 Luis Tolento Cortes
Luis Tolento Cortes Lisa Hong
Lisa Hong
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
OPINION article
Front. Cardiovasc. Med. , 27 July 2022
Sec. Heart Failure and Transplantation
Volume 9 - 2022 | https://doi.org/10.3389/fcvm.2022.943572
This article is part of the Research Topic Novel and Emerging Therapies in Acute and Chronic Heart Failure View all 12 articles
Reported 5-year mortality rates among patients diagnosed with heart failure are upwards of 50% (1, 2). Recent studies have demonstrated similar mortality rates between patients with reduced ejection fraction (HFrEF; EF ≤ 40%), mildly reduced ejection fraction (HFmrEF; EF 41%-49%) and preserved ejection fraction (HFpEF; EF ≥50%) (2, 3). While most guideline recommendations regarding pharmacotherapy pertain to patients with HFrEF, the above observation suggests a need for mortality-reducing therapy in all subtypes of heart failure (4, 5).
In the 2021 ESC update, advances in the pharmacological management of HFpEF are discussed and conclude that there are currently no convincing studies supporting morbidity/mortality benefits with HFpEF treatment as all studies have failed to achieve their primary endpoints (4). As previously accepted, the management of patients with HFpEF revolves around acute symptom management with agents such as diuretics in addition to the management of chronic comorbidities that may contribute to the progression of heart failure. However, medication management of HFpEF has recently been reassessed with some newer studies assessing the utility of various therapies in this population. Notably, these trials were conducted in patients with LVEF as low as 40% complicating the generalizability of results to patients with HFpEF as many of the study subjects would otherwise be categorized under HFmrEF. A brief synopsis of the results from select trials are summarized below and in Table 1.
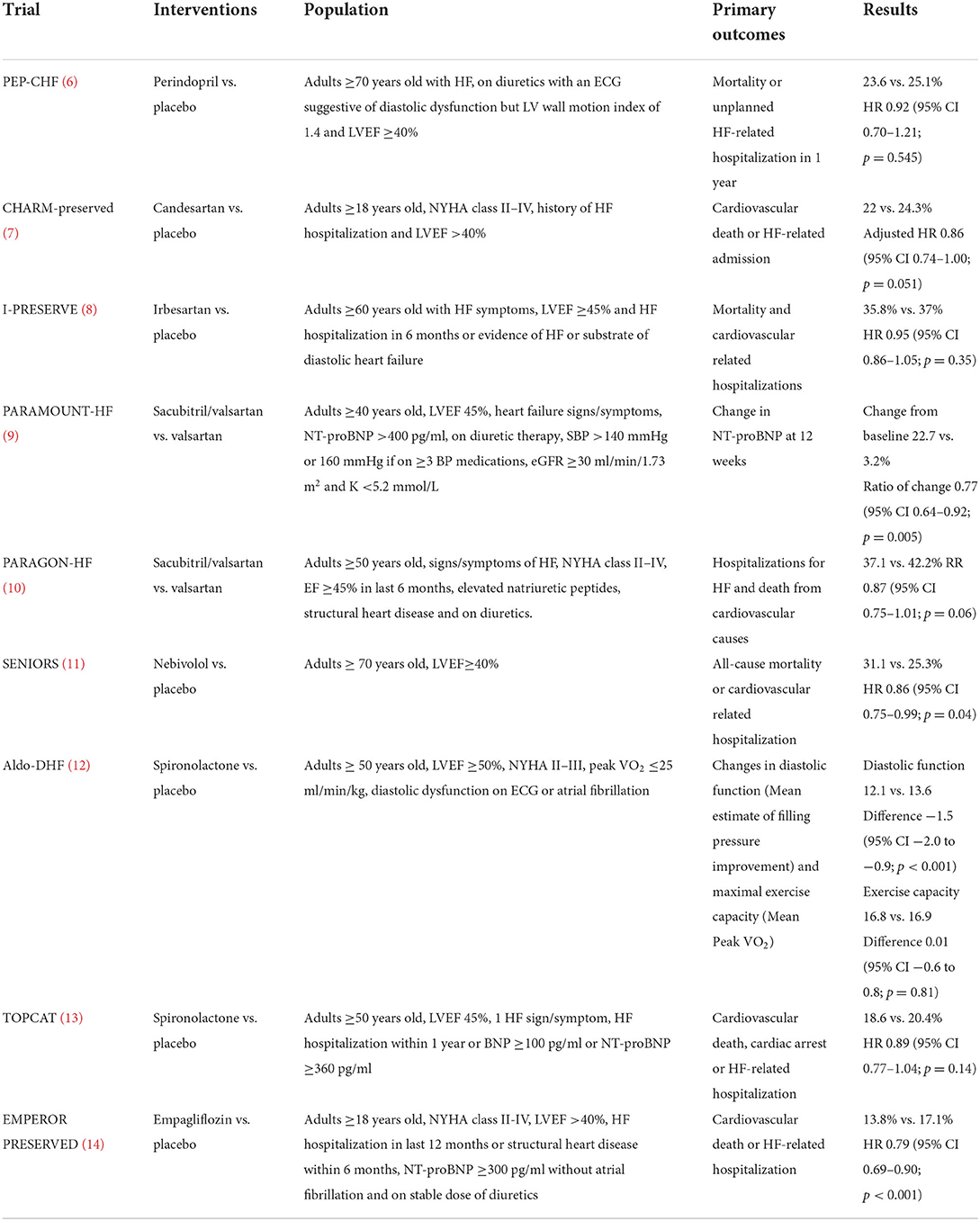
Table 1. Summary of select clinical trials.
The role of ACEI/ARB therapy in HFpEF stems from the PEP-CHF (perindopril), I-PRESERVE (irbesartan) and CHARM-Preserved (candesartan) studies. The PEP-CHF trial did not show any statistically significant differences in mortality/HF-related hospitalizations between those who received perindopril vs. placebo and was underpowered for the primary outcome. Notably, the study showed a benefit in the reduction of HF hospitalizations favoring perindopril at 1 year, but this benefit was not sustained as the difference was negligible when compared to placebo thereafter (6). The CHARM-Preserved trial reported that patients who received candesartan vs. placebo had a reduction in HF-related admissions after covariate adjustment (p = 0.072 before adjustment vs. p = 0.047 after adjustment) (7). Though, for the composite primary outcome including CV-related death and HF-related admissions, the observed difference was not significant despite covariate adjustment. Furthermore, the I-PRESERVE trial failed to find a difference in mortality or cardiovascular admissions in patients who received irbesartan vs. placebo (8). Reduction in HF hospitalization was seen in only one of these three trials, which had the most patients with HFmrEF and improved outcomes associated with use of ACEI/ARB therapy in HFpEF are likely derived from their benefit in the management of common comorbidities such as hypertension.
The role of ARNI in HFpEF was assessed in the PARAMOUNT-HF and PARAGON-HF trials. These trials compared sacubitril/valsartan vs. valsartan. While the PARAMOUNT-HF trial demonstrated a reduction in NT-proBNP (a marker for LV wall stress), the clinical relevance of this surrogate outcome is not clear and the PARAGON-HF trial demonstrated no difference in cardiovascular deaths or HF hospitalizations (9, 10). A subgroup analysis in the PARAGON-HF trial suggested a reduction in hospitalizations in patients with a LVEF ≤ 57% and sacubitril/valsartan carries an FDA-approved indication for HFpEF based on these results. The subgroup analysis included patients who would be categorized under HFmrEF but only a limited number of those who would fall within the parameters for HFpEF. The inclusion of patients with HFmrEF in these results precludes the ability to conclude the same benefit with sacubitril/valsartan exclusively among patients with HFpEF. Despite these data, there is insufficient evidence to support a strong recommendation for ARNI therapy in patients with HFpEF at this time. However, for patients with other chronic diseases where an ARB is indicated, ARNI therapy may be reasonable to consider, provided the patient can afford it.
The role of beta-blocker therapy has not been extensively studied in patients with HFpEF. The SENIORS trial reported a reduction in all-cause mortality or cardiovascular-related hospitalizations associated with the use of nebivolol vs. placebo. However, the generalizability of this study to patients with HFpEF is limited as only ~15% of participants had a LVEF >50% (11). Coupled with a high discontinuation rate secondary to drug intolerance in the SENIORS trial, it may be best to reserve beta-blocker therapy for patients with alternative indications where there is proven clinical benefit.
The role of spironolactone in HFpEF was assessed in the Aldo-DHF trial, which demonstrated an improvement in diastolic function (reported as an estimate of filling pressure), but not maximal exercise capacity at 12 months compared with placebo and the clinical relevance remained in question (12). The TOPCAT trial found no difference in the composite primary outcome of cardiovascular death, cardiac arrest and HF hospitalizations, but did find a reduction in the incidence of HF-related hospitalizations (13). Notably, this study included patients with EF ≥45%, meaning that the benefit of spironolactone was not exclusive to those with EF ≥50%. While the evidence to support use of an aldosterone antagonist in HFpEF is weak, given most patients in TOPCAT had HFpEF, the plausible reduction in HF hospitalization in this population, and the low medication cost, initiation of spironolactone in patients with HFpEF may be reasonable.
The EMPEROR-PRESERVED trial demonstrated fewer events in the composite outcome of cardiovascular death and HF hospitalization with empagliflozin vs. placebo, regardless of diabetes. However, this effect was driven by the reduced incidence of HF-related hospitalizations with zero difference in all-cause mortality (14). This is yet another trial that did not exclusively study patients with EF ≥50%. Although a reduction in hospitalizations would otherwise support the initiation of SGLT2I therapy in patients with HFpEF, several patients included in the EMPEROR- PRESERVED trial had HFmrEF with subgroup analysis illustrating attenuation of this benefit as EF increased. Furthermore, the benefit among those with HFpEF may be offset by the high-cost of SGLT2I agents. In accordance with this discussion, the recently published 2022 AHA/ACC/HFSA guideline suggests that SGTL2-I can be beneficial in patients with HFpEF (2b; moderate strength recommendation and quality of evidence) (5).
Additional trials have evaluated whether medications from other therapeutic classes play a role in the management of HFpEF. Digoxin was evaluated in the DIG-PEF trial and whilst a potential reduction in the composite outcome of mortality and hospitalizations was observed at 2 years, the benefit was not sustained at the conclusion of the study (37 months) (15). Cyclic guanosine monophosphate pathway stimulators were studied in various trials (INDIE-HFpEF, VITALITY- HF-pEF, CAPACITY-HFpEF, and NEAT-HFpEF), but failed to show an increase in either exercise tolerance or quality of life (16–19). Lastly, the phosphodiesterase-5 inhibitor, sildenafil was studied in the RELAX trial, but also failed to show any benefit in exercise tolerance (20).
The pharmacological management of HFpEF continues to be an area of uncertainty due to multiple studies failing to show a clear benefit associated with therapies that have otherwise proven useful in the management of other HF subtypes. Currently, there are no approved medications that have demonstrated improved survival in patients with HFpEF. The initiation of therapies such as ACEI/ARB or beta-blockers is primarily based on their efficacy in the management of other comorbid conditions. The 2021 ESC guideline update recommends that “in the absence of recommendations regarding disease-modifying therapies, treatment should be aimed at reducing symptoms of congestion with diuretics.” Likewise, the strong recommendation in the recently published 2022 AHA/ACC/HFSA guideline for use of diuretics, as needed in this patient population are concordant with those in the 2021 ESC guideline.
One of the most significant limitations in the current literature is the lack of data pertaining to those exclusively with EF ≥50% and future studies should aim to recruit only patients who meet this definition of HFpEF. In order to best evaluate the clinical implications of these therapies, studies should attempt to measure outcomes such as mortality, hospitalization, exercise tolerance and quality of life with adequate duration of follow up to ensure that any benefits seen early on are sustained. As we continue to search for therapies that may provide mortality/morbidity benefits to those with HFpEF, it is important for us as clinicians to understand the results and limitations of these pivotal clinical trials as they continue to emerge in order to make informed decisions in the interest of balancing risks and benefits to our patients. Until then, I guess we will stick with diuretics as our mainstay of therapy.
Information was gathered by both LT and LH. Both authors have read and agreed to the content of the manuscript.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Gerber Y, Weston SA, Redfield MM, Chamberlain AM, Manemann SM, Jiang R, et al. A contemporary appraisal of the heart failure epidemic in Olmsted County, Minnesota, 2000 to 2010. JAMA Intern Med. (2015) 175:996–1004. doi: 10.1001/jamainternmed.2015.0924
2. Tsao CW, Lyass A, Enserro D, Larson MG, Ho JE, Kizer JR, et al. Temporal trends in the incidence of and mortality associated with heart failure with preserved and reduced ejection fraction. JACC Heart Fail. (2018) 6:678–85. doi: 10.1016/j.jchf.2018.03.006
3. Kitai T, Miyakoshi C, Morimoto T, Yaku H, Murai R, Kaji S. et al. Mode of death among japanese adults with heart failure with preserved, midrange, and reduced ejection fraction. JAMA Network Open. (2020) 3:e204296. doi: 10.1001/jamanetworkopen.2020.4296
4. McDonagh TA, Metra M, Adamo M, Gardner RS, Baumbach A, Böhm M, et al. 2021 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure. Eur Heart J. (2021) 42:3599–726. doi: 10.1093/eurheartj/ehab368
5. Heidenreich PA, Bozkurt B, Aguilar D, Allen LA, Byun JJ, Colvin MM, et al. 2022 AHA/ACC/HFSA guideline for the management of heart failure: a report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. Circulation. (2022) 145:e895–1032. doi: 10.1161/CIR.0000000000001063
6. Cleland JG, Tendera M, Adamus J, Freemantle N, Polonski L, Taylor J, et al. The perindopril in elderly people with chronic heart failure PEP-CHF study. Eur Heart J. (2006) 27:2338–45. doi: 10.1093/eurheartj/ehl250
7. Yusuf S, Pfeffer MA, Swedberg K, Granger CB, Held P, McMurray JJ, et al. Effects of candesartan in patients with chronic heart failure and preserved left-ventricular ejection fraction: the CHARM-preserved trial. Lancet. (2003) 362:777–81. doi: 10.1016/S0140-6736(03)14285-7
8. Massie BM, Carson PE, McMurray JJ, Komajda M, McKelvie R, Zile MR, et al. Irbesartan in patients with heart failure and preserved ejection fraction. N Engl J Med. (2008) 359:2456–67. doi: 10.1056/NEJMoa0805450
9. Solomon SD, Zile M, Pieske B, Voors A, Shah A, Kraigher-Krainer E, et al. The angiotensin receptor neprilysin inhibitor LCZ696 in heart failure with preserved ejection fraction: a phase 2 double-blind randomised controlled trial. Lancet. (2012) 380:1387–95. doi: 10.1016/S0140-6736(12)61227-6
10. Solomon SD, McMurray JJV, Anand IS, Ge J, Lam CSP, Maggioni AP, et al. Angiotensin-neprilysin inhibition in heart failure with preserved ejection fraction. N Engl J Med. (2019) 381:1609–20. doi: 10.1056/NEJMoa1908655
11. Flather MD, Shibata MC, Coats AJ, Van Veldhuisen DJ, Parkhomenko A, Borbola J, et al. Randomized trial to determine the effect of nebivolol on mortality and cardiovascular hospital admission in elderly patients with heart failure SENIORS. Eur Heart J. (2005) 26:215–25. doi: 10.1093/eurheartj/ehi115
12. Edelmann F, Wachter R, Schmidt AG, Kraigher-Krainer E, Colantonio C, Kamke W et al. Effect of spironolactone on diastolic function and exercise capacity in patients with heart failure with preserved ejection fraction: the Aldo-DHF Randomized Controlled Trial. JAMA. (2013) 309:781–91. doi: 10.1001/jama.2013.905
13. Pitt B, Pfeffer MA, Assmann SF, Boineau R, Anand IS, Claggett B, et al. Spironolactone for heart failure with preserved ejection fraction. N Engl J Med. (2014) 370:1383–92. doi: 10.1056/NEJMoa1313731
14. Anker SD, Butler J, Filippatos G, Ferreira JP, Bocchi E, Böhm M, et al. Empagliflozin in heart failure with a preserved ejection fraction. N Engl J Med. (2021) 385:1451–61. doi: 10.1056/NEJMoa2107038
15. Ahmed A, Rich MW, Fleg JL, Zile M, Young J, Kitzman D, et al. Effects of digoxin on morbidity and mortality in diastolic heart failure: the ancillary digitalis investigation group trial. Circulation. (2006) 114:397–403. doi: 10.1161/CIRCULATIONAHA.106.628347
16. Borlaug BA, Anstrom KJ, Lewis GD, Shah SJ, Levine JA, Koepp GA, et al. Effect of inorganic nitrite vs placebo on exercise capacity among patients with heart failure with preserved ejection fraction: the INDIE-HFpEF randomized clinical trial. JAMA. (2018) 320:1764–73. doi: 10.1001/jama.2018.14852
17. Armstrong PW, Lam CSP, Anstrom KJ, Ezekowitz J, Hernandez AF, O'Connor CM, et al. Effect of vericiguat vs placebo on quality of life in patients with heart failure and preserved ejection fraction: the VITALITY-HFpEF randomized clinical trial. JAMA. (2020) 324:1512–21. doi: 10.1001/jama.2020.15922
18. Udelson JE, Lewis GD, Shah SJ, Zile MR, Redfield MM, Burnett J Jr, et al. Effect of praliciguat on peak rate of oxygen consumption in patients with heart failure with preserved ejection fraction: the CAPACITY HFpEF randomized clinical trial. JAMA. (2020) 324:1522–31. doi: 10.1001/jama.2020.16641
19. Redfield MM, Anstrom KJ, Levine JA, Koepp GA, Borlaug BA, Chen HH, et al. Isosorbide mononitrate in heart failure with preserved ejection fraction. N Engl J Med. (2015) 373:2314–24. doi: 10.1056/NEJMoa1510774
Keywords: heart failure, preserved ejection fraction, HFpEF, pharmacology, heart failure management
Citation: Tolento Cortes L and Hong L (2022) Heart failure with preserved ejection fraction—Out with the old and out with the new? Front. Cardiovasc. Med. 9:943572. doi: 10.3389/fcvm.2022.943572
Received: 13 May 2022; Accepted: 08 July 2022;
Published: 27 July 2022.
Edited by:
Konstantinos Dean Boudoulas, The Ohio State University, United StatesReviewed by:
Bibhiti Das, University of Mississippi Medical Center, United StatesCopyright © 2022 Tolento Cortes and Hong. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Lisa Hong, bGhvbmdAbGx1LmVkdQ==
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.