 Muharrem Akin1*
Muharrem Akin1* Jan-Thorben Sieweke1
Jan-Thorben Sieweke1 Vera Garcheva1
Vera Garcheva1 Carolina Sanchez Martinez1
Carolina Sanchez Martinez1 John Adel1
John Adel1 Pia Plank1Paris Zandian1
Pia Plank1Paris Zandian1 Kurt-Wolfram Sühs2
Kurt-Wolfram Sühs2 Johann Bauersachs1
Johann Bauersachs1 Andreas Schäfer1
Andreas Schäfer1- 1Cardiac Arrest Center, Department of Cardiology and Angiology, Hannover Medical School, Hanover, Germany
- 2Department of Neurology, Hannover Medical School, Hanover, Germany
Background: Patients after out-of-hospital cardiac arrest (OHCA) are at increased risk for mortality and poor neurological outcome. We assessed the additive impact of interleukin 6 (IL-6) at admission to neuron-specific enolase (NSE) at day 3 for prognosis of 30-day mortality and long-term neurological outcome in OHCA patients.
Methods: A total of 217 patients from the HAnnover COoling REgistry with return of spontaneous circulation (ROSC) after OHCA and IL-6 measurement immediately after admission during 2017–2020 were included to investigate the prognostic value and importance of IL-6 in addition to NSE obtained on day 3. Poor neurological outcome was defined by cerebral performance category (CPC) ≥ 3 after 6 months.
Results: Patients with poor outcome showed higher IL-6 values (30-day mortality: 2,224 ± 524 ng/l vs 186 ± 15 ng/l, p < 0.001; CPC ≥ 3 at 6 months: 1,440 ± 331 ng/l vs 180 ± 24 ng/l, p < 0.001). IL-6 was an independent predictor of mortality (HR = 1.013/ng/l; 95% CI 1.007–1.019; p < 0.001) and poor neurological outcome (HR = 1.004/ng/l; 95% CI 1.001–1.007; p = 0.036). In ROC-analysis, AUC for IL-6 was 0.98 (95% CI 0.96–0.99) for mortality, but only 0.76 (95% CI 0.68–0.84) for poor neurological outcome. The determined cut-off value for IL-6 was 431 ng/l for mortality (NPV 89.2%). In patients with IL-6 > 431 ng/l, the combination with NSE < 46 μg/l optimally identified those individuals with potential for good neurological outcome (CPC ≤ 2).
Conclusion: Elevated IL-6 levels at admission after ROSC were closely associated with 30-day mortality. The combination of IL-6 and NSE provided clinically important additive information for predict poor neurological outcome at 6 months.
Introduction
High rates of mortality and poor neurological outcome limit short and long-term prognosis in patients with out-of-hospital cardiac arrest (OHCA) (1). Compromised circulation during cardiac arrest leads to cellular hypoxemia causing anaerobic metabolism and subsequent induction of cell death, a process which continuously progresses even after return of spontaneous circulation (ROSC) (2). This leads to an inflammatory sepsis-like syndrome, the so called post-cardiac arrest syndrome, with marked increase in cytokine levels as a sign of activated inflammation and hemostasis which in turn may lead to secondary brain injury and myocardial dysfunction (3). While interleukin 1 and TNF-α are the primary pro-inflammatory cytokines, interleukin 6 (IL-6) is considered as a major “messenger” cytokine (4).
IL-6 is associated with an increased immune response and an unfavorable outcome in asphyxic neonates (5). Besides its role as a differentiation factor for B-cells, IL-6 also regulates hematopoiesis, inflammation, and neurogenesis (6, 7). Elevated IL-6 levels also have been observed in cerebral ischemia (7). Cerebral ischemia results in release of several pro-inflammatory cytokines, including IL-6 (8). During cardiac arrest, blood-brain barrier permeability is increased leading to elevated serum interleukin concentrations (9, 10).
Increased IL-6 levels were associated with poor outcome in OHCA patients (11–14). While approaches with untargeted cytokine hemoadsorption after OHCA aiming for IL-6 reduction showed no benefit in survival (15, 16), the impact of targeted antibody therapy with an IL-6 receptor antagonist, tocilizumab, is currently investigated (17).
Here, we investigated the prognostic value of additive IL-6 measurements on top of routine sampling of neuron-specific enolase (NSE) to predict 30-day mortality and/or 6-month poor neurological outcome in patients from the HAnnover COoling REgistry (HACORE) population, since more recent analyses indicated that relying on NSE alone to predict poor neurological outcome with reasonable accuracy will require much higher cut-offs than previously recommended (18, 19). HACORE is suitable for this investigation since all OHCA patients receive standardized care according to a specific regimen (HaCRA) without routine application of early prognostication with intention of withdrawing life-support (20). Thereby, our cohort is not confounded by a self-fulfilling prophecy regarding poor outcome.
Materials and Methods
Study Design and Patients
HACORE, a prospective observational registry, is in accordance with the Declaration of Helsinki and approved by the ethics committee (#3567–2017) at Hannover Medical School. Written informed consent was obtained from legal guardians during the unconscious period and re-consented by survivors after gaining consciousness. HACORE includes anonymized data from all OHCA patients treated at our cardiac arrest center with a standardized protocol including therapeutic hypothermia (20).
In the present study, we included all adult patients (n = 217) with OHCA and ROSC at admission to our center between 2017 and 2020 including complete data for IL-6 values at hospital admission and follow-up data from HACORE (Supplementary Figure 1). Patients were followed up for the period of their hospital stay and data were extracted from the electronic hospital patient data management system. Discharge letters from rehabilitation facilities were collected. Telephone-follow up was performed to assess long-term data, and neurological outcome was assessed by the Glasgow-Pittsburgh cerebral performance category (CPC) after 6 months. CPC is recommended by the Utsetin guidelines and is used for outcome measure for post-arrest neurological deficits as result of hypoxic-ischemic insult and reperfusion injury (21). It consist of 5 categories defined as 1: good cerebral performance, 2: moderate cerebral disability, 3: severe cerebral disability, 4: coma or vegetative state and 5: brain death. For scientific assessment in generous it is divided in good (CPC 1 and 2) and poor (CPC 3-5) outcome (21).
Patients were excluded from the analysis when they had ongoing cardiopulmonary resuscitation at admission. Because IL-6 values are influenced by chronic alcohol abuse, OHCA-patients with history of chronic alcohol abuse were excluded (22).
Patient Management After Out-of-Hospital Cardiac Arrest Using Hannover Cardiac Resuscitation Algorithm
The Hannover Cardiac Resuscitation Algorithm (HaCRA) for patients after OHCA was performed as described previously (20). In summary, this approach includes a standardized procedure for the care of patients with OHCA. Patients are screened in an interdisciplinary manner in the emergency room, stabilized and cared for to the extent to transfer the patients for further clarification by cardiac catheterization and computed tomographic examination. Subsequently, standardized care is provided in the cardiac ICU of the cardiac arrest center, where patients receive therapeutic hypothermia using an intravascular cooling catheter (Coolguard Quattro®, ZOLL Medical, San Jose, CA, United States) with the aim of maintaining a core body temperature of 32°C for 24 to 48 h, followed by a controlled rewarming phase of 0.25°C per hour (23). During intensive care, neurological monitoring included 24-h recording of a 3-pole EEG, regular assessment of pupils by an automated measuring device, and determination of markers by laboratory chemistry were performed. First blood samples were collected in the emergency room prior to any treatment. Out of this sample using standard serum tubes IL-6 was measured by immune assay (Roche, Electro-Chemi-Luminescent-Immuno Assay (ECLIA) test kit on Cobas 8000 auto-analyzer, Roche Diagnostics GmbH, Germany). Neuromarkers were determined from clinical routine blood samples taken at day 3 after admission using standard serum tubes by immune assay (for NSE even like IL-6 with ECLIA test kit and for S-100b with sandwich-immunoassay both determined on a Cobas 8000 auto-analyzer (Roche Diagnostics GmbH, Germany) (18). None of these components served at any time solely for decision making for neurological outcome nor for withdrawal of life support. Those were only considered as indicators to trigger further diagnostics, e.g., repetitive brain imaging to detect extensive anoxic brain injury. Nevertheless, despite rather weak level of evidence for prognostication its use has been recommended in different ways by certain guidelines (24–26). After acute intensive care and stabilization, patients were transferred to appropriate rehabilitation centers with neurological-intensive care to achieve an optimal neurological outcome.
Statistical Analysis
Baseline characteristics are presented as frequencies (n) and percentages (%), means ± standard deviation (SD) for normally distributed variables, or median and interquartile ranges (IQR) for non-normally distributed variables. Normally distributed variables were compared by Student’s t-test and Mann–Whitney test for non-parametric data, respectively. All group comparisons of continuous measures were performed using Wilcoxon’s test, whereas the chi-square or Fisher’s exact test was used to assess categorical data. Univariate Cox regression was performed including all variables potentially associated with 30-day mortality and 6 month poor neurological outcome, respectively. Predictors were specified using a multivariate Cox regression analysis with those variables, which were statistically significant in univariate Cox regression analysis. Results from the regression analyses were displayed as hazard ratios (HRs) with 95% confidence intervals (CIs). Prior multi-collinearity was assessed by variance inflation factor (VIF). We assessed the predictive accuracy of IL-6 and NSE for 30-day survival and neurological outcome in the first 6 months according to CPC-score by receiver operating characteristic (ROC) curves. Results were expressed in terms of area under the curve (AUC) and 95% CI for this area. Cut-off values for prediction were defined as the cut-off point having the highest Youden index (Yi = sensitivity + specificity -1). Sensitivity, specificity, positive and negative predictive value, accuracy for determined cut-offs were calculated.
Statistical analyses were performed using SPSS Statistics 26 (IBM SPSS Statistics 26) and GraphPad Prism 6.0 (GraphPad Software, Inc., La Jolla, CA, United States) for creating figures. A two-sided p-value of < 0.05 was considered statistically significant.
Results
Patient Characteristics
Out of 217 patients identified and included for our analysis, 120 (55%) patients survived to day 30. Good neurological outcome at 6 months after OHCA defined by CPC of ≤ 2 was observed in 59 (27%) admitted patients (Table 1). Mean age was 62 ± 15 years, and younger age was more common in survivors (58 ± 16 vs. 67 ± 12 years, p < 0.001) as well as in patients with good neurological outcome (56 ± 14 vs. 65 ± 14 years, p < 0.001). A shockable first rhythm after ROSC was more common in patients surviving 30-days and those with good neurologic outcome. IL-6, NSE, S-100b and lactate were significantly higher in patients with poor neurological outcome and in patients dying within the first 30 days. Characteristics such as cardiovascular risk factors, history of atherosclerosis and manifestation of pre-existing health conditions were almost equally distributed between those groups (Table 1). Patients with poor outcome showed higher IL-6 values (30-day mortality: 2,224 ± 524 ng/l vs 186 ± 15 ng/l, p < 0.001; CPC ≥ 3 at 6 months: 1,440 ± 331 ng/l vs 180 ± 24 ng/l, p < 0.001). IL-6 in particular was a better discriminator regarding mortality than to detect good neurological outcome (Figure 1). On the other hand NSE and S-100b were more discriminative for neurological outcome than for mortality and lactate was unspecific (Supplementary Figure 2).
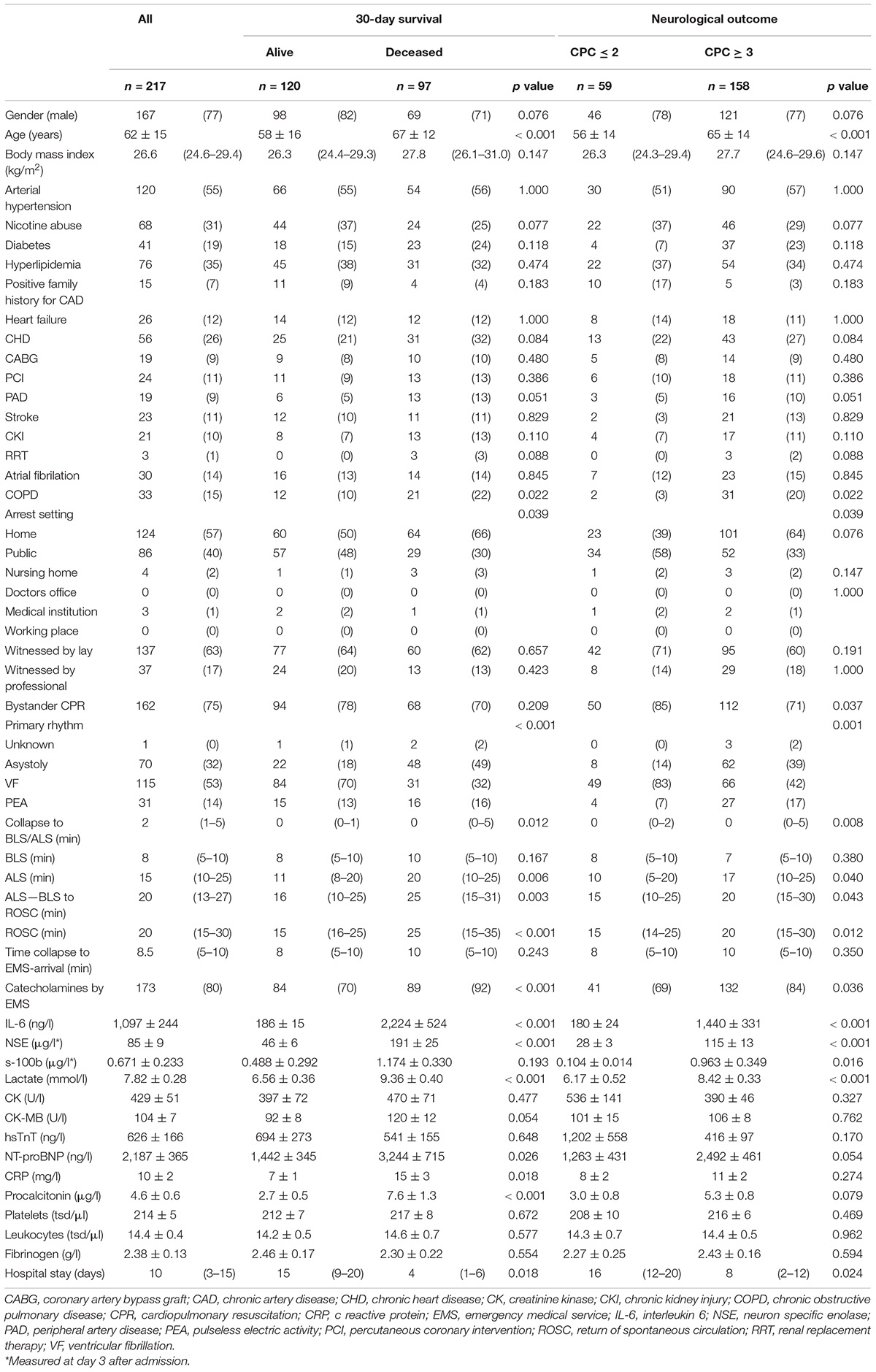
Table 1. Baseline characteristics and distribution according to 30-day survival and neurological outcome during first 6 month.
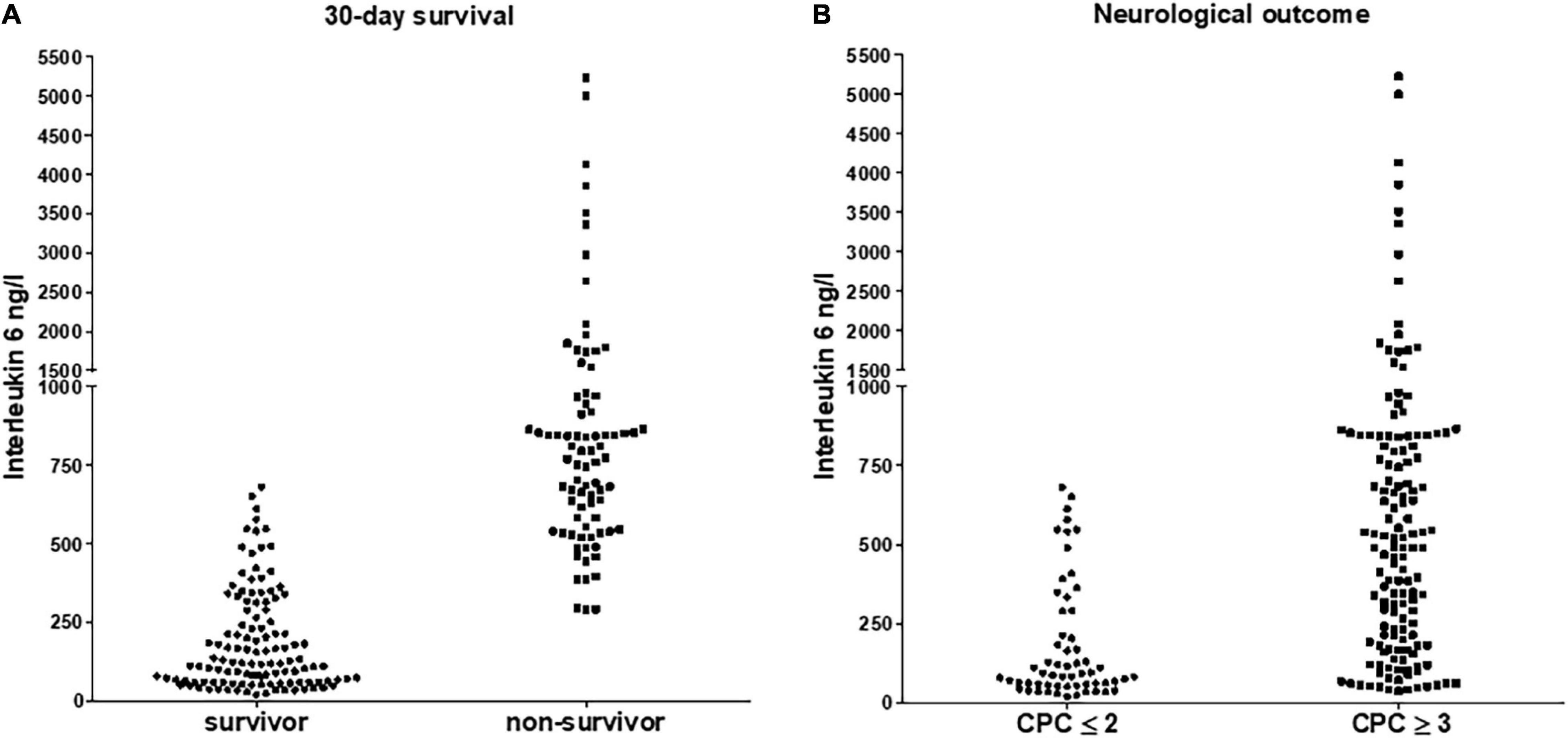
Figure 1. Distribution of interleukin 6 according to 30-day survival (A) for survivors and non-survivors and according to neurological outcome (B) for patients with good (CPC ≤ 2) and poor outcome (CPC ≥ 3), respectively. For both p was < 0.05.
Univariate and Multivariate Cox Regression Analysis
Overall 30-day mortality was only associated with admission IL-6 levels (HR = 1.013/ng/l; 95% CI 1.007–1.019; p < 0.001) and NSE at day 3 after arrest (HR = 1.013/μg/l; 95% CI 1.004–1.022; p = 0.005) in multivariate analysis (Table 2A), whereas impaired neurological outcome including deceased patients was associated with IL-6 (HR = 1.004/ng/l; 95% CI 1.001–1.007; p = 0.036), NSE (HR = 1.018/μg/l; 95% CI 1.004–1.032; p = 0.011), a history of diabetes, non-public arrest and a primary non-shockable rhythm (Table 2B and Supplementary Figure 3).
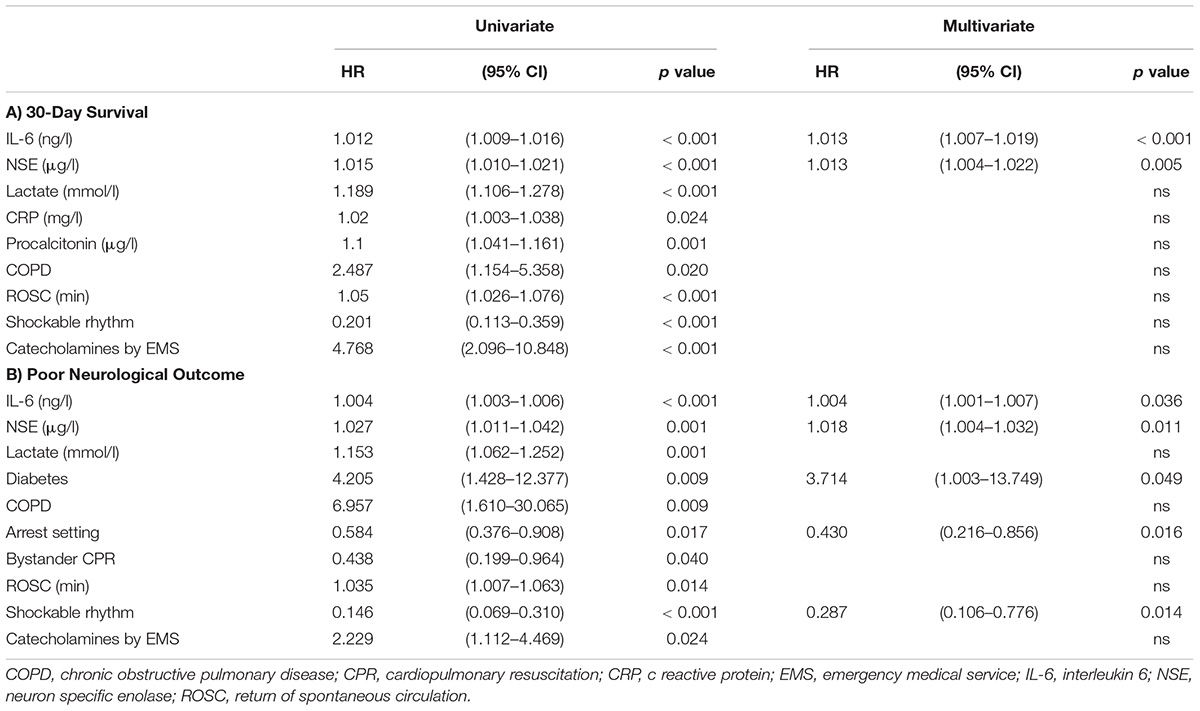
Table 2. Univariate and Multivariate Cox regression Analysis for (a) 30-day survival and (b) poor neurological outcome.
Interquartile Proportions of IL-6 in Relation to 30-Day Survival
No patient within the lowest IL-6 quartile (<110 ng/l) of our population died within the first 30 days, whereas no patient within the highest quartile (>797 ng/l) survived longer than 27 days. Of patients in the second IL-6 quartile (110–384 ng/l) 9% and, of patients in the third IL-6 quartile (384–797 ng/l) 70% died within the first 30 days (Figure 2).
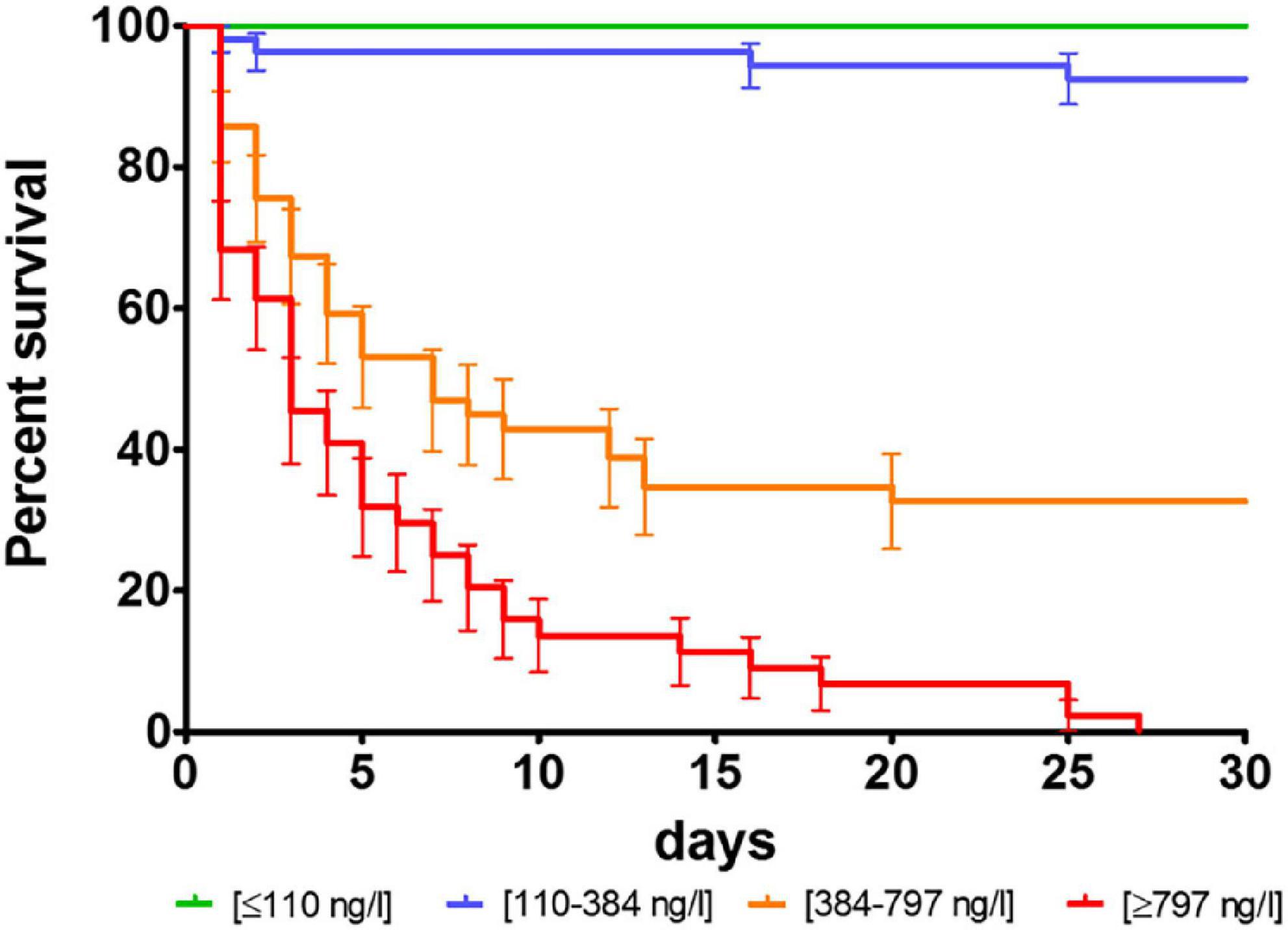
Figure 2. Survival proportions of interleukin 6 according to quartiles of HACORE population. p was < 0.0001 in log-rank test.
Receiver Operating Characteristic Analysis and Definition of Cut-Off Values
The discriminative value of IL-6 and NSE to predict 30-day mortality and poor 6-months neurological outcome was determined using ROC analysis (Figure 3). The area under the curve was higher for both, IL-6 and NSE, predicting 30-day mortality than poor neurological outcome (AUC 0.98; 95% CI 0.96–0.99 vs. 0.76; 95% CI 0.68–0.84 for IL-6, and 0.88; 95% CI 0.81–0.94 vs. 0.76; 95% CI 0.68–0.083 for NSE, respectively). According to the highest Youden-Index a cut-off value for IL-6 of 431 ng/l (YI: 0.863) and for NSE of 46.5 μg/l (YI: 0.690) for 30-day mortality as well as a cut-off for IL-6 of 131 ng/l (YI: 0.433) and for NSE of 44.5 μg/l (YI: 0.469) for poor neurological outcome could be identified. Overall, IL-6 was most useful in predicting 30-day mortality while NSE was more helpful to discriminate long-term neurological outcome (Table 3). The lowest IL-6 value to predict good neurological outcome with a 100% specificity was 21 ng/l and highest value to predict poor outcome with a 100% specificity was 682 ng/l.
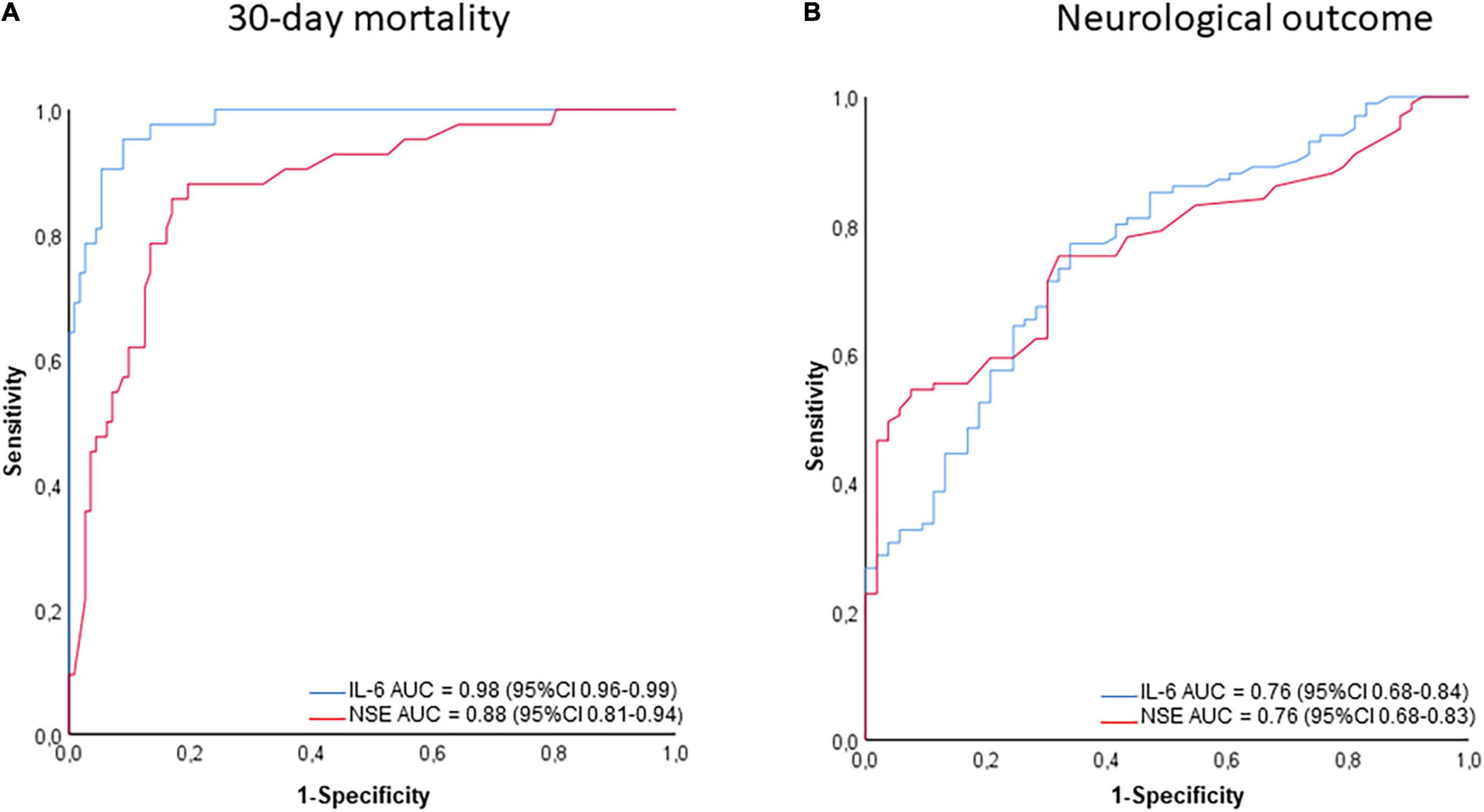
Figure 3. ROC curves for NSE and IL-6 for 30-day survival (A) and poor neurological outcome (B). For both p was < 0.001.

Table 3. Sensitivity, specificity and predictive values for identified cut-off values.
Survival Proportions and Prognostic Value According to Identified Cut-Off Values
Overall 47 patients died within the first 3 days. As NSE was originally determined only on day 3, there were no NSE values for these patients. For these 47 patients the median value of IL-6 at admission was 846 ng/l (IQR 643–1,876 ng/l). Regarding to the determined cut-off values for mortality in patients surviving for more than 3 days, 92 patients had lower values [IL-6 < 431 ng/l (median 103 ng/l; IQR 59–184 ng/l) and NSE < 46.5 μg/l (median 23 μg/l; IQR 18–30 μg/l)]. One of 92 (1%) died within the first 30 days. After 6 months, 48 out of 91 patients (53%) showed a good neurological outcome (CPC ≤ 2).
An IL-6 < 431 ng/l (median 213 ng/l; IQR 99–335 ng/l) and NSE > 46.5 μg/l (median 142 μg/l; IQR 86–178 μg/l) was present in 19 patients. Of those one patient (5%) died within the first 30 days. After 6 months, 3 out of 18 (17%) showed a good neurological outcome (CPC ≤ 2).
An IL-6 > 431 ng/l (median 612 ng/l; IQR 544–826) and NSE < 46.5 μg/l (median: 28 μg/l; IQR 22–35 μg/l) was present in 15 patients, while 5 out of 15 (33%) died within the first 30 days. After 6 months, 8 out of 15 (53%) showed a good neurological outcome (CPC ≤ 2) and 7 out of 15 (47%) showed a poor neurological outcome (CPC 3 or 4).
Values above the determined cut-off values [IL-6 > 431 ng/l (median: 804 ng/l; IQR 618–1,142 ng/l) and NSE > 46.5 μg/l (median: 189 μg/l; IQR 126–260 μg/l)] was present in 44 patients and 43 of them (98%) died within the first 30 days. After 6 months, the only one survivor had a poor neurological outcome (CPC = 4).
Overall, a value of IL-6 above the cut-off value has a more prognostic impact on the prediction of 30-day mortality than on neurological outcome. On the other hand, an elevated NSE value seems to be more predictive of poor neurological outcome than mortality. Exceeding both cut-offs is highly predictive for mortality (Figure 4). Importantly, low NSE values in patients with high IL-6 helps to identify patients who are likely to have a good neurological outcome if they survive the initial post-resuscitation phase (Figure 5).
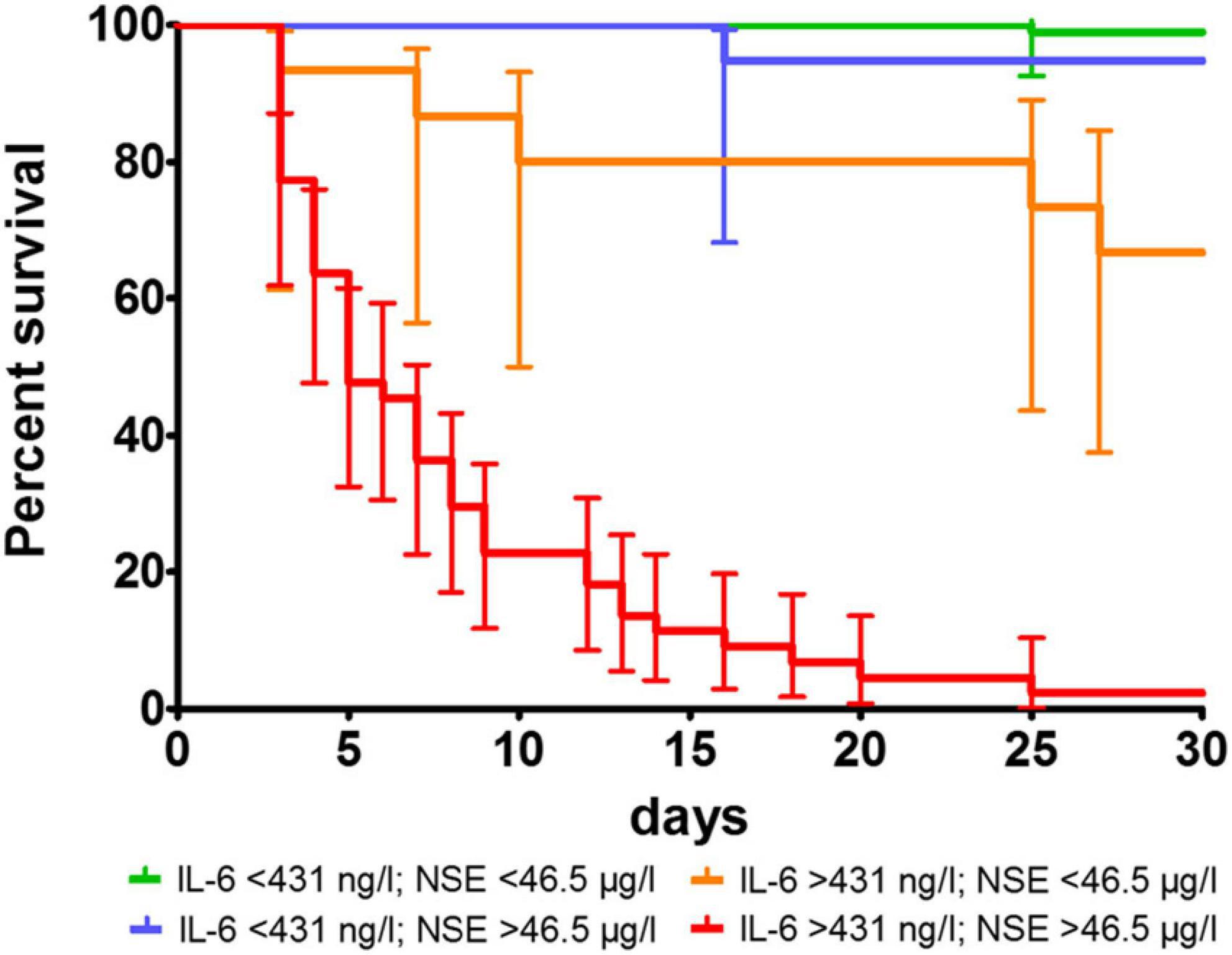
Figure 4. Survival proportions of combined determined cut-off values for mortality for IL-6 and NSE. p was < 0.0001 in log-rank test.
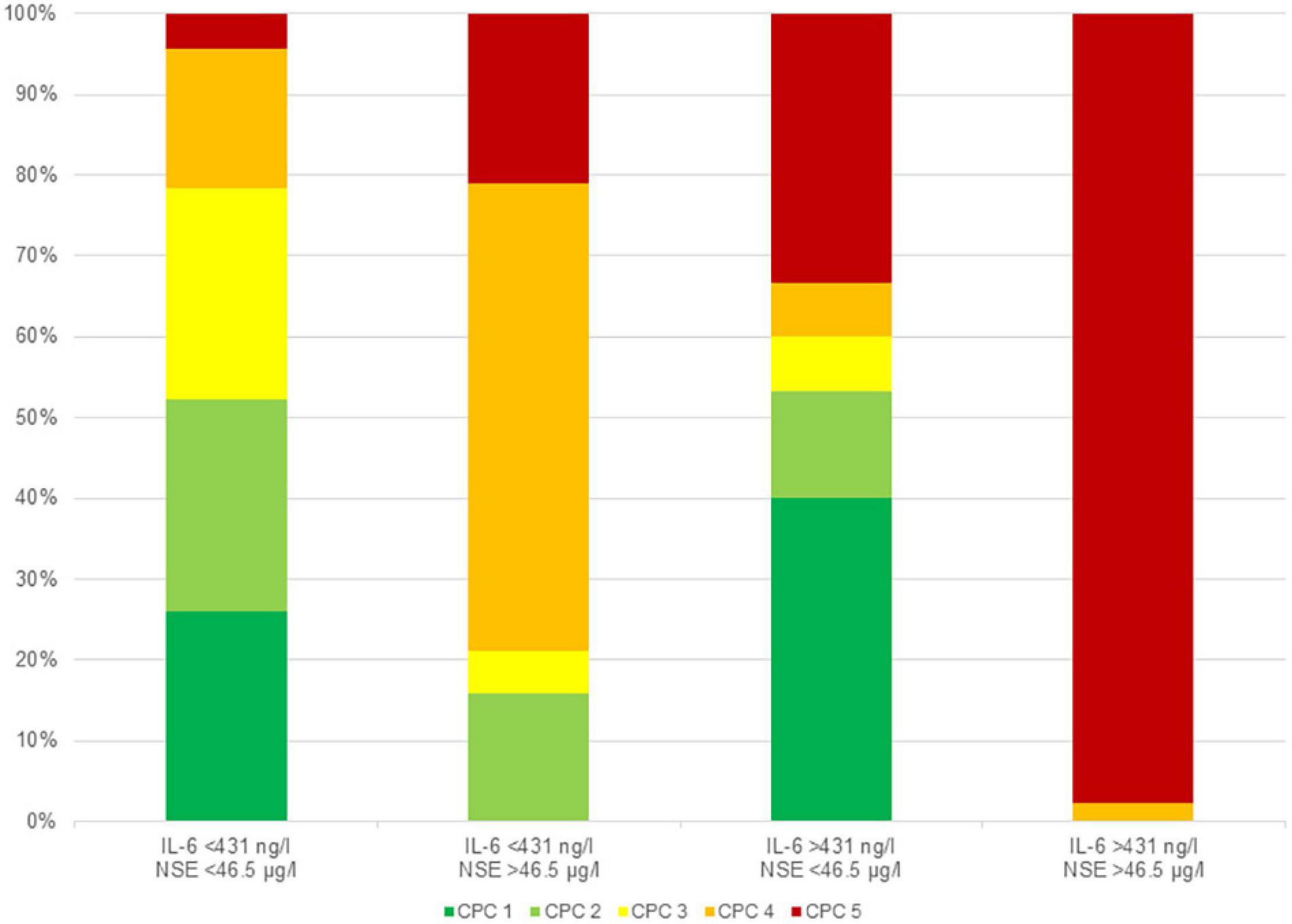
Figure 5. Neurological outcome according to CPC class in the corresponding groups depending to the determined cut-off values for mortality without patients dying during the first 3 days.
Discussion
Patients successfully resuscitated following OHCA and being treated within the HACORE cohort who died within 30 days or showed a less favorable neurological outcome at 6-months had higher levels of IL-6 immediately after hospital admission than survivors or those with good neurological outcome. While NSE was more favorable to predict poor neurological outcome, IL-6 was more strongly associated with 30-day overall survival. An IL-6 cut-off of 431 ng/l was best suited to predict 30-day mortality and a cut-off of 44.5 μg/l for NSE to predict neurological outcome.
Systemic ischemia/reperfusion response, cerebral injury and myocardial dysfunction as consequences of post-cardiac arrest syndrome are leading to a sepsis-like inflammatory reaction and release of interleukins in the brain as well as in the entire body (11, 27). IL-6 plays a key role as it is associated with leukocytes, vascular endothelium and parenchymal cells and is associated with unfavorable outcome even after cardiac arrest (17). Although IL-6 is present in the cerebrospinal fluid and brain, it remains undetermined whether the elevation in IL-6 levels after initiation of a systemic response by cardiac arrest is due to release from the cerebrospinal fluid or from necrotizing brain cells. For an exact differentiation, a direct sampling of cerebrospinal fluid would be necessary, but this is not feasible considering the urgent need for revascularization and antiplatelet therapy in many patients. Imaging using detection of previously labeled substances or cells could possibly help, but would be associated with a delay in the necessary primary care such as rapid induction of therapeutic hypothermia. Recognized effects of IL-6 include increased vascular permeability, fever, acute phase response, pro-coagulant effects, and induction of myocardial dysfunction (27). Also there are several observations in patients who have an increased release of IL-6 as a result of an infectious cause, which was accompanied by poor outcome (28). As a consequence, modulation of the systemic response has moved to the forefront as a therapeutic target to influence prognosis (29). Although an untargeted elimination and regulation of this response seems to be beneficial in systemic inflammatory response syndrome like in septic patients or in the setting of cardiac surgery, this may not be applicable for patients after cardiac arrest (15). However, there are new approaches that are more promising through targeted modulation (29, 30). The most recent approach is inhibiting IL-6 using tocilizumab, a monoclonal antibody against IL-6, in a post-cardiac arrest setting (17). The treatment with antibodies directed against IL-6 could reduce C-reactive protein and leukocyte levels as indicators for systemic inflammation as well as creatinine kinase myocardial band and troponin as indicators for myocardial injury (17). However, there was no benefit in survival or neurological outcome. Thus, the elimination of the inflammatory parameter, a potential factor leading to deterioration of neurological as well as cardiac function, will not be sufficient to cure these patients. Therefore, the goal remains in primary prevention of inflammation instead of secondary antagonism. One aspect might still be early initiation of therapeutic hypothermia in combination with causative treatment and high-quality intensive care medicine.
Neuroprognostication is a challenging task when treating post-arrest patients. While it is desirable to detect a futile outcome early during hospitalization, false-positive prognostication of poor outcome must be avoided. Current evidence regarding prognostication is weak (24). When using biomarkers for predicting neurological outcome, NSE is often used and recommended in guidelines, however, with differing cut-off levels (31, 32). While European guidelines use a cut-off above 60 ng/l for NSE as a marker of poor prognosis (32), we and others have recently shown that the false-positive prediction of poor neurological outcome by NSE at values between 60 and 100 ng/l is still too high (18, 19, 33). Trying to avoid the false-positive prediction when using NSE would result in a cut-off about 100 ng/l leading to many patients not being properly detected who will have a poor outcome. Although earlier studies have suggested to combine neuromarkers with other modalities trying to predict neurological prognosis, a NSE cut-off above 97 ng/ml had been suggested (34). Others have calculated different sometimes lower cut-offs, in particular when assessing the 72 h time-point (35). Depending on local protocols, cut-offs for one specific neuromarker might differ between populations. While the approach proposed by Daubin et al., suggesting the combination of NSE with non-biomarker predictors, is nowadays recommended by several guidelines, we believe that the combination of a neurological outcome-specific and a rather global mortality-related biomarker might further improve the quality and validity on the biomarker approach. Notwithstanding, the combined biomarker approach should still be accompanied by at least two other modalities (highly-malignant EEG, sever anoxic brain damage in cerebral imaging, non-reactive pupils in pupillometry, or bilateral absence of N20 peak in SSEP) in order to postulate a negative prognostication. Therefore, it might be of particular interest to combine certain easily measurable biomarkers, which assess different facets of the post-arrest syndrome. The combination of IL-6 and NSE appears to be a very promising approach allowing to combine lower thresholds for both parameters to predict a futile outcome. In particular, IL-6 helps to identify patients who are unlikely to survive and NSE further discriminates between likely good or poor neurological outcome. Therefore, we suggest to use both biomarkers in a sequential way.
Limitations
This observational and retrospective registry-based analysis reflects a realistic picture of association of admission IL-6 with 30-day mortality and neurological outcome in patients with OHCA who underwent a standardized intrahospital care with early coronary diagnostics and, if necessary, intervention and hypothermia- according to the HaCRA protocol. However, there are some limitations to address. First of all data were extracted from a monocentric retrospective registry. It cannot be ruled out that there is a bias, since not all factors related to changes in IL-6 and NSE levels have been investigated. If IL-6 were to be used as a tool for early decision making in post-arrest care, such strategy needs to be tested in a randomized controlled trial. An additional cause of inconsistency between studies is the variability of techniques used to measure biomarkers, which can cause a significant systematic error between techniques. For these reasons, current guidelines do not recommend any particular biomarker threshold to predict poor outcome with 100% specificity. An additional caveat for use of biomarkers is represented by extracerebral sources, which may cause false positive results. For NSE these include red blood cells, neuroendocrine tumors, and small cell carcinoma.
Conclusion
After out-of-hospital cardiac arrest IL-6 is elevated and particularly associated with 30-day mortality. Compared to established neuromarkers such as NSE, IL-6 seems to be less specific to predict neurological outcome. Therefore, it might be used as an early predictor for short-term mortality. Adjunctive use of NSE in patients identified as potential survivors by IL-6 can further discriminate between patients with favorable and unfavorable neurological outcome.
Data Availability Statement
The original contributions presented in the study are included in the article/Supplementary Material, further inquiries can be directed to the corresponding author/s.
Ethics Statement
The studies involving human participants were reviewed and approved by Hannover Medical School Ethics Committee (#3567–2017). The patients/participants provided their written informed consent to participate in this study.
Author Contributions
MA and AS designed the registry, recruited patients, analyzed the data, and drafted the manuscript. J-TS, VG, CM, JA, PP, and PZ recruited patients, analyzed the data, and revised the manuscript. K-WS revised the manuscript. JB designed the registry and drafted manuscript. All authors contributed to the article and approved the submitted version.
Funding
This study was partly supported by the Clinical Research Group (KFO) 311 of the Deutsche Forschungsgemeinschaft to JB. There was no additional external or internal funding received for this study. The funders had no role in study design, data collection and analysis, decision to publish, or preparation of the manuscript.
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s Note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary Material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fcvm.2022.899583/full#supplementary-material
Supplementary Figure 1 | Flow chart of identified HACORE patients with OHCA in 2017–2020 and selection for further analyzed patient’s.
Supplementary Figure 2 | Distribution of NSE (A,D), S-100b (B,E) and lactate (C,F) according to 30-day survival (A–C) for survivors and non-survivors and according to neurological outcome (D–F) for patients with good (CPC ≤ 2) and poor outcome (CPC ≥ 3), respectively.
Supplementary Figure 3 | Forest chart for univariate (A,C) and multivariate (B,D) analysis for 30-day survival (A,B) and poor neurological outcome (C,D).
Abbreviations
CPC, cerebral performance category; HACORE, HAnnover COoling REgistry; IL-6, interleukin 6; NSE, neuron-specific enolase; OHCA, out-of hospital cardiac arrest; ROSC, return of spontaneous circulation.
References
1. Grasner JT, Herlitz J, Tjelmeland IBM, Wnent J, Masterson S, Lilja G, et al. European resuscitation council guidelines 2021: epidemiology of cardiac arrest in Europe. Resuscitation. (2021) 161:61–79. doi: 10.1016/j.resuscitation.2021.02.007
2. Mentzelopoulos SD, Zakynthinos SG. Post-cardiac arrest syndrome: pathological processes, biomarkers and vasopressor support, and potential therapeutic targets. Resuscitation. (2017) 121:A12–4. doi: 10.1016/j.resuscitation.2017.10.013
3. Jou C, Shah R, Figueroa A, Patel JK. The role of inflammatory cytokines in cardiac arrest. J Intensive Care Med. (2020) 35:219–24. doi: 10.1177/0885066618817518
4. Libby P, Ridker PM. Novel inflammatory markers of coronary risk: theory versus practice. Circulation. (1999) 100:1148–50. doi: 10.1161/01.cir.100.11.1148
5. Ruhfus M, Giannakis S, Markus M, Stein A, Hoehn T, Felderhoff-Mueser U, et al. Association of routinely measured proinflammatory biomarkers with abnormal MRI findings in asphyxiated neonates undergoing therapeutic hypothermia. Front Pediatr. (2021) 9:624652. doi: 10.3389/fped.2021.624652
6. Erta M, Quintana A, Hidalgo J. Interleukin-6, a major cytokine in the central nervous system. Int J Biol Sci. (2012) 8:1254–66. doi: 10.7150/ijbs.4679
7. Spooren A, Kolmus K, Laureys G, Clinckers R, De Keyser J, Haegeman G, et al. Interleukin-6, a mental cytokine. Brain Res Rev. (2011) 67:157–83. doi: 10.1016/j.brainresrev.2011.01.002
8. Tarkowski E, Rosengren L, Blomstrand C, Wikkelso C, Jensen C, Ekholm S, et al. Intrathecal release of pro- and anti-inflammatory cytokines during stroke. Clin Exp Immunol. (1997) 110:492–9. doi: 10.1046/j.1365-2249.1997.4621483.x
9. Kaur C, Ling EA. Blood brain barrier in hypoxic-ischemic conditions. Curr Neurovasc Res. (2008) 5:71–81. doi: 10.2174/156720208783565645
10. Kossmann T, Hans VH, Imhof HG, Stocker R, Grob P, Trentz O, et al. Intrathecal and serum interleukin-6 and the acute-phase response in patients with severe traumatic brain injuries. Shock. (1995) 4:311–7. doi: 10.1097/00024382-199511000-00001
11. Chong JY, Ahn HJ, Park JS, You Y, Min JH, Jeong W, et al. Interleukin-6 as a potential predictor of neurologic outcomes in cardiac arrest survivors who underwent target temperature management. J Emerg Med. (2020) 59:828–35. doi: 10.1016/j.jemermed.2020.09.021
12. Peberdy MA, Andersen LW, Abbate A, Thacker LR, Gaieski D, Abella BS, et al. Inflammatory markers following resuscitation from out-of-hospital cardiac arrest-a prospective multicenter observational study. Resuscitation. (2016) 103:117–24. doi: 10.1016/j.resuscitation.2016.01.006
13. Vaahersalo J, Skrifvars MB, Pulkki K, Stridsberg M, Rosjo H, Hovilehto S, et al. Admission interleukin-6 is associated with post resuscitation organ dysfunction and predicts long-term neurological outcome after out-of-hospital ventricular fibrillation. Resuscitation. (2014) 85:1573–9. doi: 10.1016/j.resuscitation.2014.08.036
14. Bro-Jeppesen J, Johansson PI, Kjaergaard J, Wanscher M, Ostrowski SR, Bjerre M, et al. Level of systemic inflammation and endothelial injury is associated with cardiovascular dysfunction and vasopressor support in post-cardiac arrest patients. Resuscitation. (2017) 121:179–86. doi: 10.1016/j.resuscitation.2017.09.019
15. Akin M, Garcheva V, Sieweke JT, Flierl U, Daum HC, Bauersachs J, et al. Early use of hemoadsorption in patients after out-of hospital cardiac arrest – a matched pair analysis. PLoS One. (2020) 15:e0241709. doi: 10.1371/journal.pone.0241709
16. Supady A, Zahn T, Kuhl M, Maier S, Benk C, Kaier K, et al. Cytokine adsorption in patients with post-cardiac arrest syndrome after extracorporeal cardiopulmonary resuscitation (cyter) - a single-centre, open-label, randomised, controlled trial. Resuscitation. (2022) 173:169–78. doi: 10.1016/j.resuscitation.2022.02.001
17. Meyer MAS, Wiberg S, Grand J, Meyer ASP, Obling LER, Frydland M, et al. Treatment effects of interleukin-6 receptor antibodies for modulating the systemic inflammatory response after out-of-hospital cardiac arrest (the IMICA trial): a double-blinded, placebo-controlled, single-center, randomized, clinical trial. Circulation. (2021) 143:1841–51. doi: 10.1161/CIRCULATIONAHA.120.053318
18. Akin M, Garcheva V, Sieweke JT, Adel J, Flierl U, Bauersachs J, et al. Neuromarkers and neurological outcome in out-of-hospital cardiac arrest patients treated with therapeutic hypothermia-experience from the Hannover cooling registry (HACORE). PLoS One. (2021) 16:e0245210. doi: 10.1371/journal.pone.0245210
19. Lissner Ostlund E, Levin H, Nielsen N, Frigyesi A, Lybeck A. Neuron-specific enolase and long-term neurological outcome after OHCA – a validation study. Resuscitation. (2021) 168:206–13. doi: 10.1016/j.resuscitation.2021.09.001
20. Akin M, Sieweke JT, Zauner F, Garcheva V, Tongers J, Napp LC, et al. Mortality in patients with out-of-hospital cardiac arrest undergoing a standardized protocol including therapeutic hypothermia and routine coronary angiography: experience from the HACORE registry. JACC Cardiovasc Interv. (2018) 11:1811–20. doi: 10.1016/j.jcin.2018.06.022
21. Grossestreuer AV, Abella BS, Sheak KR, Cinousis MJ, Perman SM, Leary M, et al. Inter-rater reliability of post-arrest cerebral performance category (CPC) scores. Resuscitation. (2016) 109:21–4. doi: 10.1016/j.resuscitation.2016.09.006
22. Gruol DL, Melkonian C, Huitron-Resendiz S, Roberts AJ. Alcohol alters IL-6 signal transduction in the CNS of transgenic mice with increased astrocyte expression of IL-6. Cell Mol Neurobiol. (2021) 41:733–50. doi: 10.1007/s10571-020-00879-2
23. Lott C, Truhlar A, Alfonzo A, Barelli A, Gonzalez-Salvado V, Hinkelbein J, et al. European resuscitation council guidelines 2021: cardiac arrest in special circumstances. Resuscitation. (2021) 161:152–219. doi: 10.1016/j.resuscitation.2021.02.011
24. Geocadin RG, Callaway CW, Fink EL, Golan E, Greer DM, Ko NU, et al. Standards for studies of neurological prognostication in comatose survivors of cardiac arrest: a scientific statement from the American heart association. Circulation. (2019) 140:e517–42. doi: 10.1161/CIR.0000000000000702
25. Sandroni C, D’Arrigo S, Cacciola S, Hoedemaekers CWE, Kamps MJA, Oddo M, et al. Prediction of poor neurological outcome in comatose survivors of cardiac arrest: a systematic review. Intensive Care Med. (2020) 46:1803–51. doi: 10.1007/s00134-020-06198-w
26. Sandroni C, D’Arrigo S, Cacciola S, Hoedemaekers CWE, Westhall E, Kamps MJA, et al. Prediction of good neurological outcome in comatose survivors of cardiac arrest: a systematic review. Intensive Care Med. (2022) 48:389–413. doi: 10.1007/s00134-022-06618-z
27. Bro-Jeppesen J, Kjaergaard J, Wanscher M, Nielsen N, Friberg H, Bjerre M, et al. Systemic inflammatory response and potential prognostic implications after out-of-hospital cardiac arrest: a substudy of the target temperature management trial. Crit Care Med. (2015) 43:1223–32. doi: 10.1097/CCM.0000000000000937
28. Song J, Park DW, Moon S, Cho HJ, Park JH, Seok H, et al. Diagnostic and prognostic value of interleukin-6, pentraxin 3, and procalcitonin levels among sepsis and septic shock patients: a prospective controlled study according to the sepsis-3 definitions. BMC Infect Dis. (2019) 19:968. doi: 10.1186/s12879-019-4618-7
29. Tanaka T, Narazaki M, Kishimoto T. Immunotherapeutic implications of IL-6 blockade for cytokine storm. Immunotherapy. (2016) 8:959–70. doi: 10.2217/imt-2016-0020
30. Kang S, Tanaka T, Narazaki M, Kishimoto T. Targeting interleukin-6 signaling in clinic. Immunity. (2019) 50:1007–23. doi: 10.1016/j.immuni.2019.03.026
31. Bender A. S1-Leitlinie Hypoxisch-Ischämische Enzephalopathie Im Erwachsenenalter. Deutsche Gesellschaft Für Neurologie, Hrsg Leitlinien Für Diagnostik Und Therapie in Der Neurologie. Berlin: German Neurological Society (2018).
32. Nolan JP, Sandroni C, Bottiger BW, Cariou A, Cronberg T, Friberg H, et al. European resuscitation council and European society of intensive care medicine guidelines 2021: post-resuscitation care. Resuscitation. (2021) 161:220–69. doi: 10.1016/j.resuscitation.2021.02.012
33. Schafer A, Bauersachs J, Akin M. Therapeutic hypothermia following cardiac arrest after the TTM2 trial - more questions raised than answered. Curr Problems Cardiol. (2021). doi: 10.1016/j.cpcardiol.2021.101046 [Epub ahead of print].
34. Daubin C, Quentin C, Allouche S, Etard O, Gaillard C, Seguin A, et al. Serum neuron-specific enolase as predictor of outcome in comatose cardiac-arrest survivors: a prospective cohort study. BMC Cardiovasc Disord. (2011) 11:48. doi: 10.1186/1471-2261-11-48
35. Ryczek R, Kwasiborski PJ, Dymus J, Galas A, Kazmierczak-Dziuk A, Karasek AM, et al. Neuron-specific enolase concentrations for the prediction of poor prognosis of comatose patients after out-of-hospital cardiac arrest: an observational cohort study. Kardiol Pol. (2021) 79:546–53. doi: 10.33963/KP.15917
Keywords: out-of-hospital cardiac arrest, interleukin 6, neuron-specific enolase, neurological outcome, prognosis
Citation: Akin M, Sieweke J-T, Garcheva V, Martinez CS, Adel J, Plank P, Zandian P, Sühs K-W, Bauersachs J and Schäfer A (2022) Additive Impact of Interleukin 6 and Neuron Specific Enolase for Prognosis in Patients With Out-of-Hospital Cardiac Arrest – Experience From the HAnnover COoling REgistry. Front. Cardiovasc. Med. 9:899583. doi: 10.3389/fcvm.2022.899583
Received: 18 March 2022; Accepted: 13 May 2022;
Published: 31 May 2022.
Edited by:
Pier Leopoldo Capecchi, University of Siena, ItalyReviewed by:
Sonia D’Arrigo, Agostino Gemelli University Polyclinic (IRCCS), ItalyPawel Krzesinski, Military Institute of Medicine, Poland
Copyright © 2022 Akin, Sieweke, Garcheva, Martinez, Adel, Plank, Zandian, Sühs, Bauersachs and Schäfer. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Muharrem Akin, YWtpbi5tdWhhcnJlbUBtaC1oYW5ub3Zlci5kZQ==