str.0000000000000407
97. Hemphill JC 3rd, Greenberg SM, Anderson CS, Becker K, Bendok BR, Cushman M, et al. Guidelines for the management of spontaneous intracerebral hemorrhage: a guideline for healthcare professionals from the American heart association/American stroke association. Stroke. (2015) 46:2032–60. doi: 10.1161/STR.0000000000000069
98. Greenberg SM, Charidimou A. Diagnosis of cerebral amyloid angiopathy: evolution of the Boston criteria. Stroke. (2018) 49:491–7. doi: 10.1161/STROKEAHA.117.016990
99. Raposo N, Calviere L, Cazzola V, Planton M, Patsoura S, Wargny M, et al. Cortical superficial siderosis and acute convexity subarachnoid hemorrhage in cerebral amyloid angiopathy. Eur J Neurol. (2018) 25:253–9. doi: 10.1111/ene.13484
100. Wilson D, Hostettler IC, Ambler G, Banerjee G, Jäger HR, Werring DJ. Convexity subarachnoid haemorrhage has a high risk of intracerebral haemorrhage in suspected cerebral amyloid angiopathy. J Neurol. (2017) 264:664–73. doi: 10.1007/s00415-017-8398-y
101. Hawkes MA, Rabinstein AA. Anticoagulation for atrial fibrillation after intracranial hemorrhage: a systematic review. Neurol Clin Pract. (2018) 8:48–57. doi: 10.1212/cpj.0000000000000425
102. Biffi A, Kuramatsu JB, Leasure A, Kamel H, Kourkoulis C, Schwab K, et al. Oral anticoagulation and functional outcome after intracerebral hemorrhage. Ann Neurol. (2017) 82:755–65. doi: 10.1002/ana.25079
103. Cannegieter SC, Rosendaal FR, Briet E. Thromboembolic and bleeding complications in patients with mechanical heart valve prostheses. Circulation. (1994) 89:635–41. doi: 10.1161/01.cir.89.2.635
104. Vahanian A, Beyersdorf F, Praz F, Milojevic M, Baldus S, Bauersachs J, et al. 2021 ESC/EACTS guidelines for the management of valvular heart disease. Eur Heart J. (2022) 43:561–632. doi: 10.1093/eurheartj/ehab395
105. Chandra D, Gupta A, Grover V, Kumar Gupta V. When should you restart anticoagulation in patients who suffer an intracranial bleed who also have a prosthetic valve? Interact Cardiovasc Thorac Surg. (2013) 16:520–3. doi: 10.1093/icvts/ivs545
106. Kuramatsu JB, Sembill JA, Gerner ST, Sprugel MI, Hagen M, Roeder SS, et al. Management of therapeutic anticoagulation in patients with intracerebral haemorrhage and mechanical heart valves. Eur Heart J. (2018) 39:1709–23. doi: 10.1093/eurheartj/ehy056
107. Sánchez-Fuentes A, Rivera-Caravaca JM, López-Gálvez R, Marín F, Roldán V. Non-vitamin K antagonist oral anticoagulants and drug-food interactions: implications for clinical practice and potential role of probiotics and prebiotics. Front Cardiovasc Med. (2021) 8:787235. doi: 10.3389/fcvm.2021.787235
108. Gerritsen J, Smidt H, Rijkers GT, de Vos WM. Intestinal microbiota in human health and disease: the impact of probiotics. Genes Nutr. (2011) 6:209–40. doi: 10.1007/s12263-011-0229-7
109. Goldin BR. Intestinal microflora: metabolism of drugs and carcinogens. Ann Med. (1990) 22:43–8. doi: 10.3109/07853899009147240
110. Stöllberger C, Ernst G, Finsterer J. Is the left atrial appendage our most lethal attachment? Eur J Cardiothorac Surg. (2000) 18:625–6; author reply 627. doi: 10.1016/s1010-7940(00)00562-5
111. Vallurupalli S, Sharma T, Al'Aref S, Devabhaktuni SR, Dhar G. Left atrial appendage closure: an alternative to anticoagulation for stroke prevention in patients with kidney disease. Kidney360. (2022) 3:396–402. doi: 10.34067/kid.0004082021
112. Turagam MK, Osmancik P, Neuzil P, Dukkipati SR, Reddy VY. Left atrial appendage closure versus oral anticoagulants in atrial fibrillation: a meta-analysis of randomized trials. J Am Coll Cardiol. (2020) 76:2795–7. doi: 10.1016/j.jacc.2020.08.089
113. Reddy VY, Sievert H, Halperin J, Doshi SK, Buchbinder M, Neuzil P, et al. Percutaneous left atrial appendage closure vs warfarin for atrial fibrillation: a randomized clinical trial. JAMA. (2014) 312:1988–98. doi: 10.1001/jama.2014.15192
114. Fountain RB, Holmes DR, Chandrasekaran K, Packer D, Asirvatham S, Van Tassel R, et al. The PROTECT AF (WATCHMAN left atrial appendage system for embolic PROTECTion in patients with atrial fibrillation) trial. Am Heart J. (2006) 151:956–61. doi: 10.1016/j.ahj.2006.02.005
115. Holmes DR Jr., Kar S, Price MJ, Whisenant B, Sievert H, Doshi SK, et al. Prospective randomized evaluation of the watchman left atrial appendage closure device in patients with atrial fibrillation versus long-term warfarin therapy: the PREVAIL trial. J Am Coll Cardiol. (2014) 64:1–12. doi: 10.1016/j.jacc.2014.04.029
116. Osmancik P, Herman D, Neuzil P, Hala P, Taborsky M, Kala P, et al. Left atrial appendage closure versus direct oral anticoagulants in high-risk patients with atrial fibrillation. J Am Coll Cardiol. (2020) 75:3122–35. doi: 10.1016/j.jacc.2020.04.067
117. Lip GYH, Banerjee A, Boriani G, Chiang CE, Fargo R, Freedman B, et al. Antithrombotic therapy for atrial fibrillation: cHEST guideline and expert panel report. Chest. (2018) 154:1121–201. doi: 10.1016/j.chest.2018.07.040
118. Li YH, Fang CY, Hsieh IC, Huang WC, Lin TH, Sung SH, et al. 2018 Expert consensus on the management of adverse effects of antiplatelet therapy for acute coronary syndrome in Taiwan. Acta Cardiol Sin. (2018) 34:201–10. doi: 10.6515/acs.201805_34(3).20180302a
119. Brieger D, Amerena J, Attia J, Bajorek B, Chan KH, Connell C, et al. National heart foundation of Australia and the cardiac society of Australia and New Zealand: australian clinical guidelines for the diagnosis and management of atrial fibrillation 2018. Heart Lung Circ. (2018) 27:1209–66. doi: 10.1016/j.hlc.2018.06.1043
120. January CT, Wann LS, Calkins H, Chen LY, Cigarroa JE, Cleveland JC Jr., et al. 2019 AHA/ACC/HRS focused update of the 2014 AHA/ACC/HRS guideline for the management of patients with atrial fibrillation: a report of the American college of cardiology/American heart association task force on clinical practice guidelines and the heart rhythm society in collaboration with the society of thoracic surgeons. Circulation. (2019) 140:e125–151. doi: 10.1161/cir.0000000000000665
121. Andrade JG, Aguilar M, Atzema C, Bell A, Cairns JA, Cheung CC, et al. The 2020 Canadian cardiovascular society/Canadian heart rhythm society comprehensive guidelines for the management of atrial fibrillation. Can J Cardiol. (2020) 36:1847–948. doi: 10.1016/j.cjca.2020.09.001
122. Renou P, Thambo JB, Iriart X, Nicot S, Kabore N, Jalal Z, et al. Left atrial appendage closure in patients with atrial fibrillation and previous intracerebral hemorrhage. J Stroke Cerebrovasc Dis. (2017) 26:545–51. doi: 10.1016/j.jstrokecerebrovasdis.2016.11.126
123. Horstmann S, Zugck C, Krumsdorf U, Rizos T, Rauch G, Geis N, et al. Left atrial appendage occlusion in atrial fibrillation after intracranial hemorrhage. Neurology. (2014) 82:135–8. doi: 10.1212/wnl.0000000000000022
124. Fahmy P, Spencer R, Tsang M, Gooderham P, Saw J. Left atrial appendage closure for atrial fibrillation is safe and effective after intracranial or intraocular hemorrhage. Can J Cardiol. (2016) 32:349–54. doi: 10.1016/j.cjca.2015.07.723
125. Nielsen-Kudsk JE, Johnsen SP, Wester P, Damgaard D, Airaksinen J, Lund J, et al. Left atrial appendage occlusion versus standard medical care in patients with atrial fibrillation and intracerebral haemorrhage: a propensity score-matched follow-up study. EuroIntervention. (2017) 13:371–8. doi: 10.4244/eij-d-17-00201
126. Tzikas A, Freixa X, Llull L, Gafoor S, Shakir S, Omran H, et al. Patients with intracranial bleeding and atrial fibrillation treated with left atrial appendage occlusion: results from the amplatzer cardiac plug registry. Int J Cardiol. (2017) 236:232–6. doi: 10.1016/j.ijcard.2017.02.042
127. Casu G, D'Angelo G, Ugo F, Ronco F, Simonetto F, Barbierato M, et al. Left atrial appendage occlusion in atrial fibrillation patients with previous intracranial bleeding: a national multicenter study. Int J Cardiol. (2021) 328:75–80. doi: 10.1016/j.ijcard.2020.11.045
128. Boersma LV, Schmidt B, Betts TR, Sievert H, Tamburino C, Teiger E, et al. Implant success and safety of left atrial appendage closure with the WATCHMAN device: peri-procedural outcomes from the EWOLUTION registry. Eur Heart J. (2016) 37:2465–74. doi: 10.1093/eurheartj/ehv730
129. Holmes DR, Reddy VY, Turi ZG, Doshi SK, Sievert H, Buchbinder M, et al. Percutaneous closure of the left atrial appendage versus warfarin therapy for prevention of stroke in patients with atrial fibrillation: a randomised non-inferiority trial. Lancet. (2009) 374:534–42. doi: 10.1016/s0140-6736(09)61343-x
130. Viles-Gonzalez JF, Kar S, Douglas P, Dukkipati S, Feldman T, Horton R, et al. The clinical impact of incomplete left atrial appendage closure with the watchman device in patients with atrial fibrillation: a PROTECT AF (percutaneous closure of the left atrial appendage versus warfarin therapy for prevention of stroke in patients with atrial fibrillation) substudy. J Am Coll Cardiol. (2012) 59:923–9. doi: 10.1016/j.jacc.2011.11.028
131. Bergmann MW, Betts TR, Sievert H, Schmidt B, Pokushalov E, Kische S, et al. Safety and efficacy of early anticoagulation drug regimens after WATCHMAN left atrial appendage closure: three-month data from the EWOLUTION prospective, multicentre, monitored international WATCHMAN LAA closure registry. EuroIntervention. (2017) 13:877–84. doi: 10.4244/eij-d-17-00042
132. Krumsdorf U, Ostermayer S, Billinger K, Trepels T, Zadan E, Horvath K, et al. Incidence and clinical course of thrombus formation on atrial septal defect and patient foramen ovale closure devices in 1,000 consecutive patients. J Am Coll Cardiol. (2004) 43:302–9. doi: 10.1016/j.jacc.2003.10.030
133. Park JW, Bethencourt A, Sievert H, Santoro G, Meier B, Walsh K, et al. Left atrial appendage closure with amplatzer cardiac plug in atrial fibrillation: initial European experience. Catheter Cardiovasc Interv. (2011) 77:700–6. doi: 10.1002/ccd.22764
134. Hildick-Smith D, Landmesser U, Camm AJ, Diener HC, Paul V, Schmidt B, et al. Left atrial appendage occlusion with the amplatzer™ amulet™ device: full results of the prospective global observational study. Eur Heart J. (2020) 41:2894–901. doi: 10.1093/eurheartj/ehaa169
135. Takeda K, Tsuboko Y, Iwasaki K. Latest outcomes of transcatheter left atrial appendage closure devices and direct oral anticoagulant therapy in patients with atrial fibrillation over the past 5 years: a systematic review and meta-analysis. Cardiovasc Interv Ther. (2022) 37:725–38. doi: 10.1007/s12928-022-00839-1
136. Boersma LV, Ince H, Kische S, Pokushalov E, Schmitz T, Schmidt B, et al. Efficacy and safety of left atrial appendage closure with WATCHMAN in patients with or without contraindication to oral anticoagulation: 1-year follow-up outcome data of the EWOLUTION trial. Heart Rhythm. (2017) 14:1302–8. doi: 10.1016/j.hrthm.2017.05.038
137. Kirchhof P, Benussi S, Kotecha D, Ahlsson A, Atar D, Casadei B, et al. 2016 ESC guidelines for the management of atrial fibrillation developed in collaboration with EACTS. Eur J Cardiothorac Surg. (2016) 50:e1–88. doi: 10.1093/ejcts/ezw313
138. Block PC, Burstein S, Casale PN, Kramer PH, Teirstein P, Williams DO, et al. Percutaneous left atrial appendage occlusion for patients in atrial fibrillation suboptimal for warfarin therapy: 5-year results of the PLAATO (percutaneous left atrial appendage transcatheter occlusion) study. JACC Cardiovasc Interv. (2009) 2:594–600. doi: 10.1016/j.jcin.2009.05.005
139. Freeman JV, Higgins AY, Wang Y, Du C, Friedman DJ, Daimee UA, et al. Antithrombotic therapy after left atrial appendage occlusion in patients with atrial fibrillation. J Am Coll Cardiol. (2022) 79:1785–98. doi: 10.1016/j.jacc.2022.02.047
140. Della Rocca DG, Magnocavallo M, Di Biase L, Mohanty S, Trivedi C, Tarantino N, et al. Half-Dose direct oral anticoagulation versus standard antithrombotic therapy after left atrial appendage occlusion. JACC Cardiovasc Interv. (2021) 14:2353–64. doi: 10.1016/j.jcin.2021.07.031
141. Cohen JA, Heist EK, Galvin J, Lee H, Johnson M, Fitzsimons M, et al. A comparison of postprocedural anticoagulation in high-risk patients undergoing WATCHMAN device implantation. Pacing Clin Electrophysiol. (2019) 42:1304–9. doi: 10.1111/pace.13796
142. Holmes DR Jr., Korsholm K, Rodés-Cabau J, Saw J, Berti S, Alkhouli MA. Left atrial appendage occlusion. EuroIntervention. (2023) 18:e1038–1065. doi: 10.4244/eij-d-22-00627
143. Barakat AF, Wazni OM, Saliba WI, Saqi B, Abdur Rehman K, Tarakji K, et al. Initial experience with non-vitamin K antagonist oral anticoagulants for short-term anticoagulation after left atrial appendage closure device. JACC Clin Electrophysiol. (2017) 3:1472–3. doi: 10.1016/j.jacep.2017.02.013
144. Cepas-Guillen PL, Flores-Umanzor E, Regueiro A, Brugaletta S, Ibañez C, Sanchis L, et al. Low dose of direct oral anticoagulants after left atrial appendage occlusion. J Cardiovasc Dev Dis. (2021) 8:142. doi: 10.3390/jcdd8110142
145. Rodriguez-Gabella T, Nombela-Franco L, Regueiro A, Jiménez-Quevedo P, Champagne J, O'Hara G, et al. Single antiplatelet therapy following left atrial appendage closure in patients with contraindication to anticoagulation. J Am Coll Cardiol. (2016) 68:1920–1. doi: 10.1016/j.jacc.2016.08.016
146. Darmon A, Couture EL, Stein G, Cormier B, Chevalier B, Lefèvre T, et al. Left atrial appendage closure in patients with atrial fibrillation at very high bleeding risk without postimplantation antithrombotic therapy. J Invasive Cardiol. (2020) 32:385–91. PMID: 32999093.32999093
147. Pouru JP, Jaakkola S, Lund J, Biancari F, Saraste A, Airaksinen KEJ. Effectiveness of only aspirin or clopidogrel following percutaneous left atrial appendage closure. Am J Cardiol. (2019) 124:1894–9. doi: 10.1016/j.amjcard.2019.08.050
148. Jalal Z, Dinet ML, Combes N, Pillois X, Renou P, Sibon I, et al. Percutaneous left atrial appendage closure followed by single antiplatelet therapy: short- and mid-term outcomes. Arch Cardiovasc Dis. (2017) 110:242–9. doi: 10.1016/j.acvd.2016.09.006
149. Glikson M, Wolff R, Hindricks G, Mandrola J, Camm AJ, Lip GYH, et al. EHRA/EAPCI expert consensus statement on catheter-based left atrial appendage occlusion—an update. Europace. (2020) 22:184. doi: 10.1093/europace/euz258
150. Reddy VY, Möbius-Winkler S, Miller MA, Neuzil P, Schuler G, Wiebe J, et al. Left atrial appendage closure with the watchman device in patients with a contraindication for oral anticoagulation: the ASAP study (ASA plavix feasibility study with watchman left atrial appendage closure technology). J Am Coll Cardiol. (2013) 61:2551–6. doi: 10.1016/j.jacc.2013.03.035
151. Dukkipati SR, Kar S, Holmes DR, Doshi SK, Swarup V, Gibson DN, et al. Device-Related thrombus after left atrial appendage closure: incidence, predictors, and outcomes. Circulation. (2018) 138:874–85. doi: 10.1161/circulationaha.118.035090
152. Landmesser U, Tondo C, Camm J, Diener HC, Paul V, Schmidt B, et al. Left atrial appendage occlusion with the AMPLATZER amulet device: one-year follow-up from the prospective global amulet observational registry. EuroIntervention. (2018) 14:e590–7. doi: 10.4244/eij-d-18-00344
153. Weise FK, Bordignon S, Perrotta L, Konstantinou A, Bologna F, Nagase T, et al. Short-term dual antiplatelet therapy after interventional left atrial appendage closure with different devices. EuroIntervention. (2018) 13:e2138–46. doi: 10.4244/eij-d-17-00901
154. Price MJ, Gibson DN, Yakubov SJ, Schultz JC, Di Biase L, Natale A, et al. Early safety and efficacy of percutaneous left atrial appendage suture ligation: results from the U.S. Transcatheter LAA ligation consortium. J Am Coll Cardiol. (2014) 64:565–72. doi: 10.1016/j.jacc.2014.03.057
155. Lakkireddy D, Afzal MR, Lee RJ, Nagaraj H, Tschopp D, Gidney B, et al. Short and long-term outcomes of percutaneous left atrial appendage suture ligation: results from a US multicenter evaluation. Heart Rhythm. (2016) 13:1030–6. doi: 10.1016/j.hrthm.2016.01.022
156. Parikh V, Bartus K, Litwinowicz R, Turagam MK, Sadowski J, Kapelak B, et al. Long-term clinical outcomes from real-world experience of left atrial appendage exclusion with LARIAT device. J Cardiovasc Electrophysiol. (2019) 30:2849–57. doi: 10.1111/jce.14229
157. Mohanty S, Gianni C, Trivedi C, Gadiyaram V, Della Rocca DG, MacDonald B, et al. Risk of thromboembolic events after percutaneous left atrial appendage ligation in patients with atrial fibrillation: long-term results of a multicenter study. Heart Rhythm. (2020) 17:175–81. doi: 10.1016/j.hrthm.2019.08.003
158. Tomaselli GF, Mahaffey KW, Cuker A, Dobesh PP, Doherty JU, Eikelboom JW, et al. 2017 ACC expert consensus decision pathway on management of bleeding in patients on oral anticoagulants: a report of the American college of cardiology task force on expert consensus decision pathways. J Am Coll Cardiol. (2017) 70:3042–67. doi: 10.1016/j.jacc.2017.09.1085
159. Ahmed N, Audebert H, Turc G, Cordonnier C, Christensen H, Sacco S, et al. Consensus statements and recommendations from the ESO-karolinska stroke update conference, Stockholm 11–31 November 2018. Eur Stroke J. (2019), 4:307–17. doi: 10.1177/2396987319863606
160. Steffel J, Collins R, Antz M, Cornu P, Desteghe L, Haeusler KG, et al. 2021 European heart rhythm association practical guide on the use of non-vitamin K antagonist oral anticoagulants in patients with atrial fibrillation. Europace. (2021) 23:1612–76. doi: 10.1093/europace/euab065
161. January CT, Wann LS, Calkins H, Chen LY, Cigarroa JE, Cleveland JC Jr., et al. 2019 AHA/ACC/HRS focused update of the 2014 AHA/ACC/HRS guideline for the management of patients with atrial fibrillation: a report of the American college of cardiology/American heart association task force on clinical practice guidelines and the heart rhythm society. J Am Coll Cardiol. (2019) 74:104–32. doi: 10.1016/j.jacc.2019.01.011
Keywords: atrail fibrillation, oral anti coagulation, left atrial appendage (LAA) occlusion, intracranial hemorrhage, NOAC drugs
Citation: Lucà F, Colivicchi F, Oliva F, Abrignani M, Caretta G, Di Fusco SA, Giubilato S, Cornara S, Di Nora C, Pozzi A, Di Matteo I, Pilleri A, Rao CM, Parlavecchio A, Ceravolo R, Benedetto FA, Rossini R, Calvanese R, Gelsomino S, Riccio C and Gulizia MM (2023) Management of oral anticoagulant therapy after intracranial hemorrhage in patients with atrial fibrillation. Front. Cardiovasc. Med. 10:1061618. doi: 10.3389/fcvm.2023.1061618
Received: 4 October 2022; Accepted: 14 April 2023;
Published: 25 May 2023.
Edited by:
Matteo Anselmino, University of Turin, ItalyReviewed by:
Carlo de Asmundis, University Hospital Brussels, BelgiumMario Matta, AOU Città della Salute e della Scienza, Italy
© 2023 Lucà, Colivicchi, Oliva, Abrignani, Caretta, Di Fusco, Giubilato, Cornara, Di Nora, Pozzi, Di Matteo, Pilleri, Rao, Parlavecchio, Ceravolo, Benedetto, Rossini, Calvanese, Gelsomino, Riccio and Gulizia. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Fabiana Lucà ZmFiaWFuYS5sdWNhOTJAZ21haWwuY29t