
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Cardiovasc. Med. , 29 November 2022
Sec. Coronary Artery Disease
Volume 9 - 2022 | https://doi.org/10.3389/fcvm.2022.984952
 Ben Cohen1,2*
Ben Cohen1,2* Tamir Bental1,2Liat Perl2,3
Tamir Bental1,2Liat Perl2,3 Hana Vaknin Assa1,2
Hana Vaknin Assa1,2 Pablo Codner1,2
Pablo Codner1,2 Katia Orvin1,2
Katia Orvin1,2 Yeela Talmor Barkan1,2
Yeela Talmor Barkan1,2 Amos Levi1,2
Amos Levi1,2 Ran Kornowski1,2
Ran Kornowski1,2 Leor Perl1,2
Leor Perl1,2Background: The link between thyroid dysfunction and cardiovascular disease is well established. Hypothyroidism has been significantly associated with increased risk of dyslipidemia, atherosclerosis and heart failure. However, little is known regarding its effect on patients undergoing percutaneous coronary intervention (PCI).
Aim: The aim of study was to examine the impact of concomitant hypothyroidism on mortality and major adverse cardiac event (MACE) in patients undergoing PCI.
Methods: The Rabin Medical Center PCI registry includes all consecutive patients who have undergone PCI between 2004 and 2020. We identified patients with prior diagnosis of hypothyroidism, and compared rates of mortality and MACE (comprising death, myocardial infarction, target vessel revascularization and/or coronary bypass surgery).
Results: Among 28,274 patients, 1,922 (6.8%) were found to have hypothryoidism. These patients were older (70.3 ± 10.4 vs. 66.0 ± 11.8 y.o, P < 0.001) and more likely to be women (34.2% vs. 26.1%, P < 0.001). They had a higher prevalence of atrial fibrillation (10.8% vs. 7.7%, P < 0.001), chronic renal dysfunction (25.1% vs. 18.7%, P = 0.04) and dementia (2.9% vs. 1.8%, P = 0.004). PCI was performed on ACS setting in 52–54% of patients in both groups (p = 0.569). Unadjusted 5-year rates of all-cause mortality (26.9% vs. 20.3%, P < 0.001) and MACE (40.3% vs. 29.4%, P < 0.001) were higher for hypothyroid patients. A propensity match score was able to form 672 matched pairs of HT and control patients, showing similar results. Moreover, following multivariate analysis, TSH as a continuous parameter was associated with a higher risk of mortality and MACE (HR, 1.06 per additional 1 mIU/L; CI, 1.02–1.11; P < 0.001 and HR, 1.07; CI, 1.02–1.12; P < 0.001, respectively) at 5-year follow up.
Conclusion: In our study, hypothyroidism confers worse outcomes in patients undergoing PCI. Further research is needed to establish effective ways to mitigate this augmented risk.
Thyroid hormones are known to affect the cardiovascular system. Both hypo- and hyperthyroidism have been linked to cardiovascular disease (1, 2). Hypothyroidism (HT) has been suggested as a causative factor in dyslipidemia and metabolic syndrome (3). Hyperthyroidism, on the other hand has been associated with high-output heart failure, dilated cardiomyopathy and atrial fibrillation (4). That is why determination of the thyroid hormonal status is indicated in many cardiovascular diseases, as reflected in the European Society of Cardiology 2021 heart failure and the European Society of Cardiology 2020 atrial fibrillation guidelines (5, 6).
The prevalence of HT is between 4 and 10% of the population (7). HT is associated with cardiovascular changes of arterial compliance, diastolic blood pressure, endothelial dysfunction and hyperlipidemia (8). Hence, it is not surprising that HT and to a lesser degree subclinical hypothyroidism (SHT) are associated with an accelerated atherosclerosis and a higher prevalence of ischemic heart disease (9, 10). The association of HT with atherosclerosis seems to be mediated with intima-media thickness and the above mentioned pathophysiological entities. However, the exact mechanisms in which it may hasten atherosclerosis are not fully understood (11).
Whether thyroid hormone status matters in patients with established ischemic heart disease, in terms of mortality, re-infarction, restenosis and in stent thrombosis has long been a subject of debate. Previous studies imply HT, and to a lesser extent- SHT, are associated with a higher incidence of major adverse cardiovascular or cerebrovascular events (MACCE) compared with euthyroid patients undergoing percutaneous coronary intervention (PCI) (12–15). However, as previous studies were based on small groups of patients, and usually defined thyroid hormonal status based on a single measurement done in the setting of acute coronary syndrome, we thought that further research is needed.
Understanding the additional relative risk posed in patients with HT, and whether it is preventable with thyroid replacement therapy, may impact a substantial percentage of patients undergoing PCI. The following study attempts to shed light on the correlation between HT and prognosis in patients with concomitant ischemic heart disease undergoing PCI (Figure 1).
Figure 1. Central illustration.
The current study is an observational study based on the prospective Rabin Medical Center PCI registry. This database includes all consecutive patients who have undergone PCI at the Rabin Medical Center, Israel, between 2004 and 2020 PCI at two hospitals: the Beilinson and HaSharon medical centers. We identified patients with prior diagnosis of HT and compared their baseline and procedural characteristics and long terms prognosis to euthyroid patients. Data before and after hospitalization were obtained from the hospital’s and the Clalit healthcare services’ (largest healthcare provider in Israel) databases. Mortality data were obtained from the national Ministry of Interior database.
The obtained data included demographic and clinical characteristics, cardiovascular risk factors, co-morbidities (based on ICD-9 diagnoses codes), procedural characteristics, and clinical workup (e.g., blood tests, echocardiography) as was previously reported (16). Most patients who underwent PCI, regardless of etiology, were hospitalized for at least 1 day thereafter. In addition to detailed information on the medical conditions and medications of all patients, we extracted thyroid stimulating hormone (TSH) values 6 months before PCI and considered values above 10.0 mIU/L as an indication of undiagnosed HT and values above 5 mIU/L in the presence of HT as a suboptimal treatment. Patients with hyperthyroidism or SHT were excluded from the study, as well as those with missing data regarding TSH levels, baseline characteristics or outcomes. Included in the final study group were all patients with an established diagnosis of HT or permanent thyroid replacement therapy according to their electronic medical records. They were compared to patients with no known diagnosis of HT and TSH levels within the normal range. Patients were not screened for development of thyroidal illness post PCI unless diagnosis was made as part of the hospital admission in which the PCI was performed.
The hospital’s ethics committee approved the study, which was performed in accordance with the Helsinki declaration.
All patients provided an explicit written informed consent before undergoing cardiac catheterization and PCI as indicated. Administration of anticoagulants before and after PCI was in accordance with the clinical setting (acute versus chronic coronary syndrome) and the latest guidelines which have been updated throughout the years of this study.
All patients were treated with aspirin 200–300 mg before PCI, clopidogrel 300–600 mg, prasugrel 60 mg or ticagrelor 180 mg (in acute coronary syndromes) either before PCI (pretreatment, in cases of acute coronary syndromes) or immediately after completion of the procedure (in elective cases). Glycoprotein IIb/IIIa inhibitors were used during the procedure and immediately following the PCI, at the discretion of the operator. The choice of the type of coronary stent and other adjunct therapy were left to the discretion of the primary operator and shifted exclusively toward drug eluting stents and trans-radial access in recent years. All stents were implanted with moderate-to-high deployment pressure (∼12 atm) with or without post dilatation as needed. All patients received recommendation to continue dual antiplatelet therapy with aspirin 100 mg daily and a P2Y12 inhibitor (clopidogrel, prasugrel, or ticagrelor) for at least 12 months after the PCI.
Immediate and in-hospital clinical events were prospectively documented in the Rabin Medical Center PCI registry. Information on patient outcomes (mortality and other clinical outcomes) was drawn from the databases listed above on December 2021.
Outcomes included all-cause mortality and major adverse cardiac event (MACE), which comprised death, myocardial infarction (MI) excluding peri-procedural MI, need for target vessel revascularization, and/or coronary artery bypass surgery (CABG) at 1 and 5 years.
Continuous data are presented as median and interquartile range, and categorical data, as frequency (%). Student t-test or analysis of variance was used to compare continuous variables between groups, and Chi-square was used for categorical variables. The normality of variable distributions was assessed using the Kolmogorov–Smirnov test. Survival curves were constructed using the Kaplan–Meier method and compared using log-rank test. Cox regression analysis was performed to determine independent predictors of the primary end points, assessing the contribution of increased TSH as a continuous parameter and known baseline cardiovascular risk factors. Finally, due to several differences in baseline characteristics, we compiled a cohort of propensity score matched patients with a 1:1 ratio between patients with HT and controls. The propensity score was derived from a multivariate logistic regression model that included the presence of hypothyroidism, considered as the independent (outcome) variable, and all baseline clinical characteristics and procedural characteristics as covariates. The propensity score matched cohort was analyzed for the main combined outcome. All statistical analyses were performed with IBM SPSS version 28.0 (IBM Corp. Armonk, NY, United States). A P-value of < 0.05 was considered statistically significant.
We have analyzed information based on 28,274 patients who have undergone PCI between the years 2004 to 2020. After exclusion of 2,679 patients due to missing data regarding thyroid function, evidence of hyperthyroidism or SHT, 25,595 patients were eligible for our final analysis. 1,922 of these patients, 6.8% of the total PCI cohort, were diagnosed as HT based on the above criteria (Figure 2).
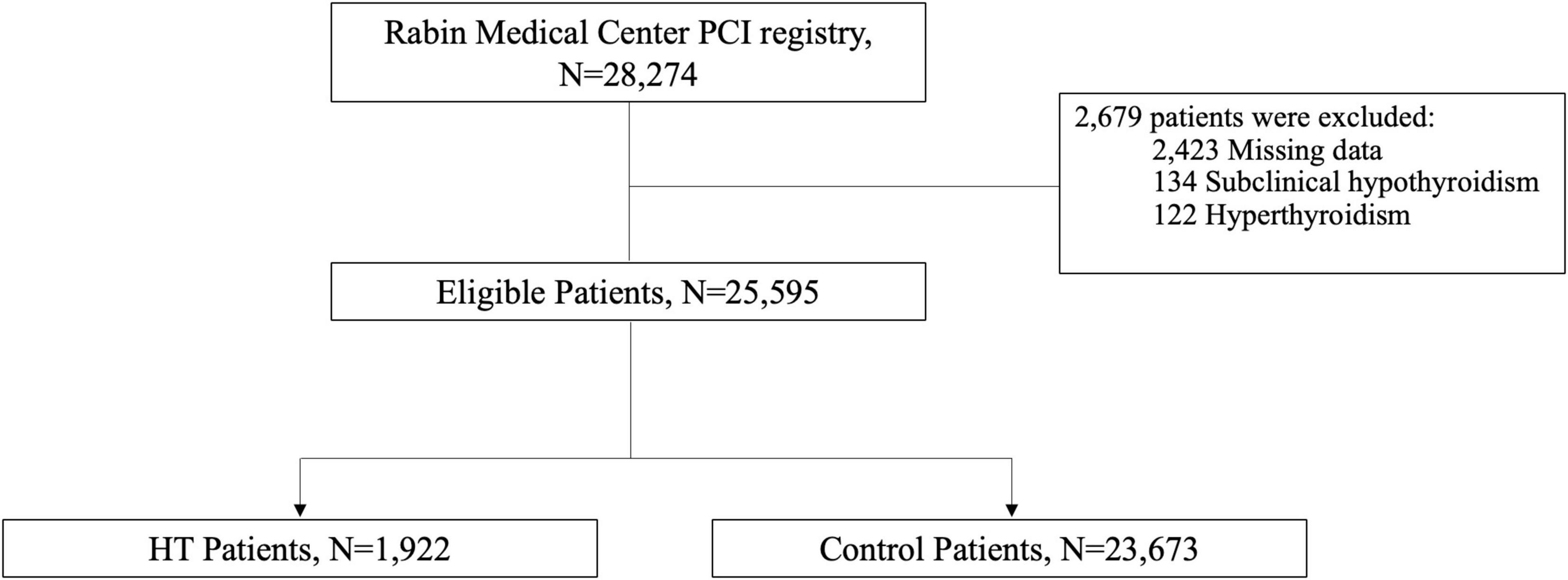
Figure 2. Description of the study cohort.
Patients with HT were ∼4 years older (70.4 ± 10.4 vs. 66.0 ± 11.8 y.o, P < 0.001), were more likely to be women (34.2% vs. 26.1%, P < 0.001). They had a higher prevalence of atrial fibrillation (10.8% vs. 7.7%, P < 0.001), chronic kidney disease (251% vs. 18.7%, P = 0.04), anemia (54.1% vs. 50.8%, P = 0.052), and demetia (2.9% vs. 1.8%, P = 0.004). Moreover, HT patients had slightly worse lipid profile (baseline low-density lipoprotein 98.2 ± 37.0 vs. 94.8 ± 38.3 mg/dl, P < 0.001), and as expected had higher baseline TSH value (mean 4.6 vs. 1.8 mIU/L, P < 0.001) (Tables 1, 2).
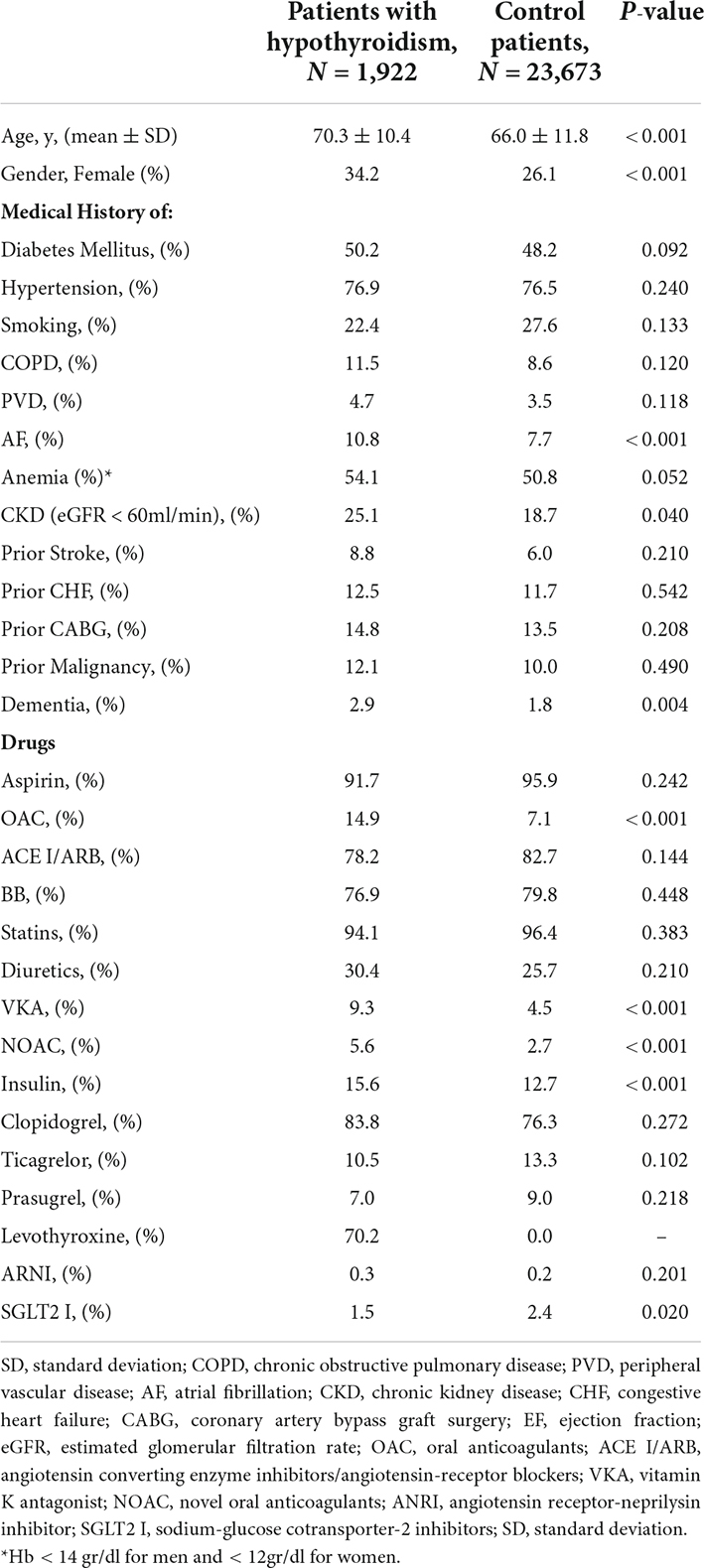
Table 1. Baseline patients characteristics.
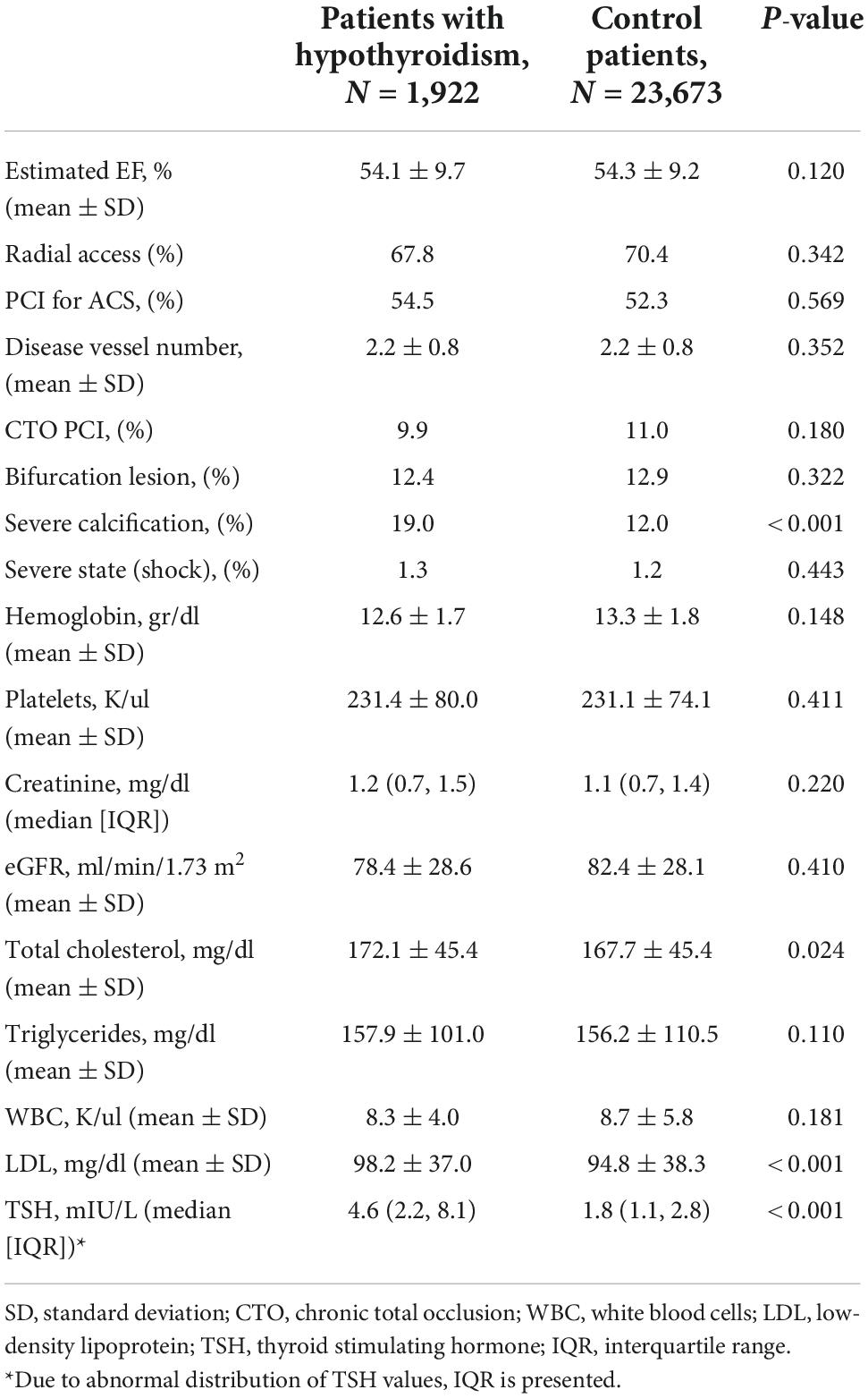
Table 2. Main clinical parameters at presentation.
Regarding patient presentation, both groups presented with preserved mean left ventricular ejection fraction (∼54%), while the minority of patients, about 1%, presented with hemodynamic instability. PCI in an urgent ACS setting was not significantly different between the groups and included 52–54% of cases (P = 0.569). In terms of baseline medications, HT patients were more frequently treated with vitamin K antagonist (9.3% vs. 4.5%, P < 0.001), novel oral anticoagulants (5.6% vs. 2.7%, P < 0.001), and insulin (15.6% vs. 12.7%, P < 0.001). A trend toward less frequent use of potent P2Y12 inhibitors was noticed in this group. Additionally, coronary angiography differed between groups in that severe calcification was more frequent in HT patients (19.0% vs. 12.0%, P < 0.001) (Table 2).
The presence of HT was associated with a significant higher risk of mortality and MACE over 5-year follow-up (Figures 3, 4, respectively). At 1-year, mortality and MACE were 8.4% vs. 5.8% and 18.8% vs. 12.7%, respectively (P < 0.001). At 5-year, mortality and MACE were 26.9% vs. 20.3% and 40.3% vs. 29.4%, respectively (P < 0.001). Following multivariate analysis, using Cox proportional hazards regression and increased TSH as a continuous parameter, the presence of increased TSH was still associated with significant higher rates of mortality (HR, 1.06; CI, 1.02–1.11; P < 0.001) and MACE (HR, 1.07; CI, 1.02–1.12; P < 0.001), (Table 3 and Figure 5). A propensity match score was able to form 672 matched pairs of HT and control patients, showing similar results; Following Cox regression, patients presenting with HT demonstrated higher rates 5-year mortality and MACE than patients without HT (HR 1.19; CI: 1.06–1.74 and HR 1.18; CI: 1.09–1.48, respectively; p < 0.001).
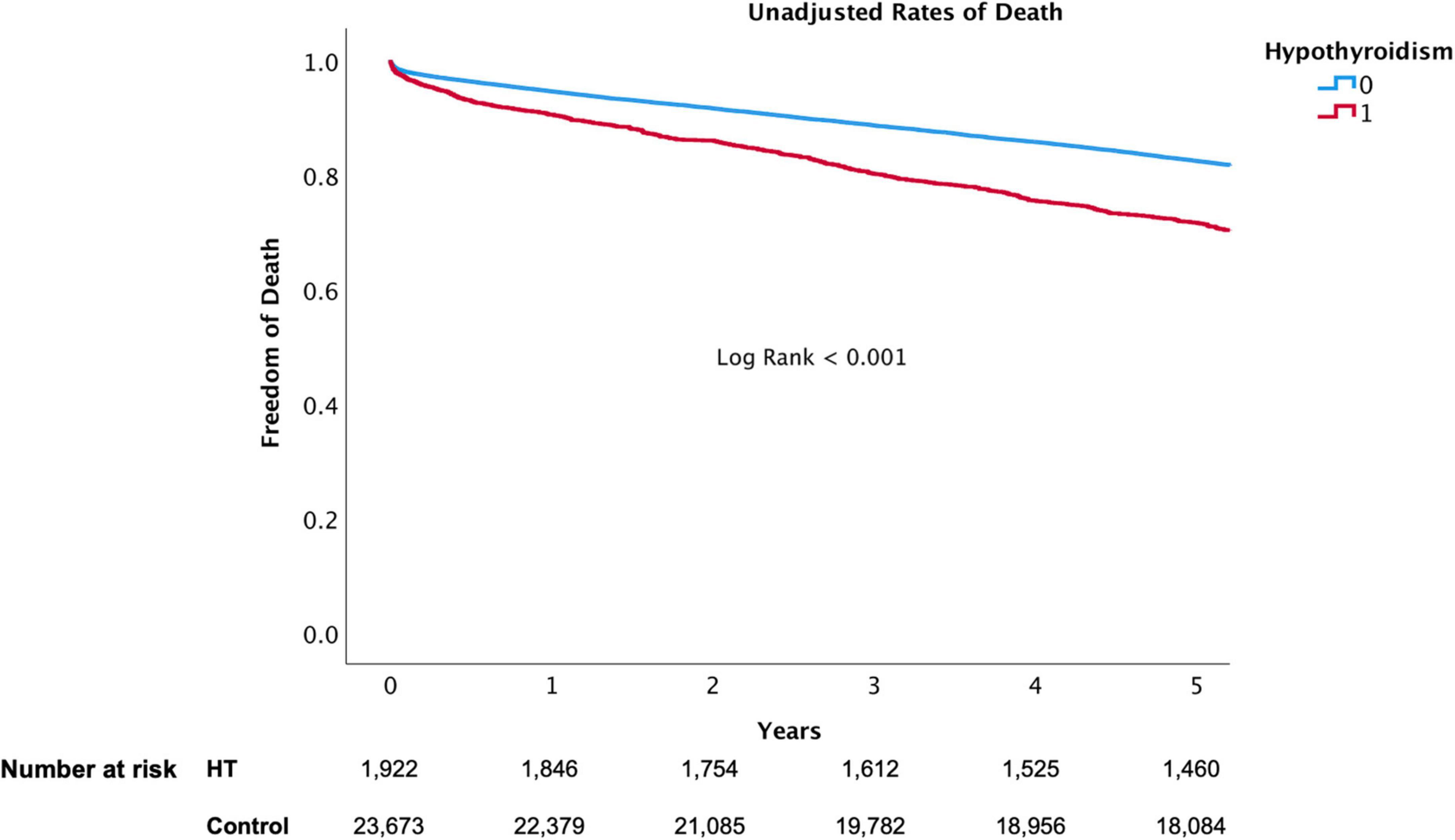
Figure 3. 5-Year all-cause mortality of hypothyroidism versus euthyroid patients.
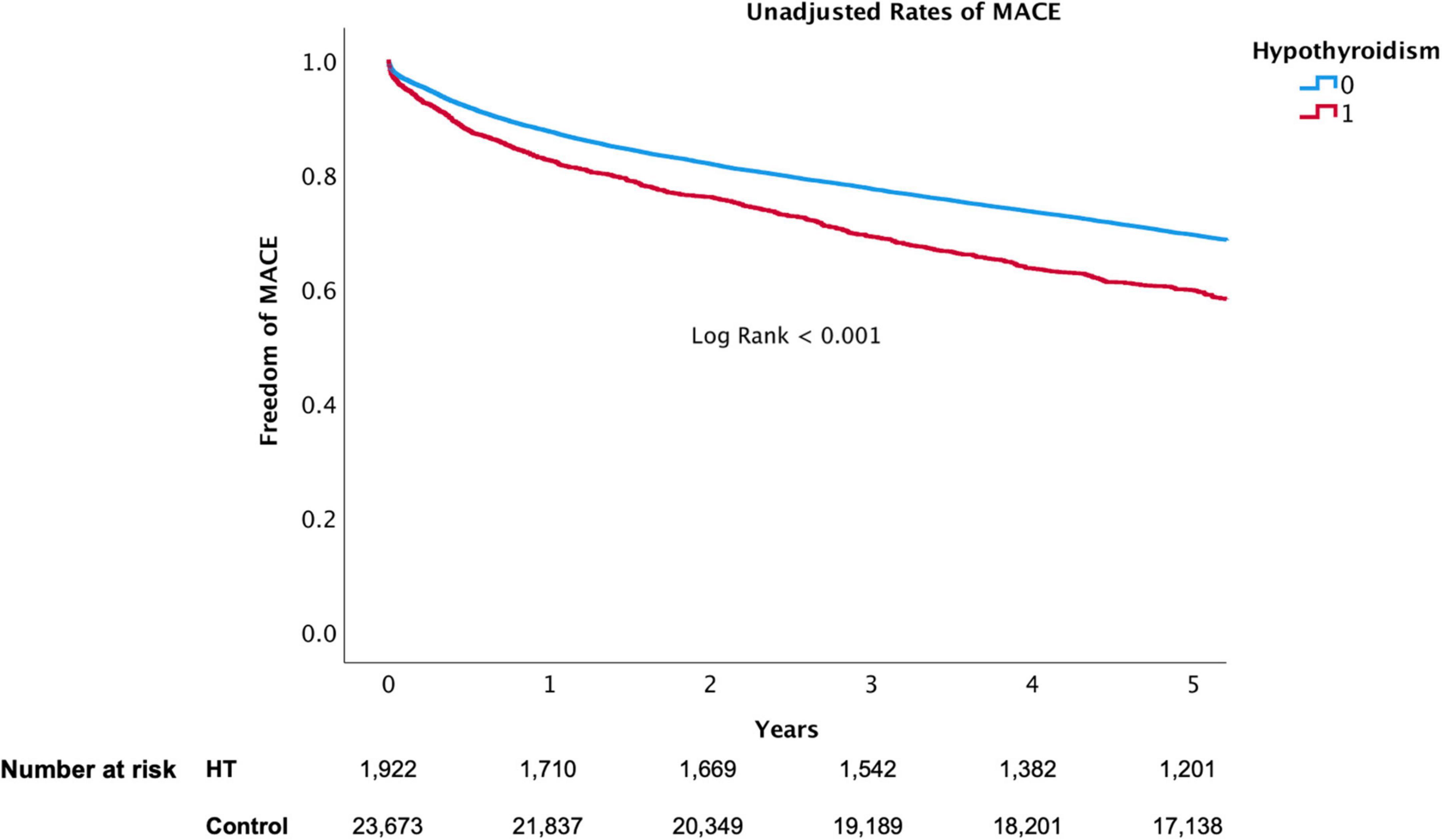
Figure 4. 5-Year MACE of hypothyroidism versus euthyroid patients.
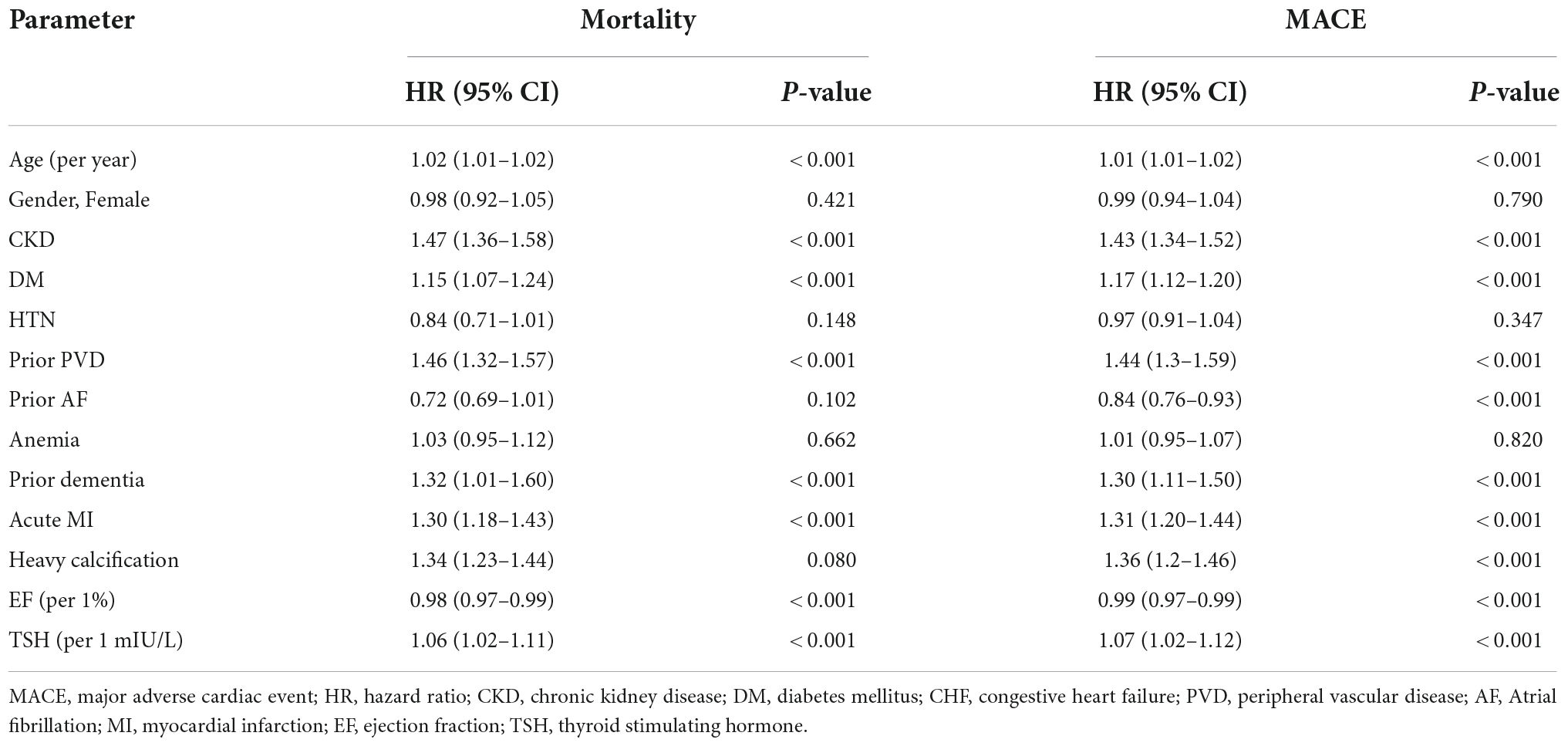
Table 3. Cox regression analyses for mortality and MACE at 5 years.
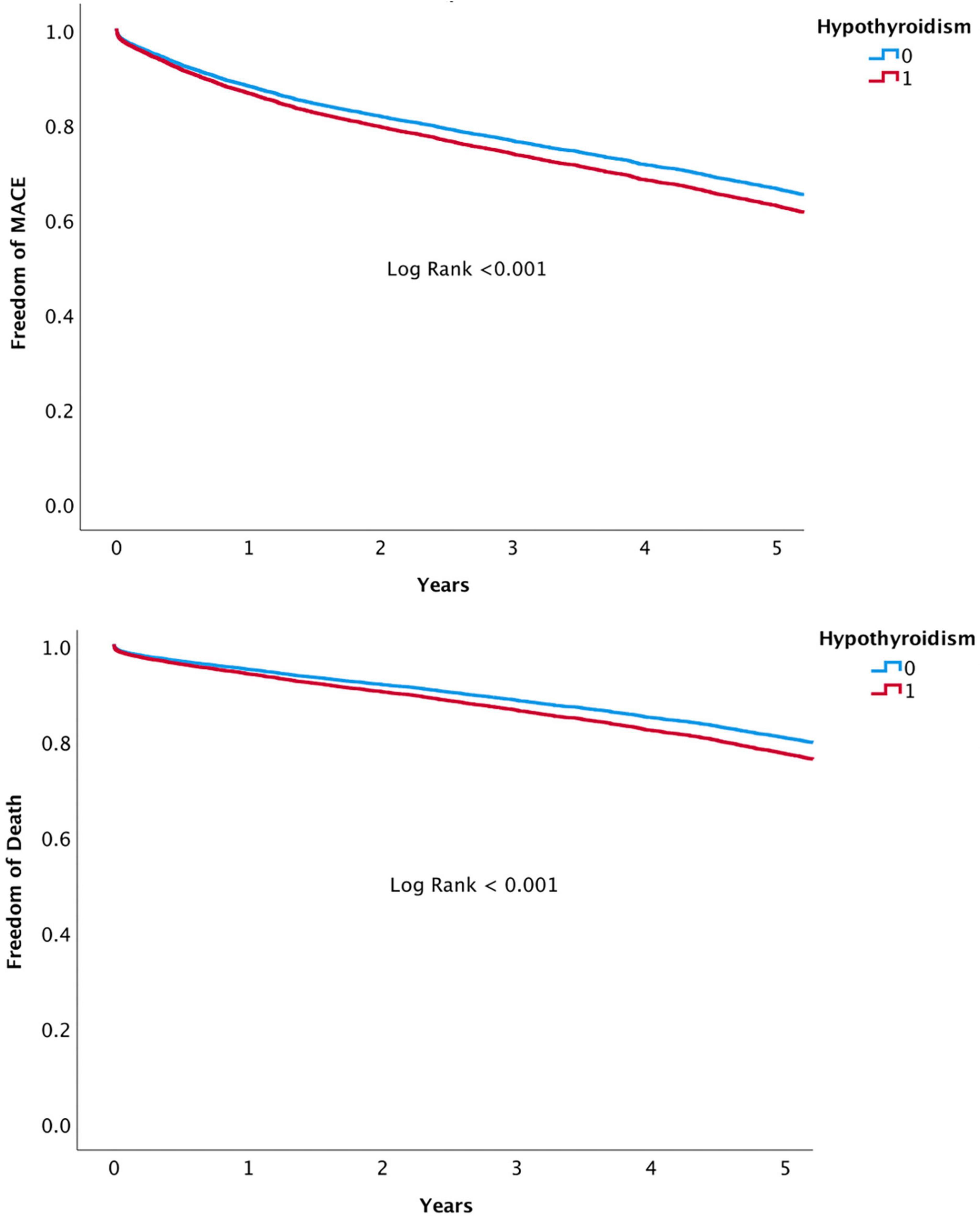
Figure 5. Adjusted rates of all-cause mortality and MACE at 5 years.
Our study assessed the impact of HT on the outcomes of patients undergoing PCI and found an increased risk of both death and MACE following PCI among HT patients compared to counterpart patients. To the best of our knowledge, it is the largest outcome analysis of HT patients following PCI. This confirms prior smaller retrospective studies, which demonstrated a significant association of HT with all-cause mortality (10, 17–19).
The previous retrospective study by Zhang et al., based on the Mayo Clinic PCI registry, examined a similar research question (12). This study showed that HT was associated with a higher incidence of MACCE (MACE plus cerebral events) compared with euthyroid patients undergoing PCI. Moreover, it showed that adequate hormone replacement therapy with TSH corrected to the normal range was associated with a lower incidence of MACCE compared to untreated or inadequately treated patients (12). Related to our study, although the initial cohort of this study was quite similar and stands at about 25,000 patients, due to missing data, and strict exclusion criteria, only 686 patients (<3%) were included in the hypothyroid group of this previous study. It implies a possible underestimation of this patients population and a potential for selection bias in this study. In addition, the median duration of follow-up in this study was shorter (3 vs. 5 years in our study). Furthermore, the long (e.g., 7-year) time interval passed since this study allow us to evaluate the changes in PCI performance (such as advanced-generation stents and potent P2Y12 inhibitors) in the context of patients with HT.
As for the etiology of the increased mortality and MACE incidence in HT patients, our study confirms previous observations that patients with HT have a significantly higher prevalence of comorbidities associated with a high cardiovascular risk profile, such as prior myocardial infarction, diabetes mellitus, hypertension, COPD, and chronic renal disease. However, using propensity score matching, we were also able to demonstrate an independent effect of HT on adverse clinical outcomes. This observation supports previous studies that demonstrated many pathophysiological effects of thyroid hormones on the cardiovascular systems, and make it plausible that HT itself is not only a risk marker but rather a risk target that should be treated to decrease mortality and cardiovascular morbidities (7, 20). Previously demonstrated effects that linked HT and the cardiovascular system include changes of arterial compliance, diastolic blood pressure, endothelial dysfunction, hyperlipidemia and intima-media thickening, which is a known surrogate marker for atherosclerosis (8, 11). While not completely understood, it is apparent that HT affects many physiological processes including systemic diseases with known detrimental prognostic cardiovascular aspects, and some effect the cardiovascular system directly.
Subclinical hypothyroidism correlates with worse cardiovascular outcome to a lesser extent than HT. To date, there is no recommendation to prescribe thyroid hormone replacement therapy to SHT patients (21, 22). Due to seemingly SHT underdiagnosis in our study, we chose to exclude SHT. We, however, performed Cox proportional hazards regression with increased TSH as a continuous parameter, including mildly elvated TSH values due to suboptimal treatment in HT patients. The significant higher rates of mortality with increased TSH support previous observation regarding worse cardiovascular outcome in HT patients with suggested worst prognosis in untreated patients. A recently published large retrospective cohort study examined 705,307 adults who received thyroid hormone treatment from the US Veterans Health Administration Corporate Data Warehouse and demonstrated a highed cardiovascular mortality among patients with TSH and free thyroxine levels that were not controlled within the normal range, whether it resulted in HT or exogenous hyperthyroidism (23). Our study demonstrates for the first time that a cohort of patients with HT suffer higher mortality and MACE rates following PCI. Our Propensity score matching analysis strengthen this observation as HT was independently associated with significant higher rates of mortality. Moreover, TSH as a continuous parameter in a Cox proportional hazards regression was still associated with significant higher rates of mortality. Whether it implies a possible beneficial effect of TSH targeted therapy on mortality remains to be explored. Further studies, preferably randomized prospective studies, are needed to examine the clinical benefit of thyroid hormone replacement therapy targeted to a middle-normal TSH level in patients undergoing PCI.
Our study has several limitations. First, it is based on an all-comer PCI registry from two medical centers, and thus is liable to the limitations of observational study design. Second, the definition of HT was based on medical records and TSH values that were not available for all patients. We also lacked free T4 levels, data regarding TPO/Tg antibodies and the etiology of HT. Finally, many patients (∼8.5% of the cohort) were excluded from the final analysis due to missing data. Nevertheless, to date, this is the largest contemporary study examining the independent impact of HT on outcomes of patients undergoing PCI, showing significantly worse outcomes.
In conclusion, our findings strengthen previous retrospective studies demonstrating the association between HT and worse outcomes in coronary artery disease undergoing PCI. As mortality and MACE were significantly higher for patients with HT, it may suggest TSH targeted therapy in this patients population. As our study design was not targeted to answer this question, future interventional studies are warranted to establish methods to mitigate this risk.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
The studies involving human participants were reviewed and approved by Rabin Medical Center Ethics Committee. Written informed consent for participation was not required for this study in accordance with the national legislation and the institutional requirements.
BC and LiP: study concept and design, methodology, interpretation of data, and drafting of the manuscript. TB: database queries formation. LeP: statistical analysis. LiP, TB, HV, PC, KO, YT, AL, and RK: establishing and maintaining the PCI database. All authors contributed to the data and final manuscript were critically discussed, revised, and approved.
This research project was investigator-initiated and locally funded by a research grant from our medical center.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
2. Klein I, Danzi S. Thyroid disease and the heart. Curr Probl Cardiol. (2016) 41:65–92. doi: 10.1016/j.cpcardiol.2015.04.002
3. Mehran L, Amouzegar A, Rahimabad PK, Tohidi M, Tahmasebinejad Z, Azizi F. Thyroid function and metabolic syndrome: a population-based thyroid study. Horm Metab Res. (2017) 49:192–200. doi: 10.1055/s-0042-117279
4. Osuna PM, Udovcic M, Sharma MD. Hyperthyroidism and the heart. Methodist Debakey Cardiovasc J. (2017) 13:60–3.
5. McDonagh TA, Metra M, Adamo M, Gardner RS, Baumbach A, Böhm M, et al. 2021 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure developed by the Task Force for the diagnosis and treatment of acute and chronic heart failure of the European society of cardiology (ESC) With the special contribution of the heart failure association (HFA) of the ESC. Eur Heart J. (2021) 42:3599–726.
6. Hindricks G, Potpara T, Dagres N, Arbelo E, Bax JJ, Blomström-Lundqvist C, et al. 2020 ESC Guidelines for the diagnosis and management of atrial fibrillation developed in collaboration with the European association for cardio-thoracic surgery (EACTS)the Task Force for the diagnosis and management of atrial fibrillation of the European society of cardiology (ESC) developed with the special contribution of the European heart rhythm association (EHRA) of the ESC. Eur Heart J. (2021) 42:373–498. doi: 10.1093/eurheartj/ehab648
7. Udovcic M, Pena RH, Patham B, Tabatabai L, Kansara A. Hypothyroidism and the heart. Methodist Debakey Cardiovasc J. (2017) 13:55–9.
8. Cooper DS, Biondi B. Subclinical thyroid disease. Lancet. (2012) 379:1142–54. doi: 10.1016/S0140-6736(11)60276-6
9. Tseng FY, Lin WY, Lin CC, Lee LT, Li TC, Sung PK, et al. Subclinical hypothyroidism is associated with increased risk for all-cause and cardiovascular mortality in adults. J Am Coll Cardiol. (2012) 60:730–7.
10. Rodondi N, den Elzen WPJ, Bauer DC, Cappola AR, Razvi S, Walsh JP, et al. Subclinical hypothyroidism and the risk of coronary heart disease and mortality. JAMA. (2010) 304:1365–74. doi: 10.1001/jama.2010.1361
11. Papadopoulou AM, Bakogiannis N, Skrapari I, Moris D, Bakoyiannis C. Thyroid dysfunction and atherosclerosis: a systematic review. In Vivo. (2020) 34:3127–36. doi: 10.21873/invivo.12147
12. Zhang M, Sara JDS, Matsuzawa Y, Gharib H, Bell MR, Gulati R, et al. Clinical outcomes of patients with hypothyroidism undergoing percutaneous coronary intervention. Eur Heart J. (2016) 37:2055–65. doi: 10.1093/eurheartj/ehv737
13. Seo SM, Koh Y, Park H, Kim DB, Her SH, Lee JM, et al. Thyroid stimulating hormone elevation as a predictor of long-term mortality in patients with acute myocardial infarction. Clin Cardiol. (2018) 41:1367–73. doi: 10.1002/clc.23062
14. Lee Y, Lim YH, Shin JH, Park J, Shin J. Impact of subclinical hypothyroidism on clinical outcomes following percutaneous coronary intervention. Int J Cardiol. (2018) 253:155–60. doi: 10.1016/j.ijcard.2017.09.192
15. Wang W, Wang S, Zhang K, Chen J, Zhang X, Shao C, et al. Hypothyroidism is associated with clinical outcomes in patients with acute myocardial infarction: subgroup analysis of China PEACE study. Endocrine. (2021) 74:128–37. doi: 10.1007/s12020-021-02742-w
16. Bental T, Assali A, Vaknin-Assa H, Lev EI, Brosh D, Fuchs S, et al. A comparative analysis of major clinical outcomes using drug-eluting stents versus bare-metal stents in a large consecutive patient cohort. Catheter Cardiovasc Interv. (2010) 76:374–80. doi: 10.1002/ccd.22507
17. Inoue K, Ritz B, Brent GA, Ebrahimi R, Rhee CM, Leung AM. Association of subclinical hypothyroidism and cardiovascular disease with mortality. JAMA Netw Open. (2020) 3:e1920745. doi: 10.1001/jamanetworkopen.2019.20745
18. Journy NMY, Bernier MO, Doody MM, Alexander BH, Linet MS, Kitahara CM. Hyperthyroidism, hypothyroidism, and cause-specific mortality in a large cohort of women. Thyroid. (2017) 27:1001–10. doi: 10.1089/thy.2017.0063
19. Tsai TY, Tu YK, Munir KM, Lin SM, Chang RHE, Kao SL, et al. Association of hypothyroidism and mortality in the elderly population: a systematic review and meta-analysis. J Clin Endocrinol Metab. (2020) 105:dgz186. doi: 10.1210/clinem/dgz186
20. Vale C, Neves JS, von Hafe M, Borges-Canha M, Leite-Moreira A. The role of thyroid hormones in heart failure. Cardiovasc Drugs Ther. (2019) 33:179–88. doi: 10.1007/s10557-019-06870-4
21. Bekkering GE, Agoritsas T, Lytvyn L, Heen AF, Feller M, Moutzouri E, et al. Thyroid hormones treatment for subclinical hypothyroidism: a clinical practice guideline. BMJ. (2019) 365:l2006. doi: 10.1136/bmj.l2006
22. Gencer B, Moutzouri E, Blum MR, Feller M, Collet TH, Delgiovane C, et al. The impact of levothyroxine on cardiac function in older adults with mild subclinical hypothyroidism: a randomized clinical trial. Am J Med. (2020) 133:848–56.e5.
Keywords: hypothyroid, percutaneous coronary intervention (PCI), major cardiovascular adverse event, outcomes, ischemic heart disease
Citation: Cohen B, Bental T, Perl L, Vaknin Assa H, Codner P, Orvin K, Barkan YT, Levi A, Kornowski R and Perl L (2022) Hypothyroidism predicts worsened prognosis in patients undergoing percutaneous coronary intervention. Front. Cardiovasc. Med. 9:984952. doi: 10.3389/fcvm.2022.984952
Received: 02 July 2022; Accepted: 14 November 2022;
Published: 29 November 2022.
Edited by:
Branko Dusan Beleslin, Clinical Center of Serbia, SerbiaReviewed by:
Hamayak Sisakian, Yerevan State Medical University, ArmeniaCopyright © 2022 Cohen, Bental, Perl, Vaknin Assa, Codner, Orvin, Barkan, Levi, Kornowski and Perl. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Ben Cohen, aTkxNmJjQGdtYWlsLmNvbQ==; YmVuY29oQGNsYWxpdC5vcmcuaWw=
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.