 Manuel Chacón-Diaz1,2
Manuel Chacón-Diaz1,2 Akram Hernández-Vásquez
Akram Hernández-Vásquez Rodrigo Vargas-Fernández
Rodrigo Vargas-Fernández- 1Facultad de Ciencias de la Salud, Universidad Científica del Sur, Lima, Peru
- 2Instituto Nacional Cardiovascular, EsSalud, Lima, Peru
- 3Hospital Nacional Alberto Sabogal Sologuren, Lima, Peru
- 4Centro de Excelencia en Investigaciones Económicas y Sociales en Salud, Vicerrectorado de Investigación, Universidad San Ignacio de Loyola, Lima, Peru
Background: Heart failure (HF) is a global problem with a high mortality rate, and advanced HF (AHF) represents the stage with the highest morbidity and mortality. We have no local data on this population and its treatment. The aim of this study will be to determine the epidemiological, clinical, therapeutic, and annual survival characteristics of patients diagnosed with AHF treated in hospitals with HF units in the city of Lima, Peru.
Methods and Analysis: An observational, prospective, multicenter study will be conducted with evaluation at baseline and follow-up at 1, 3, 6, and 12 months after study entry. Patients over 18 years of age with AHF seen in referral health facilities in metropolitan Lima will be included. The cumulative mortality during follow-up will be estimated by the Kaplan-Meier method, and Cox regression models will calculate hazard ratios (HRs) and 95% confidence intervals (CI). Likewise, risk ratio (RR) and 95% CI will be estimated using generalized linear models with binomial family and log link function. This study was approved by the Ethics and Research Committee of the National Cardiovascular Institute (Instituto Nacional Cardiovascular “Carlos Alberto Peschiera Carrillo”—INCOR [in Spanish]; Approval report 46/2021-CEI).
Discussion: In Peru, there are no scientific data on the epidemiology of AHF in the population. This means that physicians are not adequately trained in the characteristics of the Peruvian population to identify patients who could be candidates for advanced therapies and to recognize the optimal time to refer these patients to more complex HF units. This study will be the first to examine the clinical-epidemiological characteristics of AHF in Peru with a follow-up of 1 year after the event and will provide relevant information on these observable characteristics for the management of high-complexity patients.
Introduction
Heart failure (HF) is a nosological entity of slow, progressive and sometimes unpredictable course, characterized by clinical, structural and functional deterioration of the heart, resulting from increased diastolic filling pressures and inadequate cardiac output unable to meet the metabolic and energetic demands of the organism (1). Globally, HF is a public health problem (2) with more than 60 million people suffering from this condition (29% have mild, 19% moderate and 51% have severe HF) in 2017. It is more frequent in females (34.8 million cases) than in males (29.5 million cases) and in high-income countries (871.1 cases per 100,000 population) (3), in which it is estimated that 1–2% of people live with HF (4). In addition, HF is estimated to have a high burden of disease, high rates of mortality and re-hospitalizations, impaired quality of life, and a significant economic burden, particularly due to frequent readmissions with a median hospital stay of 8.5 days [interquartile range (IQR: 7.38–11 days)] exceeding costs of $39 billion annually for health care systems (5–7).
In recent decades, the prognosis of patients with HF has considerably improved mainly due to significant innovations in medical therapy with neuromodulatory drugs and the development of device engineering (8). The prevalence of HF is increasing but with the development of effective treatment the survival is longer (9). Nonetheless, despite optimal medical therapy, 5% of patients with HF will inevitably progress to more advanced stages of the disease (10), being predominantly refractory with more severe signs and symptoms, more frequent decompensations and re-hospitalizations, poor quality of life and survival of <25% at 1 year and <8% at 2 years after diagnosis (11). From a health economics perspective, although advanced HF (AHF) affects only 1% of the population with HF, its high frequency of re-hospitalizations generates a significant consumption of resources that account for 60% of care costs, especially when surgical interventions such as heart transplantation or the implantation of a mechanical ventricular assist device are indicated (12). Therefore, the Interagency Registry for Assisted Mechanical Circulation (INTERMACS) classification system is a useful strategy to meet the needs of patients who are not eligible for advanced therapies, optimizing and implementing management strategies that reduce the high symptomatic burden of AHF and improving the quality of life of these end-stage patients. This system allows for better patient selection, better prognosis and determines the urgency of intervention (13).
The incidence of AHF is 0.2% of the world population (14). In the U.S., it is estimated that 250,000–500,000 patients are refractory to maximized medical therapy (7). In low- and middle-income countries, the severity of HF varies between countries and regions, with a prevalence of AHF ranging from 30.1 to 56.4% at diagnosis (15). Africa and Asia are the regions with the most severe HF phenotypes and have the lowest rate of health insurance, medication and educational level (16). In Latin America and the Caribbean, the prevalence of AHF varies between countries; between 4 and 6% of patients in Colombia have AHF with an annual mortality rate of almost 75% (17), about 2% of HF cases in Chile are refractory (18), and in Peru, 61 patients with AHF were transplanted between March 2010 and February 2018, and 26.3% of these patients required some type of mechanical circulatory assistance for bridging to cardiac transplantation (19).
In recent years, there have been reports of an increase in cardiovascular risk factors and in the survival of patients with HF in Latin American and Caribbean countries (20, 21). However, there is still little epidemiological evidence on AHF in the Peruvian population, which is corroborated by a bibliometric study on cardiovascular health in Peru, in which the main publications are related to HF in clinical trials (22). This increases the need to know the clinical and epidemiological profile and the therapeutic management of AHF in Peru in order to provide scientific evidence that is useful in clinical practice. Information on AHF in the Peruvian population is necessary and will serve as scientific evidence for the evaluation and development of strategies to reduce mortality and morbidity rates in patients with this medical condition.
Materials and Methods
Aim, Design and Setting of the Study
The general objective will be to determine the epidemiological, clinical, therapeutic, and annual survival characteristics of patients diagnosed with AHF treated in hospitals with HF units in the city of Lima, Peru. The specific objectives of the study will be: to determine the annual mortality of patients with AHF, calculate the rehospitalization rate of patients with AHF, determine the factors associated with a higher annual mortality in patients with AHF, correlate the INTERMACS profile with the outcomes of death, cardiac transplantation or mechanical assistance at 1 year in patients with AHF, determine the prevalence of patients with AHF in palliative therapy and with intermittent inotropic infusion, and finally, to build a prognostic score with the study variables and correlate with known scores such as the Seattle Heart Failure model.
This will be an observational, prospective, multicenter study with evaluation at baseline and follow-up at 1, 3, 6, and 12 months after study entry.
It will be performed in the cardiology services of the referral health facilities at the national level of social security, which are located in Metropolitan Lima: Instituto Nacional Cardiovascular-INCOR, Hospital Nacional Guillermo Almenara Irigoyen, Hospital Nacional Edgardo Rebagliati Martins and Hospital Nacional Alberto Sabogal Sologuren of Essalud.
Participants and Selection Criteria
The inclusion and exclusion criteria are specified in Table 1.
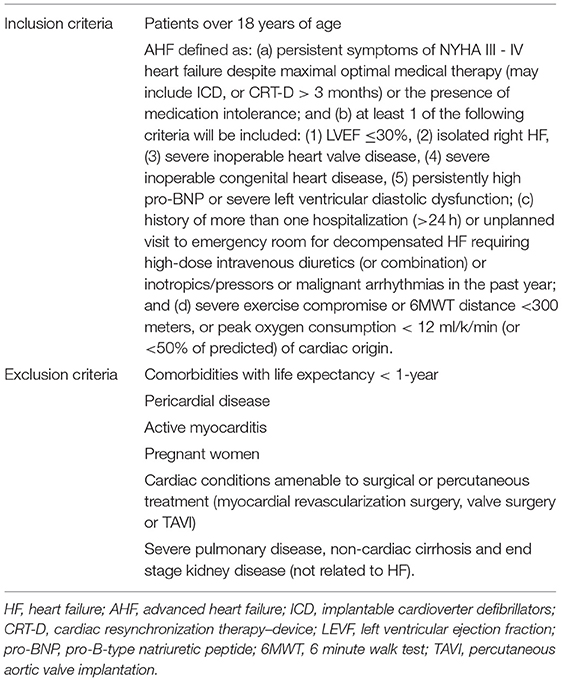
Table 1. Selection criteria for participants to be included in the study.
Informed Consent
Patients must provide consent by means of a written, signed and dated form. This document was approved on November 17, 2021, by the Ethics Committee of the National Cardiovascular Institute INCOR with resolution N°. 46/2021-CEI.
Study Procedures
At each institution included in the study, a cardiologist will be responsible for collecting the data during outpatient consultation or hospitalization and sending them to the registry coordinating center (Instituto Nacional Cardiovascular-INCOR) after obtaining informed consent. The data collection process will be performed on the data collection sheet designed for the study. The final database will only be accessible with an electronic user ID and password and will be stored in a secure electronic database.
For each patient included we will record the general characteristics (age, sex, care center), epidemiological characteristics (history of cardiovascular risk factors), etiology of HF, medication used (doses of the main HF medicines achieved), tests performed (echocardiography, 6-minute walk test, cardiopulmonary test, etc.), inpatient and/or outpatient treatment (intermittent ambulatory inotropic therapy, iron deficit treatment, etc.), number of hospitalizations due to decompensation or malignant arrhythmias, treatment during hospitalizations, and outcomes (death, transplantation and/or placement of mechanical assistance devices).
Follow-up data at 1, 3, 6, and 12 months after study entry will be collected by telephone interview (for remote data collection in a timely manner and taking pandemic conditions) and by reviewing patients' electronic medical records. Detailed information on the variables to be collected can be found in the Supplementary Table S1.
Sample Size and Power
All patients attended in the centers participating in the study over the course of 1 year who meet the inclusion criteria will be included. It is known from studies in other countries that AHF is present in up to 5% of patients with HF (23). Thus, for an unknown population of patients with HF, a minimum sample of 81 patients with AHF is estimated, based on an alpha value of 0.05, a 95% confidence interval (95% CI), and an expected 10% loss to follow-up.
Outcome Measures
Cardiovascular mortality (up to the first year after study entry). Cardiac transplantation. Time to first hospitalization for HF decompensation (requiring hospitalization with use of intravenous diuretics or inotropics).
Statistical and Analytical Plans
Stata version 14 will be used to conduct the analyses. Clinical and demographic characteristics of the patients will be reported according to the type of variable included. Numerical variables will be reported as means and standard deviation or medians and IQR, while categorical variables will be reported by absolute frequencies and proportions.
Comparisons of predictor variables for the outcomes of interest will be performed using the chi-square test for categorical variables. For numerical variables, the Student's t-test or one-way analysis of variance or non-parametric test will be used depending on fulfillment of the normal distribution assumption. The risk ratio (RR) and 95% CI will be estimated using generalized linear models with binomial family and log-link function. The variables age, sex, Seattle HF model score, HF etiology, and hospitalizations will be considered as variable predictors.
In addition, the cumulative in-hospital mortality during follow-up will be estimated with the Kaplan-Meier method, and the log-rank test will be used to evaluate the differences between survival curves. Finally, Cox regression models will calculate Hazard ratios (HRs) and 95% CI.
P-values <0.05 will be deemed statistically significant.
Data Storage and Management
The principal investigator (PI) (cardiologist) at the participating tertiary health centers will enter the data of the participants included in the study. A physical registration system will be used for this process. Each registered patient will be assigned a unique identification code to preserve anonymity. The physical forms will be entered into an electronic database that will be preserved with a password with which only the PI of the study will have access to the final data set of the study.
Ethics and Dissemination
The study was approved by the Ethics Committee of the “Instituto Nacional Cardiovascular Carlos Alberto Peschiera Carrillo-INCOR”, an institutional review committee recognized by the National Health Institute of Peru (https://www.ins.gob.pe/registroEC/listaregistroCIEI.asp), with Approval Report N° 46/2021-CEI. The study will be conducted in accordance with the Declaration of Helsinki.
At the end of the study, the results will be published in articles in peer-reviewed scientific journals and at scientific congresses. To improve the quality of the reporting of the results, this study will follow the guidelines of the STROBE statement for the writing of articles generated from the study (24).
Status and Timeline of the Study
Patient enrollment will be from January 15, 2022 to December 31, 2022 in EsSalud hospitals with trained cardiologist medical staff who provide care to patients with AHF. Once the patient is admitted to the study, telephone and/or face-to-face follow-up will be performed at 1, 3, 6, and 12 months after study entry. Thus, follow-up is expected to end in December 2023 and presentation of the final results will be in April 2024. The timeline of the study is specified in Figure 1.
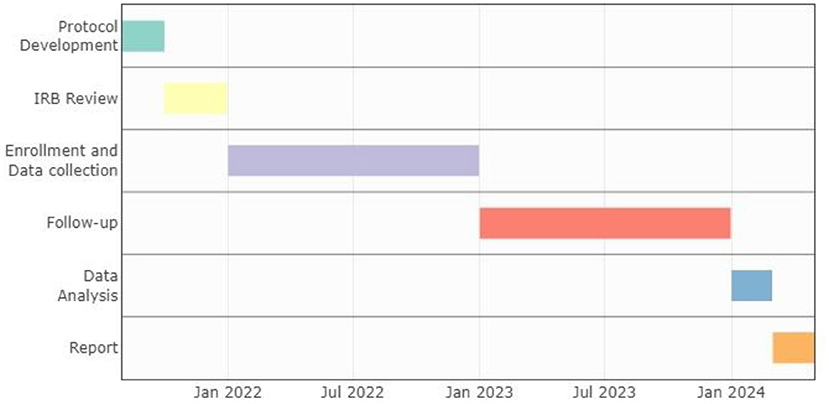
Figure 1. Study timeline and milestones. We use package vistime in RStudio for visualization.
Discussion
The present study will provide information on the epidemiological, clinical, therapeutic, and annual survival characteristics of patients diagnosed with AHF treated in hospitals with HF units in the city of Lima, Peru. Therefore, we seek to increase knowledge about the epidemiology and appropriate management of AHF in high resolution hospitals in Peru, which have a high demand for medical care and where patients do not have a palliative care program when they do not have therapeutic options.
However, patients with AHF should be properly defined and identified to facilitate the application of treatments such as cardiac transplantation or long-term mechanical circulatory support devices. In Peru, there is no scientific evidence describing the current panorama of AHF in the population. This means that physicians are not properly trained with the characteristics of the Peruvian population to identify patients who could be candidates for such therapies and to recognize the optimal time to refer them to more complex HF units. Therefore, a hospital registry of AHF in the network of hospitals with HF units in the country is necessary to know the incidence, prevalence, and prognostic implications of this pathology in the Peruvian population.
Among the strengths of the study is its multicenter character, which will help to obtain a representative sample of the population with the condition studied, increasing the external validity of the results. In addition, it will be the first study to examine the epidemiological characteristics of AHF in public hospitals in Peru, providing relevant information on these observable characteristics in the management of high complexity patients. On the other hand, among the limitations of the study, the study can only describe associations and not causality due to its observational design. AHF is an infrequent pathology that will generate a low number of patients to be included in the study and there could be errors in data collection when using medical records.
Currently, the coronavirus disease pandemic (COVID-19) has led to changes in the epidemiology and management of HF worldwide, with decreased hospital admissions, delayed emergency care, and increased risk of complications (25, 26). In addition, these changes extrapolate into barriers to research, especially in the conduct of studies that require extensive physical examination, primary data collection, and face-to-face follow-up of participants (27, 28). Despite the fact that the study will be conducted in a pandemic context and with limited access to hospital centers, it is a priority to have clinical-epidemiological information on AHF in high resolution hospital centers in Peru to help Peruvian cardiologists in the search for the optimal management of these patients.
Author Contributions
MC-D: conceptualization, project administration, resources, investigation, supervision, methodology, writing—original draft, and writing—review and editing. RL, AH-V, and RV-F: investigation, methodology, writing—original draft, and writing—review and editing. All authors contributed to the article and approved the submitted version.
Funding
This protocol was self-funded by the authors.
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's Note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Acknowledgments
We thank the heads of the Cardiology Departments of the participating hospitals for providing the facilities to carry out the study. The authors are grateful to Donna Pringle for reviewing the language and style.
Supplementary Material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fcvm.2022.896821/full#supplementary-material
References
1. McDonagh TA, Metra M, Adamo M, Gardner RS, Baumbach A, Böhm M, et al. 2021 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure. Eur Heart J. (2021) 42:3599–726. doi: 10.1093/eurheartj/ehab368
2. Adams KF, Fonarow GC, Emerman CL, LeJemtel TH, Costanzo MR, Abraham WT, et al. Characteristics and outcomes of patients hospitalized for heart failure in the United States: rationale, design, and preliminary observations from the first 100,000 cases in the Acute Decompensated Heart Failure National Registry (ADHERE). Am Heart J. (2005) 149:209–16. doi: 10.1016/j.ahj.2004.08.005
3. Bragazzi NL, Zhong W, Shu J, Abu Much A, Lotan D, Grupper A, et al. Burden of heart failure and underlying causes in 195 countries and territories from 1990 to 2017. Eur J Prev Cardiol. (2021) 15:1682–90. doi: 10.1093/eurjpc/zwaa147
4. Groenewegen A, Rutten FH, Mosterd A, Hoes AW. Epidemiology of heart failure. Eur J Heart Fail. (2020) 22:1342–56. doi: 10.1002/ejhf.1858
5. Blumer V, Mentz RJ, Sun J-L, Butler J, Metra M, Voors AA, et al. Prognostic role of prior heart failure hospitalization among patients hospitalized for worsening chronic heart failure. Circ Heart Fail. (2021) 14:4. doi: 10.1161/CIRCHEARTFAILURE.120.007871
6. Lippi G, Sanchis-Gomar F. Global epidemiology and future trends of heart failure. AME Med J. (2020) 5:15–15. doi: 10.21037/amj.2020.03.03
7. Norton C, Georgiopoulou VV, Kalogeropoulos AP, Butler J. Epidemiology and cost of advanced heart failure. Prog Cardiovasc Dis. (2011) 54:78–85. doi: 10.1016/j.pcad.2011.04.002
8. Choi H-M, Park M-S, Youn J-C. Update on heart failure management and future directions. Korean J Intern Med. (2019) 34:11–43. doi: 10.3904/kjim.2018.428
9. Crespo-Leiro MG, Metra M, Lund LH, Milicic D, Costanzo MR, Filippatos G, et al. Advanced heart failure: a position statement of the Heart Failure Association of the European Society of Cardiology. Eur J Heart Fail. (2018) 20:1505–35. doi: 10.1002/ejhf.1236
10. Costanzo MR, Mills RM, Wynne J. Characteristics of “Stage D” heart failure: insights from the Acute Decompensated Heart Failure National Registry Longitudinal Module (ADHERE LM). Am Heart J. (2008) 155:339–47. doi: 10.1016/j.ahj.2007.10.020
11. Rose EA, Gelijns AC, Moskowitz AJ, Heitjan DF, Stevenson LW, Dembitsky W, et al. Long-term use of a left ventricular assist device for end-stage heart failure. N Engl J Med. (2001) 345:1435–43. doi: 10.1056/NEJMoa012175
12. Saldarriaga Giraldo CI. Visión de la insuficiencia cardiaca avanzada. ¿Es demasiado tarde? Rev Colomb Cardiol. (2019) 26:245–6. doi: 10.1016/j.rccar.2019.09.001
13. Stevenson LW, Pagani FD, Young JB, Jessup M, Miller L, Kormos RL, et al. INTERMACS profiles of advanced heart failure: the current picture. J Heart Lung Transplant. (2009) 28:535–41. doi: 10.1016/j.healun.2009.02.015
14. Ammar KA, Jacobsen SJ, Mahoney DW, Kors JA, Redfield MM, Burnett JC, et al. Prevalence and prognostic significance of heart failure stages: application of the American College of Cardiology/American Heart Association heart failure staging criteria in the community. Circulation. (2007) 115:1563–70. doi: 10.1161/CIRCULATIONAHA.106.666818
15. Dokainish H, Teo K, Zhu J, Roy A, AlHabib KF, ElSayed A, et al. Global mortality variations in patients with heart failure: results from the International Congestive Heart Failure (INTER-CHF) prospective cohort study. Lancet Glob Health. (2017) 5:e665–72. doi: 10.1016/S2214-109X(17)30196-1
16. Dokainish H, Teo K, Zhu J, Roy A, AlHabib KF, ElSayed A, et al. Heart Failure in Africa, Asia, the Middle East and South America: The INTER-CHF study. Int J Cardiol. (2016) 204:133–41. doi: 10.1016/j.ijcard.2015.11.183
17. Gómez-Mesa JE, Saldarriaga C, Jurado AM, Mariño A, Rivera A, Herrera Á, et al. Consenso colombiano de falla cardíaca avanzada: capítulo de Falla Cardíaca, Trasplante Cardíaco e Hipertensión Pulmonar de la Sociedad Colombiana de Cardiología y Cirugía Cardiovascular. Rev Colomb Cardiol. (2019) 26:3–24. doi: 10.1016/j.rccar.2019.06.001
18. Castro GP, Vukasovic RJL, Garcés SE, Sepúlveda ML, Ferrada KM, Alvarado OS. Insuficiencia cardíaca en hospitales chilenos: resultados del Registro Nacional de Insuficiencia Cardíaca, Grupo ICARO. Rev Médica Chile. (2004) 132:655–62. doi: 10.4067/S0034-98872004000600001
19. Aguilar C, Alarco W, Soplopuco F, Morón J, Lescano M, Morales J, et al. Patología del trasplante cardiaco en el Perú: Experiencia con 61 casos en un centro de referencia nacional. Rev Peru Med Exp Salud Pública. (2018) 35:241. doi: 10.17843/rpmesp.2018.352.3264
20. Bocchi EA, Arias A, Verdejo H, Diez M, Gómez E, Castro P, et al. The reality of heart failure in Latin America. J Am Coll Cardiol. (2013) 62:949–58. doi: 10.1016/j.jacc.2013.06.013
21. Ciapponi A, Alcaraz A, Calderón M, Matta MG, Chaparro M, Soto N, et al. Burden of heart failure in Latin America: a systematic review and meta-analysis. Rev Esp Cardiol Engl Ed. (2016) 69:1051–60. doi: 10.1016/j.rec.2016.04.054
22. Vargas-Fernández R, Visconti-Lopez FJ, Barón-Lozada FA, Basualdo-Meléndez GW. Análisis bibliométrico de la producción científica peruana en cardiología y medicina cardiovascular. Arch Peru Cardiol Cir Cardiovasc. (2021) 2:167–74. doi: 10.47487/apcyccv.v2i3.157
23. Truby LK, Rogers JG. Advanced heart failure: epidemiology, diagnosis, and therapeutic approaches. JACC Heart Fail. (2020) 8:523–36. doi: 10.1016/j.jchf.2020.01.014
24. von Elm E, Altman DG, Egger M, Pocock SJ, Gøtzsche PC, Vandenbroucke JP, et al. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement: guidelines for reporting observational studies. J Clin Epidemiol. (2008) 61:344–9. doi: 10.1016/j.jclinepi.2007.11.008
25. Solomon MD, McNulty EJ, Rana JS, Leong TK, Lee C, Sung S-H, et al. The Covid-19 pandemic and the incidence of acute myocardial infarction. N Engl J Med. (2020) 383:691–3. doi: 10.1056/NEJMc2015630
26. Tomasoni D, Adamo M, Italia L, Branca L, Chizzola G, Fiorina C, et al. Impact of COVID-2019 outbreak on prevalence, clinical presentation and outcomes of ST-elevation myocardial infarction. J Cardiovasc Med. (2020) 21:874–81. doi: 10.2459/JCM.0000000000001098
27. Custodio-Sánchez P, Miranda D, Murillo L. Impacto de la pandemia por COVID-19 sobre la atención del infarto de miocardio ST elevado en el Perú. Arch Peru Cardiol Cir Cardiovasc. (2020) 1:87–94. doi: 10.47487/apcyccv.v1i2.22
Keywords: heart failure, heart disease risk factor, prospective study design, Peru, cardiovascular diseases
Citation: Chacón-Diaz M, Laymito Quispe R, Hernández-Vásquez A and Vargas-Fernández R (2022) Study Protocol for the Peruvian Registry of Advanced Heart Failure (REPICAV). Front. Cardiovasc. Med. 9:896821. doi: 10.3389/fcvm.2022.896821
Received: 15 March 2022; Accepted: 06 May 2022;
Published: 31 May 2022.
Edited by:
Gaetano Ruocco, Regina Montis Regalis Hospital, ItalyReviewed by:
Guido Pastorini, Regina Montis Regalis Hospital, ItalyFrancesca Valentini, Azienda USL Toscana Sud Est, Italy
Copyright © 2022 Chacón-Diaz, Laymito Quispe, Hernández-Vásquez and Vargas-Fernández. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Akram Hernández-Vásquez, YWhlcm5hbmRleiYjeDAwMDQwO3VzaWwuZWR1LnBl