 Dashuai Wang
Dashuai Wang Yang Lu2†
Yang Lu2† Xiaofan Huang
Xiaofan Huang Xinling Du
Xinling Du Fei Xie
Fei Xie
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
REVIEW article
Front. Cardiovasc. Med. , 30 June 2022
Sec. Cardiovascular Surgery
Volume 9 - 2022 | https://doi.org/10.3389/fcvm.2022.911878
Postoperative pneumonia (POP) is prevalent in patients undergoing cardiovascular surgery, associated with poor clinical outcomes, prolonged hospital stay and increased medical costs. This article aims to clarify the incidence, risk factors, and interventions for POP after cardiovascular surgery. A comprehensive literature search was performed to identify previous reports involving POP after cardiovascular surgery. Current situation, predictors and preventive measures on the development of POP were collected and summarized. Many studies showed that POP was prevalent in various cardiovascular surgical types, and predictors varied in different studies, including advanced age, smoking, chronic lung disease, chronic kidney disease, cardiac surgery history, cardiac function, anemia, body mass index, diabetes mellitus, surgical types, cardiopulmonary bypass time, blood transfusion, duration of mechanical ventilation, repeated endotracheal intubation, and some other risk factors. At the same time, several targeted interventions have been widely reported to be effective to reduce the risk of POP and improve prognosis, including preoperative respiratory physiotherapy, oral care and subglottic secretion drainage. Through the review of the current status, risk factors and intervention measures, this article may play an important role in clinical prevention and treatment of POP after cardiovascular surgery.
With the improvement of economic conditions and living standards, the incidence of cardiovascular disease has increased year by year, with high morbidity and mortality (1). Although considerable progress have been made in diagnostic techniques, medical options and interventional therapy over the past decades, surgical operation remains one of the most important treatments (2, 3). However, the circumstances of the overall survival after cardiovascular surgery is hardly optimistic and a high proportion of patients may develop various complications (4).
Postoperative pneumonia (POP) is one of the most common pulmonary complications after cardiovascular surgery, related to poor clinical outcomes, prolonged hospital stay and increased medical costs (5, 6). The incidence of POP varies greatly in previous reports due to various definitions and surgical patients in different studies (7–10). Several studies aimed to identify predictors for the development of POP after cardiovascular surgery have been conducted and some predictors have been reported, however, those risk factors reported in different studies varied greatly (11, 12). In addition, studies focused on the prevention and treatment of POP have been carried out and several interventions have been widely reported to be effective to reduce the incidence of POP and resultant adverse outcomes (13–16). Recently, several related studies conducted in patients undergoing cardiovascular surgery have been reported, nonetheless, a comprehensive review of the current status, risk factors, and interventions for cardiovascular surgery is still lacking.
Understanding the current status and clarifying the risk factors for the development of POP may play an important guiding role for early recognition, targeted prevention and treatment. The aims of this study was to clarify the incidence, risk factors, and interventions for POP after cardiovascular surgery through comprehensive literature search, and provide new ideas for clinical prevention and treatment.
We conducted a literature search of peer-reviewed publications to obtain a comprehensive review of published data on POP after cardiovascular surgery using the Cochrane, PubMed and EMBASE databases. These sources were searched up to the end of April 2022. Search terms used included a variety of synonyms and types of surgical approach, as well as pneumonia. Article titles and abstracts were screened and potentially valuable articles were read in full text. The review included only English language articles, and studies in other languages were excluded. A data extraction form was used to capture key issues in the articles. We compiled data pertaining to the number of patients, anatomical procedure sites, pneumonia rates, risk factors, preventative measures, and interventions. Primary researches, systematic reviews, studies relevant to guideline implementation and can be transferable to clinical practice were eligible for inclusion. Where appropriate the findings were also supported by additional theoretical literature. The main contents of this study have been summarized in Figure 1.
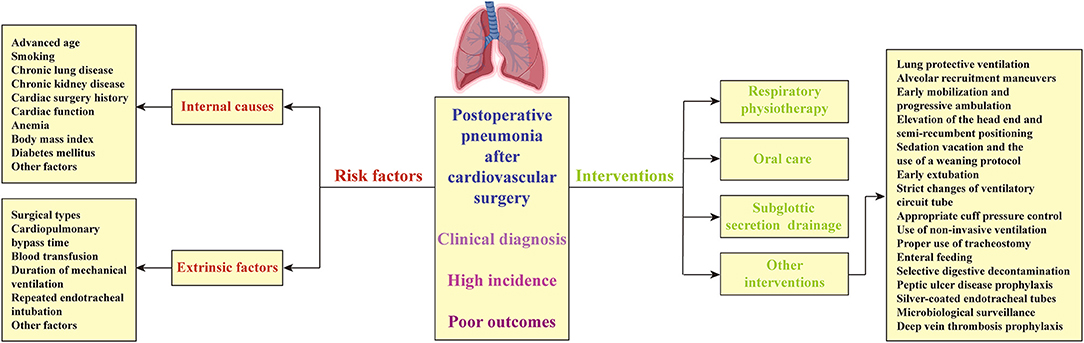
Figure 1. Incidence, risk factors and interventions of pneumonia after cardiovascular surgery.
POP is one of the most common pulmonary complications after cardiovascular surgery. According to the recommendation of clinical practice guidelines, the clinical diagnosis of pneumonia is mainly based on objective indicators such as clinical syndromes and chest imaging changes (17, 18). Generally speaking, POP can be diagnosed when patients have cough, sputum or sputum character changes after cardiovascular surgery, chest ray or computerized tomographic scanning shows new or progressive infiltration, consolidation or ground glass shadow, and meet two or more of the following three conditions at the same time: (1) body temperature rises to more than 38°C or falls below 36°C, (2) white blood cell count >10 × 109/L or <4 × 109/L, and (3) purulent secretions in the lower respiratory tract. On the basis of clinical diagnosis, etiological diagnosis can be established if one or more of the following conditions are met: (1) pathogens can be cultured in qualified lower respiratory secretions, bronchoalveolar lavage fluid or bronchoscopic anti-contamination brushes and are consistent with clinical manifestations, (2) pathogens can be seen by microscopy, cytopathology or in the lung tissues and relevant evidence of tissue damage exists, (3) history of epidemiological exposure to respiratory viruses and isolation of virus, detection of viral antigen or positive nucleic acid test.
The incidence of POP reported in previous literature varied greatly due to various surgical populations, from 2 to 15% in most of the studies (7, 9, 19, 20). The most frequently reported studies for POP were conducted in patients undergoing surgery for valvular and coronary disease, the incidence of which was mostly between 2.1–8.2% (7, 9). However, POP most frequently develops following surgery for aortic dissection, with an incidence rate of up to 36.9% in the literature (21). Although the incidence of POP varies in different studies, researchers find that the development of POP can significantly prolong the duration of intensive care unit (ICU) and hospital stay, increase the morbidity and mortality, aggravate patient's physical and mental pains, and increase their medical burden (6, 12, 22, 23).
Advanced age has been widely reported to be associated with the development of POP after cardiovascular surgery (10, 19, 20, 24–26). In a prospective multicenter study, Ailawadi et al. found that the risk of POP after cardiac surgery increased significantly with age, presenting a dose-effect relationship (27). Kilic et al. found that compared to patients younger than 65 years, the risk of POP after cardiac surgery increased 1.4-fold in patients older than 65 years (24). For patients older than 70 years, Hortal et al. found a 3.5-fold increased risk of POP on the day of surgery, and 16.8 times for patients requiring more than 3 days of postoperative mechanical ventilation (28). In addition, advanced age has been reported to be a strong predictor of postoperative multidrug-resistant bacterial infection, closely associated with an increased risk of in-hospital mortality (29).
With the increase of patient's age, the function of various organs gradually declines, the risk of various comorbidities increases, the body's defense mechanism and immune function weaken, together resulting in a higher risk of POP after cardiovascular surgery. Compared with young patients, elderly patients have weakened cough reflex, decreased airway self-purification ability, weakened respiratory muscle strength, reduced pulmonary ventilation and air-exchanging functions, which make pathogens easier to move down the respiratory tract and then cause infection (30). In addition, the ability of elderly patients to metabolize drugs and nutrients is weakened, the ability to resist pathogenic invasion becomes poorer, the tolerance to pain, surgery, trauma and external stimuli is weakened, and the response to changes decreases, which may significantly increase the risk of POP in elderly patients. Therefore, additional attention should be given to older surgical patients to timely deal with abnormal conditions, and some targeted measures should be given in advance to prevent and reduce the risk of POP.
Smoking has been identified as an independent predictor for POP after cardiovascular surgery in previous studies, which may be due to the fact that smoking can increase the risk of airway pathogens colonization (7, 19, 20). Kinlin et al. found that patients with a history of smoking had a 1.79-fold increased risk of POP after cardiac surgery, which is very close to the findings of Wang et al. (7, 19). Saxena et al. found that compared with patients who had quitted smoking or who had never smoked, current smokers had a 2.05-fold increased risk of POP after coronary artery bypass grafting (CABG) (31). Al-sarraf et al. found that compared with patients who quitted smoking for more than 4 weeks, current smokers had a significantly higher risk of pulmonary complications after CABG (32). However, compared with patients who had never smoked, the risk of POP was not significantly increased in patients who quitted for more than 4 weeks. Guidelines recommend that all smokers should receive inpatient education counseling when treated with CABG and hospitals should provide appropriate smoking cessation strategies for these patients (33). Active preoperative smoking cessation counseling and treatment can not only reduce the risk of postoperative respiratory complications, but also have a certain protective effect on the long-term postoperative survival. It has been reported that patients who quitted smoking for more than a week before surgery were 10 times more likely to remain smoking cessation within 1 year after CABG and had a significantly improved 5-year survival rate postoperatively (34, 35). Therefore, in clinical practice, not only high-risk patients, but also the general public should be encouraged to quit smoking to pursue long-term primary prevention and public health protection (36).
Chronic lung disease is another important predictor for POP after cardiovascular surgery, which has been extensively reported in various literature (10, 24, 25). Both Kilic et al. and Strobel et al. found that the risk of POP after cardiac surgery increased significantly with increasing severity of chronic lung disease (10, 24). The findings of Wang et al. showed that patients with chronic obstructive pulmonary disease had a 2.1-fold increased risk of POP compared with patients with good respiratory conditions (19). A systematic review and meta-analysis conducted by Furukawa et al. found that preoperative inspiratory muscle training in adult patients undergoing cardiac surgery can significantly reduce the risk of POP and shorten the length of hospital stay (37). Therefore, preoperative respiratory optimization with respiratory physiotherapy may be a good option for patients undergoing elective cardiac surgery.
Renal insufficiency and chronic kidney disease have also been reported to be an independent risk factor for POP after cardiac surgery in previous literature (7, 19). Kinlin et al. found that patients with preoperative creatinine levels >1.2 mg/dL had a 1.6-fold increased risk of POP after CABG (7). Hortal et al. found that patients with preoperative creatinine levels >1.5 mg/dL had a 2.2-fold increased risk of POP after cardiac surgery (28). A series of studies by Wang et al. showed that patients with renal insufficiency had a 2.7-fold increased risk of POP after cardiac surgery, a 2.1-fold increased risk of POP after elective cardiac surgery, a 2.7-fold increased risk of POP after valve surgery, a 2.5-fold increased risk of POP after aortic dissection surgery, and the risk of POP increased with creatinine levels after redo cardiac surgery (8, 9, 19, 20, 26). Therefore, preoperative improvement of renal function may be a feasible strategy to reduce complications and improve prognosis in patients with renal dysfunction.
Patients with a history of cardiac surgery have a significantly increased risk of postoperative complications such as POP and in-hospital mortality, which has been confirmed in multiple studies (9, 19, 20, 26, 38). Compared with patients undergoing primary surgery, patients undergoing redo cardiac surgery tend to have poorer physical fitness and tolerance, more underlying diseases, more complicated anatomy and surgical operations. Therefore, the risk of postoperative adverse outcomes and death tends to be higher in this surgical population (38, 39). Hortal et al. found that the risk of POP increased 3 times in patients with cardiac surgery history (28). Kinlin et al. found that the risk of POP after CABG was 2.3 times higher in patients with previous internal mammary artery transplantation (7). Bianco et al. compared the underlying disease conditions between primary and redo cardiac surgery patients through a large propensity-matched cohort, finding that patients with cardiac surgery history had more comorbidities, more blood transfusion, longer mechanical ventilation, and higher postoperative mortality (39). Similar results were also obtained by Norton et al. who found that compared with primary surgery patients, patients undergoing redo cardiac surgery had older age, more underlying diseases, more complicated procedures, more intraoperative blood transfusion, and longer cardiopulmonary bypass time (40).
Poor cardiac function as an independent risk factor for POP after cardiac surgery has been demonstrated in numerous previous studies (5, 10, 24, 28, 41–43). Strobel et al. found that left ventricular ejection fraction was inversely associated with the risk of POP after CABG, which meant that the lower the left ventricular ejection fraction, the higher the risk of POP (10). In patients requiring intra-aortic balloon pumping, the risk of POP increased to 1.59 times. Hortal et al. found that the need for intraoperative inotropic support was identified as an independent risk factor for POP after cardiac surgery in the multivariate regression analysis (28). The risk of POP increased 2.2 times in patients with NYHA class IV, which was included as a predictor into their risk scoring model. Similar results were also obtained by Kilic et al. (24). In their study, the need for preoperative and intraoperative intra-aortic balloon pumping was identified as an independent risk factor and was included in their final risk prediction model, which was associated with a 2.01-fold increased risk of POP after cardiac surgery.
Preoperative anemia, low red blood cell count, low hemoglobin levels and low hematocrit have also been reported to be closely associated with the development of POP after cardiac surgery in previous literature (11, 12, 27, 44). Ailawadi et al. found that hemoglobin levels were inversely associated with the risk of POP after cardiac surgery and lower hemoglobin level was identified as an independent risk factor in the multivariate regression analysis (27). Similar results were also obtained by Strobel et al. who found that hematocrit was inversely associated with the risk of POP after CABG, and lower hematocrit was identified as a predictor for POP in their analysis (10). In a study by Wang et al. preoperative anemia was identified as an independent risk factor in multivariate regression analysis, with a 1.6-fold increased risk of POP compared with patients without that (20). Canet et al. obtained similar results in a cohort study, and the risk of POP reached 3 times higher in this population (45). As the largest amount of blood cells in human body, the main function of red blood cells is transporting oxygen and carbon dioxide, participating in acid-base balance regulation, and modulating the clearance of circulating immune complexes. Therefore, attention should be paid to strengthening nutrition, enhancing immunity and improving anemia for patients with preoperative anemia. In recent years, the research on the effect of preoperative hematocrit on blood transfusion has gradually increased, but the optimal threshold for transfusion remains to be further investigated (46). Meanwhile, additional attention should be paid to reducing intraoperative bleeding and close observation should be given to prevent the development of POP and other adverse outcomes (45).
BMI has been reported to be an independent predictor for POP after cardiovascular surgery in several previous studies (7, 20, 43). Xiao et al. found that the BMI of patients with POP after mitral valve replacement was significantly higher compared with patients without POP, and higher BMI was identified as an independent predictor for POP in the multivariate analysis (43). Wang et al. divided BMI into two groups based on a 24 kg/m2 boundary and found that BMI ≥ 24 kg/m2 was an independent risk factor for POP after cardiac surgery (20). However, Kinlin et al. had different findings in their study (7). They found that lower body weight was independently associated with the development of POP after cardiac surgery, with a 2.89-fold increased risk. In the results of Santos et al. the risk reached up to 9.8 times in patients with lower body weight (44). These findings suggest that whether overweight and obesity or underweight and wasting all increase the risk of postoperative complications such as POP after cardiac surgery. Thus, scientific and reasonable diet and proper exercise should be valued to maintain a fine body weight and shape and resultant health. In addition, a positive association between obesity and frailty has been found in previous studies, which was associated with higher risk of morbidity and mortality (47, 48). Therefore, preoperative assessment of frailty index in patients undergoing elective cardiac surgery may be instructive to some extent.
Diabetes mellitus has also been reported to be a risk factor for POP after cardiovascular surgery in some previous reports (10). Strobel et al. found that patients with diabetes mellitus had a 1.3-fold increased risk of POP after CABG (10). Similar results were also obtained by Wang et al. who found that the risk of POP after cardiac surgery increased to 1.4 times in patients with diabetes mellitus, and the risk increased to 2.1 times in patients undergoing heart valve surgery (9, 20). However, a systematic review and meta-analysis conducted by He et al. found that the association between diabetes mellitus and POP after cardiac surgery was not significant (12). The influence of preoperative level of glycosylated hemoglobin A1c and postoperative glycemic variability on major adverse outcomes following cardiac surgery has been reported in previous studies, which indicated that both had a predictive value for postoperative complications including POP (49–52). Therefore, good glycemic control for patients undergoing elective cardiac surgery may significantly reduce the risk of POP and other adverse outcomes.
In addition to those widely reported risk factors mentioned above, some of the following factors have also been reported to be associated with the development of POP after cardiovascular surgery in the literature, including hypertension, cerebrovascular disease, peripheral vascular disease, white blood cell count, platelet count, serum albumin levels, liver disease, pulmonary hypertension, steroid use, and re-intervention (10–12, 20, 21, 24, 27, 42, 53). The presence of these factors may increase the risk of POP and other adverse outcomes to some extent. Therefore, more attention should be paid to reducing the risk of postoperative adverse outcomes and improving prognosis in clinical practice.
Cardiovascular surgery as a whole contains numerous sub-types. The risk of various postoperative complications, the lengths of hospitalization and the risk of postoperative death may vary greatly among different surgical types due to different operation procedures, surgical time and complexity of different diseases (8, 9). According to clinical experience and previous reports, the risk of POP after multiple types of combined cardiovascular surgery is higher than that of single type of cardiovascular surgery. Wang et al. found that compared with patients undergoing isolated heart valve surgery, the risk of POP increased 3.2 times in patients undergoing combined CABG, 2.9 times in patients undergoing combined aortic surgery, and 4.8 times in patients undergoing combined coronary and aortic surgery (9). For isolated type of cardiovascular surgery, aortic dissection surgery has a much higher risk of POP and other postoperative complications than other surgical types due to its more complicated operation, greater trauma and longer operation time (8). In the findings of Hortal et al. ascending aorta surgery was an independent risk factor for POP, with a 6.2-fold increased risk compared with other types of cardiovascular surgery (53). In the analysis of Wang et al. the probability of POP after Stanford type A aortic dissection was 34.6%, and the rate reached up to 36.9% in the study of Yao et al. (8, 21). Meanwhile, compared with elective cardiac surgery, patients undergoing emergency surgery may have a significantly increased risk of POP (28, 53). In the findings of Strobel et al. patients undergoing emergency surgery had a 2.2-fold increased risk of POP after CABG (10). In addition, patients undergoing surgeries for end stage heart failure such as left ventricular assist device insertion and heart transplantation had ultrahigh risk of developing POP (54–56). A single-center retrospective study conducted by Pons et al. reported that pneumonia was the most common infectious complications postoperatively, which developed in 52.5% of the patients undergoing heart transplantation (57).
CPB time has been widely reported to be associated with the development of POP after cardiovascular surgery in previous studies (12, 19, 24, 58). In a meta-analysis and systematic review, He et al. concluded that prolonged duration of CPB was significantly associated with an increased risk of POP (12). In the results of Olga et al. CPB time was positively associated with the risk of POP after cardiac surgery, and the risk increased by 1% for each additional minute (58). Kilic et al. found that patients on CPB for more than 100 min had a 1.7-fold increased risk nt of various complications and aof POP after cardiac surgery (24). Allou et al. also reported a positive relationship between CPB duration and POP after cardiac surgery, and the risk of POP increased significantly with the extension of CPB duration in their multivariate analysis (41). After selection and inclusion of interaction between variables, the interaction between CPB time >60 min and intraoperative red blood cell transfusion was identified as an independent predictor and included in the final risk model, and the risk of POP increased to 2.98 times in these patients.
CPB can reduce lung compliance and lead to pulmonary dysfunction by inducing ischemia-reperfusion injury and systemic inflammatory response (59). However, the importance of CPB in the developmedverse outcomes is often underestimated or even ignored by some cardiac surgeons. In recent years, minimally invasive CPB (MICPB) has been introduced clinically, and the use of MICPB has been reported to significantly improve clinical outcomes (60). MICPB is a closed system that can provide optimal intraoperative perfusion, with near-normal systemic vascular resistance and higher mean arterial pressure, which may reduce the need for vasoactive drugs. In the past few years, this system has developed into the best perfusion technique in clinical practice, however, in the field of science and technology, many trials, improvement and research work are still being conducted to further improve the biocompatibility of MICPB systems and reduce adverse effects (61). Current clinical evidence has demonstrated that MICPB is superior to conventional CPB in reducing hemodilution and better preserving hematocrit, which may reduce the need for perioperative blood transfusion. In addition, this system can significantly attenuate systemic inflammatory response and protect end-organ function (61). A large meta-analysis and systematic review of randomized controlled trials conducted by Anastasiadis et al. showed that the use of MICPB can significantly reduce the morbidity of various complications and mortality after cardiac surgery compared with conventional CPB (62). Recently, they have also introduced the concept of a “more physiologic” cardiac surgery to emphasize the need of further improvement of patient outcomes (63).
The amount of blood transfusion has also been widely reported to be an independent risk factor for POP in patients undergoing cardiovascular surgery (19). Although the transfusion of blood and blood products is an important guarantee for the success of the operation and can be lifesaving in cardiovascular surgery, there is increasing evidence that massive blood transfusion may significantly increase the risk of adverse outcomes (64–67). Likosky et al. conducted a large prospective multicenter cohort study to explore the relationship between blood transfusion and POP in patients undergoing CABG, finding that patients who received blood transfusion had a 3.4-fold increased risk of POP, and the risk increased significantly with each additional unit of red blood cells transfused, showing a dose-effect relationship (68). The results of Wang et al. showed that patients who were intraoperatively transfused had a 3.5-fold increased risk of POP after general cardiac surgery, a 2.8-fold increased risk in valve surgery, and the risk increased by 23.2% with each additional unit of red blood cells transfused in aortic dissection surgery, showing a dose-effect relationship (8, 9, 20). However, the results of a multicenter study conducted by Lapar et al. showed that limiting the amount of perioperative blood transfusion can not only reduce the risk of mortality and postoperative complications such as POP, but also greatly reduce the medical burden (69). Therefore, in clinical practice, unnecessary blood transfusion should be avoided, blood transfusion indications should be strictly controlled, and autologous blood transfusion can be used when conditions permit, so as to reduce the risk of POP and other blood transfusion-related diseases (70, 71). At the same time, proper fluid supplementation before operation, rapid and precise operation during operation, improvement of surgical techniques and hemostasis means, and shortening of operation time may be helpful for effective control of bleeding and resultant less need for transfusion (24).
The association between allogeneic blood transfusion and increased risk of POP can be partly explained by changes in immune function (72, 73). In addition, longer storage time of blood and blood products has also been reported to be associated with an increased risk of POP and worse prognosis, which may be due to the reduced oxygen-carrying capacity of red blood cells and transfusion-related inflammatory responses (74–76). Although massive blood transfusion is often due to massive blood loss and anemia in clinical practice, according to the recommendations of clinical practice guidelines, restrictive blood transfusion strategies are still strongly recommended to reduce the risk of postoperative complications and improve prognosis, even in major operations such as cardiovascular surgery (77–79). In addition, the exploration of blood transfusion replacement therapy and autologous blood transfusion may be new research directions in future work (80).
The use of ventilator and mechanical ventilation are indispensable life support techniques for cardiovascular surgery. However, prolonged mechanical ventilation has been reported to be strongly associated with an increased risk of POP in many studies, which is associated with the damage to the defense mechanism of the respiratory system caused by tracheal intubation (5, 42, 53, 81, 82). The use of endotracheal intubation and ventilator changes the normal airway structure and damages the natural barrier of the respiratory system, resulting in a weakened cough reflex, disappearance of the gag reflex, weakened ciliary movement, reduced ability to clear secretions, and damage to the defenses of the upper respiratory tract. These changes make the pathogens in the upper respiratory tract such as the oral cavity and throat more likely to migrate to the lower respiratory tract, and then colonize and breed in the distal bronchi and lung tissue, thereby leading to the development of POP. It has been reported that the risk of POP increases by 1–3% for each additional day of mechanical ventilation, and endotracheal intubation should be removed as soon as possible when the extubation conditions are met (83, 84). In addition, prolonged mechanical ventilation can cause diaphragmatic atrophy, which may significantly increase the risk of POP and affect prognosis (85).
Hortal et al. found that the duration of mechanical ventilation was an independent predictor for POP after cardiac surgery in the multivariate analysis, and the risk increased significantly with the extension of mechanical ventilation, showing a dose-effect relationship (28). Bouza et al. found that patients who were mechanically ventilated for more than 96 h had a 12.3-fold increased risk of POP after cardiac surgery, and the in-hospital mortality increased significantly in these patients (42). In a meta-analysis and systematic review conducted by He et al. the overall incidence of POP after cardiac surgery was 6.37%, however, the incidence reach 35.2% in patients mechanically ventilated for more than 48 h, which demonstrated that prolonged mechanical ventilation was significantly associated with an increased risk of POP (12). Therefore, close attention should be paid to the recovery of respiratory function and more stringent ventilation strategies should be implemented, so as to shorten the duration of mechanical ventilation, reduce the risk of postoperative complications, and improve prognosis.
Repeated tracheal intubation has also been identified as an independent risk factor for POP after cardiovascular surgery in the literature (86–90). Tracheal intubation may inevitably destroy the integrity of the airway mucosa, and the operation of reintubation can cause more damage to the respiratory tract, thus can significantly increase the risk of POP. Sheng et al. found that reintubation was an independent predictor for POP after cardiac surgery, with an 8.9-fold increased risk in patients who were reintubated compared with patients without reintubation (81). In the results of Hortal et al. the risk of POP was as high as 14.3 times in patients reintubated (28). In a systematic review and meta-analysis by Gao et al. they found that reintubation significantly increased the risk of POP and in-hospital mortality, and the risk of extubation failure after cardiac surgery increased significantly compared with other surgical types (89). He et al. obtained similar results and concluded that reintubation was significantly associated with the development of POP after cardiac surgery (12). Garcia et al. found that appropriate application of non-invasive ventilation after extubation could avoid the respiratory tract injury caused by reintubation and consequent increased risk of POP and death, however, non-invasive ventilation should be performed under strict conditions and standards (91).
Previous studies have shown that preoperative respiratory physiotherapy can significantly reduce the incidence of postoperative complications such as POP and atelectasis (13, 37, 92). In order to explore the preventive effect of short-term preoperative inspiratory muscle training on the incidence of postoperative pulmonary complications in patients undergoing elective cardiac surgery, Chen et al. conducted a randomized controlled trial in which the intervention group received 5 days of preoperative respiratory muscle training on the basis of routine care (15). The results showed that compared to the control group, patients in the intervention group had significantly reduced incidence of pulmonary complications, shortened postoperative hospital stay, and a significant increase in inspiratory muscle strength, forced expiratory volume in the first second of expiration, forced vital capacity and maximal voluntary ventilation. In a systematic review and meta-analysis conducted by Neto et al. they found that preoperative inspiratory muscle training could result in improvement in the inspiratory muscle strength, endurance, forced expiratory volume in 1 second, forced vital capacity, duration of hospital stay and reduced risk of postoperative pulmonary complications, and postoperative inspiratory muscle training could result in significant improvement in tidal volume, maximal inspiratory pressure and peak expiratory flow in patients undergoing cardiac surgery (93). Another systematic review and meta-analysis conducted by Kendall et al. showed that inspiratory muscle training was effective to reduce postoperative pulmonary complications and length of hospital stay (94). Similar results were also obtained by Thybo et al. who found that preoperative inspiratory muscle training may significantly reduce the risk of developing POP and atelectasis in patients undergoing CABG and heart valve surgery (95).
Turquetto et al. conducted a randomized controlled trial studying the effects of aerobic exercise and inspiratory muscle training on functional capacity, pulmonary function and autonomic control in patients after Fontan operation, finding that inspiratory muscle training cound significantly improve functional capacity and increase inspiratory muscle strength and spirometry (13). Another similar randomized controlled trial conducted by Cordeiro et al. showed that inspiratory muscle training was effective in improving functional capacity and inspiratory muscle strength in patients undergoing cardiac surgery (96). Santos et al. found that short-term moderate-to-high intensity inspiratory muscle training plus aerobic and resistance exercise could provide additional benefits in exercise capacity, inspiratory muscle strength, inspiratory muscle endurance, 6-min walk test, quality of life, and antioxidant profile in patients undergoing CABG (97). Despite differences in the specific measures and methods adopted across the studies, previous findings consistently suggested that preoperative respiratory physiotherapy could significantly improve patient outcomes. Therefore, it may be a feasible strategy to reduce postoperative respiratory complications and improve outcomes to implement appropriate respiratory physiotherapy in patients undergoing elective cardiac surgery in clinical practice.
A growing number of studies have found that active and systematic preoperative oral care can play an important role in preventing and reducing the development of POP after cardiovascular surgery, among which tooth brushing is one of the most acceptable and common measures. Oral care intervention by multiple tooth brushing can effectively remove oropharyngeal pathogens, improve oral hygiene, and reduce the risk of POP (98). In addition to tooth brushing, the commonly used oral care methods are mainly the use of chlorhexidine gluconate mouthwash and the combination of the two.
A prospective study conducted by Nicolosi et al. found that tooth brushing plus 0.12% chlorhexidine gluconate oral rinse was effective in preventing ventilator-associated pneumonia after cardiovascular surgery (99). The risk of POP was 3-fold higher and the hospital stay was significantly prolonged in patients without preoperative oral care. A systematic review and meta-analysis conducted by Bardia et al. demonstrated that the use of chlorhexidine gluconate was associated with reduced risk of POP after cardiac surgery, and this protective effect was particularly profound for gram-positive organisms (100). Among the patients receiving preoperative chlorhexidine mouthwash, the risk of POP was reduced by approximately one-half and the outcomes could be significantly improved. In addition, None of these studies reported adverse effects of chlorhexidine gluconate mouthwash.
To investigate the potential cost-effectiveness of administering preoperative chlorhexidine mouthwash at reducing POP among patients undergoing abdominal surgery, Kachapila et al. constructed a decision analytic model to compare costs and benefits within the first 30 days postoperatively (101). They found that patients receiving mouthwash had lower average costs and lower proportion of POP, and mouthwash surgery was more likely to be cost-effective. To explore the association between perioperative chlorhexidine oral care and POP in non-cardiac surgical patients, Liang et al. conducted a systematic review and meta-analysis (102). They found that nurse-led chlorhexidine oral care could significantly decrease the risk of POP and could be more convenient and economical than dental professional-led perioperative oral care.
Subglottic secretion drainage refers to a technique of continuous or intermittent suction during mechanical ventilation in order to remove secretions and retention from the subglottis and air sacs. The subglottic secretions contain a large number of pathogens, which is an important source of pathogenic bacteria for POP after cardiovascular surgery. Previous studies have shown that subglottic secretion drainage is of great value for the prevention of POP after cardiovascular surgery. Hudson et al. conducted a large retrospective observational study to explore the impact of subglottic suction on the incidence of POP after cardiac surgery (16). They found that continuous aspiration of subglottic secretions could significantly reduce the risk of POP and 30-day in-hospital mortality and shorten the lengths of mechanical ventilation and ICU stay. Similar results were also obtained by Granda et al. who found that the use of aspiration of subglottic secretions in patients undergoing cardiac surgery could significantly reduce the incidence density of POP, days on mechanical ventilation, the use of antibiotics, and medical burden (103). They considered this to be a very effective procedure and recommended that all patients undergoing major heart surgery should routinely receive aspiration of subglottic secretions from the moment of induction of anesthesia rather than entering ICU after surgery. Another randomized controlled trial conducted by Bouza et al. also showed that the use of continuous aspiration of subglottic secretions in patients undergoing major heart surgery could significantly reduce the risk of POP, shorten the length of hospital stay, reduce the amount of antibiotics and medical costs (88). Therefore, implementing timely and regular subglottic suction to remove and prevent secretions from flowing into the lower respiratory tract is an important preventive measure for POP in patients undergoing cardiovascular surgery.
Some other measures have also been reported to be effective in prevention and treatment, including lung protective ventilation management, alveolar recruitment maneuvers, early mobilization and progressive ambulation, elevation of the head end and semi-recumbent positioning, sedation vacation and the use of a weaning protocol, early extubation, strict changes of ventilatory circuit tube, appropriate cuff pressure control, use of non-invasive ventilation, proper use of tracheostomy, enteral feeding, selective digestive decontamination, peptic ulcer disease prophylaxis, silver-coated endotracheal tubes, microbiological surveillance, and deep vein thrombosis prophylaxis (104–109). In recent years, some prevention care bundles and prevention checklists which consist a series of rationalized measures have been developed and validated to be effective and convenient in preventing POP and shortening the duration of mechanical ventilation. The combined use of several interventions is currently recommended in clinical practice (109, 110). For high-risk patients, it may be effective to reduce the risk of POP and improve clinical outcomes by implementing multiple interventions such as respiratory physiotherapy, oral care, subglottic secretion drainage, and other appropriate measures.
In conclusion, POP is one of the most common respiratory complications in patients undergoing cardiovascular surgery, which is closely related to the increase of adverse outcomes and medical burden. Through the review of the current status, risk factors and intervention measures, this article provides new ideas for clinical prevention and treatment of POP after cardiovascular surgery.
FX, FS, and DW: conception, design, and writing. XH, YL, and XD: administrative support. ZJ, MS, DW, and FX: collection, assembly, and analysis of data. All authors read and approved the final manuscript.
This work was supported by a grant from the National Natural Science Foundation of China (No. 81800413).
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The authors would like to thank Dr. John S for the language help.
BMI, body mass index; CABG, coronary artery bypass grafting; CPB, cardiopulmonary bypass; ICU, intensive care unit; POP, postoperative pneumonia.
1. Zhao D, Liu J, Wang M, Zhang X, Zhou M. Epidemiology of cardiovascular disease in China: current features and implications. Nat Rev Cardiol. (2019) 16:203–12. doi: 10.1038/s41569-018-0119-4
2. Malaisrie SC, Szeto WY, Halas M, Girardi LN, Coselli JS, Sundt TM, et al. 2021 The American Association for Thoracic Surgery expert consensus document: Surgical treatment of acute type A aortic dissection. J Thorac Cardiovasc Surg. (2021) 162:735–58. doi: 10.1016/j.jtcvs.2021.04.053
3. Otto CM, Nishimura RA, Bonow RO, Carabello BA, Erwin JP, Gentile F, et al. 2020 ACC/AHA Guideline for the Management of Patients With Valvular Heart Disease: A Report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. Circulation. (2021) 77:450–500. doi: 10.1161/CIR.0000000000000923
4. Benedetto U, Dimagli A, Kaura A, Sinha S, Mariscalco G, Krasopoulos G, et al. Determinants of outcomes following surgery for type A acute aortic dissection: the UK National Adult Cardiac Surgical Audit. Eur Heart J. (2022) 43:44–52. doi: 10.1093/eurheartj/ehab586
5. He S, Wu F, Wu X, Xin M, Ding S, Wang J, et al. Ventilator-associated events after cardiac surgery: evidence from 1,709 patients. J Thorac Dis. (2018) 10:776–83. doi: 10.21037/jtd.2018.01.49
6. Greco G, Shi W, Michler RE, Meltzer DO, Ailawadi G, Hohmann SF, et al. Costs associated with health care–associated infections in cardiac surgery. J Am Coll Cardiol. (2015) 65:15–23. doi: 10.1016/j.jacc.2014.09.079
7. Kinlin LM, Kirchner C, Zhang H, Daley J, Fisman DN. Derivation and validation of a clinical prediction rule for nosocomial pneumonia after coronary artery bypass graft surgery. Clin Infect Dis. (2010) 50:493–501. doi: 10.1086/649925
8. Wang D, Abuduaini X, Huang X, Wang H, Chen X, Le S, et al. Development and validation of a risk prediction model for postoperative pneumonia in adult patients undergoing Stanford type A acute aortic dissection surgery: a case control study. J Cardiothorac Surg. (2022) 17:22. doi: 10.1186/s13019-022-01769-y
9. Wang D, Huang X, Wang H, Le S, Du X. Clinical risk score for postoperative pneumonia following heart valve surgery. Chinese Med J-Peking. (2021) 134:2447–56. doi: 10.1097/CM9.0000000000001715
10. Strobel RJ, Liang Q, Zhang M, Wu X, Rogers MAM, Theurer PF, et al. A preoperative risk model for postoperative pneumonia after coronary artery bypass grafting. Ann Thorac Surg. (2016) 102:1213–9. doi: 10.1016/j.athoracsur.2016.03.074
11. Vera UR, Bucio RE, Berrios BE, Choreno MT. Risk factors for the development of postoperative pneumonia after cardiac surgery. Arch Cardiol Mex. (2016) 86:203–7. doi: 10.1016/j.acmx.2015.12.005
12. He S, Chen B, Li W, Yan J, Chen L, Wang X, et al. Ventilator-associated pneumonia after cardiac surgery: a meta-analysis and systematic review. J Thorac Cardiovasc Surg. (2014) 148:3148–55. doi: 10.1016/j.jtcvs.2014.07.107
13. Turquetto ALR, Dos Santos MR, Agostinho DR, Sayegh ALC, de Souza FR, Amato LP, et al. Aerobic exercise and inspiratory muscle training increase functional capacity in patients with univentricular physiology after Fontan operation: A randomized controlled trial. Int J Cardiol. (2021) 330:50–8. doi: 10.1016/j.ijcard.2021.01.058
14. Zanini M, Nery RM, de Lima JB, Buhler RP, Da Silveira AD, Stein R. Effects of different rehabilitation protocols in inpatient cardiac rehabilitation after coronary artery bypass graft surgery. J Cardiopulm Rehabil. (2019) 39:E19–25. doi: 10.1097/HCR.0000000000000431
15. Chen X, Hou L, Zhang Y, Liu X, Shao B, Yuan B, et al. The effects of five days of intensive preoperative inspiratory muscle training on postoperative complications and outcome in patients having cardiac surgery: a randomized controlled trial. Clin Rehabil. (2019) 33:913–22. doi: 10.1177/0269215519828212
16. Hudson JKC, McDonald BJ, MacDonald JC, Ruel MA, Hudson CCC. Impact of subglottic suctioning on the incidence of pneumonia after cardiac surgery: a retrospective observational study. J Cardiothor Vasc an. (2015) 29:59–63. doi: 10.1053/j.jvca.2014.04.026
17. Kalil AC, Metersky ML, Klompas M, Muscedere J, Sweeney DA, Palmer LB, et al. Management of adults with hospital-acquired and ventilator-associated pneumonia: 2016 clinical practice guidelines by the infectious diseases society of america and the american thoracic society. Clin Infect Dis. (2016) 63:e61–e111. doi: 10.1093/cid/ciw353
18. American Thoracic Society Infectious Infectious Diseases Society of America. Guidelines for the management, of adults with hospital-acquired, ventilator-associated, and healthcare-associated pneumonia. Am J Resp Crit Care. (2005) 171:388–416. doi: 10.1164/rccm.200405-644ST
19. Wang D, Chen X, Wu J, Le S, Xie F, Li X, et al. Development and validation of nomogram models for postoperative pneumonia in adult patients undergoing elective cardiac surgery. Front Cardiov Med. (2021) 8:750828. doi: 10.3389/fcvm.2021.750828
20. Wang D, Huang X, Wang H, Le S, Yang H, Wang F, et al. Risk factors for postoperative pneumonia after cardiac surgery: a prediction model. J Thorac Dis. (2021) 13:2351–62. doi: 10.21037/jtd-20-3586
21. Yao R, Liu X, He Y, Mei C, Shen Y, Zhan Q, et al. Low platelet count is a risk factor of postoperative pneumonia in patients with type A acute aortic dissection. J Thorac Dis. (2020) 12:2333–42. doi: 10.21037/jtd.2020.03.84
22. Tamayo E, Álvarez FJ, Martínez-Rafael B, Bustamante J, Bermejo-Martin JF, Fierro I, et al. Ventilator-associated pneumonia is an important risk factor for mortality after major cardiac surgery. J Crit Care. (2012) 27:18–25. doi: 10.1016/j.jcrc.2011.03.008
23. LaPar DJ, Crosby IK, Rich JB, Fonner EJ, Kron IL, Ailawadi G, et al. A contemporary cost analysis of postoperative morbidity after coronary artery bypass grafting with and without concomitant aortic valve replacement to improve patient quality and cost-effective care. Ann Thorac Surg. (2013) 96:1621–7. doi: 10.1016/j.athoracsur.2013.05.050
24. Kilic A, Ohkuma R, Grimm JC, Magruder JT, Sussman M, Schneider EB, et al. A novel score to estimate the risk of pneumonia after cardiac surgery. J Thorac Cardiovasc Surg. (2016) 151:1415–21. doi: 10.1016/j.jtcvs.2015.12.049
25. Fitch ZW, Whitman GJ. Incidence, risk, and prevention of ventilator-associated pneumonia in adult cardiac surgical patients: a systematic review. J Card Surg. (2014) 29:196–203. doi: 10.1111/jocs.12260
26. Wang D, Li Y, Sheng W, Wang H, Le S, Huang X, et al. Development and validation of a nomogram model for pneumonia after redo cardiac surgery. J Cardiovasc Med. (2022) 23:325–34. doi: 10.2459/JCM.0000000000001302
27. Ailawadi G, Chang HL, O'Gara PT, O'Sullivan K, Woo YJ, DeRose JJ, et al. Pneumonia after cardiac surgery: experience of the national institutes of health/Canadian institutes of health research cardiothoracic surgical trials network. J Thorac Cardiovasc Surg. (2017) 153:1384–91. doi: 10.1016/j.jtcvs.2016.12.055
28. Hortal J, Giannella M, Pérez MJ, Barrio JM, Desco M, Bouza E, et al. Incidence and risk factors for ventilator-associated pneumonia after major heart surgery. Intens Care Med. (2009) 35:1518–25. doi: 10.1007/s00134-009-1523-3
29. Torres A, Niederman MS, Chastre J, Ewig S, Fernandez-Vandellos P, Hanberger H, et al. International ERS/ESICM/ESCMID/ALAT guidelines for the management of hospital-acquired pneumonia and ventilator-associated pneumonia. Eur Respir J. (2017) 50:1700582. doi: 10.1183/13993003.00582-2017
30. Banki F. Pulmonary assessment for general thoracic surgery. Surg Clin North Am. (2010) 90:969–84. doi: 10.1016/j.suc.2010.07.001
31. Saxena A, Shan L, Reid C, Dinh DT, Smith JA, Shardey GC, et al. Impact of smoking status on early and late outcomes after isolated coronary artery bypass graft surgery. J Cardiol. (2013) 61:336–41. doi: 10.1016/j.jjcc.2013.01.002
32. Al-Sarraf N, Thalib L, Hughes A, Tolan M, Young V, McGovern E. Effect of smoking on short-term outcome of patients undergoing coronary artery bypass surgery. Ann Thorac Surg. (2008) 86:517–23. doi: 10.1016/j.athoracsur.2008.03.070
33. Hillis LD, Smith PK, Anderson JL, Bittl JA, Bridges CR, Byrne JG, et al. 2011 ACCF/AHA guideline for coronary artery bypass graft surgery: executive summary: a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines. J Thorac Cardiovasc Surg. (2012) 143:4–34. doi: 10.1016/j.ycar.2012.02.094
34. Rigotti NA, McKool KM, Shiffman S. Predictors of smoking cessation after coronary artery bypass graft surgery. Results of a randomized trial with 5-year follow-up. Ann Intern Med. (1994) 120:287–93. doi: 10.7326/0003-4819-120-4-199402150-00005
35. Vlietstra RE, Kronmal RA, Oberman A, Frye RL, Killip TR. Effect of cigarette smoking on survival of patients with angiographically documented coronary artery disease. Report from the CASS registry. JAMA. (1986) 255:1023–7. doi: 10.1001/jama.255.8.1023
36. Rotstein C, Evans G, Born A, Grossman R, Light RB, Magder S, et al. Clinical practice guidelines for hospital-acquired pneumonia and ventilator-associated pneumonia in adults. Canad J Infect Dis Med Microbiol. (2008) 19:19–53. doi: 10.1155/2008/593289
37. Katsura M, Kuriyama A, Takeshima T, Fukuhara S, Furukawa TA. Preoperative inspiratory muscle training for postoperative pulmonary complications in adults undergoing cardiac and major abdominal surgery. Cochrane Database Syst Rev. (2015) 10:CD010356. doi: 10.1002/14651858.CD010356.pub2
38. Roselli EE, Pettersson GB, Blackstone EH, Brizzio ME, Houghtaling PL, Hauck R, et al. Adverse events during reoperative cardiac surgery: frequency, characterization, and rescue. J Thorac Cardiovasc Surg. (2008) 135:316–323. doi: 10.1016/j.jtcvs.2007.08.060
39. Bianco V, Kilic A, Gleason TG, Aranda-Michel E, Habertheuer A, Wang Y, et al. Reoperative cardiac surgery is a risk factor for long-term mortality. Ann Thorac Surg. (2020) 110:1235–42. doi: 10.1016/j.athoracsur.2020.02.028
40. Norton EL, Rosati CM, Kim KM, Wu X, Patel HJ, Deeb GM, et al. Is previous cardiac surgery a risk factor for open repair of acute type A aortic dissection? J Thorac Cardiovasc Surg. (2020) 160:8–17. doi: 10.1016/j.jtcvs.2019.07.093
41. Allou N, Bronchard R, Guglielminotti J, Dilly MP, Provenchere S, Lucet JC, et al. Risk factors for postoperative pneumonia after cardiac surgery and development of a preoperative risk score*. Crit Care Med. (2014) 42:1150–6. doi: 10.1097/CCM.0000000000000143
42. Bouza E, Pérez A, Muñoz P, Jesús Pérez M, Rincón C, Sánchez C, et al. Ventilator-associated pneumonia after heart surgery: A prospective analysis and the value of surveillance*. Crit Care Med. (2003) 31:1964–70. doi: 10.1097/01.ccm.0000084807.15352.93
43. Xiao P, Song W, Han Z. Characteristics of pulmonary infection after mitral valve repair in patients with metabolic syndrome and its relationship with blood pressure, blood glucose and blood lipid. Exp Ther Med. (2018) 16:5003–8. doi: 10.3892/etm.2018.6839
44. Santos M, Braga JU, Gomes RV, Werneck GL. Predictive factors for pneumonia onset after cardiac surgery in Rio de Janeiro, Brazil. Infect Control Hosp Epidemiol. (2007) 28:382–8. doi: 10.1086/513119
45. Canet J, Gallart L, Gomar C, Paluzie G, Valles J, Castillo J, et al. Prediction of postoperative pulmonary complications in a population-based surgical cohort. Anesthesiology. (2010) 113:1338–50. doi: 10.1097/ALN.0b013e3181fc6e0a
46. Tanaka KA, Alejo D, Ghoreishi M, Salenger R, Fonner C, Ad N, et al. Impact of preoperative hematocrit, body mass index, and red cell mass on allogeneic blood product usage in adult cardiac surgical patients: report from a statewide quality initiative. J Cardiothor Vascan. (2022). doi: 10.1053/j.jvca.2022.03.034. [Epub ahead of print].
47. Yuan L, Chang M, Wang J. Abdominal obesity, body mass index and the risk of frailty in community-dwelling older adults: a systematic review and meta-analysis. Age Ageing. (2021) 50:1118–28. doi: 10.1093/ageing/afab039
48. Kojima G, Iliffe S, Walters K. Frailty index as a predictor of mortality: a systematic review and meta-analysis. Age Ageing. (2018) 47:193–200. doi: 10.1093/ageing/afx162
49. Ozturk S, Kayacoglu I, Sensoz Y, Ozcelik S, Arslan Y, Ozturk I. Is there a predictive value of hemoglobin A1C for complications of cardiac surgery? J Coll Physic Surg Pak. (2021) 30:686–93. doi: 10.29271/jcpsp.2021.06.686
50. Subramaniam B, Lerner A, Novack V, Khabbaz K, Paryente-Wiesmann M, Hess P, et al. Increased Glycemic Variability in Patients with Elevated Preoperative HbA1C Predicts Adverse Outcomes Following Coronary Artery Bypass Grafting Surgery. Anesthes Analgesia. (2014) 118:277–87. doi: 10.1213/ANE.0000000000000100
51. Sato H, Carvalho G, Sato T, Lattermann R, Matsukawa T, Schricker T. The association of preoperative glycemic control, intraoperative insulin sensitivity, and outcomes after cardiac surgery. J Clin Endocrinol Metabol. (2010) 95:4338–44. doi: 10.1210/jc.2010-0135
52. Duncan AE, Abd-Elsayed A, Maheshwari A, Xu M, Soltesz E, Koch CG. Role of intraoperative and postoperative blood glucose concentrations in predicting outcomes after cardiac surgery. Anesthesiology. (2010) 112:860–71. doi: 10.1097/ALN.0b013e3181d3d4b4
53. Hortal J, Munoz P, Cuerpo G, Litvan H, Rosseel PM, Bouza E. Ventilator-associated pneumonia in patients undergoing major heart surgery: an incidence study in Europe. Crit Care. (2009) 13:R80. doi: 10.1186/cc7896
54. Zhou Y, Cai J, Wang X, Du S, Zhang J. Distribution and resistance of pathogens in infected patients within 1 year after heart transplantation. Int J Infect Dis. (2021) 103:132–7. doi: 10.1016/j.ijid.2020.11.137
55. Vidal C, Pasqualotto R, James A, Dureau P, Rasata J, Coutance G, et al. Predictive risk factors for postoperative pneumonia after heart transplantation. Bmc Anesthesiol. (2020) 20:8. doi: 10.1186/s12871-019-0923-3
56. Lerman DT, Hamilton KW, Byrne D, Lee DF, Zeitler K, Claridge T, et al. The impact of infection among left ventricular assist device recipients on post-transplantation outcomes: A retrospective review. Transpl Infect Dis. (2018) 20:e12995. doi: 10.1111/tid.12995
57. Pons S, Sonneville R, Bouadma L, Styfalova L, Ruckly S, Neuville M, et al. Infectious complications following heart transplantation in the era of high-priority allocation and extracorporeal membrane oxygenation. Ann Intensive Care. (2019) 9:17. doi: 10.1186/s13613-019-0490-2
58. de la Varga-Martínez O, Gómez-Sánchez E, Muñoz MF, Lorenzo M, Gómez-Pesquera E, Poves-Álvarez R, et al. Impact of nosocomial infections on patient mortality following cardiac surgery. J Clin Anesth. (2021) 69:110104. doi: 10.1016/j.jclinane.2020.110104
59. McDonald CI, Fraser JF, Coombes JS, Fung YL. Oxidative stress during extracorporeal circulation. Eur J Cardio-Thorac. (2014) 46:937–43. doi: 10.1093/ejcts/ezt637
60. Anastasiadis K, Argiriadou H, Deliopoulos A, Antonitsis P. Minimal invasive extracorporeal circulation (MiECC): the state-of-the-art in perfusion. J Thorac Dis. (2019) 11:S1507–14. doi: 10.21037/jtd.2019.01.66
61. Anastasiadis K, Murkin J, Antonitsis P, Bauer A, Ranucci M, Gygax E, et al. Use of minimal invasive extracorporeal circulation in cardiac surgery: principles, definitions and potential benefits. A position paper from the Minimal invasive Extra-Corporeal Technologies international Society (MiECTiS). Interact Cardiovasc Thorac Surg. (2016) 22:647–62. doi: 10.1093/icvts/ivv380
62. Anastasiadis K, Antonitsis P, Haidich A, Argiriadou H, Deliopoulos A, Papakonstantinou C. Use of minimal extracorporeal circulation improves outcome after heart surgery; a systematic review and meta-analysis of randomized controlled trials. Int J Cardiol. (2013) 164:158–69. doi: 10.1016/j.ijcard.2012.01.020
63. Anastasiadis K, Antonitsis P, Deliopoulos A, Argiriadou H. A multidisciplinary perioperative strategy for attaining “more physiologic” cardiac surgery. Perfusion. (2017) 32:446–53. doi: 10.1177/0267659117700488
64. Möhnle P, Snyder-Ramos SA, Miao Y, Kulier A, Böttiger BW, Levin J, et al. Postoperative red blood cell transfusion and morbid outcome in uncomplicated cardiac surgery patients. Intens Care Med. (2011) 37:97–109. doi: 10.1007/s00134-010-2017-z
65. Leal-Noval SR, Rincón-Ferrari MD, García-Curiel A, Herruzo-Avilés A, Camacho-Laraña P, Garnacho-Montero J, et al. Transfusion of blood components and postoperative infection in patients undergoing cardiac surgery. Chest. (2001) 119:1461–8. doi: 10.1378/chest.119.5.1461
66. Horvath KA, Acker MA, Chang H, Bagiella E, Smith PK, Iribarne A, et al. Blood transfusion and infection after cardiac surgery. Ann Thorac Surg. (2013) 95:2194–201. doi: 10.1016/j.athoracsur.2012.11.078
67. Crawford TC, Magruder JT, Fraser C, Suarez-Pierre A, Alejo D, Bobbitt J, et al. Less is more: results of a statewide analysis of the impact of blood transfusion on coronary artery bypass grafting outcomes. Ann Thorac Surg. (2018) 105:129–36. doi: 10.1016/j.athoracsur.2017.06.062
68. Likosky DS, Paone G, Zhang M, Rogers MAM, Harrington SD, Theurer PF, et al. Red blood cell transfusions impact pneumonia rates after coronary artery bypass grafting. Ann Thorac Surg. (2015) 100:794–801. doi: 10.1016/j.athoracsur.2015.03.089
69. LaPar DJ, Crosby IK, Ailawadi G, Ad N, Choi E, Spiess BD, et al. Blood product conservation is associated with improved outcomes and reduced costs after cardiac surgery. J Thorac Cardiovasc Surg. (2013) 145:796–804. doi: 10.1016/j.jtcvs.2012.12.041
70. Salpeter SR, Buckley JS, Chatterjee S. Impact of more restrictive blood transfusion strategies on clinical outcomes: a meta-analysis and systematic review. Am J Med. (2014) 127:124–31. doi: 10.1016/j.amjmed.2013.09.017
71. Halpin L, Henry L, Szelkowski L, Hunt S, Vourlekis J, Ad N. Ventilator-associated pneumonia among cardiac surgery patients: what can we do for prevention? J Nurs Care Qual. (2013) 28:345–51. doi: 10.1097/NCQ.0b013e318292907c
72. Tormey CA, Hendrickson JE. Transfusion-related red blood cell alloantibodies: induction and consequences. Blood. (2019) 133:1821–30. doi: 10.1182/blood-2018-08-833962
73. Karsten E, Herbert BR. The emerging role of red blood cells in cytokine signalling and modulating immune cells. Blood Rev. (2020) 41:100644. doi: 10.1016/j.blre.2019.100644
74. Tinmouth A, Fergusson D, Yee IC, Hébert PC. Clinical consequences of red cell storage in the critically ill. Transfusion. (2006) 46:2014–27. doi: 10.1111/j.1537-2995.2006.01026.x
75. Roback JD, Neuman RB, Quyyumi A, Sutliff R. Insufficient nitric oxide bioavailability: a hypothesis to explain adverse effects of red blood cell transfusion. Transfusion. (2011) 51:859–66. doi: 10.1111/j.1537-2995.2011.03094.x
76. Hod EA, Brittenham GM, Billote GB, Francis RO, Ginzburg YZ, Hendrickson JE, et al. Transfusion of human volunteers with older, stored red blood cells produces extravascular hemolysis and circulating non-transferrin-bound iron. Blood. (2011) 118:6675–82. doi: 10.1182/blood-2011-08-371849
77. Carson JL, Guyatt G, Heddle NM, Grossman BJ, Cohn CS, Fung MK, et al. Clinical practice guidelines from the aabb: red blood cell transfusion thresholds and storage. JAMA. (2016) 316:2025–35. doi: 10.1001/jama.2016.9185
78. Ferraris VA, Ferraris SP, Saha SP, Hessel EA, Haan CK, Royston BD, et al. Perioperative blood transfusion and blood conservation in cardiac surgery: the society of thoracic surgeons and the society of cardiovascular anesthesiologists clinical practice guideline. Ann Thorac Surg. (2007) 83:S27–86. doi: 10.1016/j.athoracsur.2007.02.099
79. Ferraris VA, Brown JR, Despotis GJ, Hammon JW, Reece TB, Saha SP, et al. 2011 update to the society of thoracic surgeons and the society of cardiovascular anesthesiologists blood conservation clinical practice guidelines. Ann Thorac Surg. (2011) 91:944–82. doi: 10.1016/j.athoracsur.2010.11.078
80. Apfelbaum JL, Nuttall GA, Connis PT CRHM D, Miller RD, Nickinovich DG, et al. Practice guidelines for perioperative blood management: an updated report by the American Society of Anesthesiologists Task Force on Perioperative Blood Management*. Anesthesiology. (2015) 122:241–75. doi: 10.1097/ALN.0000000000000463
81. Sheng W, Xing QS, Hou WM, Sun L, Niu ZZ, Lin MS, et al. Independent risk factors for ventilator-associated pneumonia after cardiac surgery. J Invest Surg. (2014) 27:256–61. doi: 10.3109/08941939.2014.892652
82. Tobin M, Manthous C. Mechanical ventilation. Am J Respir Crit Care Med. (2017) 196:P3–4. doi: 10.1164/rccm.1962P3
83. Bouadma L, Wolff M, Lucet JC. Ventilator-associated pneumonia and its prevention. Curr Opin Infect Dis. (2012) 25:395–404. doi: 10.1097/QCO.0b013e328355a835
84. Papazian L, Klompas M, Luyt C. Ventilator-associated pneumonia in adults: a narrative review. Intens Care Med. (2020) 46:888–906. doi: 10.1007/s00134-020-05980-0
85. Goligher EC, Dres M, Fan E, Rubenfeld GD, Scales DC, Herridge MS, et al. Mechanical Ventilation-induced Diaphragm Atrophy Strongly Impacts Clinical Outcomes. Am J Respir Crit Care Med. (2018) 197:204–13. doi: 10.1164/rccm.201703-0536OC
86. Galal YS. Ventilator-associated pneumonia: incidence, risk factors and outcome in paediatric intensive care units at cairo university hospital. J Clin Diagn Res. (2016) 10:SC06–11. doi: 10.7860/JCDR/2016/18570.7920
87. Boeken U, Schurr P, Kurt M, Feindt P, Lichtenberg A. Early reintubation after cardiac operations: impact of nasal continuous positive airway pressure (nCPAP) and noninvasive positive pressure ventilation (NPPV). Thorac Cardiovasc Surg. (2010) 58:398–402. doi: 10.1055/s-0030-1249940
88. Bouza E, Perez MJ, Munoz P, Rincon C, Barrio JM, Hortal J. Continuous aspiration of subglottic secretions in the prevention of ventilator-associated pneumonia in the postoperative period of major heart surgery. Chest. (2008) 134:938–46. doi: 10.1378/chest.08-0103
89. Gao F, Yang L, He H, Ma X, Lu J, Zhai Y, et al. The effect of reintubation on ventilator-associated pneumonia and mortality among mechanically ventilated patients with intubation: a systematic review and meta-analysis. Heart Lung. (2016) 45:363–71. doi: 10.1016/j.hrtlng.2016.04.006
90. El Solh AA, Bhora M, Pineda L, Dhillon R. Nosocomial pneumonia in elderly patients following cardiac surgery. Resp Med. (2006) 100:729–36. doi: 10.1016/j.rmed.2005.07.011
91. García-Delgado M, Navarrete-Sánchez I, Colmenero M. Preventing and managing perioperative pulmonary complications following cardiac surgery. Curr Opin Anaesthesiol. (2014) 27:146–52. doi: 10.1097/ACO.0000000000000059
92. Hulzebos EHJ, Smit Y, Helders PPJM, van Meeteren NLU. Preoperative physical therapy for elective cardiac surgery patients. Cochrane Db Syst Rev. (2012) 11:D10118. doi: 10.1002/14651858.CD010118.pub2
93. Gomes Neto M, Martinez BP, Reis HF, Carvalho VO. Pre- and postoperative inspiratory muscle training in patients undergoing cardiac surgery: systematic review and meta-analysis. Clin Rehabil. (2017) 31:454–64. doi: 10.1177/0269215516648754
94. Kendall F, Oliveira J, Peleteiro B, Pinho P, Bastos PT. Inspiratory muscle training is effective to reduce postoperative pulmonary complications and length of hospital stay: a systematic review and meta-analysis. Disabil Rehabil. (2018) 40:864–82. doi: 10.1080/09638288.2016.1277396
95. Thybo Karanfil EO, Møller AM. Preoperative inspiratory muscle training prevents pulmonary complications after cardiac surgery - a systematic review. Dan Med J. (2018) 65:A5450.
96. Cordeiro ALL, de Melo TA, Neves D, Luna J, Esquivel MS, Guimarães ARF, et al. Inspiratory muscle training and functional capacity in patients undergoing cardiac surgery. Rev Brasileira de Cirurgia Cardiov. (2016) 31:140–4. doi: 10.5935/1678-9741.20160035
97. Dos Santos TD, Pereira SN, Portela LOC, Cardoso DM, Lago PD, Dos Santos Guarda N, et al. Moderate-to-high intensity inspiratory muscle training improves the effects of combined training on exercise capacity in patients after coronary artery bypass graft surgery: a randomized clinical trial. Int J Cardiol. (2019) 279:40–6. doi: 10.1016/j.ijcard.2018.12.013
98. Akutsu Y, Matsubara H, Shuto K, Shiratori T, Uesato M, Miyazawa Y, et al. Pre-operative dental brushing can reduce the risk of postoperative pneumonia in esophageal cancer patients. Surgery. (2010) 147:497–502. doi: 10.1016/j.surg.2009.10.048
99. Nicolosi LN, Del Carmen Rubio M, Martinez CD, Gonzalez NN, Cruz ME. Effect of oral hygiene and 012% chlorhexidine gluconate oral rinse in preventing ventilator-associated pneumonia after cardiovascular surgery. Resp Care. (2014) 59:504–9. doi: 10.4187/respcare.02666
100. Bardia A, Blitz D, Dai F, Hersey D, Jinadasa S, Tickoo M, et al. Preoperative chlorhexidine mouthwash to reduce pneumonia after cardiac surgery: a systematic review and meta-analysis. J Thorac Cardiovasc Surg. (2019) 158:1094–100. doi: 10.1016/j.jtcvs.2019.01.014
101. Kachapila M, Ademuyiwa AO, Biccard BM, Ghosh DN, Glasbey J, Monahan M, et al. Preliminary model assessing the cost-effectiveness of preoperative chlorhexidine mouthwash at reducing postoperative pneumonia among abdominal surgery patients in South Africa. PLoS ONE. (2021) 16:e254698. doi: 10.1371/journal.pone.0254698
102. Liang S, Zhang X, Hu Y, Yang J, Li K. Association between perioperative chlorhexidine oral care and postoperative pneumonia in non-cardiac surgical patients: A systematic review and meta-analysis. Surgery. (2021) 170:1418–31. doi: 10.1016/j.surg.2021.05.008
103. Pérez Granda MJ, Barrio JM, Hortal J, Muñoz P, Rincón C, Bouza E. Routine aspiration of subglottic secretions after major heart surgery: impact on the incidence of ventilator-associated pneumonia. J Hosp Infect. (2013) 85:312–5. doi: 10.1016/j.jhin.2013.08.006
104. Kollef MH, Afessa B, Anzueto A, Veremakis C, Kerr KM, Margolis BD, et al. Silver-coated endotracheal tubes and incidence of ventilator-associated pneumonia: the NASCENT randomized trial. JAMA. (2008) 300:805–13. doi: 10.1001/jama.300.7.805
105. Schnabel RM, Scholte JBJ, Van Der Velden KEHM, Roekaerts PMHJ, Bergmans DCJJ. Ventilator-associated pneumonia rates after introducing selective digestive tract decontamination. Infect Dis-Nor. (2015) 47:650–3. doi: 10.3109/23744235.2015.1031172
106. Resar R, Pronovost P, Haraden C, Simmonds T, Rainey T, Nolan T. Using a bundle approach to improve ventilator care processes and reduce ventilator-associated pneumonia. Joint Commission J Quality Patient Safety. (2005) 31:243. doi: 10.1016/S1553-7250(05)31031-2
107. Yana R, Jo RM. Getting guidelines into practice: a literature review. Nurs Stand. (2004) 18:33–40. doi: 10.7748/ns2004.08.18.50.33.c3677
108. Strobel RJ, Harrington SD, Hill C, Thompson MP, Cabrera L, Theurer P, et al. Evaluating the impact of pneumonia prevention recommendations after cardiac surgery. Ann Thorac Surg. (2020) 110:903–10. doi: 10.1016/j.athoracsur.2019.12.053
109. Rello J, Lode H, Cornaglia G, Masterton R. A European care bundle for prevention of ventilator-associated pneumonia. Intens Care Med. (2010) 36:773–80. doi: 10.1007/s00134-010-1841-5
Keywords: cardiovascular surgery, risk factor, incidence, intervention, pneumonia
Citation: Wang D, Lu Y, Sun M, Huang X, Du X, Jiao Z, Sun F and Xie F (2022) Pneumonia After Cardiovascular Surgery: Incidence, Risk Factors and Interventions. Front. Cardiovasc. Med. 9:911878. doi: 10.3389/fcvm.2022.911878
Received: 03 April 2022; Accepted: 13 June 2022;
Published: 30 June 2022.
Edited by:
Gary David Lopaschuk, University of Alberta, CanadaReviewed by:
Manoj Sahu, All India Institute of Medical Sciences, IndiaCopyright © 2022 Wang, Lu, Sun, Huang, Du, Jiao, Sun and Xie. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Fei Xie, eGllZmVpMDEwM0BodXN0LmVkdS5jbg==; Fuqiang Sun, c2ZxMTAxMEAxMjYuY29t; Zhouyang Jiao, amlhb3pob3V5YW5nQDEyNi5jb20=
†These authors have contributed equally to this work
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.