
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Cardiovasc. Med. , 17 June 2022
Sec. Cardiac Rhythmology
Volume 9 - 2022 | https://doi.org/10.3389/fcvm.2022.900023
 Antonella Groppelli1Michele Brignole1*Mohamed Chefrour2Marguerite Gastaldi2,3
Antonella Groppelli1Michele Brignole1*Mohamed Chefrour2Marguerite Gastaldi2,3 Farid El Oufir3
Farid El Oufir3 Jean Claude Deharo4
Jean Claude Deharo4 Gianfranco Parati1,5
Gianfranco Parati1,5 Régis Guieu2,3
Régis Guieu2,3Background: Either high or low values of adenosine blood level (ABL) can differentiate some forms of neurally mediated syncope (NMS). A rapid method of measurement has recently been developed. The aim of the present study was: (1) to compare ABLs in an unselected population of consecutive patients referred for evaluation of suspected NMS syncope and in healthy controls; and (2) to assess the relative prevalence of low and high adenosine forms among an unselected syncope population.
Method: Whole blood was collected after finger puncture, blood being deposit on a blot paper and adenosine concentration was measured by liquid chromatography/mass spectrometry (LC-MS/MS).
Results: Among 89 control subjects, the median ABL value was 0.54 μM (IQR, 0.46–0.65). The lowest 5% and the upper 95% percentile were 0.40 and 0.80 μM, respectively. Compared with healthy subjects, the 146 patients with syncope showed, on average, a higher median ABL value [0.63 (IQR 0.45–0.73, p = 0.04)] and a larger distribution of values. Low ABL values below the 5th percentile were observed in 28 (19%) patients, and, in five controls, p = 0.003 and high ABL values were observed in 26 (18%) patients and five controls, p = 0.009.
Conclusions: ABL is different in patients with suspected NMS than in healthy subjects. Patients with low and high adenosine values account for 19% and 18% of the general population. Thus, low and high ABL limits, as defined in this study, may help to define the purinergic profile of unselected subjects with a clinical diagnosis of suspected NMS.
Either central or peripheral baroreceptor reflex abnormalities and/or alterations in neurohumoral mechanisms could play a pivotal role in the genesis of extrinsic (functional) and neurally mediated syncope (NMS) (1). Among the several biochemical mediators that are advocated to play a role, adenosine has recently been investigated in typical vasovagal syncope and in syncope without prodromes in subjects with a normal heart. Either high- or low-adenosine values have been reported to be able to differentiate some forms of syncope, but adenosine does not seem to be involved in other forms. Schematically, high-adenosine and low-adenosine forms have been identified (2). When baseline adenosine is low, the effect of adenosine on the AV node and the sino-atrial node is mainly due to the stimulation of high-affinity A1 receptors, (A1R) which are much more numerous in the AV node than in the sino-atrial node. The effects of adenosine on A1 R leads to bradycardia, sinus arrest or atrio-ventricular block (3, 4). Conversely, the high adenosine values are compatible with the activation of low-affinity A2A receptors (A2AR) that are in the vessels and which cause vasodilation (2).
The prevalence of patients with low and high adenosine syncope is uncertain because, until now, adenosine has been studied in small, selected populations. A barrier to the widespread evaluation of adenosine in clinical practice has been the difficulty of obtaining rapid reliable measures. Indeed, owing to its short half-life in the blood, adenosine is not easy to sample and measure. At the time of venepuncture, a stop solution – not commercially available - must be utilized to inhibit the degradation of adenosine in body fluid. After plasma deproteinization, adenosine concentration is evaluated by means of high-performance liquid chromatography. A rapid method (“blot spot”) has recently been developed and assessed in a small population (5). It consists of measuring adenosine concentration in whole blood instead of plasma, using fixed potential amperometry. This method is rapid, well-accepted by the patient, not expensive, and easily replicable.
The aim of the present study was: (1) to compare ABLs in an unselected population of subjects with a history of suspected NMS and in healthy controls; and (2) to assess the relative prevalence of low and high adenosine forms among this population.
We assessed the rapid method of adenosine dosage in whole blood using Liquid Chromatography, Mass Spectrometry (LC-MS/MS) (5) in unselected consecutive patients with a history of suspected NMS and in healthy volunteers. The blood samples were shipped to the Laboratory of Biochemistry of Timone Hospital for analysis.
The Syncope group was formed by patients aged >14 years referred to the syncope clinic of Istituto Auxologico Italiano, Milan, Italy because affected by one or more episodes of unexplained syncope to confirm or reject the clinical suspicion of NMS after exclusion of competing diagnoses. In particular, according to the diagnostic criteria of ESC guidelines (6), the patients with likely cardiac syncope and those with a transient loss of consciousness of likely non-syncopal origin were excluded. The patients underwent head-up tilt test (HUTT) according to the Italian protocol (7).
The day of blood sampling, the participants were allowed to take their usual drug therapies and had no dietary restrictions. Whole blood was collected using finger puncture, while the patient was sitting in a quiet environment, followed by deposit of a drop of blood (20 μL) on a blotting paper (Whatman 903 protein saver cards™) and dried overnight at room temperature to obtain dried blood spot. Then, the blot spots were stored at room temperature and shipped to the Laboratory of Biochemistry of Timone Hospital for analysis.
The method has been previously described (5). Briefly, six millimeters of dried blood spot were cut out, followed by extraction with mixture, consisting of methanol and internal standards mixed for 90 min at 45°C. After extraction, aliquots (350 μL) were transferred into a new 2-ml safe-lock tube and evaporated to dryness at 60°C under nitrogen; 150 μl of 0.1% formic acid in water was added and quickly vortexed before transferring into an HPLC auto sampler vial.
After the extraction, adenosine concentration was measured by LC-MS/MS. Samples were analyzed using a Shimadzu UFLC XR system (Shimadzu, Marne la Vallee, France). The LC system was interfaced with an ABSciex 4,500 triple quadrupole mass spectrometer (Les Ulis, France), operating with an electrospray ionization source (ESI) using nitrogen (purity: 99.99%). Ten microliters of the extracted sample were injected onto a 2.1-mm- × -100-mm, 3-μm Atlantis R T3 column, Waters (Guyancourt, France). The starting mobile phase consisted of 3% methanol and 97% acidified water (0.1% formic acid), with a flow of 0.7 ml/min for 3.5 min. Then, the gradient of methanol was increased to 30% for 3 min. The column was re-equilibrated for 2 min to starting conditions.
ABL values were reported as median and interquartile range [IQR] and compared between groups by means of Mann–Whitney non-parametric test. Categorical variables were shown as absolute and relative frequencies and compared between groups by means of the Fisher exact test or Chi-squared test for a trend as appropriate.
The study population consisted of 146 patients with a diagnosis of likely neurally mediated syncope; their mean age was 57 ± 20 years, 67 were males (46%). The clinical features of patients with syncope were consistent with those of an unselected general population: 108 had prodromes, suggesting an autonomic activation, 54 had recognizable triggers (orthostatic, emotional, situational or post-prandial, single or in combination); 55 were taking antihypertensive drugs. HUTT was positive in 101 (72%) patients (vasodepressor or mixed in 88 and cardioinhibitory in 13) and negative in 45 (28%) patients. The control group consisted of 89 healthy volunteers; their mean age was 51 ± 18 years, 46 were males (52%).
In controls, the average median ABL value was 0.54 μM (IQR, 0.46–0.65). The lowest 5th and the highest 95th percentiles were 0.40 μM and 0.80 μM, respectively; these values were, therefore, considered as the normal limit for low ABL and high ABL in patients with syncope. Table 1 shows the results of ABL dosage in both groups. Compared with healthy subjects, the patients with NMS showed, on average, a higher median ABL value [0.63 (IQR, 0.45–0.73, p = 0.04)] and a larger distribution of values (Figure 1). The low ABL zone included 28 (19%) patients and five controls, p = 0.003, and the high APL zone included 26 (18%) patients and five controls, p = 0.009.

Table 1. Comparison of adenosine values between healthy controls and patients with syncope by the blot spot method.
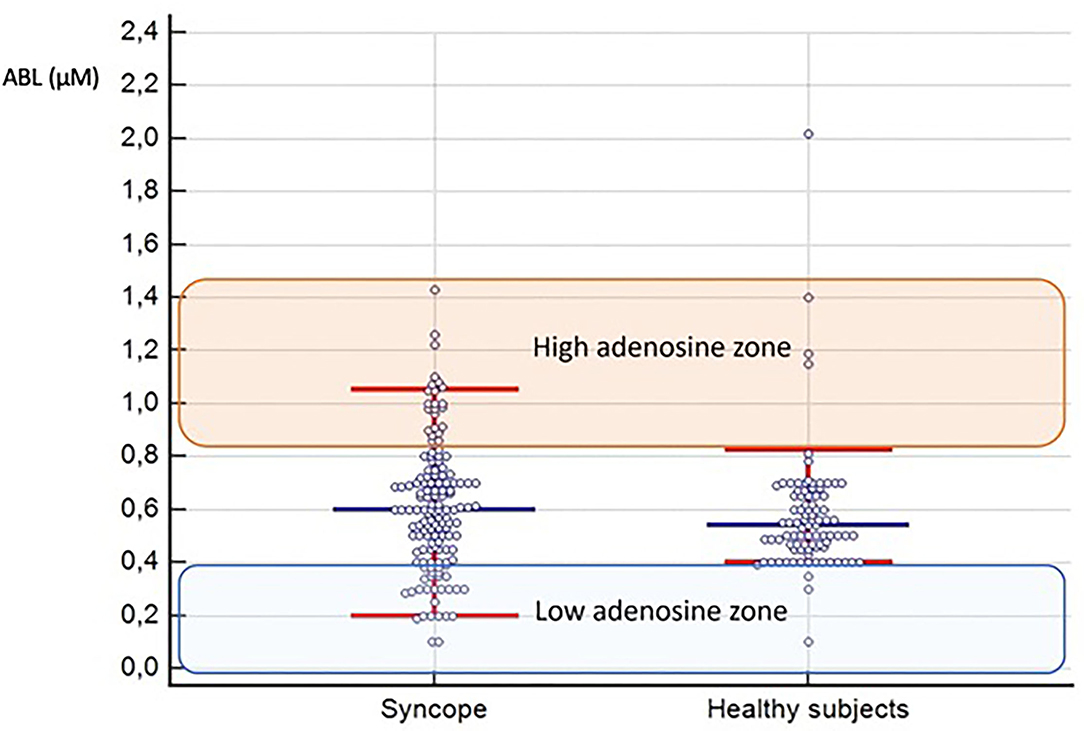
Figure 1. Distribution of patients with syncope and healthy controls based on their adenosine levels. The blue horizontal line shows the median; the red horizontal lines show the 5th and the 95th percentiles of the two groups. The low adenosine zone and the high adenosine zone, based on the normal ABL range in control subjects, are identified as well.
Thus, the phenotype of low adenosine syncope could be identified in 19% and that of high adenosine syncope in 18% of the whole syncope population (Figure 2). The clinical features of patients with low, normal, and high ABL are shown in Table 2. The clinical differences were modest, not reaching the level of significance.
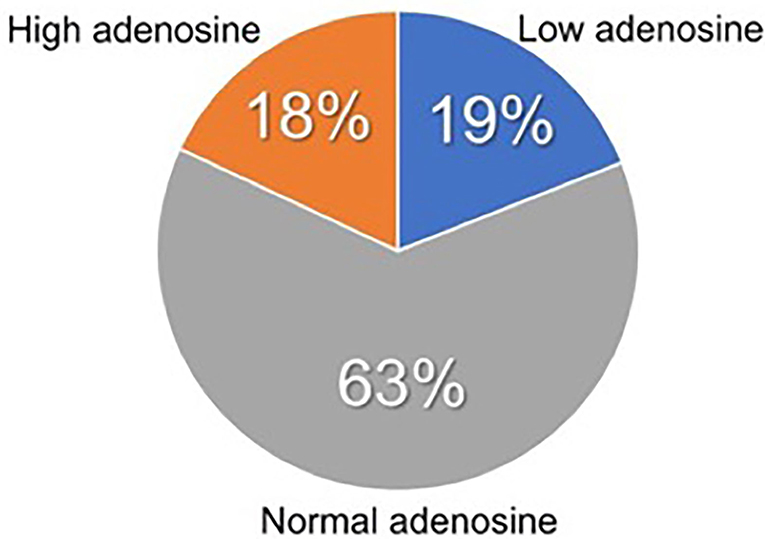
Figure 2. Prevalence of patients with low ABL syncope and with high ABL syncope among an unselected population of adult patients with NMS.
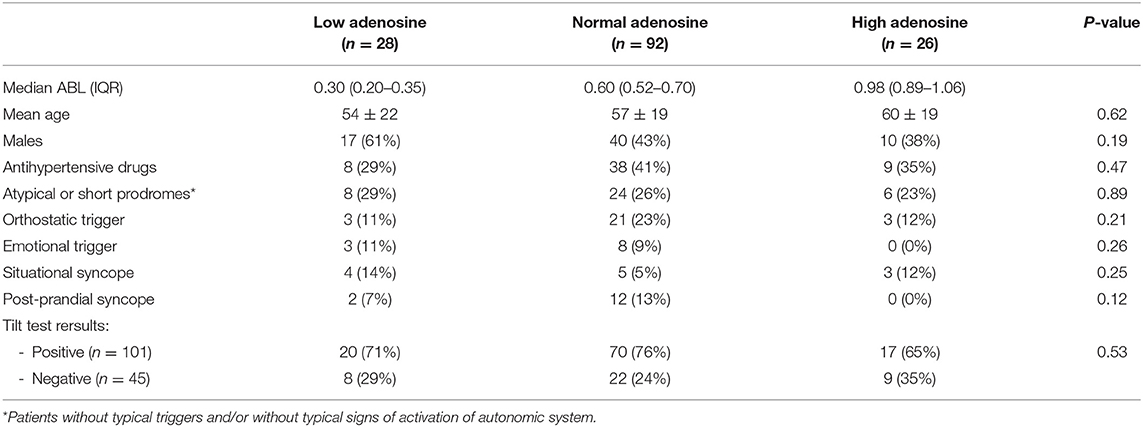
Table 2. Clinical features according to adenosine values.
The main findings of the study are that rest ABL, measured with the rapid “blot spot” method on whole blood, can distinguish a general population of patients with suspected NMS from healthy subjects. Among an unselected NMS population, two groups of patients with low and high outlier ABL values can be identified, which account for 19% and 18% of the population, respectively. These results are consistent with those of previous studies performed with the standard method of high-performance liquid chromatography in plasma with stop solution (3, 4, 8, 9). The normal range of ABL observed with the “blot spot” method was similar to that of 0.40 to 0.78 μM observed with the chromatographic method in the laboratory of Biochemistry of Timone Hospital in 120 healthy subjects (10).
In our previous studies (3, 4, 8, 9), we showed that several patients with syncope without prodromes and normal heart had value of adenosine plasma levels below the 5th percentile of healthy subjects and that several patients with positive vasovagal response during tilt testing had values above the 95th percentile of healthy subjects. The result of the present study shows that such correlation is more difficult to be found in an unselected general population. In a recent trial (10), the efficacy of theophylline, an adenosine receptor antagonist, was similar in patients with low and high AP measured with the chromatographic method, suggesting a lack of correlation between adenosine and clinical effect. Thus, it seems that the identification of low-adenosine syncope and high-adenosine syncope is more effective when the dosage of adenosine is performed in well-selected population affected by typical severe forms of syncope without prodromes and normal heart (3, 10) or in patients with typical features of vasovagal syncope as was the case in the pivotal studies (3, 9).
In conclusion, in this study, we have validated a rapid method (“blot spot”) for rapid, easy-to-perform, and cheap measurement of adenosine in the whole blood. The low and high ABL limits, as defined in this study, may help to define the purinergic profile of patients affected by NMS and can be used in future studies. Because the expression level of adenosine receptor is also crucial to interpret the relationship between the adenosinergic system and NHS, further studies are necessary to explore notably the ratio A1 R or A2AR expression/adenosine level ratio.
Many subjects with NMS were on antihypertensive treatment, which can modify plasma adenosine values. In previous studies, antihypertensive therapy was stopped at the time of adenosine blood sampling (8, 9, 11, 12). Furthermore, we did not ask our patients to stop coffee or tea before the study, although caffeine modifies the concentration of plasma adenosine (13) and makes the receptors more sensitive to the action of adenosine (14, 15) and thus may influence the occurrence of syncope. We did not take this step because we wanted to study the basal values of adenosine in the daily life of patients without changing their lifestyle. Similarly, tilt test was not performed in fasting state that could have influenced its result.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethical review and approval was not required for the study on human participants in accordance with the local legislation and institutional requirements. The patients/participants provided their written informed consent to participate in this study.
AG: conceptualization, investigation, data curation, methodology, writing–original draft, and writing-review and editing. MB: conceptualization, formal analysis, methodology, writing–original draft, and writing-review and editing. MC and MG: adenosine measurement. FE: data collection. JD and GP: investigation and writing–review and editing. RG: conceptualization, investigation, and writing–review and editing. All authors contributed to the article and approved the submitted version.
This work was supported by Amidex Méditerranée Foundation and Aix Marseille University.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Mosqueda-Garcia R, Furlan R, Tank J, Fernandez-Violante R. The elusive pathophysiology of neurally mediated syncope. Circualtion. (2000) 102:2898–906. doi: 10.1161/01.CIR.102.23.2898
2. Brignole M, Groppelli A, Brambilla R, Caldara GL, Torresani E, Parati G, et al. Plasma adenosine and neurallymediatedsyncope: ready for clinical use. Europace. (2020) 22:847–53. doi: 10.1093/europace/euaa070
3. Deharo J-C, Guieu R, Mechulan A, Peyrouse E, Kipson N, Ruf J, et al. Syncope without prodromes in patients with normal heart and normal electrocardiogram: a distinct entity. J Am Coll Cardiol. (2013) 62:1075–80. doi: 10.1016/j.jacc.2013.05.060
4. Guieu R, Deharo JC, Ruf J, Mottola G, Kipson N, Bruzzese L, et al. Adenosine and clinical forms of neurally-mediated syncope. J Am Coll Cardiol. (2015) 66:202–3. doi: 10.1016/j.jacc.2015.04.066
5. Marlinge M, Vairo D, Marolda V, Bruzzese L, Adjriou N, Guiol C, et al. Rapid measurement of adenosine concentration in human blood using fixed potential amperometry: comparison with mass spectrometry and high-performance liquid chromatography. J AnalBioanal Tech. (2017) 8:371. doi: 10.4172/2155-9872.1000371
6. Brignole M, Moya A, de Lange FJ, Deharo JC, Elliott PM, Fanciulli A, et al. ESC scientific document group. 2018 ESC guidelines for the diagnosis and management of syncope. Eur Heart J. (2018) 39:1883–948. doi: 10.1093/eurheartj/ehy037
7. Bartoletti A, Alboni P, Ammirati F, Brignole M, Del Rosso A, FogliaManzillo G, et al. 'The Italian Protocol': a simplified head-up tilt testing potentiated with oral nitroglycerin to assess patients with unexplained syncope. Europace. (2000) 2:339–42. doi: 10.1053/eupc.2000.0125
8. Saadjian AY, Le'vy S, Franceschi F, Zouher I, Paganelli F, Guieu RP, et al. Role of endogenous adenosine as a modulator of syncope induced during tilt testing. Circulation. (2002) 106:569–74. doi: 10.1161/01.CIR.0000023924.66889.4C
9. Deharo J-C, Mechulan A, Giorgi R, Franceschi F, Prevot S, Peyrouse E, et al. Adenosine plasma level and A2A adenosine receptor expression: correlation with laboratory tests in patients with neurally mediated syncope. Heart. (2012) 98:855–9. doi: 10.1136/heartjnl-2011-301411
10. Brignole M, Guieu R, Tomaino M, Iori M, Ungar A, Bertolone C, et al. Mechanism of syncope without prodromes with normal heart and normal electrocardiogram. Heart Rhythm. (2017) 14:234–9. doi: 10.1016/j.hrthm.2016.08.046
11. Saadjian AY, Gerolami V, Giorgi R, Mercier L, Berge-Lefranc JL, Paganelli F, et al. Head-up tilt induced syncope and adenosine A2A receptor gene polymorphism. Eur Heart J. (2009) 30:1510–5. doi: 10.1093/eurheartj/ehp126
12. Franceschi F, By Y, Peyrouse E, Fromonot J, Gerolami V, Kipson N, et al. A2A adenosine receptor function in patients with vasovagal syncope. Europace. (2013) 15:1328–32. doi: 10.1093/europace/eut066
13. Conlay LA, Conant JA, deBros F, Wurtman R. Caffeine alters plasma adenosine levels. Nature. (1997) 389:136. doi: 10.1038/38160
14. von Borstel RW, Wurtman RJ, Conlay LA. Chronic caffeine consumption potentiates the hypotensive action of circulating adenosine. Life Sci. (1983) 32:1151–8. doi: 10.1016/0024-3205(83)90121-2
Keywords: adenosine, syncope, neurally-mediated syncope, methodology, adenosine receptors
Citation: Groppelli A, Brignole M, Chefrour M, Gastaldi M, El Oufir F, Deharo JC, Parati G and Guieu R (2022) Adenosine Concentration in Patients With Neurally Mediated Syncope. Front. Cardiovasc. Med. 9:900023. doi: 10.3389/fcvm.2022.900023
Received: 19 March 2022; Accepted: 17 May 2022;
Published: 17 June 2022.
Edited by:
Antonio Sorgente, EpiCURA, BelgiumReviewed by:
Juan Idiaquez, Pontificia Universidad Católica de Chile, ChileCopyright © 2022 Groppelli, Brignole, Chefrour, Gastaldi, El Oufir, Deharo, Parati and Guieu. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Michele Brignole, bWJyaWdub2xlQG91dGxvb2suaXQ=
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.