
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
CASE REPORT article
Front. Cardiovasc. Med. , 15 December 2022
Sec. Heart Valve Disease
Volume 9 - 2022 | https://doi.org/10.3389/fcvm.2022.978874
 Neguemadji Ngardig Ngaba1*
Neguemadji Ngardig Ngaba1* Uzoego Nwakaku Chibuzo2
Uzoego Nwakaku Chibuzo2 Meet Patel3
Meet Patel3 Amit Gulati4Olatunde Ola5Allarangué Djindimadje1Imteyaz A. Khan6
Amit Gulati4Olatunde Ola5Allarangué Djindimadje1Imteyaz A. Khan6Introduction: Mitral stenosis (MS) is a widely known complication of mitral valve repair for non-rheumatic mitral regurgitation (MR). Few reports are available on the occurrence of MS after mitral valve repair for rheumatic MR in young populations.
Case summary: A 14-year-old girl presented with orthopnea, abdominal distension, and bilateral lower-limb edema. She was cachectic, with a high-pitched holosystolic murmur best heard at the cardiac apex, bilateral basal crackles, tender hepatomegaly, pitting pedal edema, and jugular venous distension. Antistreptolysin O (ASO) titer was elevated. Transthoracic echocardiography (TTE) revealed the loss of central coaptation of the mitral valve with leaflet restriction and MR, annular dilatation of the tricuspid valve, and tricuspid regurgitation (TR). She had AHA/ACC stage D mitral and TR s. Tricuspid annuloplasty and mitral valve repair for rheumatic MR were performed using Carpentier Edwards numbers 30 and 34, respectively. Following surgery, the weight and body mass index (BMI) rapidly normalized. The patient also developed progressive MS.
Discussion: Previous studies in adults have described the etiopathogenesis of MS after non-rheumatic mitral valve repair. There is a paucity of reports describing the development of MS over the span of months after rheumatic MR valve repair in early pubescent children.
Conclusion: Growth spurts during puberty can potentially affect MR repair, as the mitral valve prosthesis based on the preoperative Body Surface Area (BSA) is outgrown. There is a need for research on planning, prognostication, and development of an optimal, individualized, and adaptable approach to MR intervention in early pubescence.
The first successful mitral valve repair was performed for rheumatic mitral stenosis (MS) by Dr. Elliot Cutler at Brigham and Women’s Hospital of Boston in 1923 (1).
It was Dr. C. Walton Lillehei from the University of Minnesota who did the first mitral valve repair for mitral regurgitation (MR) by annuloplasty in 1957 (2).
The implementation of mitral valve repair of MR beyond the degenerative etiology (3, 4) has spread because of the meaningful contributions of Carpentier (5), Duran et al. (6), and many cardiac surgeons (7, 8).
Recent studies (9–12) have shown a relative benefit of mitral valve repair for organic MR over mitral valve replacement. Despite the improvements and advances in the procedure, there are still some complications after mitral valve repair.
MS is a known complication after surgical mitral valve repair for MR (13).
Currently, functional MS is defined as a mean transmitral pressure gradient (TMPG) of > 5 mmHg or mitral valve area (MVA) of < 1.5 cm2 regardless of the cause (14, 15).
The development of MS after mitral valve repair has not been well investigated despite its high incidence ranging from 9 to 54% (15–17).
Several studies (18–20) have reported the development of MS after non-rheumatic MR valve repair in adult patients.
The literature has not yet described the cases of MS after mitral valve repair using the Carpentier Edwards ring for rheumatic MR in the younger population or the mechanism behind the occurrence of this complication.
Herein, we report the case of a 14-year-old girl who developed progressive severe MS after valve mitral repair using Carpentier Edwards ring 34 for severe rheumatic MR. We recapped the clinical and paraclinical aspects of the patient in preoperative status and postoperative (POD) follow-up for up to many years. Knowing that the peak height velocity of 8–10 cm per year (21, 22) occurs prior to the onset of menses, and according to the five Tanner stages (23) of puberty, this study chronologically correlated patient development with POD clinical findings. The study also reported the intraoperative mechanism of the affected cardiac valves and the repair surgical technique was performed accordingly.
A 14-year-old female patient presented with an 8-month history of new-onset murmur, progressively worsening palpitations, orthopnea, chest pain, and syncope. She was 158 cm tall, weighed 37 kg, and was cachectic with a BMI at the first centile for age and sex (14.8 kg/m2). Apart from tachycardia, vital signs were normal for age and sex (blood pressure 110/70 mm Hg; temperature 36.5°C; heart rate 110 beats/min). Tanner stage was 2 (downy pubic hair and palpable breast tissue without areola enlargement).
Physical examination findings were as follows: 4/6 MR murmur (24, 25) and regular tachycardia at 110/min; bilateral pulmonary crackles with dullness to percussion in the lower lobes; jugular venous distention and tender hepatomegaly with a liver span of 18 cm; and ascites and mild bilateral lower extremity edema classified as grade 2 + (26).
Antistreptolysin O (ASO) titers were elevated. Chest radiography and electrocardiography revealed a cardiothoracic ratio of 0.6 and left atrial enlargement with a cardiac axis of 30°.
Transthoracic echocardiography (TTE) revealed a mitral valve annulus diameter of 27 mm, severe MR due to leaflet restriction and loss of central coaptation, proximal isovelocity surface area (PISA) radius measuring 10 mmHg, and a mean gradient of 100 mmHg, an anatomically normal tricuspid valve with a hiatus measuring approximately 3 mm and an axial leak reaching the bottom of the right atrium (RA), and elevated pulmonary artery systolic pressure (PASP) at 55 mmHg. These clinical and TTE findings classified our patient as stage D for both mitral and TR (27).
The case was addressed to the cardiac surgery team of the Hôpital Européen George Pompidou in France through the non-governmental organization named chaîne de l’Espoir.
The patient received captopril, digoxin, furosemide, aspirin, spironolactone, and benzathine penicillin while awaiting surgery.
She underwent open cardiac surgery on 2 April 2010 at the Hôpital Européen George Pompidou, Paris, France.
Intraoperative findings during cardiac surgery were as follows: posterior mitral leaflet retraction and dilatation of the tricuspid annulus; mitral leaflets were enlarged using an autologous pericardial patch for the posterior and an oval pericardial patch for the anterior leaflets; mitral and tricuspid annuli were remodeled using Carpentier-Edwards Physio annuloplasty ring numbers 34 and 30, respectively.
There were no perioperative complications, and the immediate POD period was uneventful.
Clinical and paraclinical assessments were performed, which revealed tachycardia and decreased bilateral lower lung vesicular murmur. Chest radiography confirmed mild bilateral pleural effusion. Type 1 atrioventricular block was observed (Figure 1).
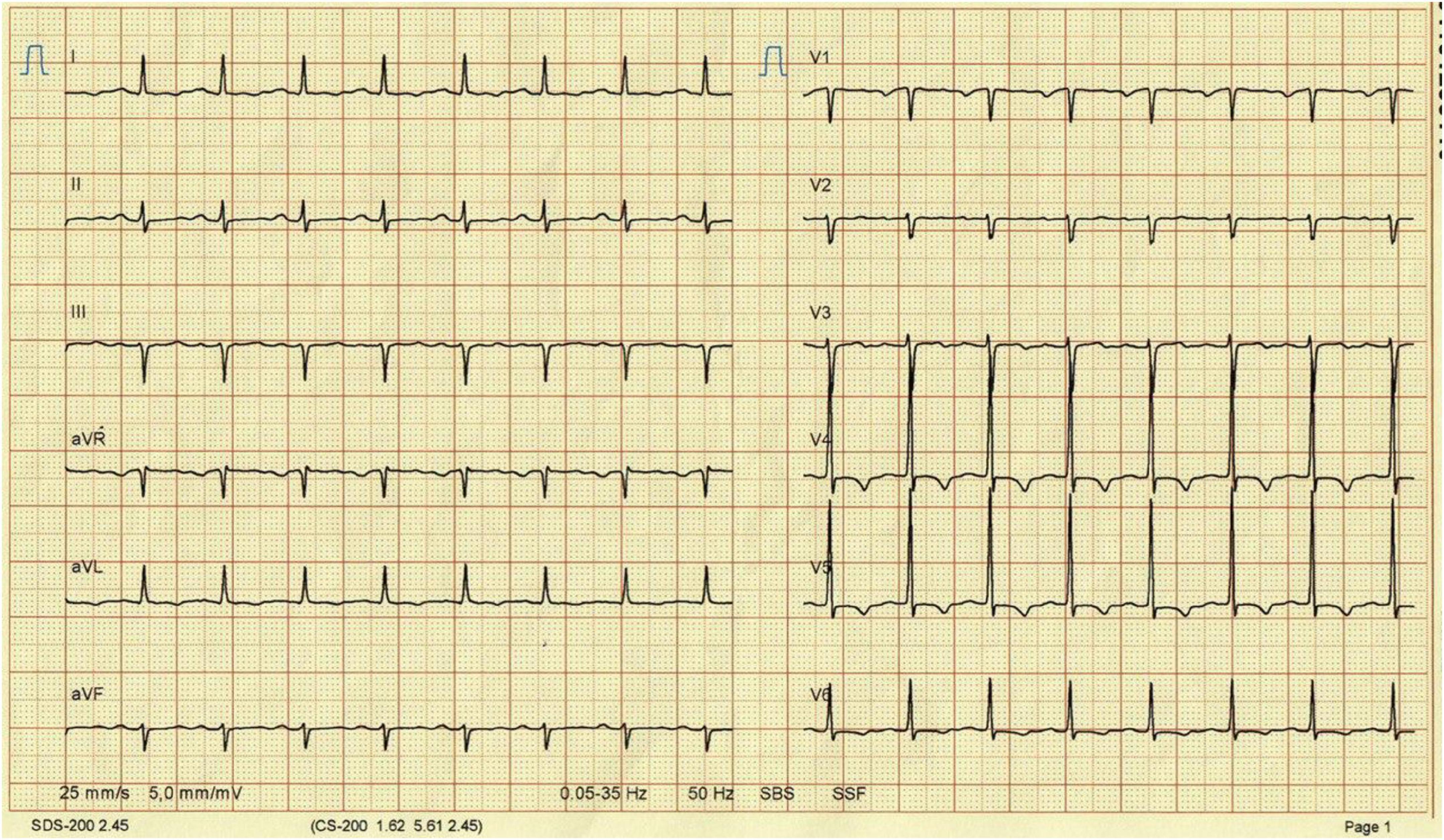
Figure 1. Electrocardiography reveals an atrioventricular type 1.
A serial TMPG measured in the immediate POD period revealed the following: 9 mmHg on the 4th postoperative (POD) day which was related to the tachycardia at 120 beats/min because the MVA was at 3.6 cm2; 2.7 mmHg on the 11th POD; and 4 mmHg on the 33rd POD.
A TTE was performed on the 33rd POD, which revealed a residual MR type A with an MVA of 4 cm2 (Figure 2), the pressure half-time (PHT) of the mitral valve at 49.51 ms (Figure 3A) with a TMPG of 4 mmHg (Figure 3B) and the left auricle at 29 cm2; and a residual TR type A with a PASP at 40 mmHg. None of the POD TTE (immediate, midterm, or long-term follow-up) revealed pannus formation on fibrous tissue growth of the mitral valve.
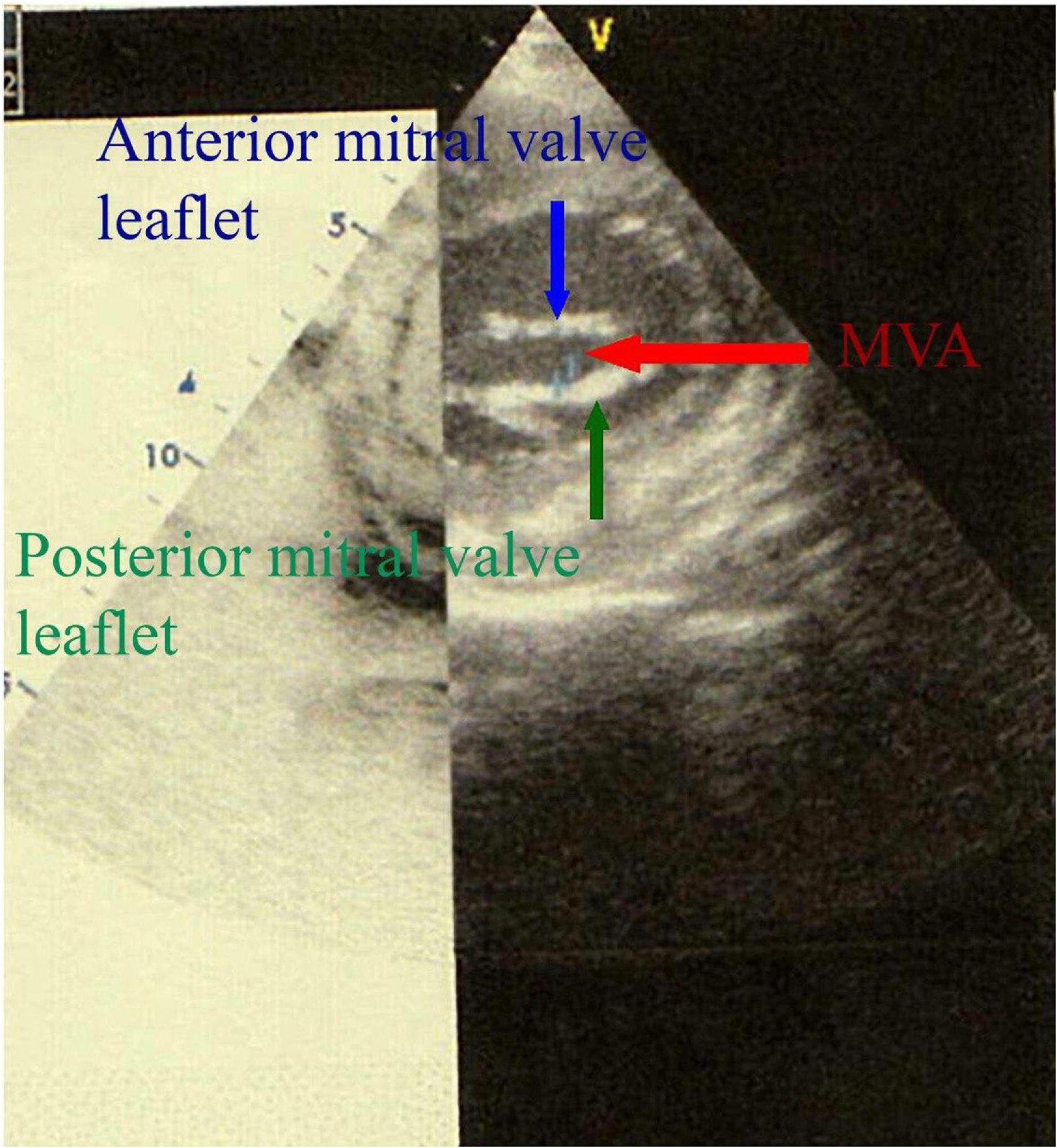
Figure 2. Two-dimensional (2D) transthoracic echocardiography in parasternal short-axis view shows the MVA measurement by planimetry.
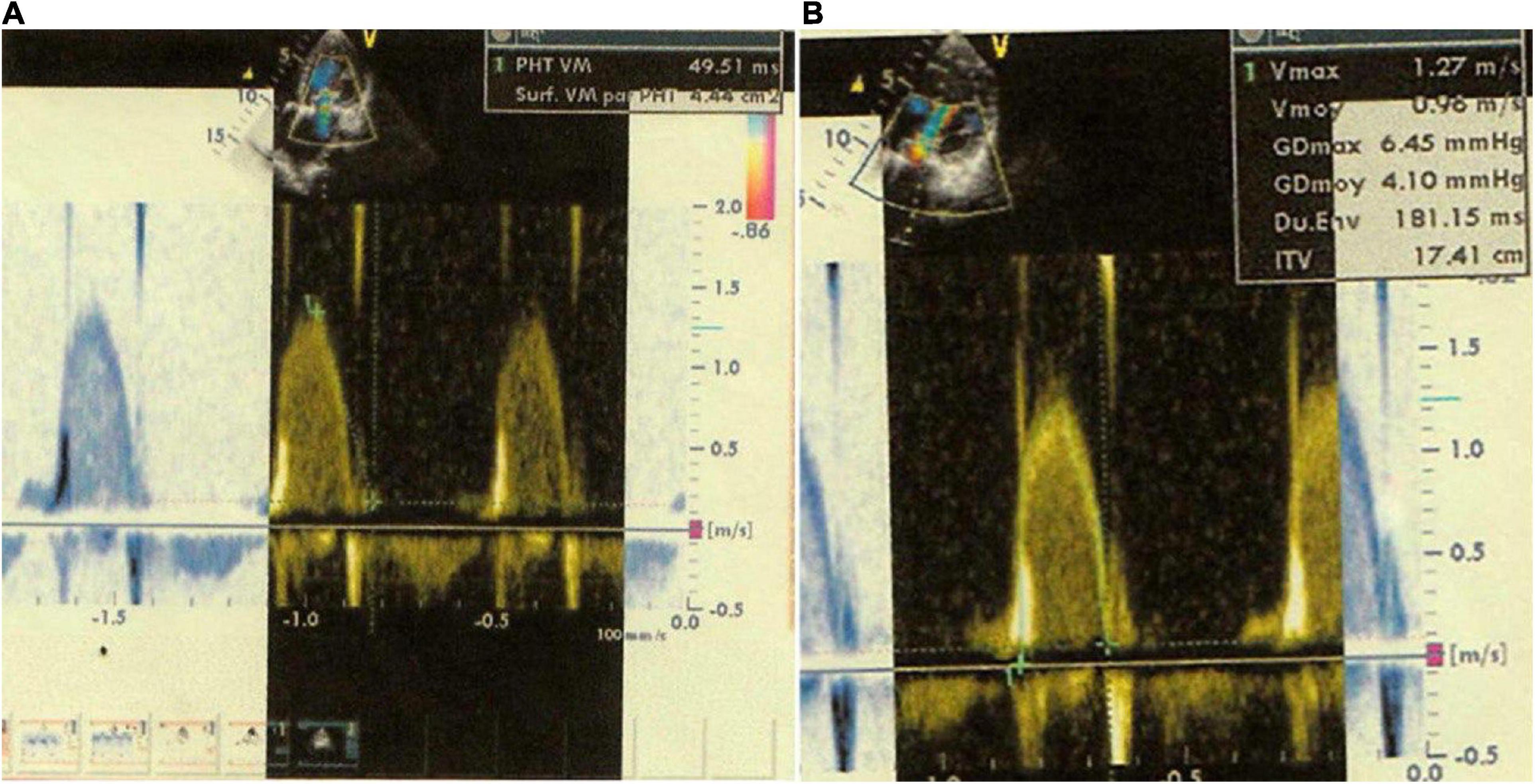
Figure 3. (A) Two-dimensional (2D) apical 4-chamber view shows a mitral valve pressure half-time (PHT) of 49.51 ms. (B) Two-dimensional (2D) apical 4-chamber view shows a transmitral gradient pressure of 4.10 mmHg.
The patient was advised to follow up at the ambulatory care setting every month with a trained general practitioner to manage POD cardiac patients. At this visit, functional signs and complaints of the patient are collected, and a physical examination is performed after taking the patient’s vitals (weight, height, blood pressure, heart rate, respiratory rate, and temperature). During POD surgery, she was administered daily oral medications (furosemide, spironolactone, and acetylsalicylic acid) and monthly intramuscular penicillin benzathine. The patient has an appointment every 3–4 months with the cardiologist. At that visit, an electrocardiogram and an echocardiogram are performed as well as laboratory tests (complete blood counts, comprehensive metabolic panels, and isolated potassium). The patient was counseled about strict compliance with the medical follow-up and to come to the emergency room if any other concerns. She gradually gained weight and increased in height. Menarche occurred 17 months (October 2011) after the procedure. POD development of MS was observed by TTE, with worsening clinical findings during follow-up (Table 1).
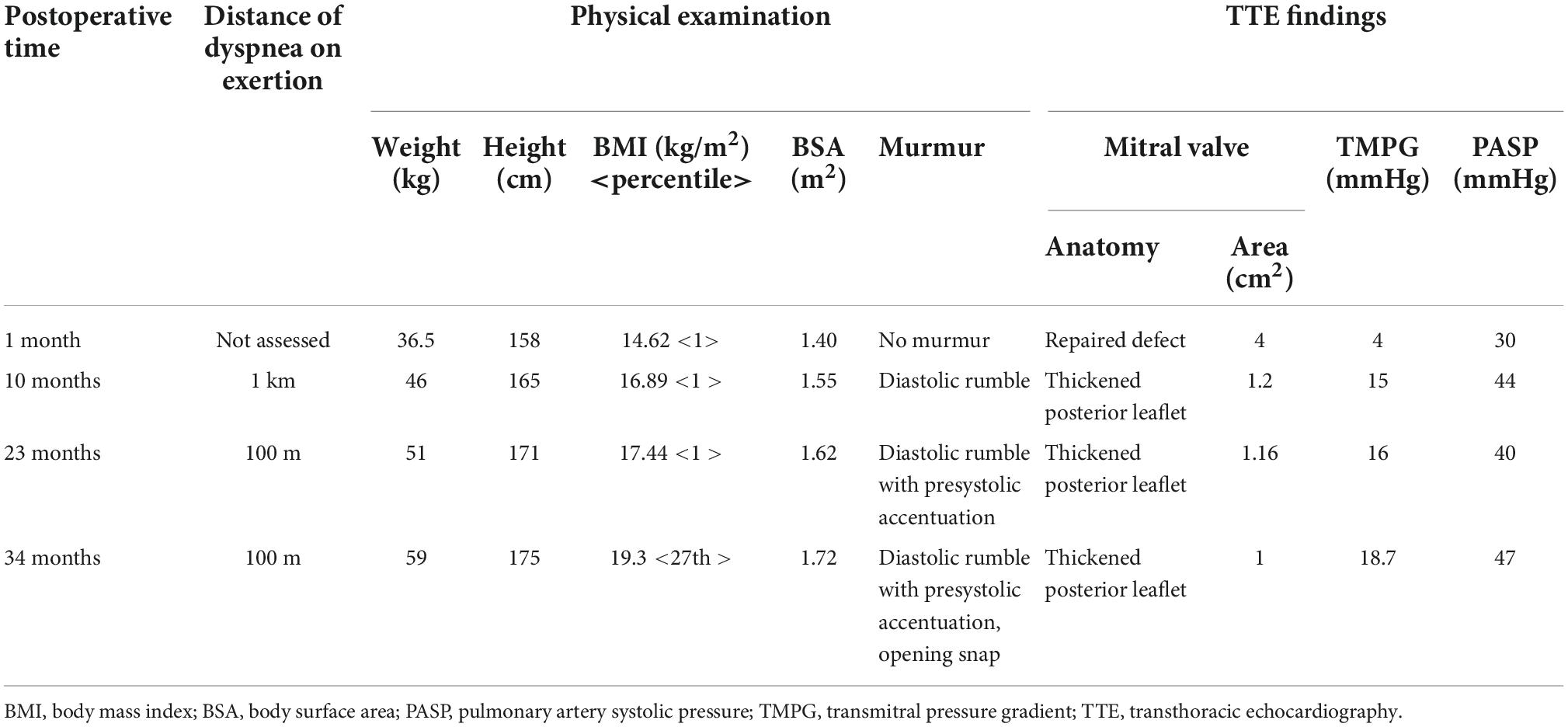
Table 1. Postoperative follow-up findings.
The patient underwent rheumatic mitral valve repair for MR with a Carpentier Edwards ring, which has been known to be a good therapeutic option (9–12).
This study revealed the development of MS after MR repair in a young patient. This complication has been reported solely in the adult population undergoing non-rheumatic MR repair (18–20).
Various mechanisms (28–30) have been implicated in the development of MS after MR repair, including pannus formation, annuloplasty ring size, and subvalvular tethering.
Mitral annulus pannus formation is the predominant POD pathology in delayed MS following MR repair. Our patient underwent rheumatic mitral valve repair for MR with a rigid CE ring. Compared to flexible Duran, this therapeutic option is less commonly associated with POD MS (31). Retrospective studies (31, 32) that compared the outcomes of surgeries in patients who used CE to those who used more flexible annuloplasty options, such as the Duran ring, found a progressive reduction in POD MVA and an increase in TMPG, which were significantly more prevalent in surgeries involving the flexible annuloplasty ring. In these patients, imaging revealed pannus formation around the mitral annulus, which was implicated in the causation of their MS. However, this was not the cause of the changes in MVA and TMPG observed in our patient, as no pannus formation was observed in serial TTE.
The choice of annuloplasty ring (33) has been described as the main mechanism related to the development of early stenosis. When this is the operative mechanism, the POD TMPG is higher than the pre-operative values and the MVA is < 1.5 cm2. However, in our patient, both the post-operative MVA of 3.6 cm2 and TMPG of < 5 mmHg correlate with an appropriately sized annuloplasty ring.
Subvalvular tethering, the cause of MS in patients with ischemic MR (30), was not observed in our patient.
We hypothesized that hemodynamic changes due to rapid body growth lead to a greater BSA, higher circulating blood volume, transvalvular flow, trans-prosthetic pressures, and a decreased effective orifice area indexed to BSA (EOA). Our patient had two pre-operative characteristics that accounted for the rapid increase in the BSA after surgery. Our pre-menarchal patient did not attain peak height velocity and had a BMI below the 3rd percentile. In the first year after surgery, she attained Tanner stage 3 and experienced a corresponding peak growth velocity of 8.4 cm per year. In addition, she had a rapid increase in BMI from the 1st to 10th percentile over a period of 10 months. This rapid increase in height and weight culminated in a corresponding change in BSA, circulating blood volume, and cardiac output. However, the prosthetic ring size remained unchanged. For the transvalvular pressures to remain low, the EOA and flow requirements must be proportionate (34). As the patient size continued to increase, the EOA of the mitral valve became increasingly smaller with the BSA and cardiac output leading to a prosthesis patient mismatch. We hypothesized that this was due to the observed elevation in TMPG.
Different mechanisms have been reported to lead to the occurrence of early or delayed MS after MV repair, which includes surgical technique (16), elevated mean TMPG (15, 35), annuloplasty that reduces ring size (30), and pannus formation on fibrous tissue growth (36). The increase in cardiac output in our patient, proportional to the considerable weight and height gain and the lack of mitral annulus area growth, can account for the development of progressive MS, which is similar to a mismatch between cardiac output and MVA.
Our case is just to reveal the occurrence of this complication in a growing young population, which was added to previous in-depth studies to explain this phenomenon.
Growth spurts in pubescent children have hemodynamic effects that can potentially affect the outcome of MR repair, as children outgrow a mitral valve prosthesis matched based on a projected EOA at their preoperative BSA. Identification of similar groups of patients at risk for post-reconstruction sequela due to hemodynamic changes that occur with rapid growth may assist in prognostication and planning prior to mitral valve surgery. This case also demonstrates the need for further research on an optimal, individualized, and adaptable approach to MR interventions in early pubescence.
The studies involving human participants were reviewed and approved by the Bioethics Committee of Chad. The patients/participants provided their written informed consent to participate in this study. Written informed consent was obtained from the patient for publication of any potentially identifiable images or data included in this case report.
NN, UNC, MP, AG, OO, AD, and IAK: case treatment, manuscript preparation, diagnosis, and literature review. All authors contributed to the study and approved the submitted manuscript.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Cuttler E, Levine S. Cardiotomy and valvulotomy for MS; experimental observations and clinical notes concerning an operated case with recovery. Boston Med Surg J. (1923) 188:1023–7. doi: 10.1056/NEJM192306281882601
2. Lillehei C, Gott V, Dewall R, Varco R. Surgical correction of pure mitral insufficiency by annuloplasty under direct vision. J Lancet. (1957) 77:446–9.
3. Galloway A, Colvin S, Baumann F, Grossi E, Ribakove G, Harty S, et al. A comparison of mitral valve reconstruction with mitral valve replacement: intermediate-term results. Ann Thorac Surg. (1989) 47:655–62. doi: 10.1016/0003-4975(89)90113-6
4. David T, Komeda M, Pollick C, Burns R. Mitral valve annuloplasty: the effect of the type on left ventricular function. Ann Thorac Surg. (1989) 47:524–8. doi: 10.1016/0003-4975(89)90426-8
5. Carpentier A. Cardiac valve surgery—the “French correction”. J Thorac Cardiovasc Surg. (1983) 86:323–37. doi: 10.1016/S0022-5223(19)39144-5
6. Duran C, Pomar J, Revuelta J, Gallo I, Poveda J, Ochoteco A, et al. Conservative operation for mitral insufficiency. J Thorac Cardiovasc Surg. (1980) 79:326–37. doi: 10.1016/S0022-5223(19)37941-3
7. Antunes M. Mitral valve repair into the 1990s. Eur J Cardio Thorac Surg. (1992) 6, (Suppl. 1):S13–6. doi: 10.1093/ejcts/6.Supplement_1.S13
8. Galloway A, Colvin S, Baumann F, Harty S, Spencer F. Current concepts of mitral valve reconstruction for mitral insufficiency. Circulation. (1988) 78:1087–98. doi: 10.1161/01.CIR.78.5.1087
9. Goldstein D, Moskowitz A, Gelijns A, Ailawadi G, Parides M, Perrault L, et al. Two-year outcomes of surgical treatment of severe ischemic MR. N Engl J Med. (2016) 374:344–53. doi: 10.1056/NEJMoa1512913
10. Michler R, Smith P, Parides M, Ailawadi G, Thourani V, Moskowitz A, et al. Two-year outcomes of surgical treatment of moderate ischemic MR. N Engl J Med. (2016) 374:1932–41. doi: 10.1056/NEJMoa1602003
11. Chan V, Ruel M, Elmistekawy E, Mesana T. Determinants of left ventricular dysfunction after repair of chronic asymptomatic MR. Ann Thorac Surg. (2015) 99:38–42. doi: 10.1016/j.athoracsur.2014.07.025
12. Chotivatanapong T. rheumatic mitral valve repair: a personal perspective and results. Asian Cardiovasc Thorac Ann. (2020) 28:366–70. doi: 10.1177/0218492320927315
13. Mesana T, Lam B, Chan V, Chen K, Ruel M, Chan K. Clinical evaluation of functional MS after mitral valve repair for degenerative disease: potential affect on surgical strategy. J Thorac Cardiovasc Surg. (2013) 146:1418–25. doi: 10.1016/j.jtcvs.2013.08.011
14. Bertrand P, Verbrugge F, Verhaert D, Smeets C, Grieten L, Mullens W, et al. Mitral valve area during exercise after restrictive mitral valve annuloplasty. J Am Coll Cardiol. (2015) 65:452–61. doi: 10.1016/j.jacc.2014.11.037
15. Kainuma S, Taniguchi K, Daimon T, Sakaguchi T, Funatsu T, Kondoh H, et al. Does stringent restrictive annuloplasty for functional MR cause functional MS and pulmonary hypertension? Circulation. (2011) 124, (11 Suppl. 1):S97–106. doi: 10.1161/CIRCULATIONAHA.110.013037
16. Bertrand P, Gutermann H, Smeets C, Van Kerrebroeck C, Verhaert D, Vandervoort P, et al. Functional impact of transmitral gradients at rest and during exercise after restrictive annuloplasty for ischemic MR. J Thorac Cardiovasc Surg. (2014) 148:183–7. doi: 10.1016/j.jtcvs.2013.10.013
17. Williams M, Daneshmand M, Jollis J, Horton J, Shaw L, Swaminathan M, et al. Mitral gradients and frequency of recurrence of MR after ring annuloplasty for ischemic MR. Ann Thorac Surg. (2009) 88:1197–201. doi: 10.1016/j.athoracsur.2009.06.022
18. Shabsigh M, Lawrence C, Rosero-Britton B, Kumar N, Kimura S, Durda M, et al. Mitral valve stenosis after open repair surgery for non-rheumatic mitral valve regurgitation: a review. Front Cardiovasc Med. (2016) 3:8. doi: 10.3389/fcvm.2016.00008
19. Chan V, Mesana T, Verma S. Functional MS following mitral valve repair. Curr Opin Cardiol. (2017) 32:161–5. doi: 10.1097/HCO.0000000000000364
20. Kawamoto N, Fujita T, Fukushima S, Shimahara Y, Kume Y, Matsumoto Y, et al. Functional MS after mitral valve repair for type II dysfunction: determinants and impacts on long-term outcome†. Eur J Cardio Thorac Surg. (2018) 54:453–9.
21. Zemel B, Johnston F. Application of the preece-baines growth model to cross-sectional data: problems of validity and interpretation. Am J Hum Biol. (1994) 6:563–70. doi: 10.1002/ajhb.1310060504
22. Bogin B, Wall M, Macvean R. Longitudinal analysis of adolescent growth ofladino and Mayan school children in Guatemala: effects of environment and sex. Am J Phys Anthropol. (1992) 89:447–57. doi: 10.1002/ajpa.1330890406
24. Dolgin M. Nomenclature and Criteria for Diagnosis of Diseases of the Heart and Great Vessels. Boston, MA: Little, Brown and Co (1994).
25. Keren R, Tereschuk M, Luan X. Evaluation of a novel method for grading heart murmur intensity. Archives of Pediatrics & Adolescent Medicine. (2005) 159:329. doi: 10.1001/archpedi.159.4.329
26. Med-Health.net. Grading of Edema. (n.d.). Available online at: http://www.med-health.net/Edema-Grading.html (accessed February 13, 2022).
27. Otto C, Nishimura R, Bonow R, Carabello B, Erwin J, Gentile F, et al. 2020 ACC/AHA guideline for the management of patients with valvular heart disease: a report of the American college of cardiology/American heart association joint committee on clinical practice guidelines. Circulation. (2021) 143:e72–227.
28. Song S, Cho S, Yang J, Park P. Repair for MS due to Pannus formation after duran ring annuloplasty. Ann Thorac Surg. (2010) 90:e93–4. doi: 10.1016/j.athoracsur.2010.08.056
29. El-Eshmawi A, Sun E, Boateng P, Pandis D, Rimsukcharoenchai C, Anyanwu A, et al. Lessons from reoperations for MS after mitral valve repair. J Thorac Cardiovasc Surg. (2021) 161:937–46. doi: 10.1016/j.jtcvs.2020.12.022
30. Kubota K, Otsuji Y, Ueno T, Koriyama C, Levine R, Sakata R, et al. Functional MS after surgical annuloplasty for ischemic MR : importance of subvalvular tethering in the mechanism and dynamic deterioration during exertion. J Thorac Cardiovasc Surg. (2010) 140:617–23. doi: 10.1016/j.jtcvs.2009.11.003
31. Cheol C, Joon B, Suk J, Kyung S, Hyun S, Meong G, et al. Long-term outcomes after mitral ring annuloplasty for degenerative MR : Duran ring vs. Carpentier-Edwards ring. J Heart Valve Dis. (2007) 16:536–45.
32. Okada Y, Shomura T, Yamaura Y, Yoshikawa J. Comparison of the Carpentier and Duran prosthetic rings used in mitral reconstruction. Ann Thorac Surg. (1995) 59:658–63. doi: 10.1016/0003-4975(94)01008-0
33. Kiyoshi D, Tetsuhiro Y, Suguru O, Sachiko Y, Satoshi N, Hitoshi Y. Annuloplasty ring size determines exercise-induced MS severity after valve repair. J Heart Valve Dis. (2015) 24:744–51.
34. Pibarot P. Prosthesis-patient mismatch: definition, clinical impact, and prevention. Heart. (2006) 92:1022–9. doi: 10.1136/hrt.2005.067363
35. Chan K, Chen S, Chan V, Hay K, Mesana T, Lam B. Functional significance of elevated mitral gradients after repair for degenerative MR. Circ Cardiovasc Imaging. (2013) 6:1041–7. doi: 10.1161/CIRCIMAGING.112.000688
Keywords: rheumatic mitral regurgitation, mitral valve (MV) repair, complication, mitral stenosis, case report
Citation: Ngardig Ngaba N, Chibuzo UN, Patel M, Gulati A, Ola O, Djindimadje A and Khan IA (2022) Mitral stenosis in a teenager after rheumatic mitral valve regurgitation valve repair: A case report. Front. Cardiovasc. Med. 9:978874. doi: 10.3389/fcvm.2022.978874
Received: 26 June 2022; Accepted: 16 November 2022;
Published: 15 December 2022.
Edited by:
Liang Xiao, Second Military Medical University, ChinaReviewed by:
Chaoqun Ma, Second Military Medical University, ChinaCopyright © 2022 Ngardig Ngaba, Chibuzo, Patel, Gulati, Ola, Djindimadje and Khan. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Neguemadji Ngardig Ngaba, ZHJuZ2FiYS5ubkBnbWFpbC5jb20=
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.