 Xi Rong
Xi Rong Yawen Zhu2†
Yawen Zhu2† Kai Liu
Kai Liu Xiaoping Chen
Xiaoping Chen- 1Department of Cardiology, The Affiliated Hospital of Southwest Medical University, Southwest Medical University, Luzhou, China
- 2Department of General Practice, West China Hospital, Sichuan University, Chengdu, China
- 3dMed Biopharmaceutical Company Limited, Shanghai, China
- 4Department of Cardiology, West China Hospital, Sichuan University, Chengdu, China
Aim of the review: To assess the risk of hypovolemia for sodium–glucose cotransporter-2 (SGLT2) inhibitors treatment.
Method: A systematic literature retrieval was performed in PubMed, Embase, Cochrane Central Register of Controlled Trials (CENTRAL), Web of Science, and Scopus from inception up to 4 October 2022, Data for study characteristics and outcomes of interest were extracted from each eligible study. Risk ratios (RRs) with a 95% confidence interval (CI) for hypovolemia were calculated using a random-effect model.
Results: A total of 57 studies (n = 68,622) were included in our meta-analysis, with a result of 1,972 hypovolemia incidents (1,142 in the SGLT2 inhibitors group and 830 in the control group). The pooled RR was 1.12 (95% CI: 1.02–1.22). It is evident that receiving SGLT2 inhibitors increased the risk of hypovolemia. When stratified by category of SGLT2 inhibitors the result was consistent; when the subgroup was analyzed by age, the pooled RR was 1.07 (95% CI: 0.94–1.23) in patients aged ≥65 years and 1.14 (95% CI: 1.02–1.28) in those aged <65 years. When comparing the baseline estimated glomerular filtration rate (eGFR) of less than or equal to 60 mL/min/1.73 m2 with a baseline eGFR greater than 60 mL/min/1.73 m2, the pooled RR was 1.21, (95% CI: 1.00–1.46) and 1.08, (95%CI: 0.98–1.20), respectively.
Conclusion: Our meta-analysis has demonstrated that SGLT2 inhibitors increased the risk of hypovolemia in patients with Type 2 Diabetes Mellitus (T2DM). It is necessary to pay attention to the risk of hypovolemia associated with SGLT2 inhibitors, especially in older individuals and those with moderate renal impairment.
Systematic review registration: [https://www.crd.york.ac.uk/prospero/], identifier [CRD42020156254].
Introduction
Type 2 diabetes mellitus (T2DM) is an important health problem worldwide, which is characterized by insulin resistance, β-cell dysfunction, and impaired glucose tolerance (1). The prevalence of diabetes has been increasing dramatically. It is estimated that the overall prevalence of adult diabetes patients was 10.9% in China (2). Diabetes will be the 7th leading cause of death in 2030 (3). Optimal control of plasma glucose is the crucial treatment for T2DM (4).
Sodium–glucose cotransporter-2 (SGLT2) inhibitors are a new class of drugs, which improves glycemia by enhancing glycosuria, subsequently reducing blood pressure by osmotic diuresis and natriuresis (5). There are multiple large-scale randomized control trials demonstrating that SGLT2 inhibitors had a salutary effect on the cardiovascular-renal outcomes, especially on heart failure (6). Although SGLT2 inhibitors exhibited promising potential value in treatment for type 2 diabetes mellitus (T2DM) with cardiovascular-renal comorbidities, the potential adverse events (AEs) related to osmotic diuresis such as hypovolemia should not be neglected. Moreover, older individuals, those with moderate renal impairment, and those aged ≥65 years are susceptible to adverse events related to hypovolemia.
As for the above reasons, our systematic review targeted to investigate the hypovolemia incidents related to SGLT2 inhibitors by meta-analyzing, and we also performed subgroup analysis depended on the category of SGLT2 inhibitors, patients’ age, and baseline estimated glomerular filtration rate (eGFR) to evaluate whether the risk of hypovolemia could be affected by clinical variables.
Materials and methods
Literature search
We performed a systematic and comprehensive literature search in PubMed, Embase, Cochrane Central Register of Controlled Trials (CENTRAL), Web of Science, and Scopus from inception up to 4 October 2022. And we adhered to the 2020 PRISMA (Preferred Reporting Items for Systematic reviews and Meta-Analyses) statement in conducting this study and reporting the results (Supplementary material 1). The search strategy combined the Medical Subject Heading and the text words canagliflozin, dapagliflozin, empagliflozin, ipragliflozin, remogliflozin, ertugliflozin, sergliflozin, luseogliflozin, Sotagliflozin, Tofogliflozin, Sodium glucose co-transporter, SGLT2, SGLT-2, and SGLT 2 (Supplementary material 2). These terms were adjusted to conform with the searching principle of each database; citations without any limits were searched. This systematic review was registered in PROSPERO (CRD42020156254).
Study selection
Two authors (Xinran Li and Qiling Gou) independently reviewed all relevant studies according to prespecified criteria. Inclusion criteria were: (a) RCTs reported in the English language and included adult patients with T2DM; (b) SGLT2 inhibitors compared with placebo or active comparator; (c) duration of follow-up of at least 12 weeks; and (d) the hypovolemia adverse events, which were investigated using a pre-specified list of Medical Dictionary for Regulatory Activities (MedDRA) preferred terms to identify events of hypotension, dehydration, or hypovolemia in the database (Supplementary material 3). Data from completed published manuscripts were considered for inclusion in this analysis.
Data extraction and validity assessment
Two researchers (Xinran Li and Qiling Gou) independently screened and extracted the data using a previously defined standardized Microsoft excel sheet; the following information was extracted from each eligible trial: first author, year of publication, trial identifier, study duration, intervention drug, control drug, sample size, patients characteristics, duration of T2DM, and incident of hypovolemia events. These data were further examined by another investigator (Xi Rong), and any discrepancies were resolved by discussion. If hypovolemia events were not reported in the published paper, then these data were instead extracted from the trial register website. If the trial register website also did not provide the data on hypovolemia events, we attempted to contact the author to get the data. Two reviewers independently applied Cochrane risk-of-bias tool (7) to assess the quality of included RCTs based on the following domains: random sequence generation, allocation concealment, blinding of study participants and personnel, incomplete outcome data, selective reporting, and other biases.
Data synthesis and statistical analysis
Most of the analyses were performed by using RevMan (version 5.3.5; Cochrane Collaboration). For dichotomous data, risk ratios (RRs) and 95% confidence interval (CI) were calculated to appraise the risk of hypovolemia with SGLT2 inhibitors treatment. Furthermore, subgroup analyses were conducted on the category of SGLT2 inhibitors, patients’ age, and baseline estimated glomerular filtration rate (eGFR) to evaluate whether the risk of hypovolemia could be modified by clinical variables. Sensitivity analysis was assessed by omitting one study at a time and re-estimated the combined RR for the remaining studies yielding consistent results to determine whether the result of the original analysis was robust. The Chi-square test (χ2) and I2 statistics were used to assess heterogeneity, Heterogeneity was assessed as low, moderate, and high with I2 values of 25, 50, and 75%, respectively. A random-effects model was adopted if there was evidence of statistical heterogeneity or clinical diversity (P<0.01, I2>50%); otherwise, a fixed-effects model was used if there was no statistical significance of heterogeneity (P>0.01, I2<50%). The presence of publication bias was evaluated by visual inception for funnel plot asymmetry; Begg’s test and trim-and-fill method were also performed using STATA (version15.0; STATA software) to assess publication bias.
Results
Eligible studies and characteristics
Figure 1 shows the result of our literature retrieval; in brief, 11,727 citations were initially screened and 7,606 duplications were excluded. An additional 3,137 articles were excluded based on their titles and abstracts. The remaining 984 citations were evaluated by inclusion criteria, further removing 927 citations. At last, there were 55 papers (57 studies) involving 68,622 patients that met the inclusion criteria at last (8–62). In the paper reported by Barnett (20), patients were recruited and randomized by the stage of chronic kidney disease, and the incident of hypovolemia was presented separately, thus each of them was considered as a separate study in this meta-analysis. Twelve RCTs (n = 11,576) evaluated canagliflozin, 22 RCTs (n = 36,508) evaluated dapagliflozin, 13 RCTs (n = 17,284) evaluated empagliflozin, four RCTs (n = 970) evaluated luseogliflozin, two RCTs (n = 310) evaluated ipragliflozin, two RCTs (n = 440) evaluated tofogliflozin, and the remaining one RCT (n = 312) evaluated bexagliflozin. The last one RCTs (n = 1,222) evaluated sotagliflozin. Among those 57 studies 51 studies compared SGLT2 inhibitors with a placebo, and another six studies compared SGLT2 inhibitors with other antidiabetic drugs. All eligible studies were randomized and double-blind design, and the publication year of studies ranged from 2009 to 2022, The follow-up duration of studies varies from 12 weeks to 208 weeks. The overview of the characteristics of included studies is presented in Table 1.
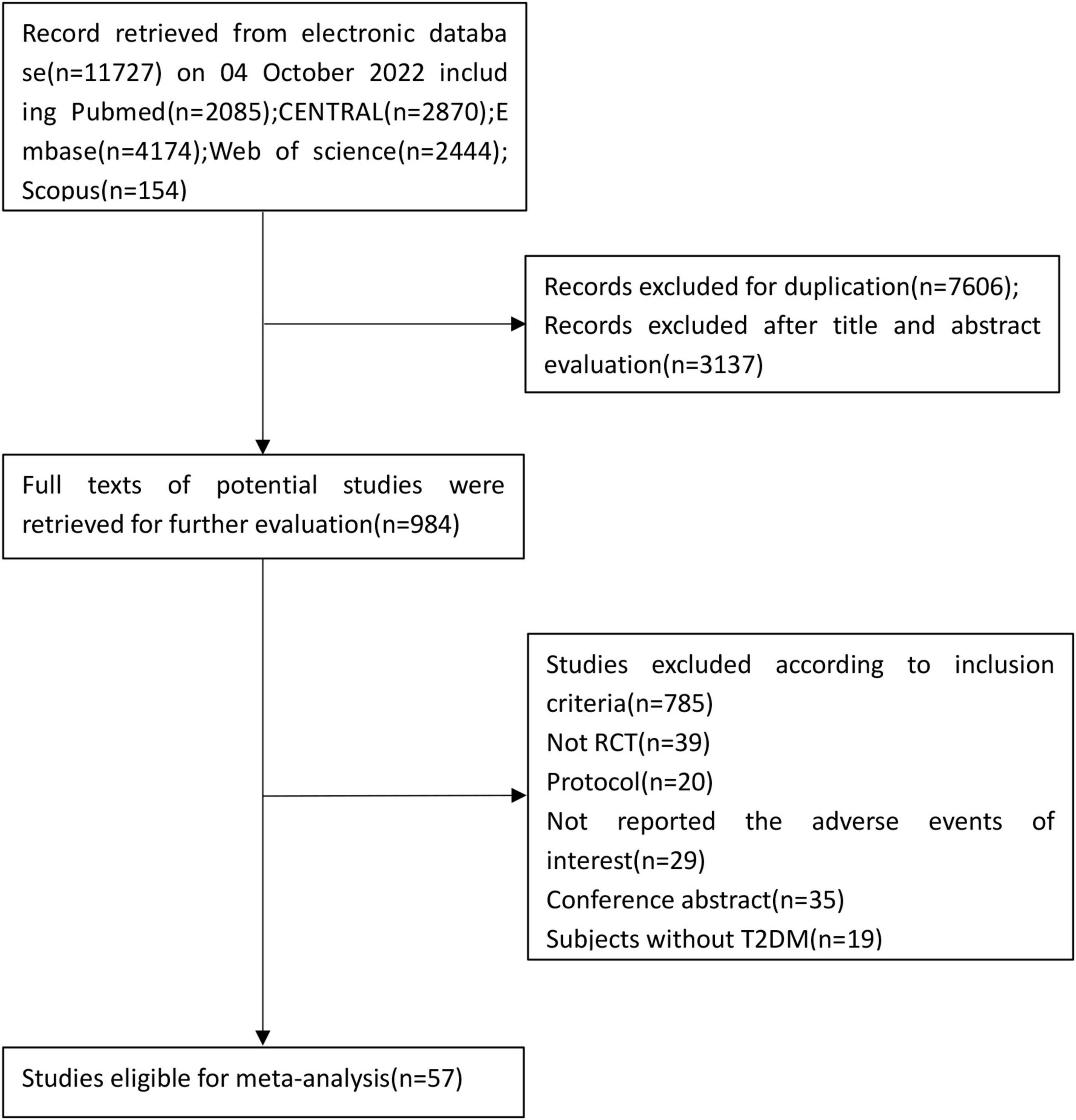
Figure 1. Flowchart showing identification of the included studies.
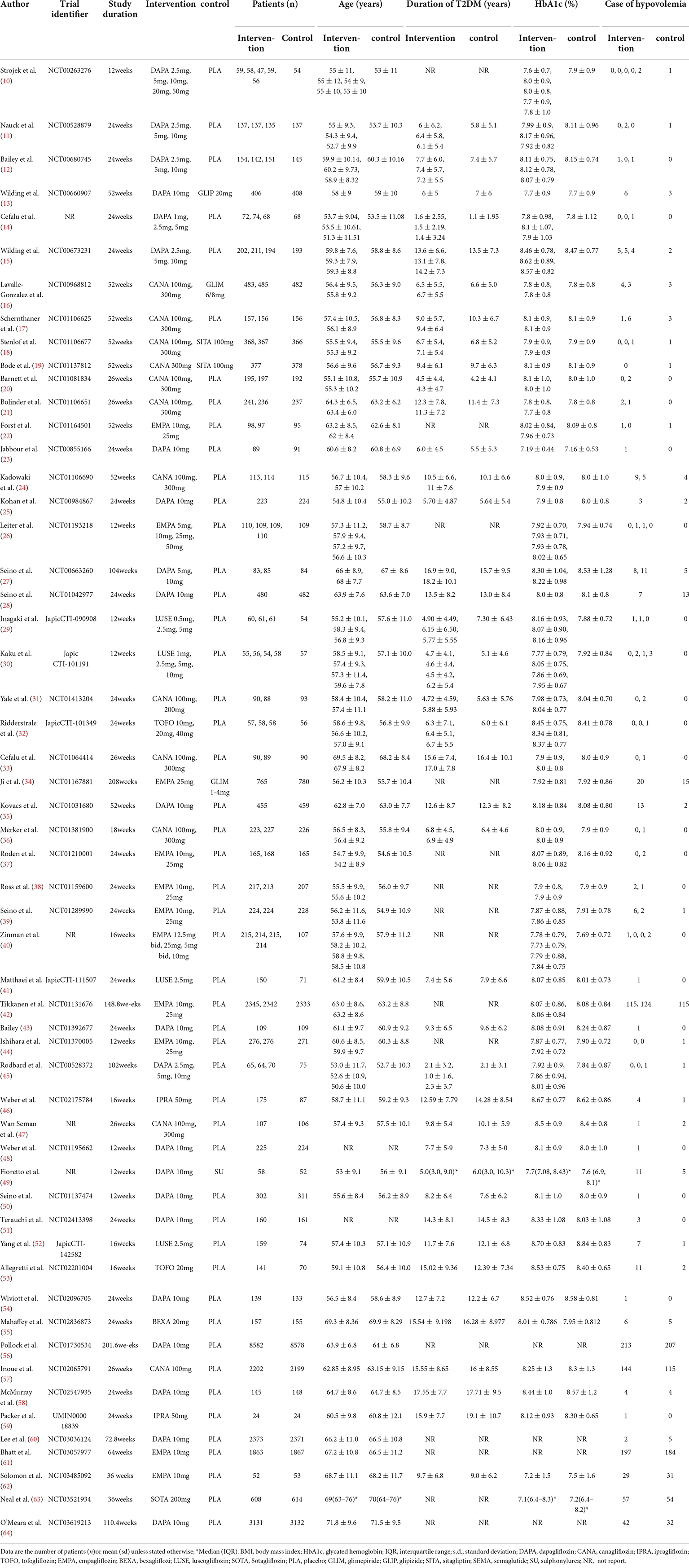
Table 1. Characteristics of the randomized controlled studies (RCTs) included in the meta-analysis.
Quality assessment
We applied Cochrane risk-of-bias tool to assess the study quality. Detailed information about risk-of-bias is presented in Figure 2. Overall, taking the risk of sponsorship bias into consideration, all studies’ other sources of bias were assessed as high. With respect to methods of sequence generation, allocation concealment, and/or blinding of patients and personnel, 25 RCTs had not provided enough information to evaluate.
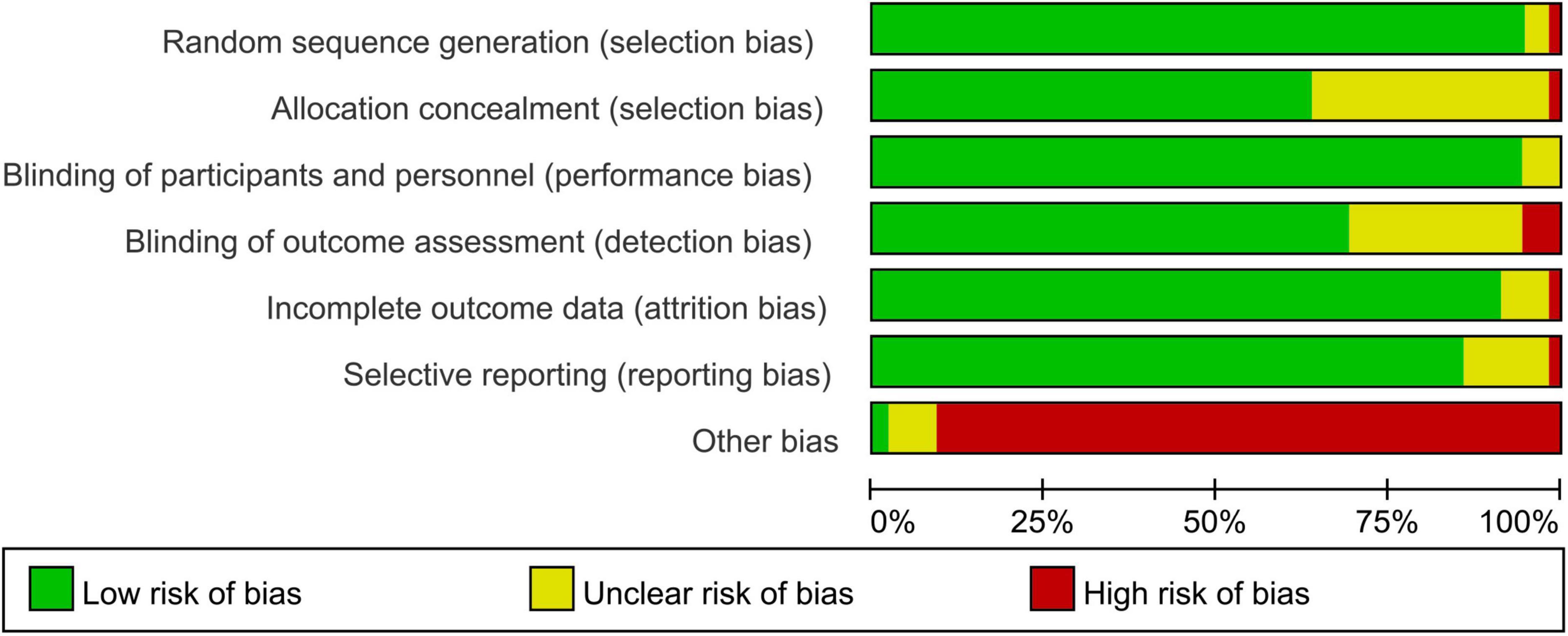
Figure 2. Risk of bias and methodologic quality of the randomized controlled trials. Green represents low risk of bias, red represents high risk of bias, and yellow indicates unclear risk.
Publication bias and sensitivity analysis
A symmetrical funnel plot of SGLT2 inhibitors vs. placebo for hypovolemia indicated no evidence of publication bias (Figure 3). Begg’s test signified there was no publication bias in the included studies (z = 0.06; P = 0.954). We performed the trim-and-fill method to detect and adjust for publication bias; after trim-and-fill, the pooled RR was 1.117 (95% CI: 1.025; 1.218), which was approximately equal to the original pooled RR (1.12). Collectively, in the result of the funnel plot, Begg’s test, and trim-and-fill method, there was no evidence of publication bias. The result of sensitivity analyses indicated that the combined RRs were all not statistically significant and were similar to one another, with a range from 1.14 (95% CI: 1.052; 1.253) to 1.20 (95% CI: 1.088; 1.326). This implied that the result of our meta-analysis was robust.
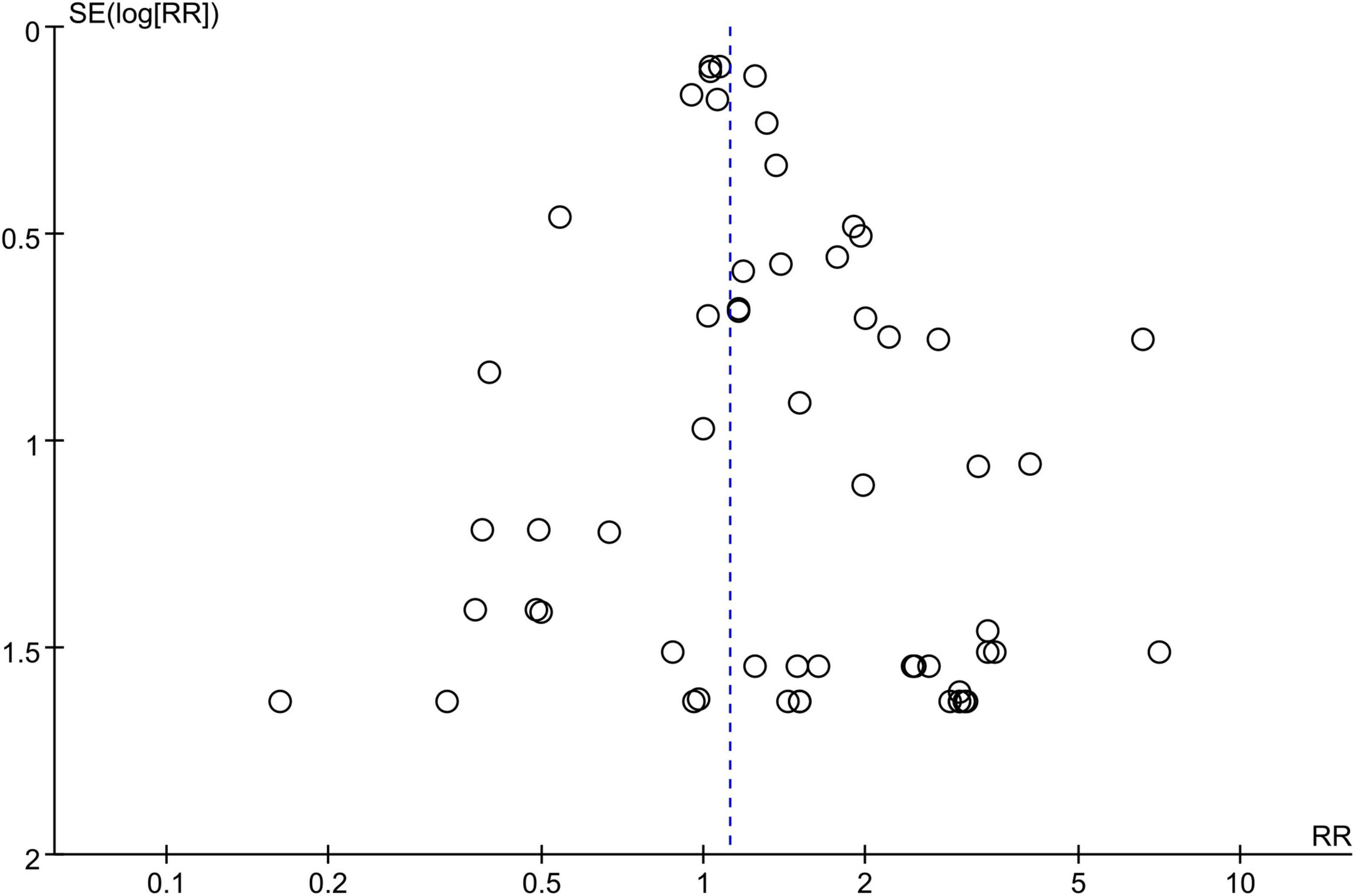
Figure 3. Funnel plot of publication bias for hypovolemia comparing the SGLT2 inhibitors group vs. the placebo group.
Sodium–glucose cotransporter-2 inhibitors and hypovolemia
Compared to the placebo, the combined RR of SGLT2 inhibitors was 1.12 (95% CI:1.02–1.22). The heterogeneity, as assessed by I2, was 0% (P = 0.99), suggesting there was no significant heterogeneity between studies (Figure 4). Additional subgroup analyses were performed to assess the effect of the category of SGLT2 inhibitors, patients’ age, and baseline eGFR on the risk of hypovolemia. When stratified by category of SGLT2 inhibitors, the pooled RRs of sotagliflozin, luseogliflozin, Tofogliflozin, ipragliflozin, canagliflozin, bexagliflozin, dapagliflozin, and empagliflozin were 1.07 (95% CI:0.75–1.52), 2.44 (95% CI:0.64–9.28), 2.28 (95% CI:0.60–8.71), 2.27 (95% CI:0.38–13.61), 1.28 (95% CI:1.02–1.59), 1.18 (95% CI:0.37–3.80), 1.11 (95% CI:0.95–1.30), and 1.06 (95% CI:0.93–1.20), respectively (Figure 5). When the subgroup was analyzed by age, the pooled RR of patients with age ≥65 years and those with age < 65 years were (1.07; 95% CI: 0.94–1.23) and (1.14; 95% CI: 1.02–1.28), respectively (Figure 6). The pooled RR (1.21, 95% CI: 1.00–1.46) was slightly higher in the subgroup with a baseline eGFR less than or equal to 60 mL/min/1.73 m2 than in the subgroup with a baseline eGFR greater than 60 mL/min/1.73 m2 (RR, 1.08; 95% CI: 0.98–1.20), but there was no statistical significance for eGFR subgroup differences (p = 0.30) (Figure 7).
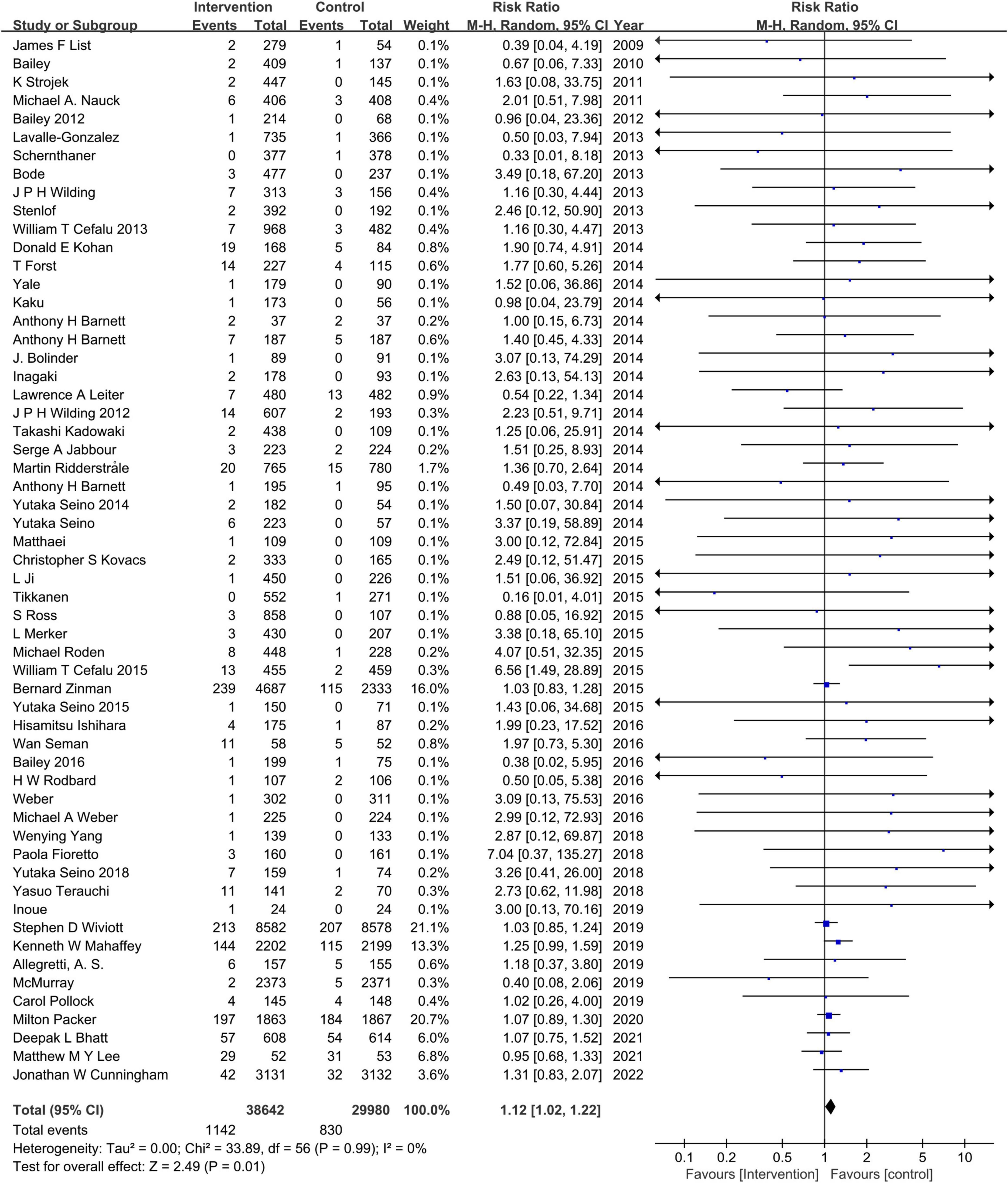
Figure 4. Comparisons of hypovolemia events between the SGLT2 inhibitors group vs. the placebo group.
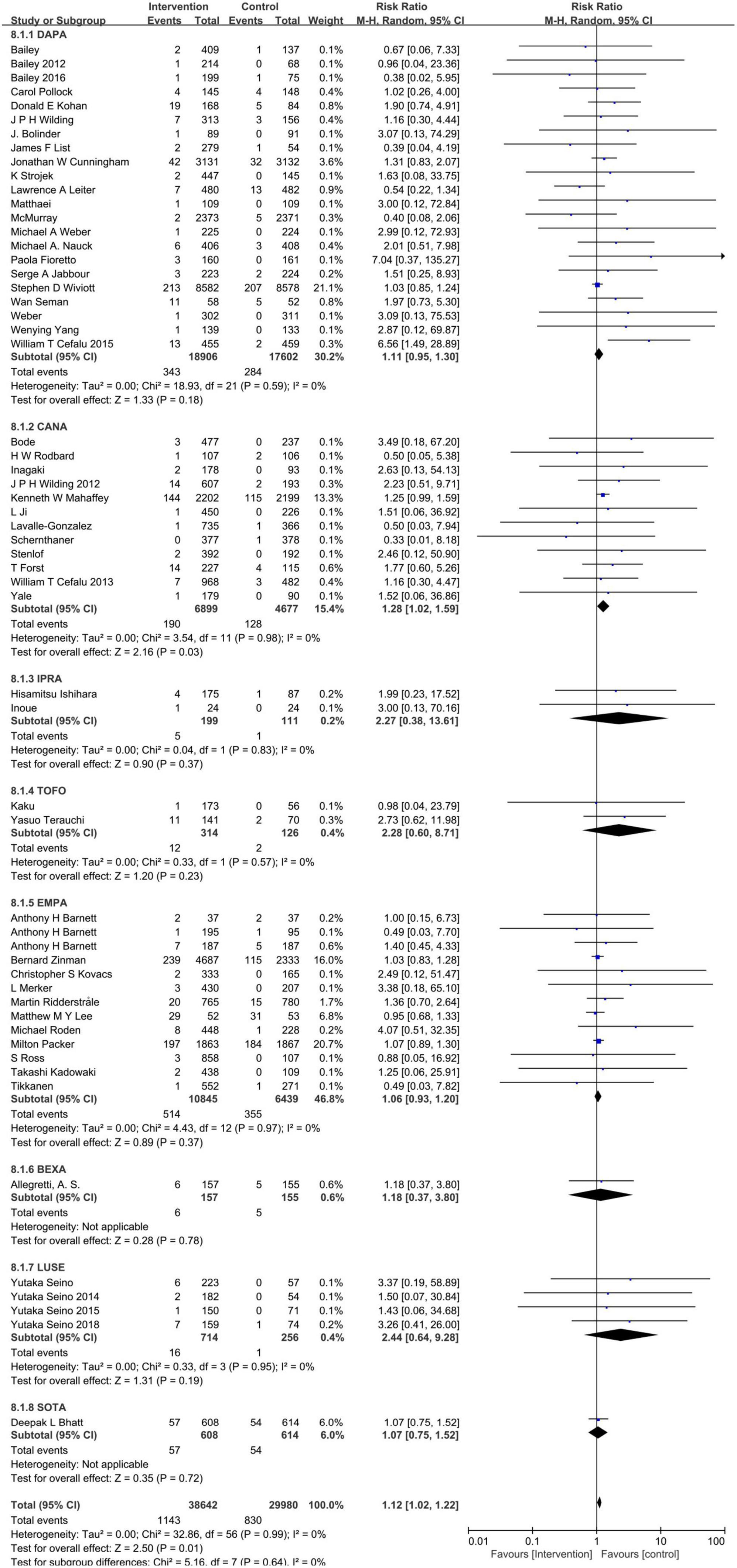
Figure 5. Subgroup analysis of the hypovolemia events between the SGLT2 inhibitors group vs. placebo group stratified by category of SGLT2 inhibitors. DAPA, dapagliflozin; CANA, canagliflozin; IPRA, ipragliflozin; TOFO, Tofogliflozin; EMPA, empagliflozin; BEXA, bexagliflozin; LUSE, luseogliflozin; SOTA, Sotagliflozin.
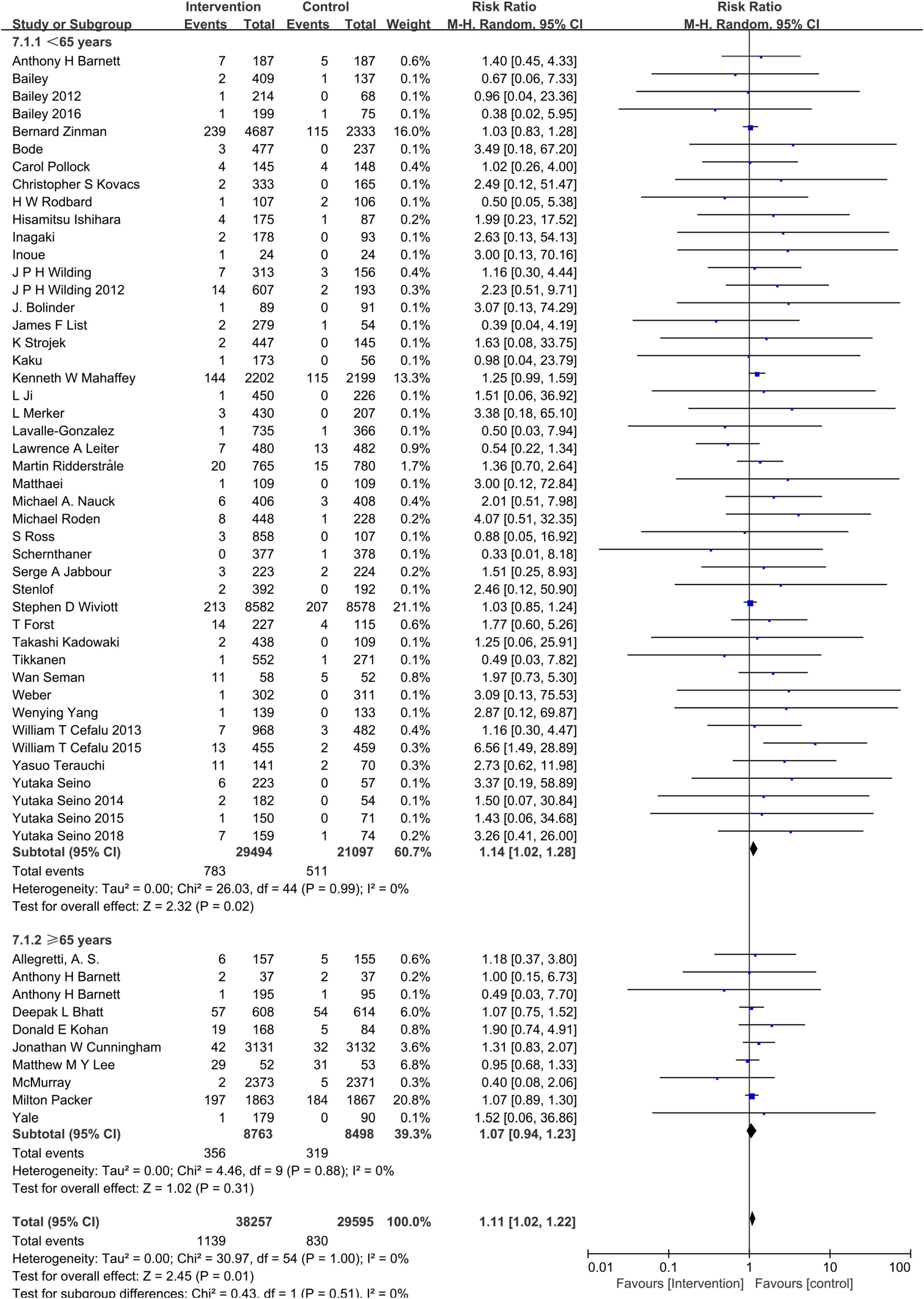
Figure 6. Subgroup analysis of the hypovolemia events between the SGLT2 inhibitors group vs. the placebo group stratified by age.
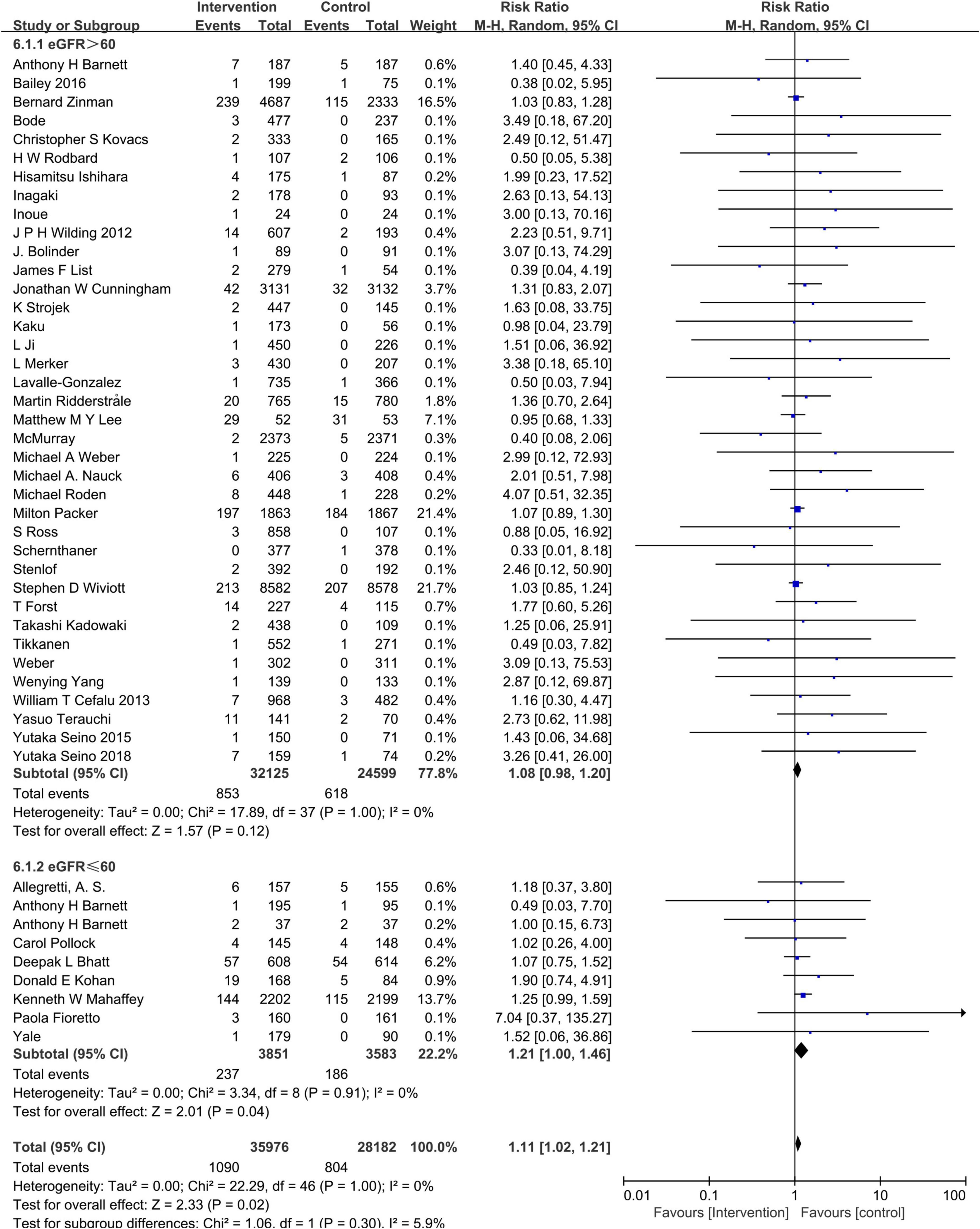
Figure 7. Subgroup analysis of the hypovolemia events between the SGLT2 inhibitors group vs. the placebo group stratified by eGFRs.
Discussion
With 57 included RCTs involving 68,622 patients, this meta-analysis indicated that SGLT2 inhibitors increased the risk of hypovolemia, especially in patients with older age and lower eGFR. Both EMPA-REG OUTCOME trial and the CANVAS trial demonstrated that prescribing SGLT2 inhibitors reduces the risk of hospitalization for heart failure (40, 63). Researchers subsequently conducted a serial clinical trial to confirm this prevailing benefit. The recently finished DAPA-HF trial suggests that dapagliflozin decreases the risk of worsening heart failure or death from cardiovascular causes among those with or without T2DM (58). Although the 2020 CCS/CHFS heart failure guidelines recommended applicating SGLT2 inhibitors to heart failure patients with or without T2DM (64), the mechanisms underpinning the cardioprotective effects of SGLT2 inhibitors remain in debate (65). Natriuresis and osmotic diuresis of SGLT2 inhibitors was thought to play a crucial role in cardioprotective effects (66). Just like every coin has two sides, depending on the osmotic diuresis of SGLT2 inhibitors, it is plausible to consider the possibility of the increased risk of volume depletion with caution. Although individual large multicentral RCTs reported the frequency of adverse events related to volume depletion did not differ between SGLT2 inhibitors and control groups (59, 62). Because of the low statistical power of individual studies and the heterogeneity of the population included in studies (e.g., with or without diabetes), the conclusion remained to be discussed. There is also a lot of meta-analysis evaluating the efficacy and safety of SGLT2 inhibitors, the majority of them focuses on analyzing the risk of hypoglycemia, and genital and urinary tract infections (67). Some of them threw light on the osmotic diuresis-related adverse event, with the result of there being no evidence of SGLT2 inhibitors increasing the risk of hypovolemia (68). This conclusion is not consistent with our meta-analysis. We thought there are three explanations for this inconsistency. First, in contrast to the earlier analysis, our meta-analysis covered a wider spectrum of the category of SGLT2 inhibitors. Second, adopting different analysis methods could impact the result. At last, the differences in included RCTs could also contribute to the inconsistency.
Our meta-analysis also investigated the category of SGLT2 inhibitors, patients’ age, and baseline eGFR impact on the risk of hypovolemia associated with SGLT2 inhibitors treatment. When stratified by category of SGLT2 inhibitors, luseogliflozin, Tofogliflozin and ipragliflozin had RRs greater than 2. It should be noted that they exist a broad 95% CIs as well, which implies the imprecision of statistics. It should be cautious to interpret this point. Canagliflozin showed an increased risk of hypovolemia compared with dapagliflozin or empagliflozin. This might be explained by canagliflozin having the lowest SGLT2/SGLT1 affinity ratio and empagliflozin the highest (69). People aged ≥65 years and with baseline eGFR <60 mL/min/1.73 m2 were more predisposed to hypovolemia; the deteriorative kidney function could be responsible for the conclusion.
We further noticed that our meta-analysis included several trials that tested high doses of SGLT2 inhibitors, such as Dapagliflozin 50 mg, Empagliflozin 12.5 mg, Empagliflozin 25 mg, and so on. With the concerns of whether the result may be influenced by these dosages, we performed an additional subgroup analysis depending on the dosage of SGLT2 with U.S. Food and Drug Administration (FDA) approval. As presented in Figure 8, even though excluded the study arms of dosages that were without FDA approval, the combined RR of SGLT2 was 1.11(95% CI:1.02–1.22), which means SGLT2 inhibitors increase the risk of hypovolemia. So, we conclude that the result could not be influenced by high doses of SGLT2 inhibitors.
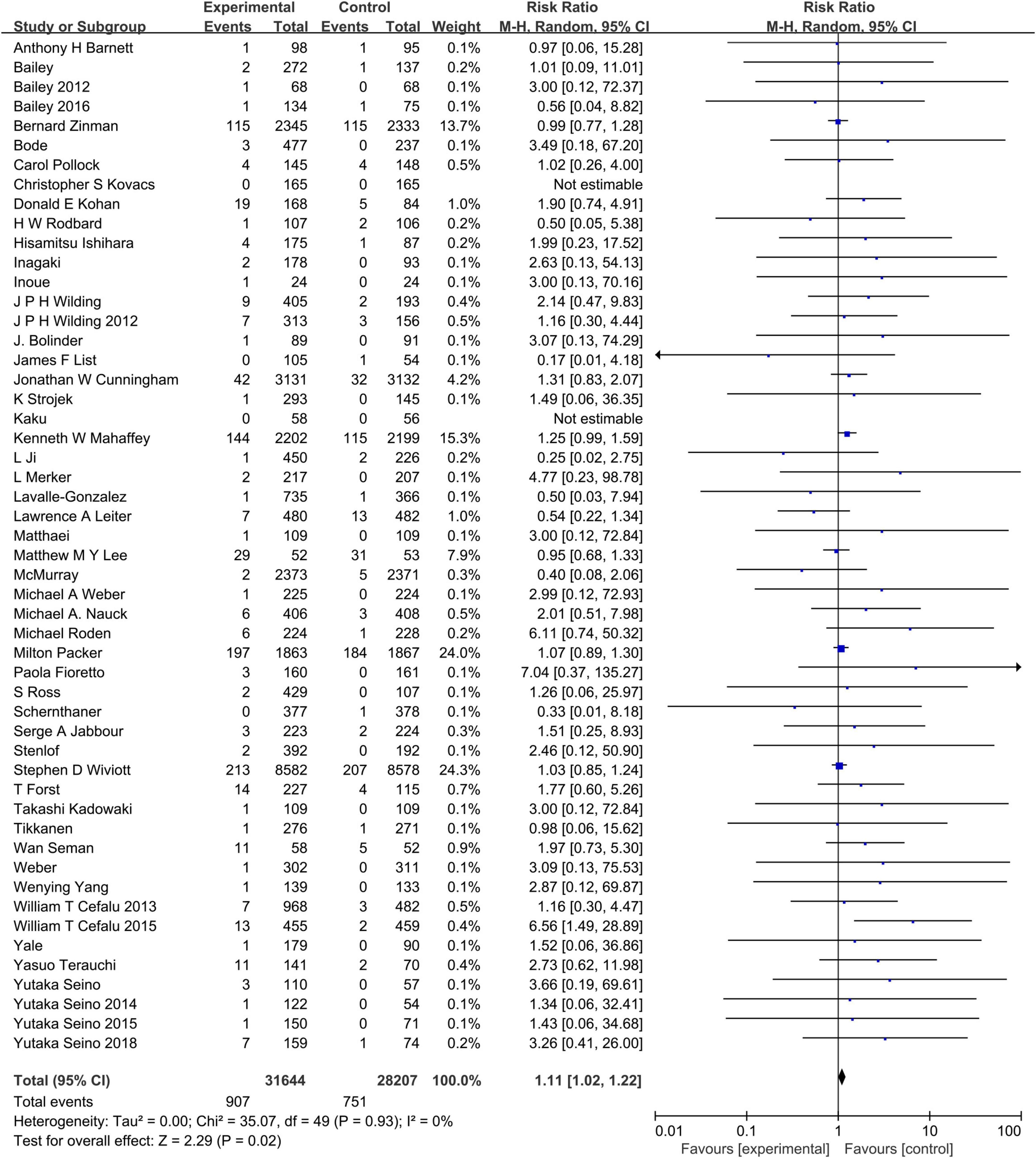
Figure 8. Subgroup analysis of the hypovolemia events between the SGLT2 inhibitors group vs. the placebo group stratified by FDA approval dosage.
Because diuretics might augment the effect of SGLT2 inhibitors, with increasing risk of hypovolemia. The issue of whether the increased risk of hypovolemia associated with SGLT2 inhibitors ascribes to the diuretic treatment should be examined. Among the included 57 studies, there were 15 citations (20, 24, 29, 31, 38, 39, 49, 51, 53–55, 60, 61) providing the information on SGLT2 inhibitors add-on to the background diuretic treatment. Figure 9 shows that the pooled RR of interest in patients not treated without a diuretic at baseline is 1.14 (95% CI: 1.01–1.29) vs. 1.09 (95%CI: 0.96–1.23) in patients treated with a diuretic and the P for interaction is 0.57, which implied the difference of subgroup did not be attributed to diuretic treatment.
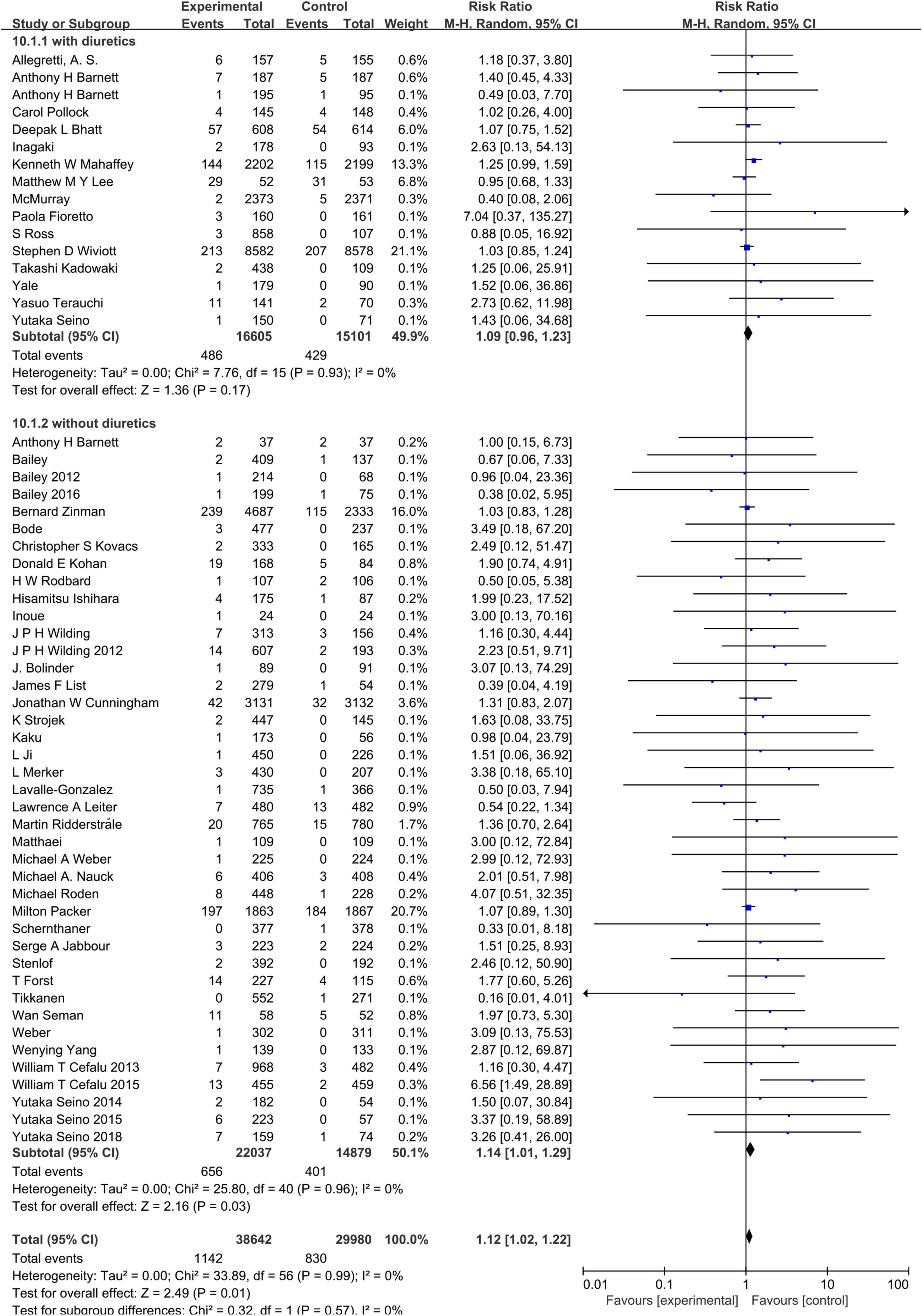
Figure 9. Subgroup analysis of the hypovolemia events between the SGLT2 inhibitors group vs. the placebo group stratified by diuretics treatment.
Collectively, the result of our meta-analysis, that SGLT2 inhibitors increased the risk of hypovolemia, was robust.
This meta-analysis also had some limitations. First, the assessment of hypovolemia was based on a predefined list of preferred terms. This strategy may underestimate the risk of hypovolemia associated with SGLT2 inhibitors. Second, the pooled data was basically drawn from 22 RCTs evaluating dapagliflozin,12 RCTs with canagliflozin, and 13 RCTs with empagliflozin, it should be cautious to extrapolate the conclusion to another category of SGLT2 inhibitors. Finally, we were unable to further stratify the concomitant drug, due to the paucity of data provided by eligible RCTs.
In conclusion, our present meta-analysis indicated that increased risk of hypovolemia associated with SGLT2 inhibitors in T2DM patients. The incidence of hypovolemia is different among the category of SGLT2 inhibitors and may keep rising with the age, and degeneration of renal function. To achieve an optimal fluid volume in patients with heart failure is an exquisite skill, hypovolemia in HF patients may be detrimental (70). Our meta-analysis unveils the increasing risk of hypovolemia associated with SGLT2 inhibitors, if ignoring this risk, hypovolemia resulting in hypotension and renal hypoperfusion may overwhelm the benefit of SGLT2 inhibitors treatment. It is necessary to pay attention for the risk of hypovolemia associated with SGLT2 inhibitors under the context of some heart failure guidelines recommending prescribe SGLT2 inhibitors for heart failure patients with or without T2DM. The interrelation between SGLT2 inhibitors and hypovolemia and the underlying mediating mechanisms of cardio-protection deserves to be further investigated. It is important to take the advantage of the cardio-protection effect of SGLT2 inhibitors to the maximum extent and avoid the risk of hypovolemia associated with SGLT2 inhibitors to the utmost. It is also intriguing to conduct large-scale, multicenter, double-blind, head-to-head RCTs to compare the efficacy and safety of SGLT2 inhibitors with diuretics.
Conclusion
In summary, the present meta-analysis indicated that SGLT2 inhibitors increased the risk of hypovolemia in patients with T2DM. The incidence of hypovolemia may increase with the decreasing of eGFR and growth of age. It is important to pay attention to the potential adverse event, except the common adverse event such as hypoglycemia, and genitourinary infection. Our meta-analysis indicates that there is an increase in hypovolemia associated with SGLT2 inhibitors treatment. It is necessary to be concerned about the risk of hypovolemia associated with SGLT2 inhibitors, especially in older individuals and those with moderate renal impairment.
Data availability statement
The original contributions presented in this study are included in the article/Supplementary material, further inquiries can be directed to the corresponding author/s.
Author contributions
XR was involved in designing the study, literature retrieval, quality assessment, and manuscript writing. YZ, BW, XL, and QG contributed to the extract data. KL provided suggestions on carrying out the study. XC was involved in manuscript preparation. All authors contributed to the study’s conception and design.
Funding
This analysis received a grant from the Science and Technology Pillar Program in Sichuan Province, China (grant no. 2022YFS0356).
Acknowledgments
The meta-analysis had been accepted by ESC Congress 2020 as an ePoster abstract.
Conflict of interest
Author BW was employed by dMed Biopharmaceutical Company Limited.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fcvm.2022.973129/full#supplementary-material
References
1. Pearson ER. Type 2 diabetes: a multifaceted disease. Diabetologia. (2019) 62:1107–12. doi: 10.1007/s00125-019-4909-y
2. Wang L, Gao P, Zhang M, Huang Z, Zhang D, Deng Q, et al. Prevalence and ethnic pattern of diabetes and prediabetes in China in 2013. JAMA. (2017) 317:2515–23. doi: 10.1001/jama.2017.7596
3. World Health Organiziation. Global Report on Diabetes. Geneva: World Health Organiziation (2016).
4. Vijan S. In the clinic. type 2 diabetes. Ann Intern Med. (2015) 162:Itc1–16. doi: 10.7326/AITC201503030
5. Ferrannini E. Sodium-glucose co-transporters and their inhibition: clinical physiology. Cell Metab. (2017) 26:27–38. doi: 10.1016/j.cmet.2017.04.011
6. Heerspink HJ, Perkins BA, Fitchett DH, Husain M, Cherney DZ. Sodium glucose cotransporter 2 inhibitors in the treatment of diabetes mellitus: cardiovascular and kidney effects, potential mechanisms, and clinical applications. Circulation. (2016) 134:752–72. doi: 10.1161/CIRCULATIONAHA.116.021887
7. Sterne JAC, Savoviæ J, Page MJ, Elbers RG, Blencowe NS, Boutron I, et al. RoB 2: a revised tool for assessing risk of bias in randomised trials. BMJ. (2019) 366:l4898. doi: 10.1136/bmj.l4898
8. List JF, Woo V, Morales E, Tang W, Fiedorek FT. Sodium-glucose cotransport inhibition with dapagliflozin in type 2 diabetes. Diabetes Care. (2009) 32:650–7. doi: 10.2337/dc08-1863
9. Bailey CJ, Gross JL, Pieters A, Bastien A, List JF. Effect of dapagliflozin in patients with type 2 diabetes who have inadequate glycaemic control with metformin: a randomised, double-blind, placebo-controlled trial. Lancet. (2010) 375:2223–33. doi: 10.1016/S0140-6736(10)60407-2
10. Strojek K, Yoon KH, Hruba V, Elze M, Langkilde AM, Parikh S. Effect of dapagliflozin in patients with type 2 diabetes who have inadequate glycaemic control with glimepiride: a randomized, 24-week, double-blind, placebo-controlled trial. Diabetes Obesity Metab. (2011) 13:928–38. doi: 10.1111/j.1463-1326.2011.01434.x
11. Nauck MA, Del Prato S, Meier JJ, Duran-Garcia S, Rohwedder K, Elze M, et al. Dapagliflozin versus glipizide as add-on therapy in patients with type 2 diabetes who have inadequate glycemic control with metformin: a randomized, 52-week, double-blind, active-controlled noninferiority trial. Diabetes Care. (2011) 34:2015–22. doi: 10.2337/dc11-0606
12. Bailey CJ, Iqbal N, T’Joen C, List JF. Dapagliflozin monotherapy in drug-naïve patients with diabetes: a randomized-controlled trial of low-dose range. Diabetes Obesity Metab. (2012) 14:951–9. doi: 10.1111/j.1463-1326.2012.01659.x
13. Wilding JPH, Woo V, Soler NG, Pahor A, Sugg J, Rohwedder K, et al. Long-term efficacy of dapagliflozin in patients with type 2 diabetes mellitus receiving high doses of insulin: A randomized trial. Deutsche Medizin Wochensch. (2013) 138(Suppl 1):S27–38.
14. Cefalu WT, Leiter LA, Yoon KH, Arias P, Niskanen L, Xie J, et al. Efficacy and safety of canagliflozin versus glimepiride in patients with type 2 diabetes inadequately controlled with metformin (CANTATA-SU): 52 week results from a randomised, double-blind, phase 3 non-inferiority trial. Lancet. (2013) 382:941–50. doi: 10.1016/S0140-6736(13)60683-2
15. Wilding JP, Charpentier G, Hollander P, Gonzalez-Galvez G, Mathieu C, Vercruysse F, et al. Efficacy and safety of canagliflozin in patients with type 2 diabetes mellitus inadequately controlled with metformin and sulphonylurea: a randomised trial. Int J Clin Pract. (2013) 67:1267–82. doi: 10.1111/ijcp.12322
16. Lavalle-Gonzalez FJ, Januszewicz A, Davidson J, Tong C, Qiu R, Canovatchel W, et al. Efficacy and safety of canagliflozin compared with placebo and sitagliptin in patients with type 2 diabetes on background metformin monotherapy: a randomised trial. Diabetologia. (2013) 56:2582–92. doi: 10.1007/s00125-013-3039-1
17. Schernthaner G, Gross JL, Rosenstock J, Guarisco M, Fu M, Yee J, et al. Canagliflozin compared with sitagliptin for patients with type 2 diabetes who do not have adequate glycemic control with metformin plus sulfonylurea: a 52-week randomized trial. Diabetes Care. (2013) 36:2508–15. doi: 10.2337/dc12-2491
18. Stenlof K, Cefalu WT, Kim KA, Alba M, Usiskin K, Tong C, et al. Efficacy and safety of canagliflozin monotherapy in subjects with type 2 diabetes mellitus inadequately controlled with diet and exercise. Diabetes Obesity Metab. (2013) 15:372–82. doi: 10.1111/dom.12054
19. Bode B, Stenlof K, Sullivan D, Fung A, Usiskin K. Efficacy and safety of canagliflozin treatment in older subjects with type 2 diabetes mellitus: a randomized trial. Hosp Pract. (2013) 41:72–84. doi: 10.3810/hp.2013.04.1020
20. Barnett AH, Mithal A, Manassie J, Jones R, Rattunde H, Woerle HJ, et al. Efficacy and safety of empagliflozin added to existing antidiabetes treatment in patients with type 2 diabetes and chronic kidney disease: a randomised, double-blind, placebo-controlled trial. Lancet Diabetes Endocrinol. (2014) 2:369–84. doi: 10.1016/S2213-8587(13)70208-0
21. Bolinder J, Ljunggren O, Johansson L, Wilding J, Langkilde AM, Sjostrom CD, et al. Dapagliflozin maintains glycaemic control while reducing weight and body fat mass over 2 years in patients with type 2 diabetes mellitus inadequately controlled on metformin. Diabetes Obesity Metab. (2014) 16:159–69. doi: 10.1111/dom.12189
22. Forst T, Guthrie R, Goldenberg R, Yee J, Vijapurkar U, Meininger G, et al. Efficacy and safety of canagliflozin over 52 weeks in patients with type 2 diabetes on background metformin and pioglitazone. Diabetes Obesity Metab. (2014) 16:467–77. doi: 10.1111/dom.12273
23. Jabbour SA, Hardy E, Sugg J, Parikh S. Dapagliflozin is effective as add-on therapy to sitagliptin with or withoutmetformin: a 24-week, multicenter, randomized, double-blind, placebo-controlled study. Diabetes Care. (2014) 37:740–50. doi: 10.2337/dc13-0467
24. Kadowaki T, Haneda M, Inagaki N, Terauchi Y, Taniguchi A, Koiwai K, et al. Empagliflozin monotherapy in Japanese patients with type 2 diabetes mellitus: a randomized, 12-week, double-blind, placebo-controlled, phase II trial. Adv Therapy. (2014) 31:621–38. doi: 10.1007/s12325-014-0126-8
25. Kohan DE, Fioretto P, Tang W, List JF. Long-term study of patients with type 2 diabetes and moderate renal impairment shows that dapagliflozin reduces weight and blood pressure but does not improve glycemic control. Kidney Int. (2014) 85:962–71. doi: 10.1038/ki.2013.356
26. Leiter LA, Cefalu WT, de Bruin TW, Gause-Nilsson I, Sugg J, Parikh SJ. Dapagliflozin added to usual care in individuals with type 2 diabetes mellitus with preexisting cardiovascular disease: a 24-week, multicenter, randomized, double-blind, placebo-controlled study with a 28-week extension. J Am Geriatr Soc. (2014) 62:1252–62. doi: 10.1111/jgs.12881
27. Seino Y, Sasaki T, Fukatsu A, Sakai S, Samukawa Y. Efficacy and safety of luseogliflozin monotherapy in Japanese patients with type 2 diabetes mellitus: a 12-week, randomized, placebo-controlled, phase II study. Curr Med Res Opin. (2014) 30:1219–30. doi: 10.1185/03007995.2014.901943
28. Seino Y, Sasaki T, Fukatsu A, Ubukata M, Sakai S, Samukawa Y. Dose-finding study of luseogliflozin in Japanese patients with type 2 diabetes mellitus: a 12-week, randomized, double-blind, placebo-controlled, phase II study. Curr Med Res Opin. (2014) 30:1231–44. doi: 10.1185/03007995.2014.909390
29. Inagaki N, Kondo K, Yoshinari T, Takahashi N, Susuta Y, Kuki H. Efficacy and safety of canagliflozin monotherapy in Japanese patients with type 2 diabetes inadequately controlled with diet and exercise: a 24-week, randomized, double-blind, placebo-controlled, Phase III study. Expert Opin Pharmacother. (2014) 15:1501–15. doi: 10.1517/14656566.2014.935764
30. Kaku K, Watada H, Iwamoto Y, Utsunomiya K, Terauchi Y, Tobe K, et al. Efficacy and safety of monotherapy with the novel sodium/glucose cotransporter-2 inhibitor tofogliflozin in Japanese patients with type 2 diabetes mellitus: a combined Phase 2 and 3 randomized, placebo-controlled, double-blind, parallel-group comparative study. Cardiovasc Diabetol. (2014) 13:65. doi: 10.1186/1475-2840-13-65
31. Yale JF, Bakris G, Cariou B, Nieto J, David-Neto E, Yue D, et al. Efficacy and safety of canagliflozin over 52 weeks in patients with type 2 diabetes mellitus and chronic kidney disease. Diabetes Obesity Metab. (2014) 16:1016–27. doi: 10.1111/dom.12348
32. Ridderstrale M, Andersen KR, Zeller C, Kim G, Woerle HJ, Broedl UC. Comparison of empagliflozin and glimepiride as add-on to metformin in patients with type 2 diabetes: a 104-week randomised, active-controlled, double-blind, phase 3 trial. Lancet Diabetes Endocrinol. (2014) 2:691–700. doi: 10.1016/S2213-8587(14)70120-2
33. Cefalu WT, Leiter LA, De Bruin TWA, Gause-Nilsson I, Sugg J, Parikh SJ. Dapagliflozin’s effects on glycemia and cardiovascular risk factors in high-risk patients with type 2 diabetes: A 24-week, multicenter, randomized, double-blind, placebo-controlled study with a 28-week extension. Diabetes Care. (2015) 38:1218–27. doi: 10.2337/dc14-0315
34. Ji L, Han P, Liu Y, Yang G, Dieu Van NK, Vijapurkar U, et al. Canagliflozin in Asian patients with type 2 diabetes on metformin alone or metformin in combination with sulphonylurea. Diabetes Obesity Metab. (2015) 17:23–31. doi: 10.1111/dom.12385
35. Kovacs CS, Seshiah V, Swallow R, Jones R, Rattunde H, Woerle HJ, et al. Empagliflozin improves glycaemic and weight control as add-on therapy to pioglitazone or pioglitazone plus metformin in patients with type 2 diabetes: a 24-week, randomized, placebo-controlled trial. Diabetes Obesity Metab. (2014) 16:147–58. doi: 10.1111/dom.12188
36. Merker L, Haring HU, Christiansen AV, Roux F, Salsali A, Kim G, et al. Empagliflozin as add-on to metformin in people with Type 2 diabetes. Diabetic Med. (2015) 32:1555–67. doi: 10.1111/dme.12814
37. Roden M, Merker L, Christiansen AV, Roux F, Salsali A, Kim G, et al. Safety, tolerability and effects on cardiometabolic risk factors of empagliflozin monotherapy in drug-naïve patients with type 2 diabetes: a double-blind extension of a Phase III randomized controlled trial. Cardiovasc Diabetol. (2015) 14:154. doi: 10.1186/s12933-015-0314-0
38. Ross S, Thamer C, Cescutti J, Meinicke T, Woerle HJ, Broedl UC. Efficacy and safety of empagliflozin twice daily versus once daily in patients with type 2 diabetes inadequately controlled on metformin: a 16-week, randomized, placebo-controlled trial. Diabetes Obesity Metab. (2015) 17:699–702. doi: 10.1111/dom.12469
39. Seino Y, Inagaki N, Haneda M, Kaku K, Sasaki T, Fukatsu A, et al. Efficacy and safety of luseogliflozin added to various oral antidiabetic drugs in Japanese patients with type 2 diabetes mellitus. J Diabetes Investig. (2015) 6:443–53. doi: 10.1111/jdi.12316
40. Zinman B, Wanner C, Lachin JM, Fitchett D, Bluhmki E, Hantel S, et al. Empagliflozin, cardiovascular outcomes, and mortality in type 2 diabetes. N Engl J Med. (2015) 373:2117–28. doi: 10.1056/NEJMoa1504720
41. Matthaei S, Bowering K, Rohwedder K, Grohl A, Parikh S. Dapagliflozin improves glycemic control and reduces body weight as add-on therapy to metformin plus sulfonylurea: a 24-Week randomized, double-blind clinical trial. Diabetes Care. (2015) 38:365–72. doi: 10.2337/dc14-0666
42. Tikkanen I, Narko K, Zeller C, Green A, Salsali A, Broedl UC, et al. Empagliflozin reduces blood pressure in patients with type 2 diabetes and hypertension. Diabetes Care. (2015) 38:420–8. doi: 10.2337/dc14-1096
43. Bailey CJ. Efficacy and safety of dapagliflozin monotherapy in people with type 2 diabetes: a randomized double-blind placebo-controlled 102-week trial. Therap Res. (2016) 37:382–3.
44. Ishihara H, Yamaguchi S, Nakao I, Okitsu A, Asahina S. Efficacy and safety of ipragliflozin as add-on therapy to insulin in Japanese patients with type 2 diabetes mellitus (IOLITE): a multi-centre, randomized, placebo-controlled, double-blind study. Diabetes Obesity Metab. (2016) 18:1207–16. doi: 10.1111/dom.12745
45. Rodbard HW, Seufert J, Aggarwal N, Cao A, Fung A, Pfeifer M, et al. Efficacy and safety of titrated canagliflozin in patients with type 2 diabetes mellitus inadequately controlled on metformin and sitagliptin. Diabetes Obesity Metab. (2016) 18:812–9. doi: 10.1111/dom.12684
46. Weber MA, Mansfield TA, Cain VA, Iqbal N, Parikh S, Ptaszynska A. Blood pressure and glycaemic effects of dapagliflozin versus placebo in patients with type 2 diabetes on combination antihypertensive therapy: a randomised, double-blind, placebo-controlled, phase 3 study. Lancet Diabetes Endocrinol. (2016) 4:211–20. doi: 10.1016/S2213-8587(15)00417-9
47. Wan Seman WJ, Kori N, Rajoo S, Othman H, Mohd Noor N, Wahab NA, et al. Switching from sulphonylurea to a sodium-glucose cotransporter2 inhibitor in the fasting month of Ramadan is associated with a reduction in hypoglycaemia. Diabetes Obesity Metab. (2016) 18:628–32. doi: 10.1111/dom.12649
48. Weber MA, Mansfield TA, Alessi F, Iqbal N, Parikh S, Ptaszynska A. Effects of dapagliflozin on blood pressure in hypertensive diabetic patients on renin-angiotensin system blockade. Blood Press. (2016) 25:93–103. doi: 10.3109/08037051.2015.1116258
49. Fioretto P, Del Prato S, Buse JB, Goldenberg R, Giorgino F, Reyner D, et al. Efficacy and safety of dapagliflozin in patients with type 2 diabetes and moderate renal impairment (chronic kidney disease stage 3A): The DERIVE Study. Diabetes Obesity Metab. (2018) 20:2532–40. doi: 10.1111/dom.13413
50. Seino Y, Sasaki T, Fukatsu A, Imazeki H, Ochiai H, Sakai S. Efficacy and safety of luseogliflozin added to insulin therapy in Japanese patients with type 2 diabetes: a multicenter, 52-week, clinical study with a 16-week, double-blind period and a 36-week, open-label period. Curr Med Res Opin. (2018) 34:981–94. doi: 10.1080/03007995.2018.1441816
51. Terauchi Y, Tamura M, Senda M, Gunji R, Kaku K. Long-term safety and efficacy of tofogliflozin as add-on to insulin in patients with type 2 diabetes: results from a 52-week, multicentre, randomized, double-blind, open-label extension, Phase 4 study in Japan (J-STEP/INS). Diabetes Obesity Metab. (2018) 20:1176–85. doi: 10.1111/dom.13213
52. Yang W, Ma J, Li Y, Li Y, Zhou Z, Kim JH, et al. Dapagliflozin as add-on therapy in Asian patients with type 2 diabetes inadequately controlled on insulin with or without oral antihyperglycemic drugs: a randomized controlled trial. J Diabetes. (2018) 10:589–99. doi: 10.1111/1753-0407.12634
53. Allegretti AS, Zhang W, Zhou W, Thurber TK, Rigby SP, Bowman-Stroud C, et al. Safety and effectiveness of bexagliflozin in patients with type 2 diabetes mellitus and stage 3a/3b CKD. Am J Kidney Dis. (2019) 74:328–37. doi: 10.1053/j.ajkd.2019.03.417
54. Wiviott SD, Raz I, Bonaca MP, Mosenzon O, Kato ET, Cahn A, et al. Dapagliflozin and cardiovascular outcomes in type 2 diabetes. N Engl J Med. (2019) 380:347–57. doi: 10.1056/NEJMoa1812389
55. Mahaffey KW, Jardine MJ, Bompoint S, Cannon CP, Neal B, Heerspink HJL, et al. Canagliflozin and cardiovascular and renal outcomes in type 2 diabetes mellitus and chronic kidney disease in primary and secondary cardiovascular prevention groups. Circulation. (2019) 140:739–50. doi: 10.1161/CIRCULATIONAHA.119.042007
56. Pollock C, Stefansson B, Reyner D, Rossing P, Sjostrom CD, Wheeler DC, et al. Albuminuria-lowering effect of dapagliflozin alone and in combination with saxagliptin and effect of dapagliflozin and saxagliptin on glycaemic control in patients with type 2 diabetes and chronic kidney disease (DELIGHT): a randomised, double-blind, placebo-controlled trial. Lancet Diabetes Endocrinol. (2019) 7:429–41. doi: 10.1016/S2213-8587(19)30086-5
57. Inoue H, Morino K, Ugi S, Tanaka-Mizuno S, Fuse K, Miyazawa I, et al. Ipragliflozin, a sodium-glucose cotransporter 2 inhibitor, reduces bodyweight and fat mass, but not muscle mass, in Japanese type 2 diabetes patients treated with insulin: a randomized clinical trial. J Diabetes Investig. (2019) 10:1012–21. doi: 10.1111/jdi.12985
58. McMurray JJV, Solomon SD, Inzucchi SE, Kober L, Kosiborod MN, Martinez FA, et al. Dapagliflozin in patients with heart failure and reduced ejection fraction. N Engl J Med. (2019) 381:1995–2008.
59. Packer M, Anker SD, Butler J, Filippatos G, Pocock SJ, Carson P, et al. Cardiovascular and renal outcomes with empagliflozin in heart failure. N Engl J Med. (2020) 383:1413–24.
60. Lee MMY, Brooksbank KJM, Wetherall K, Mangion K, Roditi G, Campbell RT, et al. Effect of empagliflozin on left ventricular volumes in patients with type 2 diabetes, or prediabetes, and heart failure with reduced ejection fraction (SUGAR-DM-HF). Circulation. (2021) 143:516–25.
61. Bhatt DL, Szarek M, Steg PG, Cannon CP, Leiter LA, McGuire DK, et al. Sotagliflozin in patients with diabetes and recent worsening heart failure. N Engl J Med. (2021) 384:117–28. doi: 10.1056/NEJMoa2030183
62. Solomon SD, McMurray JJV, Claggett B, de Boer RA, DeMets D, Hernandez AF, et al. Dapagliflozin in heart failure with mildly reduced or preserved ejection fraction. N Engl J Med. (2022) 387:1089–98.
63. Neal B, Perkovic V, Mahaffey KW, de Zeeuw D, Fulcher G, Erondu N, et al. Canagliflozin and cardiovascular and renal events in Type 2 Diabetes. N Engl J Med. (2017) 377:644–57. doi: 10.1056/NEJMoa1611925
64. O’Meara E, McDonald M, Chan M, Ducharme A, Ezekowitz JA, Giannetti N, et al. CCS/CHFS heart failure guidelines: clinical trial update on functional mitral regurgitation, SGLT2 Inhibitors, ARNI in HFpEF, and tafamidis in amyloidosis. Can J Cardiol. (2020) 36:159–69. doi: 10.1016/j.cjca.2019.11.036
65. Packer M. Reconceptualization of the molecular mechanism by which sodium-glucose cotransporter 2 inhibitors reduce the risk of heart failure events. Circulation. (2019) 140:443–5. doi: 10.1161/CIRCULATIONAHA.119.040909
66. Verma S, McMurray JJV, Cherney DZI. The metabolodiuretic promise of sodium-dependent glucose cotransporter 2 inhibition: the search for the sweet spot in heart failure. JAMA Cardiol. (2017) 2:939–40. doi: 10.1001/jamacardio.2017.1891
67. Yang L, Zhang L, He H, Zhang M, An Z. Efficacy and safety of sodium-glucose cotransporter 2 inhibitors in East Asians with type 2 diabetes: a systematic review and meta-analysis. Diabetes Therapy. (2019) 10:1921–34. doi: 10.1007/s13300-019-0674-7
68. Johnsson K, Johnsson E, Mansfield TA, Yavin Y, Ptaszynska A, Parikh SJ. Osmotic diuresis with SGLT2 inhibition: analysis of events related to volume reduction in dapagliflozin clinical trials. Postgrad Med. (2016) 128:346–55. doi: 10.1080/00325481.2016.1153941
69. Mudaliar S, Polidori D, Zambrowicz B, Henry RR. Sodium-glucose cotransporter inhibitors: effects on renal and intestinal glucose transport: from bench to bedside. Diabetes Care. (2015) 38:2344–53. doi: 10.2337/dc15-0642
Keywords: sodium-glucose cotransporter-2 inhibitors, adverse event (AE), volume depletion, meta-analysis, RCTs, hypovolemia
Citation: Rong X, Zhu Y, Wen B, Liu K, Li X, Gou Q and Chen X (2022) Risk of hypovolemia associated with sodium–glucose cotransporter-2 inhibitors treatment: A meta-analysis of randomized controlled trials. Front. Cardiovasc. Med. 9:973129. doi: 10.3389/fcvm.2022.973129
Received: 19 June 2022; Accepted: 26 October 2022;
Published: 14 November 2022.
Edited by:
Matteo Pagnesi, ASST Spedali Civili di Brescia, ItalyReviewed by:
Emanuele Bobbio, Sahlgrenska University Hospital, SwedenVincenzo Nuzzi, University of Trieste, Italy
Copyright © 2022 Rong, Zhu, Wen, Liu, Li, Gou and Chen. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Kai Liu, Mjk3MzAwMDU4QHFxLmNvbQ==; Xiaoping Chen, eGlhb3BpbmdjaGVuMTFAMTI2LmNvbQ==
†These authors have contributed equally to this work and share first authorship