 Xinqiang Han
Xinqiang Han Yongzhen Zhang†
Yongzhen Zhang† Mengpeng Zhao
Mengpeng Zhao
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
CASE REPORT article
Front. Cardiovasc. Med. , 29 September 2022
Sec. Atherosclerosis and Vascular Medicine
Volume 9 - 2022 | https://doi.org/10.3389/fcvm.2022.892025
This article is part of the Research Topic Case Reports in Atherosclerosis and Vascular Medicine: 2022 View all 10 articles
Background: Cement leakage into the inferior vena cava (IVC) is one of the most common complications associated with cement vertebroplasty, and can lead to potentially life-threatening complications such as pulmonary cement embolism (PCE). Implantation of an IVC filter is effective in the prevention of fatal pulmonary embolism. Here, we present an extremely rarely case of cement entrapped in an IVC filter after pedicle screw augmentation, and discuss all similar cases reported in the literature.
Case presentation: A 70-year-old female presented with significant back and lower extremities pain and was unable to walk. MRI of the lumbar spine revealed an osteoporotic compression fracture of the L1–L3. She underwent cement-augmented pedicle screws implanted at the L1 and L3 vertebral bodies. A retrievable IVC filter was implanted due to the presence of calf vein thrombosis before cement vertebroplasty. Cement leaked into the IVC and was trapped by the filter, rendering the filter unretrievable using a conventional method. The asymptomatic patient received rivaroxaban 20 mg daily for anticoagulant postoperatively and lifelong anticoagulation was administered to prevent secondary IVC and cemented filter thrombosis.
Methods: A literature search was conducted utilizing the PUBMED/MEDLINE using the following terms: “vertebroplasty,” “complication,” “bone cement,” and “inferior vena cava (IVC),” or “inferior vena cava (IVC) filter.” All relevant articles published in English or in other languages with English abstracts since 1962 were included.
Results: A total of 36 articles were retrieved according to the search strategy. Only 6 out of these 36 studies contained information regarding the inferior vena cava filter and cement. Of the patients, 85.7% (36/42) reported in the literature whose gender was known were female and 14.3% were male. 28.5% (45/158) patients with pulmonary arterial and cardiovascular complications.
Conclusion: Cement embolization occurring in the IVC filter is rare. Accurate knowledge about the lumbar vertebral venous anatomy and skillful operation during vertebral cementoplasty should be required in clinical practice.
Bone cement has been widely injected into diseased or fractured vertebral bodies to provide an expected increase in the stabilization and strength of the vertebral and pedicle screws, and is especially suitable for the management of osteoporotic compression fractures (1). However, spillage of cement frequently occurs in the process of vertebroplasty and may result in serious sequelae. Cement leakage into the venous plexus is the most frequent complication, and can lead to severe and potentially life-threatening complications such as pulmonary cement embolism (PCE) or myocardial perforation (2). Here, we present a case that underwent cement augmentation for improving fixation of pedicle screws, in which the cement leaked into the peripheral venous system causing large masses extending to the IVC that were eventually captured in the previously implanted IVC filter. This case study is significant because it illustrates the rare occurrence of cemented filter, making clinicians aware of the potential possibility of cement leakage into the IVC in patients with cement-based augmentation of vertebroplasty. We discuss this case and all similar cases reported in the literature.
There was a 70-year-old female patient who had significant back and lower extremities pain and was unable to walk. An outpatient MRI of the lumbar spine showed an osteoporotic compression fracture of the L1–L3. She had cement- (polymethylmethacrylate) augmented pedicle screws implanted at the L1 and L3 vertebral bodies after hospital admission. A total of 5.8 ml of “tooth-paste-like” bone cement was injected to provide stabilization and pain relief within 5 min after mixing, and the procedure was performed under the guidance of C-arm X-ray fluoroscopy. Before cement vertebroplasty, a retrievable IVC filter (Aegisy, LifeTech, Shenzhen, China) was implanted into the IVC to prevent pulmonary embolism (PE) since the routine preoperative ultrasound revealed an isolated distal deep vein thrombosis in the vein of her left calf. The patient received rivaroxaban 20 mg daily for anticoagulant postoperatively.
Thereafter, X-ray examination showed paravertebral venous cement leak and cement entry into the IVC, resulting in the deposition of a cement cast in the IVC filter, and CT images demonstrating cement leaking out of the vertebral body (Figure 1). An inferior vena cavography prior to retrieval of the filter showed that cement had migrated into the IVC and attached to the caval wall at the level of the IVC filter tip and was trapped within the filter (Figure 2), resulting in the IVC filter failing to be retrieved in the conventional way.

Figure 1. CT scans revealed strip-like high density cement extravasation (arrows) in vertebra bone.
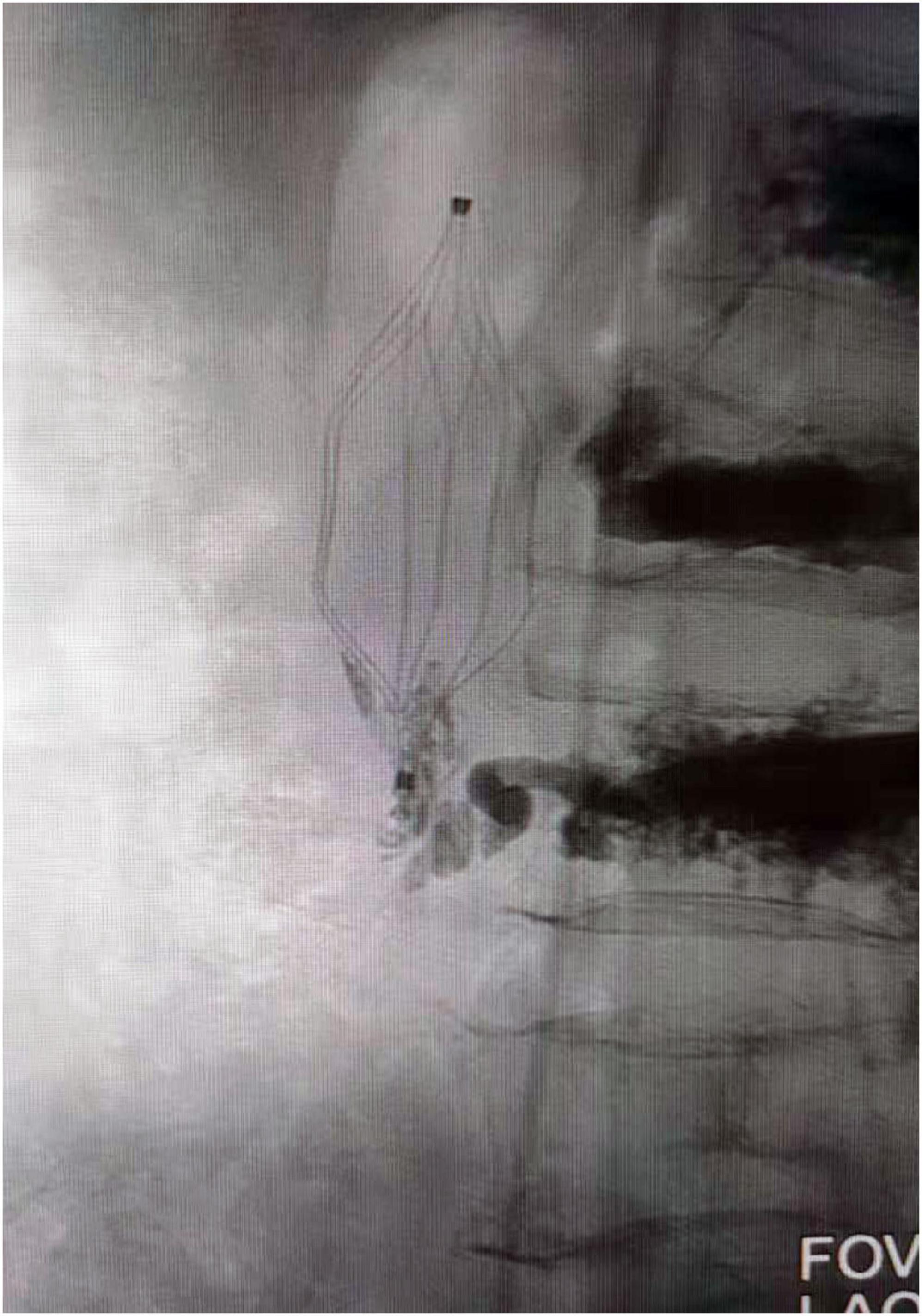
Figure 2. Venography showed cement attached to the IVC filter hook and trapped in the filter. IVC, inferior vena cava.
Bone cement injection was performed by spinal surgeons with more than 10 years of clinical experience, and cavography and DSA image judgment were performed by interventional radiologists with more than 10 years of clinical experience. The asymptomatic patient continued with rivaroxaban 20 mg daily and was discharged from the hospital, and close follow-up and lifelong anticoagulation was administered to prevent secondary IVC and cemented filter thrombosis.
A literature search was conducted utilizing the PUBMED/MEDLINE using the following terms: “vertebroplasty,” “complication,” “bone cement,” and “inferior vena cava (IVC),” or “inferior vena cava (IVC) filter.” All relevant articles published in English or in other languages with English abstracts since 1962 were included.
The literature search yielded 36 articles whose clinical reports contained information regarding the coexistence of cement and inferior vena cava or inferior vena cava filter. Of these patients, 85.7% (36/42) of individuals whose gender was known were female (n = 36) and 14.3% (6/42) were male (n = 6). Cement leakage into the IVC that primarily resulted in pulmonary arterial and cardiovascular complications despite the majority of the patients being asymptomatic accounted for 45 of 158 cases. Only 6 out of these 36 studies contained information regarding the inferior vena cava filter and cement.
Our personal experience includes one unpublished female patient seen and followed-up at our institutions. In addition, another earlier and similar case to this has been accepted for publication in a future issue of CardioVascular and Interventional Radiology, but has not been fully edited. The clinical features of those 36 previously reported are presented in Tables 1, 2.
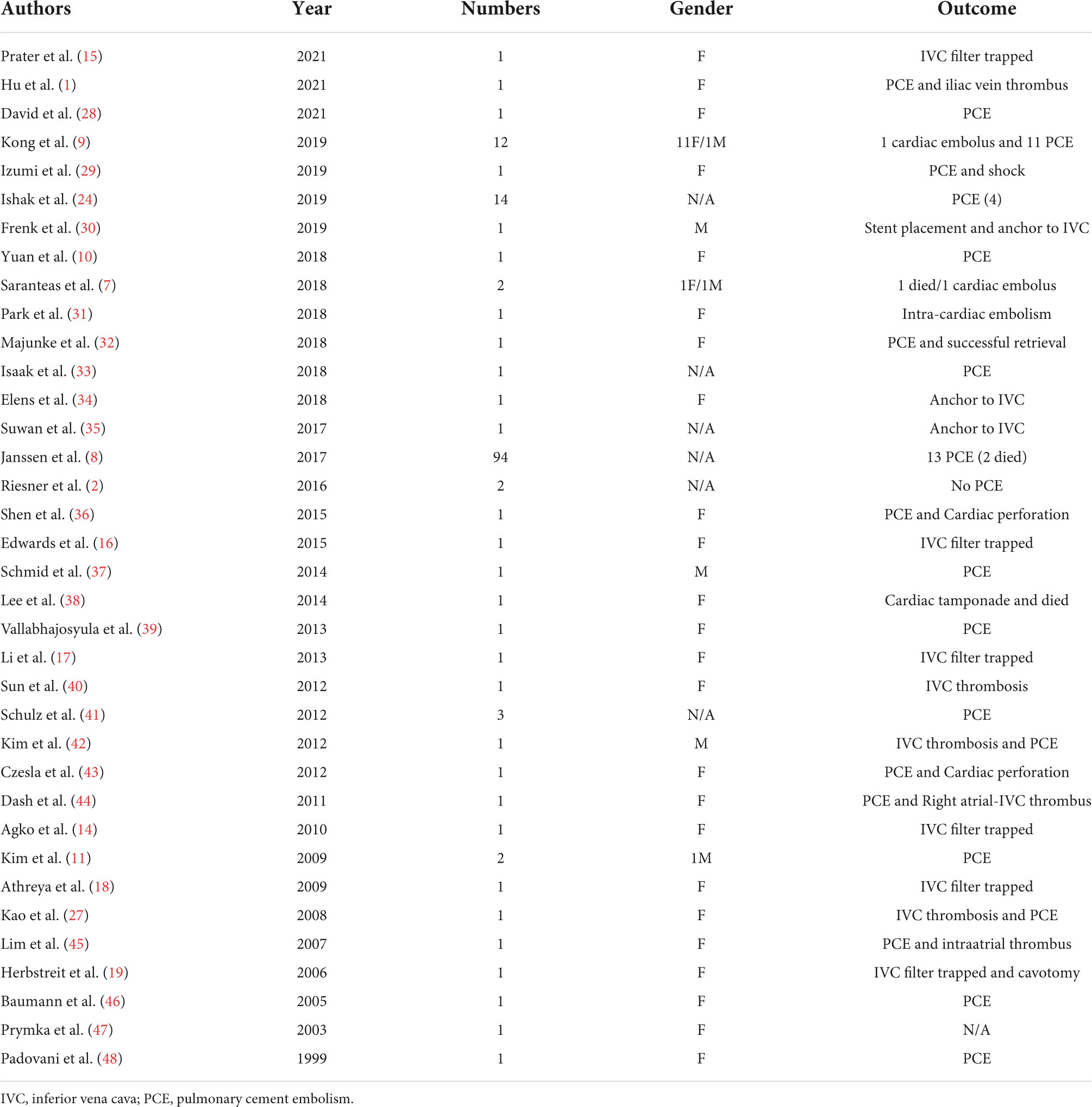
Table 1. Cases of cement leakage extended into the inferior vena cava reported in literature.
Cement augmentation with polymethylmethacrylate is a reliable method for increasing the compressive strength of vertebral bodies, and it is an accepted treatment for osteoporotic compression fracture and reinforcement of vertebral pedicle screws fixation. Perivertebral cement leakage is a frequently reported complication following pedicle screw augmentation and it could potentially be a life-threatening condition; the leaked cement may migrate into IVC and pulmonary arterial circulation with varying incidence rates of 0.9–26% (3–5). However, it is often the case that there were no routine chest CT examinations before or after vertebroplasty. The true incidence of PCE is unknown and may even be underestimated. In addition, the mortality data related to cement leakage was not systematically documented in the literature (6, 7). Although a number of patients have bone cement leakage into the azygos vein or IVC, most cases remain asymptomatic (8). Despite this, some catastrophic outcomes, such as fatal PCE, cardiovascular collapse, and myocardial perforation, have still been documented in the literature (6, 9, 10). Kim found that cement leakage into the IVC showed a statistically significant correlation with PCE (p = 0.03) (11).
It is well known that implantation of IVC filter is effective in the prevention or reduction of the risk of fatal PE in patients with high risk of lower extremity deep vein thrombosis (12). In rare cases, some IVC filters have also been used as a prevention strategy against cement emboli in IVC, which may migrate into the pulmonary circulation (13, 14). However, it appears to be quite rare for leaked cement to become entrapped in an IVC filter. So far as we know, only six cases of cemented filters have previously been reported in the literature (Table 2) (14–19). In our case, cement leaked into the IVC and was trapped by the filter, preventing cement cast migration to the pulmonary arterial circulation. However, it is extremely difficult to retrieve the cemented filter into the outer sheath by utilizing conventional endovascular procedures. Management guidelines vary because of the rare nature of this event. In our case, careful observation and long-term anticoagulation were recommended. Nevertheless, with secondary events, IVC foreign bodies serve as a nidus for thromboembolism and should be taken into consideration.
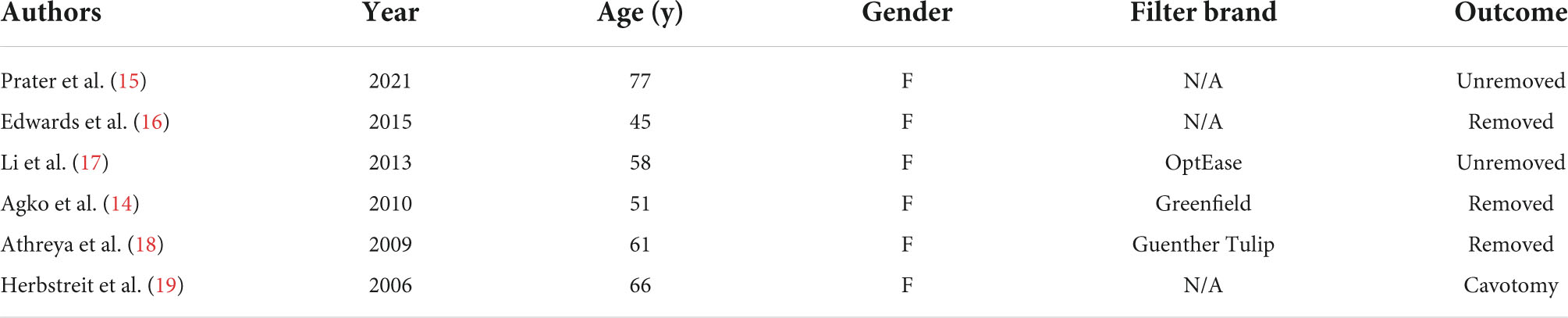
Table 2. Cases of cement trapped by inferior vena cava filter reported in literature.
Therefore, do we need to implant an IVC filter to prevent PCE before vertebral cementoplasty? The only randomized trial regarding pulmonary complications during the cementoplasty procedure is the VERTOS II trial, and 26% (14/54) of the patients with PCE were confirmed by chest CT scans after the vertebral cementoplasty despite none of the patients having related symptoms due to the small size of the cement embolus and its random distribution in the pulmonary vascular endings (20). Among the 158 patients with cement leakage into the IVC after vertebral cementoplasty of all relevant retrieved articles by 2021 in our study, 45 (28.5%) had cardiopulmonary complications despite the majority presenting as mild cases, but severe complications such as cardiac perforation and circulatory failure did occur (Table 1). However, some cardiopulmonary complications were not well documented, and the incidence appeared to be underestimated. Apparently, the risk–benefit ratio for IVC filter implantation is far from certain. Therefore, decisions need to be made on a case-by-case basis.
The reasons why cement embolization occurs in the IVC during cementoplasty procedure have been much discussed in the literature. It is known to all that lumbar vertebral veins enter the IVC at L1-L5 vertebral levels, and numerous connections exist with basivertebral vein and segmental vein (Figure 3) (5, 21). Iwanaga found that latex or air can flow into the IVC at the internal/external vertebral plexus through anatomical location (5). This is the anatomic risk factor for the occurrence of cement venous leakage. However, it should be noted that there may be other reasons, such as incompletely polymerizing cement, the proximity of the needle to the vertebral venous plexus, or the higher volume and faster pushing of the cement (22). Additionally, intraoperative X-ray fluoroscopy may also be helpful to reduce cement leakage (23). But Ishak, who found that 55 of 86 patients had venous cement leakage despite 52 of them having no symptoms, suggested that using CT navigation for screw placement did not reduce the cement leakage risk (24). This may be in part related to a non-radiologist operator with C-arm fluoroscopy (11). Phillips found that injection of contrast medium into the vertebral body could also predict and reduce the occurrence of bone cement leakage (25). Post-procedure chest CT scans may be useful in guiding early diagnosis and treatment. In all literature reports, the proportion of females is significantly higher than that of males. It is not clear why cement leakage into the IVC is more likely to occur in females, although Zhan found no significant association between gender and cement leakage after vertebroplasty or kyphoplasty in a recent systematic review (26).
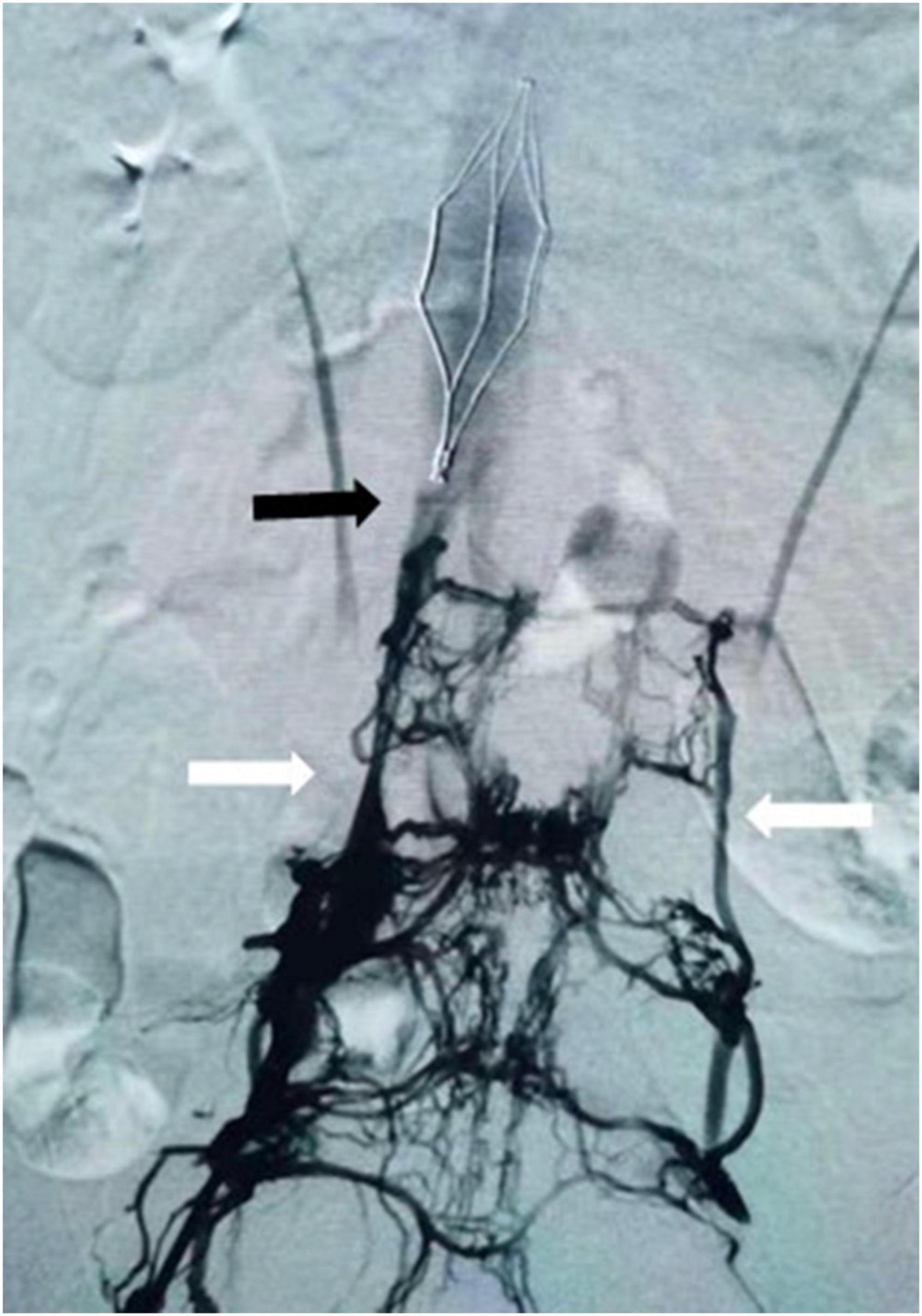
Figure 3. Venography showed collateral drainage veins between inferior vena cava (black arrow) and paravertebral venous (white arrow).
These interesting cases illustrate that the IVC filter could capture cement that leaks into the IVC and prevent fatal pulmonary arterial and cardiovascular complications. The present study, as with any other (27), contributed to making clinicians aware of the potential occurrence of cement leakage into the IVC during vertebroplasty procedures. In other words, surgeons should be aware of the possibility of cement leakage when patients develop clinical symptoms of PE, such as decreased blood pressure, tachycardia, and dyspnea.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Written informed consent was obtained from the individual(s) for the publication of this case report and the publication of any potentially identifiable images or data included in this article.
XH, YZ, and MZ: study concept, acquisition of data and figures, and writing of the manuscript. MZ and ZW: critical revision of manuscript for intellectual content. All authors cared for the patient and contributed to writing of the report.
This work was supported by the Medical and Health Science and Technology Development Plan of Shandong Province, China (Grant No. 2017WS688).
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Hu Y, Wang Y, Yu Z, Li X. Cement-associated thrombotic embolism in the inferior vena cava and bilateral iliac veins after percutaneous vertebroplasty: a case report. J Int Med Res. (2021) 49:3000605211046115. doi: 10.1177/03000605211046115
2. Riesner HJ, Kiupel K, Lang P, Stuby F, Friemert B, Palm HG. Clinical relevance of cement leakage after radiofrequency kyphoplasty vs. balloon kyphoplasty: a prospective randomised study. Z Orthop Unfall. (2016) 154:370–6. doi: 10.1055/s-0042-104069
3. Tang B, Cui L, Chen X, Liu Y. Risk factors for cement leakage in percutaneous vertebroplasty for osteoporotic vertebral compression fractures: an analysis of 1456 vertebrae augmented by low-viscosity bone cement. Spine. (2021) 46:216–22. doi: 10.1097/brs.0000000000003773
4. Drigalla D, Stone CK, Juergens AL. Delayed symptomatic pulmonary embolism secondary to bone cement after percutaneous vertebroplasty. J Emerg Med. (2021) 60:e45–7. doi: 10.1016/j.jemermed.2020.10.045
5. Iwanaga J, Rustagi T, Ishak B, Johal J, David G, Reina MA, et al. Venous drainage of lumbar vertebral bodies: anatomic study with application to kyphoplasty, vertebroplasty, and pedicle screw complications. World Neurosurg. (2020) 137:e286–90. doi: 10.1016/j.wneu.2020.01.174
6. Kang HR, Kim TH, Chung CK, Lee CH. The impact of incidental pulmonary cement embolism on mortality risk. J Thromb Thrombolysis. (2020) 49:468–74. doi: 10.1007/s11239-019-02027-0
7. Saranteas T, Giannoulis D, Anagnostopoulos D, Igoumenou V, Mavrogenis A. Using intraoperative TTE evaluates cardiac function during bone cement placement in orthopedic trauma patients. J Cardiothorac Vasc Anesth. (2018) 32:e67–8. doi: 10.1053/j.jvca.2017.11.034
8. Janssen I, Ryang YM, Gempt J, Bette S, Gerhardt J, Kirschke JS, et al. Risk of cement leakage and pulmonary embolism by bone cement-augmented pedicle screw fixation of the thoracolumbar spine. Spine J. (2017) 17:837–44. doi: 10.1016/j.spinee.2017.01.009
9. Kong M, Xu X, Shen J, Liu Q, Wang G. Clinical characteristics and management of cardiac and/or pulmonary cement embolus after percutaneous vertebroplasty: a single center experience. Ann Transl Med. (2019) 7:372. doi: 10.21037/atm.2019.06.81
10. Yuan Z, Zhou Y, Zhou X, Liao X. Severe pulmonary embolism was secondary to cement inferior vena cava embolism after percutaneous vertebroplasty. Ann Vasc Surg. (2018) 48:.255.e1–255.e3. doi: 10.1016/j.avsg.2018.01.003
11. Kim YJ, Lee JW, Park KW, Yeom JS, Jeong HS, Park JM, et al. Pulmonary cement embolism after percutaneous vertebroplasty in osteoporotic vertebral compression fractures: incidence, characteristics, and risk factors. Radiology. (2009) 251:250–9. doi: 10.1148/radiol.2511080854
12. Young T, Sriram KB. Vena caval filters for the prevention of pulmonary embolism. Cochrane Database Syst Rev. (2020) 10:Cd006212. doi: 10.1002/14651858.CD006212.pub5
13. Guo W, Zheng Q, Li B, Shi X, Xiang D, Wang C. An experimental study to determine the role of inferior vena cava filter in preventing bone cement implantation syndrome. Iran J Radiol. (2015) 12:e14142. doi: 10.5812/iranjradiol.14142v2
14. Agko M, Nazzal M, Jamil T, Castillo-Sang M, Clark P, Kasper G. Prevention of cardiopulmonary embolization of polymethylmethacrylate cement fragment after kyphoplasty with insertion of inferior vena cava filter. J Vasc Surg. (2010) 51:210–3. doi: 10.1016/j.jvs.2009.07.110
15. Prater S, Awan MA, Antuna K, Colon JZ. Prevention of pulmonary cement embolism by inferior vena cava filter following vertebroplasty-related cement intravasation. J Radiol Case Rep. (2021) 15:17–27. doi: 10.3941/jrcr.v15i4.4139
16. Edwards C II, Blight A, Kim K, Edwards C Sr. polymethylmethacrylate entrapped in inferior vena cava filter after a scheuermann kyphosis revision surgery. Spine Deform. (2015) 3:604–7. doi: 10.1016/j.jspd.2015.03.004
17. Li Z, Ni RF, Zhao X, Yang C, Li MM. Cement embolus trapped in the inferior vena cava filter during percutaneous vertebroplasty. Korean J Radiol. (2013) 14:451–4. doi: 10.3348/kjr.2013.14.3.451
18. Athreya S, Mathias N, Rogers P, Edwards R. Retrieval of cement embolus from inferior vena cava after percutaneous vertebroplasty. Cardiovasc Intervent Radiol. (2009) 32:817–9. doi: 10.1007/s00270-009-9550-6
19. Herbstreit F, Kühl H, Peters J. A cemented caval vein filter: case report. Spine. (2006) 31:E917–9. doi: 10.1097/01.brs.0000245824.63150.ef
20. Venmans A, Klazen CA, Lohle PN, van Rooij WJ, Verhaar HJ, de Vries J, et al. Percutaneous vertebroplasty and pulmonary cement embolism: results from VERTOS II. AJNR Am J Neuroradiol. (2010) 31:1451–3. doi: 10.3174/ajnr.A2127
21. Tucker WD, Shrestha R, Burns B. Anatomy, Abdomen and Pelvis, Inferior Vena Cava. Treasure Island, FL: StatPearls Publishing (2021).
22. Geng Z, Zhou Q, Shang G, Ji Y, Kou H, Liu H. Short-term efficacy of the percutaneous vertebroplasty using a curved versus straight vertebroplasty needle in osteoporotic vertebral compression fractures. Orthopedics. (2021) 44:e131–8. doi: 10.3928/01477447-20201012-03
23. Amoretti N, Huwart L. Percutaneous extraction of cement leakage after vertebroplasty under CT and fluoroscopy guidance: a new technique. Cardiovasc Intervent Radiol. (2012) 35:1492–5. doi: 10.1007/s00270-012-0414-0
24. Ishak B, Bajwa AA, Schneider T, Tubbs RS, Iwanaga J, Ramey WL, et al. Early complications and cement leakage in elderly patients who have undergone intraoperative computed tomography (CT)-guided cement augmented pedicle screw placement: eight-year single-center experience. World Neurosurg. (2019) 128:e975–81. doi: 10.1016/j.wneu.2019.05.047
25. Phillips FM, Todd Wetzel F, Lieberman I, Campbell-Hupp M. An in vivo comparison of the potential for extravertebral cement leak after vertebroplasty and kyphoplasty. Spine. (2002) 27:2173–8. doi: 10.1097/00007632-200210010-00018
26. Zhan Y, Jiang J, Liao H, Tan H, Yang K. Risk factors for cement leakage after vertebroplasty or kyphoplasty: a meta-analysis of published evidence. World Neurosurg. (2017) 101:633–42. doi: 10.1016/j.wneu.2017.01.124
27. Kao FC, Tu YK, Lai PL, Yu SW, Yen CY, Chou MC. Inferior vena cava syndrome following percutaneous vertebroplasty with polymethylmethacrylate. Spine. (2008) 33:E329–33. doi: 10.1097/BRS.0b013e31816f6a10
28. David S, Kleber FX. Cement embolism in the vena cava after pedicle screw augmentation. Unfallchirurg. (2021) 124:512–6. doi: 10.1007/s00113-020-00920-5
29. Izumi Y, Ishihara S, Cammack I, Miyawaki I. Massive mass embolism detected by transesophageal echocardiography in bone cement implantation syndrome: a case report. JA Clin Rep. (2019) 5:5. doi: 10.1186/s40981-019-0225-2
30. Frenk NE, Salazar GM, Vazquez R, Irani Z. Intravascular cement leak after vertebroplasty treated with stent graft placement in the inferior vena cava. J Vasc Interv Radiol. (2019) 30:74–5. doi: 10.1016/j.jvir.2018.07.013
31. Park JS, Kim J, Lee Y, Gwon JG, Park YS. Intra-cardiac embolism of a large bone cement material after percutaneous vertebroplasty removed through a combination of an endovascular procedure and an inferior vena cava exploration: a case report. J Korean Med Sci. (2018) 33:e141. doi: 10.3346/jkms.2018.33.e141
32. Majunke N, Unger E, Besler C, Sandri M. Differential diagnosis for an intracaval foreign body. JACC Cardiovasc Interv. (2018) 11:e171–2. doi: 10.1016/j.jcin.2018.07.033
33. Isaak A, Takes M, Kingsmore D, Gürke L. Endovascular retrieval of intracaval cement: a fishing net technique. Cardiovasc Intervent Radiol. (2018) 41:1958–61. doi: 10.1007/s00270-018-2061-6
34. Elens M, Lecouvet F. Vertebral cement leak: how far will it go… ?. Eur J Vasc Endovasc Surg. (2018) 55:416. doi: 10.1016/j.ejvs.2017.09.008
35. Suwan TZ. Foreign body in the infrarenal inferior vena cava: is it a filter?. J Vasc Interv Radiol. (2017) 28:1750. doi: 10.1016/j.jvir.2017.05.025
36. Shen C, Liu G, Hu JZ, Yang XH. Cardiac perforation and multiple emboli after percutaneous vertebroplasty. Orthopedics. (2015) 38:e947–50. doi: 10.3928/01477447-20151002-93
37. Schmid R, Efinger K, Schulz C, Sparwasser C, Martinschek A. Vena cava cement embolism after percutaneous kyphoplasty. Interventional radiological recovery in metastasized urothelial cancer. Urologe A. (2014) 53:62–6. doi: 10.1007/s00120-013-3315-1
38. Lee V, Patel R, Meier P, Lawrence D, Roberts N. Conservative management of inferior vena cava cement spike after percutaneous vertebroplasty causes fatal cardiac tamponade. J Rheumatol. (2014) 41:141–2. doi: 10.3899/jrheum.130570
39. Vallabhajosyula S, Sundaragiri PR, Bansal O, Townley TA. A rare nidus for pulmonary thromboembolism after vertebroplasty. BMJ Case Rep. (2013) 2013:bcr2013200763. doi: 10.1136/bcr-2013-200763
40. Sun R, Maier B, Theilmann L, Abdel Samie A. [Partial thrombosis of the inferior vena cava in a patient with non-Hodgkin lymphoma and history of lumbar spine surgery]. Internist. (2012) 53:474–7. doi: 10.1007/s00108-011-2991-4
41. Schulz C, Efinger K, Schwarz W, Mauer UM. Experiences with cement leakage after balloon kyphoplasty. Orthopade. (2012) 41:881–8. doi: 10.1007/s00132-012-1964-1
42. Kim SM, Min SK, Jae HJ, Min SI, Ha J, Kim SJ. Successful thrombolysis, angioplasty, and stenting of delayed thrombosis in the vena cava following percutaneous vertebroplasty with polymethylmethacrylate cement. J Vasc Surg. (2012) 56:1119–23. doi: 10.1016/j.jvs.2012.02.039
43. Czesla M, Karnari O, Götte J, Schulte B, Pfeilsticker U, Narr A, et al. Unusual cause of acute back pain mimicking aortic dissection: a case report. Thorac Cardiovasc Surg. (2012) 60:e28–30. doi: 10.1055/s-0031-1295580
44. Dash A, Brinster DR. Open heart surgery for removal of polymethylmethacrylate after percutaneous vertebroplasty. Ann Thorac Surg. (2011) 91:276–8. doi: 10.1016/j.athoracsur.2010.06.106
45. Lim KJ, Yoon SZ, Jeon YS, Bahk JH, Kim CS, Lee JH, et al. An intraatrial thrombus and pulmonary thromboembolism as a late complication of percutaneous vertebroplasty. Anesth Analg. (2007) 104:924–6. doi: 10.1213/01.ane.0000256974.84535.7a
46. Baumann A, Tauss J, Baumann G, Tomka M, Hessinger M, Tiesenhausen K. Cement embolization into the vena cava and pulmonal arteries after vertebroplasty: interdisciplinary management. Eur J Vasc Endovasc Surg. (2006) 31:558–61. doi: 10.1016/j.ejvs.2005.11.008
47. Prymka M, Pühler T, Hirt S, Ulrich HW. [Extravertebral cement drainage with occlusion of the extradural venous plexus into the vena cava after vertebrobplasty. Case report and review of the literature]. Unfallchirurg. (2003) 106:860–4. doi: 10.1007/s00113-003-0644-3
Keywords: vertebroplasty, bone cement, inferior vena cava, inferior vena cava filter, complication
Citation: Han X, Zhang Y, Wang Z and Zhao M (2022) Case report: Cement entrapped in the inferior vena cava filter after pedicle screw augmentation. Front. Cardiovasc. Med. 9:892025. doi: 10.3389/fcvm.2022.892025
Received: 08 March 2022; Accepted: 29 August 2022;
Published: 29 September 2022.
Edited by:
Xin Zhao, Shanghai Jiao Tong University, ChinaReviewed by:
Mark G. Davies, The University of Texas Health Science Center at San Antonio, United StatesCopyright © 2022 Han, Zhang, Wang and Zhao. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Zhu Wang, YnlmeXdhbmd6QDEyNi5jb20=; Mengpeng Zhao, Ynp6cDIwMTFAMTI2LmNvbQ==
†These authors have contributed equally to this work
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.