
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Cardiovasc. Med. , 03 November 2022
Sec. Atherosclerosis and Vascular Medicine
Volume 9 - 2022 | https://doi.org/10.3389/fcvm.2022.945421
 Esmeralda Castelblanco1,2†
Esmeralda Castelblanco1,2† Minerva Granado-Casas3,4†Marta Hernández5,6Montserrat Pinyol7Eudald Correig8
Minerva Granado-Casas3,4†Marta Hernández5,6Montserrat Pinyol7Eudald Correig8 Josep Julve3,4Marina Idalia Rojo-López4Núria Alonso3,9
Josep Julve3,4Marina Idalia Rojo-López4Núria Alonso3,9 Angelo Avogaro10Emilio Ortega11,12,13*
Angelo Avogaro10Emilio Ortega11,12,13* Didac Mauricio3,4,14*
Didac Mauricio3,4,14*Background: Diabetic retinopathy (DR) and preclinical atherosclerosis are associated with higher cardiovascular risk. However, no studies have investigated the predictive role of DR and preclinical atherosclerosis jointly on cardiovascular events in subjects with type 2 diabetes (T2D). We aimed to assess the contribution of DR and subclinical atherosclerosis on the risk of adverse cardiovascular events in subjects with T2D without previous cardiovascular disease (CVD).
Methods: We included two prospective cohorts of subjects with T2D from the same geographical area. Assessment of subclinical atherosclerosis was performed by carotid ultrasound. An ophthalmologist classified DR according to standard criteria. Cardiovascular outcomes considered for analysis were the following: ischemic heart disease, stroke, heart failure, peripheral artery disease, revascularization procedures, and cardiovascular mortality. Bivariable and multivariable predictive models were performed.
Results: From a total of 374 subjects with T2D 44 developed cardiovascular events during the 7.1 years of follow-up. Diabetes duration, total cholesterol, and glycated hemoglobin (HbA1c) at baseline were higher in subjects who developed cardiovascular outcomes (p < 0.001, p = 0.026, and p = 0.040, respectively). Compared with subjects without events, those developing cardiovascular events had higher prevalence of retinopathy (65.9% vs. 38.8%, p = 0.001; respectively) and more than mild retinopathy (43.2% vs. 31.8%, p = 0.002; respectively). Furthermore, all-cause mortality was higher in subjects with MACE than those without events (13.6% vs. 3.3%, p = 0.009; respectively). The multivariable analyses showed that HbA1c and the presence of DR at baseline were predictive of cardiovascular outcomes (p = 0.045 and p = 0.023, respectively). However, the burden of subclinical atherosclerosis was not (p = 0.783 and p = 0.071, respectively).
Conclusion: DR is a strong predictor of cardiovascular events in T2D individuals at primary CVD prevention, even after accounting for the presence of preclinical carotid atherosclerosis. These results may help to individualize CVD prevention strategies in T2D.
Type 2 diabetes mellitus is associated with a higher risk of cardiovascular disease (CVD) (1). The most common clinical expression of CVD is coronary heart disease, cerebrovascular disease, peripheral artery disease, and congestive heart failure (2). These are often manifested as major adverse cardiovascular events with hospitalizations, procedures, and deaths derived from acute coronary syndromes, myocardial infarction, and stroke, as well as sudden death (1, 2). According to the American Diabetes Association (ADA), diabetic retinopathy (DR) is the most common microvascular and neurovascular complication (3). DR is an independent predictor of subclinical CVD in type 2 diabetes (T2D) (4). Furthermore, DR is associated with CVD in patients with T2D (5). Similarly, subclinical atherosclerosis is an independent predictor of cardiovascular events and death in subjects with type 2 diabetes (6, 7). Besides, DR alone or in combination with other microvascular complications has been independently associated with the presence of carotid atherosclerosis in this population (8–10).
A significant number of studies were performed to assess the relative risk of CVD with the presence of DR in subjects with diabetes (11–29). Retrospective studies conducted with large T2D samples found that the CVD risk increases with the cumulative burden of microvascular complications, i.e., DR, diabetic nephropathy, and neuropathy (11, 13). Furthermore, a recent prospective study determined that incident myocardial infarction and stroke events were associated with the presence and severity of DR in this population (12). The World Health Organization (WHO) multinational study group reported that DR is positively associated with cardiovascular mortality and incident myocardial infarction in individuals with T2D (22). Moreover, other studies found that subjects with T2D with a mild or moderate DR had a higher risk of coronary heart disease, stroke, and any CVD (17, 18, 26, 27). A meta-analysis of observational studies found a higher risk of heart failure and stroke in individuals with DR (16). In addition, a prospective study performed with individuals with T2D found that DR was a predictor of cardiovascular events independently of classical risk factors (21). Moreover, a recent retrospective cohort study performed with Catalan population found that DR was associated with coronary heart disease, cardiovascular events, and all-cause mortality among subjects with T2D (20).
Furthermore, a recent meta-analysis reported that DR increases the risk of cardiovascular death in patients with diabetes (30). However, a post hoc analysis from a randomized clinical trial did not show any association between DR and increased risk of recurrent cardiovascular events in subjects with T2D (14). Nevertheless, other post hoc analyses from two cardiovascular outcome clinical trials found an increased risk of CVD associated with microvascular complications (15).
On the other hand, subclinical atherosclerosis has been associated with a higher risk of CVD in subjects with T2D (6, 7, 31, 32). Specifically, carotid plaque calcification predicted cardiovascular events in T2D subjects with a low degree of stenosis (6). Furthermore, carotid plaques were predictors of cardiovascular morbidity in individuals with T2D without prior CVD (7). Moreover, the presence of carotid plaques was more predictive for prevalent silent coronary atherosclerosis, severity, and extent in asymptomatic T2D individuals (31); besides, intima-media thickness (IMT) and carotid plaques were independent predictors of CVD (32). However, the role of subclinical atherosclerosis in CVD risk assessment is still unclear (33).
To our knowledge, there are no reports investigating together in the same study the potential predictor role of DR and subclinical atherosclerosis on the development of cardiovascular events in subjects with T2D. We hypothesized that as the presence of subclinical atherosclerosis involves detecting the etiological process leading to atherosclerotic cardiovascular events, DR may contribute to further predicting CVD in type 2 diabetes. Therefore, we aimed to assess the predictive role of subclinical atherosclerosis and DR on the development of cardiovascular outcomes in subjects with T2D without prior CVD without chronic kidney disease.
Two cohorts of individuals with T2D from the same geographical area recruited in two previous studies were included (10, 34). These subjects were prospectively followed to determine incident cardiovascular events. The first cohort (Cohort 1) was previously selected to study the relationship between carotid atherosclerosis and diabetic retinopathy in T2D. From 312 subjects recruited in this cohort, we included 310 subjects with complete eye and carotid ultrasound assessments from this cohort. The characteristics of the individuals were detailed in a previous publication (10). Briefly, the inclusion criteria in this study were as follows: diagnosis of T2D; age from 40 to 75 years; absence of a prior history of CVD; absence of impaired renal function defined as a estimated glomerular filtration rate (eGFR) < 60 ml/min or macroalbuminuria; no previous history of diabetic foot disease; absence of major psychiatric disorders. The second cohort (Cohort 2) was recruited to investigate the frequency of preclinical carotid atherosclerosis (the DIABIMCAP Study) (34). From a cohort of 106 subjects with T2D included in the DIABIMCAP Study, a total sample of 64 subjects with eye and carotid ultrasound data were included in the current study. A detailed description of this cohort can be found elsewhere (34). The inclusion criteria were a diagnosis of T2D within the previous year; the absence of prior CVD, cancer, chronic renal or liver disease; history of alcohol or drug abuse; major psychiatric or chronic illness, and short life expectancy. Therefore, a final sample of 374 individuals with T2D was prospectively followed. Written informed consent was obtained from each patient included in the study. The study protocol conforms to the ethical guidelines of the 1975 Declaration of Helsinki, and the study has been priorly approved by both Institution’s ethics committees on research on humans.
A description of the procedures to collect clinical variables of the two cohorts has been previously published (10, 34). Age, sex, tobacco exposure (current or former smoking), systolic blood pressure (sBP), diastolic blood pressure (dBP), and diabetes duration were collected. Hypertension and dyslipidemia were defined as active treatment with antihypertensive and lipid-lowering agents, respectively. Weight, height, waist, and blood pressure were measured by standard procedures. Blood and urine samples were collected in the fasting state to obtain biochemical parameters using standardized methods. The estimated glomerular filtration rate (eGFR) was calculated using The Modification of Diet in Renal Disease (MDRD-4) formula (35). A thorough revision of the medical records, including all the available information from the health system was performed to identify death and its causes and cardiovascular events during the follow-up period; these included ischemic heart disease (including any recorded diagnosis of any form of ischemic heart disease, and angina pectoris), stroke, heart failure, peripheral artery disease, procedures of revascularization, and cardiovascular mortality. The cardiovascular events were only confirmed when the treating physician had recorded a new diagnosis corresponding to that given event after hospital admission or, alternatively, in the outpatient medical records.
The study participants underwent a complete baseline examination by an ophthalmologist. According to the international consensus on DR (36), DR was assessed with a multifield stereoscopic retinal photography. Moreover, this was classified as follows: (a) no DR; (b) mild non-proliferative DR if only microaneurysms were observed; (c) moderate non-proliferative DR if more than just microaneurysms but less than severe non-proliferative DR were detected; (d) severe non-proliferative DR if any of the following characteristics were observed: over 20 intraretinal hemorrhages in each of 4 quadrants, definite venous beading in 2 + quadrants, prominent intraretinal microvascular abnormalities in 1 + quadrant, as well as no signs of proliferative DR; and (e) proliferative DR if neovascularization and/or vitreous/preretinal hemorrhage was detected (10, 34).
All the study subjects underwent the same carotid ultrasound imaging protocol. Bilateral carotid artery B-mode ultrasound imaging to assess IMT and the presence of atherosclerotic plaques was performed following the standardized protocol (10, 34). A semiautomatic software measured IMTs of the common carotid artery (CCA), bulb, and internal carotid artery (ICA). IMT-mean and IMT-maximum from each carotid segment were collected. Atherosclerotic plaques were assessed by using B-mode and color Doppler; these were defined as a focal wall thickening encroaching into the arterial lumen by at least 50% of the surrounding IMT value or with a thickness of 1.5 mm at minimum measuring from the media adventitia interference to the intima-lumen surface, following the Mannheim consensus (37).
Continuous variables were tested for normality using the Shapiro–Wilk test. Data are presented as median and 25th and 75th percentiles for continuous variables with a non-normal distribution or the mean and standard deviation (SDs) for variables with a normal distribution. Categorical variables are reported as percentages. Differences between groups were analyzed using the non-parametric Mann–Whitney U-test, Welch’s parametric t-test for continuous variables, and the chi-square test or Fisher’s exact test for categorical variables. All continuous variables were standardized and normalized whether necessary.
We included subjects with T2D from two different cohorts in the current study. As these patients harbor a different baseline risk, we could not perform Kaplan-Meier and Cox regressions, as they are not appropriate to estimate the survival function in this setting. Therefore, we carried out a series of multivariate predictive models to assess the relationship between prevalent plaque and retinopathy and the cardiovascular outcome. As for the exposure, we divided plaque into Yes (1 or more plaques) and No, or as Multiple plaques (two or more) or Advanced atherosclerosis (three or more plaques). Moreover, DR was classified into either Yes or No, or into No or Mild vs. Severe. For each set of models, we took a dual approach to assess the effect of the predictive variables on the target variable. Random forests prove to be more accurate models for such complex scenarios (38) and, as an added advantage, allowed us to assess the relative importance of each variable via out-of-bag accuracy. However, the downside is that random forests do not allow to evaluate whether each variable has a protective or harmful effect. For this reason, we used the result of the regularized regression through which we can evaluate the direction of the effect through the negativity or positivity of the coefficient. Furthermore, in the logistic regression models, we imposed a highly constrained regularization that forces model coefficients to be as small as possible, sometimes even 0. Therefore, if two variables were closely associated with each other, the model removes the effect of the least important one. In the random forests, we constrained the ability of the trees to generate branches, thus reducing the effect of colinear variables. In both cases, the models identified the variable of interest as the most important one in explaining the outcome. Furthermore, in the logistic regression models, we imposed a highly constrained regularization that forces model coefficients to be as small as possible, sometimes even 0. Therefore, if two variables were closely associated with each other, the model removes the effect of the least important one. In the random forests, we constrained the ability of the trees to generate branches, thus reducing the effect of colinear variables. In both cases, the models identified the variable of interest as the most contributing one in explaining the outcome. We provide odds ratios for the logistic regressions and estimates for the linear regressions, both with 95% confidence intervals and p-values.
Finally, to study further the etiology of our study, we also built a Bayesian Network among the variables using the PC algorithm (39). This algorithm is able to compute causal relationships between variables. This network provides a graphical representation of the conditional independence relationships among all the variables, allowing us to infer causal relationships between predictor and predicted variables.
All statistical analyses were performed using the R software package version 4.0 (40).
Clinical characteristics of the study subjects are shown in Table 1. After a median (SD) follow-up of 7.1 (1.0) years, among the 374 participants, 46 reported cardiovascular events. This represents a 1.2% annual rate of cardiovascular events in this primary prevention cohort. Subjects who reported cardiovascular outcomes had a longer diabetes duration (p < 0.001), higher total cholesterol (p = 0.030), and glycated hemoglobin (HbA1c) (p = 0.023) in comparison with those who remained free of cardiovascular events at the end of the follow-up. Furthermore, they had also a higher prevalence of DR (67.4% vs. 38.4%, p = 0.001; respectively) and DR severity (45.7% vs. 21.3%, p < 0.001; respectively). In addition, mortality was higher in the group with cardiovascular events (17.4% vs. 2.7%, p < 0.001; respectively). The description of the study sample according to the presence of atherosclerotic plaques and DR is shown in Supplementary Table 1. Those participants with plaque(s) were older (p < 0.001), had higher sBP (p = 0.010) and higher frequency of hypertension (p = 0.034), tobacco exposure (p < 0.001) compared with individuals without atherosclerosis. On the other hand, individuals with DR had a higher frequency of hypertension (p = 0.007), atherosclerotic plaques (p = 0.014), deaths (p = 0.028), cardiovascular mortality (p = 0.030), and cardiovascular events (p = 0.001) in comparison with the non-DR group. Moreover, they had higher waist (p = 0.003), diabetes duration (p < 0.001), sBP (p < 0.001), HDL-cholesterol (p = 0.021), and albumin/creatinine ratio (p < 0.001). The clinical characteristics of both study cohorts are shown in Supplementary Table 2. Participants from Cohort 1 were older (p = 0.030) and had a lower frequency of tobacco exposure (p < 0.001) in comparison with those from Cohort 2. Furthermore, these participants had a higher diabetes duration (p < 0.001), sBP (p = 0.032), HbA1c (p < 0.001), eGFR (p < 0.001), and a higher frequency and severity of DR (p < 0.001). However, they showed lower dBP (p < 0.001), total cholesterol (p = 0.007), LDL-cholesterol (p = 0.003), and presence of subclinical carotid atherosclerosis (p < 0.001) compared with Cohort 2.
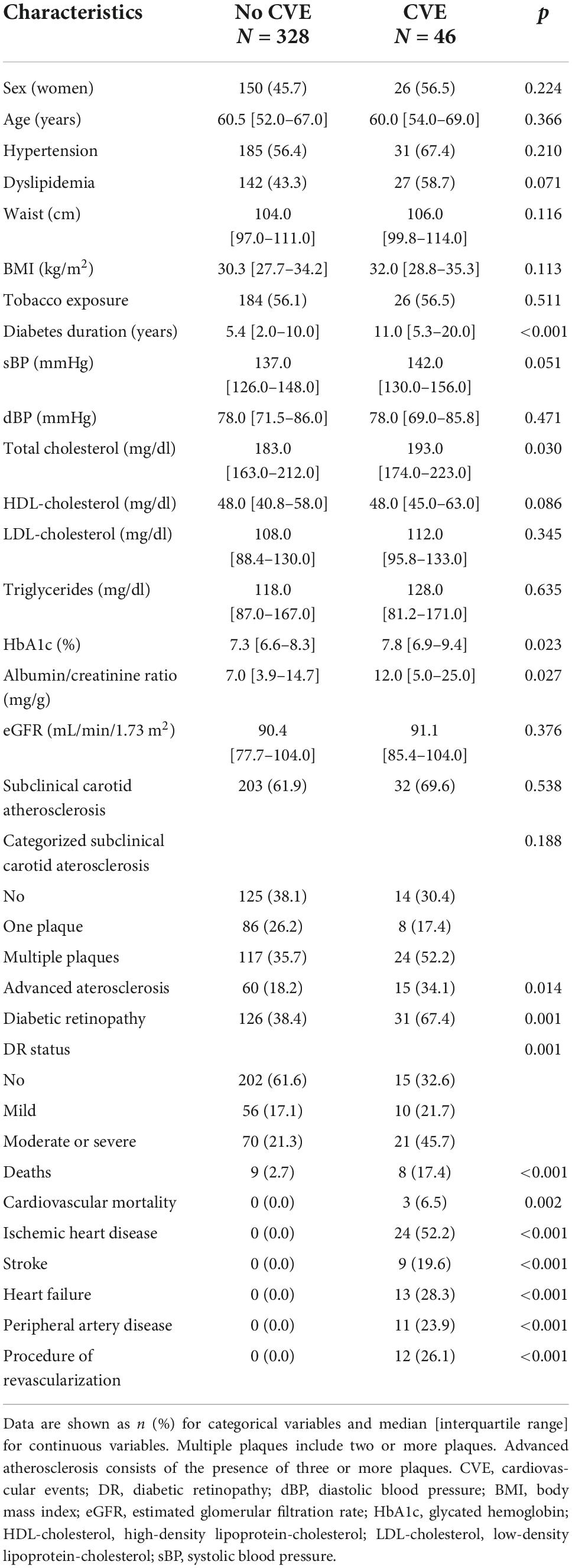
Table 1. Clinical characteristics of the study group according to incident cardiovascular events.
The multivariate predictive model for cardiovascular events showed that both HbA1c (1% change) and the presence of DR were predictors of cardiovascular events [OR 1.09, 95% CI (1.00–1.18), p = 0.045 and OR 1.27, 95% CI (1.06–1.52), p = 0.023; respectively] after accounting for confounders (Table 2). However, the presence of subclinical carotid atherosclerotic plaques was not associated with cardiovascular events [OR 1.06, 95% CI (0.90–1.25), p = 0.833]. In the relative variable importance of this model, HbA1c and DR had a higher mean decrease accuracy being the two most important variables of this model (Figure 1).
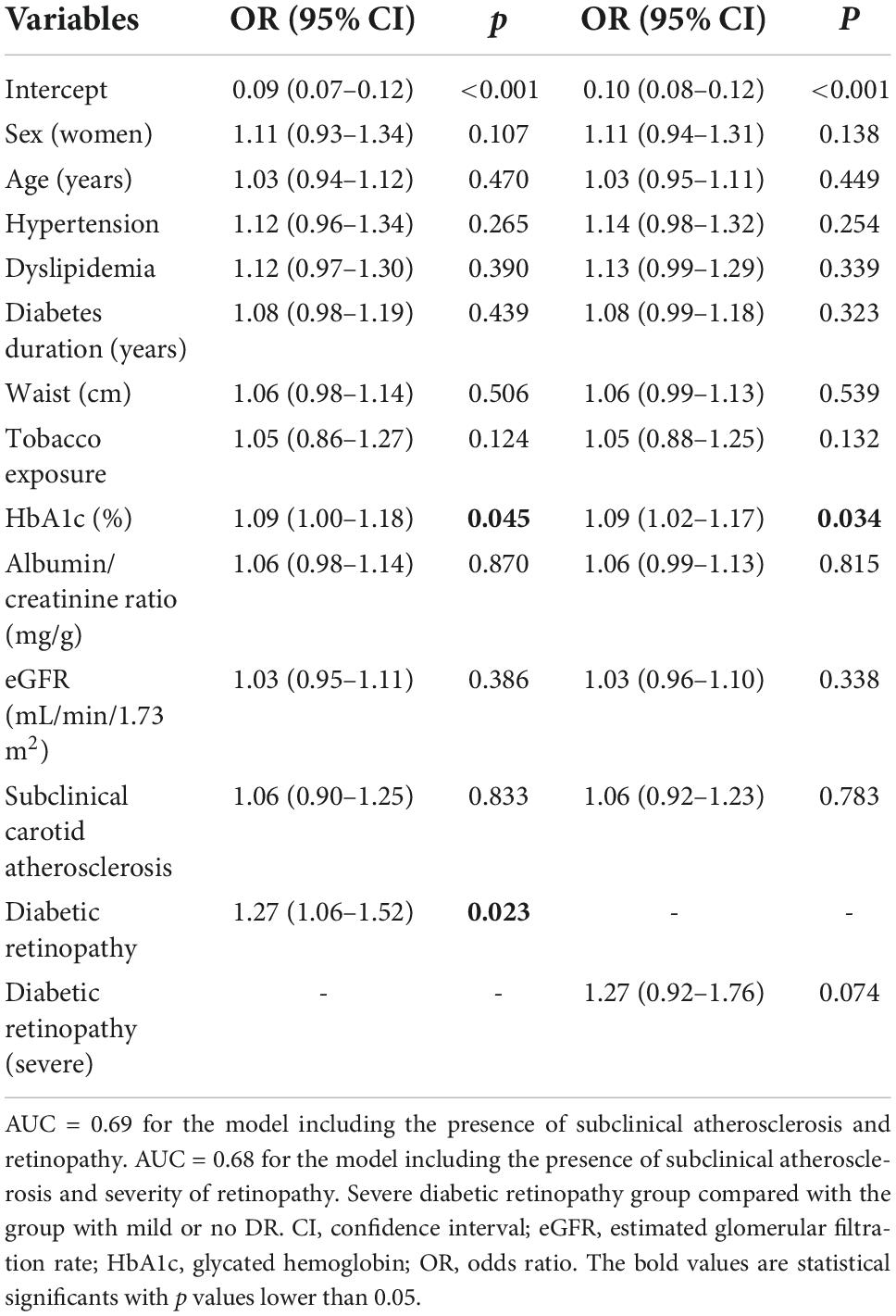
Table 2. Regularized logistic regression models for the association between the different variables, including plaque and diabetic retinopathy, and incident major adverse cardiovascular events.
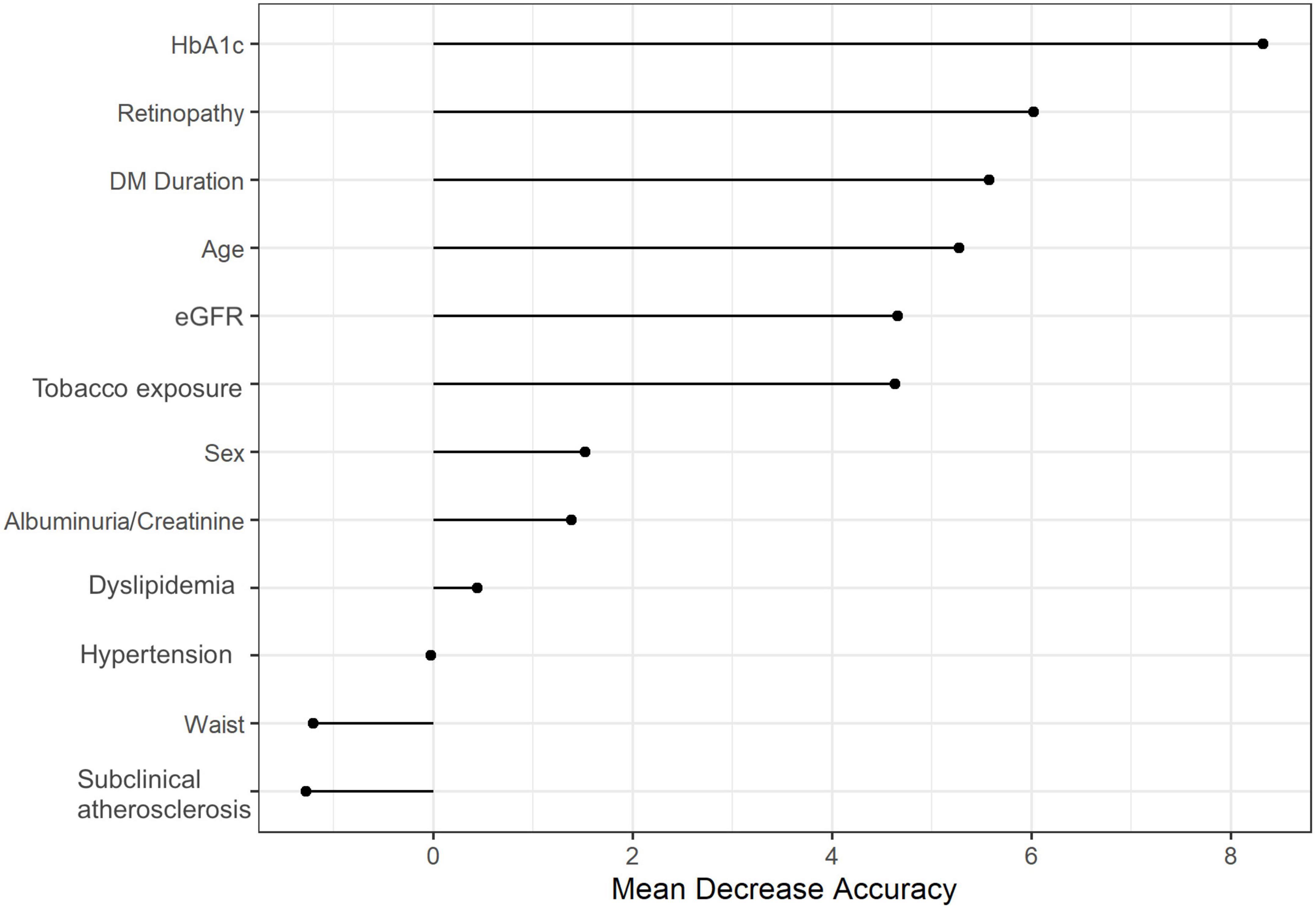
Figure 1. Random forest of the relative importance of each variable in the multivariate model for the association between the presence of atherosclerotic plaque and diabetic retinopathy with cardiovascular events. HbA1c, glycated hemoglobin; DM_duration, diabetes mellitus duration; Plaque, presence of carotid plaques; eGFR, estimated glomerular filtration rate.
On the other hand, when considering in this model a more advanced definition of DR, preclinical atherosclerosis did not have a predictive role in the development of cardiovascular events either [OR 1.06, 95% CI (0.92–1.23); p = 0.783] (Table 2). In this case, severe DR was not significantly associated with cardiovascular events [OR 1.27, 95% CI (0.92–1.76); p = 0.074]. Besides, diabetes duration and HbA1c had a decisive role in this multivariate prediction model, as shown in Figure 2. Nevertheless, HbA1c had a risk association of cardiovascular events [OR 1.09, 95% CI (1.02–1.17), p = 0.034]. Furthermore, the presence of DR or advanced atherosclerosis (three or greater plaques) were not predictive factors of cardiovascular events [OR 1.41 95% CI (1.12–1.77); p = 0.091, and OR 1.44 (1.16–1.78); p = 0.071, respectively] in multivariate models (Supplementary Table 3).
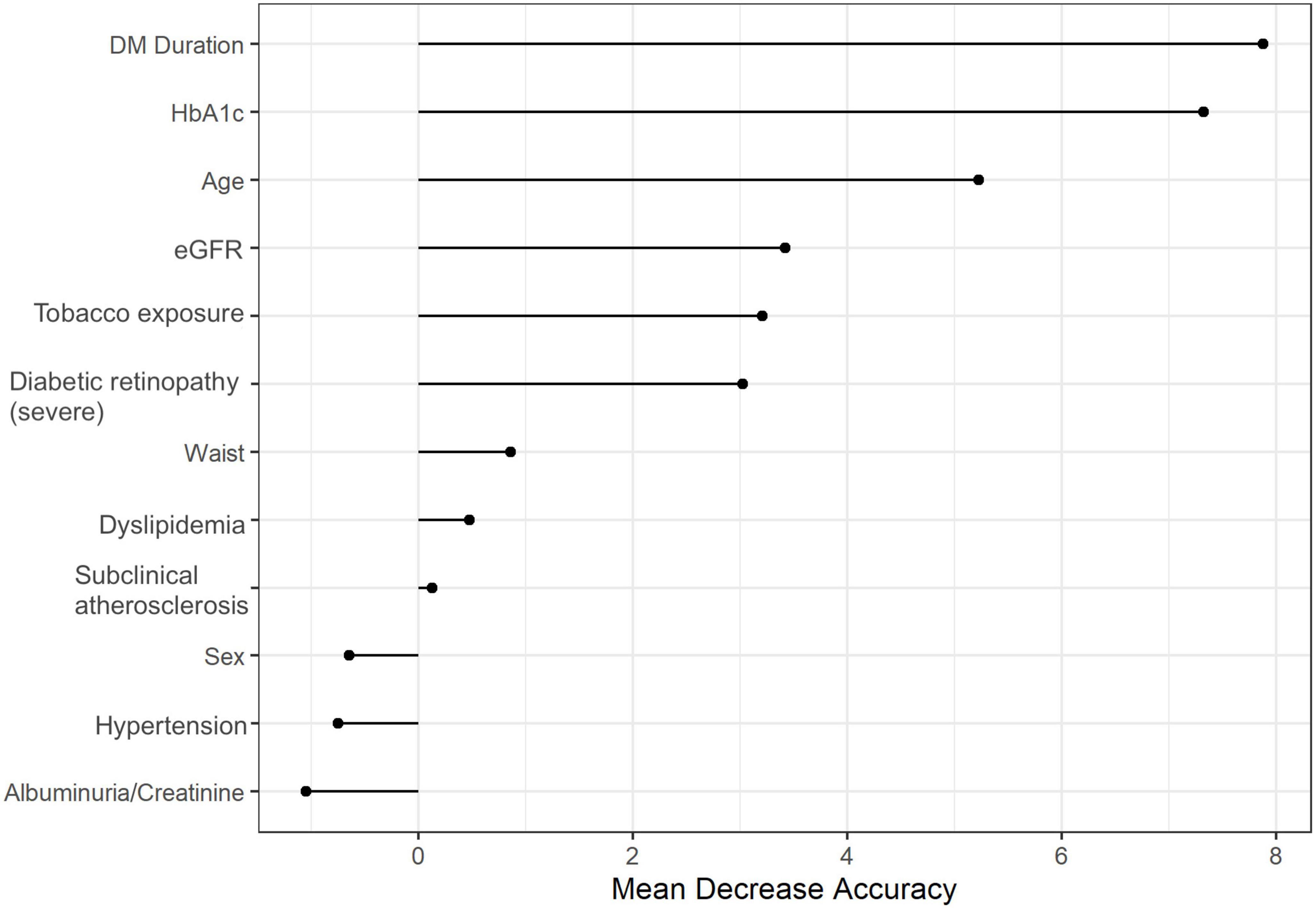
Figure 2. Random forest of the relative importance of each variable in the multivariate predictive model for the association between severe diabetic retinopathy and the presence of subclinical atherosclerosis with cardiovascular events. DM_duration, diabetes mellitus duration; eGFR, estimated glomerular filtration rate; Plaque, presence of carotid plaques. Diabetic retinopathy severe, reference group: no or mild diabetic retinopathy.
The prediction causation algorithm to explore the causal relationship between DR, subclinical carotid atherosclerosis and cardiovascular outcomes showed that severe DR had a causal solid connection for the development of cardiovascular events (Figure 3). Subclinical atherosclerosis was not related to cardiovascular events in our study sample. Nevertheless, female sex, obesity, and tobacco exposure were associated with the development of severe atherosclerosis, defined as the presence of three or more plaques. In addition, all-cause mortality was not associated with any of the other clinical variables even though, as expected, classical cardiovascular risk factors were related to the increasing albumin/creatinine ratio and, consequently, the presence of severe DR.
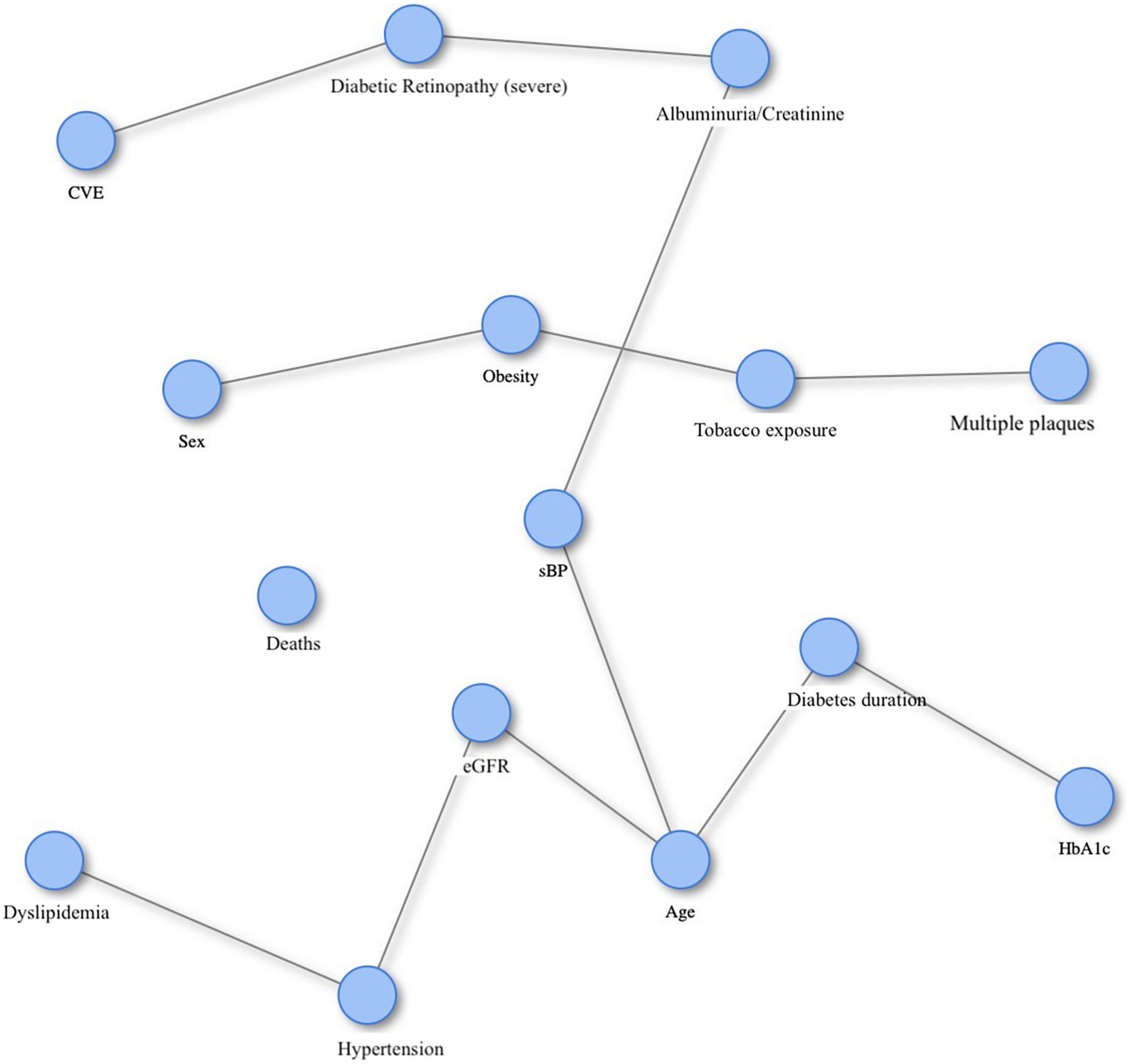
Figure 3. The prediction causation algorithm for the causal relationship between diabetic retinopathy, subclinical atherosclerosis and cardiovascular events in subjects with type 2 diabetes. CVE, cardiovascular events; Multiple plaques, multiple carotid plaques (two or more); sBP, systolic blood pressure; eGFR, estimated glomerular filtration rate; DM_duration, diabetes mellitus duration; HbA1c, glycated hemoglobin.
This is the first study that assessed the independent predictive role of DR and subclinical atherosclerosis in developing cardiovascular events in T2D individuals without a history of the previous CVD at baseline and established chronic kidney disease. Our findings showed that HbA1c and DR, but not preclinical atherosclerosis, were predictors of cardiovascular events considering the presence of subclinical atherosclerosis.
The presence of DR and a poorer glycemic control were associated with a higher risk of developing a cardiovascular event in subjects with T2D, adjusting for classical risk factors and considering the presence and burden of subclinical atherosclerosis; this is in line with previous studies (20, 21). The burden of microvascular complications such as DR, nephropathy, and neuropathy was associated with a cumulative risk of cardiovascular death, non-fatal myocardial infarction, or non-fatal ischemic stroke in subjects with T2D (11). Furthermore, microvascular complications were independently related to the 10-year risk of death and cardiovascular events in individuals with T2D (13). A recent systematic review reported that DR is a strong predictor of stroke and CVD, suggesting that patients with DR have an overall worse prognosis than those without this condition (5). On the other hand, a post hoc analysis from a clinical trial did not find any association between DR or neuropathy with cardiovascular death, non-fatal myocardial infarction, stroke, hospitalization for unstable angina, and recent acute coronary syndrome (14). Nevertheless, the authors identified the diabetes duration as an independent predictor of cardiovascular events beyond DR, neuropathy, and cardiovascular risk factors, which is in line with our findings on the importance of the disease duration in the predictive models. In addition, the WHO study researchers found that diabetes duration and glycemic control predicted incident fatal and non-fatal myocardial infarction in subjects with diabetes (22). Therefore, the role of DR, glycemic control, and diabetes duration in predicting cardiovascular events should be considered in this population. The potential relationship between DR and subclinical atherosclerosis has been published in previous studies (8–10, 41); additionally, the American Heart Association (AHA) and the European Society of Cardiology (ESC) included DR as an independent risk factor to predict cardiovascular events in patients treated in primary prevention (42, 43).
On the other hand, subclinical atherosclerosis did not predict a higher risk of developing cardiovascular events in subjects with T2D; however, the high prevalence (63%) of patients with subclinical atherosclerosis in our study sample may be a limitation to assess its predictive role, as well as that of other highly prevalent classical risk factors such as age, dyslipidemia, and hypertension. The presence of atherosclerotic plaques predicts future cardiovascular events and mortality in patients with T2D (6, 7), a finding that is in contrast with our results. However, participants in previously published studies had other late diabetic complications, such as nephropathy, that could strongly influence the outcome. Individuals with a higher burden of plaques have a higher incidence of renal endpoints (7); moreover, carotid plaques are predictors of renal outcomes in subjects with T2D. Nevertheless, microvascular complications and subclinical atherosclerosis may be closely linked in their respective pathogenetic pathways (19). Our findings identify DR as a causal predicting factor in developing a cardiovascular events in the prediction causation algorithm; however, this cannot be definitively established because microangiopathy and carotid atherosclerosis are closely linked (8).
One of the limitations of our study is that we used two different cohorts to establish the predictive role of DR and subclinical atherosclerosis in the development of cardiovascular events. However, regularized logistic regression models were performed to calculate the study participants’ risk. Although the causal relationships between cardiovascular events and predictors were calculated using a Bayesian method, we cannot conclude this causal relationship due to the study design. Moreover, definitive conclusions cannot be established due to the rather insufficient number of incident cardiovascular events and the short follow-up study period of the participants; for this reason, the burden of subclinical atherosclerosis and severe DR, as well as the other classical risk factors such as age, dyslipidemia, and hypertension did not have either a significant association with cardiovascular events. Moreover, classical risk factors such as hypertension and dyslipidemia could be associated with each other which could influence the results. Furthermore, any association of cardiovascular events with HbA1c and DR would have not been found if the traditional definition of major adverse cardiovascular events (MACE, i.e., non-fatal myocardial infarction, non-fatal stroke and cardiovascular death) were used as the total number of events would have been even lower. In addition, data from study subjects on their dietary pattern, physical activity and alcohol consumption were not available. Therefore, their potential contribution of these factors to the main outcome of the study could not be included in the models. On the other hand, this is the first prospective study that analyzed the predictive role of DR and subclinical atherosclerosis on the cardiovascular events. Therefore, these results may be highly relevant for the design of further studies focused on this issue. Furthermore, this study included a well-defined sample including participants without other diabetic complications and no history of previous CVD, allowing us specifically assessing the predictive role of DR and subclinical atherosclerosis.
In conclusion, the presence of DR was a strong predictor of CVD independently from the presence of subclinical carotid atherosclerosis in subjects with T2D without previous clinical CVD. Our findings point to a solid linkage between DR and future CVD in T2D, which aligns with the published studies and guidelines in this issue. However, more extensive studies are needed to confirm the current findings.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
The studies involving human participants were reviewed and approved by the University Hospital Arnau de Vilanova, Lleida, Spain (CEIC 7/2011) and University Hospital Clinic de Barcelona, Barcelona, Spain (CEIC 2011/6466). The patients/participants provided their written informed consent to participate in this study.
EC, MG-C, EO, and DM contributed to the conception and design of the study. EC, MG-C, MH, MP, JJ, MR-L, and NA conducted the study. ECo analyzed the data. EC, MG-C, AA, EO, and DM interpreted the results. EC and MG-C wrote the manuscript. EO and DM were guarantors of this work and as such had full access to all the data in the study and take full responsibility for the integrity of the data, and the accuracy of the data analysis. All authors have revised the manuscript critically for important intellectual content and given final approval of the version to be published.
This study was supported by grants PS09/01035 and PI11/01723 from the Instituto de Salud Carlos III, Ministry of Economy and Competitiveness and FEDER, Spain. CIBER for Diabetes and Associated Metabolic Diseases (CIBERDEM) and CIBEROBN were initiatives of Instituto de Salud Carlos III, Spain. MR-L held a predoctoral fellowship from the Departament de Salut, SLT017/20/000107. JJ was recipient of a Miguel Servet Type 2 contract (CPII18/00004; ISCIII). JJ was member of Red de Investigación en “Enfermedades Metabólicas y Cáncer” (RED2018-102799-T), Ministerio de Economía y Competitividad (MINECO), Madrid, Spain. Institut de Recerca del Hospital de la Santa Creu i Sant Pau and Biomedical Research Institute’s Dr. Pifarré Foundation from Lleida (IRBLleida) were accredited by the Generalitat de Catalunya as Centre de Recerca de Catalunya (CERCA).
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fcvm.2022.945421/full#supplementary-material
1. Viigimaa M, Sachinidis A, Toumpourleka M, Koutsampasopoulos K, Alliksoo S, Titma T. Macrovascular complications of type 2 diabetes mellitus. Curr Vasc Pharmacol. (2019) 18:110–6. doi: 10.2174/1570161117666190405165151
2. International Diabetes Federation. IDF Atlas 9th Edition and Other Resources (2019). Available online at: https://diabetesatlas.org/en/resources/ (accessed on Sep 21, 2021).
3. Solomon S, Chew E, Duh E, Sobrin L, Sun J, VanderBeek B, et al. Diabetic retinopathy: a position statement by the American diabetes association. Diabetes Care. (2017) 40:412–8. doi: 10.2337/DC16-2641
4. Simó R, Bañeras J, Hernández C, Rodríguez-Palomares J, Valente F, Gutierrez L, et al. Diabetic retinopathy as an independent predictor of subclinical cardiovascular disease: baseline results of the precised study. BMJ Open Diabetes Res Care. (2019) 7:e000845. doi: 10.1136/bmjdrc-2019-000845
5. Pearce I, Simó R, Lövestam-Adrian M, Wong DT, Evans M. Association between diabetic eye disease and other complications of diabetes: implications for care. a systematic review. Diabetes Obes Metab. (2019) 21:467–78. doi: 10.1111/dom.13550
6. De Kreutzenberg SV, Fadini GP, Guzzinati S, Mazzucato M, Volpi A, Coracina A, et al. Carotid plaque calcification predicts future cardiovascular events in type 2 diabetes. Diabetes Care. (2015) 38:1937–44. doi: 10.2337/dc15-0327
7. Cardoso CRL, Salles GC, Leite NC, Salles GF. Prognostic impact of carotid intima-media thickness and carotid plaques on the development of micro- and macrovascular complications in individuals with type 2 diabetes: the Rio de Janeiro type 2 diabetes cohort study. Cardiovasc Diabetol. (2019) 18:2. doi: 10.1186/s12933-019-0809-1
8. Vigili de Kreutzenberg S, Coracina A, Volpi A, Fadini GP, Frigo AC, Guarneri G, et al. Microangiopathy is independently associated with presence, severity and composition of carotid atherosclerosis in type 2 diabetes. Nutr Metab Cardiovasc Dis. (2011) 21:286–93. doi: 10.1016/j.numecd.2009.10.003
9. Zhang C, Wang S, Li M, Wu Y. Association between atherosclerosis and diabetic retinopathy in chinese patients with type 2 diabetes mellitus. Diabetes Metab Syndr Obes Targets Ther. (2020) 13:1911–20. doi: 10.2147/DMSO.S246497
10. Alonso N, Traveset A, Rubinat E, Ortega E, Alcubierre N, Sanahuja J, et al. Type 2 diabetes-associated carotid plaque burden is increased in patients with retinopathy compared to those without retinopathy. Cardiovasc Diabetol. (2015) 14:33. doi: 10.1186/s12933-015-0196-1
11. Brownrigg JRW, Hughes CO, Burleigh D, Karthikesalingam A, Patterson BO, Holt PJ, et al. Microvascular disease and risk of cardiovascular events among individuals with type 2 diabetes: a population-level cohort study. Lancet Diabetes Endocrinol. (2016) 4:588–97. doi: 10.1016/S2213-8587(16)30057-2
12. Drinkwater JJ, Davis TME, Hellbusch V, Turner AW, Bruce DG, Davis WA. Retinopathy predicts stroke but not myocardial infarction in type 2 diabetes: the fremantle diabetes study phase II. Cardiovasc Diabetol. (2020) 19:43. doi: 10.1186/s12933-020-01018-3
13. Mohammedi K, Woodward M, Marre M, Colagiuri S, Cooper M, Harrap S, et al. Comparative effects of microvascular and macrovascular disease on the risk of major outcomes in patients with type 2 diabetes. Cardiovasc Diabetol. (2017) 16:95. doi: 10.1186/s12933-017-0574-y
14. Seferovic JP, Bentley-Lewis R, Claggett B, Diaz R, Gerstein HC, Køber LV, et al. Retinopathy, neuropathy, and subsequent cardiovascular events in patients with type 2 diabetes and acute coronary syndrome in the elixa: the importance of disease duration. J Diabetes Res. (2018) 2018:1631263. doi: 10.1155/2018/1631263
15. Verma S, Bain SC, Honoré JB, Mann JFE, Nauck MA, Pratley RE, et al. Impact of microvascular disease on cardiovascular outcomes in type 2 diabetes: results from the leader and sustain 6 clinical trials. Diabetes, Obes Metab. (2020) 22:2193–8. doi: 10.1111/dom.14140
16. Zhu XR, Zhang YP, Bai L, Zhang XL, Zhou JB, Yang JK. Prediction of risk of diabetic retinopathy for all-cause mortality, stroke and heart failure evidence from epidemiological observational studies. Medicine. (2017) 96:e5894. doi: 10.1097/MD.0000000000005894
17. Yamada T, Itoi T, Kiuchi Y, Nemoto M, Yamashita S. Proliferative diabetic retinopathy is a predictor of coronary artery disease in Japanese patients with type 2 diabetes. Diabetes Res Clin Pract. (2012) 96:e4–6. doi: 10.1016/j.diabres.2011.12.007
18. Zhou JB, Zhu XR, Zhao W, Yin L, Li HB, Qi L, et al. Prediction of proliferative diabetic retinopathy to asymptomatic obstructive coronary artery disease in chinese type 2 diabetes individuals: an exploratory study. Metab Syndr Relat Disord. (2019) 17:367–73. doi: 10.1089/met.2018.0140
19. Barlovic DP, Harjutsalo V, Groop PH. The association of severe diabetic retinopathy with cardiovascular outcomes in long-standing type 1 diabetes: a longitudinal follow-up. Diabetes Care. (2019) 42:E49–50. doi: 10.2337/dci18-0058
20. Barrot J, Real J, Vlacho B, Romero-Aroca P, Simó R, Mauricio D, et al. Diabetic retinopathy as a predictor of cardiovascular morbidity and mortality in subjects with type 2 diabetes. Front Med. (2022) 9:945245. doi: 10.3389/fmed.2022.945245
21. Planas A, Simó-Servat O, Hernández C, Ortiz-Zúñiga Á, Marsal JR, Herance JR, et al. Diabetic retinopathy and skin tissue advanced glycation end products are biomarkers of cardiovascular events in type 2 diabetic patients. J Pers Med. (2021) 11:1344. doi: 10.3390/JPM11121344
22. Fuller JH, Stevens LK, Wang S-L, Fuller J. Risk factors for cardiovascular mortality and morbidity: the WHO multinational study of vascular disease in diabetes. Diabetologia. (2001) 44(Suppl 2.):S54–64.
23. Garofolo M, Gualdani E, Giannarelli R, Aragona M, Campi F, Lucchesi D, et al. Microvascular complications burden (nephropathy, retinopathy and peripheral polyneuropathy) affects risk of major vascular events and all-cause mortality in type 1 diabetes: a 10-year follow-up study. Cardiovasc Diabetol. (2019) 18:159. doi: 10.1186/s12933-019-0961-7
24. Melo LGN, Morales PH, Drummond KRG, Santos DC, Pizarro MH, Barros BSV, et al. Diabetic retinopathy may indicate an increased risk of cardiovascular disease in patients with type 1 diabetes—a nested case-control study in Brazil. Front Endocrinol. (2019) 10:689. doi: 10.3389/fendo.2019.00689
25. Guo VY, Cao B, Wu X, Lee JJW, Zee BCY. Prospective association between diabetic retinopathy and cardiovascular disease - a systematic review and meta-analysis of cohort studies. J Stroke Cerebrovasc Dis. (2016) 25:1688–95. doi: 10.1016/j.jstrokecerebrovasdis.2016.03.009
26. Kawasaki R, Tanaka S, Tanaka S, Abe S, Sone H, Yokote K, et al. Risk of cardiovascular diseases is increased even with mild diabetic retinopathy: the Japan diabetes complications study. Ophthalmology. (2013) 120:574–82. doi: 10.1016/j.ophtha.2012.08.029
27. Young-Hak K, Myeong-Ki H, Jong-Min S, Ki-Hoon H, Duk-Hyun K, Jae-Kwan S, et al. Diabetic retinopathy as a predictor of late clinical events following percutaneous coronary intervention. J Invasive Cardiol. (2002) 14:599–602.
28. Klein BEK, Klein R, McBride PE, Cruickshanks KJ, Palta M, Knudtson MD, et al. Cardiovascular disease, mortality, and retinal microvascular characteristics in type 1 diabetes: wisconsin epidemiologic study of diabetic retinopathy. Arch Intern Med. (2004) 164:1917–24. doi: 10.1001/archinte.164.17.1917
29. Gubitosi-Klug R, Gao X, Pop-Busui R, de Boer IH, White N, Aiello LP, et al. Associations of microvascular complications with the risk of cardiovascular disease in type 1 diabetes. Diabetes Care. (2021) 44:1499–505. doi: 10.2337/dc20-3104
30. Xu XH, Sun B, Zhong S, Wei DD, Hong Z, Dong AQ. Diabetic retinopathy predicts cardiovascular mortality in diabetes: a meta-analysis. BMC Cardiovasc Disord. (2020) 20:478. doi: 10.1186/S12872-020-01763-Z
31. Jeevarethinam A, Venuraju S, Dumo A, Ruano S, Mehta VS, Rosenthal M, et al. Relationship between carotid atherosclerosis and coronary artery calcification in asymptomatic diabetic patients: a prospective multicenter study. Clin Cardiol. (2017) 40:752–8. doi: 10.1002/CLC.22727
32. Irie Y, Katakami N, Kaneto H, Takahara M, Nishio M, Kasami R, et al. The utility of ultrasonic tissue characterization of carotid plaque in the prediction of cardiovascular events in diabetic patients. Atherosclerosis. (2013) 230:399–405. doi: 10.1016/j.atherosclerosis.2013.08.015
33. Saeed A, Ballantyne CM. Assessing cardiovascular risk and testing in type 2 diabetes. Curr Cardiol Rep. (2017) 19:19. doi: 10.1007/s11886-017-0831-4
34. Catalan M, Herreras Z, Pinyol M, Sala-Vila A, Amor AJ, de Groot E, et al. Prevalence by sex of preclinical carotid atherosclerosis in newly diagnosed type 2 diabetes. Nutr Metab Cardiovasc Dis. (2015) 25:742–8. doi: 10.1016/j.numecd.2015.04.009
35. Levey A, Bosch J, Lewis J, Greene T, Rogers N, Roth D. A more accurate method to estimate glomerular filtration rate from serum creatinine: a new prediction equation. Modification of diet in renal disease study group. Ann Intern Med. (1999) 130:461–70. doi: 10.7326/0003-4819-130-6-199903160-00002
36. Wilkinson CP, Ferris FL, Klein RE, Lee PP, Agardh CD, Davis M, et al. Proposed international clinical diabetic retinopathy and diabetic macular edema disease severity scales. Ophthalmology. (2003) 110:1677–82. doi: 10.1016/S0161-6420(03)00475-5
37. Touboul P-J, Hennerici MG, Meairs S, Adams H, Amarenco P, Bornstein N, et al. Mannheim carotid intima-media thickness consensus (2004–2006). Cerebrovasc Dis. (2007) 23:75–80. doi: 10.1159/000097034
38. Couronné R, Probst P, Boulesteix AL. Random forest versus logistic regression: a large-scale benchmark experiment. BMC Bioinform. (2018) 19:270.
39. Spirtes P, Glymour C, Scheines R. Causation, Prediction, and Search. 3rd ed. Cambridge, MA: The MIT Press (2001).
40. R Core Team. R: A language and environment for statistical computing. Vienna, Austria: R Foundation for Statistical Computing (2020).
41. Carbonell M, Castelblanco E, Valldeperas X, Betriu A, Traveset A, Granado-Casas M, et al. Diabetic retinopathy is associated with the presence and burden of subclinical carotid atherosclerosis in type 1 diabetes. Cardiovasc Diabetol. (2018) 17:66. doi: 10.1186/s12933-018-0706-z
42. Rosolova H, Pelikanova T, Motovska Z. ESC guidelines on diabetes, pre-diabetes, and cardiovascular diseases developed in collaboration with EASD. Summary of the document prepared by the czech society of cardiology. Eur Heart J. (2013) 34:3035–87. doi: 10.1016/j.crvasa.2014.01.007
43. Wilson PWF, Polonsky TS, Miedema MD, Khera A, Kosinski AS, Kuvin JT. Systematic Review for the 2018 AHA/ACC/AACVPR/AAPA/ABC/ACPM/ADA/AGS/APhA/ASPC/NLA/PCNA guideline on the management of blood cholesterol: a report of the American college of cardiology/American heart association task force on clinical practice guidelines. J Am Coll Cardiol. (2019) 73:3210–27. doi: 10.1016/j.jacc.2018.11.004
Keywords: type 2 diabetes, diabetic retinopathy, subclinical atherosclerosis, cardiovascular disease, major adverse cardiovascular events
Citation: Castelblanco E, Granado-Casas M, Hernández M, Pinyol M, Correig E, Julve J, Rojo-López MI, Alonso N, Avogaro A, Ortega E and Mauricio D (2022) Diabetic retinopathy predicts cardiovascular disease independently of subclinical atherosclerosis in individuals with type 2 diabetes: A prospective cohort study. Front. Cardiovasc. Med. 9:945421. doi: 10.3389/fcvm.2022.945421
Received: 16 May 2022; Accepted: 19 October 2022;
Published: 03 November 2022.
Edited by:
Masanori Aikawa, Brigham and Women’s Hospital and Harvard Medical School, United StatesReviewed by:
Shun Ishibashi, Jichi Medical University, JapanCopyright © 2022 Castelblanco, Granado-Casas, Hernández, Pinyol, Correig, Julve, Rojo-López, Alonso, Avogaro, Ortega and Mauricio. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Emilio Ortega, ZW9ydGVnYTFAY2xpbmljLmNhdA==; Didac Mauricio, ZGlkYWNtYXVyaWNpb0BnbWFpbC5jb20=
†These authors have contributed equally to this work and share first authorship
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.