 Se-Eun Kim
Se-Eun Kim Dae-Young Kim2
Dae-Young Kim2 Iksung Cho
Iksung Cho Geu-Ru Hong
Geu-Ru Hong Chi Young Shim
Chi Young Shim
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Cardiovasc. Med. , 04 October 2022
Sec. Cardiovascular Imaging
Volume 9 - 2022 | https://doi.org/10.3389/fcvm.2022.985122
This article is part of the Research Topic Insights in Cardiovascular Imaging: 2022 View all 29 articles
Background: This study aimed to investigate the prognostic value of left atrial (LA) strain in patients with significant mitral regurgitation (MR) after surgical mitral valve (MV) repair.
Methods: A total of 169 patients (age 55 ± 15 years, 88 men) with moderate or severe MR on echocardiogram at least 6 months after surgical MV repair for primary MR were studied. Two-dimensional, Doppler, and speckle tracking echocardiography including MR quantitative measures, chamber size, and LA strain were comprehensively analyzed. The primary outcome was a composite of cardiovascular death, heart failure hospitalization, and MV reoperation.
Results: During a median of 44.4 months [interquartile range (IQR): 18.7–70.3 months] of follow-up, 44 patients (26%) experienced clinical events; these patients had greater MR volume, elevated mean diastolic pressure gradient and pulmonary artery systolic pressure, and enlarged chamber size compared with patients who did not experience events. Patients with events showed significantly lower LA strain [13.3% (IQR: 9.3–23.8%) vs. 24.0% (IQR: 13.1–31.4%), p = 0.003] and higher MR volume/LA strain [3.09 ml/% (IQR: 2.06–5.80 ml/%) vs. 1.57 ml/% (IQR: 1.04–2.72 ml/%), p < 0.001] than those without events. MR volume/LA strain was a good predictor of clinical outcomes (cut-off 1.57 ml/%, area under the curve 0.754, p < 0.001). On multivariable Cox proportional analysis, MR volume/LA strain was independently associated with clinical outcomes (hazard ratio: 1.269, 95% confidence interval: 1.109–1.452, p < 0.001) along with pulmonary artery systolic pressure.
Conclusion: A measure of LA mechanical function relative to MR volume is associated with clinical outcomes in patients with significant MR after surgical MV repair.
Residual or recurrent mitral regurgitation (MR) after surgical mitral valve (MV) repair can occur even in excellent centers with a high MV repair success rate (1–3). Despite the relatively high recurrence of MR in patients who have undergone MV repair, treatment guidelines for these patients have not yet been established (4, 5). Therefore, when significant MR occurs after MV repair, clinicians usually decide the timing of reoperation depending on the severity of patient symptoms. In particular, significant MR after MV repair differs from primary native MR in terms of cardiac remodeling, so there is a limit to applying criteria such as increased left ventricular (LV) end-systolic dimension or decreased LV ejection fraction as indications for MV reoperation. Moreover, as the number of patients undergoing trans-catheter MV intervention for primary MR, including trans-catheter edge-to-edge repair (TEER), increases, there is a greater need for objective echocardiographic parameters to monitor the hemodynamic consequences of moderate to severe MR and determine the timing of the re-intervention or operation (6, 7).
Left atrial (LA) mechanical dysfunction assessed by two-dimensional speckle tracking echocardiography has been useful for predicting clinical outcomes in various cardiovascular diseases including atrial fibrillation, stroke, and heart failure (8–10). Theoretically, in patients who underwent MV repair, there is unavoidable restriction of the mitral annulus and little mitral stenosis physiology (11). Therefore, LA enlargement and mechanical dysfunction are more important than changes in LV in the presence of significant MR after MV repair. We hypothesized that LA strain, as a marker of LA mechanical function, can predict clinical outcomes in patients who present with significant MR after surgical MV repair. To prove this hypothesis, we sought to comprehensively analyze conventional and speckle tracking echocardiography and to identify predictors of clinical outcomes.
From the echocardiographic database from January 2005 to December 2019 at Severance Cardiovascular Hospital, Seoul, Korea, 1,549 patients who underwent surgical MV repair were identified. After exclusion of 1,239 patients with no or mild MR on echocardiogram, 310 patients with significant (at least moderate) MR, either residual or recurrent MR, were selected. Among them, a total of 169 patients with moderate or severe MR on echocardiogram at least 6 months after surgical MV repair for primary MR were enrolled, after excluding cases that met the following criteria: patients who underwent their MV repair for secondary MR; patients with poor-quality echocardiographic imaging; patients who underwent concomitant aortic valve surgery; patients who underwent reoperation for reasons other than MR; patients who underwent reoperation within 6 months of first MV repair; and patients without postoperative echocardiography 6 months after MV repair. The patients who underwent tricuspid annuloplasty and coronary artery bypass grafting surgery were included. The enrolled patients were divided into two groups according to the occurrence of clinical events (Figure 1). Clinical events were defined as a composite of cardiovascular deaths, heart failure hospitalization, and MV reoperation. All patients underwent postoperative TTE before discharge. Clinical and/or echocardiographic follow-up was performed 6 months after MV repair and annually thereafter in accordance with the institution’s follow-up protocol. Residual MR was defined when MR was confirmed in the postoperative TTE, and recurrent MR was defined as a case in which there was no MR in the postoperative TTE but confirmed in the follow-up TTE at least 6 months after surgery. The parameters of echocardiography used for the analysis are the parameters at the time of occurrence of significant MR in echocardiography at least 6 months after surgery. All laboratory or clinical information was collected from electronic medical records. A study protocol was developed according to the principles of the Declaration of Helsinki and was approved by the Institutional Review Board of Severance Hospital.
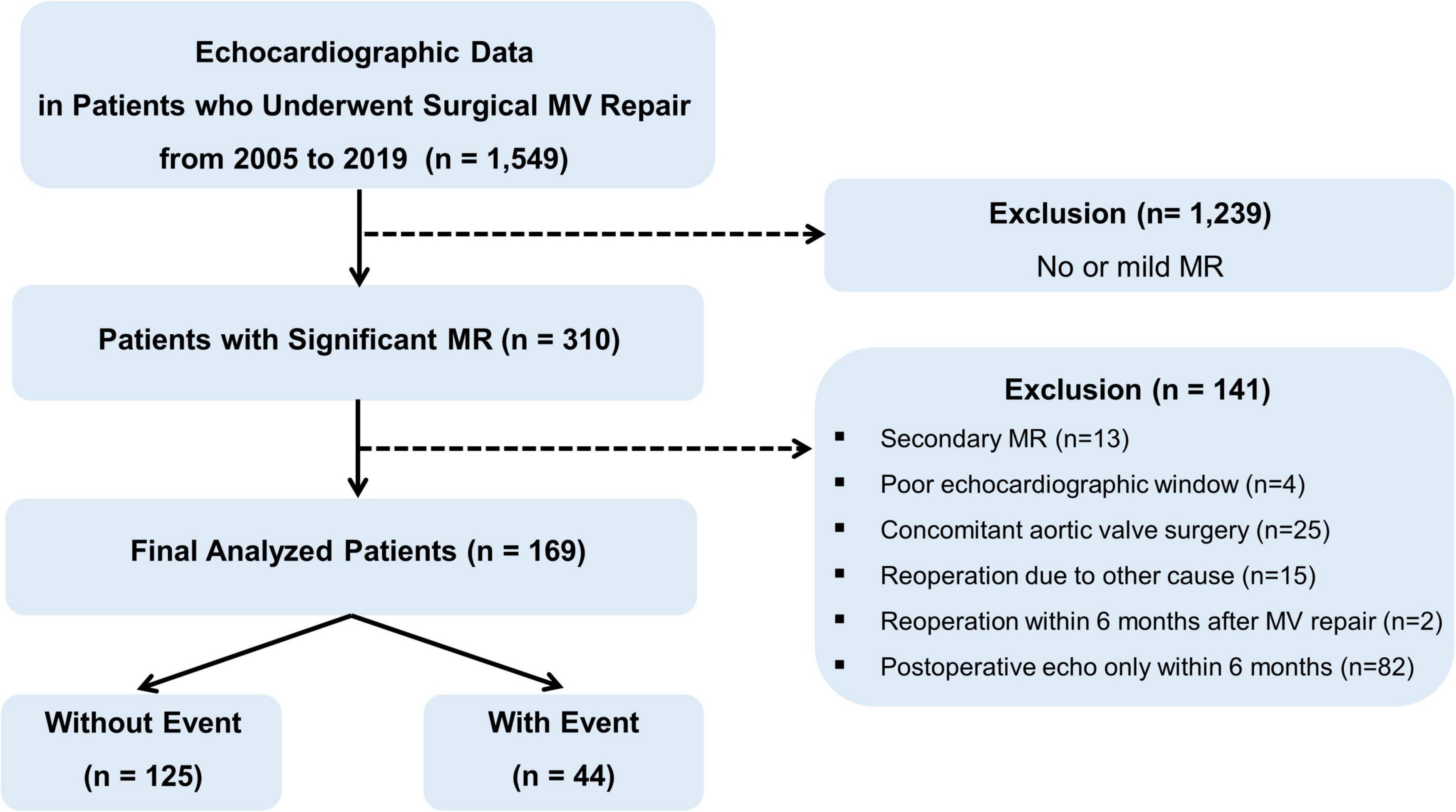
Figure 1. Study flow and design.
Transthoracic echocardiography was performed using a standard ultrasound machine (Vivid 7 or E9; GE Medical Systems; Wauwatosa, WI, Philips iE33 or Epiq7; Philips Healthcare; Netherlands) with a 2.5–3.5-MHz probe. Standard echocardiographic measurements were performed according to the recommendations of the American Society of Echocardiography guidelines (12). LA and LV volume, and LV ejection fraction (LVEF) were derived from standard apical 4- and 2-chamber views using the biplane method of disks. LA volume index was calculated by dividing LA volume by body surface area of patients (12). Total LA emptying fraction (TLAEF) was calculated as (maximal LA volume - minimal LA volume)/maximal LA volume × 100% (13). Maximal LA volume was defined as volume just before the MV closed and minimal LA volume was defined as volume just after the MV closed (13). Repaired MV function was assessed through a multi-parametric approach according to the guidelines of the American Society of Echocardiography using the following parameters (6, 14). Mean diastolic pressure gradient (MDPG) was assessed by continuous-wave Doppler. MR severity was determined based on volumetric methods including effective regurgitant orifice area (EROA), MR volume and MR fraction (6). Pulmonary artery systolic pressure (PASP) was determined using tricuspid regurgitation velocity and inferior vena cava diameter. In patients with atrial fibrillation, Doppler echocardiographic parameters were measured at the average of three cardiac cycles when the R-R interval was relatively regular.
Speckle tracking echocardiography was performed to evaluate LA and LV myocardial function. The analysis was performed offline using commercially available software (TomTec software; Image Arena 4.6, Munich, Germany). LA strain was obtained from apical 4- and 2-chamber images by semi-automatic endocardial border tracking and manual adjustment to optimize tracking (15). Among the 3 phases of atrial strain (reservoir, conduit, and contractile), LA strain was calculated by averaging the reservoir from 4- and 2-chamber images (15, 16). LV strain was obtained from acquired apical 4-chamber, apical 3-chamber, and apical 2-chamber views semi-automatically. LV global longitudinal strain (GLS) was calculated by averaging the peak strain value of 3 apical views (15, 17, 18). All data were performed and analyzed by two experienced individuals who were blinded to data analysis. To examine intra- and inter observer variability for LA and LV strain, two individuals repeated the analysis of the 20 consecutive patients. Since the amount of MR was diverse even in patients with significant MR, the ratio of MR volume to LA strain (MR volume/LA strain, ml/%) was used as a composite variable of MR severity and LA mechanical function.
The study was followed from the index date, which a significant MR was diagnosed, until clinical events occurred or the study period ended on December 31, 2020. Continuous variables with a normal distribution were expressed as mean ± standard deviation and compared using Student’s t-test. Non-normally distributed variables were expressed as median [interquartile range (IQR)] and compared using Wilcoxon Rank Sum test. Categorical variables were presented as frequencies (percentages,%) and compared using the chi-square test or Fisher’s exact test. The predictive value of MR volume, LA strain, and MR volume/LA strain for the primary outcomes was calculated using receiver operating characteristic (ROC) analysis. Kaplan-Meier survival analyses and log-rank tests were used to compare clinical outcomes according to cutoff values for LA strain and MV volume/LA strain during the follow-up period. Univariate and multivariate Cox proportional analyses were used to obtain adjusted hazard ratios (HRs) with 95% confidence intervals (CIs) for evaluating the risk of events. The variables selected for entry into multivariate analysis were those with a p-value < 0.10 in univariate analysis. Multivariate analysis was conducted in two models. Model 1 was analyzed including LA strain, while model 2 was analyzed with MR volume/LA strain. A two-sided p-value of <0.05 was considered significant. Intra- and inter-observer variability values are expressed intra-class correlation coefficients (ICCs). Statistical analyses were conducted using SPSS software version 20 (SAS Institute Inc., Cary, NC, USA) and R software (version 3.6.3; R Foundation for Statistical Computing, Vienna, Austria).
During a median 44.1 months [interquartile range (IQR): 18.7–70.3 months] of follow-up, among 169 patients, 44 patients (26%) experienced clinical events including 3 cardiovascular deaths, 10 heart failure hospitalizations, and 35 reoperations for MV (27 MV replacement and 8 redo-repair). Table 1 presents the baseline characteristics of the study population according to the occurrence of clinical events. Baseline characteristics did not differ between the two groups, except for higher prevalence of atrial fibrillation and lower estimated glomerular filtration rate in the event group. The most common etiology before MV repair was prolapse of MV. MR etiology before repair and device used for surgical MV repair were also comparable. However, LV and LA size were significantly larger in patients who experienced events compared to those who did not. There was no difference in LV function (LVEF and LV GLS) between the two groups, but LA function (LA strain and TLAEF) was significantly reduced in patients who experienced events compared to those who did not [LA strain: 13.3% (IQR: 9.3–23.8%) vs. 24.0% (IQR: 13.1–31.4%), p = 0.003]. MR was more severe in patients who experienced events, and TR was also more severe. Thus, MR volume/LA strain was remarkably higher in the event group than the non-event group [3.09 ml/% (IQR: 2.06–5.80 ml/%) vs. 1.57 ml/% (IQR: 1.04–2.72 ml/%), p < 0.001]. PASP was also significantly higher in patients who experienced events [37.5 mmHg (IQR: 28.0–46.3 mmHg) vs. 29.9 mmHg (IQR: 25.0–35.0 mmHg), p < 0.001, Table 2]. There are 75 patients who had residual significant MR. However, there were no significant difference for parameters for cardiac function assessed by TTE, except LV mass index between patients with residual MR and those with recurrent MR (Supplementary Table 1).
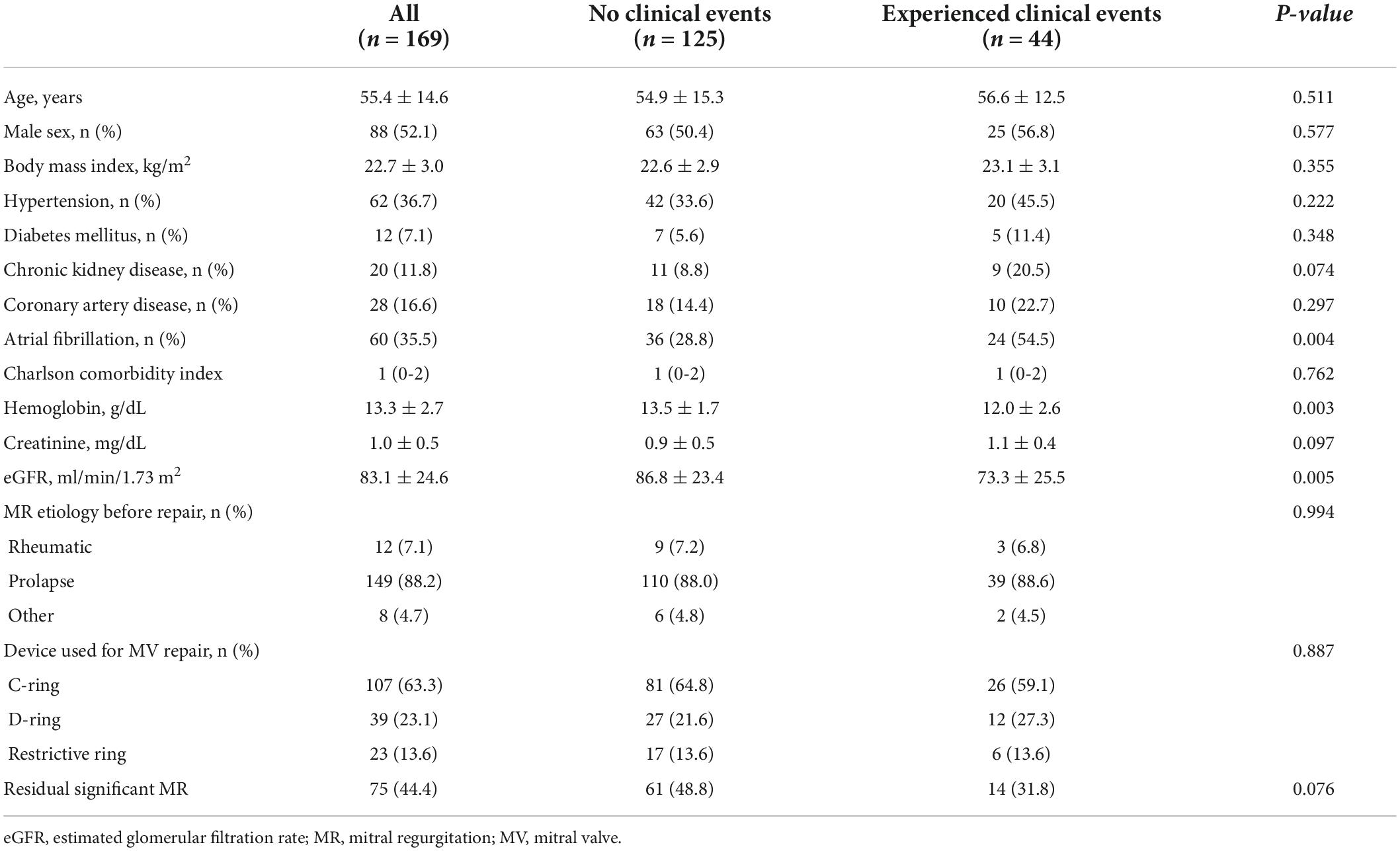
Table 1. Baseline characteristics of the study population.
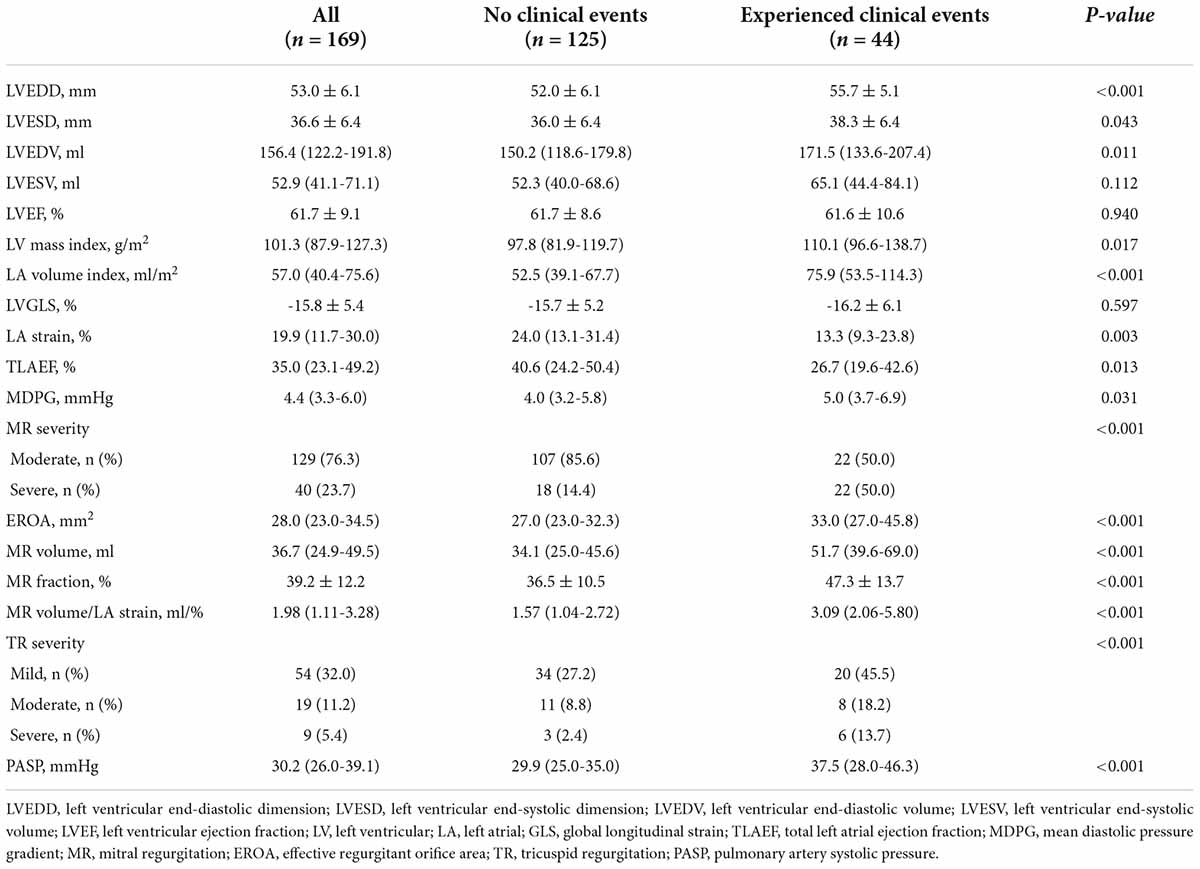
Table 2. Baseline echocardiographic characteristics of the study population.
Receiver operating characteristic was performed to evaluating the predictive value of LA mechanical function for clinical outcomes in this population. LA strain had good predictive performance for clinical outcomes [cut-off 15.3%, area under the curve (AUC) 0.661, p = 0.003]. The AUC for MR volume/LA strain was significantly larger than that of LA strain (cut-off 1.57 ml/%, AUC 0.754, p < 0.001) (comparison of both AUCs: p = 0.032) (Figure 2). Figure 3 is a representative case of reduced LA mechanical function and larger MR volume in a patient that experienced a clinical event.
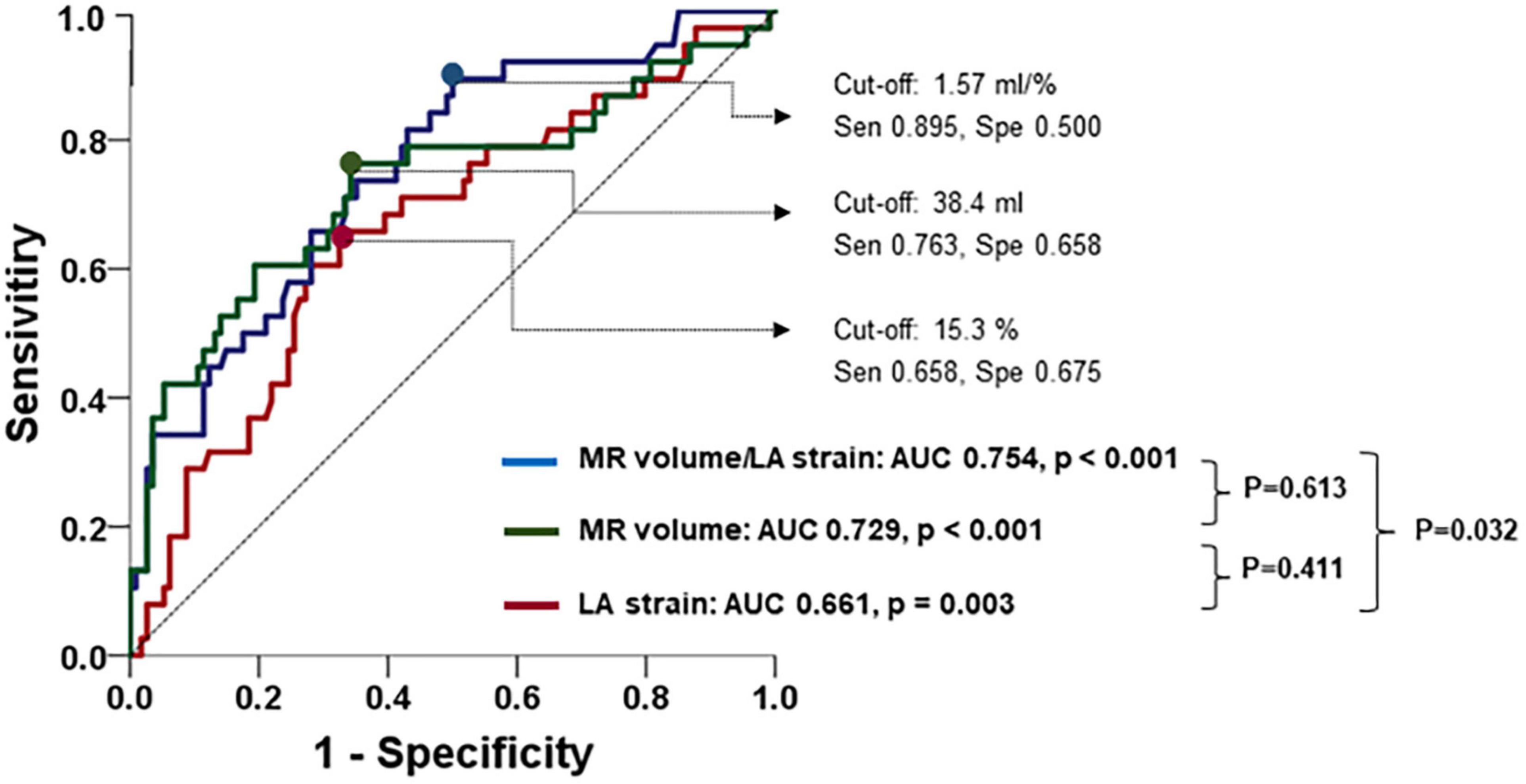
Figure 2. Predictive value of MR volume, LA strain, and their ratio for the occurrence of adverse clinical outcomes.
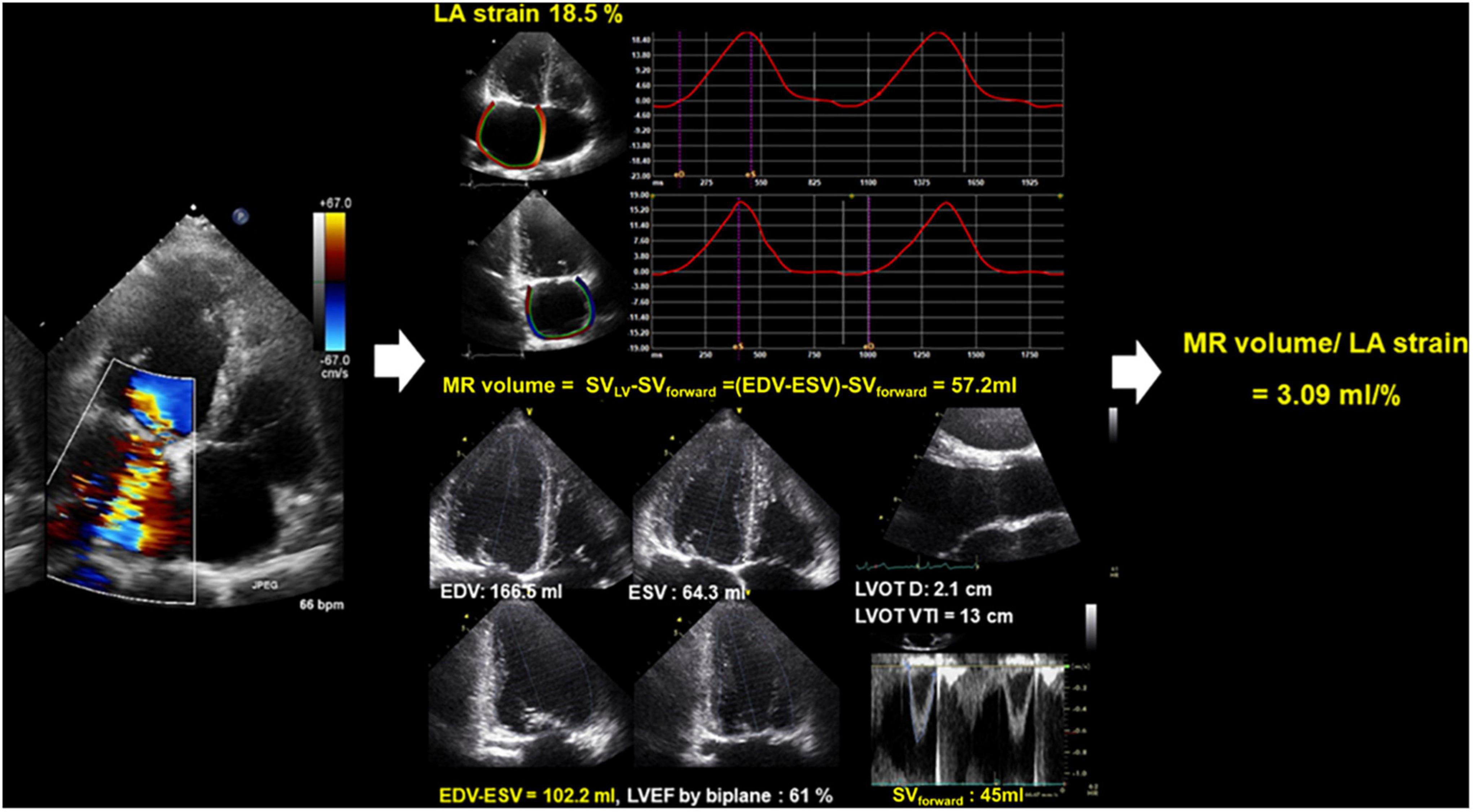
Figure 3. Representative case of LA mechanical dysfunction and the amount of MR in a patient with significant MR after surgical MV repair. EDV, end-diastolic volume; ESV, end-systolic volume; LA, left atrium; LVEF, left ventricular ejection fraction; LVOT D, left ventricular outflow tract distance; LVOT VTI, left ventricular outflow tract velocity time integral; MR, mitral regurgitation; SV, stroke volume.
Kaplan–Meier curves according to LA strain and MR volume/LA strain cutoffs are shown in Figure 4. Patients with reduced LA strain ≤15.5% had significantly more events compared with those with LA strain > 15.5% (Log-rank p = 0.001). In addition, patients with MR volume/LA strain > 1.6 ml/% exhibited poorer clinical outcomes than those with MR volume/LA strain ≤ 1.6 ml/% (Log-rank p < 0.001).
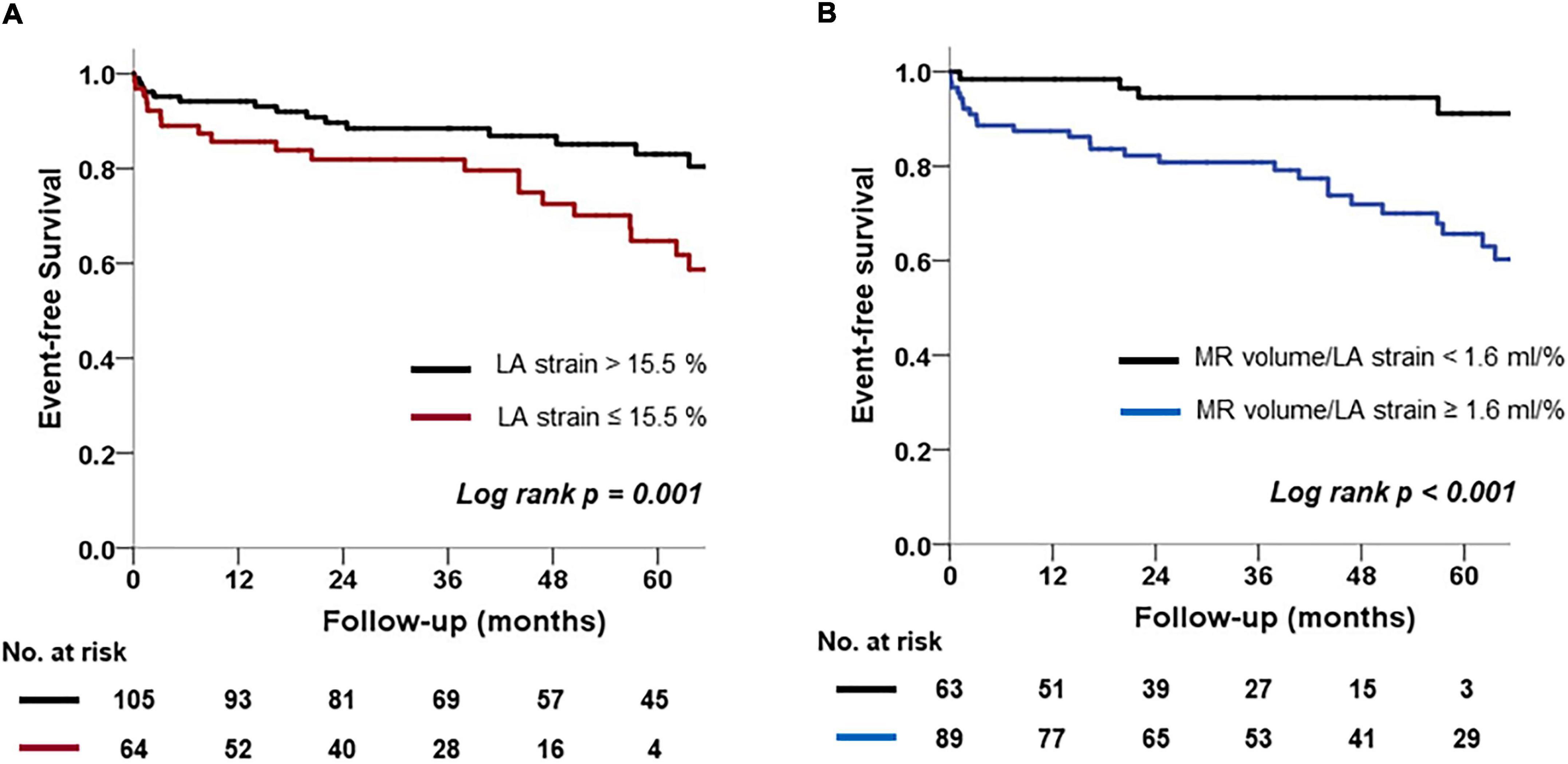
Figure 4. Kaplan-Meier analysis of freedom from clinical outcomes. (A) Comparison of two groups according to a cutoff value for LA strain. (B) Comparison of two groups according to a cutoff value for MR volume/LA strain.
Table 3 displays univariate and multivariate Cox-proportional analysis results for clinical outcomes. MR severity, LV and LA size, LA strain, MR volume/LA strain, and PASP were significantly correlated with clinical outcomes in univariate analysis. After adjustment, LA strain was not an independent factor for clinical outcomes [hazard ratio (HR): 0.993, 95% confidence interval (CI): 0.945–1.043, p = 0.765], but MR volume/LA strain, a measure of LA mechanical dysfunction relative to MR, was independently associated with clinical outcomes (HR: 1.269, 95% CI: 1.109–1.452, p < 0.001), as was PASP. As a result of Cox-proportional analysis of clinical results by dividing residual MR and recurrent MR, MR volume/LA strain was a significant factor in both groups (Supplementary Table 2).
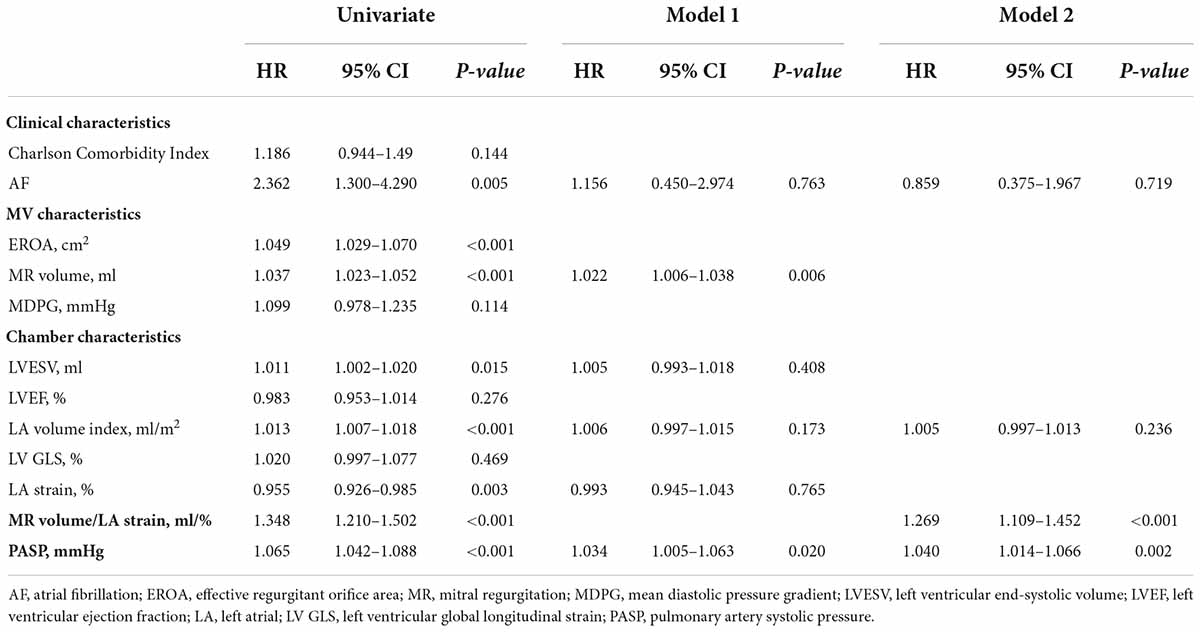
Table 3. Cox proportional analysis for clinical outcomes.
To assess variability for LA strain and LV GLS, two individuals repeated the analysis of the 20 consecutive patients. The ICCs revealed excellent reliability for LA strain and LV GLS, with the ICCs generally > 0.9. The intra- and inter-observer ICCs for LA strain were 0.97 (0.93–0.98) and 0.91 (0.79–0.96) and those for LV GLS were 0.99 (0.97–1.00) and 0.94 (0.88–0.98), respectively.
The main findings in this study are as follows: (1) in patients with significant MR after surgical MV repair, patients with clinical events exhibited decreased LA strain compared to those without clinical events; (2) LA strain assessed by two-dimensional speckle tracking echocardiography was a good predictor of clinical outcomes; (3) an index of reduced LA mechanical function relative to the amount of MR was independently associated with clinical outcomes after controlling for confounding factors. These findings suggest that an LA strain-based echocardiographic parameter might be useful for risk stratification and decision making for re-intervention in patients with significant MR after MV repair.
In the early phase of MR, LA and LV compensate for volume overload, but if chronic volume overload continues, further LA and LV remodeling occurs, resulting in cardiac chamber dilatation and dysfunction (19, 20). After successful MV surgery, reverse remodeling occurs at least 6 months (21, 22). While some patients recover from LA and LV mechanical dysfunction, other patients exhibit irreversible LA and LV damage accompanied by cardiac fibrosis (21, 23). LA and LV enlargement are commonly observed in patients who undergo MV repair. Moreover, absolute value of LA strain and LV GLS assessed by speckle tracking echocardiography in patients treated for MV are usually lower than absolute reference values (16, 24, 25). Therefore, it is difficult to decide the optimal timing of re-intervention or repeat surgery using the same chamber enlargement or dysfunction criteria used for de novo MR patients. Many studies have suggested that the presence of LA and LV mechanical dysfunction before MV surgery have prognostic implications for MV surgery in patients with chronic severe MR (26–28). However, there are no large-scale studies on which factors, including LA and LV mechanical dysfunction, have prognostic implications when significant MR occurs in patients undergoing MV repair.
The severity of valvular disease and changes in chamber function that are directly affected by severity are very important factors in determining outcomes (29). Therefore, rather than independently considering the severity of valvular disease or changes in chamber function, we focused on the fact that a robust correlation with outcome can be expected if indexed with a numerical value that reflects these two together. For example, when a large amount of water is put in a balloon, if the balloon has good distensibility, the balloon will not burst or overflow with water. Therefore, the correlation with outcomes was identified through RV/LAGLS, a new parameter representing the change in MR volume, a quantitative assessment of MR severity and LV function. As a result, in this study, it was confirmed that small RV/low LAGLS and large RV/high LAGLS showed similar outcome rates (Supplementary Figure 1B). After all, even in the similar MR severity, if the LA function is good, there may be fewer events, and conversely, if the LA function is low, many events may occur. This study showed that RV/LAGLS, as parameter that reflects LA function in MR severity, will play an important role in predicting prognosis.
Previous studies have reported the incidence and outcomes of recurrence of MR after surgical MV repair (1, 2). A study in patients with degenerative MV disease demonstrated significant recurrence of MR (3.7% annually) during 7 years of follow-up after MV repair (1). In another long-term study of 1,234 patients who underwent MV repair, 60.4% of patients did not experience any events for approximately 20 years; 12.5% had moderate or severe MR, and only 4.6% underwent re-operation for MR (2). Recently, as various trans-catheter interventions as well as surgical MV repair have been performed as alternative treatments for severe MR, there is growing interest in significant MR after MV repair (30–33). Chronic significant MR after MV repair differs from primary native MR in terms of cardiac remodeling, so there is a limit to applying criteria such as increased LV dimensions and LV dysfunction when making decisions regarding MV reoperation.
The present study suggests important points for clinical decision-making. First, increased PASP in patients with significant MR after MV repair is an important prognostic factor, as proven in patients with chronic native MR (34). Second, even in patients with significant MR, quantitative measurement of MR amount is helpful for risk stratification. Third, an index of LA mechanical dysfunction relative to MR amount is an important prognostic factor in patients with significant MR after MV repair. These findings will be clinically useful for decision-making and clinical follow-up for significant MR after MV repair.
Our study has some limitations. First, as this was a single-center, retrospective study, there are fundamental limitations. Further multicenter studies and large-scale cohorts are necessary. Second, the postoperative echocardiography period at which significant MR was observed varied, and both residual MR and recurrent MR were included in this study. However, essentially, both residual and recurrent MR are MV regurgitation, and if there are factors affecting the clinical outcome at the time when significant MR is confirmed, appropriate intervention is required regardless of residual or recurrent. Routine institutional echocardiographic follow-up after surgical MV repair was conducted 6 months after the surgery and annually thereafter. Therefore, we believe that these results meet the research objective of identifying clinically meaningful echocardiographic parameters in the presence of significant MR in patients with repaired MV. Third, LA mechanical dysfunction was an important test variable, but LA strain did not show an independent association with clinical outcomes in multivariate analysis. However, MR volume/LA strain, which is an index of MR amount in LA mechanical dysfunction, was independently associated with clinical outcome. Since our study targeted moderate or more MR, we think that it is acceptable result that the measurement value for the degree of MR is important together with the LA mechanical function.
Left atrial mechanical dysfunction relative to increased MR amount is associated with poor clinical outcomes in patients with significant MR after surgical MV repair.
The original contributions presented in this study are included in the article/Supplementary material, further inquiries can be directed to the corresponding author.
This study was reviewed and approved by the Institutional Review Board of Severance Hospital. The study protocol was developed according to the principles of the Declaration of Helsinki. Written informed consent for participation was not required for this study in accordance with the national legislation and the institutional requirements.
S-EK and CS: conception, planning and/or conducting the study, and drafting the manuscript. S-EK, D-YK, JS, IC, G-RH, J-WH, and CS: collecting and interpreting data. CS: guarantor of the article. All authors contributed to the article and approved the submitted version.
This study was supported by a faculty research grant from Yonsei University College of Medicine (6-2021-0096).
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fcvm.2022.985122/full#supplementary-material
Supplementary Figure 1 | Kaplan–Meier analysis of freedom from clinical outcomes. (A) Comparison according to MR severity. (B) Comparison of four groups according to RV and LAGLS.
CI, confidence interval; EROA, effective regurgitant orifice area; GLS, global longitudinal strain; HR, hazard ratio; ICC, intra-class correlation coefficients; LA, left atrial; LV, left ventricle; LVEF, left ventricular ejection fraction; MDPG, mean diastolic pressure gradient; MR, mitral regurgitation; MV, mitral valve; PASP, pulmonary artery systolic pressure; ROC, receiver operating characteristic; TEER, transcatheter edge-to-edge repair; TLAEF, total LA emptying fraction.
1. Flameng W, Herijgers P, Bogaerts K. Recurrence of mitral valve regurgitation after mitral valve repair in degenerative valve disease. Circulation. (2003) 107:1609–13. doi: 10.1161/01.CIR.0000058703.26715.9D
2. David TE, David CM, Tsang W, Lafreniere-Roula M, Manlhiot C. Long-term results of mitral valve repair for regurgitation due to leaflet prolapse. J Am Coll Cardiol. (2019) 74:1044–53. doi: 10.1016/j.jacc.2019.06.052
3. Kaneyuki D, Nakajima H, Asakura T, Yoshitake A, Tokunaga C, Tochii M, et al. Recurrent mitral regurgitation after mitral valve repair for bileaflet lesions in the modern era. J Cardiothorac Surg. (2019) 14:205. doi: 10.1186/s13019-019-1035-3
4. Otto CM, Nishimura RA, Bonow RO, Carabello BA, Erwin JP III, Gentile F, et al. 2020 ACC/AHA guideline for the management of patients with Valvular Heart Disease: a report of the American college of cardiology/American Heart Association joint committee on clinical practice guidelines. Circulation. (2021) 143:e72–227. doi: 10.1161/CIR.0000000000000923
5. Vahanian A, Beyersdorf F, Praz F, Milojevic M, Baldus S, Bauersachs J, et al. 2021 ESC/EACTS Guidelines for the management of valvular heart disease. Eur Heart J. (2021) 60:727–800. doi: 10.1093/ejcts/ezac209
6. Zoghbi WA, Asch FM, Bruce C, Gillam LD, Grayburn PA, Hahn RT, et al. Guidelines for the evaluation of valvular regurgitation after percutaneous valve repair or replacement: a report from the American Society of echocardiography developed in collaboration with the society for cardiovascular angiography and interventions, Japanese Society of Echocardiography, and society for cardiovascular magnetic resonance. J Am Soc Echocardiogr. (2019) 32:431–75. doi: 10.1016/j.echo.2019.01.003
7. Mantegazza V, Pasquini A, Agati L, Fusini L, Muratori M, Gripari P, et al. Comprehensive assessment of mitral valve geometry and cardiac remodeling with 3-dimensional echocardiography after percutaneous mitral valve repair. Am J Cardiol. (2018) 122:1195–203. doi: 10.1016/j.amjcard.2018.06.036
8. Sarvari SI, Haugaa KH, Stokke TM, Ansari HZ, Leren IS, Hegbom F, et al. Strain echocardiographic assessment of left atrial function predicts recurrence of atrial fibrillation. Eur Heart J Cardiovasc Imaging. (2016) 17:660–7. doi: 10.1093/ehjci/jev185
9. Kim D, Shim CY, Hong GR, Kim MH, Seo J, Cho IJ, et al. Clinical implications and determinants of left atrial mechanical dysfunction in patients with stroke. Stroke. (2016) 47:1444–51. doi: 10.1161/STROKEAHA.115.011656
10. Reddy YNV, Obokata M, Verbrugge FH, Lin G, Borlaug BA. Atrial dysfunction in patients with heart failure with preserved ejection fraction and atrial fibrillation. J Am Coll Cardiol. (2020) 76:1051–64. doi: 10.1016/j.jacc.2020.07.009
11. Chan V, Mesana T, Verma S. Functional mitral stenosis following mitral valve repair. Curr Opin Cardiol. (2017) 32:161–5. doi: 10.1097/HCO.0000000000000364
12. Lang RM, Badano LP, Mor-Avi V, Afilalo J, Armstrong A, Ernande L, et al. Recommendations for cardiac chamber quantification by echocardiography in adults: an update from the American Society of Echocardiography and the European Association of Cardiovascular Imaging. Eur Heart J Cardiovasc Imaging. (2015) 16:233–70. doi: 10.1093/ehjci/jev014
13. Blume GG, McLeod CJ, Barnes ME, Seward JB, Pellikka PA, Bastiansen PM, et al. Left atrial function: physiology, assessment, and clinical implications. Eur J Echocardiogr. (2011) 12:421–30. doi: 10.1093/ejechocard/jeq175
14. Zoghbi WA, Adams D, Bonow RO, Enriquez-Sarano M, Foster E, Grayburn PA, et al. Recommendations for noninvasive evaluation of native valvular regurgitation: a report from the American Society of Echocardiography developed in collaboration with the society for cardiovascular magnetic resonance. J Am Soc Echocardiogr. (2017) 30:303–71.
15. Badano LP, Kolias TJ, Muraru D, Abraham TP, Aurigemma G, Edvardsen T, et al. Standardization of left atrial, right ventricular, and right atrial deformation imaging using two-dimensional speckle tracking echocardiography: a consensus document of the EACVI/ASE/Industry Task Force to standardize deformation imaging. Eur Heart J Cardiovasc Imaging. (2018) 19:591–600. doi: 10.1093/ehjci/jey042
16. Pathan F, D’Elia N, Nolan MT, Marwick TH, Negishi K. Normal ranges of left atrial strain by speckle-tracking echocardiography: a systematic review and meta-analysis. J Am Soc Echocardiogr. (2017) 30:59–70.e8. doi: 10.1016/j.echo.2016.09.007
17. Voigt JU, Pedrizzetti G, Lysyansky P, Marwick TH, Houle H, Baumann R, et al. Definitions for a common standard for 2D speckle tracking echocardiography: consensus document of the EACVI/ASE/Industry Task Force to standardize deformation imaging. Eur Heart J Cardiovasc Imaging. (2015) 16:1–11. doi: 10.1093/ehjci/jeu184
18. Negishi K, Negishi T, Kurosawa K, Hristova K, Popescu BA, Vinereanu D, et al. Practical guidance in echocardiographic assessment of global longitudinal strain. JACC Cardiovasc Imaging. (2015) 8:489–92. doi: 10.1016/j.jcmg.2014.06.013
19. Borg AN, Pearce KA, Williams SG, Ray SG. Left atrial function and deformation in chronic primary mitral regurgitation. Eur J Echocardiogr. (2009) 10:833–40. doi: 10.1093/ejechocard/jep085
20. Cameli M, Lisi M, Giacomin E, Caputo M, Navarri R, Malandrino A, et al. Chronic mitral regurgitation: left atrial deformation analysis by two-dimensional speckle tracking echocardiography. Echocardiography. (2011) 28:327–34. doi: 10.1111/j.1540-8175.2010.01329.x
21. Chipeta P, Shim CY, Hong G-R, Kim D, Cho IJ, Lee S, et al. Time course of left atrial reverse remodelling after mitral valve surgery and the impact of left ventricular global longitudinal strain in patients with chronic severe mitral regurgitation. Interact Cardiovasc Thor Surgery. (2016) 23:876–82. doi: 10.1093/icvts/ivw287
22. Shafii AE, Gillinov AM, Mihaljevic T, Stewart W, Batizy LH, Blackstone EH. Changes in left ventricular morphology and function after mitral valve surgery. Am J Cardiol. (2012) 110:403–8.e3. doi: 10.1016/j.amjcard.2012.03.041
23. Liu B, Neil DAH, Bhabra M, Patel R, Barker TA, Nikolaidis N, et al. Reverse myocardial remodeling following valve repair in patients with chronic severe primary degenerative mitral regurgitation. JACC Cardiovasc Imaging. (2022) 15:224–36. doi: 10.1016/j.jcmg.2021.07.007
24. Yingchoncharoen T, Agarwal S, Popoviæ ZB, Marwick TH. Normal ranges of left ventricular strain: a meta-analysis. J Am Soc Echocardiogr. (2013) 26:185–91. doi: 10.1016/j.echo.2012.10.008
25. Lee SH, Lhagvasuren P, Seo J, Cho I, Kim DY, Hong GR, et al. Prognostic implications of left ventricular global longitudinal strain in patients with surgically treated mitral valve disease and preserved ejection fraction. Front Cardiovasc Med. (2021) 8:775533. doi: 10.3389/fcvm.2021.775533
26. Kim HM, Cho GY, Hwang IC, Choi HM, Park JB, Yoon YE, et al. Myocardial strain in prediction of outcomes after surgery for severe mitral regurgitation. JACC Cardiovasc Imaging. (2018) 11:1235–44. doi: 10.1016/j.jcmg.2018.03.016
27. Witkowski TG, Thomas JD, Debonnaire PJ, Delgado V, Hoke U, Ewe SH, et al. Global longitudinal strain predicts left ventricular dysfunction after mitral valve repair. Eur Heart J Cardiovasc Imaging. (2013) 14:69–76. doi: 10.1093/ehjci/jes155
28. Mandoli GE, Pastore MC, Benfari G, Bisleri G, Maccherini M, Lisi G, et al. Left atrial strain as a pre-operative prognostic marker for patients with severe mitral regurgitation. Int J Cardiol. (2021) 324:139–45. doi: 10.1016/j.ijcard.2020.09.009
29. Rosenhek R, Rader F, Klaar U, Gabriel H, Krejc M, Kalbeck D, et al. Outcome of watchful waiting in asymptomatic severe mitral regurgitation. Circulation. (2006) 113:2238–44. doi: 10.1161/CIRCULATIONAHA.105.599175
30. Gucuk Ipek E, Singh S, Viloria E, Feldman T, Grayburn P, Foster E, et al. Impact of the mitraclip procedure on left atrial strain and strain rate. Circ Cardiovasc Imaging. (2018) 11:e006553. doi: 10.1161/CIRCIMAGING.117.006553
31. Ikenaga H, Makar M, Rader F, Siegel RJ, Kar S, Makkar RR, et al. Mechanisms of mitral regurgitation after percutaneous mitral valve repair with the MitraClip. Eur Heart J Cardiovasc Imaging. (2020) 21:1131–43. doi: 10.1093/ehjci/jez247
32. Sugiura A, Weber MW, Tabata NT, Oeztuerk CO, Zimmer SZ, Becher UB, et al. Risk factors and etiology of recurrent mitral regurgitation after edge-to-edge mitral valve repair. European Heart Journal. (2020) 41:e010895. doi: 10.1093/ehjci/ehaa946.1970
33. Scandura S, Ussia GP, Capranzano P, Caggegi A, Sarkar K, Cammalleri V, et al. Left cardiac chambers reverse remodeling after percutaneous mitral valve repair with the MitraClip system. J Am Soc Echocardiogr. (2012) 25:1099–105. doi: 10.1016/j.echo.2012.07.015
Keywords: mitral valve repair (MV repair), mitral regurgitation (MR), left atrial strain (LA strain), speckle tracking echocardiography, outcome
Citation: Kim S-E, Kim D-Y, Seo J, Cho I, Hong G-R, Ha J-W and Shim CY (2022) Left atrial strain and clinical outcome in patients with significant mitral regurgitation after surgical mitral valve repair. Front. Cardiovasc. Med. 9:985122. doi: 10.3389/fcvm.2022.985122
Received: 03 July 2022; Accepted: 14 September 2022;
Published: 04 October 2022.
Edited by:
Sanjeev Bhattacharyya, Barts Heart Centre, United KingdomReviewed by:
Yasufumi Nagata, Massachusetts General Hospital and Harvard Medical School, United StatesCopyright © 2022 Kim, Kim, Seo, Cho, Hong, Ha and Shim. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Chi Young Shim, Y3lzcHJzQHl1aHMuYWM=
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.