 María Eugenia de la Morena-Barrio1
María Eugenia de la Morena-Barrio1 Javier Corral1*
Javier Corral1* Cecilia López-García2
Cecilia López-García2 Víctor Alonso Jiménez-Díaz3Antonia Miñano1Pablo Juan-Salvadores3
Víctor Alonso Jiménez-Díaz3Antonia Miñano1Pablo Juan-Salvadores3 María Asunción Esteve-Pastor2José Antonio Baz-Alonso3Ana María Rubio1Francisco Sarabia-Tirado4Miguel García-Navarro2Juan García-Lara2
María Asunción Esteve-Pastor2José Antonio Baz-Alonso3Ana María Rubio1Francisco Sarabia-Tirado4Miguel García-Navarro2Juan García-Lara2 Francisco Marín2Vicente Vicente1Eduardo Pinar2Sergio José Cánovas5Gonzalo de la Morena2*
Francisco Marín2Vicente Vicente1Eduardo Pinar2Sergio José Cánovas5Gonzalo de la Morena2*- 1Centro Regional de Hemodonación, Servicio de Hematología y Oncología Médica, Hospital Universitario Morales Meseguer, IMIB-Arrixaca, Centro Investigacion Biomédica en red Enferemedades Raras (CIBERER), CEIR Campus Mare Nostrum (CMN), Universidad de Murcia, Murcia, Spain
- 2Servicio de Cardiología, Hospital Clínico Universitario Virgen de la Arrixaca, Universidad de Murcia, IMIB-Arrixaca, Centro de Investigación Biomédica en Red Enfermedades Cardiovasculares (CIBERCV), Murcia, Spain
- 3Unidad de Investigación Cardiovascular, Servicio de Cardiología, Hospital Álvaro Cunqueiro, Vigo, Spain
- 4Servicio de Radiología, Hospital Clínico Universitario Virgen de la Arrixaca, Murcia, Spain
- 5Servicio de Cirugía Cardiovascular, Hospital Clínico Universitario Virgen de la Arrixaca, Murcia, Spain
Background: Aortic valve replacement is the gold standard treatment for severe symptomatic aortic stenosis, but thrombosis of bioprosthetic valves (PVT) remains a concern.
Objective: To analyze the factors involved in the contact pathway during aortic valve replacement and to assess their impact on the development of thromboembolic complications.
Methods: The study was conducted in 232 consecutive patients who underwent: transcatheter aortic valve replacement (TAVR, N = 155), and surgical valve replacement (SAVR, N = 77) (MUVITAVI project). Demographic and clinical data, outcomes including a combined end point (CEP) of thrombotic events, and imaging controls were recruited. Samples were collected 24 h before and 48 h after valve replacement. FXII, FXI and (pre)kallikrein were evaluated by Western Blot and specific ELISA with nanobodies.
Results: The CEP of thrombotic events was reached by 19 patients: 13 patients presented systemic embolic events and 6 patients subclinical PVT. Valve replacement did not cause FXII activation or generation of kallikrein. There was a significant reduction of FXI levels associated with the procedure, which was statistically more pronounced in SAVR than in TAVR. Cases with reductions of FXI below 80% of basal values had a lower incidence of embolic events during the procedure than patients in whom FXI increased above 150%: 2.7 vs. 16.7%; p: 0.04.
Conclusion: TAVR or SAVR did not significantly activate the contact pathway. A significant reduction of FXI, was observed, particularly in SAVR, associated with lower incidence of thrombotic events. These results encourage evaluating the usefulness and safety of FXI-directed antithrombotic treatments in these patients.
Introduction
Aortic stenosis (AS) has become the most common primary heart valve disease and an major cause of cardiovascular morbidity and mortality (1). Aortic valve replacement is the treatment of choice for symptomatic patient who undergo more than > 100.000 procedures annually in the United States alone (2). Bioprosthetic valves are by far the most commonly implanted valves, representing almost 80% of surgical aortic valve replacements (SAVR) (3) and all implanted transcatheter valves (TAVR). In recent years, different studies have warned about the development of bioprosthetic valves thrombosis (PVT). Clinical or subclinical thrombosis has been described in up to 10% of the patients and this complication seems to be associated with higher frequency of prosthetic dysfunction, embolic events and the need for replacement (4, 5). The significant morbidity and mortality associated with this condition warrants rapid diagnostic evaluation and predictive tools. However, diagnosis can be challenging, mainly because of variable clinical presentations, the diagnostic tools used, and the degree of valvular obstruction.
In this framework, it is interesting to analyze the impact of aortic valve replacement in different systems, particularly those involved in thrombosis, the most frequent complication observed in these patients. These studies could identify new biomarkers and new treatment targets that could improve the outcome of valve replacement. The haemostatic system is an excellent candidate to be evaluated. Particularly interesting is the contact pathway of coagulation, as it has minor physiological relevance but is activated by negatively charged surfaces and artificial surfaces of medical devices (6). The contact pathway includes three elements with proteolytic activity: factor XII (FXII), factor XI (FXI) and (pre)kallikrein, which are involved in multiple vital proteolytic cascades: host defense, inflammation and coagulation after activation by negatively charged surfaces (7). Although deficiency or inhibition of these elements has no or minor physiological consequences on hemostasis (8), recent evidence support a key pathological role for these contact elements, and different approaches are being developed to target FXII, FXI, or (pre)kallikrein with antithrombotic potential and minor risk of bleeding (9, 10). Indeed, the elements of the contact pathway have been suggested as potential targets of new anticoagulant treatments for patients receiving medical devices (11–13). This is a relevant issue because antithrombotic therapy after aortic valve replacement has not yet been defined (14).
Our study has been designed to explore the impact of aortic valve replacement on the contact pathway elements with the aim of finding new biomarkers useful for the management of these patients as well as new clues for the best antithrombotic treatment in this scenario (Figure 1).
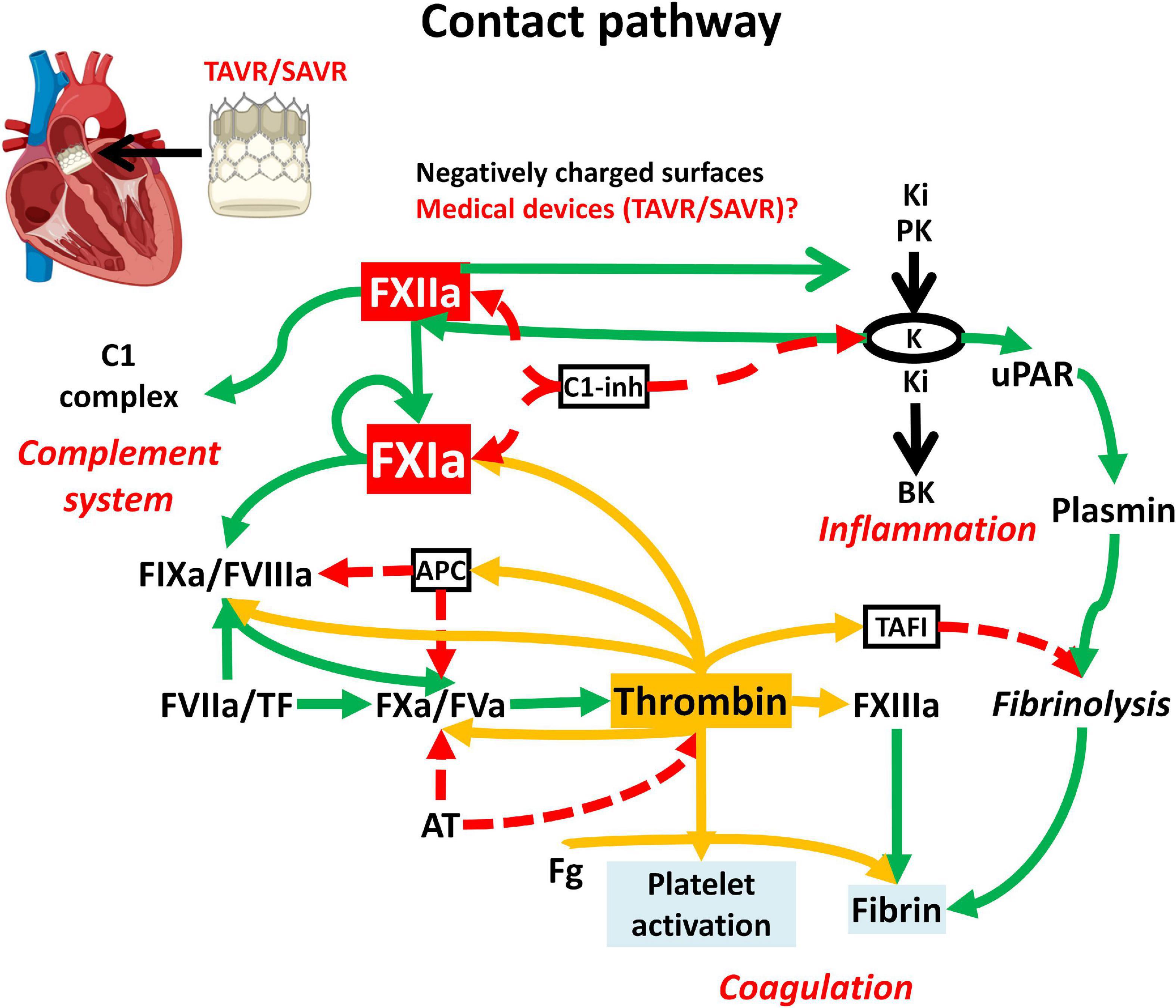
Figure 1. Scheme of the contact pathway and its involvement in coagulation, inflammation and complement system. Surgical (SAVR) or transcatheter (TAVR) aortic valve is illustrated as a potential trigger of FXII autoactivation. Dashed red arrows indicate inhibition; green arrows activation; yellow arrows activation by thrombin. APC, activated protein C; Ki, Kininogen; PK, prekallikrein; K, kallikrein; BK, bradykinin; TAFI, thrombin activable fibrinolysis inhibitor; Fg, fibrinogen; C1-inh, C1-inhibitor; uPAR, urokinase-type plasminogen; TF, Tissue Factor.
Patients and methods
Patients
The MUVITAVI (MUrcia and VIgo Transcatheter Aortic Valvular Implantation) project is an observational study of patients who underwent two aortic valve replacement procedures (TAVR and SAVR) consecutively recruited between February-2018 to February 2020 from two Spanish referenced hospitals: Hospital Clínico Universitario Virgen de la Arrixaca in Murcia, and Álvaro Cunqueiro in Vigo.
The inclusion criteria were age over 50 years, and to give their informed consent to enter the study, which was approved by the Ethics Committees from each Hospital and performed in accordance with the 1964 Declaration of Helsinki and their later amendments.
Patients with single and programmed procedures were included. Exclusion criteria included: emergency or urgent procedures two or more valves treated any suspicion of endocarditis or combined coronary revascularization.
Clinical data, imaging controls, and follow-up
Demographics and clinical data, comorbidities, and outcomes were recruited by independently observers blinded to hematologic analysis. Patients were followed-up every 6 months. Periprocedural complications, clinical follow-up, transthoracic echocardiography (TTE) and computer tomography imaging (CT) results were incorporated using an online standardized data collection.
Sample collection
Samples were collected 24 h before and 48 h after the replacement in vacuum tubes containing 0.109 M sodium citrate. Platelet-poor plasma (PPP) was obtained within 2 h after extraction by centrifugation (2000 g × 15 min) at 20°C and then stored at -80°C.
As reference plasma we used a pool of 100 healthy blood donors. Moreover, as controls we also included plasma of one patient with congenital FXI deficiency caused by the p.Cys416Tyr pathogenic gene variation in heterozygosis (FXI:C 37%), and plasma of another patient with congenital FXII deficiency caused by a homozygous deletion of a single nucleotide (c.919del G) causing a frameshift (p.Val307Cysfr*44) (FXII:C 3%).
Variations of FXI levels were calculated as the ratio between FXI levels after 48 h from procedure (B) and the FXI basal levels (A), and expressed in percentages, FXI (B/A) (%).
Contact pathway analysis
Plasma FXII, FXI and (pre)kallikrein were evaluated by SDS-PAGE and Western Blot using procedures described elsewhere (15, 16). Two antibodies targeting FXI were used: GAFXI-AP (Enzyme Research, United Kingdom) detecting the dimer under not-reducing conditions and GAFXI-HRP (Enzyme Research, United Kingdom) that also detects FXIa under reducing conditions using dithiothreitol. Densitometry analysis of Western blot results was done with ImageJ (17).
Quantification of FXIIa-C1 inhibitor and FXIa-C1 inhibitor complexes were done with specific ELISA using nanobodies provided by ISTH Cosyne programme (18, 19). Values were represented as percentages of those observed in kaolin-full activated reference plasma.
Determination of FXI levels was also done with a functional assay using the FXIa specific chromogenic substrate SC2366 after full activation of the contact pathway with kaolin.
Procoagulant markers
Activation of the coagulation cascade was evaluated by determination of antithrombin activity using a functional anti-FXa assay with heparin, bovine FXa, and S-2765 chromogenic substrate (HemosIL TH, Instrumentation Laboratory, Italy) and by quantifying thrombin-antithrombin (TAT) complexes by SDS-PAGE Western blot under reducing conditions using a polyclonal antibody (A9522, Sigma-Aldrich) and by a specific ELISA [ab108907 –Thrombin-Antithrombin Complex (TAT) Human ELISA Kit, Abcam].
Genetic analysis
The exons and flanking regions of F12 gene were amplified and sequenced as described before (20).
Thrombotic events
We recruited all embolic events happened during follow-up period. A composite end point (CEP) of thrombotic events included: any peripheral embolic event, transient ischaemic attack or stroke, and clinical or subclinical PVT. Diagnosis of subclinical PVT required at least one of the three next imaging criteria: a twofold increase in mean transaortic Doppler gradient, mobile thrombus attached to the prosthesis, or the presence of hypo attenuated leaflet thickening (HALT) with reduced leaflet motion on CT (5).
Statistical analysis
Descriptive analysis of qualitative variables included percentages. Normally distributed continuous variables were presented as means ± standard deviations (SD), whereas non-normally distributed variables were presented as median and interquartile ranges (IQR). Pearson’s Chi-Squared test and Fisher’s exact test were used for comparison of proportions or ordinal variables. Kolmogorov–Smirnov and Shapiro–Wilk tests were used for testing normality of continuous variables. Student’s-T (parametric) or Mann–Whitney-U tests were used for comparison of two means and analysis of variance (ANOVA, parametric) or Kruskal–Wallis (non-parametric) tests were used for comparison of more than two means. Apart from p-values, 95% Confidence Intervals (95% CI) were also calculated.
Statistical analysis was performed with the use of Excel ® (Microsoft), GraphPad Prism ® (GraphPad Software), and IBM SPSS Statistics 21 ® (IBM SPSS Software).
Results
Characteristics of the cohort
A total of 232 patients were included: 155 in TAVR and 77 in SAVR group. Table 1 shows the main characteristics of the patients.
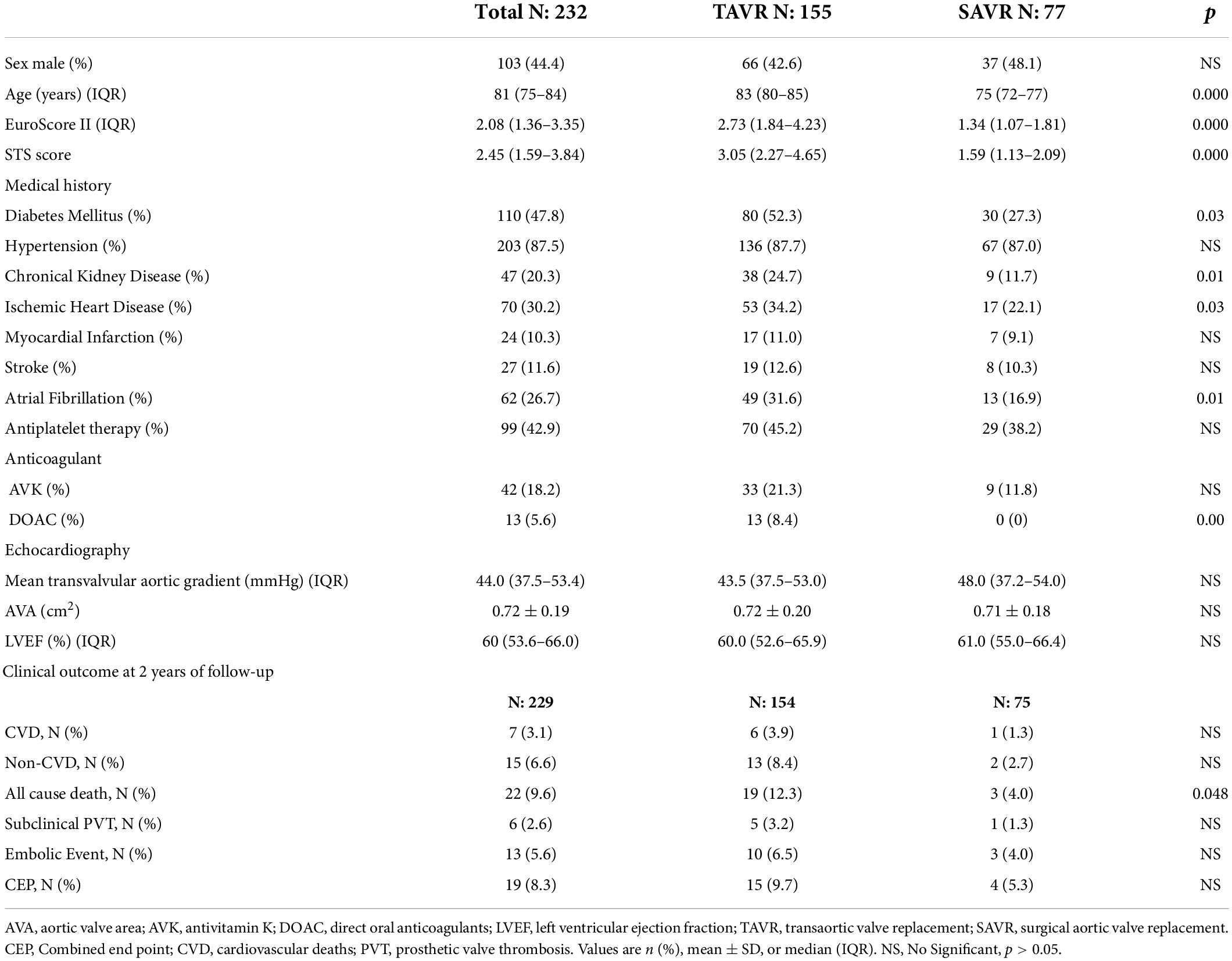
Table 1. Demographic, clinical characteristics, and clinical outcomes of patients underwent TAVR or SAVR.
Patients in the TAVR group were older and had higher mortality risk scores and comorbidity burden than patients in the SAVR group. Likewise, the incidence of atrial fibrillation and the use of direct oral anticoagulants were significantly higher in the TAVR group. Echocardiographic parameters were comparable between both groups.
In SAVR group, 39 patients (50.6%) had a “sutureless” type of rapid deployment prosthesis: 30 Perceval ®, and 9 Edwards Intuity ®; while 38 (49.3%) received a “sutured” type prosthesis: 22 Edwards Perimount Magna Ease ®, 10 Crown PRT ®, 3 Trifecta SJM ®, 2 Edwards Inspiris ® and 1 Carbomedics Top Hat ®. In TAVR group, 106 patients (68.4%) had a balloon-expandable prosthesis Edwards Sapiens ®, and 49 (31.6%) a self-expandable valve: 29 Core Valve ®, 16 AllegraTM ®, 2 Acurate ®, and 2 Portico ®.
After the procedure all patients were on standardized treatment with double antiplatelet therapy (aspirin and clopidogrel). Additionally, 49 (31%) patients in TAVR group and 7 (9.4%) patients in SAVR group were anticoagulated with either antivitamin K or direct oral anticoagulant.
Activation of the contact pathway
We firstly evaluated a potential activation of the contact pathway by the replacement of a cardiac valve. Our results show that, regardless of the procedure, it did not cause detectable activation of FXII by Western Blot (Figure 2A). Consistent with this result, neither TAVR nor SAVR caused generation of detectable kallikrein in plasma by Western Blot (Figure 2B).
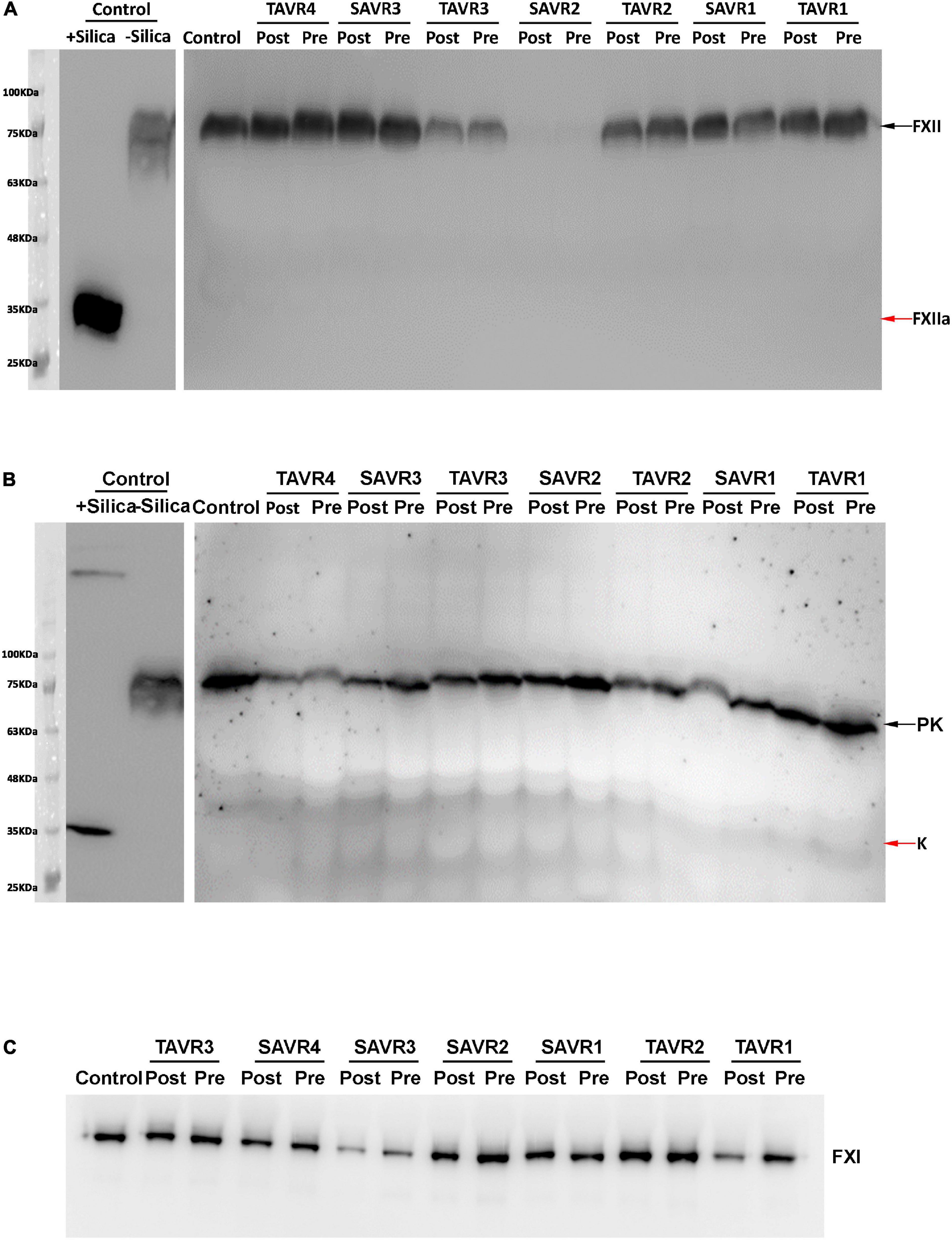
Figure 2. Plasma FXII (A), Pre(Kallikrein) (B), and FXI (C) detected by Western Blot after SDS-PAGE in representative samples of patients underwent TAVR or SAVR. The samples pre and post-procedure are indicated. Zymogens are pointed by black arrows, while activated forms are pointed by red arrows. As control of activation, plasma from a pool of 100 healthy blood donors was treated with silica.
Quantification of FXIIa-C1 inhibitor complexes by a specific ELISA using nanobodies revealed negligible activation of FXII either in basal samples or in samples collected after the transcatheter aortic valve replacement process (Figure 3), independently of the replacement procedure (TAVR; pre = 0.069 ± 0.066% post = 0.077 ± 0.065%; or SAVR; pre = 0.049 ± 0.044% post = 0.024 ± 0.038%).
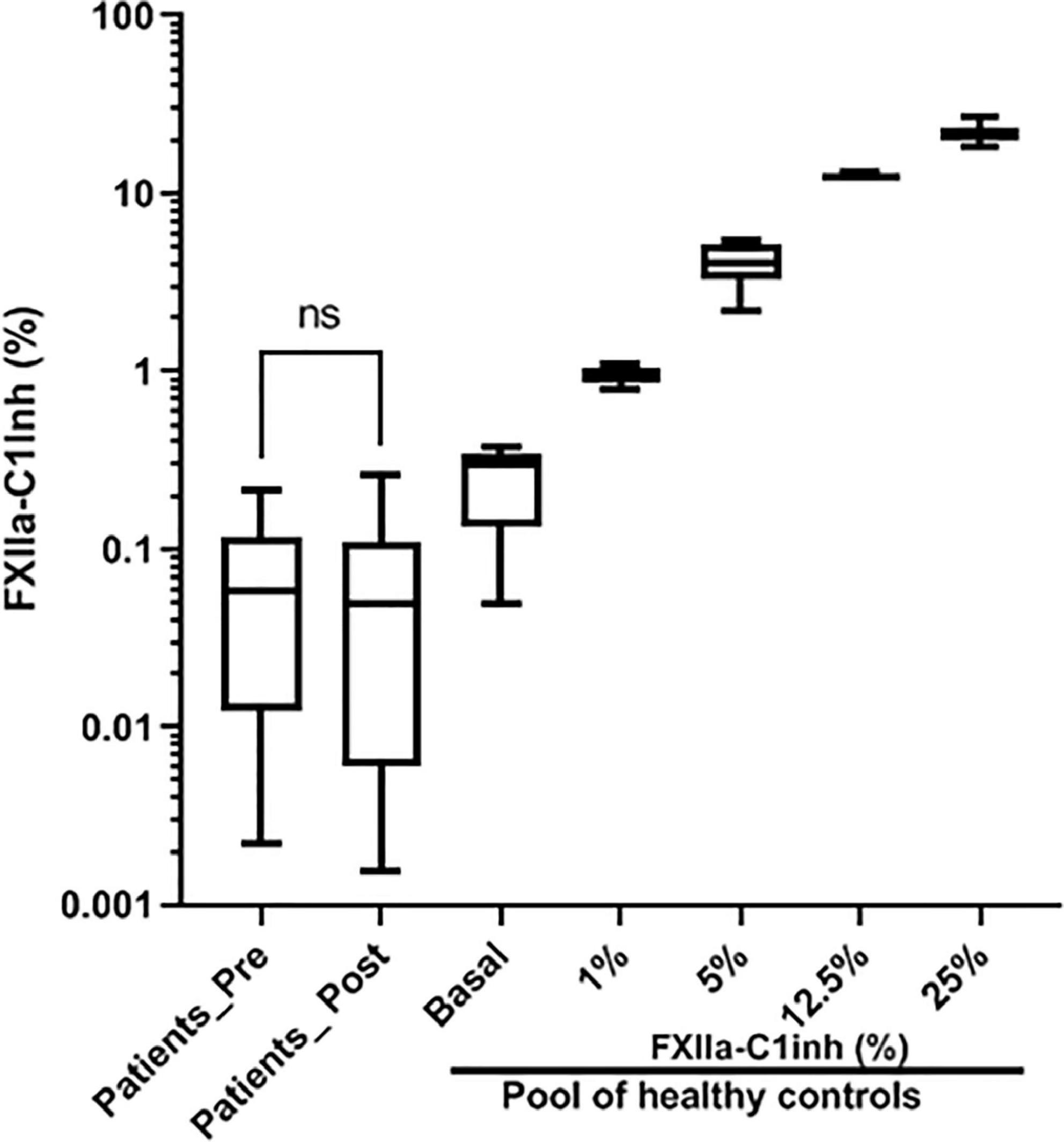
Figure 3. Levels of FXIIa-C1 Inhibitor complexes in pre- and post-procedure samples. Values, referenced as percentages of kaolin-full activated reference pool plasma generated 100 healthy subjects, were determined by a specific ELISA using nanobodies. ns: p > 0.05.
FXI activation, assessed by two methods, Western blot analysis using reducing conditions and by a FXIa-C1 inhibitor specific ELISA using nanobodies, revealed negligible FXI activation either in basal samples or in samples collected post-procedure (Figure 4), regardless of the replacement procedure [TAVR; pre = 0.03(0.01–0.14)% post = 0.10(0.01–0.67)%; or SAVR; pre = 3.49(0.01–7.04)% post = 0.27(0.02–3.27)].
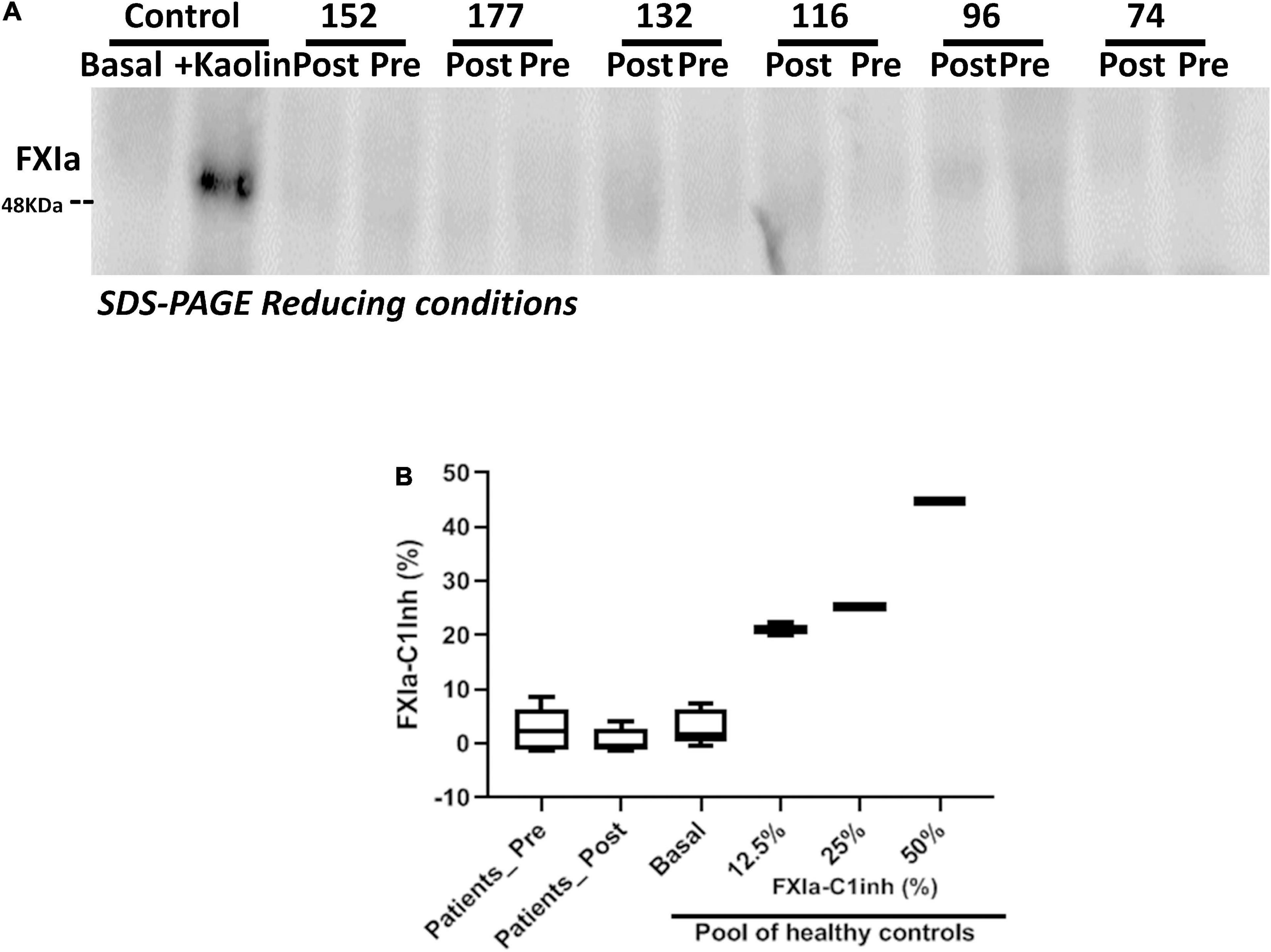
Figure 4. FXIa levels in patient samples pre and post-procedure. (A) Representative Western blot of plasma samples of patients pre- and post- procedure. As control, plasma from a healthy subject was also evaluated without and after full activation with kaolin; (B) FXIa-C1 inhibitor complexes quantified by ELISA using nanobodies. As standards, a basal sample, and dilutions of fully kaolin-activated plasma of a pool of 100 healthy control subjects were used.
Variations of FXII and FXI levels
Significant variations in FXII levels were observed between patients (Figure 2A), but as expected, they correlated with the functional and common polymorphism affecting the Kozak sequence of F12.
One patient, TAVR44, an 87-year-old-male patient who received TAVR, had a complete FXII deficiency, similar to that found in a patient with congenital FXII deficiency (Supplementary Figure 1A). As expected, all other liver proteins tested (antithrombin and FXI) reached normal levels, similar to that found in the congenital FXII-deficient patient (Supplementary Figure 1B). Genetic analysis of F12 revealed a new missense mutation, not found in ExAC or 1000 Genomes, that located in exon 11: c.1277 T > G; p.Val426Gly Supplementary Figure 1C). This genetic variant, which was found in heterozygous state, was a disease-causing mutation as predicted by Mutation Taster (21). Additionally, the patient was homozygous for an intronic variant that might affect the correct splicing of this gene: c.1251 –9°C > T, a frequent gene variation (MAF: 0.6517) with benign prediction (Supplementary Figure 1C) and homozygous T/T for the functional Kozak polymorphism (22). TAVR44 had hypertension, Charlson comorbidity index of 4, STS score of 3.36, EuroScore II of 1.94, severe aortic valve stenosis with mild insufficiency, angina and dyspnea, NYHA III, and atrial fibrillation. The patient was under oral anticoagulation (Rivaroxaban 15 mg). The patient underwent transfemoral TAVR (Edwards Sapiens N°29). No complications were recorded during the procedure. During the 6-month follow-up no adverse event was observed. FXI levels in this patient were normal according to Western blot and functional assays, and no activation of FXI was observed by Western blot or ELISA either in both samples, basal and post-TAVR procedure (Supplementary Figure 1D).
Finally, no differences in antithrombin activity were detected in basal and post-procedure samples (85 and 92%, respectively) and no TAT complexes were observed in baseline or post-procedure samples (Supplementary Figure 1B).
For the entire cohort, no significant differences were observed in the levels of FXII and FXIIa-C1 inhibitor in the samples collected before and 2 days after the valvular replacement procedure (Figures 2, 3).
No patient included in this study had FXI or (pre)kallikrein deficiency (Figures 2B,C). As described, FXI levels showed an interpersonal heterogeneity (Figure 2C). Interestingly, in 60.8% of patients the replacement of the cardiac valve reduced FXI levels in the post-procedure sample compared to the levels observed in the pre-procedure sample. Only 18 patients showed relevant increases of FXI levels (> 150% of the basal levels) after the procedure (7.8%), but in 75 cases (32.3%) FXI levels in the post-procedure sample were lower than 80% of the value observed in the baseline sample (Figure 2C). Functional assays confirmed the reduction of FXI levels in post-procedure samples (Figure 5).
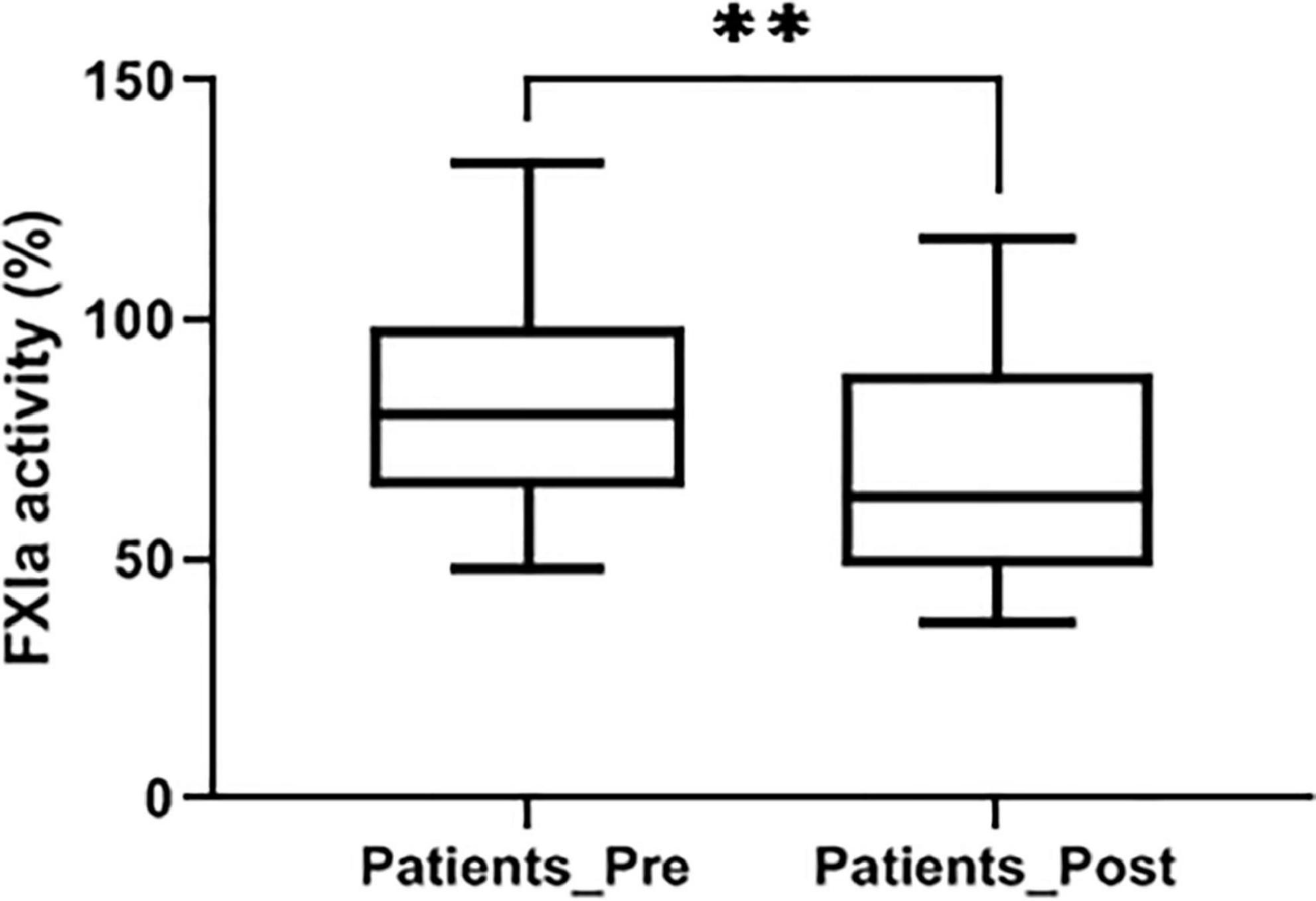
Figure 5. FXI levels determined by a chromogenic method after full activation with kaolin in pre- and post-procedure samples. Values were represented as% of a reference pool of plasma from 100 healthy subjects. **p < 0.01.
The type of procedure showed a significant effect in reducing FXI levels after the valve replacement. Thus, patients who underwent SAVR showed a more severe reduction in FXI levels than TAVR [86.0% IQR (67.0–108.5) vs. 94.5% IQR (78.7–110.0); p = 0.035]. The percentage of patients with significant reduction of FXI levels in the post-procedure sample (< 80%) was also higher among SAVR patients than TAVR patients (35/78: 44.9% vs. 40/154: 26.0%, respectively; p = 0.004).
The type of bioprosthesis, balloon-expandable vs. self-expandable, in TAVR group (100.5 ± 42.9 vs. 100.0 ± 35.3; p = ns), or sutureless vs. sutured (98.1 ± 44.8 vs. 85.4 ± 29.7; p: 0.06) in SAVR patients, did not affect FXI levels during the procedure.
All-cause death at 30-day follow-up was 1.3% without differences between groups: 1 patient on TAVR and 2 patients on SAVR. Nineteen patients had bleeding requiring transfusion: 13 (8.4%) TAVR, 6 (7.8%), SAVR (p = ns) and 24 patients required permanent pacemaker: 23 (14.5%) TAVR and 1 (1.3%) SAVR (p = 0.001).
Clinical follow-up was completed in all 229 patients who survived the first month. Table 1 shows clinical complications during a period of 22.1 ± 9.9 months (median 24 months).
Thromboembolic events after TAVR or SAVR were distributed as follows: 13 patients presented with systemic embolic events (10 stroke and 3 peripheral embolism), and only 6 patients had subclinical PVT. So, the CEP of thrombotic events was reached by 19 patients without differences between groups.
We analyzed in detail the potential role of FXI variations in the complications of these procedures. Patients with thrombotic complications or periprocedural mortality showed increased FXI levels in samples collected post-procedure compared to those from the pre-procedure, although results did not show statistical significance (96.2 ± 37.3 vs. 116.0 ± 43.1, p = 0.086, Supplementary Figure 2). Moreover, patients with elevated FXI levels after the procedure (> 150% of baseline values) showed a higher incidence of thrombotic events or periprocedural mortality than that found in patients with reduced FXI [4/18 (22.2%) vs. 2/75 (2.7%); p = 0.02] (Table 2). Among those who showed reductions in the FXI levels after the procedure, only 2 out of 75 (2.7%) had embolic events and no one died during the procedure.
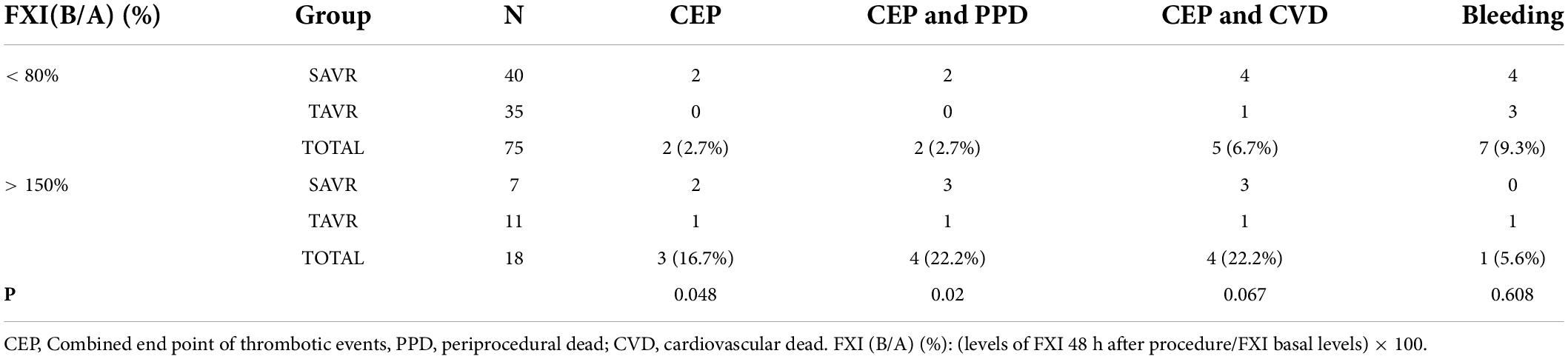
Table 2. Complications described in patients with cardiac valve replacement according to the evolution of FXI levels after the procedure.
On the other hand, 7 patients with reduced FXI after the cardiac valve replacement suffered severe bleeding during the procedure that required transfusions (9.3%) (Table 2). The incidence of bleeding requiring transfusion was similar in both groups (Table 2).
Coagulation activation was studied by quantifying two procoagulant markers: antithrombin levels by a functional method, and TAT by ELISA. As shown in Figure 6, independently of the procedure, transcatheter valve replacement caused minor, if any, activation of the coagulation cascade.
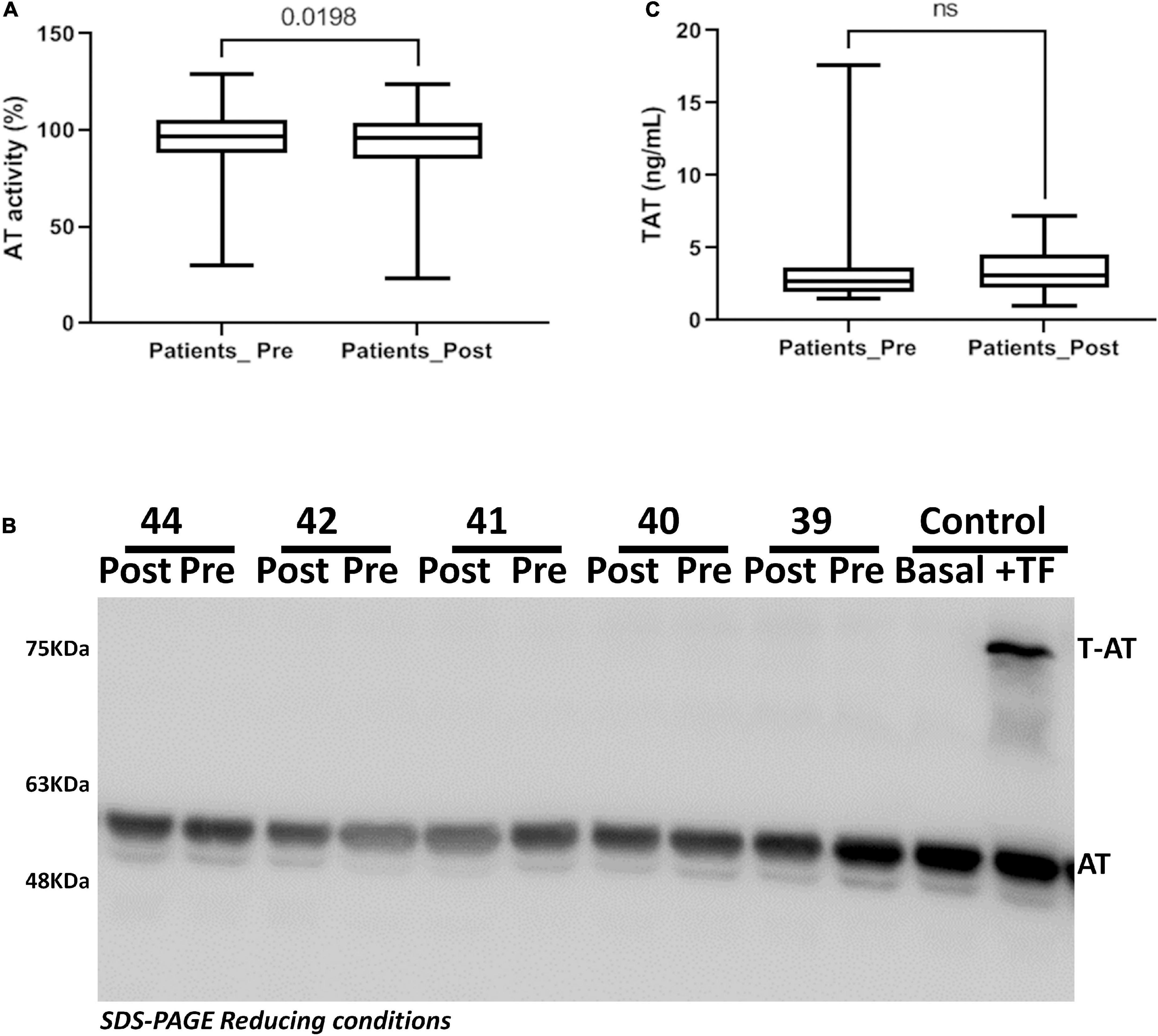
Figure 6. Antithrombin activity in patients underwent transcatheter aortic valve replacement. (A) Anti-FXa activity. (B) Thrombin-Antithrombin complexes quantified by ELISA. (C) Plasma antithrombin detected by Western blot. Representative samples are shown.
The influence of anticoagulation on the variation of FXI level was also evaluated. 42/232 patients (18%) were anticoagulated with antivitamin K before the procedure. The ratio pre/post of FXI levels was not associated with anticoagulation (anticoagulated: 104 ± 44 vs. not anticoagulated: 95 ± 36, p = 0.113).
Finally, we have evaluated the impact on FXI of possible confounder factors such as renal and hepatic function, left ventricular ejection fraction, pulmonary hypertension and other intraoperative and post-operative complications (pericardial drainage, permanent pacemaker, severe hemorrhage, cardiac tamponade, atrial fibrillation, infections, pleural effusion), and we found no significant associations (data not shown).
Discussion
This is the first study to evaluate the contact pathway in a large cohort of consecutive patients who underwent aortic valve replacement, TAVR or SAVR. Our results showed that these two procedures do not activate the contact pathway. Moreover, post-procedural reduction of FXI levels was associated with a lower incidence of thrombotic events, particularly in SAVR.
Recent evidence suggests an emerging relevance for the contact pathway in medicine. First, the number of disorders involving elements of the contact pathway is increasing due to the key role of the proteases of this pathway in different systems, such as inflammation, coagulation, immune response and fibrinolysis (7, 23). Moreover, the role of FXI, FXII and (pre)kallikrein in hemostasis and thrombosis has changed dramatically. FXI deficiency used to be considered a congenital coagulopathy (Hemophilia C), but it is now widely accepted that patients with FXI deficiency have minor risk of bleeding (24). In contrast, very recent epidemiological data support that FXI deficiency strongly protects against cardiovascular and venous thromboembolism events (25). Animal models support that deficiency of FXI or FXII, or the inhibition of these proteases by different compounds strongly protect against venous or arterial thrombosis without risk of bleeding (9), and a clinical trial using anti-FXI oligonucleotides demonstrates a better antithrombotic efficacy and lower risk of bleeding than classical anticoagulants (heparin) (26). On the other side, high levels of FXI have been shown to be a strong risk factor for both venous and arterial thrombosis (27, 28) and with an increased risk of incident ischemic stroke but not hemorrhagic stroke or incident acute coronary syndrome (29).
Moreover, activation of this pathway has been involved in different disorders with an inflammatory or coagulant phenotype, such as hereditary angioedema or sepsis (30, 31). Although some molecules have been proposed as activators of the contact pathway, such as pathogen surfaces, platelet polyphosphates, subendothelial collagen, misfolded proteins, neutrophils, glycosaminoglycans, or nucleic acids, these mechanisms have not yet been well characterized in vivo (32, 33). We speculated that the replacement of a cardiac valve is a procedure that could activate the contact pathway and might be involved in the thrombotic or bleeding complications observed in a large proportion of these patients.
In this study, we have analyzed the elements of the contact pathway in patients undergoing two cardiac valve replacement procedures, TAVR or SAVR, with different incidence of thrombotic complications. We showed that these two procedures do not activate the contact pathway, since no activated FXII or kallikrein were observed in any patient by various specific methods.
Two findings were remarkable. First, we identified a patient with congenital FXII deficiency, a rare disorder whose pathogenic relevance remains an enigma. Our data support the null risk of bleeding described for patients with congenital FXII deficiency and animal models (34, 35), as this patient did not suffer bleeding complications during the cardiac valve replacement procedure. Moreover, patient TAVR44 did not suffer any thrombotic complication. This result, despite being from a single patient, is consistent with the proposed antithrombotic role of FXII deficiency (13, 36), and the antithrombotic potential of anti-FXII drugs observed in animal models exposed to blood−contacting medical devices, including catheters, stents, grafts, filters, and extracorporeal organ support systems (ECOS) (6).
Finally, we observed that the procedure reduces the concentration of FXI in the post-procedure sample in a significant proportion of cases. The hypothesis of a consumption of FXI by activation of the contact pathway may be rejected to explain this finding due to the null detection of FXIIa or kallikrein in these samples. FXI consumption by thrombin activation can also be ruled out as our study also finds a minor activation of coagulation by the transcatheter valve replacement regardless the procedure. Further studies are required to unravel the mechanism that leads to this reduction, but it is significantly dependent on the type of procedure. Thus, patients who underwent SAVR showed a greater reduction in FXI after the procedure than patients who underwent TAVR. Independently of the mechanism that explains the differences in FXI levels after valve replacement, it seems that reduction in FXI after the procedure could be considered a good prognostic marker for thrombotic complications, especially when compared with patients with increased FXI after the procedure. These results support the antithrombotic protection associated with reduced FXI levels (9, 10) and the increased risk of thrombosis caused by increased levels of this procoagulant protease (37). However, further studies are required to verify the protection against thrombosis caused by a moderate reduction in FXI levels, since most of the studies showing such protection have been done with more severe reductions of FXI (9, 25, 26, 38).
Our results also highlight the higher frequency of vascular complications in the TAVR procedure. In fact, the most common vascular complications during TAVR are bleeding due to difficult access and closure of the femoral artery. Thrombotic complications in the vascular territory are very rare, except stroke. But stroke seems to be more related to debris produced during valve implantation and to large catheters in the aortic arch (39). The requirement of large vascular introducers used in patients with atheromatous, tortuous and calcified arterial tree due to the older patients selected for this procedure could increase FXI levels by a still unknown mechanism that increases the risk of thrombotic events.
However, the genesis of stroke and other thromboembolic complications during the mid-and long-term follow-up after TAVR and SAVR appears to be multifactorial (40). Although our data suggest minor activation of thrombin generation in these patients, the role of increased platelet activation as main seed of the thromboembolic complications is still to be clarified (41).
In contrast, the evolution of FXI levels after the procedure is not significantly associated with the risk of bleeding. Thus, the incidence of major bleeding was similar in patients who had a reduction in this procoagulant protease than in patients with increased FXI. These results are supported by the minor role of FXI levels on the risk of bleeding, provide new evidence for the safety of FXI-targeted treatments as new antithrombotic therapies (42), and outline a more personalized antithrombotic management strategy.
The main limitation of our study is the relatively small number of patients enrolled. Further studies including a larger patient population are required to validate these results and the potential role of FXI variations in the prognosis of heart valve replacement. Moreover, we restricted our analysis to the pre and post-procedures samples. Studies evaluating the contact pathway in samples collected later would provide valuable information.
Conclusion
This study shows no relevant activation of the contact pathway of coagulation by TAVR or SAVR. However, the significant reduction of FXI levels that occurs mainly in SAVR, could be a useful biomarker as it associated with lower incidence of thrombotic events. Moreover, these results encourage evaluating the usefulness and safety of antithrombotic treatments targeting FXI in patients underwent these procedures.
Data availability statement
The original contributions presented in the study are included in the article/Supplementary Material, further inquiries can be directed to the corresponding authors.
Ethics statement
The studies involving human participants were reviewed and approved by the Hospital Clínico Universitario Virgen de la Arrixaca. The patients/participants provided their written informed consent to participate in this study.
Author contributions
CL-G, ME-P, EP, VJ-D, JG-L, MG-N, FS-T, SC, PJ-S, and JB-A recruited samples and clinical outcomes. MM-B, AM, and AR performed experimental analysis. MM-B, JC, FM, GM, VJ-D, ME-P, and VV designed the research, evaluate the data, and wrote the manuscript. All authors read and approved the final manuscript.
Funding
This study was supported by the Sociedad Española de Cardiología: Proyecto FEC Investigación Clínica, 2017. CIBERCV (CB16/11/00385); Fundación Séneca (19873/GERM/15), CIBERER (ACCI18-04; ER19P5AC765/2019); Instituto de Salud Carlos III (PI21/00137); and Sociedad Española de Trombosis y Hemostasia (SETH: grupos emergentes). MM-B has a postdoctoral contract from University of Murcia, Spain.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Acknowledgments
We acknowledge the technical assistance of José Padilla and Pablo Gil-Perez from IMIB-Arrixaca (Murcia). ISTH Cosyne programme for contributing the reagents.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fcvm.2022.887664/full#supplementary-material
Supplementary Figure 1 | Identification of a patient with congenital FXII deficiency who underwent TAVR (TAVR44). The plasma levels of FXII (A) and other hepatic proteins, antithrombin (AT) and FXI (B) were detected by Western Blot. The sample pre and post-procedure are indicated. As controls we used plasma from a pool of healthy blood donors and from a patient with congenital deficiency of FXII caused by the c.919del G homozygous deletion (FXII congenital deficiency). (C) F12 gene variations identified in patient TAVR44 with congenital FXII deficiency. (D) Plasma levels of FXIa in pre- and post-procedure sample from TAVR44 were evaluated by SDS-PAGE Western blot. Plasma from a healthy subject with and without kaolin was used as control.
Supplementary Figure 2 | FXI levels (Post/Pre) according to the presence of thrombotic events or periprocedure death. Values are post- respect to pre- procedure FXI (B/A) antigen, %.
References
1. d’Arcy JL, Prendergast BD, Chambers JB, Ray SG, Bridgewater B. Valvular heart disease: the next cardiac epidemic. Heart. (2011) 97:91–3. doi: 10.1136/hrt.2010.205096
2. Osnabrugge RLJ, Mylotte D, Head SJ, Van Mieghem NM, Nkomo VT, LeReun CM, et al. Aortic stenosis in the elderly. J Am Coll Cardiol. (2013) 62:1002–12. doi: 10.1016/j.jacc.2013.05.015
3. Brown JM, O’Brien SM, Wu C, Sikora JAH, Griffith BP, Gammie JS. Isolated aortic valve replacement in North America comprising 108,687 patients in 10 years: changes in risks, valve types, and outcomes in the Society of Thoracic Surgeons National Database. J Thorac Cardiovasc Surg. (2009) 137:82–90. doi: 10.1016/j.jtcvs.2008.08.015
4. Giustino G, Genereux P. Subclinical thrombosis of bioprosthetic aortic valves. J Am Coll Cardiol. (2020) 75:3016–9. doi: 10.1016/j.jacc.2020.04.060
5. Makkar RR, Blanke P, Leipsic J, Thourani V, Chakravarty T, Brown D, et al. Subclinical leaflet thrombosis in transcatheter and surgical bioprosthetic valves: PARTNER 3 cardiac computed tomography substudy. J Am Coll Cardiol. (2020) 75:3003–15. doi: 10.1016/j.jacc.2020.04.043
6. Srivastava P, Gailani D. The rebirth of the contact pathway: a new therapeutic target. Curr Opin Hematol. (2020) 27:311–9. doi: 10.1097/MOH.0000000000000603
7. Long AT, Kenne E, Jung R, Fuchs TA, Renné T. Contact system revisited: an interface between inflammation, coagulation, and innate immunity. J Thromb Haemost. (2016) 14:427–37. doi: 10.1111/jth.13235
8. Simão F, Feener EP. The effects of the contact activation system on hemorrhage. Front Med. (2017) 4:121. doi: 10.3389/fmed.2017.00121
9. Demoulin S, Godfroid E, Hermans C. Dual inhibition of factor XIIa and factor XIa as a therapeutic approach for safe thromboprotection. J Thromb Haemost. (2021) 19:323–9. doi: 10.1111/jth.15130
10. Grover SP, Mackman N. Intrinsic pathway of coagulation and thrombosis. Arterioscler Thromb Vasc Biol. (2019) 39:331–8. doi: 10.1161/ATVBAHA.118.312130
11. Wallisch M, Lorentz CU, Lakshmanan HHS, Johnson J, Carris MR, Puy C, et al. Antibody inhibition of contact factor XII reduces platelet deposition in a model of extracorporeal membrane oxygenator perfusion in nonhuman primates. Res Pract Thromb Haemost. (2020) 4:205–16. doi: 10.1002/rth2.12309
12. Yau JW, Liao P, Fredenburgh JC, Stafford AR, Revenko AS, Monia BP, et al. Selective depletion of factor XI or factor XII with antisense oligonucleotides attenuates catheter thrombosis in rabbits. Blood. (2014) 123:2102–7. doi: 10.1182/blood-2013-12-540872
13. Wilbs J, Kong X-D, Middendorp SJ, Prince R, Cooke A, Demarest CT, et al. Cyclic peptide FXII inhibitor provides safe anticoagulation in a thrombosis model and in artificial lungs. Nat Commun. (2020) 11:3890. doi: 10.1038/s41467-020-17648-w
14. Ibanez B, James S, Agewall S, Antunes MJ, Bucciarelli-Ducci C, Bueno H, et al. 2017 ESC Guidelines for the management of acute myocardial infarction in patients presenting with ST-segment elevation. Eur Heart J. (2018) 39:119–77. doi: 10.1093/eurheartj/ehx393
15. Esteban J, de la Morena-Barrio ME, Salloum-Asfar S, Padilla J, Miñano A, Roldán V, et al. High incidence of FXI deficiency in a Spanish town caused by 11 different mutations and the first duplication of F11?: results from the Yecla study. Haemophilia. (2017) 23:e488–96. doi: 10.1111/hae.13356
16. López-Gálvez R, de la Morena-Barrio ME, López-Lera A, Pathak M, Miñano A, Serrano M, et al. Factor XII in PMM2-CDG patients: role of N-glycosylation in the secretion and function of the first element of the contact pathway. Orphanet J Rare Dis. (2020) 15:280. doi: 10.1186/s13023-020-01564-9
17. Schneider CA, Rasband WS, Eliceiri KWNIH. Image to imageJ: 25 years of image analysis. Nat Methods. (2012) 9:671–5. doi: 10.1038/nmeth.2089
18. de Maat S, Björkqvist J, Suffritti C, Wiesenekker CP, Nagtegaal W, Koekman A, et al. Plasmin is a natural trigger for bradykinin production in patients with hereditary angioedema with factor XII mutations. J Allergy Clin Immunol. (2016) 138:1414–23.e9. doi: 10.1016/j.jaci.2016.02.021
19. de Maat S, van Dooremalen S, de Groot PG, Maas C. A nanobody-based method for tracking factor XII activation in plasma. Thromb Haemost. (2013) 110:458–68. doi: 10.1160/TH12-11-0792
20. Corvillo F, de la Morena-Barrio ME, Marcos-Bravo C, López-Trascasa M, Vicente V, Emsley J, et al. The FXII c.-4T>C polymorphism as a disease modifier in patients with hereditary angioedema due to the FXII p.Thr328Lys variant. Front Genet. (2020) 11:1033. doi: 10.3389/fgene.2020.01033
21. Schwarz JM, Cooper DN, Schuelke M, Seelow D. MutationTaster2: mutation prediction for the deep-sequencing age. Nat Methods. (2014) 11:361–2. doi: 10.1038/nmeth.2890
22. Kanaji T, Okamura T, Osaki K, Kuroiwa M, Shimoda K, Hamasaki N, et al. A common genetic polymorphism (46 C to T substitution) in the 5’- untranslated region of the coagulation factor XII gene is associated with low translation efficiency and decrease in plasma factor XII level. Blood. (1998) 91:2010–4.
23. Maas C, Renné T. Coagulation factor XII in thrombosis and inflammation. Blood. (2018) 131:1903–9. doi: 10.1182/blood-2017-04-569111
24. Bravo-Perez C, Ródenas T, Esteban J, de la Morena-Barrio ME, Salloum-Asfar S, de la Morena-Barrio B, et al. Gynaecological and obstetrical bleeding in Caucasian women with congenital factor XI deficiency: results from a twenty-year, retrospective, observational study. Med Clin. (2019) 153:373–9. doi: 10.1016/j.medcli.2019.01.029
25. Preis M, Hirsch J, Kotler A, Zoabi A, Stein N, Rennert G, et al. Factor XI deficiency is associated with lower risk for cardiovascular and venous thromboembolism events. Blood. (2017) 129:1210–5. doi: 10.1182/blood-2016-09-742262
26. Büller HR, Bethune C, Bhanot S, Gailani D, Monia BP, Raskob GE, et al. Investigators. Factor XI antisense oligonucleotide for prevention of venous thrombosis. N Engl J Med. (2015) 372:232–40. doi: 10.1056/NEJMoa1405760
27. Meijers JC, Tekelenburg WL, Bouma BN, Bertina RM, Rosendaal FR. High levels of coagulation factor XI as a risk factor for venous thrombosis. N Engl J Med. (2000) 342:696–701. doi: 10.1056/NEJM200003093421004
28. Yang DT, Flanders MM, Kim H, Rodgers GM. Elevated factor XI activity levels are associated with an increased odds ratio for cerebrovascular events. Am J Clin Pathol. (2006) 126:411–5. doi: 10.1309/QC259F09UNMKVP0R
29. Chen H, Shen M, Niu R, Mu X, Jiang Q, Peng R, et al. Associations of coagulation factor X and XI with incident acute coronary syndrome and stroke: a nested case-control study. J Thromb Haemost. (2021) 19:2781–90. doi: 10.1111/jth.15486
30. Bender L, Weidmann H, Rose-John S, Renné T, Long AT. Factor XII-driven inflammatory reactions with implications for anaphylaxis. Front Immunol. (2017) 8:1115. doi: 10.3389/fimmu.2017.01115
31. Silasi R, Keshari RS, Regmi G, Lupu C, Georgescu C, Simmons JH, et al. Factor XII plays a pathogenic role in organ failure and death in baboons challenged with Staphylococcus aureus. Blood. (2021) 138:178–89. doi: 10.1182/blood.2020009345
32. Naudin C, Burillo E, Blankenberg S, Butler L, Renné T. Factor XII Contact Activation. Semin Thromb Hemost. (2017) 43:814–26. doi: 10.1055/s-0036-1598003
33. Renné T, Stavrou EX. Roles of factor XII in innate immunity. Front Immunol. (2019) 10:2011. doi: 10.3389/fimmu.2019.02011
34. Pauer H-U, Renné T, Hemmerlein B, Legler T, Fritzlar S, Adham I, et al. Targeted deletion of murine coagulation factor XII gene-a model for contact phase activation in vivo. Thromb Haemost. (2004) 92:503–8. doi: 10.1160/TH04-04-0250
35. Lämmle B, Wuillemin WA, Huber I, Krauskopf M, Zürcher C, Pflugshaupt R, et al. Thromboembolism and bleeding tendency in congenital factor XII deficiency–a study on 74 subjects from 14 Swiss families. Thromb Haemost. (1991) 65:117–21. doi: 10.1055/s-0038-1647467
36. Renné T, Pozgajová M, Grüner S, Schuh K, Pauer H-U, Burfeind P, et al. Defective thrombus formation in mice lacking coagulation factor XII. J Exp Med. (2005) 202:271–81. doi: 10.1084/jem.20050664
37. Puy C, Rigg RA, McCarty OJT. The hemostatic role of factor XI. Thromb Res. (2016) 141:S8–11. doi: 10.1016/S0049-3848(16)30354-1
38. Salomon O, Steinberg DM, Zucker M, Varon D, Zivelin A, Seligsohn U. Patients with severe factor XI deficiency have a reduced incidence of deep-vein thrombosis. ThrombHaemost. (2011) 105:269–73. doi: 10.1160/TH10-05-0307
39. Généreux P, Webb JG, Svensson LG, Kodali SK, Satler LF, Fearon WF, et al. Vascular complications after transcatheter aortic valve replacement: insights from the PARTNER (placement of AoRTic TraNscathetER valve) trial. J Am Coll Cardiol. (2012) 60:1043–52. doi: 10.1016/j.jacc.2012.07.003
40. Jimenez Diaz VA, Lozano I, Tello Montoliu A, Baz Alonso JA, Iñiguez Romo A. Is there a link between stroke, anticoagulation, and platelet reactivity?: the multifactorial stroke mechanism following TAVR. JACC Cardiovasc Interv. (2019) 12:2560–1. doi: 10.1016/j.jcin.2019.10.004
41. Jimenez Diaz VA, Tello-Montoliu A, Moreno R, Cruz Gonzalez I, Baz Alonso JA, Romaguera R, et al. Assessment of platelet reactivity after transcatheter aortic valve replacement: the REAC-TAVI trial. JACC Cardiovasc Interv. (2019) 12:22–32. doi: 10.1016/j.jcin.2018.10.005
Keywords: contact pathway, aortic valve replacement, thrombosis, factor XI, factor XII, kallikrein
Citation: de la Morena-Barrio ME, Corral J, López-García C, Jiménez-Díaz VA, Miñano A, Juan-Salvadores P, Esteve-Pastor MA, Baz-Alonso JA, Rubio AM, Sarabia-Tirado F, García-Navarro M, García-Lara J, Marín F, Vicente V, Pinar E, Cánovas SJ and de la Morena G (2022) Contact pathway in surgical and transcatheter aortic valve replacement. Front. Cardiovasc. Med. 9:887664. doi: 10.3389/fcvm.2022.887664
Received: 01 March 2022; Accepted: 07 July 2022;
Published: 22 July 2022.
Edited by:
Avi Leader, Rabin Medical Center, IsraelReviewed by:
Magdolna Nagy, Maastricht University, NetherlandsPablo Codner, Rabin Medical Center, Israel
Copyright © 2022 de la Morena-Barrio, Corral, López-García, Jiménez-Díaz, Miñano, Juan-Salvadores, Esteve-Pastor, Baz-Alonso, Rubio, Sarabia-Tirado, García-Navarro, García-Lara, Marín, Vicente, Pinar, Cánovas and de la Morena. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Gonzalo de la Morena, Z2RsbW9yZW5hQHlhaG9vLmVz; Javier Corral, amF2aWVyLmNvcnJhbEBjYXJtLmVz