 Chen-Han Zhang
Chen-Han Zhang Jun-Ming Zhu
Jun-Ming Zhu
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Cardiovasc. Med. , 08 July 2022
Sec. Cardiovascular Surgery
Volume 9 - 2022 | https://doi.org/10.3389/fcvm.2022.892696
This article is part of the Research Topic Current Trends and Strategies for the Management of Type A Aortic Dissection View all 11 articles
Background: Massive bleeding throughout aortic repair in acute type A aortic dissection (ATAAD) patients is a common but severe condition that can cause multiple serious clinical problems. Here, we report our findings regarding risk factors, short-term outcomes, and predicting model for massive bleeding in ATAAD patients who underwent emergent aortic repair.
Methods: A universal definition of perioperative bleeding (UDPB) class 3 and 4 were used to define massive bleeding and comprehensively evaluate patients. A total of 402 consecutive patients were enrolled in this retrospective study during 2019. Surgical strategies used to perform aortic arch procedures included total arch and hemiarch replacements. In each criterion, patients with massive bleeding were compared with remaining patients. Multivariable regression analyses were used to identify independent risk factors for massive bleeding. Logistic regression was used to build the model, and the model was evaluated with its discrimination and calibration.
Results: Independent risk factors for massive bleeding included male sex (OR = 6.493, P < 0.001), elder patients (OR = 1.029, P = 0.05), low body mass index (BMI) (OR = 0.879, P = 0.003), emergent surgery (OR = 3.112, P = 0.016), prolonged cardiopulmonary bypass time (OR = 1.012, P = 0.002), lower hemoglobin levels (OR = 0.976, P = 0.002), increased D-dimer levels (OR = 1.000, P = 0.037), increased fibrin degradation products (OR = 1.019, P = 0.008), hemiarch replacement (OR = 5.045, P = 0.037), total arch replacement (OR = 14.405, P = 0.004). The early-stage mortality was higher in massive bleeding group (15.9 vs. 3.9%, P = 0.001). The predicting model showed a well discrimination (AUC = 0.817) and calibration (χ2 = 5.281, P = 0.727 > 0.05).
Conclusion: Massive bleeding in ATAAD patients who underwent emergent aortic repair is highly associated with gender, emergent surgery, increased D-dimer levels, longer CPB time, anemia, and use of a complex surgical strategy. Since massive bleeding may lead to worse outcomes, surgeons should choose suitable surgical strategies in patients who are at a high risk of massive bleeding.
Acute type A aortic dissection (ATAAD) is one of the most complex and life-threatening disorders and can lead to catastrophic results, such as aortic rupture or even death (1). Medically managed ATAAD patients are at risk of poor outcomes, and mortality rates in these patients reach 20, 30, and 50% in the first 24 h after acute presentation, after 48 h, and after 1 month, respectively (2). Therefore, emergent aortic repair is the best treatment option for ATAAD and is potentially life-saving. Despite improvements in patient diagnosis and surgical techniques, aortic repair is still associated with high morbidity and mortality rates compared with other cardiac procedures (3, 4). Among all possible complications of aortic surgery, postoperative bleeding is one of the most prevalent and intractable. In particular, when the hemorrhage is massive, failed or delayed treatment may cause irreversible organ dysfunction, such as renal failure, cardiovascular events including myocardial injury, or even death (5). Therefore, a full understanding of ATAAD risk factors can significantly benefit clinical practice. Many factors may be related to postoperative hemorrhage, including surgical damage to blood vessels and hemostatic function disorders (6, 7). However, specific risk factors, and their incidence differ based on the institution as well as the country from which the data are collected (8). The present study aimed to analyze possible risk factors and short-term outcomes for massive postoperative bleeding in patients with ATAAD who underwent aortic repair emergently, we also made a predictive model which could provide details needed for clinical practitioners to avoid or minimize poor outcomes of the procedure.
This was a single-center, retrospective study, and data were collected from the electronic medical record database of Beijing Anzhen Hospital. A total of 402 consecutive patients who underwent emergent surgery for ATAAD repair during 2019 were enrolled in this study. Patients younger than 18 years old or diagnosed with hereditary connective tissue diseases before were excluded from the study. Each patient was counted only once in the analysis. The Institutional Review Board of Beijing Anzhen Hospital of Capital Medical University approved this retrospective study and waived the need for informed patient consent. The institutional approval number is 202075X.
In this study, the universal definition of perioperative bleeding (UDPB) was used to define massive bleeding (9, 10). The UDPB defines perioperative bleeding by nine clinical events during the surgery or within the first postoperative day. In UDPB, class 3 and 4 bleeding often requires or has already been performed aggressive medical interventions, otherwise, it may lead to extremely serious adverse consequences. Therefore, in this study, class 3 and 4 bleeding was defined as perioperative massive bleeding. Kidney disease: improving global outcomes (KDIGO) grade 3 was used to define the acute kidney injury in this study, and the fraction of inspired oxygen less than 300 was defined as respiratory failure.
All surgeries were performed via median sternotomy under moderate hypothermic circulatory arrest. A dual-stage atriocaval cannula was inserted into the right atrium, and the right axillary artery was isolated routinely for CPB and selected cerebral perfusion. The ascending aorta was clamped at the distal end, and then the patients’ nasopharyngeal temperature was reduced to approximately 25°C. During the cooling, proximal manipulations, such as aortic valve repair, sinus of Valsalva reconstruction, and composite valved graft replacement, would be commenced if necessary. CPB was discontinued when the nasopharyngeal temperature was lower than 25°C, while the selected cerebral perfusion was continued at a rate of approximately 5 to 10 mL × kg–1 × min–1 toward the right axial artery.
Methods of aortic arc surgery include hemiarch replacement and total arc replacement + frozen elephant trunk (FET); decision-making depends on the general condition of the patient, location of the entry tear, the distal extent of dissection, the occurrence of malperfusion, and intraoperative findings. The hemiarch replacement included arc repair of the distal anastomosis located at the proximal end of the aortic arch or part of the small curvature. In total arc replacement + FET, a stent is inserted as the FET into the descending aorta, and the remaining aortic arch is replaced by the four-branch artificial vessel. More details regarding the surgical procedure have been discussed in our previous studies (11–13).
Continuous data were presented as means ± standard deviation (SD) with a normal distribution and median (lower quartile, upper quartile) with a non-normal distribution, the categorical variables were described as percentages. For performing comparisons, a Student’s t-test or Mann–Whitney U test was used for continuous variables, and the Chi-square test or Fisher’s exact test was used for categorical variables. Multivariable regression analyses were conducted to explore relationships between perioperative parameters and severe bleeding using binary logistic modeling techniques. The risk predicting model was built using logistic regression. The area under the receiver operating characteristic curve (AUC) and 95% confidence intervals (CIs) were used to assess a model’s ability to discriminate between high- and low-risk patients. Hosmer–Lemeshow good of fit test was used to evaluate the calibration of the model. P-values determined using two-tailed distributions <0.05 were considered statistically significant. All statistical analyses were performed using SPSS 25.0 (IBM SPSS, Armonk, NY, United States) and GraphPad Prism 8.
In this study, 402 patients were enrolled, 69 of them presented with massive postoperative bleeding (17.2%), the detailed classification of massive bleeding was shown in Figure 1. The basic characteristics of patients were summarized in Table 1. The mean age was 52.13 ± 11.96 and 48.73 ± 11.63 years (P = 0.029), the mean body mass index (BMI) was 24.99 ± 3.99 in the massive bleeding group and 26.72 ± 7.86 in the non-massive bleeding group (P = 0.029), the mean hemoglobin and platelet count in two groups were 129.34 ± 22.26 g, 134.78 ± 18.41 g (P = 0.036), 180.72 ± 53.28 109/L, and 198.26 ± 75.57 109/L (P = 0.024), separately.
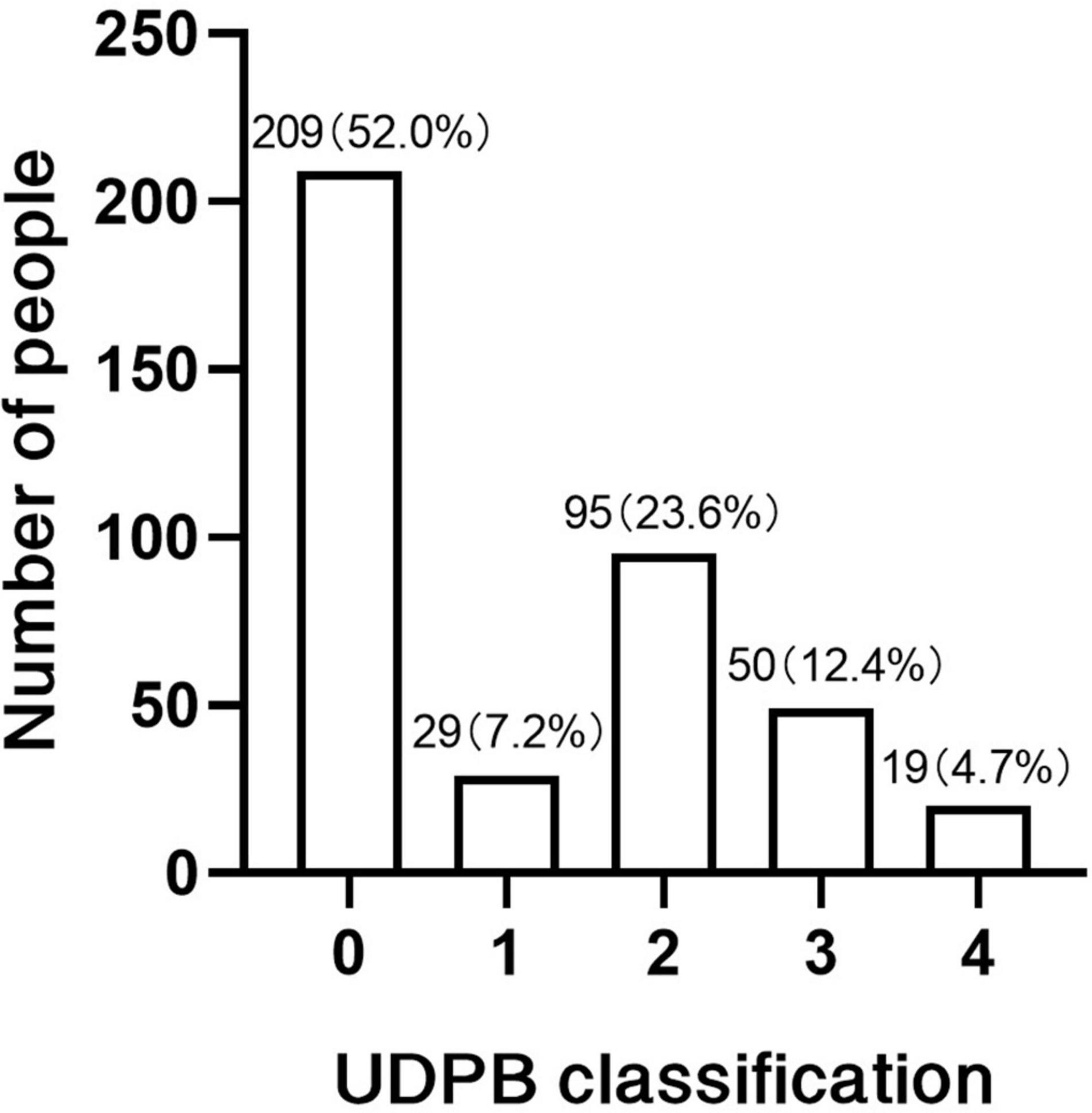
Figure 1. Bleeding classification according to the UDPB.
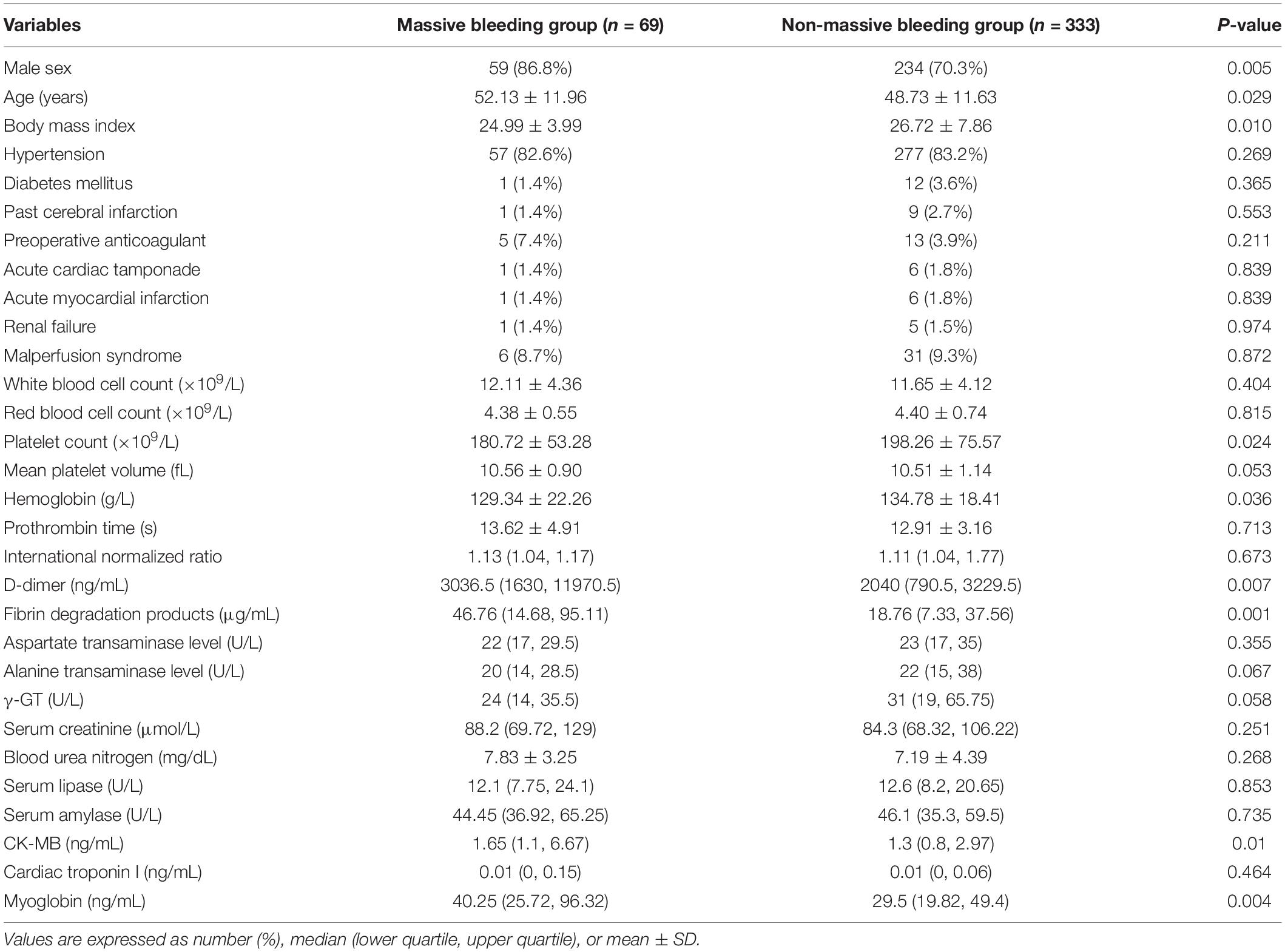
Table 1. Preoperative characteristics of the study population.
All the details of operation data were summarized in Table 2. A total of 298 patients underwent emergent aortic repairs within 24 h of onset (74.1%). In the management of the proximal aorta, 172 patients underwent aortic root replacement (Bentall procedure) (42.8%), 230 patients underwent ascending aorta replacement (58.2%). The management of the aortic arch consists of 2 procedures, 315 patients underwent total arch replacement (78.4%), 60 patients underwent hemiarch replacement (14.9%).
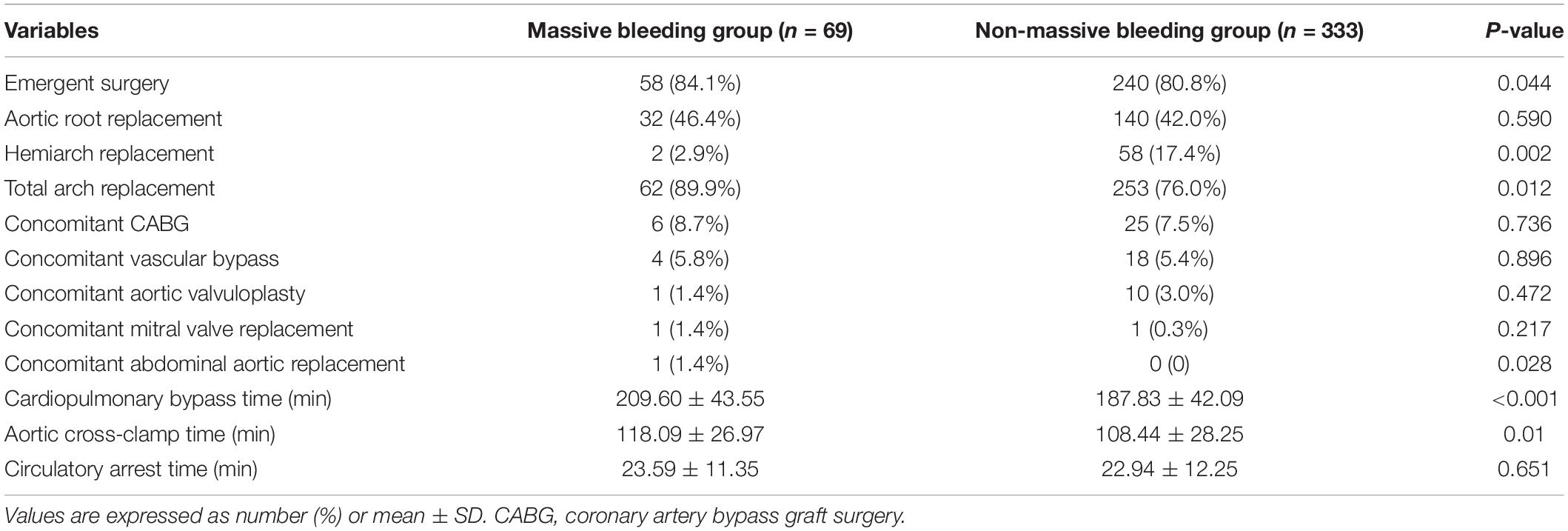
Table 2. Surgical data of study population.
Based on the definition of the UDPB bleeding classification, a univariate analysis of the patient’s perioperative condition revealed that risk factors associated with massive bleeding after the surgery included aged patients (P = 0.029), male patients (P = 0.050), emergent surgery (P = 0.044), preoperative renal dysfunction (P = 0.013), low hemoglobin level (P = 0.036), low platelet count (P = 0.024), elevated D-dimer level (P = 0.045), increased fibrin degradation products (P = 0.002), prolonged cardiopulmonary bypass time (P < 0.001), prolonged aortic cross-clamp time (P = 0.01), and total arch replacement (P = 0.012). In a multivariate regression analysis, this study set massive bleeding as the study endpoint and obtained independent risk factors associated with it including male sex (OR = 6.493, P < 0.001, 95% CI = 2.429–17.360), elder patients (OR = 1.029, P = 0.05, 95% CI = 1.000–1.059), low BMI (OR = 0.879, 95% CI: 0.806–0.957, P = 0.003), emergent surgery (OR = 3.112, 95% CI: 1.235–7.843, P = 0.016), prolonged cardiopulmonary bypass time (OR = 1.012, 95% CI: 1.004–1.021, P = 0.002), lower hemoglobin levels (OR = 0.976, 95% CI: 0.959–0.993, P = 0.002), increased D-dimer levels (OR = 1.000, P = 0.037), increased fibrin degradation products (OR = 1.019, 95% CI: 1.005–1.033, P = 0.008), hemiarch replacement (OR = 5.045, 95% CI: 1.098–23.173, P = 0.037), total arch replacement (OR = 14.405, 95% CI: 2.046–101.404, P = 0.004) (Table 3).
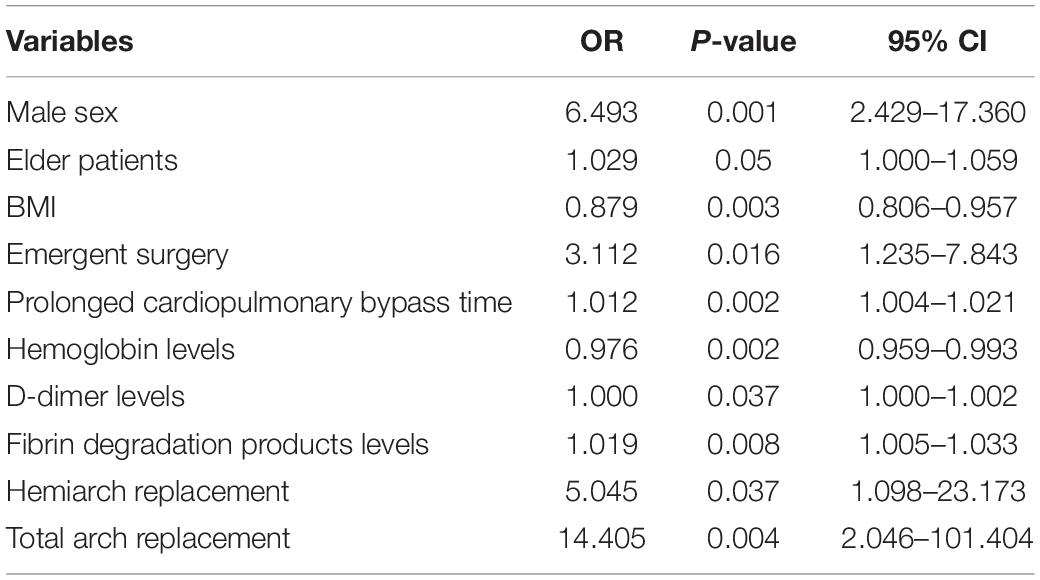
Table 3. Risk factors of postoperative massive bleeding.
In terms of prognosis, 24 patients died in the early stage after surgery, with a mortality rate of 15.9% in the massive bleeding group (11 patients) and 3.9% in the non-massive bleeding group (13 patients, P = 0.001), the in-hospital survivorship curve was shown in Figure 2. The average hospitalization time was 17.79 ± 12.73 and 14.54 ± 8.49 days, the average length of stay in the intensive care unit was 4 (2, 8) and 2 (1, 4) days, and the average duration of tracheal intubation was 41 (17.75, 96) and 16 (12, 36) h, respectively. More details were summarized in Table 4.
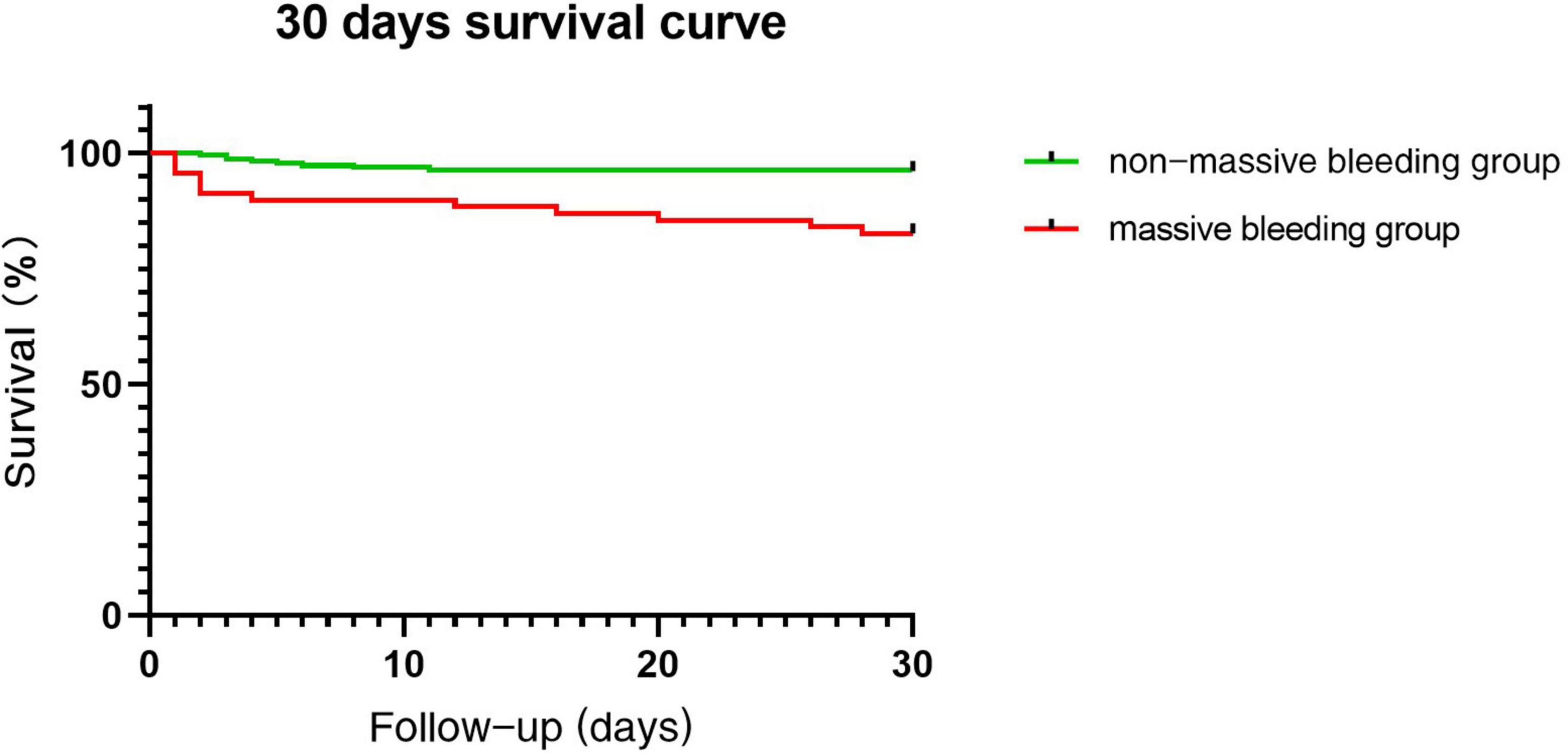
Figure 2. Survival in patients with and without massive bleeding.
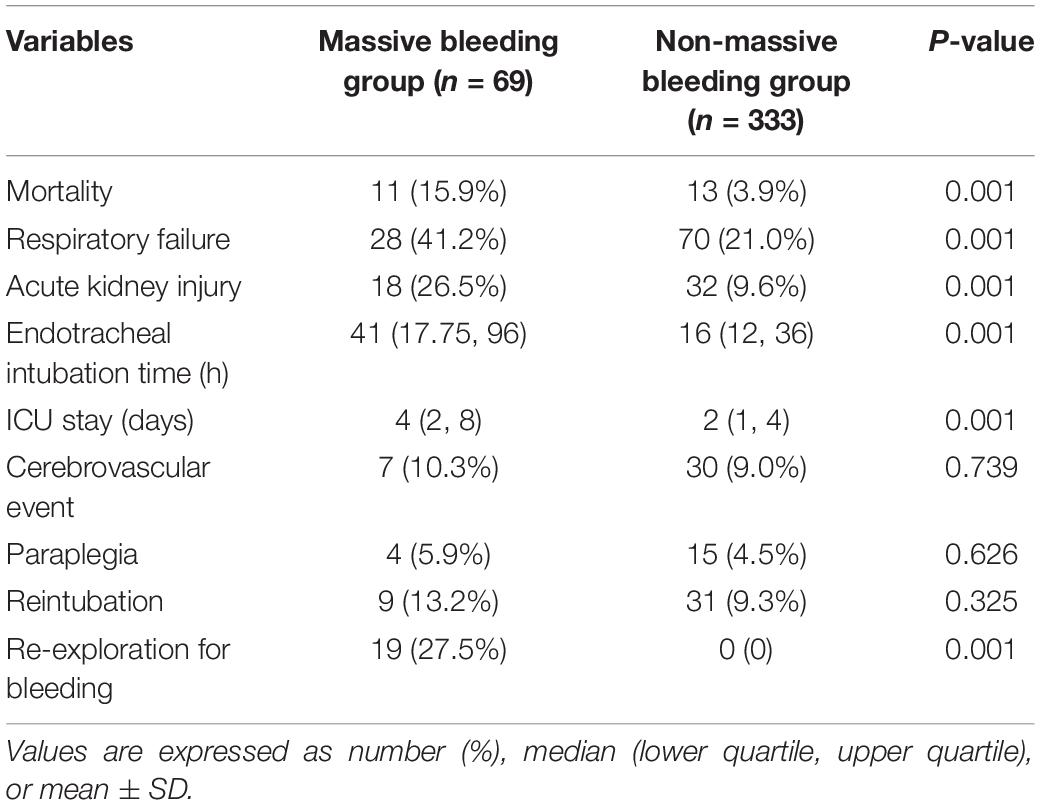
Table 4. Short-term outcomes of study population.
A logistic regression analysis was performed to develop a predicting model in this study, the R2 was 0.31 and the standardized beta coefficients for the included variables were male sex (1.871), age (0.029), emergent surgery (1.135), hemoglobin level (−0.024), CPB time (0.012), BMI (−0.129), fibrin degradation products (0.019), hemiarch replacement (1.618), and total arch replacement (2.668). The resulting regression equation to predict the mean ascending aorta length was:
Logit(P) = −3.226 + sex [m = 1, f = 0] × 1.871 + age (years) × 0.029 + emergent surgery [y = 1, n = 0] × 1.135 – hemoglobin level (g/L) × 0.024 + CPB time (min) × 0.012 – BMI × 0.129 + fibrin degradation products (μg/mL) × 0.019 + hemiarch replacement [y = 1, n = 0] × 1.618 + total arch replacement [y = 1, n = 0] × 2.668 (14). In terms of evaluating the discrimination of the model, the area under the curve (AUC) was 0.817 (95% CI: 0.760–0.873, P < 0.001, Figure 3). In the Hosmer–Lemeshow goodness-of-fit test, the model demonstrated good calibration, the Hosmer–Lemeshow χ2 was 5.281, P = 0.727 > 0.05, and the calibration plot was shown in Figure 4.
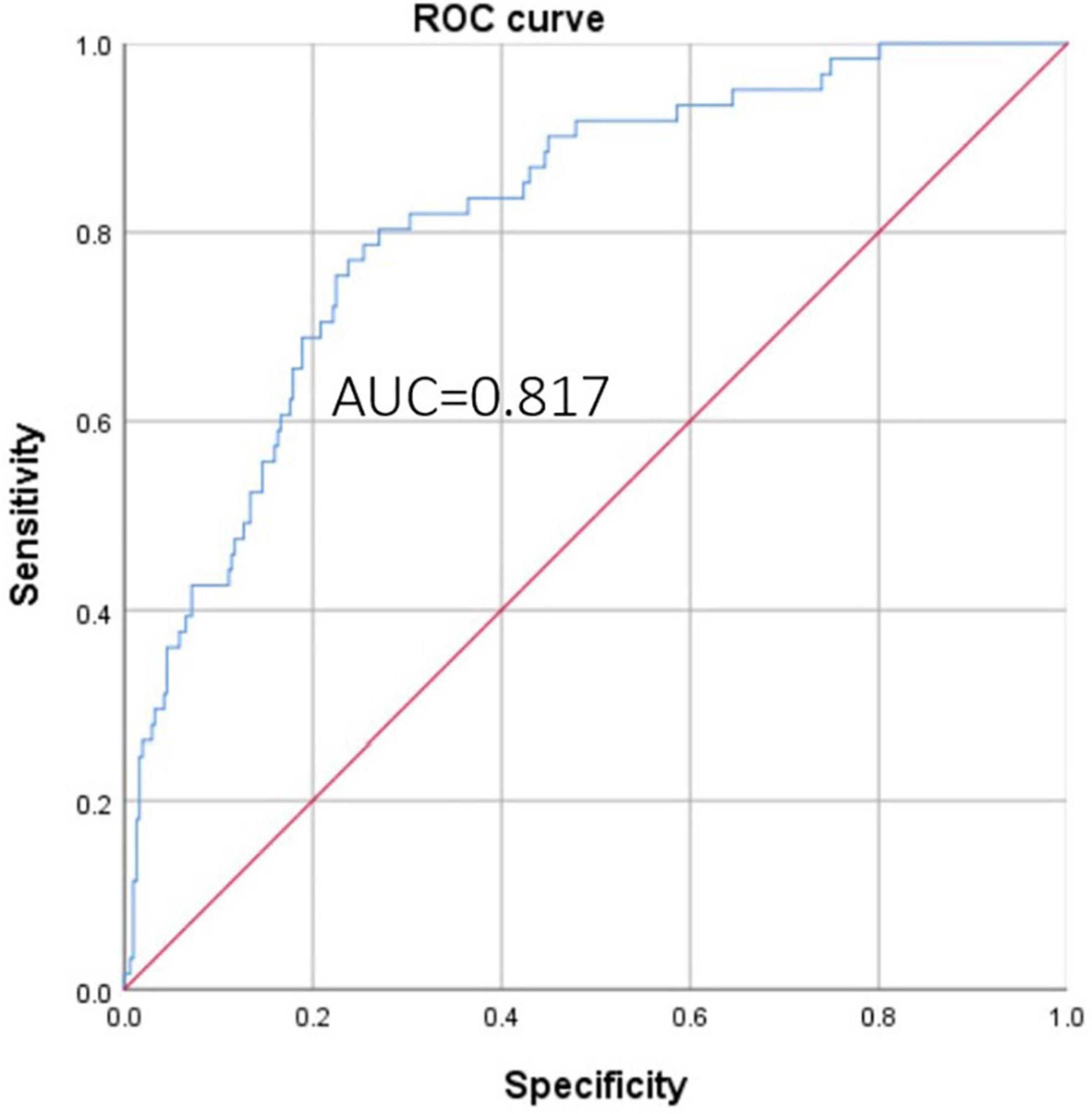
Figure 3. ROC curve of the model for predicting massive bleeding.
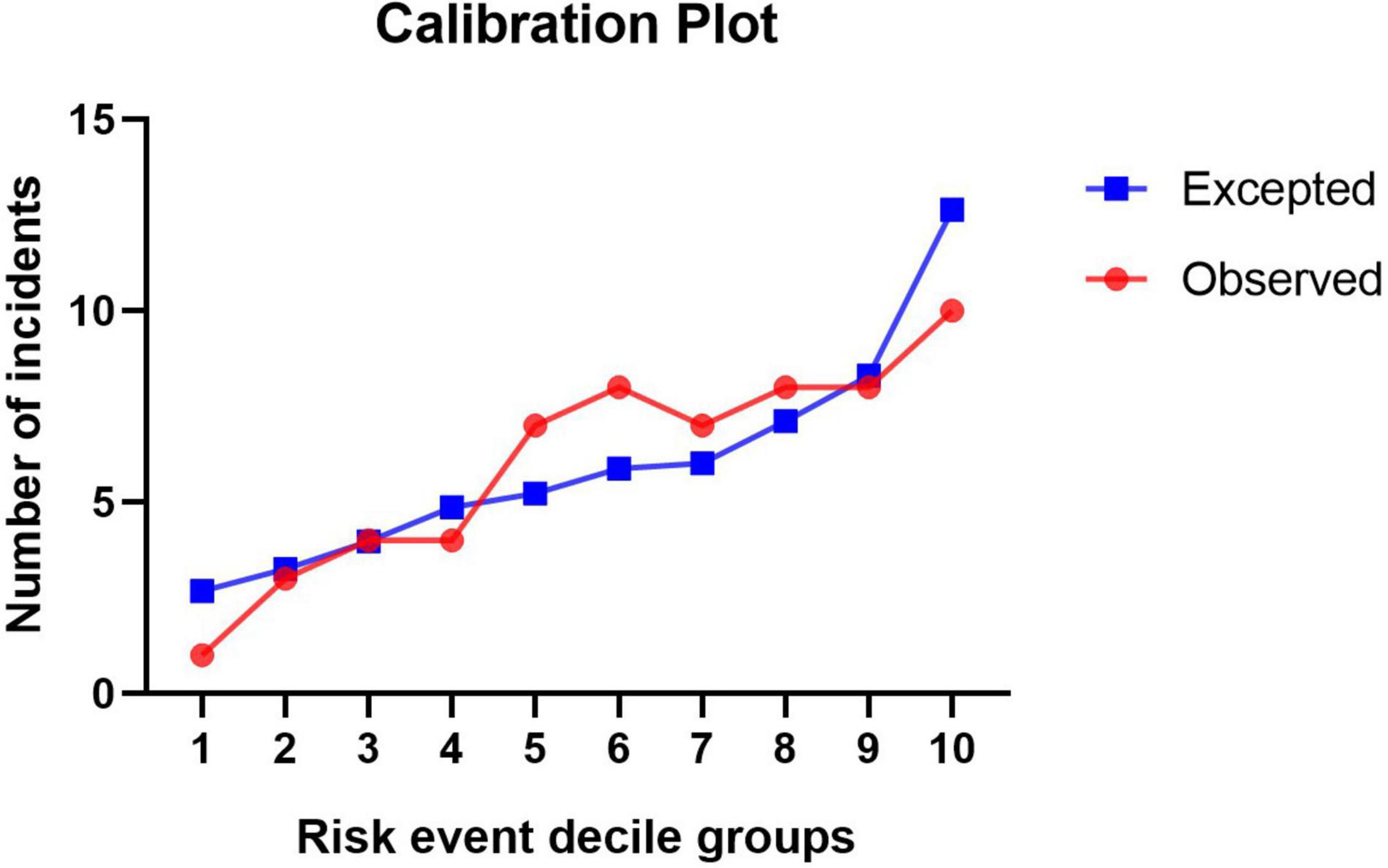
Figure 4. Calibration plot of the model for predicting massive bleeding.
Postoperative bleeding and the need for blood product transfusion are quite common after aortic surgery (3). At the same time, massive bleeding may lead to numerous complications such as re-exploration, which is associated with increased mortality (15). In previous studies, the definition of massive bleeding has varied depending on the countries and centers, and is less often measured by a uniform standard. In this study, the UDPB bleeding classification was used to measure postoperative bleeding in patients with ATAAD, with class 3–4 bleeding requiring aggressive clinical intervention and therefore defined as massive bleeding by this study. The proportion of bleeding at all levels in our center is generally consistent with previous studies.
Gender was considered an independent risk factor for massive postoperative bleeding in patients with aortic type A coarctation, along with low body mass index. In general, low weight patients are associated with female patients, but the present study concluded the opposite, that male patients are more likely to have massive postoperative bleeding after aortic repair surgery, which is consistent with the results of many previous trials (16–18). The possible reason for this is that in our study, most male patients were in middle age, with poorly controlled hypertension, which may lead to difficulty in intraoperative hemostasis, another reason might be the rate of fibrin production as well as the intensity of thrombosis is higher in healthy adult females than in healthy males (19). At the same time, elderly patients have a higher risk of massive postoperative bleeding compared to younger patients, probably because the vascular condition is worse in elderly patients, which makes the operation more difficult. The coagulation mechanism of elderly patients is not as well developed as that of younger patients, which makes them more prone to massive postoperative bleeding, and therefore the prognosis of elderly patients needs to be considered more comprehensively before and during the surgery.
In this study, elevated D-dimer and preoperative low hemoglobin status were both strongly associated with postoperative bleeding, suggesting that preoperative assessment of coagulation mechanisms is particularly important, and that D-dimer, as a degradation product of fibrinolysis of blood clots, is often indicative of fibrin production and lysis, commonly in response to inflammation, trauma, tumor, recent surgery, and acute aortic syndrome or pulmonary embolism (20, 21). Previous studies have shown that elevated D-dimer is significantly and positively associated with the severity of the tear in aortic dissection, and it has therefore been mentioned in several studies that patients with significantly elevated D-dimer tend to undergo more complex procedures, but this is accompanied by difficulties in intraoperative hemostasis and heavy bleeding in the early postoperative period, which in turn affects the early prognosis of the patient (22, 23). Itagaki et al. found that an increase in D-dimer was accompanied by a decrease in platelet count, further demonstrating the value of D-dimer as a predictor of bleeding risk in the early stages of the disease (24). Our study did not find a significant effect of preoperative anticoagulant use on postoperative massive bleeding, probably due to the young age of the patients with type A aortic dissection seen at our center and the very limited number of patients with coronary artery disease on antiplatelet agents. Most of the patients on anticoagulants were misdiagnosed at other hospitals and underwent coronary angiography or were treated as myocardial infarctions; the number of such patients was so small that it did not significantly affect the statistical results.
Although it was shown in this study that emergent surgery raises the risk of massive postoperative bleeding, and similar results were obtained in other studies such as Zindovic et al. Emergent surgical treatment to save the patient’s life is still the first choice compared to the risk of death from a ruptured aortic coarctation aneurysm that the patient is waiting to face (25). With regard to the choice of procedure, a single-center retrospective study by Xue et al. covering 958 patients suggested that differences in arch procedure alone did not result in significant mortality differences and that it was the preoperative status that really affected the prognosis of patients with type A dissection, which is generally consistent with the results of the present study (26). Our study suggests that either hemiarch replacement or total arch replacement increases the likelihood of massive postoperative bleeding compared to ascending aortic surgery alone, but the surgical approach still needs to be tailored to the patient.
The results of this study showed a significant difference in the short-term prognosis of patients undergoing aortic repair with the presence or absence of massive bleeding, with patients who had massive bleeding in the study having a worse prognosis than those in the non-massive bleeding group. Our results showed that there was a statistical difference in mortality between the two groups, and the main causes of death in the massive bleeding group included cerebrovascular accident and postoperative multiorgan failure, of which multiorgan failure was more closely related to massive bleeding, blood volume deficiency, and ischemia-reperfusion injury.
This study found that among patients who presented with massive postoperative bleeding, there was a significant increase in the need for continuous renal replacement therapy due to impaired renal function. Inadequate preoperative as well as intraoperative renal perfusion, activation of the inflammatory response triggered by postoperative bleeding, postoperative low cardiac output and hemodynamic changes are all possible predisposing factors for the occurrence of postoperative acute kidney injury (27, 28).
In terms of the respiratory system, this study suggests that the duration of tracheal intubation was significantly longer in patients who presented with massive postoperative bleeding and required longer periods of ventilator assistance. The possible causes include prolonged CPB time, endotoxemia due to poor visceral perfusion, ischemia-reperfusion injury to the lungs, surgical trauma, or the use of protamine, an inflammatory response that can cause damage to the lungs, and inappropriate postoperative ventilatory parameters and fluid management may exacerbate this damage (29). The amount of blood product infusion associated with massive bleeding can also be significantly elevated, and some studies have shown that blood product infusion significantly increases the incidence of respiratory distress after cardiac surgery. Moreover, the low blood pressure caused by massive bleeding can also make postoperative fluid management very difficult, and excessive fluid rehydration may cause pulmonary edema further aggravating the blow to the lungs (30).
Several previous studies have discussed predicting the risk of bleeding after cardiac surgery, but most of these studies were limited to coronary surgery (14, 31, 32). In this study, we used a logistic regression model to predict the risk of massive bleeding after aortic repair in ATAAD patients, the model was performed well and showed good discrimination (AUC = 0.817) and calibration. Since multiple adverse prognoses are associated with massive bleeding, patients at high risk should be more carefully assessed preoperatively and treated with a reasonable treatment plan.
The limitation of this study was the retrospective nature of the analysis. Despite the use of multivariable analyses to limit the effects of confounding variables, the effects of baseline differences as confounders could not be ruled out. Postoperative bleeding may also be related to many surgical factors such as different surgical strategies, insufficient anastomosis, improper surgical manipulation, and suture lines. Further studies investigating mechanisms underlying these risk factors for massive bleeding are required. Risk factors for each set of criteria were not completely the same, and more clinical trials are needed to identify which criteria are more favorable in clinical use. At the same time, although the predicting model showed good discrimination and calibration in our study, more data from multiple centers may validate the model in further studies.
The present study reported several risk factors for massive bleeding in patients with ATAAD who underwent emergent aortic repair, including gender, emergent surgery, increased D-dimer level, increased CPB time, and use of a complex surgical strategy. Massive bleeding may lead to higher mortality, longer stay in the intensive unit, and longer hospitalization. Our predicting model showed good discrimination and calibration, for patients who were evaluated as having a high risk of massive bleeding, surgeons should choose a suitable surgical strategy to prevent bleeding complications.
The original contributions presented in this study are included in the article/supplementary material, further inquiries can be directed to the corresponding author.
The Institutional Review Board of Beijing Anzhen Hospital of Capital Medical University approved this retrospective study and waived the need for informed patient consent. The institutional approval number is 202075X.
C-HZ was responsible for the conceptualization, data collection, statistical analysis, and writing the draft. Y-LZ and Y-PG were responsible for the statistical analysis. J-MZ was responsible for the conceptualization, methodology, and investigation. H-OH, Z-YQ, C-NL, and Y-PG were responsible for the investigation. All authors contributed to the article and approved the submitted version.
This work was supported by the Beijing Municipal Science and Technology Commission (Nos. Z191100006619093 and Z191100006619094) and the National Science Foundation of China (No. 81970393).
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Hirst AE Jr, Johns VJ Jr, Kime SW Jr. Dissecting aneurysm of the aorta: a review of 505 cases. Medicine. (1958) 37:217–79. doi: 10.1097/00005792-195809000-00003
2. Pacini D, Di Marco L, Fortuna D, Belotti LM, Gabbieri D, Zussa C, et al. Acute aortic dissection: epidemiology and outcomes. Int J Cardiol. (2013) 167:2806–12. doi: 10.1016/j.ijcard.2012.07.008
3. Trimarchi S, Nienaber CA, Rampoldi V, Myrmel T, Suzuki T, Mehta RH, et al. Contemporary results of surgery in acute type A aortic dissection: the international registry of acute aortic dissection experience. J Thorac Cardiovasc Surg. (2005) 129:112–22. doi: 10.1016/j.jtcvs.2004.09.005
4. Ranucci M. Hemostatic and thrombotic issues in cardiac surgery. Semin Thromb Hemost. (2015) 41:84–90. doi: 10.1055/s-0034-1398383
5. Christensen MC, Krapf S, Kempel A, von Heymann C. Costs of excessive postoperative hemorrhage in cardiac surgery. J Thorac Cardiovasc Surg. (2009) 138:687–93. doi: 10.1016/j.jtcvs.2009.02.021
6. Atik FA, Miana LA, Jatene FB, Auler Júnior JO, Oliveira SA. Myocardial revascularization surgery without extracorporeal circulation minimizes postoperative bleeding and the need for transfusion. Arq Bras Cardiol. (2004) 83:338–42.
7. Gwozdziewicz M, Olsak P, Lonsky V. Re-operations for bleeding in cardiac surgery: treatment strategy. Biomed Pap Med Fac Univ Palacky Olomouc Czech Repub. (2008) 152:159–62. doi: 10.5507/bp.2008.026
8. Lopes CT, Brunori EF, Cavalcante AM, Moorhead SA, Swanson E, Lopes JL, et al. Factors associated with excessive bleeding after cardiac surgery: a prospective cohort study. Heart Lung. (2016) 45:64–9.e2. doi: 10.1016/j.hrtlng.2015.09.003
9. Dyke C, Aronson S, Dietrich W, Hofmann A, Karkouti K, Levi M, et al. Universal definition of perioperative bleeding in adult cardiac surgery. J Thorac Cardiovasc Surg. (2014) 147:1458–63.e1.
10. Fergusson DA, Hébert PC, Mazer CD, Fremes S, MacAdams C, Murkin JM, et al. A comparison of aprotinin and lysine analogues in high-risk cardiac surgery. N Engl J Med. (2008) 358:2319–31. doi: 10.1056/NEJMoa0802395
11. Ma WG, Zheng J, Liu YM, Zhu JM, Sun LZ. Dr. Sun’s procedure for type A aortic dissection: total arch replacement using tetrafurcate graft with stented elephant trunk implantation. Aorta. (2013) 1:59–64. doi: 10.12945/j.aorta.2013.13.015
12. Sun L, Qi R, Chang Q, Zhu J, Liu Y, Yu C, et al. Surgery for acute type A dissection with the tear in the descending aorta using a stented elephant trunk procedure. Ann Thorac Surg. (2009) 87:1177–80. doi: 10.1016/j.athoracsur.2009.01.042
13. Liu ZG, Sun LZ, Chang Q, Zhu JM, Dong C, Yu CT, et al. Should the “elephant trunk” be skeletonized? Total arch replacement combined with stented elephant trunk implantation for Stanford type A aortic dissection. J Thorac Cardiovasc Surg. (2006) 131:107–13. doi: 10.1016/j.jtcvs.2005.09.015
14. Harris JM, Sheehan K, Rogers CA, Murphy T, Caputo M, Mumford AD. Prediction of bleeding in pediatric cardiac surgery using clinical characteristics and prospective coagulation test results. Semin Thorac Cardiovasc Surg. (2021) 34:277–88. doi: 10.1053/j.semtcvs.2021.01.006
15. Fröjd V, Jeppsson A. Reexploration for bleeding and its association with mortality after cardiac surgery. Ann Thorac Surg. (2016) 102:109–17. doi: 10.1016/j.athoracsur.2016.01.006
16. Christensen MC, Dziewior F, Kempel A, von Heymann C. Increased chest tube drainage is independently associated with adverse outcome after cardiac surgery. J Cardiothorac Vasc Anesth. (2012) 26:46–51. doi: 10.1053/j.jvca.2011.09.021
17. Dixon B, Reid D, Collins M, Newcomb AE, Rosalion A, Yap CH, et al. The operating surgeon is an independent predictor of chest tube drainage following cardiac surgery. J Cardiothorac Vasc Anesth. (2014) 28:242–6. doi: 10.1053/j.jvca.2013.09.010
18. Miceli A, Duggan SM, Aresu G, de Siena PM, Romeo F, Glauber M, et al. Combined clopidogrel and aspirin treatment up to surgery increases the risk of postoperative myocardial infarction, blood loss and reoperation for bleeding in patients undergoing coronary artery bypass grafting. Eur J Cardio Thorac Surg. (2013) 43:722–8. doi: 10.1093/ejcts/ezs369
19. Roeloffzen WW, Kluin-Nelemans HC, Mulder AB, Veeger NJ, Bosman L, de Wolf JT. In normal controls, both age and gender affect coagulability as measured by thrombelastography. Anesth Analg. (2010) 110:987–94. doi: 10.1213/ANE.0b013e3181d31e91
20. Hiratzka LF, Bakris GL, Beckman JA, Bersin RM, Carr VF, Casey DE Jr, et al. 2010 ACCF/AHA/AATS/ACR/ASA/SCA/SCAI/SIR/STS/SVM guidelines for the diagnosis and management of patients with thoracic aortic disease: executive summary. A report of the American college of cardiology foundation/American heart association task force on practice guidelines, American association for thoracic surgery, American college of radiology, American stroke association, Society of cardiovascular anesthesiologists, Society for cardiovascular angiography and interventions, Society of interventional radiology, Society of thoracic surgeons, and Society for vascular medicine. Catheter Cardiovasc Interv. (2010) 76:E43–86.
21. Giannitsis E, Mair J, Christersson C, Siegbahn A, Huber K, Jaffe AS, et al. How to use D-dimer in acute cardiovascular care. Eur Heart J Acute Cardiovasc Care. (2017) 6:69–80.
22. Hazui H, Nishimoto M, Hoshiga M, Negoro N, Muraoka H, Murai M, et al. Young adult patients with short dissection length and thrombosed false lumen without ulcer-like projections are liable to have false-negative results of D-dimer testing for acute aortic dissection based on a study of 113 cases. Circ J. (2006) 70:1598–601. doi: 10.1253/circj.70.1598
23. Ohlmann P, Faure A, Morel O, Petit H, Kabbaj H, Meyer N, et al. Diagnostic and prognostic value of circulating D-Dimers in patients with acute aortic dissection. Crit Care Med. (2006) 34:1358–64.
24. Itagaki R, Kimura N, Mieno M, Hori D, Itoh S, Akiyoshi K, et al. Characteristics and treatment outcomes of acute type A aortic dissection with elevated D-dimer concentration. J Am Heart Assoc. (2018) 7:e009144. doi: 10.1161/JAHA.118.009144
25. Zindovic I, Sjögren J, Bjursten H, Björklund E, Herou E, Ingemansson R, et al. Predictors and impact of massive bleeding in acute type A aortic dissection. Interact Cardiovasc Thorac Surg. (2017) 24:498–505. doi: 10.1093/icvts/ivw425
26. Xue Y, Pan J, Cao H, Fan F, Luo X, Ge M, et al. Different aortic arch surgery methods for type A aortic dissection: clinical outcomes and follow-up results. Interact Cardiovasc Thorac Surg. (2020) 31:254–62. doi: 10.1093/icvts/ivaa095
28. Hudson C, Hudson J, Swaminathan M, Shaw A, Stafford-Smith M, Patel UD. Emerging concepts in acute kidney injury following cardiac surgery. Semin Cardiothorac Vasc Anesth. (2008) 12:320–30. doi: 10.1177/1089253208328582
29. Laffey JG, Boylan JF, Cheng DC. The systemic inflammatory response to cardiac surgery: implications for the anesthesiologist. Anesthesiology. (2002) 97:215–52. doi: 10.1097/00000542-200207000-00030
30. Young RW. Prevention of lung injury in cardiac surgery: a review. J Extra Corpor Technol. (2014) 46:130–41.
31. Knapik P, Cieśla D, Saucha W, Knapik M, Zembala MO, Przybyłowski P, et al. Outcome prediction after coronary surgery and redo surgery for bleeding (from the KROK registry). J Cardiothorac Vasc Anesth. (2019) 33:2930–7. doi: 10.1053/j.jvca.2019.04.028
Keywords: aortic (rupture) dissection, bleeding, perioperative management, surgery strategy, clinical research
Citation: Zhang C-H, Ge Y-P, Zhong Y-L, Hu H-O, Qiao Z-Y, Li C-N and Zhu J-M (2022) Massive Bleeding After Surgical Repair in Acute Type A Aortic Dissection Patients: Risk Factors, Outcomes, and the Predicting Model. Front. Cardiovasc. Med. 9:892696. doi: 10.3389/fcvm.2022.892696
Received: 09 March 2022; Accepted: 09 June 2022;
Published: 08 July 2022.
Edited by:
Robert Jeenchen Chen, Stanford University, United StatesReviewed by:
Martin Grapow, Herzzentrum Hirslanden, SwitzerlandCopyright © 2022 Zhang, Ge, Zhong, Hu, Qiao, Li and Zhu. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Jun-Ming Zhu, YW56aGVuemptQGNjbXUuZWR1LmNu
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.