 Botao Yu
Botao Yu Zubing Mei
Zubing Mei Hang Yu4†
Hang Yu4†
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
STUDY PROTOCOL article
Front. Cardiovasc. Med. , 05 August 2022
Sec. Cardiovascular Epidemiology and Prevention
Volume 9 - 2022 | https://doi.org/10.3389/fcvm.2022.926218
Introduction: Cancer and cardiovascular disease remain leading causes of death and disability worldwide, which places a heavy burden on public health systems and causes widespread suffering. Because these entities have highly overlapping risk factors, including hyperlipidemia, hypertension, diabetes, obesity, smoking and other lifestyle factors, many studies have reported that they have similar etiological mechanisms. Accumulating evidence indicates that there is an increased risk of cardiovascular disease among cancer survivors compared with the general population. However, whether cancer is associated with an increased risk of cardiovascular disease remains controversial.
Methods and analysis: We will conduct and report the meta-analysis strictly based on the Cochrane Handbook for Systematic Reviews and the Meta-analysis of Observational Studies in Epidemiology guidelines combined with the Preferred Reporting Items for Systematic Reviews and Meta-analysis for Protocols (PRISM-P). This meta-analysis was registered with PROSPERO (registration number CRD42022307056). We will search for studies published from database inception to December 1, 2021, regardless of language or date, in three electronic databases (PubMed, EMBASE, and Cochrane Library) to identify and appraise cohort studies examining the relationship between cancer and subsequent cardiovascular disease risk. The literature screening, inclusion and data extraction will be conducted independently by two investigators using pre-designed standardized data extraction forms. A senior investigator will be consulted in cases of disagreement. We will assess risk of bias in the included cohort studies using the Newcastle–Ottawa Scale (NOS). Quantitative synthesis will be conducted using a random-effects model. To explore potential sources of heterogeneity, we will carry out multiple sensitivity analysis, meta-regression and subgroup analysis according to baseline characteristics. Publication bias will be evaluated through visual inspection of funnel plot asymmetry as well as by Begg's rank correlation test and Egger's weighted linear regression test.
Cancer and cardiovascular disease remain the leading causes of death and disability worldwide, which places a heavy burden on public health systems and causes widespread suffering (1–6). It has been reported that approximately 18 million people worldwide are diagnosed with cancer each year (7). In the last two decades, the survival rate of cancers has improved with the continuous development of early diagnosis and improvement of treatment modalities (8–11). Indeed, more than half of individuals in high-income groups are expected to survive for 10 years or more (12).
Cancer and cardiovascular disease have highly overlapping risk factors, including hyperlipidemia, hypertension, diabetes, obesity, smoking and other lifestyle factors (13–15), and many studies have reported that they share similar etiological mechanisms (16–18). Nevertheless, whether cancer is associated with an increased risk of cardiovascular disease has been controversial. Several studies have demonstrated that people diagnosed with cancer, such as breast cancer, lung cancer and hematological malignancies, have a higher risk of cardiovascular disease than the general population (12, 19–30). Other studies, however, have found that cancer survivors have a lower risk of cardiovascular disease, including those with gastric cancer (31). Therefore, these conflicting results prompted us to conduct a systematic comprehensive analysis to assess the relationship between cancer and subsequent cardiovascular disease risk. For the reasons given above, we will carry out a meta-analysis to evaluate the risk of cardiovascular disease among cancer survivors based on high-quality population-based cohort studies.
We will conduct and report our meta-analysis strictly based on the Cochrane Handbook for Systematic Reviews and the Meta-analysis of Observational Studies in Epidemiology guidelines combined with the Preferred Reporting Items for Systematic Reviews and Meta-analysis for Protocols (PRISM-P) (32) (Supplementary Table S1). Details of the meta-analysis protocol, which has been registered with the registration number CRD42022307056, can be found at the PROSPERO website (www.crd.york.ac.uk/prospero).
We will search for studies published from database inception to December 1, 2021, regardless of language or date, in three commonly used electronic databases, namely, PubMed, EMBASE, and Cochrane Library, to identify and appraise cohort studies examining the relationship between cancer and subsequent cardiovascular disease risk. We will use Medical Subject Heading (MeSH) or EMBASE Subject Heading (Emtree) terms along with free-text words that are associated with cancer and cardiovascular disease. The following search keywords and search logic will include cancer/tumor/tumor/oncology/neoplasm*/malignanc*/carcinoma AND cardiovascular diseases/coronary disease/stroke/myocardial infarction/myocardial ischemia/heart failure AND cohort study/longitudinal study/follow-up study/prospective study/retrospective study (PubMed search strategy in Table 1). We will also identify additional relevant studies by reviewing reference lists from the articles identified and a manual search of abstracts from annual meetings of the European Society for Medical Oncology (ESMO) and the American Society of Clinical Oncology (ASCO). When there are multiple studies describing the same cohort, the study involving the largest number of participants or the most recent sample cohort will be included. Duplicate citations will first be automatically removed from the initial database searches using EndNote version X9 (Thomson Reuters), after which additional duplicate citations will be manually removed by comparing authors, article titles and publication dates. We will carry out these selection processes separately by two investigators. Conflicts will be handled by discussion, and a senior investigator will be consulted if necessary.
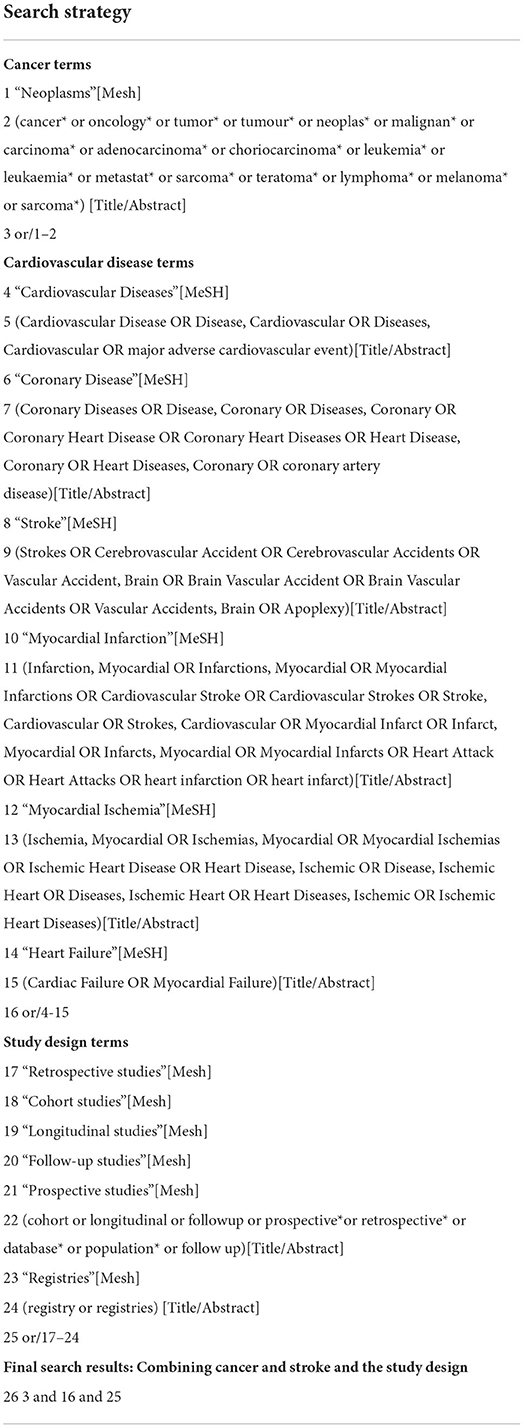
Table 1. Search strategy for the Pubmed database.
We will include studies with the following inclusion criteria in qualitative analyses: (1) studies involving a prospective or retrospective population-based cohort; (2) participants diagnosed with cancer but no history of cardiovascular disease or not diagnosed with cardiovascular disease at the time of participant enrolment based on the International Classification of Diseases, Seventh to Tenth Revision (ICD 7–10) criteria in the population-based cohort and diagnosed with one type of cardiovascular disease during the subsequent follow-up period; (3) studies reporting risk estimates, including relative risk (RR), hazard ratio (HR) and odds ratio (OR) with 95% confidence intervals (CIs), or studies that can provide relevant data to be used to estimate risk ratios. We will exclude hospital-based cohort studies and those with inadequate data to estimate risk ratios.
Data extraction will be conducted independently by two investigators using pre-designed standardized data extraction forms and crosschecked by a third investigator. Disagreements will be resolved by consensus. The following study characteristics will be abstracted: first author, publication year and design, geographic region, observation period, participant age at cancer diagnosis, comparison population, criteria of diagnosis for cancer and cardiovascular disease, study findings and risk estimates of the association of cardiovascular disease with cancer.
The risk of bias for the included studies will be assessed using the Newcastle–Ottawa scale (NOS) tool according to three major aspects: representativeness of the patients, ascertainment of exposure and outcomes and adequacy of follow-up (33). A total of nine scores will be assigned to nine item domains. Studies will be judged to be at low risk of bias (≥8 points) or moderate to high risk of bias (<8 points) (15).
All statistical meta-analyses will be carried out using Stata software (version 12.0; Stata Corp LP, College Station, TX). The summary RR among cancer survivors compared with that among the non-cancer population accompanied by its 95% CI will be defined as the primary outcome. Given the expected large heterogeneity for the participants, study design, and clinical and methodological aspects among the included studies, we will adopt the DerSimonian–Laird random-effects model to calculate risk estimates (34). RR will be regarded as the common risk estimate for the association between cancer and cardiovascular disease risk. We will include RRs that are maximally adjusted for potential confounders for meta-analysis (15, 35). As fully adjusted models include the most hypothesized confounders, we will prioritize selecting fully adjusted risk estimates to meta-analyse RRs. Heterogeneity will be assessed by using the χ2 test on Cochran's Q statistic, and the I2 statistic will be employed to quantify the proportion of the total variation leading to heterogeneity, where an I2 > 50% indicates substantial heterogeneity (36).
We will further carry out subgroup analysis to explore potential sources of heterogeneity based on the following factors post-hoc: study design, geographic regions, methodological quality, outcome division, age, sex, attained age, adjuvant therapy, cancer site and cardiovascular disease type. In addition, sensitivity analysis will be carried out by removing one study at each time and repeating the analysis to evaluate whether any individual study considerably influences the summary estimates. Meta-regression will also be performed to explain the effects of heterogeneity. We will explore the possibility of publication bias with visual inspection of a funnel plot and with Begg's rank correlation test and Egger's weighted linear regression test if 10 or more studies are included in the meta-analysis (37, 38). To further assess the potential effects of publication bias, we will apply a Duvall and Tweedle trim-and-fill technique to estimate the number of studies with null effects that are missing from the meta-analysis (39). In all statistical analyses, P ≤ 0.05 will be considered statistically significant.
This study-level pooled analysis of all population-based cohort studies will provide a comprehensive overview and a quantitative summary of the risk of cardiovascular disease for cancer survivors compared with that for the general population. Moreover, we will explore the potential of heterogeneity by multiple subgroup analyses based on study baseline characteristics and examine the robustness of the results through sensitivity analysis.
This meta-analysis of population-based cohort studies will have several strengths. First, to the best of our knowledge, this study will be the first and most comprehensive one addressing such an association with highly representative populations. Second, we will strictly follow the Cochrane Handbook (40) to carry out the meta-analysis, and the risk of bias of all the included studies will be assessed using the NOS tool, which can provide clear knowledge of the study quality in our meta-analysis. Third, by conducting multiple subgroup, meta-regression and sensitivity analyses, we will thoroughly explore the sources of heterogeneity and robustness of the pooled estimates in this meta-analysis. Finally, a major study database search combined with manual search will be involved in our meta-analysis without language or date limitations, which can reduce the possibility of publication bias. Furthermore, if publication bias exists, the trim and fill method will be applied to adjust the risk estimates, which can provide reliable estimates for ‘missing' studies.
As a major limitation of this study, significant between-study heterogeneity is anticipated because we will include all types of cancer for analysis. Although multiple subgroup analyses and meta-regression will be conducted based on the available data from the included studies, some unknown confounding factors, such as cancer histology, cancer stage, performance status, and age of onset, will be highly diverse, making this study design clinically heterogeneous. However, to maximally control the impact of heterogeneity on the results, we will strictly adhere to the inclusion and exclusion criteria when we select suitable studies and use RRs maximally adjusted for potential confounders for meta-analysis and conducted multiple subgroup analyses to explore the potential sources of heterogeneity. Therefore, this study will to some extent provide us with a general risk estimate of cardiovascular disease among cancer survivors. The findings of this study will provide valuable clinical significance for the CVD risk of cancer survivors and the approximate risk estimate of CVD for cancer survivors. Overall, prevention and treatment of CVD during early treatment after cancer diagnosis have important clinical significance. Oncologists can choose cardiovascular protection treatment strategies according to the adjuvant treatment options and risk factors for cancer patients to reduce the organ function damage caused by treatment as much as possible.
Ethical review and approval was not required as this study would only use published data without involving human participants.
Conceptualization: BY, ZM, HY, QG, and JP. Data curation, formal analysis, methodology, software, and writing–original draft: BY and ZM. Funding acquisition: BY. Investigation, resources, and visualization: BY, QG, and JP. Project administration and validation: BY, ZM, HY, YW, QG, and JP. Supervision: ZM, QG, and JP. Writing–review & editing: BY, YW, and ZM. All authors contributed to the article and approved the submitted version.
This work was supported by Qingdao Key Health Discipline Development Fund (Grant No. PD-202102018).
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fcvm.2022.926218/full#supplementary-material
ASCO, American Society of Clinical Oncology; CI, confidence interval; Emtree, EMBASE Subject Heading; ESMO, the European Society for Medical Oncology; HR, hazard ratio; ICD, International Classification of Diseases; MeSH, Medical Subject Heading; NOS, Newcastle–Ottawa scale; OR, odd ratio; PRISM-P, Preferred Reporting Items for Systematic Reviews and Meta-analysis for Protocols; RR, relative risk.
1. Sung H, Ferlay J, Siegel RL, Laversanne M, Soerjomataram I, Jemal A, et al. Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. (2021) 71:209–49. doi: 10.3322/caac.21660
2. Ferlay J, Colombet M, Soerjomataram I, Parkin DM, Piñeros M, Znaor A, et al. Cancer statistics for the year 2020: an overview. Int J Cancer. (2021). doi: 10.1002/ijc.33588
3. Fuchs FD, Whelton PK. High blood pressure and cardiovascular disease. Hypertension. (2020) 75:285–92. doi: 10.1161/HYPERTENSIONAHA.119.14240
4. Zhao D, Liu J, Wang M, Zhang X, Zhou M. Epidemiology of cardiovascular disease in China: current features and implications. Nat Rev Cardiol. (2019) 16:203–12. doi: 10.1038/s41569-018-0119-4
5. Timmis A, Townsend N, Gale CP, Torbica A, Lettino M, Petersen SE, et al. European society of cardiology: cardiovascular disease statistics 2019. Eur Heart J. (2019) 41:12–85. doi: 10.1093/eurheartj/ehz859
6. Sturgeon KM, Deng L, Bluethmann SM, Zhou S, Trifiletti DM, Jiang C, et al. A population-based study of cardiovascular disease mortality risk in US cancer patients. Eur Heart J. (2019) 40:3889–97. doi: 10.1093/eurheartj/ehz766
7. Richters A, Aben KKH, Kiemeney LALM. The global burden of urinary bladder cancer: an update. World J Urol. (2020) 38:1895–904. doi: 10.1007/s00345-019-02984-4
8. Cao M, Li H, Sun D, Chen W. Cancer burden of major cancers in China: a need for sustainable actions. Cancer Commun. (2020) 40:205–10. doi: 10.1002/cac2.12025
9. Chowdhury PS, Chamoto K, Honjo T. Combination therapy strategies for improving PD-1 blockade efficacy: a new era in cancer immunotherapy. J Int Med. (2018) 283:110–20. doi: 10.1111/joim.12708
10. Howlader N, Forjaz G, Mooradian MJ, Meza R, Kong CY, Cronin KA, et al. The effect of advances in lung-cancer treatment on population mortality. N Eng J Med. (2020) 383:640–9. doi: 10.1056/NEJMoa1916623
11. Siegel RL, Jemal A, Wender RC, Gansler T, Ma J, Brawley OW. An assessment of progress in cancer control. CA: Cancer J Clin. (2018) 68:329–39. doi: 10.3322/caac.21460
12. Strongman H, Gadd S, Matthews A, Mansfield KE, Stanway S, Lyon AR, et al. Medium and long-term risks of specific cardiovascular diseases in survivors of 20 adult cancers: a population-based cohort study using multiple linked UK electronic health records databases. Lancet. (2019) 394:1041–54. doi: 10.1016/S0140-6736(19)31674-5
13. Johnson CB, Davis MK, Law A, Sulpher J. Shared risk factors for cardiovascular disease and cancer: implications for preventive health and clinical care in oncology patients. Can J Cardiol. (2016) 32:900–7. doi: 10.1016/j.cjca.2016.04.008
14. Koene RJ, Prizment AE, Blaes A, Konety SH. Shared risk factors in cardiovascular disease and cancer. Circulation. (2016) 133:1104–14. doi: 10.1161/CIRCULATIONAHA.115.020406
15. Zhang F, Wang K, Du P, Yang W, He Y, Li T, et al. Risk of stroke in cancer survivors: a meta-analysis of population-based cohort studies. Neurology. (2021) 96:e513–e26. doi: 10.1212/WNL.0000000000011264
16. Bang OY, Chung JW, Lee MJ, Seo WK, Kim GM, Ahn MJ. Cancer-related stroke: an emerging subtype of ischemic stroke with unique pathomechanisms. J Stroke. (2020) 22:1–10. doi: 10.5853/jos.2019.02278
17. Dardiotis E, Aloizou AM, Markoula S, Siokas V, Tsarouhas K, Tzanakakis G, et al. Cancer-associated stroke: pathophysiology, detection and management (Review). Int J Oncol. (2019) 54:779–96. doi: 10.3892/ijo.2019.4669
18. Navi BB, Iadecola C. Ischemic stroke in cancer patients: a review of an underappreciated pathology. Ann Neurol. (2018) 83:873–83. doi: 10.1002/ana.25227
19. Schoormans D, Vissers PAJ, van Herk-Sukel MPP, Denollet J, Pedersen SS, Dalton SO, et al. Incidence of cardiovascular disease up to 13 year after cancer diagnosis: a matched cohort study among 32,757 cancer survivors. Cancer Med. (2018) 7:4952–63. doi: 10.1002/cam4.1754
20. Rugbjerg K, Mellemkjaer L, Boice JD, Køber L, Ewertz M, Olsen JH. Cardiovascular disease in survivors of adolescent and young adult cancer: a Danish cohort study, 1943–2009. J Natl Cancer Inst. (2014) 106:dju110. doi: 10.1093/jnci/dju110
21. Reulen RC, Guha J, Bright CJ, Henson KE, Feltbower RG, Hall M, et al. Risk of cerebrovascular disease among 13 457 five-year survivors of childhood cancer: a population-based cohort study. Int J Cancer. (2021) 148:572–83. doi: 10.1002/ijc.33218
22. Park NJ, Chang Y, Bender C, Conley Y, Chlebowski RT, van Londen GJ, et al. Cardiovascular disease and mortality after breast cancer in postmenopausal women: results from the women's health initiative. PLoS ONE. (2017) 12:e0184174. doi: 10.1371/journal.pone.0184174
23. Mulrooney DA, Yeazel MW, Kawashima T, Mertens AC, Mitby P, Stovall M, et al. Cardiac outcomes in a cohort of adult survivors of childhood and adolescent cancer: Retrospective analysis of the childhood cancer survivor study cohort. BMJ. (2009) 339:34. doi: 10.1136/bmj.b4606
24. Khan N, Mant D, Carpenter L, Forman D, Rose P. Long-term health outcomes in a British cohort of breast, colorectal and prostate cancer survivors: a database study. Br J Cancer. (2011) 105:S29–37. doi: 10.1038/bjc.2011.420
25. Hu Q, Chang C-P, Rowe K, Snyder J, Deshmukh V, Newman M, et al. Disparities in cardiovascular disease risk among hispanic breast cancer survivors in a population-based cohort. JNCI Cancer Spectrum. (2021) 5:16. doi: 10.1093/jncics/pkab016
26. Hooning MJ, Botma A, Aleman BM, Baaijens MH, Bartelink H, Klijn JG, et al. Long-term risk of cardiovascular disease in 10-year survivors of breast cancer. J Natl Cancer Inst. (2007) 99:365–75. doi: 10.1093/jnci/djk064
27. Chao C, Xu L, Bhatia S, Cooper R, Brar S, Wong FL, et al. Cardiovascular disease risk profiles in survivors of adolescent and young adult (AYA) cancer: the kaiser permanente AYA cancer survivors study. J Clin Oncol: Off J Am Soc Clin Oncol. (2016) 34:1626–33. doi: 10.1200/JCO.2015.65.5845
28. Brand JS, Hedayati E, Bhoo-Pathy N, Bergh J, Hall P, Humphreys K, et al. Time-dependent risk and predictors of venous thromboembolism in breast cancer patients: a population-based cohort study. Cancer. (2017) 123:468–75. doi: 10.1002/cncr.30364
29. Armenian SH, Xu L, Ky B, Sun C, Farol LT, Pal SK, et al. Cardiovascular disease among survivors of adult-onset cancer: a community-based retrospective cohort study. J Clin Oncol: Off J Am Soc Clin Oncol. (2016) 34:1122–30. doi: 10.1200/JCO.2015.64.0409
30. Abdel-Qadir H, Thavendiranathan P, Austin PC, Lee DS, Amir E, Tu JV, et al. The risk of heart failure and other cardiovascular hospitalizations after early stage breast cancer: a matched cohort study. J Natl Cancer Inst. (2019) 111:854–62. doi: 10.1093/jnci/djy218
31. Shin DW, Suh B, Park Y, Lim H, Suh YS, Yun JM, et al. Risk of coronary heart disease and ischemic stroke incidence in gastric cancer survivors: a nationwide study in Korea. Ann Surg Oncol. (2018) 25:3248–56. doi: 10.1245/s10434-018-6635-y
32. Moher D, Shamseer L, Clarke M, Ghersi D, Liberati A, Petticrew M, et al. Preferred reporting items for systematic review and meta-analysis protocols (PRISMA-P) 2015 statement. Syst Rev. (2015) 4:1. doi: 10.1186/2046-4053-4-1
33. Stang A. Critical evaluation of the Newcastle-Ottawa scale for the assessment of the quality of non-randomized studies in meta-analyses. Eur J Epidemiol. (2010) 25:603–5. doi: 10.1007/s10654-010-9491-z
34. DerSimonian R, Laird N. Meta-analysis in clinical trials. Control Clin Trials. (1986) 7:177–88. doi: 10.1016/0197-2456(86)90046-2
35. Zhang F, Liu L, Zhang C, Ji S, Mei Z, Li T. Association of metabolic syndrome and its components with risk of stroke recurrence and mortality: a meta-analysis. Neurology. (2021)17 97:e695–705. doi: 10.1212/WNL.0000000000012415
36. Higgins JP, Thompson SG, Deeks JJ, Altman DG. Measuring inconsistency in meta-analyses. Bmj. (2003) 327:557–60. doi: 10.1136/bmj.327.7414.557
37. Egger M, Davey Smith G, Schneider M, Minder C. Bias in meta-analysis detected by a simple, graphical test. Bmj. (1997) 315:629–34. doi: 10.1136/bmj.315.7109.629
38. Begg CB, Mazumdar M. Operating characteristics of a rank correlation test for publication bias. Biometrics. (1994) 50:1088–101. doi: 10.2307/2533446
39. Duval S, Tweedie R. Trim and fill: a simple funnel-plot-based method of testing and adjusting for publication bias in meta-analysis. Biometrics. (2000) 56:455–63. doi: 10.1111/j.0006-341X.2000.00455.x
Keywords: cardiovascular disease, cancer, population-based cohort study, risk, pooled analysis
Citation: Yu B, Mei Z, Yu H, Wang Y, Geng Q and Pu J (2022) Risk of cardiovascular disease among cancer survivors: Protocol of a pooled analysis of population-based cohort studies. Front. Cardiovasc. Med. 9:926218. doi: 10.3389/fcvm.2022.926218
Received: 26 April 2022; Accepted: 18 July 2022;
Published: 05 August 2022.
Edited by:
Harry H. X. Wang, Sun Yat-sen University, ChinaCopyright © 2022 Yu, Mei, Yu, Wang, Geng and Pu. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Jin Pu, MTM0ODIyODIzMTJAMTYzLmNvbQ==; Qian Geng, Z2VuZ3FpYW44MTVAc2luYS5jb20=; Yan Wang, d2FuZ3lhbjIwMDczMDhAMTI2LmNvbQ==; Zubing Mei, aGVycm1heW9yQDEyNi5jb20=
†These authors have contributed equally to this work
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.