
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Cardiovasc. Med. , 26 July 2022
Sec. Lipids in Cardiovascular Disease
Volume 9 - 2022 | https://doi.org/10.3389/fcvm.2022.916031
This article is part of the Research Topic Women in Lipids in Cardiovascular Disease View all 12 articles
 Sonia Ruiz-Bustillo1,2,3,4*
Sonia Ruiz-Bustillo1,2,3,4* Neus Badosa1,2
Neus Badosa1,2 Ignacio Cabrera-Aguilera1,5,6Consol Ivern1,2Marc Llagostera2Diana Mojón2Miren Vicente2Núria Ribas1,2Lluis Recasens1,2Julio Martí-Almor1,2,3Mercè Cladellas1,2,3Núria Farré1,2,3,4
Ignacio Cabrera-Aguilera1,5,6Consol Ivern1,2Marc Llagostera2Diana Mojón2Miren Vicente2Núria Ribas1,2Lluis Recasens1,2Julio Martí-Almor1,2,3Mercè Cladellas1,2,3Núria Farré1,2,3,4Aims: Despite the evidence, lipid-lowering treatment (LLT) in secondary prevention remains insufficient, and a low percentage of patients achieve the recommended LDL cholesterol (LDLc) levels by the guidelines. We aimed to evaluate the efficacy of an intensive, mobile devices-based healthcare lipid-lowering intervention after hospital discharge in patients hospitalized for acute coronary syndrome (ACS).
Methods and results: Ambiespective register in which a mobile devices-based healthcare intervention including periodic follow-up, serial lipid level controls, and optimization of lipid-lowering therapy, if appropriate, was assessed in terms of serum lipid-level control at 12 weeks after discharge. A total of 497 patients, of which 462 (93%) correctly adhered to the optimization protocol, were included in the analysis. At the end of the optimization period, 327 (70.7%) patients had LDLc levels ≤ 70 mg/dL. 40% of patients in the LDLc ≤ 70 mg/dL group were upgraded to very-high intensity lipid-lowering ability therapy vs. 60.7% in the LDLc > 70 mg/dL group, p < 0.001. Overall, 38.5% of patients had at least a change in their LLT. Side effects were relatively infrequent (10.7%). At 1-year follow-up, LDLc levels were measured by the primary care physician in 342 (68.8%) of the whole cohort of 497 patients. In this group, 71.1% of patients had LDLc levels ≤ 70 mg/dL.
Conclusion: An intensive, structured, mobile devices-based healthcare intervention after an ACS is associated with more than 70% of patients reaching the LDLc levels recommended by the clinical guidelines. In patients with LDLc measured at 1-year follow-up, 71.1% had LDLc levels ≤ 70 mg/dL.
There is extensive evidence confirming the benefit of cardiac rehabilitation programs (CRP) in patients with ischemic heart disease (IHD) (1). An intensive CRP reduces cardiovascular risk through lifestyle changes (2). However, correct pharmacological treatment is also crucial for optimal cardiovascular risk factors control, including dyslipidemia. The drop in low-density lipoprotein cholesterol (LDLc) levels in secondary prevention significantly reduces mortality, coronary events, coronary revascularization procedures, and ischemic strokes (3).
Despite the evidence, lipid-lowering treatment (LLT) in secondary prevention remains insufficient, and a low percentage of patients achieve the LDLc levels recommended by the guidelines (4–6). One factor explaining this contradiction is the so-called therapeutic inertia, defined as the failure of physicians to initiate or intensify an indicated therapy (7). Other significant barriers are lack of infrastructure and availability of CRP, lack of perceived importance of secondary prevention among professionals, and low patient motivation and financial difficulties to pay the LLT (8).
Mobile devices-based healthcare (mHealth) aimed at improving patients’ living standards (9) can be an effective tool to improve the suboptimal results in dyslipidemia control (10). Considering the disappointing results in secondary prevention, we conducted a randomized pilot study to evaluate whether an intensive mHealth lipid-lowering intervention implemented after a hospitalization due to IHD was associated with a lower LDLc level. We demonstrated that this strategy was associated with improved management of LDLc levels compared with standard care alone (11). Our current study aimed to assess whether this same structured mHealth-based protocol helped improve LDLc levels after a hospitalization due to IHD in a real-life population.
The Risk Optimization Acute Coronary Syndrome (RiskOp-ACS) study was a single-center ambispective register assessing the efficacy and safety of a lipid-lowering intervention to improve the management of LDLc levels in patients hospitalized for IHD (ClinicalTrials.gov Identifier: NCT03619395). Between July 2018 and September 2019, all patients hospitalized for IHD in our hospital not meeting any exclusion criteria (inability or refusal to sign the informed consent or presenting comorbidities with a life expectancy of less than 1 year) and willing to participate in the CRP were screened for inclusion in this study. All patients providing written informed consent were included in the RiskOp-ACS register. The Ethics Committee of the Hospital del Mar approved the study and was conducted per the Declaration of Helsinki. The Ethics Committee approved the retrospective inclusion of patients who followed the same protocol since November 2016 to increase the sample size and waived the need for written informed consent. Therefore, all patients included in the study (both prospectively and retrospectively) followed the same optimization protocol.
The multidisciplinary CRP performed in our center is coordinated by specialized nurses. It includes interventions performed by cardiologists, nurses, rehabilitation physicians, and professionals specialized in managing anxiety and other mental health disorders. All patients discharged after a hospitalization for an acute IHD event and with no severe cognitive impairment are invited to the CRP. As part of the program activities, nurses educate patients in healthy habits during the in-hospital stage and at follow-up visits at 3 and 12 months after discharge; provide and monitor the quality of life, anxiety, and depression symptoms using validated tests, and coordinate the follow-up plan and visits. Rehabilitation physicians and physiotherapists assess the patient’s functional status and indicate and supervise physical activity during follow-up. All professionals involved in the CRP participate in monthly group sessions aimed at reinforcing the health education of the patients, with a particular focus on increasing the patients’ understanding of the pathophysiology of IHD, on the role of cardiovascular risk factors, and the importance of optimal risk factor management, mainly through physical activity, control of anxiety, and adherence to guideline-recommended pharmacotherapies.
All patients were discharged under LLT. Serum lipid levels were measured at week 6 after discharge, and a virtual visit with the cardiologist was made within 1 week of the blood test. The laboratory test results were evaluated using a pre-specified algorithm based on clinical practice guidelines (Supplementary Figure 1). If there was a need to modify the LLT, the electronic prescription was changed accordingly, and the patient was informed by phone. Thus, the protocol avoided the need to come to the hospital or primary care center since the medication could be retrieved directly from the local pharmacy or printed/seen in the personal health record through a dedicated app/website created by the Health Department (Lamevasalut). This intervention was repeated every 6 weeks after every pharmacological change until the target LDLc levels (calculated by the Friedewald formula) advised in the clinical guidelines were achieved, or maximum lipid-lowering therapy according to local regulation was reached. Thus, the duration of the intervention was a maximum of 3 months (“optimization period”). From that moment, the follow-up was performed by the patient’s primary care general physician and primary care cardiologist. Creatinine kinase and liver tests were measured in all blood tests following LLT modification.
The LLT intensity was defined according to its ability to reduce LDLc (12, 13). The moderate lipid-lowering ability group comprises moderate-intensity statins and low-intensity statin plus ezetimibe. High-intensity statins, and medium-intensity statins plus ezetimibe are the high-reduction group. High-potency statins plus ezetimibe are the very-high reduction group. Finally, PCSK9 inhibitor added at maximally tolerated doses to LLT is considered extreme reduction ability treatment (Supplementary Table 1). In our country, the prescription of PCSK9 inhibitors is allowed in the public health system for patients with established cardiovascular disease and no optimal control defined as LDLc > 100 mg/dL despite the maximum tolerated dose of statins, patients intolerant to statins, or in whom statins are contraindicated (14).
The primary study endpoint was the proportion of patients with serum LDLc levels ≤ 70 mg/dL at the end of the optimization period, which was the treatment goal supported by current ESC guidelines (15) when the study was conducted. Other variables related to lipid management assessed during the intervention included lipid-lowering medication use, changes in lipid-lowering medication, and the presence of side effects, among others. As an exploratory analysis, the number of patients who reached LDLc levels < 55 mg/dL at the end of the optimization period was also analyzed. Finally, we assessed also as an exploratory analysis, clinical outcomes with the achievement of LDL ≤ 70 mg/dL at the end of the optimization period.
Data for continuous variables are expressed as mean ± standard deviation (SD) or median and interquartile range (IQR) based on normality distribution assessed by Kolmogorov-Smirnov test. Categorical variables were expressed as percentages. Differences in baseline characteristics between groups were tested using the χ2-test (categorical variables) and Student’s t-test or Mann–Whitney U-test, one-way analysis of variance, or Kruskal-Wallis test for continuous variables. All analysis was performed using IBM SPSS Statistics v25 (Armonk, NY, United States). For all tests, p < 0.05 was considered as statically significant.
The whole cohort included 497 patients, of which 462 (93%) correctly adhered to the optimization protocol and were included in the analysis. At the end of the optimization period, 327 (70.7%) patients had LDLc levels ≤ 70 mg/dL, and 159 (34.7%) had LDLc levels < 55 mg/dL.
According to LDLc levels achieved, baseline characteristics of patients are described in Table 1. Interestingly, the only differences between both groups were a higher prevalence of chronic obstructive pulmonary disease in the LDLc ≤ 70 mg/dL group and different history of smoking.

Table 1. Baseline characteristics of patients according to LDLc levels after the optimization protocol.
Table 2 shows LDLc levels at baseline and during follow-up, the type of LLT given, and the presence of side effects. Interestingly, LLT did not differ at discharge from the hospital, with 65% of patients on high lipid-lowering ability treatment. However, by the end of the optimization therapy, 40% of patients in the LDL ≤ 70 mg/dL levels were upgraded to very-high intensity lipid-lowering ability vs. 60.7% in the LDL levels > 70 mg/dL, p < 0.001. Overall, 38.5% of patients had at least a change in their LLT. The LDLc levels > 70 mg/dL group had a higher number of changes in medications (61.4 vs. 27.5%, p < 0.001). However, this treatment modification was not enough to achieve good LDLc control in this group. During the optimization period, only 14 (2.8%) received extreme lipid-lowering ability treatment with PCSK-9 inhibitors, 5 (1.5%) patients in the LDLc ≤ 70 mg/dL, and 9 (6.9%) patients in the LDL levels > 70 mg/dL, p = 0.003.
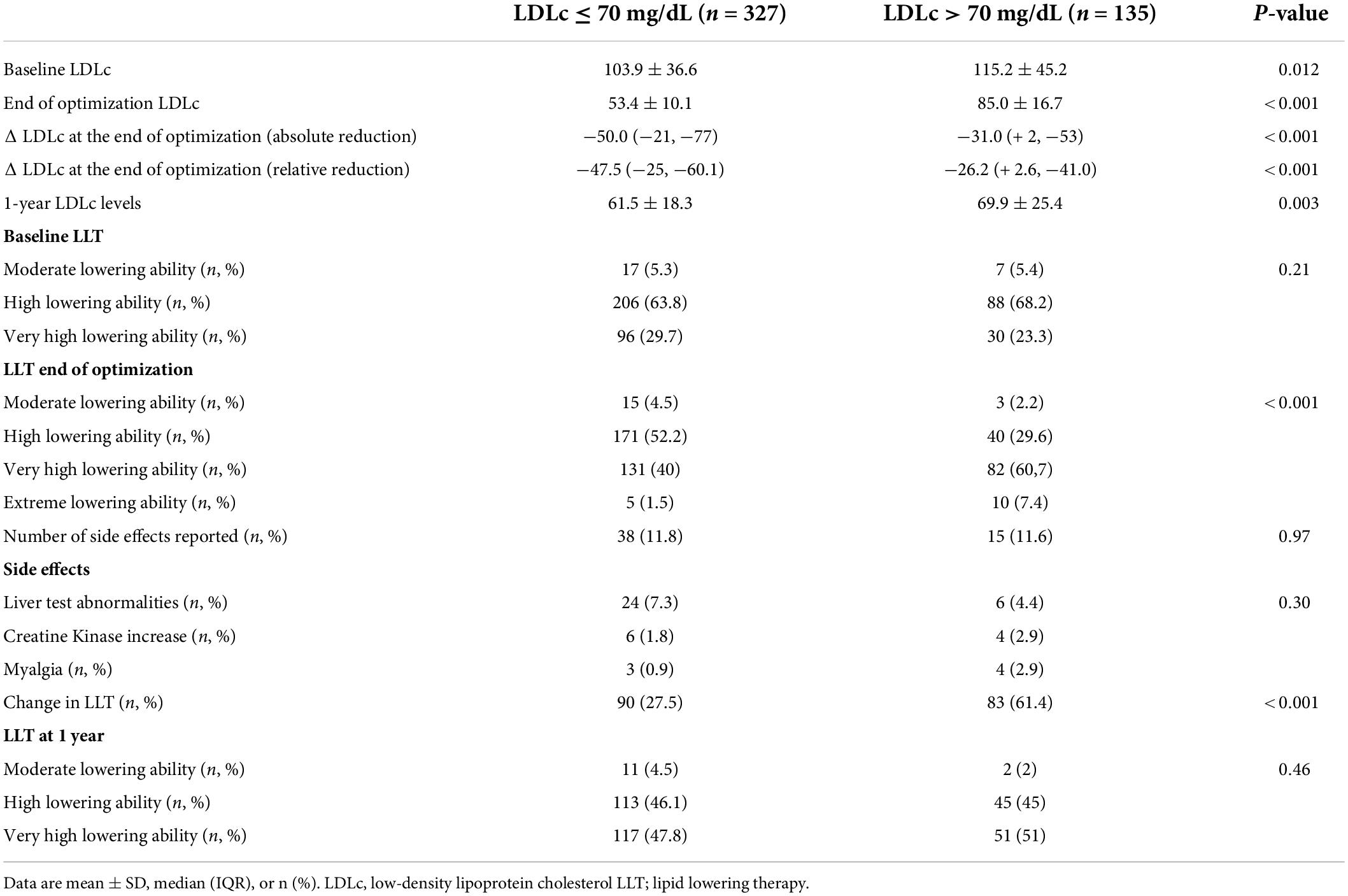
Table 2. Baseline LDL levels and medication changes according to LDL levels reached.
Side effects were relatively infrequent, with 53 reports (10.7%) of the cohort (patients could have more than one side effect reported). The more common side effects were abnormal asymptomatic liver tests, increased creatine-kinase levels, and myalgia. However, these side effects were rarely associated with LLT discontinuation. In most cases, side effects led to a change or temporary suspension in LLT in 4.3% of patients, without differences in both groups.
At 1-year follow-up, LDLc levels were measured by the local cardiologist or primary care physician in 342 (68.8%) of the whole cohort of 497 patients. In this group, 71.1% of patients had LDLc levels ≤ 70 mg/dL. Interestingly, 77.4% of patients with LDL ≤ 70 mg/dL at the end of optimization still had LDL levels ≤ 70 mg/dL at 1-year follow-up, whereas 59.6% of patients who did not reach LDLc ≤ 70 mg/dL did so at 1 year.
At a median follow-up of 30 (p25–75: 21–38) months, patients who achieved an LDLc ≤ 70 mg/dL after the optimization protocol had a numerically lower incidence of myocardial infarction [12 (3.6%) patients vs. 10 (7.5%), p = 0.08], need of new revascularization [22 (6.7%) patients vs. 10 (7.5%), p = 0.77), death (12 (3.6%) patients vs. 8 (6%), p = 0.27], and the composite end-point that comprised the 3 outcomes [33 (10%) vs. 22 (16.4%), p = 0.054] compared to those who did not achieve an LDLc ≤ 70 mg/dL.
Our study showed that an intensive, structured, mHealth post-discharge follow-up plan to optimize the lipid-lowering pharmacotherapy was associated with achieving a target LDLc ≤ 70 mg/dL in 70.7% of patients after an acute coronary syndrome (ACS). Reduction and achievement of LDLc target value were obtained early (between 6 and 12 weeks after the ACS) as recommended in the literature (16). It is also important to emphasize that the intervention was carried out using low-cost phone-based telemedicine techniques (mHealth) that facilitate its implementation and patient follow-up. The use of mHealth might explain why less than 8% of the patients did not adhere to follow-up.
Considering the few significant baseline characteristics differences between the LDLc ≤ 70 mg/dL and LDLc > 70 mg/dL groups, these differences did not allow us to identify those patients who would achieve proper LDLc control. It is worth mentioning that the percentage of patients achieving LDLc ≤ 70 mg/dL in this real-life study is even better than the results we obtained in a previous randomized study in which we used the same strategy, where an LDLc ≤ 70 mg/dL was achieved in 62% of the patients (10). Moreover, these results contrast positively with the poor results described in our hospital before implementing the study intervention (4). This insufficient control of dyslipidemia in very high-risk patients coincides with that described more recently in the literature. The ESC-EORP Euroaspire V survey performed in 27 European countries showed that the prevalence of LDLc ≤ 70 mg/dL in the entire cohort was 30% (5). Similar findings were found in a retrospective analysis of patients with ACS in Finland, where two-thirds of patients on statin therapy did not achieve the LDLc level target recommended by the guidelines (6). According to these data, our strategy could more than double the number of patients with adequate LDLc level control after a hospitalization due to IHD.
The most recent ESC/EAS guidelines for the management of dyslipidemias published in 2019 advise an LDLc < 55 mg/dL for high and very high-risk patients. The recommendations regarding the treatment goals for LDLc are based in the studies that have shown that the lower the LDLc level the better (17). These guidelines were not published during the performance of our study. In our cohort, 34.7% of the patients achieved an LDLc < 55 mg/dL. It is worth noting that it was not the target level of our study and, thus, there was some room for LLT optimization. This result improves that reported in the DA VINCI study; being one of the first comparative analyses evaluating 2019 risk-based goal attainment, showed that three-quarters of patients did not meet their 2019 LDLc goals (18).
The inability to achieve an LDLc level ≤ 70 mg/dl was not due to therapeutic inertia. Intensifications or treatment changes were done in 64% of the patients. When changes were not made, patients were already on the maximum dose of oral treatment, did not tolerate a higher dose or did not meet the local criteria for using PCSK9 inhibitors. This intensification effort is superior to the ones described in the literature. The GOULD prospective observational registry study was carried out simultaneously in the United States. A total of 5,006 patients with established atherosclerotic cardiovascular disease were enrolled. Surprisingly, only 17% had LLT intensification after 2 years, while two-thirds remained at an LDLc level > 70 mg/dL (19). Another important finding in our study is that 95% of the patients at the end of the optimization period were treated with drugs included in the high, very high, or extreme lipid-lowering ability groups. In the register published by Navar et al., of almost 3,297 patients analyzed, only 47% of the patients who required secondary prevention were treated with the appropriate intensity of treatment (20). One of the hypotheses that may justify not achieving an optimal decrease in LDLc, despite treatment is the described lack of response to statin treatment. A meta-analysis of genome-wide association studies showed that two loci of the genome are responsible for about 5% of the variation in an individual’s response to statin treatment (21). The JUPITER study highlights that 43% of high-risk patients had an LDLc reduction < 50 and 11% showed no reduction or even an increase in LDLc with statin treatment (22).
Large cardiovascular outcomes trials showed a prognostic benefit with PCSK9 inhibitors monoclonal antibodies (23, 24), and it has been estimated that 30% of patients could be candidates of PCSK9 inhibitors (25). However, the use of PCSK9 inhibitors in our study was low due to prescription restrictions in our country. PCSK9 inhibition obtains further lowering of LDLc beyond that achieved with statin therapy and cholesterol absorption inhibitors; an incremental reduction in LDLc of 50% from baseline has been shown (26). Knowing that the LDLc levels in the group with LDLc > 70 mg/dL were 85.0 ± 16.7 mg/dL and the hypothetical additional reduction of 50%, we theorized that we could have even achieved 100% of patients with LDLc target levels if we had been allowed to expand the use of PCSK9 inhibitors.
Numerous studies with lipid-lowering drugs have shown that the reduction of LDLc levels translates into a reduction in cardiovascular events, giving rise to the current recommendations in secondary prevention (17). We saw that patients who achieved an LDLc ≤ 70 mg/dL after the optimization protocol had numerically fewer clinical endpoints. However, it is important to remark that the study was underpowered to detect hard endpoint due to the relatively small sample size and the number of events.
One of the reasons that might limit LLT is side effects. Some physicians and patients might be reluctant to begin or maintain statins, most commonly because of perceived side effects that are not confirmed (i.e., the nocebo effect) (27). However, statins are generally well-tolerated drugs (25). 11% of the patients had any side effects in our cohort, with no significant differences between the LDLc group ≤ 70 mg/dL and the LDLc group > 70 mg/dL. The most frequent side effect was the liver tests abnormalities (79%), followed by an increase in creatinine kinase (26%) and finally myalgias (18%). These data are comparable to those previously described (15, 28).
After the treatment optimization period, the patient’s primary care general physician and primary care cardiologist performed the follow-up. We decided to analyze whether the good results achieved in the first 3 months were maintained after 12 months. Surprisingly, 31% of the patients did not have a follow-up blood test at month 12. In those patients who did have an LDLc assessment at 1 year, 71.1% of the patients maintained an LDLc ≤ 70 mg/dl. This group comprises 77.4% of the patients who already had an LDLc ≤ 70 mg/dl initially and patients who had not reached this target level originally (59.6%). This percentage of patients with a target LDLc level after 12 months remains significantly higher than the results reported in the literature (4–6).
Our study used the simplest and most readily usable form of mHealth, such as telephone calls. We believe that it was a determining factor in the success of this follow-up protocol. A randomized study in Sweden (29) and a meta-analysis of randomized controlled trials (10) showed improved LDLc levels with mHealth.
As a single-center study, the results might not apply to other settings. Some of the patients were included retrospectively, potentially leading to bias. Still, given that all patients followed the same protocol and that the information was documented in the medical record, we believe that the risk of bias in this study is negligible.
An intensive, structured, mobile devices-based healthcare intervention after an ACS is associated with more than 70% of patients reaching the LDLc levels recommended by the clinical guidelines. This strategy uses low-cost and easy-to-apply telemedicine techniques that can be replicated in various clinical settings.
The original contributions presented in this study are included in the article/Supplementary material, further inquiries can be directed to the corresponding author.
The patients/participants prospectively included in the study provided their written informed consent. The patients/participants included retrospectively did not require informed consent after evaluation by the Research Ethics Committee of the Hospital del Mar.
SR-B: conceptualization and writing original draft preparation. SR-B and NF: methodology, project administration, and validation. NF: formal analysis and writing – review and editing. SR-B, NB, CI, NF, and NR: investigation. IC-A, MV, DM, ML, LR, SR-B, and NF: data curation. NB, CI, IC-A, DM, MV, ML, NR, LR, JM-A, and MC: visualization. NF, JM-A, and MC: supervision. All authors contributed to the article and approved the submitted version.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fcvm.2022.916031/full#supplementary-material
SUPPLEMENTARY FIGURE 1 | Lipid-lowering treatment optimization algorithm.
1. Visseren FLJ, Mach F, Smulders YM, Carballo D, Koskinas KC, Bäck M, et al. 2021 ESC guidelines on cardiovascular disease prevention in clinical practice. Eur Heart J. (2021) 42:3227–337. doi: 10.1093/eurheartj/ehab484
2. Wood DA, Kotseva K, Connolly S, Jennings C, Mead A, Euroaction Study Group, et al. Nurse-coordinated multidisciplinary, family-based cardiovascular disease prevention programme (EUROACTION) for patients with coronary heart disease and asymptomatic individuals at high risk of cardiovascular disease: a paired, cluster-randomised controlled trial. Lancet. (2008) 371:1999–2012. doi: 10.1016/S0140-6736(08)60868-5
3. Cannon CP, Braunwald E, McCabe CH, Rader DJ, Rouleau JL, Belder R, et al. Intensive versus moderate lipid lowering with statins after acute coronary syndromes. N Engl J Med. (2004) 350:1495–504. doi: 10.1056/NEJMoa040583
4. Ribas N, García-García C, Meroño O, Recasens L, Pérez-Fernández S, Bazán V, et al. Secondary prevention strategies after an acute ST-segment elevation myocardial infarction in the AMI code era: beyond myocardial mechanical reperfusion. BMC Cardiovasc Disord. (2017) 17:54. doi: 10.1186/s12872-017-0493-6
5. De Backer G, Jankowski P, Kotseva K, Mirrakhimov E, Reiner Ž, Rydén L, et al. Management of dyslipidaemia in patients with coronary heart disease: results from the ESC-EORP EUROASPIRE V survey in 27 countries. Atherosclerosis. (2019) 285:135–46. doi: 10.1016/j.atherosclerosis.2019.03.014
6. Leskelä RL, Torvinen A, Rissanen TT, Virtanen V, Herse F, Nuutinen M, et al. Outcomes of lipid control in secondary prevention of coronary artery disease in Finland: a 24-month follow-up after acute coronary syndrome. Atherosclerosis. (2020) 296:4–10. doi: 10.1016/j.atherosclerosis.2020.01.018
7. Lázaro P, Murga N, Aguilar D, Hernández-Presa MA. Therapeutic inertia in the outpatient management of dyslipidemia in patients with ischemic heart disease. The inertia study. Rev Esp Cardiol. (2010) 63:1428–37. doi: 10.1016/s1885-5857(10)70277-2
8. Fitzsimons D, Stȩpińska J, Kerins M, Piepoli MF, Hill L, Nuutinen M, et al. Secondary prevention and cardiovascular care across Europe: a survey of European society of cardiology members’ views. Eur J Cardiovasc Nurs. (2020) 19:201–11. doi: 10.1177/1474515119877999
9. Akter S, Roy P. mHealth – an ultimate platformto serve the unserved. Yearbook Med Inform. (2010) 1:94–100.
10. Akbari M, Lankarani KB, Naghibzadeh-Tahami A, Tabrizi R, Honarvar B, Kolahdooz F, et al. The effects of mobile health interventions on lipid profiles among patients with metabolic syndrome and related disorders: a systematic review and meta-analysis of randomized controlled trials. Diabetes Metab Syndr. (2019) 13:1949–55. doi: 10.1016/j.dsx.2019.04.011
11. Ruiz-Bustillo S, Ivern C, Badosa N, Farre N, Marco E, Bruguera J, et al. Efficacy of a nurse-led lipid-lowering secondary prevention intervention in patients hospitalized for ischemic heart disease: a pilot randomized controlled trial. Eur J Cardiovasc Nurs. (2019) 18:366–74. doi: 10.1177/1474515119831511
12. Masana L, Pedro-Botet J, Civeira F. IMPROVE-IT clinical implications. Should the “high-intensity cholesterol-lowering therapy” strategy replace the “high-intensity statin therapy”? Atherosclerosis. (2015) 240:161–2. doi: 10.1016/j.atherosclerosis.2015.03.002
13. Escobar C, Anguita M, Arrarte V, Barrios V, Cequier A, Cosín-Sales J, et al. Recommendations to improve lipid control. Consensus document of the Spanish society of cardiology. Rev Esp Cardiol. (2020) 73:161–7. doi: 10.1016/j.rec.2019.08.012
14. Agencia Española de Medicamentos y Productos Sanitarios. Informe de Posicionamiento Terapéutico de Evolocumab en Hipercolesterolemia. Fecha de Adopción de la Actualización de la Fase I del Informe Por el GCPT. Madrid: Agencia Española de Medicamentos y Productos Sanitarios (2020).
15. Piepoli MF, Hoes AW, Agewall S, Albus C, Brotons C, Catapano AL, et al. ESC scientific document group. 2016 European guidelines on cardiovascular disease prevention in clinical practice: the sixth joint task force of the European society of cardiology and other societies on cardiovascular disease prevention in clinical practice (constituted by representatives of 10 societies and by invited experts). Developed with the special contribution of the European association for cardiovascular prevention & rehabilitation (EACPR). Eur Heart J. (2016) 37:2315–81. doi: 10.1093/eurheartj/ehw106
16. Schiele F, Farnier M, Krempf M, Bruckert E, Ferrières J. A consensus statement on lipid management after acute coronary syndrome. Eur Heart J Acute Cardiovasc Care. (2018) 7:532–43. doi: 10.1177/2048872616679791
17. Mach F, Baigent C, Catapano AL, Koskinas KC, Casula M, Badimon L, et al. 2019 ESC/EAS guidelines for the management of dyslipidaemias: lipid modification to reduce cardiovascular risk. Eur Heart J. (2020) 41:111–88. doi: 10.1093/eurheartj/ehz455
18. Vrablik M, Seifert B, Parkhomenko A, Banach M, Jóźwiak JJ, Kiss RG, et al. Lipid-lowering therapy use in primary and secondary care in central and Eastern Europe: DA VINCI observational study. Atherosclerosis. (2021) 334:66–75. doi: 10.1016/j.atherosclerosis.2021.08.035
19. Cannon CP, de Lemos JA, Rosenson RS, Ballantyne CM, Liu Y, Gao Q, et al. Use of lipid-lowering therapies over 2 years in GOULD, a registry of patients with atherosclerotic cardiovascular disease in the US. JAMA Cardiol. (2021) 6:1–9. doi: 10.1001/jamacardio.2021.1810
20. Navar AM, Wang TY, Li S, Robinson JG, Goldberg AC, Virani S, et al. Lipid management in contemporary community practice: results from the provider assessment of lipid management (PALM) registry. Am Heart J. (2017) 193:84–92. doi: 10.1016/j.ahj.2017.08.005
21. Postmus I, Trompet S, Deshmukh HA, Barnes MR, Jóźwiak JJ, Kiss RG, et al. Pharmacogenetic meta-analysis of genome-wide association studies of LDL cholesterol response to statins. Nat Commun. (2014) 5:5068. doi: 10.1038/ncomms6068
22. Ridker PM, Mora S, Rose L, Jupiter Trial Study Group. Percent reduction in LDL cholesterol following high-intensity statin therapy: potential implications for guidelines and for the prescription of emerging lipid-lowering agents. Eur Heart J. (2016) 37:1373–9. doi: 10.1093/eurheartj/ehw046
23. Sabatine MS, Giugliano RP, Keech AC, Honarpour N, Wiviott SD, Murphy SA, et al. FOURIER Steering Committee and Investigators. Evolocumab and clinical outcomes in patients with cardiovascular disease. N Engl J Med. (2017) 376:1713–22. doi: 10.1056/NEJMoa1615664
24. Schwartz GG, Steg PG, Szarek M, Bhatt DL, Bittner VA, Diaz R, et al. ODYSSEY OUTCOMES committees and Investigators. Alirocumab and cardiovascular outcomes after acute coronary syndrome. N Engl J Med. (2018) 379:2097–107. doi: 10.1056/NEJMoa1801174
25. Elamin AFM, Grafton-Clarke C, Chen KW, Obafemi T, Luvai A, Katira R, et al. Potential use of PCSK9 inhibitors as a secondary preventative measure for cardiovascular disease following acute coronary syndrome: a UK real-world study. Postgrad Med J. (2019) 95:61–6. doi: 10.1136/postgradmedj-2018-136171
26. Furtado RHM, Giugliano RP. What lessons have we learned and what remains to be clarified for PCSK9 inhibitors?. A review of FOURIER and ODYSSEY Outcomes Trials. Cardiol Ther. (2020) 9:59–73. doi: 10.1007/s40119-020-00163-w
27. Howard JP, Wood FA, Finegold JA, Nowbar AN, Thompson DM, Arnold AD, et al. Side effect patterns in a crossover trial of statin, placebo, and no treatment. J Am Coll Cardiol. (2021) 78:1210–22. doi: 10.1016/j.jacc.2021.07.022
28. Collins R, Reith C, Emberson J, Armitage J, Baigent C, Blackwell L, et al. Interpretation of the evidence for the efficacy and safety of statin therapy. Lancet. (2016) 388:2532–61. doi: 10.1016/S0140-6736(16)31357-5
Keywords: ischemic heart disease, secondary prevention, cardiovascular risk factors, lipid-lowering therapy, mobile devices-based healthcare
Citation: Ruiz-Bustillo S, Badosa N, Cabrera-Aguilera I, Ivern C, Llagostera M, Mojón D, Vicente M, Ribas N, Recasens L, Martí-Almor J, Cladellas M and Farré N (2022) An intensive, structured, mobile devices-based healthcare intervention to optimize the lipid-lowering therapy improves lipid control after an acute coronary syndrome. Front. Cardiovasc. Med. 9:916031. doi: 10.3389/fcvm.2022.916031
Received: 08 April 2022; Accepted: 08 July 2022;
Published: 26 July 2022.
Edited by:
Nathalie Pamir, Oregon Health and Science University, United StatesReviewed by:
Federico Vancheri, S. Elia Hospital, ItalyCopyright © 2022 Ruiz-Bustillo, Badosa, Cabrera-Aguilera, Ivern, Llagostera, Mojón, Vicente, Ribas, Recasens, Martí-Almor, Cladellas and Farré. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Sonia Ruiz-Bustillo, c3J1aXpAcHNtYXIuY2F0
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.